surgery ii 3.1a appendix - dr. haw
TRANSCRIPT

7/24/2019 Surgery II 3.1a Appendix - Dr. Haw
http://slidepdf.com/reader/full/surgery-ii-31a-appendix-dr-haw 1/9
Su
Page 1 of 9
Dr. Haw | September 1, 2014
Surgery II Surgery 3.1a Appendix3rd Year1stSe
Group 21 Gabor, Gaerlan, Galan, Galang K., Galang C., Gammad
OUTLINE
I. Acute Appendicitis
II. Acute Appendicitis in Special Populations
III. Meckel’s Diverticulum
IV. V. Appendiceal Tumors
Resources: Recording, PowerPoint, Schwartz and Sabiston (Dr. Haw got most of it
from Sabiston though)
I. ACUTE APENDICITITS
A. Epidemiology
Most commonly encountered acute surgical condition of the
abdomen.
o 1% of all operations is due to acute appendicitis
o 10/10000 patients every year
Appendicitis according to type:
o 15% -normal
o
20% - perforated
o 65% - acute
Appendicitis according to age:
o Most common during the 2nd to 4th decade of life
Mean age of 31.3 years
Median at 23 years
o
Less common among extremes of age
o But can occur at any time in your life up to the age of 90
But in the elderly, the appendiceal lumen is already
closed and scarred and so fecalith don’t obstruct it and
they rarely develop appendicitis.
Appendicitis according to gender:
o M:F ratio is 1.2:1
o Lifetime risk for Males: 8.6%
o
Lifetime risk for Females: 6.7%
Misdiagnosis
o Rate of misdiagnosis and rate of appendicle rupture is 15.3%
o Percentage of misdiagnosis is higher in females (22.9%) than
men (9.3%) respectively.
Appendectomy
o
Lifetime rate for appendectomy: 17%
o
Men: 12%
o Women: 25%
Negative Appendectomy
o The highest negative appendectomy rate among women of
reproductive age is 23.2%, highest in the 4th decade (40-49
years old)
This is why we often ask for a gynecologic clearance for
this age group. Rate of misdiagnosis is higher and it
could be a primarily gynecologic problem.
The highest negative appendectomy rate is reported for
women >80 years of age (this is for women overall)
Summary: the typical patient will be a male in his 20s or 30s
presenting with an acute abdomen but an appendectomy is more
often performed among women and the chances for a misdiagnosis
is higher especially among women in their 40s.
B. Etiology
Obstruction of the lumen of the appendix due to:
o
Fecalith is most common
40% of simple appendicitis
65% of gangrenous appendicitis
90% of perforated appendicitis
o
Hypertrophy of lymphoid tissue
More common in young patients because it degenerates
in teenage years
o
Inspissated barium from previous x-ray studies
o
Tumors
o Vegetable and fruit seeds
o
Intestinal parasites like ascariasis
Frequency of obstruction rises with the severity of the
inflammatory process.
C. Pathophysiology
The lumen of the appendix only has a luminal capacity of 0.1 mwhich is small in relation to its length
o This configuration may predispose to closed-loop
obstruction
o Fecalith and other debris lodge into the appendiceal lumen
and build up over time
o As little as 0.5mL of fluid distal to an obstruction raises
intraluminal pressure to 60cm H2O.
Obstruction contributes to bacterial overgrowth and despite
this, the appendix continues its function: mucus secretion
Both bacterial overgrowth and continuous mucus secretion lead
to intraluminal distention and increased wall pressure which
leads to:
o Stimulation of nerve endings of visceral afferent stretch
fibers production of vague, dull, diffuse visceral pain thatis sensed in the mid abdomen or lower epigastrium or
periumbilical region
o
Reflex nausea and vomiting
o Subsequent impairment of lymphatic (affected earlier) and
venous drainage leads to mucosal ischemia
But arterial inflow continues, resulting in engorgement and
vascular congestion
Later on there will be arterial compromise as well,
contributing to perforation
Peristalsis also stimulated by rather sudden distention so
that some cramping may be superimposed on the viscera
pain early in the course of appendicitis.
Inflammation later on involves the serosa of the appendix and
later the parietal peritoneumo This produces characteristic shift in pain to the right lowe
abdomen
The mucosa of the appendix is susceptible to impairment o
blood supply; thus, its integrity is compromised early in the
process, which allows bacterial invasion.
o Ellipsoidal infarcts: develop in the antimesenteric border
area with the poorest blood supply

7/24/2019 Surgery II 3.1a Appendix - Dr. Haw
http://slidepdf.com/reader/full/surgery-ii-31a-appendix-dr-haw 2/9
Surgery II 3.1a
Page 2 of 9
Figure 1. Factors leading to Perforation.. As distension, bacterial invasion,
compromise of the vascular supply, and infarction progress, perforation
occurs, usually on the antimesenteric border just beyond the point of
obstruction. This sequence is not inevitable, however, and some episodes of
acute appendicitis may resolve spontaneously.
Figure 2. Plain abdomen where a fecaltih can appreciated in the RLQ.
D. Microbiology
Bacteria present in the appendix is similar to those found in the
colon
o Anaerobes are most prominent!
The principal organisms that are seen in the normal appendix, in
acute appendicitis, and in perforated appendicitis are
Escherichia coli and Bacteroides fragilis, with the latter present
in greatest amounts
2nd Gen Cephalosporin and Metronidazole = first line defense
o The antibiotic coverage should include coverage for gram
positive, gram negative, and anaerobes.
o Clindamycin is rarely used because it is a causative factor of
pseudomembranous colitis
Table 1. Common Organisms seen in Patients with Acute Appendicitis
Aerobic & Facultative Anaerobic
Gram Negative
Bacilli
Escherichia coli
Pseudomonas
aeruginosa
Klebsiella sp.
Bacteroides fragilis
Other Bacteroides sp.
Fusobacterium sp.
Gram Positive
Cocci
Streptococcus
anginosus
Other Streptococcus sp.
Enterococcus species
Peptostreptococcus sp.
Gram Positive
Bacilli
Clostridium sp.
E. Symptoms
Pain usually begins as epigastric pain or periumbilical area
followed by nausea with or without vomiting
Classic localized appendicitis usually shifts to RLQ in 8 hours,
o Classic history (pain shift) only happens in about 45% of
patients and often in young males
o This again is due to irritation of the parietal peritoneum
Nausea and vomiting usually occurs AFTER onset of pain.
o
N&V is the most common associated symptom occurring in70-80% of patients
o Vomiting present only in 75% of cases
o
Gastrointestinal symptoms that develop before the onset of
pain suggest a different etiology such as gastroenteritis
Anorexia is almost always present.
Anorexia nearly always accompanies appendicitis. So
constant in fact the diagnosis of appendicitis is questioned o
the patient is not anorectic.
ABDOMINAL PAIN ANOREXIA VOMITING sequence
observed in 95% of patients with acute appendicitis
Variations:
o Sometimes pain begins in the RLQ
o
Elderly patients are difficult to diagnose due to atypical
presentation, expanded differential diagnosis and
communication difficulty (use ancillary work up like CT scan)
o Very young patients usually present with perforation.
Newborns present with generalized peritonitis because
the omentum has not developed yet to localize the
infection
o
Constipation and diarrhea - not very helpful although
majority will complain of constipation
F. Signs / Physical Exam
General Survey & Vital Signs
o
Walk slowly, prefer to lie supine due to peritoneal irritation
o Temperature is normal or mild early on
o
Pulses may also be normal or slightly elevated Pain
o Need to ask the patient to point to the area of maximal
tenderness using only one finger. Area where the patient
points is usually in the area of the appendix.
o But remember that 10-15% of patients have an appendix
located in the pelvic area will have a positive recta
examination.
Tenderness
o RLQ tenderness (often maximal at or near the McBurney’s
point)
o Direct tenderness – elicited via palpation
o
Indirect tenderness – elicited via Rovsing’s sign
o Voluntary muscle guarding - early in the disease process.
o
Involuntary muscle guarding – due to peritoneal irritationand increased muscle spasm
Signs of Peritoneal Irritation
o Cough (Dunphy’s sign), walking, bouncing
o
Tenderness is maximal at McBurney’s point at the RLQ
o
Muscular resistance or Guarding in the right iliac fossa
o
Rebound tenderness when the examiner’s hand is quickly
relieved
o Indirect tenderness or Rovsing’s sign is pain in the right
lower quadrant when the left lower quadrant is palpated
o Psoas Sign and Obturator Sign
Perforation
Distention
BacterialInvasion
CompromisedVascularSupply
Infarction
(Ellipsoidal)

7/24/2019 Surgery II 3.1a Appendix - Dr. Haw
http://slidepdf.com/reader/full/surgery-ii-31a-appendix-dr-haw 3/9
Surgery II 3.1a
Page 3 of 9
Figure 3. Psoas Sign
o Irritative focus in proximity to psoas muscle
o
Patient lie in the left side as the examiner slowly extends the
patient’s right thigh, thus stretching the psoas muscle.
o
Positive when extension produces pain.
Figure 4. Obturator Sign
o Pain upon stretching of the obturator internus muscle via
internal rotation of a flexed thigh
o Suggests inflammation near the muscle
Remember that your decision to operate will be based on your
Physical Exam. Patient with history and associated signs and
symptoms should be operated on.
G. Variability in Presentation
Table 2. Variations in the Presentation of Acute Appendicitis
Location of Appendix Location of Pain
Classic appendicitis presentation RLQ
Long appendix with tip at the LLQ LLQ
Retrocecal appendix Flank or back
Pelvic appendix Suprapubic area
Pelvic appendix with irritation of the
urinary bladder
Hypogastric area
Retroileal appendix with irritation of
spermatic artery and ureter
Testicular area
The visceral component is in the normal location
The somatic component is felt in that part of the abdomen
where the cecum has been arrested in rotation.
Remember that there is about a 10%-15% margin of error. A
disease that can commonly present as appendicitis is acute
mesenteric adenitis. In the event that you already opened up the
patient and see that the cause of RLQ is mesenteric adenitis, you
can still do an incidental appendectomy since appendicitis can
occur anytime during your lifetime.
It is also important to examine the male genitalia because there
has been incidences where they found an incarcerated inguinal
hernia, rule this out.
H. Laboratory Findings
Appendicitis is associated with an inflammatory response that is
strongly related to the severity of the disease. Laboratory
examinations are therefore an important part of the diagnosis.
WBC
o
Mild to moderate leukocytosis with a SHIFT TO THE LEFT is
the rule
Less than 4% will have normal leukocyte count (more
often seen in the elderly)o Acute uncomplicated appendicitis: mild leukocytosis
(10,000-18,000 cells/mm3) with PMN predominance
o Perforated appendix with or without abscess: >18,000
o
Complicated appendicitis: increased C-reactive protein
concentration
o Sepsis: WBC may be low due to sepsis but neutrophils will be
proportionately higher
o Appendicitis is very unlikely if the white blood cell count,
proportion of neutrophils, and CRP are normal
Urinalysis
o Important in differential diagnosis if with significant number
of RBC, WBC and bacteria to rule out UTI.
o Acute pyelonephritis, on the right side particularly, may
mimic a retroileal acute appendicitis
I. Clinical Scoring Systems
The Alvarado score
o The most widespread scoring system
o Especially useful for ruling out appendicitis and selecting
patients for further diagnostic workup.
The Appendicitis Inflammatory Response Score
o Resembles the Alvarado score but uses more graded
variables and includes CRP
o Studies have shown it to perform better than the Alvarado
score in accurately predicting appendicitis.
However, clinical scoring systems have not gained widespread
acceptance in making the diagnosis of appendicitis Remember that most of the time the diagnosis and treatment of
appendicitis will be based on your clinical findings!
J. Radiography
Plain abdomen
o Presence of fecalith and fecal loading in the cecum
o But are rarely useful for diagnosing acute appendicitis
o
Benefit is that it will help rule out other causes:
Pneumoperitonium - operate on the patient based on
ruptured viscous.
Segmental ileus - you will see small amount of dilated
small bowel called sentinel loop.
Obliteration of psoas shadow – psoas on the right is not
as clear as the left.
Chest X-Ray
o
Sometimes called to rule out referred pain from a right
lower lobe pneumonic process.
Barium enema in selected patients
o If appendix fill on barium enema then appendicitis can be
excluded.
o If appendix does not fill, no conclusion can be made.
o
Not indicated in the acute setting

7/24/2019 Surgery II 3.1a Appendix - Dr. Haw
http://slidepdf.com/reader/full/surgery-ii-31a-appendix-dr-haw 4/9
Surgery II 3.1a
Page 4 of 9
K. Graded Compression Ultrasonography
Technique is inexpensive, performed rapidly, does not require
contrast medium, and can be used in pregnant patients.
85% inflamed appendix, may rule out pelvic disease,
gynecological problems and enlarged mesenteric lymph nodes.
Appendix can be seen as a blind ending pouch originating from
the cecum. Results are considered positive if appendix measure
>6mm in the anterior posterior direction. Presence of an
appendicolith establishes diagnosis. In females of childbearing age, pelvic organs must be adequately
visualized either by transabdominal or endovaginal ultrasound
to exclude gynecologic pathology as a cause of acute abdominal
pain. Has a sensitivity of 55-96% and specificity of 85-98%
Disadvantages:
o Results are user dependent and false positives have been
reported
o False positives include periappendicits from surrounding
inflammation, dilated fallopian tube, inspissated stool which
can mimic appendicitis.
o Obese patients, the appendix may not be compressible
because of overlying fat.
Figure 5: Ultrasound showing acute appendicitis. 85% of ultrasounds done
in the RLQ will diagnose acute appendicitis. Can appreciate the lumen of the
appendix, thickened walls, and appendicolith.
Figure 6: Another ultrasound done in the longitudinal view showing similar
findings as figure 4.
Figure 7: Older generation CT scan, but can still see a markedly thickened
appendix.
L. High Resolution CT scan
Lower rates of negative appendectomy from 19% - 12%
Decreased negative appendectomies in women from 24% to 5%
Altered the care of 24%
Provided alternative diagnosis in 50%
Excellent technique for identifying other inflammatory processes
masquerading as acute appendicitis.
Appendix can perforate as early as 18 hours from onset of
symptoms.
Study done Massachusetts General Hospital where CT was done
for all patients with abdominal pain. Results showed:
o Reduced negative appendectomy from 20 to 7%
o Reduced perforation from 22% to 14%
In U.S. routinely done by ER Physicians before referred to
surgeons
Disadvantages:
o
Expensive
o Exposes the patient to significant radiation
o
Cannot be used during pregnancy
o Allergy to dye is a contraindication and some patients
cannot take oral ingestion of luminal dye due to nausea andvomiting.
Figure 8: High resolution CT scan showing dilated appendix >5cm, thickened
walls, evidence of inflammation, “dirty fat”, thickened mesoappendix,
phlegmon, fecaliths, and arrowhead sign. (Arrowhead sign is caused by
thickening of the cecum which funnels contrast agent toward the orifice of
the inflamed appendix)

7/24/2019 Surgery II 3.1a Appendix - Dr. Haw
http://slidepdf.com/reader/full/surgery-ii-31a-appendix-dr-haw 5/9
Surgery II 3.1a
Page 5 of 9
Figure 9. CT scan showing a cecal mass masquerading as an acute process.
Can also be a tuberculoma or other inflammatory conditions.
From Schwartz
The rational approach is the selective use of CT scanning. The
likelihood of appendicitis can be ascertained with the use of the
Alvarado Scale. This helps improve the diagnosis of appendicitis, by
giving weight to specific clinical manifestations.
See the appendix for Alvarado Scale and its scoring system
M. Differential Diagnosis
Essentially as diverse as that of the acute abdomen
The differential diagnosis depends upon 4 major factors:
o The anatomic location of the inflamed appendix
o
Stage of the process (e.g. simple or ruptured)
o Age of the patient
o Patient’s sex
75% includes:
o
Mesenteric adenitis
o No organic pathology seen
o
PID (pelvic inflammatory disease)
o IBD (Inflammatory bowel disorder)
Crohn’s disease – most common site is at the terminal
ileum , if you open up the patient and you see terminal
ileitis. If there’s no obstruction, do not biopsy it due to
propensity to fistulize. If the appendix is normal then
perform an incidental appendectomy. If the cecum is
involved, leave the appendix behind.
o Twisted Ovarian Cyst, Mittelschmerz
Mittelschmerz occurs in females in midcycle, pain is
caused by the irritation of the blood from the ruptured
Graafian follicle
o
Acute gastroenteritis
o Typhoid Ileitis
Other differentials:
o
PUD
o
Males: Testicular torsion, epididymitiso UTI, hernias (incarcerated)
o Meckel’s diverticulitis
o Diverticulitis
o
Ureteral colic
N. Interval Appendectomy
Done 6 to 8 weeks after the presentation of symptoms
Lower morbidity and mortality than immediate appendectomy
Greater expenses and longer hospitalization time
Failure rate is 9-15%
Major argument: 50% of patients undergoing initial conservative
treatment never develop surgical manifestations.
Non-operative option may still be applicable to those with
recurrence of appendicitis
Supporting evidences:
o 40% needed appendectomy at an earlier mean time (4.3
weeks)
o Rate of late failure: 20%
o
Continue to have recurrence: 14%
o Persistent peri-appendiceal abscess: 90%
o
Pathologic findings of acute appendicitis: 50%o Neoplasm?
Not done anymore, but in earlier times when there is a
periappendiceal abscess they treat with massive antibiotics then
after a month or two they perform an interval appendectomy
O. Rupture of the Appendix
Infection contained - soft tender mass, if you have a very
competent omentum it will cover the rupture and will have
periappendiceal abscess or if localized deep peritonitis.
o Involuntary guarding
o Rebound tenderness more marked
o Elevated temperature, tachycardia
Fails to localize - diffuse peritonitis
o
Patients
o Tenderness and guarding becomes generalized
o Temperature spikes
o
Tachycardia >100 beats per minute
From Schwartz
Immediate appendectomy has been long recommended treatment
for acute appendicitis because of the presumed risk of rupture.
Rates of perforation is 25.8%
o Children under 5 years old and >65years have the highest rates of
perforation.
Recent studies suggest that in selected patients, observation and
antibiotic therapy alone may be an appropriate treatment for acute
appendicitis.
Rupture occurs most frequently distal to the point of luminal
obstruction along the antimesenteric border of the appendix.
In 2-6% of cases and ill-defined mass is detected on PE which could
represent a phlegmon which consists of matted loops of bowel
adherent to the adjacent inflamed appendix or periappendiceal
abscess. Patients with this presentation will have experienced
symptoms for a longer duration, at least 5-7 days.
Phlegmon and small abscess can be treated conservatively with IV
antibiotics; well localized abscesses can be managed with
percutaneous drainage; complex abscess should be considered for
surgical drainage.
P. Complications
Occur in 5% of unperforated appendicitis cases, and 30% o
perforated appendicitis cases
Complications include:o
Wound infection (Surgical Site Infection) – most common
side effect
o
Intraabdominal abscess – due to break in technique
o Fecal fistula – usually secondary to a slip in the tie of the
appendiceal stub
o
Pyephlebitis – portal pyemia, does not occur anymore due
to antibiotics
o
Intestinal obstruction – occurs later on
o
Prolonged ileus
o
Pulmonary embolism

7/24/2019 Surgery II 3.1a Appendix - Dr. Haw
http://slidepdf.com/reader/full/surgery-ii-31a-appendix-dr-haw 6/9
Surgery II 3.1a
Page 6 of 9
Q.
Prognosis
Mortality rate: 0.2/100,000 appendectomies,
o 1% with rupture in general
o
5% with rupture in the elderly
Mortality is mostly seen in the extremes of ages
Principal Factor: Perforation, Age
o Morbidity parallels mortality rates
o It is significantly higher with ruptured appendicitis or old
age!
Death due to uncontrolled sepsis:
o Peritonitis
o Intra-abdominal abscess
o Gram negative septicemia
Figure 10. Laparoscopic appendectomy. Appendix is congested and
slightly enlarged or inflamed.
Figure 11. Open appendectomy. If the appendiceal stub slips off, a fecal
fistula may form and if it spreads, patient may present with peritonitis.
I. APPENDICITIS IN SPECIAL POPULATIONS
A. Appendicitis in the Young
More serious – 50-80% in pre-school children
o Higher rate of and rapid progression to rupture
o Mortality rate as high as 5%
o Later diagnosis – inability of young children to give an
accurate history and frequency of GI upsets in children
o
In one series 40% already seen by physician <1 year old
o
Rupture frequently diffuse because of a less developed
omentum – almost 100%
<5 years old
o negative appendectomy rate – 25%
o perforation rate – 45%
5-12 years old
o
negative appendectomy rate - <10%
o perforation rate – 20%
PE findings:
o Maximal tenderness in the RLQ, the inability to walk or
walking with a limp, and pain with percussion, coughing, and
hopping were found to have the highest sensitivity for
appendicitis.
o
Abdominal distension most consistent
Incidence of major complications after appendectomy in
children is correlated with appendiceal rupture
Management:o We have to operate, you cannot afford not to.
o For perforated appendicitis – generally includes immediate
appendectomy and irrigation of the peritoneal cavity. IV
antibiotics usually are given until the WBC count is norma
and the patient is afebrile for 24 hours.
o
For non-perforated appendicitis – antibiotic coverage is
limited to 24 to 48 hours.
o Laparoscopic appendectomy has been shown to be safe and
effective for the treatment of appendicitis in children.
B. Appendicitis in the Elderly
Similar but less pronounced symptomatology (since perception
of pain becomes lesser as we age)
o
30% have rupture during surgery
o Delay in diagnosis because of atypical presentation,
expanded differential diagnosis and communication
difficulty
Usually presents with lower abdominal pain, and localized RLQ
tenderness is present in only 80-90% of patients. Periumbilica
pain migrating to the RLQ is reported infrequently.
Increased comorbidities and increased rate of perforation (50
70%); postoperative morbidity, mortality and hospital length o
stay
Management: benefit more from laparoscopic approach –
reduction in complications
C.
Appendicitis during Pregnancy 1 in 2000
Most common surgical emergency in pregnancy
o
Appendicitis in pregnancy should be suspected when a
pregnant woman complains of abdominal pain of new
onset. The most consistent sign is pain in the right side of
the abdomen
Should be operated on as in non-pregnant
Displacement laterally during third trimester
Omentum also displaced cephalad
A higher rate of negative appendectomy is seen in the 2 n
trimester, and the lowest rate is in the 3rd trimester
o Difficulty attributed to the diversity of clinical presentation
secondary to the anatomic changes in the location of the
appendix during pregnancy and increased abdominal laxity.
Diagnosis is Clinical
o When diagnosis is in doubt, abdominal ultrasound may be
beneficial
o
Graded Compression Sonography
Accurate way to establish the diagnosis of appendicitis
Safe for children and pregnant women
Blind-ending nonperistaltic bowel loop originating from
the cecum
Noncompressible appendix >6mm (AP dimension)
Presence of appendicolith
Thickening of appendiceal wall

7/24/2019 Surgery II 3.1a Appendix - Dr. Haw
http://slidepdf.com/reader/full/surgery-ii-31a-appendix-dr-haw 7/9
Surgery II 3.1a
Page 7 of 9
Figure 12. (Left) Graded Compression Sonography of appendix; (Right) Acute
appendicitis in pregnancy
Management
o Incision will now be different. Usually, the appendix is more
lateral because it is being pushed by the uterus, and goes
higher in the abdomen as the baby grows.
o But you still have to ask where the point of maximal
tenderness is.
II. MECKEL’S DIVERTICULUM
A.
Introduction
When you do your appendectomy, examine the distal 2/5ths of
your small intestine because 2% will have Meckel’s diverticulum
Most prevalent congenital anomaly of the GIT
REMEMBER THE RULE OF 2’S!
o 2% prevalence rate
o
2:1 Female:Male ratio
o Located 2 ft. from the ileocecal valve
o
Symptoms: <2 years of age
The most common cause of bleeding in 2 year olds is Meckel’s
diverticulum, due to the presence of gastric mucosa in the
diverticulum. Small intestines cannot tolerate the acidic content
and it leads to bleeding
60% contains heterotopic mucosa, of which 60% consists of
gastric mucosa
o
Next most common is the presence of pancreatic acini
o Others:
Brunner’s glands
Pancreatic islets
Colonic mucosa
Endometriosis
Hepatobiliary tissue
in Meckel’s diverticulum, only the mucosa is involved versus
Crohn’s disease wherein all layers are involved given that it’s
intramural
B. Pathophysiology
Normally, at the 8th week of gestation the omphalomesenteric(vitelline) duct normally undergoes obliteration
Meckel’s diverticulum arises from the failure of vitelline duct
obliteration
Other abnormalities include:
o Omphalomesenteric fistula
o Enterocyst
o Fibrous band connecting the intestine to the umbilicus
o
Mesodiverticular band- remnant of left vitelline artery
Bleeding – secondary to heterotropic gastric mucosa located
within the diverticulum; the intestines cannot tolerate the high
acidity of the gastric mucosa
Obstruction can result from either of the following:
o
Volvulus of the intestine around the fibrous band attaching
the diverticulum to the umbilicus
o
Entrapment of intestine by a mesodiverticular band
o Intussusception with the diverticulum acting as a lead point
o
Stricture secondary to chronic diverticulitis
Figure 13. Picture of a resected Meckel’s diverticulum
C. Clinical Presentation
Usually presents asymptomatically
Lifetime incidence of complications is 4-6% and this does no
change with age
o
Very low complication rate. Not routinely removed becausethere may be more complications if you remove it electively.
Can present with:
o Bleeding – most common presentation in children. Rare
among those 30 y.o and older
o Intestinal obstruction – most common presentation in adults
o Diverticulitis – indistinguishable from acute appendicitis
D. Diagnosis
Majority are incidental findings on radiographic imaging
endoscopy, or at the time of surgery
It is rarely diagnosed pre-operatively, unless there is bleeding
CT Scan – has low sensitivity
EnterocolysiS – 75% accuracy, not applicable in acutepresentation
Radionuclide Scans – positive only when ectopic gastric mucosa
is capable of uptake of tracer, 90% accurate in pediatric patients
but less than 50% accurate in adults
Angiography – used to localize the bleeding
Figure 14. Radionuclide scan diagnosing Meckel’s diverticulum. It has
affinity for gastric cells. You can see absorption of the radionuclide material
(green arrow), which is a Meckel’s diverticulum.
7/24/2019 Surgery II 3.1a Appendix - Dr. Haw
http://slidepdf.com/reader/full/surgery-ii-31a-appendix-dr-haw 8/9
Surgery II 3.1a
Page 8 of 9
E. Treatment
Diverticulectomy with removal of associated bands
Segmental resection of ileum that includes both the
diverticulum and the adjacent ileal peptic ulcer for:
o Bleeding
o
Diverticulum contains tumor
o Inflamed or perforated base
Treatment in asymptomatic cases is controversial
o
This condition usually has a low complication rate and morecomplications may arise if you operate on this.
o If you do an appendectomy and you have an incidental
finding of Meckel ’ s, you may leave it alone and just note it
for future procedures
An indication for surgery is obstruction.
III.
APPENDICEAL TUMORS
Appendiceal malignancies are extremely rare
o Diagnosed in 0.9 to 1.4% of appendectomy specimens
o
0.12 cases/1,000,000 people
Rarely diagnosed pre-operatively
o Fewer than 50% are diagnosed at operation
Carcinoid – most common (>50%) appendiceal malignancyo Mucinous adenocarcinoma – 38%
o
Adenocarcinoma – 26%
o Carcinoid – 17%
o Goblet cell CA – 15%
o Signet Ring CA – 4%
Survival
o Carcinoid – 83% 5 year survival
o
Signet Ring – 18% 5 year survival
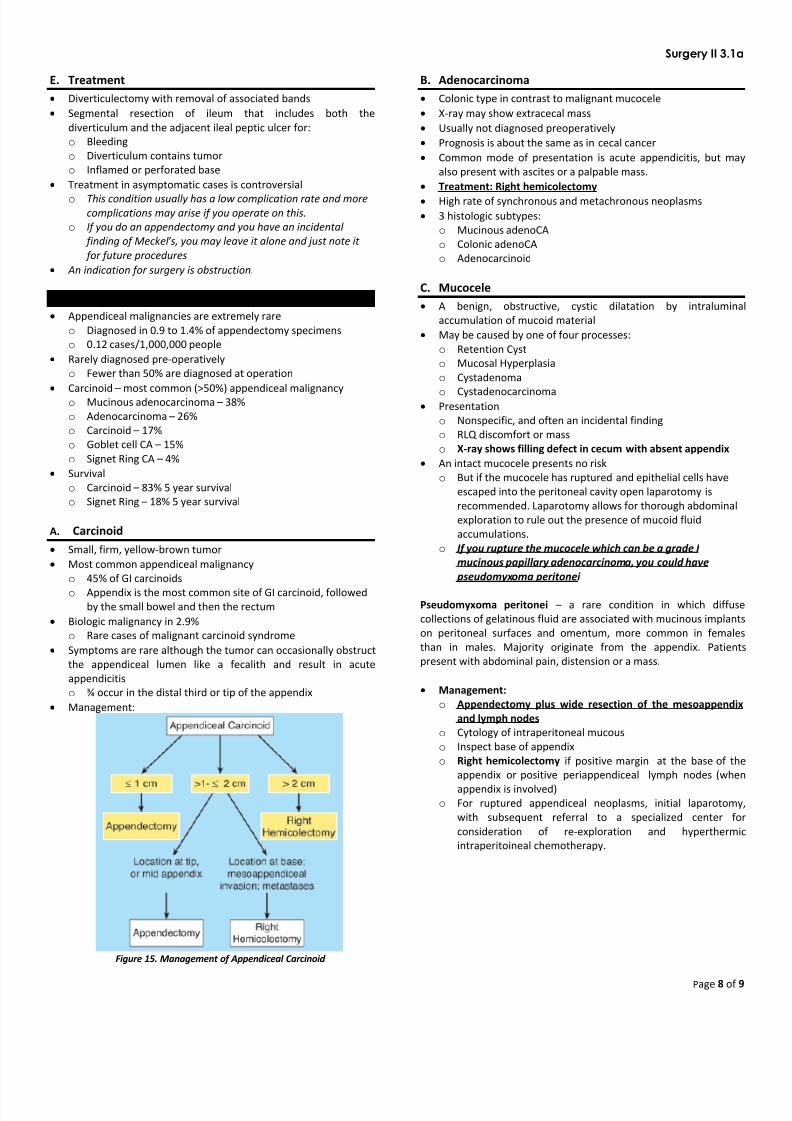
A. Carcinoid
Small, firm, yellow-brown tumor
Most common appendiceal malignancy
o 45% of GI carcinoids
o
Appendix is the most common site of GI carcinoid, followedby the small bowel and then the rectum
Biologic malignancy in 2.9%
o
Rare cases of malignant carcinoid syndrome
Symptoms are rare although the tumor can occasionally obstruct
the appendiceal lumen like a fecalith and result in acute
appendicitis
o
¾ occur in the distal third or tip of the appendix
Management:
Figure 15. Management of Appendiceal Carcinoid
B. Adenocarcinoma
Colonic type in contrast to malignant mucocele
X-ray may show extracecal mass
Usually not diagnosed preoperatively
Prognosis is about the same as in cecal cancer
Common mode of presentation is acute appendicitis, but may
also present with ascites or a palpable mass.
Treatment: Right hemicolectomy
High rate of synchronous and metachronous neoplasms
3 histologic subtypes:
o Mucinous adenoCA
o Colonic adenoCA
o Adenocarcinoid
C. Mucocele
A benign, obstructive, cystic dilatation by intralumina
accumulation of mucoid material
May be caused by one of four processes:
o Retention Cyst
o Mucosal Hyperplasia
o Cystadenoma
o
Cystadenocarcinoma Presentation
o
Nonspecific, and often an incidental finding
o RLQ discomfort or mass
o X-ray shows filling defect in cecum with absent appendix
An intact mucocele presents no risk
o
But if the mucocele has ruptured and epithelial cells have
escaped into the peritoneal cavity open laparotomy is
recommended. Laparotomy allows for thorough abdominal
exploration to rule out the presence of mucoid fluid
accumulations.
o If you rupture the mucocele which can be a grade I
mucinous papillary adenocarcinoma, you could have
pseudomyxoma peritonei
Pseudomyxoma peritonei – a rare condition in which diffuse
collections of gelatinous fluid are associated with mucinous implants
on peritoneal surfaces and omentum, more common in females
than in males. Majority originate from the appendix. Patients
present with abdominal pain, distension or a mass.
Management:
o
Appendectomy plus wide resection of the mesoappendix
and lymph nodes
o
Cytology of intraperitoneal mucous
o Inspect base of appendix
o
Right hemicolectomy if positive margin at the base of the
appendix or positive periappendiceal lymph nodes (when
appendix is involved)o For ruptured appendiceal neoplasms, initial laparotomy
with subsequent referral to a specialized center fo
consideration of re-exploration and hyperthermic
intraperitoineal chemotherapy.

7/24/2019 Surgery II 3.1a Appendix - Dr. Haw
http://slidepdf.com/reader/full/surgery-ii-31a-appendix-dr-haw 9/9
Surgery II 3.1a
Page 9 of 9
D. Lymphoma
The GI tract is the most frequently involved extranodal site for
Non-Hodgkin’s lymphoma
Primary lymphoma of the appendix accounts for 1-3% of GI
lymphomas
Presentation: Acute Appendicitis
CT scan: Appendiceal diameter >2.5cm or surrounding soft tissue
thickening
Management
o Localized to appendix: Appendectomy
o Extends beyond the appendix onto the cecum or mesentery:
Right Hemicolectomy
o A post-operative staging workup is indicated before
initiating adjuvant therapy. Adjuvant therapy is not indicated
for lymphoma confined to the appendix.