summer 2005.qxd - anesthesia patient safety foundation
TRANSCRIPT
Inside: MH News ................................Pages 30-31
Descending Bellows(Dear SIRS)..............................Page 34
Syringe Reuse Transmits Infection ..............Page 37
Safety Implications of JCAHO Standards..................Page 38
Donors ..........................................Page 39
NEWSLETTERVolume 20, No. 2, 25-44 Circulation 75,648 Summer 2005
www.apsf.org The Official Journal of the Anesthesia Patient Safety Foundation
by Michael A. Olympio, MD
There is increasing evidence that exposure ofvolatile anesthetics to desiccated carbon dioxideabsorbents may result in exothermic reactions lead-ing to fires in anesthetic breathing circuits and pro-duction of toxic products (e.g., carbon monoxide,compound A, methanol, formaldehyde). Althoughfires have only been reported in association withsevoflurane exposed to desiccated Baralyme®
(Allied Healthcare/Chemetron, withdrawn from themarket), there is significant evidence that potentiallytoxic products can be produced upon exposure ofvolatile anesthetics to other desiccated absorbentscontaining strong bases, particularly potassium andsodium hydroxide. In some cases this may lead tosub-clinical carbon monoxide exposure.
In view of these continued anesthesia patientsafety concerns, the Anesthesia Patient Safety Foun-dation invited medical experts and industry repre-sentatives (manufacturers of carbon dioxideabsorbents, anesthesia machines, and volatile anes-thetics) to attend a conference entitled Carbon Diox-ide Absorbent Desiccation: APSF Conference on SafetyConsiderations on April 27, 2005, in Chicago, IL. Inaddition to medical experts and industry represen-tatives (Table 1), APSF invited several organiza-tions, including the American Society ofAnesthesiologists and the American Association ofNurse Anesthetists to send observers to the confer-ence (Table 2). The conference was funded by theAnesthesia Patient Safety Foundation with the sup-port of unrestricted educational grants from the 10industry cosponsors.
The format of the conference included formalpresentations by the 4 medical experts as well as pre-sentations by representatives of industry. Followingreports generated from small group break-out ses-sions there was general discussion among all atten-dees and development of a consensus statement toreflect the stated goal of the conference, which was“to develop a consensus statement to share withanesthesia professionals on the use of carbon dioxideabsorbents so as to reduce the risk of adverse inter-actions with volatile anesthetic drugs.”
Summary of Expert Medical and Industry Representative
PresentationsJerry A. Dorsch, MD, speaking on Anesthesia
Machine Characteristics That Promote Absorbent Desiccation:
The retrograde flow of fresh gas through theabsorber can desiccate the absorbent. This may beaffected by a number of factors, including thedesign of the anesthesia breathing system, the pres-ence or absence of the reservoir bag, whether theAPL valve is open or closed, the relative resistancethrough the components of the breathing circuit,the fresh gas flow rate, I:E ratio, use of heat andmoisture exchangers, and scavenger suction. Withconventional breathing system design, removingthe bag, opening the APL valve, and occluding theY-piece all enhance retrograde flow and desicca-tion. The effects of these maneuvers in newer, moremodern machines are variable, complex, and mayhave the opposite effect. Furthermore, we do notknow of published data that describe the flow ofgas under these various conditions. Unfortunately,the flow of gas in these breathing systems has notbeen well studied.
®
See “Absorbents,” Page 27
Carbon Dioxide Absorbent DesiccationSafety Conference Convened by APSF
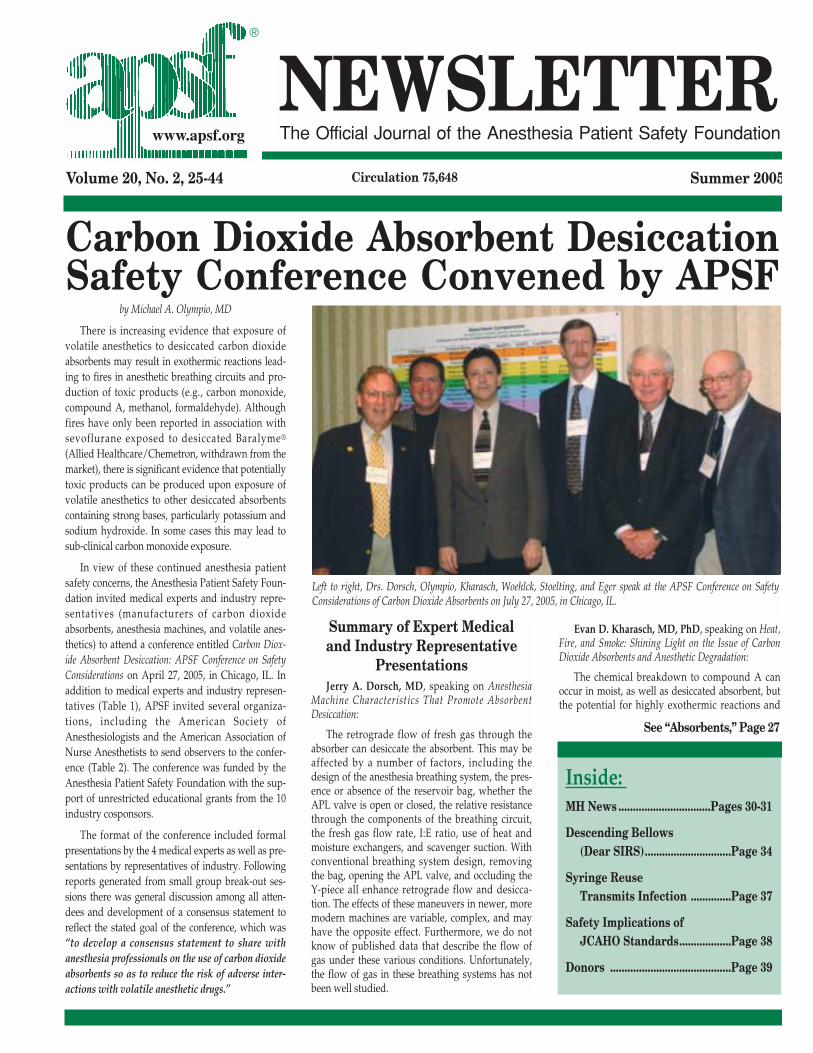
Left to right, Drs. Dorsch, Olympio, Kharasch, Woehlck, Stoelting, and Eger speak at the APSF Conference on SafetyConsiderations of Carbon Dioxide Absorbents on July 27, 2005, in Chicago, IL.
Evan D. Kharasch, MD, PhD, speaking on Heat,Fire, and Smoke: Shining Light on the Issue of CarbonDioxide Absorbents and Anesthetic Degradation:
The chemical breakdown to compound A canoccur in moist, as well as desiccated absorbent, butthe potential for highly exothermic reactions and

APSF NEWSLETTER Summer 2005 PAGE 26
The Anesthesia Patient Safety FoundationNewsletter is the official publication of thenonprofit Anesthesia Patient Safety Foundationand is published quarterly at Wilmington,Delaware. Annual member-ship: Individual -$100.00, Corporate - $1,000.00. This and anyadditional contributions to the Foundation are taxdeductible. © Copyright, Anesthesia Patient SafetyFoundation, 2005.
The opinions expressed in this Newsletter arenot necessarily those of the Anesthesia PatientSafety Foundation or its members or board ofdirectors. Validity of opinions presented, drugdosages, accuracy, and completeness of content arenot guaranteed by the APSF.
APSF Executive Committee:
Robert K. Stoelting, MD, President; Jeffrey B.Cooper, PhD, Executive Vice President; George A.Schapiro, Executive Vice President; David M.Gaba, MD, Secretary; Casey D. Blitt, MD,Treasurer; Sorin J. Brull, MD; Robert A. Caplan,MD; Nassib G. Chamoun; Robert C. Morell, MD;Michael A. Olympio, MD; Richard C. Prielipp, MD.
Newsletter Editorial Board:
Robert C. Morell, MD, Editor; Sorin J. Brull,MD; Joan Christie, MD; Jan Ehrenwerth, MD; JohnH. Eichhorn, MD; Regina King; Lorri A. Lee, MD ;Rodney C. Lester, PhD, CRNA; Glenn S. Murphy,MD; Denise O’Brien, BSN, RN; Karen Posner,PhD; Keith Ruskin, MD; Wilson Somerville, PhD;Jeffery Vender, MD.
Address all general, membership, and sub-scription correspondence to:
Administrator, Deanna WalkerAnesthesia Patient Safety FoundationBuilding One, Suite Two8007 South Meridian StreetIndianapolis, IN 46217-2922
e-mail address: [email protected]
FAX: (317) 888-1482
Address Newsletter editorial comments, questions, letters, and suggestions to:
Robert C. Morell, MDEditor, APSF Newsletter
c/o Addie Larimore, Editorial AssistantDepartment of AnesthesiologyWake Forest University School of Medicine9th Floor CSBMedical Center BoulevardWinston-Salem, NC 27157-1009
e-mail: [email protected]
Boston UniversityVideo Honors Dr. Leroy Vandam
Dr. Leroy Vandam (1914-2004) was a great anes-thesiologist, teacher, scientist, author, and artist.His career began in surgery and, under the leader-ship of Dr. Robert Dripps, became focused on anes-thesiology. During his tenure at the Peter BentBrigham Hospital (now known as Brigham andWomen’s), Dr. Vandam served as a mentor to Dr.Ellison C. (Jeep) Pierce, who became the founder ofthe Anesthesia Patient Safety Foundation. In fact,Dr. Vandam assigned Dr. Pierce the topic of “Anes-thesia Accidents” to be given as a resident’s lecture.Under the directorship of Dr. Rafael Ortega, BostonUniversity Medical Center’s Department of Anes-thesiology, in conjunction with Anesthesia Associ-ates of Massachuseetts, has honored Dr. Vandam’smemory with a wonderful DVD entitled Leroy D.Vandam, MD: An Anesthesia Journey. This produc-tion illustrates numerous fascinating and historicalaspects of Dr. Vandam’s career, in the context of theevolution of anesthesia equipment. Safety ramifica-tions of anesthesia equipment are obvious through-out this production. Dr. Vandam’s own words andaccounts of his experiences are a living history, andhighlight his contributions throughout his incredi-ble career. Copies of the DVD can be obtained bycontacting the Anesthesia Department at BostonUniversity Medical Center.
Check out the Virtual Anesthesia Machine Website
and theAPSF Anesthesia
Machine Workbookat
www.anest.ufl.edu/vam
SUPPORTYOURAPSF
Your Donation:
• Funds ResearchGrants
• Supports YourAPSF Newsletter
• PromotesImportant SafetyInitiatives
• FacilitatesClinician-ManufacturerInteractions
• Supports theWebsite
Please make checks payable to the APSF
and mail donations to:
Anesthesia Patient Safety Foundation (APSF)520 N. Northwest HighwayPark Ridge, IL 60068-2573

fires with sevoflurane (liberating carbon monoxide,formaldehyde, and methanol) only occurs in desic-cated absorbent and is enhanced by the type andquantity of strong base (KOH>NaOH). The renaleffects of compound A formation under low flowsevoflurane anesthesia have been extensively evalu-ated in surgical patients and found to have no clini-cally significant adverse effects. The breakdown ofdesflurane, enflurane, and isoflurane (in descend-ing order of magnitude) to carbon monoxide,requires desiccated absorbent and is also enhanced bystrong base, and particularly Baralyme®. Baralyme®
and Drägersorb® 800 produce more carbon monox-ide than Drägersorb® 800 Plus (Dräger Medical, Inc.),Intersorb® and Spherasorb® (Intersurgical Ltd.), indescending order and with descending amounts ofstrong base. Clinical effects of carbon monoxideexposure have been described, but they may beconcealed by post-anesthetic effects and cannot bedetected by pulse oximetry. Fires have been reportedin the USA with sevoflurane only and desiccatedBaralyme®. However, cases of extreme heat associ-ated with desiccated sodalime have also beenreported in Europe. Dr. Kharasch strongly advocatedthe conversion to, and use of only carbon dioxideabsorbents that do not contain strong base.
Harvey J. Woehlck, MD, speaking on Monitor-ing for Desiccation and Carbon Monoxide:
The production of carbon monoxide is greaterwith desiccated KOH absorbents than with desic-cated NaOH absorbents, and is proportional to baseconcentration. By-products of sevoflurane includecarbon monoxide, formaldehyde, methanol, methylformate, dimethoxymethane, and perhaps hydro-gen gas at high temperatures. [The relative abilityof these by-products versus other combustiblematerials, such as plastics or gaskets, to serve as afuel in a high heat oxygen-enriched environment isnot known.] Desiccation of traditional absorbentand its production of carbon monoxide cannot bedetected with routine anesthetic monitors. Theblue-violet discoloration of traditional absorbentstypically indicates exhaustion, and not desiccation.Rapid discoloration might also indicate degradationof the anesthetic agent. One absorbent (Amsorb®
Plus, Armstrong Medical) does change color withdesiccation, as desiccation is expected to occur withabsorbent exhaustion. Diagnosing carbon monoxidetoxicity is difficult with its indiscriminate and non-diagnostic symptoms of confusion, nausea, dysp-nea, headaches, and dizziness that might also besymptoms of anesthetic emergence. Studies showthat total cessation of carbon monoxide productioncannot be achieved despite implementation of anti-desiccation strategies. Monitoring of carbon monox-ide gas in the circuit is currently possible with moresophisticated and more expensive detectors, andcarboxyhemoglobin monitoring is availablethrough co-oximetry, but is not routinely assessed.
APSF NEWSLETTER Summer 2005 PAGE 27
“Absorbents,” From Page 25 could clarify the issues and make recommendationsto clinicians, manufacturers, and regulatory orinsurance agencies alike. They agreed that cliniciansneed simple and straightforward consensus adviceon how to promote patient safety.
The chemical cycle of soda lime production,absorption of carbon dioxide, and regeneration ofchalk was reviewed (see Figure 1). Chalk (calciumcarbonate or CaCO3) is converted to lime (calciumoxide or CaO), while slaking with water convertslime to slaked lime (calcium hydroxide orCa(OH)2). Gaseous carbon dioxide (in solution withwater) reacts slowly with Ca(OH)2. Therefore,“soda” lime was created with the addition of thecatalyst sodium hydroxide. This hydroxyl ion (OH-)reacts with carbon dioxide producing bicarbonate(HCO3
-), which then has strong affinity forCa(OH)2, recreating chalk and regenerating thehydroxyl (OH-) catalyst. Other formulations ofabsorbent do not rely upon strong base to catalyzethe reaction, but instead are using substances suchas CaCl2 or CaSO4.
Numerous brands and formulations ofabsorbent are listed in Table 3. All contain a highconcentration of Ca(OH)2. Discrepancies regard-ing their content exist in the literature. For exam-ple, legacy formulations of Sodasorb® (W. R.Grace and Company) had KOH, with NaOHbelow 4%. Current formulations have no KOHand the NaOH concentration is 3.7%. Sodalimevariations also exist. Absorbent manufacturers havealready developed products that produce insignifi-cant or no compound A or carbon monoxide,whether moist or desiccated. They also produceminimal heat and minimally adsorb volatile agents.
Indirect methods require particular gas analyzersthat can detect trifluoromethane, an intermediatebyproduct of isoflurane and desflurane. Volatileagents are not known to react with, or to producecompound A or carbon monoxide from Ca(OH)2,LiOH, or Ba(OH)2; however, theoretical chemistryprovides for the potential reactivity of Ba(OH)2.
Edmond I Eger, II, MD, speaking on Thoughtson Untoward Absorbent-Anesthetic Interactions:
The production of compound A and carbonmonoxide arises from the action of the strong basesKOH and NaOH [and perhaps Ba(OH)2] on potentinhaled anesthetics. Compound A (implicated as apotential nephrotoxin) is produced in moist or des-iccated absorbents with sevoflurane only. Carbonmonoxide is only produced with desiccatedabsorbents, most with Baralyme® acting upon des-flurane. Fires are known to occur only in the combi-nation of sevoflurane and desiccated Baralyme®.Desiccated absorbents without KOH or Ba(OH)2,and with lesser amounts of NaOH, produce lessheat and no fires, and dramatically less carbonmonoxide or compound A. There is general recog-nition that all untoward events are rare and pre-ventable at modest cost. Dr. Eger further stated thatthe production of toxic products can be eliminatedthrough the use of absorbents containing onlyCa(OH)2 with catalysts such as CaCl2 or CaSO4.
Industry RepresentativeComments
Industry representatives provided summaryinformation on foundational topics. They appreci-ated the significance of a conference that wouldbring together a core group of professionals who
Experts Review Absorbent Fundamentals
See “Absorbents,” Next Page
CaO
Kiln (1000°C)(-CO2)
CaCO3
Use(+CO2)
Ca(OH)2NaOH
ManufacturingProcessNaOH
CA(OH)2
Slaker(+H2O)
Lime
ChalkSodaLime
Figure 1: The Soda Lime Cycle, courtesy of Dr. Michael Clarke, Molecular Products

APSF NEWSLETTER Summer 2005 PAGE 28
humidity of the gas flowing out of the absorbentmay be directly related to, and therefore indicate, itsmoisture content. Simple (home) devices to measurecarbon monoxide are disrupted in the presence ofvolatile agents, but more sophisticated monitors areavailable. Some desiccated absorbents will continueto absorb carbon dioxide; therefore, the presence ofan acceptable capnographic waveform should notbe taken as confirmation that the breathing gas isfree from carbon monoxide. Alternatively, an ele-vated baseline of inspired carbon dioxide on thecapnogram should alert the clinician to the possibil-ity of desiccation and/or exhaustion.
Consensus StatementAt the conclusion of this conference, attendees
were asked to again consider the goal of the confer-ence, “to develop a consensus statement to sharewith anesthesia professionals on the use of carbondioxide absorbents so as to reduce the risk ofadverse interactions with volatile anestheticdrugs,” and make appropriate recommendations.Based on those responses, the APSF drew the fol-lowing conclusions:
The APSF recommends use of carbon dioxideabsorbents whose composition is such thatexposure to volatile anesthetics does not
result in significant degradation of thevolatile anesthetic.
The APSF further recommends that thereshould be institutional, hospital, and/ordepartmental policies regarding steps toprevent desiccation of the carbon dioxideabsorbent should they choose conventionalcarbon dioxide absorbents that may degradevolatile anesthetics when absorbentdesiccation occurs.
In such circumstances of using absorbents thatmay degrade volatile anesthetics, conference atten-dees generally agreed that users could take the follow-ing steps, consistent with ECRI recommendations:
1. Turn off all gas flow when the machine is not in use.
2. Change the absorbent regularly, on Mondaymorning for instance.
3. Change absorbent whenever the color changeindicates exhaustion.
4. Change all absorbent, not just 1 canister in a 2-canister system.
5. Change absorbent when uncertain of the state ofhydration, such as if the fresh gas flow has been lefton for an extensive or indeterminate time period.
6. If compact canisters are used, consider changingthem more frequently.
There was also support for the APSF to createan “Expert Task Force” to define further the charac-teristics of carbon dioxide absorbents that do notsignificantly degrade volatile anesthetics.
Dr. Olympio is Professor of Anesthesiology, formerDirector and Founder of the Patient Simulation Labora-tory, and former Vice Chair for Education for theDepartment of Anesthesiology at Wake Forest Univer-sity School of Medicine in Winston-Salem, NC. He isalso Chair of the APSF Committee on Technology andserves on the APSF Executive Board as well.
Recommended References1. Holak EJ, Mei DA, Dunning MB III, et al. Carbon
monoxide production from sevoflurane breakdown:modeling of exposures under clinical conditions. AnesthAnalg 2003;96:757-64.
2. Olympio MA, Morell RC. Canister fires become a hotsafety concern. APSF Newsletter 2003-04;18:45, 47-8.
3. Fatheree RS, Leighton BL. Acute respiratory distresssyndrome after an exothermic Baralyme-sevofluranereaction. Anesthesiology 2004;101:531-3.
4. Wu J, Previte JP, Adler E, et al. Spontaneous ignition,explosion, and fire with sevoflurane and bariumhydroxide lime. Anesthesiology 2004;101:534-7.
One absorbent provides a graded and permanentcolorimetric indicator of both expected desiccationand exhaustion (Amsorb® Plus, Armstrong MedicalLtd.), while another (Spherasorb®, IntersurgicalLtd.) contains a substance that delays the total des-iccation of the absorbent. Reducing by-products tonegligible levels does not require strong-base-freeabsorbents.
The incidence of patient exposure to carbon monox-ide is unknown. ECRI, Abbott Laboratories, and otherinvestigators have already published recommendationsto minimize the risk of unintended desiccation ofabsorbents. Anesthesia machine manufacturers areaware that fresh gas flow through modern and uniquebreathing circuits may promote desiccation ofabsorbent in different ways. Clinicians are directed tothose resources for detailed information.
Monitoring absorbent temperature is one poten-tially useful adjunct, but the critical location of theprobe and the quantity of heat that is worrisomehave not been clearly identified. Temperature is ele-vated during normal carbon dioxide absorptionreactions, and varies widely throughout theabsorbent. Furthermore, carbon monoxide can stillbe produced at temperatures that might otherwisebe associated with normal absorption. Relative
Consensus Statement Agreed Upon“Absorbents,” From Preceding Page
Table 1. Invited Medical Experts, APSF, and Industry Representatives
Medical Experts
Jerry A. Dorsch, MDJacksonville, FL
Edmond I Eger, II, MDProfessor of AnesthesiologyUniversity of California, San Francisco, CA
Evan D. Kharasch, MD, PhDProfessor of AnesthesiologyUniversity of Washington School of MedicineSeattle, WA
Harvey J. Woehlck, MDProfessor of AnesthesiologyMedical College of WisconsinMilwaukee, WI
Anesthesia Patient Safety Foundation
Robert C. Morell, MDEditor, APSF Newsletter
Michael A. Olympio, MDChair, APSF Committee on TechnologyCo-moderator of Conference
George A. SchapiroExecutive Vice President
Robert K. Stoelting, MDPresidentCo-moderator of Conference
Industry Representatives
Drug and Equipment ManufacturersRandall D. Ostroff, MD (Abbott Laboratories)Raul A. Trillo, Jr., MD (Baxter Healthcare)Christoph Manegold (Datascope)Juergen-Ralf Lange (Dräger Medical)Michael Mitton, CRNA (GE Healthcare)
Carbon Dioxide Absorbent ManufacturersDr. Ciarán Magee (Armstrong Medical, Ltd.)Dr. Michael Clarke (Molecular Products, Ltd.)Mike Holder (Intersurgical, Ltd.)Eldon P. Rosentrater (Allied Healthcare)Jeffrey H. Mack (W.R. Grace) See “Absorbents,” Next Page
Editor’s Note: There is not uniform agreement among experts as to the specific types and amounts of degradation products that may form when volatile anesthetics are exposed to desic-cated absorbents that contain significant amounts of KOH and NaOH. Hence, no specific conclusions can be drawn from this conference about the relative contribution of any specificdegradation product or circuit material [including plastics] as a combustible fuel in a high heat, oxygen-enriched environment.

APSF NEWSLETTER Summer 2005 PAGE 29
5. Castro BA, Freedman LA, Craig WL, Lynch C III. Explo-sion within an anesthesia machine: Baralyme, high freshgas flows and sevoflurane concentration. Anesthesiology2004;101:537-9.
6. Woehlck HJ. Sleeping with uncertainty: anesthetics anddesiccated absorbent. Anesthesiology 2004;101:276-8.
7. Knolle E, Heinze G, Gilly H. Small carbon monoxideformation in absorbents does not correlate with smallcarbon dioxide absorption. Anesth Analg 2002;95:650-5.
8. Woehick HJ, Dunning M III, Nithipatikom K, et al. Massspectrometry provides warning of carbon monoxideexposure via trifluoromethane. Anesthesiology1996;84:1489-93.
9. “Dear Health Care Professional” Ultane® (sevoflurane)letter from Abbott Laboratories, November 17, 2003.Available at: www.fda.gov/medwatch/SAFETY/2003/Ultane_deardoc.pdf. Accessed June 27, 2005
10. Anesthesia carbon dioxide absorber fires. Health Devices2003;32:436-40.
11. Hazard update: revised recommendation for “Anesthe-sia carbon dioxide absorber fires” (published November2003). Health Devices 2003;32:487.
Absorbent Composition Summarized for Conference
Table 3. Absorbent ComparisonsThis table was formulated based on information supplied by the various manufacturers. The APSF assumes no responsiblity for variations in, or deviations from the formulations that arerepresented in this table. The table is supplied for educational and conceptual purposes.
Company Product Name H2O% NaOH% KOH% Ca(OH)2% Significant Other US Availability
Allied Healthcare/Chemetron Baralyme® 11.0 – 16.0 0.0 <5 73 Ba(OH)2 No longer
Allied Healthcare *Carbolime™ 12.0 – 19.0 3 0.0 >75 — Yes
W.R. Grace and Company Sodasorb® 15.0 – 17.0 3.7 — 50 – 100 — Yes
Intersurgical Ltd. Intersorb Plus® 13.5 – 17.5 2.6 0.0 81 — Yes
Intersurgical Ltd. Spherasorb® 13.5 – 17.5 1.3 0.0 78 4% Zeolite Yes
Intersurgical Ltd. LoFloSorb® 13.5 – 17.5 0.0 0.0 78 6.5% Silica Yes
Armstrong Medical Ltd. Amsorb® 13.5 – 16.5 0.0 0.0 79 – 82 CaCl2 No longer
Armstrong Medical Ltd. Amsorb® Plus 13.0 – 18.0 0.0 0.0 >80 CaCl2 Yes
Dräger Medical, Inc. Drägersorb® 800 — ~2 ~3 — — No longer
Dräger Medical, Inc. Drägersorb® 800 Plus ~16 1 – 3 NA 75 – 83 — Yes
Dräger Medical, Inc. Drägersorb® Free 14 – 18 0.5 – 2 NA 74 – 82 CaCl2 Yes
Airgas†/Molecular Products Sodalime — <3.5 2.6 >80 — Yes
Molecular Products Sofnolime® 12 – 19 <3.5 0.0 — — No‡
GE Medical†/Molecular Products Medisorb™ — <3.5 0.0 — — Yes
*Manufactured by Molecular Products†Distributor of product manufactured by Molecular Products.‡Not available in US market as a medical product, although diving and military grades are available in the US. Medical grade is available outside US.More than one manufacturer reported variable absorption capacity based on cannister design, shape, volume FGF, hydration, and carbon dioxide concentration. Nearly all reported price variabil-
ity dependent upon marketing and type of fill.
Table 2. Invited Observers
Invited Observers
John Armstrong ....................................................Armstrong MedicalJonnalee Bill ............................................................American Society of Anesthesia Technologists and TechniciansJoe Ciccone, PhD ....................................................W.R. GraceRobert Clark ..........................................................Dräger MedicalJohn T. Collins ........................................................American Hospital AssociationAlbert L. de Richemond, MS, PE ........................ECRIJonathan Deutsch, MD..........................................Baxter HealthcareCharlotte Guglielmi, RN ......................................Association of periOperative Registered NursesRobert Herdzina ....................................................Intersurgical, Ltd.Steven Hoff ............................................................Abbott LaboratoriesElizabeth F. Holland..............................................Abbott LaboratoriesGavin Keogh ..........................................................Armstrong MedicalNancy Kupka, RN, DNSc, MPH..........................Joint Commission on Accredition of Healthcare OrganizationsDeborah Lawson, AA............................................American Academy of Anesthesiologists AssistantsDonald E. Martin, MD ........................................American Society of AnesthesiologistsMarion McGowan..................................................Dräger MedicalKaren Meehan, RN ................................................The Doctors CompanyVic Velton................................................................DatascopeTom Noonan ..........................................................Allied HealthcareJohn M. O’Donnell, CRNA ..................................American Association of Nurse AnesthetistsBonnie Reinke ........................................................GE Healthcare
“Absorbents,” From Preceding Page
The APSF continues to accept and appreciate contributions. Please make checks payable to the APSF and mail donations to:
Anesthesia Patient Safety Foundation (APSF), 520 N. Northwest Highway, Park Ridge, IL 60068-2573

APSF NEWSLETTER Summer 2005 PAGE 30
molecular genetic testing for MH in the US. The lab-oratory is CLIA and CAP certified.
There are several important issues to bear inmind when considering referral of a patient for MHtesting by molecular techniques. First, the test is nota screening test. The sensitivity of the test in a pop-ulation of patients with a positive contracture test issomewhere between 30 and 40%. Second, theabsence of a mutation does not rule out MH suscep-tibility. Third, a referral for testing should be madeonly by a physician or genetic counselor. Fourth, ablood sample is all that is required for testing. Fifth,the test does not replace the contracture test.Because of the limited sensitivity of the genetic test,those without a mutation should be referred forcontracture testing to determine MH susceptibilitysince the caffeine halothane test is very sensitive.And sixth, if one of the known mutations for MH isfound in a family member, other family memberswith that mutation are MH susceptible for certainand may bypass the contracture test.
Who Should Be Referred for Testing?
A. Those patients with a positive caffeine halothanetest or a confirmed clinical episode of MH.
B. Those with an identified mutation as part of aresearch protocol.
C. Family members of these patients listed aboveshould also be considered for genetic testingafter discussion with a biopsy center director or agenetic counselor.
Patients with a positive caffeine halothane testwill first have their DNA assessed for the presenceof 17 known mutations at a cost of about $790. Ifone of the mutations is found, that mutation may besought in specimens from family members. The costfor the assay for a specific mutation is about $200.Reimbursement for such testing is dependent onthe specific insurance company. Although notrequired, genetic counseling is advised for thoseundergoing genetic testing.
What Are the Advantages of the Genetic Test?
Genetic testing will avoid the use of the invasivemuscle biopsy contracture test. As such, it is lessexpensive than the contracture test and does not carrythe morbidity of the muscle biopsy. Another advan-tage of such testing (in some cases) is the clarificationof the likelihood that a perioperative morbidity ormortality is related to MH, since the DNA analysismay be performed on preserved tissue samples.
It is clear that with time, the sensitivity of thetest will improve significantly. In an individual thismay not require a repeat sample since the DNA
analysis is based on sequencing the hot spots of thegene, and DNA variants of undetermined signifi-cance at this point may turn out to be causal for MHwith further investigation.
Patients and physicians are urged to provide theNorth American MH Registry with a detailed clini-cal history in order to advance the understanding ofthe relation between clinical events and the molecu-lar genetics of MH. Appropriate forms are availablefor this purpose by contacting the Registry(www.mhreg.org). The Registry database and col-lection vehicle are approved by the IRB of the Uni-versity of Pittsburgh Medical Center and are in fullcompliance with regulations for protection of confi-dential medical information.
The MHAUS board and Professional AdvisoryCouncil and hotline consultants are very pleasedwith the introduction of genetic testing for MH inNorth America. Nevertheless, we realize that this isjust the first step in devising a highly sensitive, spe-cific, minimally invasive diagnostic test for MH. Wealso expect that other laboratories will offer clinicalgenetic testing for MH in the near future.
Further information on the test, including Fre-quently Asked Questions, may be found on theMHAUS website (www.mhaus.org) or by contact-ing MHAUS directly.
Dr. Rosenberg is President of the Malignant Hyper-thermia Association of the United States (MHAUS) andDirector of the Department of Medical Education andClinical Research at the St. Barnabas Medical Center inLivingston, NJ. He is also a Professor of Anesthesiologyat Mt. Sinai School of Medicine, NY.
by Henry Rosenberg, MD, CPE
Drs. M.A. Denborough and R.R. Lovell first for-mally described the syndrome we know today asmalignant hyperthermia (MH) in a Letter to theEditor of Lancet titled “Anaesthetic Deaths in aFamily” in 1960. They described a near fatality in apatient with a family history of deaths in appar-ently healthy individuals during or shortly afteranesthesia. Once the syndrome was described,rapid progress was made in describing how, in cer-tain individuals, anesthetic gases and succinyl-choline could precipitate muscle rigidity,myonecrosis, acidosis, hyperthermia, and death.Families from all parts of the world were reportedwith this syndrome, which apparently followed anautosomal dominant inheritance pattern.
A major advance in the understanding of thepathomechanism of MH was the demonstrationthat various swine breeds develop a similar set ofclinical signs, often in the absence of anesthesia,termed “Porcine Stress Syndrome” or “Pale, SoftExudative Pork Syndrome.” The pig model is simi-lar in many ways to human MH, but different inothers. Nevertheless it helped in the understandingof the clinical presentations of MH and in thedemonstration of the efficacy of dantrolene inreversing the clinical signs of MH.
From the 1970s to the present, investigators inthe United States, Europe, Australia, New Zealand,Japan, and South Africa enhanced our knowledgeof the clinical description of MH, the characteriza-tion and standardization of the muscle biopsy con-tracture test, the demonstration of defectiveintracellular calcium flux in MH, and the differenti-ation of MH from other syndromes.
When the molecular genetic era dawned in the1980s, several groups began the investigation of themolecular genetic defects responsible for MH.Using the pig model, David MacLennan's group atthe University of Toronto was the first to demon-strate a consistent mutation in the gene that elabo-rates the ryanodine receptor in skeletal muscle(RYR-1). However, in humans it was soon apparentthat many other mutations (the count at present is23) in that gene and in others are causal for MH. Inthose patients with a positive halothane-caffeinecontracture test for MH, approximately 30% of suchpatients were shown to harbor one of 15-20 knownRYR-1 mutations. The good news is that the speci-ficity of the mutation analysis is close to 100% infamilies at risk to MH.
The adaptation of mutation detection to clinicaldiagnostic testing started a few years ago inEurope. Guidelines for testing have been publishedby the European MH group (www.emhg.org).
In the spring of 2005, Prevention Genetics, acompany located in Marshfield, WI, began offering
Malignant Hyperthermia Syndrome: FromBarnyard to Molecular Genetics Laboratory
Contact Information
Anesthesia Patient Safety FoundationBuilding One, Suite Two8007 South Meridian StreetIndianapolis, IN 46217-2922
President: Robert K. Stoelting, MDAdministrator: Deanna M. Walker
Please address all inquires by email ([email protected]) or facsimile (317-888-1482).

APSF NEWSLETTER Summer 2005 PAGE 31
Twenty minutes later, the ECG showed broadcomplex bradycardia that rapidly progressed toventricular tachycardia and fibrillation, whichresponded to defibrillation (20 J). The patientwas reintubated. Serum potassium concentrationduring resuscitation was >9 mEq/L on the firstarterial blood gas with a base deficit of -4.3mmol/L. The child’s esophageal temperaturewas 37.7 ºC. The patient received intravenous(IV) calcium gluconate, sodium bicarbonate, anda glucose-insulin infusion. Serum creatine kinase(CK) within an hour of the arrest was 17,821U/L, and peaked at 613,120 mEq/L 48 hourspostoperatively. The urine was noted to be palepink in color. As advised by the MH Hotlineconsultant, dantrolene was withheld, as therewas no evidence of hypermetabolism. Theventilatory requirements were normal, and therewas no evidence of increased carbon dioxideproduction.
Subsequent molecular genetic analysis of aperipheral blood sample demonstrated a deletionin the dystrophin gene from at least exon 47 toexon 52 (exons 45 and 60 were present), which isconsistent with a diagnosis of DMD. There wasno history of musculo-skeletal developmentaldelays or any abnormality on clinicalexamination.
2. The second patient was a 5-year-old maleweighing 19-kg with a history of hereditaryspherocytosis. He underwent uneventfullaparoscopic splenectomy with generalendotracheal anesthesia with sevoflurane,nitrous oxide, and vecuronium. In the PACU hesustained a cardiac arrest with potassium of 9.2mEq/L. One CK was elevated to 23,000 IU;testing of a blood sample drawn preoperativelyrevealed a CK of 15,000 IU. Following prolongedresuscitative efforts, the cardiovascular systemstabilized. However, the patient sustainedsignificant neurologic damage, oliguric renalfailure, and expired. It was unclear from thefamily history as to whether there were any signsof myopathy or family history of musculardystrophy. Histologic examination of the musclerevealed changes typical for DMD.
3. The third patient was a 7-year-old, 30-kg,asymptomatic female who developed laryngo-spasm at the end of general endotrachealanesthesia for tonsillectomy and adenoidectomywith sevoflurane anesthesia without musclerelaxant. Succinylcholine (6 mg) wasadministered, and ventricular fibrillation ensued.Prompt treatment with glucose, insulin,bicarbonate, hyperventilation, and calciumchloride combined with defibrillation restored
normal sinus rhythm. The potassium levelpeaked at >9 mEq/L, and the CK peaked at150,000 IU. The patient left the hospital fullyrecovered. No evidence of myopathy has beendetermined at the present time.
We report these findings in order to underlinethat young patients with asymptomatic dys-trophinopathy may develop hyperkalemic cardiacarrest in the absence of succinylcholine when potentvolatile agents are used. Of special interest in thesecases is that the cardiac arrest occurred not duringsurgery but in the PACU. In addition, in the onecase the hyperkalemic cardiac arrest after succinyl-choline occurred in a female.
One lesson from these and similar cases is thattherapy for sudden cardiac arrest in a young childduring anesthesia or in the PACU, in the absence ofairway compromise, hypovolemia, or known car-diac abnormalities, should be directed at hyper-kalemia. Evidence of myoglobinuria andhyperkalemia should be sought and the patienttreated accordingly. Whether precipitated by suc-cinylcholine or not, the presumptive diagnosis ofoccult myopathy should be entertained, specificallya dystrophinopathy.
Often sudden cardiac arrest in the perioperativeperiod in an otherwise asymptomatic child isthought to represent an episode of MH and treat-ment with dantrolene is instituted. However, clini-cians should consider hyperkalemia to be a morelikely reason. Cardiac arrest related to MH is usu-ally preceded by rapidly rising end-tidal carbondioxide, muscle rigidity, acidosis, and hyperther-mia, and most often occurs during anestheticadministration rather than in the postoperativeperiod. In such cases, the cause of the cardiac arrestis usually related to significant metabolic and/orrespiratory acidosis rather than hyperkalemia.
Package insert and other drug information con-cerning potent inhalation anesthetic agents (i.e.,sevoflurane, desflurane, halothane, and enflurane)should emphasize that when unexpected suddencardiac arrest occurs in a young child, hyper-kalemia is a likely precipitating cause, even in theabsence of succinylcholine. Myoglobinuria shouldbe considered, and the patient evaluated for anoccult myopathy, especially DMD.
Dr. Rosenberg is President of the Malignant Hyper-thermia Association of the United States (MHAUS) andDirector of the Department of Medical Education andClinical Research at the St. Barnabas Medical Center inLivingston, NJ. He is also a Professor of Anesthesiologyat Mt. Sinai School of Medicine, NY.
by Henry Rosenberg, MD, CPE, Arjunan Ganesh, MD,Albert J. Saubermann, MD, and Susan C. Nicolson, MD
The Malignant Hyperthermia Association of theUnited States (MHAUS) is a patient advocacy orga-nization that has operated a “hotline” since 1982staffed by volunteer anesthesiologists with exper-tise in the management of this rather unusual,potentially fatal syndrome. Fortunately, cardiacarrest and death related to malignant hyperthermia(MH) have been rare, thanks to early detection ofthe syndrome by capnography, and education ofthe anesthesia community to the early signs of thedisorder as well as the availability of dantrolene,the specific antidote for the metabolic effects of MH.
In the early 1990s members of the professionaladvisory committee of the MHAUS recorded sev-eral cases of sudden hyperkalemic cardiac arrests inyoung males (generally <5 years of age) during orfollowing anesthesia. Investigation revealed thatmost were in the asymptomatic or minimally symp-tomatic stage of Duchenne muscular dystrophy(DMD). The mortality associated with this syn-drome was 60%.1 In most cases, the cardiac arrestoccurred following the administration of succinyl-choline after induction of anesthesia with aninhalation anesthetic. A report to the FDA led to achange in the package insert of succinylcholine anda black box warning concerning the use of succinyl-choline in children.
Even at that time, however, there were sporadiccases in this population of hyperkalemic arrest dur-ing or immediately following general anesthesia inthe absence of succinylcholine. We would now liketo report 2 apparently asymptomatic male patientswho sustained hyperkalemic cardiac arrest in thepostanesthesia care unit (PACU) where the anes-thetic was conducted with sevoflurane in theabsence of succinylcholine. In addition, a thirdpatient, a young female, developed sudden hyper-kalemic cardiac arrest following a minimal dose ofsuccinylcholine to treat laryngospasm at the conclu-sion of surgery. All of these cases occurred over aperiod of 7 months.
1. The first patient was a 4-year-old male whounderwent uneventful atrial septal defect repairusing sevoflurane anesthesia for inductionfollowed by isoflurane for maintenance. Thenon-depolarizing neuromuscular blocking agentwas pancuronium. The procedure lasted for 2 hrs45 min, including a 29-min bypass time.Following the procedure, he entered the recoveryroom and met the criteria for extubation, and thetrachea was extubated. The patient was awake,alert, and breathing regularly with an oxygensaturation of 100% at the time of extubation.
MHAUS Reports 3 Unique Casesof Hyperkalemic Cardiac Arrest
See “MHAUS,” Page 43

APSF NEWSLETTER Summer 2005 PAGE 32
State, after being hit in the head in the MRI scannerby a ferromagnetic oxygen cylinder. I was suddenlypersonally confronted with absolute restrictions pro-hibiting anything “non-FDA approved MRI compati-ble” from entering the scanner room. I was suddenlyforced out into the SCR with my “magnetic” equip-ment, monitoring at 40 feet from the SCR, which cre-ated great anxiety to apparently only myself. In thepast decade, I am aware of 2 deaths having occurredin this city using these “40 foot/next door” tech-niques: 1) the expiratory limb of a circle systemoccluded and the patient succumbed to tensionpneumothorax, and 2) a mini-drip infusion of propo-fol (no volumetric pump) ran uncontrolled with afatal outcome. Astonishingly, a picture of a mini-drippropofol infusion (without volumetric pump) of thiskind is pictured, as well as “monitoring from thescanner control room” in a recent MRI-anesthesiareview article.1
Incident Illustrates Need for Monitoring
More astonishing is that modern MRI suitescontinue to function with antiquated equipment,although modern and MRI-compatible operatingroom suites have been introduced in the US andEurope!2,3 Here all anesthetic and surgical needs aremet in the scanner room itself. MRI-compatibleequipment has now been procured here at my insti-tution, including infusion pumps and MRI ventila-tors. Anesthesia personnel should now remain inthe room, as no biological hazard exists to normalhuman beings in the scanner room, especially at 10feet from the magnet coil.4 However, individualscontinue, by choice, to monitor from the SCR. Thisrecently led to the following incident:
A patient was brought to the MRI from theradiology suite after coils were inserted in ananeurysm of the carotid artery. This 70-year-oldfemale came intubated, paralyzed, with a radialarterial catheter, and on a propofol infusion. Theinfusion was switched to the MRI compatible,battery operated pump, and she was ventilatedwith the ventilator without ETCO2 analysis.Neither piece of equipment is electricallyconnected to alarms visible or audible in theSCR. The arterial pressure trace could not bedisplayed, because no MRI compatibletransducers were available in the institution. TheETCO2 was not monitored, as this was notroutine for this ventilator type; however, anairway pressure gauge was connected andviewable in the SCR via 40-foot tubing. The MRIdepartment’s monitor is capable of both arterialtracing and ETCO2, as well as non-invasiveblood pressure (NIBP), ECG, and pulse oximetry,and all monitored parameters are viewable bothin the SCR and scanner room.
After a short period in the scanner, the NIBP wasnot obtaining results, and a second stat attemptyielded no result. The airway pressure was nownoted to cycle between 20-40 torr and at a rate of30-40. This was noted from the SCR, and after ashort interval to interpret the situation and toenter the scanner room, the patient waswithdrawn urgently from the scanner. At thistime, no radial pulse was detected, althoughheart and breath sounds were present. Recyclingthe BP cuff yielded 44/20, immediately afterwhich she was placed on bag-valve ventilation,while no visible or auscultatory problems werenoted with ventilation. Phenylephrine wasobtained from the SCR. Before the phenylephrinecould be administered, renewed NIBPmeasurement now yielded 169/110. Thepropofol infusion pump was noted to display ared light indicating “downward occlusion” of theCVP line — duration unknown. A second MRIventilator was obtained, propofol reinstituted,and the patient returned to the scanner for scan,with the anesthesia provider instructed toremain at the patient's side.
The first ventilator was isolated for inspectionand found to function within parameters. Theseventilators are gas powered, non-electrical/mechanical ventilators using “Bird-1970stechnology.” The problem appeared to be due tochanges in patient compliance resulting in“autocycle” of unwanted, yet available, SIMVprogramming, atypical of anesthesia ventilators.These ventilators are managed by the respiratorytherapy department and are unfamiliar toanesthesia personnel. This incident resulted in aperiod of hypoperfusion from the sustained highairway pressures, a “valsalva maneuver” ofsorts, as well as the potential for awareness dueto interruption of the propofol infusion. Theinterruption of the propofol may have been life-saving in this situation (as well as perhapscausative). Had the anesthesia provider beenpresent in the room, the rapid cycling of themechanical ventilator and audible alarm of theinfusion pump would have been noticed. Visualobservation from the SCR is significantlyimpaired by the reduced transparency of theglass windows, which are part of the Faradaycage screen for radiofrequency energy, andaudio alarms typically remain unheard in theSCR. Emphasis on the use of audible alarms hasbeen recently noted, and MRI alarms may needto be much louder than in the OR, due to thesignificant scanner noise.5 Had the arterial tracebeen available, earlier recognition might haveprevailed in this instance, but as the NIBP wascycling at 5-minute intervals, a significant period
To the Editor:
I am writing to suggest it may be appropriatefor the ASA/ASPF to specifically address monitor-ing standards for the provision of sedation, anesthe-sia, and ventilation of patients in the magneticresonance imaging (MRI) suite. When I heard IreneP. Osborn, MD, Director (Division of Neuroanesthe-sia, Mount Sinai Medical Center, NY, NY), speak atthe California Society Refresher Course in SanDiego earlier this year, I specifically asked if it wasappropriate to monitor the patient, not from thescanner room itself (where the patient is in the scan-ner tube), but from the scanner control room (SCR-the room next door with all controls separated by awall with a large dark glass window). This questionwas answered informally by those in attendance,with more than 50% of the attendees (including Dr.Osborn) indicating this was their practice for adultand pediatric patients. I believe this indicated that,typically, NO provider remained in the scannerroom itself with the patient—MD or CRNA. Ibelieve this is in contradiction to ASA basic stan-dards for monitoring, which make no provision forsuch exception. The Standard reads:
Qualified anesthesia personnel shall be present in theroom throughout the conduct of all general anesthetics,regional anesthetics and monitored anesthesia care.
Having had opportunity to practice in multipleprivate and university settings since my graduationfrom medical school in 1981, I have seen manydevelopments in providing anesthesia for MRI overthe years. Historically, many standard items werenot “MRI compatible,” yet were made available inthe scanner room with exceptional precautions.Until I came to this university center, I had alwaysremained in the scanner room with my patientsunder anesthesia and had never seen anesthesiaprovided from the scanner control room, althoughthis methodology was “standard” at PresbyterianUniversity Hospital in Pittsburgh when I arrived.Here infusion and ventilator tubings were runthrough wall portholes at distances of 40 feet, andof course, direct monitoring of the patient was notdone, but rather the anesthesia machines and tele-metric monitor screens in the SCR room wereobserved. I was for a time, however, able to practiceMRI anesthesia from within the scanner room using“non MRI approved” pumps and anesthesiamachines maintained at a safe distance from themagnet. In this way, all aspects of anesthetic carecould be directly observed and actively managed,as in the operating room and per ASA guidelines.
MRI Death ReinforcesPrecautions
This all changed drastically in 2001, when a childdied in the Westchester Medical Center in New York
Letter to the Editor
Stand Near By in the MRI
See “MRI,” Page 36

APSF NEWSLETTER Summer 2005 PAGE 33
somehow, all this technology stops at the post-anes-thesia care unit (PACU) door, and patients are sentto the hospital floor with their narcotic laden infu-sions, where currently acceptable standards ofmonitoring are a flow sheet with vital signs andpump data that are manually updated at best every30 minutes. The patient’s only safety net is the may-day team, an often poorly choreographed band ofpractitioners left to initiate resuscitation at an oftenundetermined period of time after the critical event.
In the mid 1990s, management of acute postop-erative pain and PCA was, in effect, transferred tothe surgical service when the government(HCFA/CMS) and private insurers stopped com-pensating anesthesiologists for managing postoper-ative pain. It was left to the surgeons to managepain, narcotics, and respiratory insufficiency. Yet ifyou asked first-year medical students which spe-cialist is the expert in pain, narcotics, respiratoryphysiology, and resuscitation, they would reply“anesthesiologist,” not “surgeon,” “internist,” or“hospitalist.” We define ourselves as perioperativephysicians,6 yet in the ever increasing number ofhospitals without an anesthesia-run acute pain ser-vice, patients are discharged from the PACU withPCA technology that exposes them to great riskwithout our oversight.
Capnography May Warn ofHyperventilation
Some may argue that my experience lacks adenominator, and that these may be rare events. Icontend that one such adverse outcome in a friend orfamily member undergoing elective surgery is onetoo many. Cashman et al., in a recent meta analysisof the literature, reported an incidence of “respira-tory depression” of 11.5% by oximetry (O2Sat <90%)and 1.3% by bradypnea (RR <10), which translates tothousands of patients with potentially catastrophicrespiratory depression per day.7 Others take comfortin using oximeters in “high-risk” patients, yet this isa deceptively ineffective approach. The first patientabove could hardly be described as “high risk.” Fur-thermore, Stemp recently highlighted the dangers ofsimply adding supplemental oxygen, the typical“therapeutic” response to desaturation.8 Supplemen-tal oxygen does not treat desaturation due tohypoventilation, but merely postpones the patient’sinsidious progress from bradypnea to apnea. Theaddition of a capnograph, however, may anticipate apatient’s desaturation by warning of a decrease inrespiratory rate and rise in end-tidal carbon dioxide.In the OR setting, these monitors together werejudged to potentially prevent 93% of respiratorymishaps in the closed claims database.2
Perhaps the APSF could take a more active rolein measuring the scope of the problem, proposemonitoring guidelines for PCA, and encouragedevelopment of technology that closes the monitor-
ing void that exists with PCA. It would once againdemonstrate that it is the premier organizationdevoted to patient safety in the perioperative envi-ronment.
Frank J. Overdyk, MSEE, MDCharleston, SC
References
1. Pierce EC. The establishment of the APSF and the ASAClosed Claims Study. The 34th Rovenstine Lecture.Available on the web at: http://www.apsf.org/about/rovenstine/part1.mspx. Accessed on April 26, 2005.
2. Tinker J, Dull D, Caplan RA, et al. Role of monitoringdevices in prevention of anesthetic mishaps: a closedclaims analysis. Anesthesiology 1989;71:541-6.
3. Sidebotham D, Dijkhuizen M, Schug S. The safety andutilization of patient-controlled analgesia. J Pain Symp-tom Manage 1997;14:202-9.
4. Sullivan M, Phillips MS, Schneider P. Patient-controlledanalgesia pumps. USP Quality Review 2004;81:1-3.Available on the web at: http://www.usp.org/pdf/patientSafety/qr812004-09-01.pdf. Accessed April25, 2005.
5. Manufacturer and User Facility Device ExperienceDatabase - (MAUDE). U.S. Food and Drug Administra-tion, Center for Devices and Radiologic Health, Depart-ment of Health and Human Services. Available on theweb at: http://www.fda.gov/cdrh/maude.html.
6. Alpert CC, Conroy JM, Roy RC. Anesthesia and periop-erative medicine: a department of anesthesiologychanges its name. Anesthesiology 1996;84:712-5.
7. Cashman JN, Dolin SJ. Respiratory and haemodynamiceffects of acute postoperative pain management: evi-dence from published data. Br J Anaesth 2004;93:212-23.
8. Stemp L. Etiology of hypoxemia often overlooked.APSF Newsletter 2004;19(3): 38-9.
To the Editor:
A healthy 26-year-old soccer player undergoescruciate ligament repair and is discharged to thefloor with patient-controlled analgesia (PCA). Hismother, concerned that he rest comfortably afterpoor postoperative pain control, repeatedly presseshis morphine PCA button while he is asleep. Hestops breathing and is resuscitated, albeit with ahypoxic brain injury.
A mother of 3 small children with chronic lowerback pain, for which she takes PercocetTM, under-goes uneventful emergency appendectomy and isdischarged to the floor on hydromorphone PCA.Frustrated by her difficult pain management, floornurses give supplemental intravenous hydromor-phone outside of PCA parameters. She suffers a res-piratory arrest and hypoxic brain injury.
Almost 20 years after the APSF spearheaded theadoption of pulse oximetry and capnography asstandards for patient monitoring in the OR,1 andwith a resultant decrease in catastrophic respiratoryevents,2 I still encounter such cases as an expert wit-ness in defense of hospitals liable for these devas-tating outcomes.
PCA by Proxy Presents Great Danger
There is accumulating evidence that PCA pre-sents serious risks to patients and liability exposureto hospitals. The 2 main safety mechanisms inte-grated in current PCA pumps, the lock-out intervaland maximum dose limit, fall woefully short of pre-venting overdosage of narcotics. PCA “by proxy,”in which family members or persons other than thepatient administer bolus doses, as occurred in theexample above, are well documented.3 The risk ofpatient harm due to medication errors with PCApumps, the most common form of PCA error, is 3.5-times the risk of harm to a patient from any othertype of medication administration error.4 TheFDA’s Manufacturer and User Facility Device Expe-rience (MAUDE) Database for 2004, a voluntarydatabase for reporting problems with devices,reports 21 deaths related to PCA pumps versus 16deaths for all other large volume infusion pumps(LVP).5 The installed number of LVPs is approxi-mately 10-times greater than the number of PCApumps, suggesting the risk of death from anadverse event with a PCA pump is at least 10-timesgreater than with LVPs. Recent University HospitalConsortium (UHC) survey data found that 9 of 15members who responded to a survey identifiedrecent PCA adverse events as potentially costly interms of liability exposure.
The 2004 ASA Annual Meeting (www.asaab-stracts.com) featured many “better mousetraps” forpulse oximetry, capnography, and systems to pre-vent and intervene in respiratory insufficiency. Yet
Letter to the Editor
PCA Presents Serious Risks
Check out our new andimproved website at
www.apsf.org• Grant Guidelines• Search Engine• Back Issues of Newsletter• Safety Links• Sponsor List• Foundation Information
User-Friendly & Informative!

APSF NEWSLETTER Summer 2005 PAGE 34
See “Bellows,” Next Page
Dear SIRS:
We are currently evaluating new anesthesiamachines for purchase. One of the models is a 2005Datascope Anestar model. It has a hanging bellows.
The company states that the hanging bellows isno longer a concern. The uncoupling of the freshgas flow means that an increase in fresh gas flowwill NOT increase the tidal volume.
Do you have any resources, evaluations, or com-ments about the hanging bellows on the newmachines? Dräger and Datex-Ohmeda do not havethis type of bellows.
David A. Ciochetty, MDDirector, Anesthesia DepartmentPassavant Area HospitalJacksonville, IL
Response:
Dear Dr. Ciochetty,
Datascope appreciates the opportunity torespond to your inquiry about descending bellowsand their relationship to a fresh-gas decoupledanesthesia circuit. However, before I get into thetechnical description of the Anestar’s circuit, Iwould like to unequivocally state that any modernanesthesia machine, marketed in the U.S. today,including the Anestar, is safe regardless of whichventilation technology is being employed. Informa-tion to the contrary may be outdated or intended tomislead.
As cost-effective sensor technology and embed-ded software have been integrated into anesthesiamachines over the recent past, clinicians have bene-fited from new functionality unattained in previousgenerations of anesthesia delivery equipment. Moreimportantly, such technology adds and automatesan increased level of vigilance, with the ultimatebenefit of increasing patient safety. Similarly, I amreminded of how driver safety is improved in amodern automobile through accepted invisible fea-tures such as ABS and traction control. All anesthe-sia systems on the market today control the freshgas flow within the breathing cycle to achieve con-stant tidal volume delivery. In part, they depend ontheir alarm technology and other monitoring, suchas capnography, to alert the user in case of discon-nects or leaks.
Besides accepted visual indications of discon-nects and leaks, manufacturers nowadays includeadditional alarms to appropriately alert the user.Several national and international standards havebeen developed to increase the safety and reliabilityof such indications.
Datascope’s Anestar has alarms which specifi-cally indicate the following conditions:
• Breathing circuit disconnect
• Peak pressure below minimum pressure alarm
• Tidal volume lower than VTmin
• Minute volume below alarm limit
• Ambient air intake: check fresh gas setting.
These alarms are in addition to a graphic,breath-by-breath, display of the pressure wave-form.
Besides the electronic vigilance, in the case of afresh-gas decoupled system, the physical/visualindication has shifted from the bellows to the reser-voir (breathing) bag, which is always in the circuit.During normal operation, the bag has a full appear-ance and appears to pulsate, inflating slightly dur-ing inspiration and returning to normal volumeduring expiration. But, in case of a disconnect, or amajor leak, the bag will deflate after a few breaths,simulating the behavior of ascending bellows.
If the leak is less than the fresh gas flow, the bag(reservoir) will supplement the fresh gas flow,while continuing to ventilate the patient and thebag will appear to pulsate more deeply. Since, indi-rectly, leaks are an implied topic of this discussion,I would like to point out that the Anestar breathingcircuit, including the ventilator, absorber, valves,and sensors, are implemented in a module within asingle aluminum block virtually eliminating thepossibility of internal system leaks. Furthermore,the breathing module is warmed to 35˚C to preventcondensation from occurring within the breathingcircuit and the bellows.
At this point, I would like to provide a briefdescription of the operation of the Anestar’s freshgas decoupling breathing circuit. Simply stated, afresh gas decoupled anesthesia circuit delivers theset tidal volume to the patient independently of thefresh gas setting. We believe that the accurate deliv-ery of set tidal volume is clinically important, espe-cially when ventilating children.
In such a circuit, the bellows, reservoir bag, anddecoupling valve facilitate a straightforward way toimplement this technology without the need forexternal sensors and a feedback mechanism. Inaddition, this circuit’s configuration also facilitatesa compliance compensation method, which correctsfor compliance deviations external to the breathingmodule (e.g., patient’s breathing hoses).
Descending Bellows Drives Question
Dear SIRS refers to the Safety Information
Response System. The purpose of this column is
to expeditiously communicate technology-related
safety concerns raised by our readers, with input
and responses from manufacturers and industry
representatives. This process was developed by
Drs. Michael Olympio, Chair of the Committee on
Technology, and Robert Morell, Editor of this
newsletter. Dr. Olympio is overseeing the column
and coordinating the readers’ inquiries and the
responses from industry. Dear SIRS made its
debut in the Spring 2003 issue.
Michael Olympio, MD, Chair of the APSF Committee onTechnology and Co-Founder of the SIRS Initiative.
S AFETY
I NFORMATION
RESPONSE
S YSTEM
Dear SIRS

APSF NEWSLETTER Summer 2005 PAGE 35
2. During inspiration, the decoupling, PEEP, andbellows valves close while the ventilatorcontroller generates a calculated flow of drivegas into the bellows housing. The bellows isdisplaced by the volume flowing into the bellowshousing to create a positive pressure in thepatient’s lungs and in the pathway between the
decoupling and PEEP valves. The carbon dioxideabsorber, APL valve, and reservoir bag areisolated from the patient circuit. Duringinspiration, fresh gas flows into the reservoirbag. Once the bag is filled, excess gas flows outthe waste gas scavenger. Airway pressure ismonitored inside the breathing module, and isadditionally used to compensate for compliance.
3. During expiration, based on the selected breathrate and I:E ratio, the decoupling, PEEP, andbellows valves open to allow gas to flow. At thattime, the ventilator controller stops the flow ofdrive gas to the bellows housing. When thesevalves open, exhaled gas flows back through theone-way expiratory valve and carbon dioxideabsorber. Based on the fresh gas flow rate, aportion of the exhaled gas flows out the APL anda portion is re-circulated. During exhalation,fresh gas flows through the open decouplingvalve to refill the bellows, as the drive gasvolume in the bellows housing is vented throughthe open bellows valve. As the bellows falls, gasis sourced from the fresh gas inlet first, which isthe path of least resistance. The next source ofgas is the gas returning from the absorber, andonly if there is an interruption in the fresh gassource is gas drawn from the bag. The gas flowpriority scheme, described above, is facilitated bythe design of the Anestar’s breathing module.Exhaled volume is measured by a hot wiresensor located inside the breathing module, nearthe expiratory valve.
In summary, Dr. Ciochetty, the descending bel-lows is an essential part of the Anestar’s safe, state-of-the-art, reliable, and cost effective anesthesiacircuit.
Fresh gas decoupling keeps complexity to aminimum and offers the clinical advantage of main-taining the set tidal volume independently of thefresh gas flow.
Respectfully Submitted,
Abe AbramovichDirector, Anesthesia Systems DevelopmentDatascope Corp., Patient Monitoring DivisionMahwah, NJ
Following the Anestar’s simplified schematicrepresentation:
1. When activated, the ventilator is immediatelyready to deliver volume to the patient.
Inspiration
PEEP Valve
To WasteGas Scavenger
Drive Gas
Neg. Press. Relief Valve
Decoupling Valve
Fresh Gas Inlet
Bellows Valve
V
V
P
Expiration
PEEP Valve
To WasteGas Scavenger
Drive Gas
Neg. Press. Relief Valve
Decoupling Valve
Fresh Gas Inlet
Bellows Valve
V
V
P
Figure 1: Anestar Simplified Schematic Representation During Inspiration
Fresh Gas Decoupling Minimizes Complexity“Bellows,” From Preceding Page
Figure 2: Anestar Simplified Schematic Representation During Expiration
New APSF web address:
www.apsf.org
summer 2005.qxd 8/15/05 2:24 PM Page 20

APSF NEWSLETTER Summer 2005 PAGE 36
of compromise of up to 10 minutes may haveoccurred. The patient was not found to havesustained awareness or other lasting injury uponemergence.
In conclusion, it would seem appropriate tohave specific national standards for MRI anesthesiawhich meet general published OR guidelines. Edu-cation of colleagues regarding the complete lack ofdanger in the MRI for personnel without metalimplants appears necessary, while individuals withcontraindications to undergo MRI scanning mayneed to exclude themselves from work in this area.MRI-compatible equipment can seem very expen-sive, until the cost of the scanner or patient deathputs it into perspective. Equipment chosen by MRIdepartments may be so foreign to anesthesia per-sonnel (as in this instance) as to present an addi-tional danger due to non-familiarity. Oddlyenough, even some of these MRI-approved devicesare highly magnetic and non-"MRI-FDA approveddevices" have been used safely for years. Modernstandards should enhance safer, modern anesthesiatechniques and may serve to facilitate the acquisi-tion of appropriate equipment in financially tryingtimes. Anesthesia safety should not be compro-mised by historic patterns, unfounded fears, or areluctance to remain at the side of the patient with-out specifically identified dangers. The separationof anesthesia providers and equipment from thepatient’s side in the MRI suite should be relegatedto the annals of history.
Paul M Kempen, MD, PhDPittsburgh, PA
References
1. Gooden CK, Dilos B. Anesthesia for magnetic resonanceimaging. Int Anesthesiol Clin 2003;41:29-37.
2. Hall WA, Liu H, Martin AJ, et al. Safety, efficacy, andfunctionality of high-field strength interventional mag-netic resonance imaging for neurosurgery. Neurosurgery2000;46:632-42
3. Schmitz B, Nimsky C, Wendel G, et al. Anesthesia dur-ing high-field intraoperative magnetic resonance imag-ing experience with 80 consecutive cases. J NeurosurgAnesthesiol 2003;15:255-62.
4. Menon DK, Peden CJ, Hall AS, Sargentoni J, WhitwamJG. Magnetic resonance for the anaesthetist. Part I:Physical principles, applications, safety aspects. Anaes-thesia 1992;47:240-55.
5. Stoelting RK: APSF stresses use of audible monitoralarms. ASPF Newsletter 2004;19:1, 19.
Later, and resource information. The content is per-sonal, dramatic, and extremely important. Thedestructive forces of drug addiction are presentedthrough the eyes of family, friends, and coworkersof real anesthesia providers whose lives weredestroyed, and ended, by substance abuse. Duringour careers, we will all likely encounter a colleagueor coworker who is an addict. Education may helpus recognize the problem and intervene appropri-ately. During my 22 years in anesthesia, I have per-sonally known 4 anesthesia providers who wereaddicts: 2 physicians, and 2 CRNAs. One physicianwas resuscitated after being found in full arrestwith a needle in his arm, 1 CRNA fell unconsciouswhile administering a general anesthetic, and 1anesthesia resident (who appears on this video) isnow dead, despite intervention and multipleattempts at treatment and rehabilitation. This is areal problem, affecting real people, and impactingpatient safety in a dramatic way. Wearing Masks II isa tremendous educational tool that all anesthesiaproviders should watch. Contact and orderinginformation is available from the websitewww.allanesthesia.com.
SAAC/AAPD (Society of Academic Anesthesi-ology Chairs/the Association of AnesthesiologyProgram Directors) has also recently produced aDVD entitled Collateral Damage: Drug Abuse andAnesthesiology. Contact and ordering informationfor this video is available from the websitewww.aapd-saac.org. Finally, a recent article inJAMA by Domino, Hornbein, et al.1 examined riskfactors for relapse in health care professionals witha history substance abuse.
Reference
1. Domino KB, Hornbein, Polissar NL, et al. Risk factorsfor relapse in health care professionals with substanceuse disorders. JAMA 2005;293:1453-60.
by Robert C. Morell, MD, Editor
Drs. Tom Hornbein, Raymond Roy, and LynnHankes along with Diana Quinlan, CRNA, servedas Executive Directors for the new video WearingMasks II. The video, produced by the Coalition forthe Prevention of Substance Abuse in Anesthesia, isan excellent educational tool illustrating the dan-gers of substance abuse and drug addiction in anes-thesia. Specific focus is directed toward behavioralpatterns that may be recognized in impaired healthcare professionals along with signs of addiction.The goal of this presentation is to help identifyaddicted anesthesia providers and help them entersafe and anonymous treatment. This video is avail-able in DVD format and has 5 parts, which includean introduction, the original Wearing Masks I video,discussion questions, Wearing Masks: Ten Years
New Video Drives HomeDangers of Substance Abuse
A Statement by the ExecutiveCommittee of the APSF
From time to time, the Anesthesia Patient Safety Foundation reconfirms its
commitment of working with all who devote their energies to making anesthesia
as safe as humanly possible. Thus, the Foundation invites collaboration from all
who administer anesthesia, all who supply the tools of anesthesia, and all who
provide the settings in which anesthesia is practiced, all individuals and all
organizations who, through their work, affect the safety of patients receiving
anesthesia. All will find us eager to listen to their suggestions and to work with
them toward the common goal of safe anesthesia for all patients.
“MRI,” From Page 32
MRI RequiresHigh Vigilance
® working forpatient safety

APSF NEWSLETTER Summer 2005 PAGE 37
dle and/or syringe on multiple patients. These find-ings indicate that millions of patients per year werebeing exposed to used needles and syringes poten-tially contaminated with life-threatening diseaseorganisms. The study also indicates that there is agreat deal of confusion regarding proper syringeand needle usage among all health care providers.
The AANA sent letters and press releases to theAmerican Hospital Association, American MedicalAssociation, American Society of Anesthesiologists,American Dental Association, American Associa-tion of Oral and Maxillofacial Surgeons, AmericanNurses Association, and Nurse OrganizationalAlliance to inform them of the issue and to invitethem to join in developing an agenda for an upcom-ing patient safety initiative. Involvement of theAnesthesia Patient Safety Foundation was dis-cussed with foundation leadership. In addition, theAANA initiated a project to solicit input fromselected national health care organizations, accred-iting agencies, federal government agencies, andmedical and nursing professional organizations.The goal of this collaboration was to identifyactions to date, identify additional strategies toaddress the reuse issue, and gauge interest in par-ticipation with AANA and other stake holders onfuture initiatives.
An article entitled “Transmission of Hepatitis Band C Viruses in Outpatient Settings—New York,Oklahoma, and Nebraska, 2000-2002” appeared inthe September 26, 2005, issue of Morbidity and Mortal-ity Weekly Report. The article noted the AANA initia-tive and stated, “CDC is working with professionalorganizations, advisory groups, and state and localhealth departments to address these issues.”
JCAHO Plans to Raise AwarenessIn late 2003, a project was completed by AANA
that surveyed national health care organizations,accrediting agencies, federal government agenciesand medical and nursing professional organizations.The majority of organizations responding to the sur-vey indicated that they thought targeted educationalinitiatives to improve infection control practicesrelated to syringe and needle reuse were needed.Nursing organizations offered to collaborate withthe educational initiatives. The following excerptsfrom the final report reflect some of the findings:
“Most organizations report that they are makingthe information about needle/syringe reuseavailable to leaders and members throughpublications and web sites. Several organizationspointed to their position statements on infectioncontrol standards as their position on the issueincluding the American Hospital Association(AHA). AHA reported that the issue is one ofreprocessing and not reuse of devices, notingthat a caregiver who takes a syringe/needle,presumably labeled as a single use medicaldevice, and uses it more than once (on a different
patient) is engaging in reuse of a single usedevice. . . unless the syringe/needle is reprocessed.If a caregiver is simply using it again and again. . .it is a clear violation of federal regulations. TheAmerican College of Healthcare Executivesreported that they would not take a position onthe issue but would look to AHA to address thematter. The American Organization of NurseExecutives remarked that they learned of thismatter from AANA and had distributed theinformation to members. The American Societyfor Healthcare Risk Managers recognized theneedle/syringe reuse problem and advised,“Attention needs to be kept on this issue throughthe JCAHO infection advisory panel, particularlyas it relates to clinics and doctors’ offices.”
The Joint Commission on the Accreditation ofHealthcare Organizations (JCAHO) reportedplans to raise the awareness of their surveyorsabout reuse of “single use” devices on more thanone patient, including needles and syringes.JCAHO reported that the “whole issue of singleuse devices” is a problematic matter. JCAHOreported that they have revamped their infectioncontrol standards and 1 standard to be posted in2005, IC 4-10, will relate to infection control andaddress the matter of reuse of devices that aredeemed disposable by the manufacturer.
Early in 2004, the CDC’s Division of HealthcareQuality Promotion and the Division of ViralHepatitis were developing proposed initiatives toaddress the problem of patient-to-patient transmis-sion of blood-borne pathogens in health care set-tings. In late 2004, a representative from the CDCwork group charged with infection control inambulatory care settings shared with AANA theCDC’s concern that despite their 2002 bulletinregarding reuse of needles and syringes on multiplepatients, outbreaks of Hepatitis B and Hepatitis Cattributed to syringe reuse continue. While dis-cussing the issue, the representative noted, “The[AANA’s] recommendations seem so intuitive, yetit is so difficult to reach groups who may providepatient care and who are not aware of the risks ofreusing injection apparatus and contamination ofmulti-dose vials. We [CDC] will be addressing thistopic again soon and will pass on this informationto the working group.”
In April 2005 the CDC sent the AANA a requestfor the work group to continue with an initial focuson injection safety. The CDC expressed a concernthat in spite of publicized outbreaks of Hepatitis Band C, some unsafe injection practices, particularlythe injection of residual medication left in a syringethat has already been used on another patient, con-tinue during anesthesia care and are underreported.
Dr. Lester is a Certified Registered Nurse Anes-thetist, past President of the American Association ofNurse Anesthetists, and a member of the APSF Board ofDirectors and Editorial Board.
by Rodney Lester, PhD, CRNA
News reports in September 2002 revealed thatclusters of patients in Oklahoma, Nebraska, andNew York had been diagnosed with Hepatitis C.The common element in all 3 of these outbreakswas that syringes and needles had been reused,including the injection of an expensive or con-trolled drug into the IV line of more than 1 patientin order to avoid “wasting” medication. Even moretroubling were the anecdotal reports that thesewere not isolated incidents—that the practice wasnot only permitted, but encouraged, as a cost-sav-ing measure. Infection control specialists saw thereusing of syringes and needles as part of the cul-ture in some areas of practice and had given uptrying to change it.
In response to these events, the American Asso-ciation of Nurse Anesthetists (AANA) convened atask force to develop a series of short-term andlong-range strategies to address this serious patientsafety issue. The following are some of the strate-gies suggested for further consideration:
• educating providers and consumers as to theproper use of devices and the consequences ofmisuse
• issuing of a joint statement by health careorganizations condemning the practice andciting best practices
• conducting more research into the practice todetermine how prevalent misuse is
• identifying the gap between infection controlstandards and compliance with standards, i.e.,why is misuse happening and what can be doneabout it
• inspecting the use of syringes and needles as partof the JCAHO and Magnet processes
• publishing a booklet or manual on use andmisuse of needles and syringes.
As the initial step, the AANA sent more than40,000 letters with copies of Infection ControlGuidelines to all CRNAs, nurse anesthesia students,and program directors to raise awareness of thisissue and urge strict adherence to the guidelines.Letters were also sent to the CEOs of hospitals andambulatory surgery centers urging them to take anactive role in assuring compliance with infectioncontrol guidelines. The AANA also developed aseries of educational offerings addressing infectioncontrol, which continue to be presented.
Survey Reviews ContinuedSyringe Use
In October 2002, a telephone survey was con-ducted by Cooper Research to determine the scopeof the problem on needle and syringe reuse byhealth care providers. The survey findings revealedthat 1 in 100 of those surveyed reuse the same nee-
Syringe Reuse Transmits Infection

APSF NEWSLETTER Summer 2005 PAGE 38
tice” as recommended by the IOM report, the stan-dard was subject to a period of national review andpublic comment and was promulgated with therequirement that it be enforced by state boards ofpharmacy and subjected to survey by accreditingorganizations. Of course, the pharmacy licensingboards only have jurisdiction over pharmacies andpharmacists, but the USP and JCAHO requirementsresulting from this standard apply to practitionersof all types, in all health care settings where med-ications are compounded, including anesthesiaproviders in the operating room (OR).
USP Standard Has Long HistoryTo go back a step further, what was the back-
ground for this new USP Standard on medicationcompounding? For the past 3 decades, publishedcases or series of cases of infections in patientsresulting from contaminated medications elevatedthe concern for the safety of compounded medica-tions, including parenteral nutrition, cardioplegia,steroids, and analgesics. This history included 4cases of fungal meningitis in North Carolina, onefatal, following epidural methylprednisolone injec-tion contaminated at the same compounding phar-macy.2 Additional cases of meningitis fromepidural injection of contaminated steroids werereported in California and Michigan. A series of 11patients receiving cardioplegia contaminated byEnterobacter was reported in 1986, with 8 patientsrebleeding after surgery and 5 patients dying.3 Overthis long history of safety concerns, particularly fordrug contamination by compounding pharmacies,the American Society of Health-System Pharmacists(ASHP), the National Association of Boards ofPharmacy (NABP), and the USP have performedpractice surveys and made recommendations topharmacists and pharmacy technicians to try toimprove medication safety. In 1991, the firstnational survey of compounding practices was per-formed by the ASHP,4 and that organization pub-lished voluntary practice guidelines in 1993.Another survey was performed in 1995, the guide-lines were revised in 2000, and a third survey wasperformed in 2002. None of these surveys showedsignificant improvement or compliance with thevoluntary (and expensive) ASHP guidelines, andtherefore national standards were promulgated in2004 (USP 797).
How does the United States Pharmacopeiadevelop such standards? The USP “is a nonprofit,nongovernmental, standard-setting organizationthat advances public health by ensuring the qualityand consistency of medicines, promoting the safe
and proper use of medications, and verifying ingre-dients in dietary supplements. These standards,which are recognized worldwide, are developed bya unique process of public involvement through thecontributions of volunteers representing pharmacy,medicine, and other health care professions, as wellas science, academia, government, the pharmaceuti-cal industry, and consumer organizations.” Thedetails of the new, 2004, USP Standard (797) includeits goal “to prevent harm and fatality to patients” asa result of microbial contamination, content errors,or ingredient errors in the compounding of sterilepreparations. The definition of a “compounded ster-ile preparation” from USP is quite broad, andincludes any of the following:
a) Preparations prepared according tomanufacturer’s labeled instructions and othermanipulations when manufacturing sterileproducts that expose the original contents topotential contamination.
b) Preparations containing non-sterile ingredientsor employing non-sterile components anddevices that must be sterilized beforeadministration.
c) Biologics, diagnostics, drugs, nutrients, orradiopharmaceuticals that possess either of the 2previous characteristics and which include, butare not limited to, baths and soaks for live organsand tissues, implants, inhalations, injections,powder for injection, irrigations, metered sprays,and ophthalmic and otic preparations.
Obviously, nearly any manipulation of IV medica-tions could expose the contents “to potential contami-nation,” and other medical specialties such as nuclearmedicine have expressed concern for the effect ofthese far-reaching regulations on their practice.5
The Standards identify various risk levels formedication compounding, and anesthesia providersonly prepare sterile solutions from sterile ingredi-ents, for immediate administration or administra-tion over a limited number of (but <24) hours. Thiswould likely qualify as a “low-risk” level for micro-bial contamination6 in the professional judgment ofpharmacy and anesthesiology practitioners, com-pared to preparation of IV admixtures for adminis-tration over several days (“medium risk”), orpreparation from non-sterile components for latersterilization (“high risk”). Medication preparationby anesthesia providers also usually takes place inan OR with a required minimum of 15 air changesper hour (ACH), and usually by an individual
by Robert S. Weller, MD
Patient safety is an issue that has received wide-spread national attention following the Institute ofMedicine’s (IOM) report in 1999: To Err is Human:Building a Safer Health System, in which the risk ofpatient harm from medical errors was identified.1Included in this report was Recommendation 8.2:“Health care organizations should implementproven medication safety practices.”
The Joint Commission on the Accreditation ofHealthcare Organizations (JCAHO) has includedimproving the safety of medication administrationin its “National Patient Safety Goals” for both 2004and 2005, and will be looking closely at compliancewith Medication Administration Standards. Threespecific line-items in the Patient Safety Goals are toremove concentrated electrolyte solutions frompatient care units, to standardize and limit the num-ber of drug concentrations available, and to identifyand annually review a list of look-alike/sound-alike drugs and take action to prevent errors involv-ing the interchange of these drugs.
JCAHO Standards Are Detailed and Sweeping
The actual JCAHO Medication ManagementStandards for January 2004 are far more detailedand sweeping than the “Goals,” and directly impactanesthesia providers. The 2004 Standards includeMedication Management Standard MM 4.20:“When an on-site, licensed pharmacy is available,only the pharmacy compounds or admixes all ster-ile medications, intravenous admixtures, or otherdrugs except in emergencies or when not feasible(for example, when the product’s stability isshort).” Intravenous admixture is defined as “thepreparation of pharmaceutical product whichrequires the measured addition of a medication to a50 ml or greater bag or bottle of IV fluid. It does notinclude the drawing-up of medications into asyringe, adding medication to a buretrol, or theassembly and activation of an IV system that doesnot involve the measurement of an additive. ThisStandard 4.20 specifies that preparation of such anIV admixture must be performed in a Class 100environment (airborne >0.5 micron particulatecount of <100 per cubic foot).
Where did this requirement originate? Itappears that the JCAHO has adopted, word-for-word, the compounding standard from the UnitedStates Pharmacopeia (USP), which went into effectin January 2004. Although the USP might not meetthe definition of “proven medication safety prac-
Safety Implications of JCAHOStandards Raise Concerns
See “JCAHO,” Next Page

APSF NEWSLETTER Summer 2005 PAGE 39
wearing a mask and non-sterile gloves, but clearlynot under a Class 100 hood. Having said this, anes-thesia medication has been implicated (rarely) inthe transmission of fungal and bacterial infection,most notably with the original propofol formulationwith resultant sepsis and multiple organ failure.7
Heightened awareness of the risk,8,9 handling rec-ommendations from the manufacturer, and refor-mulation of the solution have apparently reducedreports of patient infection, but other drugs havealso been shown to be contaminated after anesthe-sia provider preparation, and 2 reported cases ofhepatitis C transmission were linked to anesthesiamedication. Still, these are rare reports, and theIOM report identified Anesthesiology and its Anes-thesia Patient Safety Foundation (APSF) as a spe-cialty that had dramatically improved patient safetyover the last 20 years by collective action. Also, theAmerican Society of Anesthesiologists specificallydefines the anesthesiologist’s responsibilities inperianesthetic care as including the preparation andcheck of (equipment and) drugs.
Clearly, although pharmacy organizations havebeen struggling with these medication safety issuesfor many years, this new JCAHO MM 4.20 Standardhas caught anesthesia providers by surprise, andwe have had little direction in determining itsscope. In a recent list-serve query, the interpretationof MM 4.20 by academic health centers was quitevariable. Many institutions have adopted a practicethat requires pharmacy preparation of all IV admix-tures, while others consider the OR to be a uniquesite where infusions and other IV admixtures maycontinue to be prepared by anesthesia providers.
The careful consideration of the application ofJCAHO Standard MM 4.20 to anesthesia providerssuggests there may be a real and dangerous safetytrade-off that has not been part of the discussion todate. Once again, the intent of USP (797) and MM4.20 is to improve medication safety both from thestandpoint of reducing microbial contaminationand reducing the potential for errors in measure-ment or dilution. Since anesthesia is commonly pro-vided in the emergency setting which is anexclusion for pharmacy preparation of solutions,anesthesia providers will be placed in the positionof preparing IV admixtures only in crisis situations.The risk of measurement or contamination error islikely to be increased by lack of familiarity andexperience previously gained by compoundingsuch solutions on a daily basis. The emergency situ-ation with a critically ill patient is already a time-pressured and risk-laden setting; this is the lastplace one would want to increase the potential formedication error.
It seems far more rational to adopt institutionalpractice guidelines that document safe practice andminimize the already low risk of microbial contami-nation of solutions, and allow anesthesia providersto continue to prepare all manner of medications inthe OR environment. Such practices might include
• Mandatory use of gloves and mask whenpreparing IV admixtures from sterile ingredientsin an OR.
• Annual training in aseptic medicationpreparation and written exam competencedemonstration.
• Labeling of preparations with medication name,concentration, and time of preparation orexpiration date (Standard MM 4.30).
• Discarding of preparations used in the OR within24 hours, or when the patient leaves the OR orpost-anesthesia care unit (PACU) and istransferred to another patient care area.
If adopting these simple safeguards could meetthe requirements for safe compounding in a low-risk situation for contamination, one might avoidthe potential for increasing the risk of medicationmeasurement error.
Dr. Weller is an Associate Professor and Director ofOrthopaedic Anesthesia at Wake Forest UniversitySchool of Medicine, Winston-Salem, NC.
References
1. Kohn LT, Corrigan JM, Donaldson MS. To Err isHuman: Building a Safer Health System. Institute ofMedicine, Washington, DC: National Academy Press,1999.
2. Exophiala infection from contaminated injectablesteroids prepared by a compounding pharmacy--UnitedStates, July-November 2002. MMWR Morb Mortal WklyRep 2002;51:1109-12.
3. Hughes CF, Grant AF, Leckie BD, Baird DK. Cardio-plegic solution: a contamination crisis. J Thorac Cardio-vasc Surg 1986;91:296-302.
4. Crawford SY, Narducci WA, Augustine SC. Nationalsurvey of quality assurance activities for pharmacy-pre-pared sterile products in hospitals. Am J Hosp Pharm1991;48:2398-413.
5. Hung JC. USP general chapter <797> pharmaceuticalcompounding-sterile preparations. J Nucl Med2004;45:20N,28N.
6. Schubert A, Hyams KC, Longfield RN. Sterility of anes-thetic multiple-dose vials after opening. Anesthesiology1985;62:634-6.
7. Postsurgical infections associated with an extrinsicallycontaminated intravenous anesthetic agent--California,Illinois, Maine, and Michigan, 1990. MMWR Morb Mor-tal Wkly Rep 1990;39:426-7, 433.
8. Zacher AN, Zornow MH, Evans G. Drug contaminationfrom opening glass ampules. Anesthesiology 1991;75:893-5.
Institutional Guidelines May ReduceContamination of I.V. Solutions“JCAHO,” From Preceding Page
Web Survey on theAnesthesia MachinePre-Use Check
Many significant developments have occurredsince the Food and Drug Administration releasedthe latest version of the Anesthesia ApparatusCheckout Recommendations in 1993. Anesthesiaworkstations that include electronics and softwareas an integral part of their design and feature differ-ent variations of semi-automated pre-use checkshave begun to replace purely pneumatic anesthesiamachines. Not all anesthesia ventilators use a bel-lows design anymore; there are now also pistonventilators. There are substantive differences indesign, even within a given manufacturer’s productline. Monitoring, whether integrated into an anes-thesia workstation or as stand-alone units, is moreprevalent. The new ASTM standard F-1850 foranesthesia workstations was released in 1998.
An anonymous survey is currently being con-ducted via the web to assess compliance with the1993 Food and Drug Administration recommenda-tion to perform a pre-use check of the anesthesiamachine before every case. The survey questionsare designed to obtain insight about the reasons fornon-compliance and to seek patterns for non-com-pliance that could potentially be used to re-designthe pre-use check to enhance compliance and effec-tiveness. This survey is for all who perform theanesthesia machine pre-use check, including anes-thesia providers and anesthesia technicians.
We encourage active and candid participation ofthe APSF membership in the survey so that yourinput, concerns, and educational and training needsare adequately and accurately represented in thecurrent survey.
The survey can be accessed and completedanonymously at the University of Florida’sVi r tua l Anesthesia Machine website:http://www.vam.anest.ufl.edu/logincheck.html.To access the survey, one needs to register as a Vir-tual Anesthesia Machine user, which is free. Aftercompletion of the anonymous survey, you will beprovided access to a preview of a free web simula-tion of the 1993 FDA Anesthesia Apparatus Check-out Recommendations, whose development isfunded by the Anesthesia Patient Safety Founda-tion.
Sem Lampotang, PhDMember, APSF Committee on Education and TrainingProject Director, Virtual Anesthesia MachineProfessor of Anesthesiology
www.vam.anest.ufl.eduCheck out the Virtual Anesthesia Machine!

APSF NEWSLETTER Summer 2005 PAGE 40
Corporate DonorsFounding Patron ($400,000 and higher)American Society of Anesthesiologists (asahq.org)
Foundation Patron
($50,000 to $99,999)GE Healthcare
(gemedical.com)
Benefactor Patron ($25,000 to $49,999)
Abbott Laboratories (abbott.com)
Aspect Medical Systems (aspectms.com)
AstraZeneca Pharmaceuticals LP(astrazeneca.com)
Philips Medical Systems (med-ical.philips.com)
Tyco Healthcare (tycohealthcare.com)
Grand Patron ($15,000 to $24,999)Baxter Anesthesia and Critical Care (baxter.com)Dräger Medical (nad.com)Preferred Physicians Medical Risk Retention Group (ppmrrg.com)
Patrons ($10,000 to $14,999)Endo Pharmaceuticals (endo.com)Spacelabs Medical (spacelabs.com)
Sustaining Members ($5,000 to $9,999)Arrow International (arrowintl.com)B. Braun Medical (bbraun.co.uk)Becton Dickinson (bd.com)Cardinal Health, Alaris Products (alarismed.com)Datascope Corporation (datascope.com)Kimberly-Clark (kimberly-clark.com) LMA of North America (lmana.com)Medical Education Technologies, Inc. (meti.com)Organon (organon.com)Smiths Medical (smiths-medical.com)The Doctors Company (thedoctors.com)Vance Wall FoundationVital SignsSponsoring Members ($1,000 to $4,999)Anesthesia Business Consultants (anesthesiallc.com)Allied Healthcare (alliedhpi.com)
Armstrong Medical (armstrongmedical.net)Cerner Corporation (cerner.com)Cook Critical Care (cookgroup.com)Docusys, Inc. (docusys.net)Intersurgical Ltd (intersurgical.com)King Systems Corporation (kingsystems.com)Masimo Corporation (masimo.com)Molecular Products Ltd (molecularproducts.co.uk)Oridion (oridion.com)Somnia, Inc. (somniainc.com) Trifid Medical Group, LLC (trifidmedical.com)W.R. Grace (wrgrace.com)
Corporate Level Members ($500 to $999)Belmont Instrument Corporation (belmontinstrument.com)Boehringer Laboratories (autovac.com)Hoana Medical, Inc. (hoana.com)Lippincott Williams and Wilkins
Participating AssociationsAmerican Association of Nurse Anesthetists (aana.com)
Subscribing SocietiesAmerican Society of Anesthesia Technologists & Technicians (asatt.org)American Academy of Anesthesiologist Assistants (anesthetist.org)
Anesthesia Patient Safety Foundation
Community Donors (includes Anesthesia Groups, Individuals, Specialty Organizations, and State Societies)
Grand Sponsor ($5,000 and higher)American Association of Nurse AnesthetistsAmerican Medical Foundation Asheville Anesthesia AssociatesFlorida Society of AnesthesiologistsIndiana Society of AnesthesiologistsRobert K. Stoelting, MD
Sustaining Sponsor ($2,000 to $4,999)Alabama State Society of AnesthesiologistsAnesthesia Associates of MassachusettsAnesthesia Consultants Medical GroupAnesthesia Resources ManagementArizona Society of AnesthesiologistsNassib G. ChamounGeorgia Society of AnesthesiologistsGlenn P. Gravlee, MDIndianapolis Society of AnesthesiologistsIowa Society of AnesthesiologistsMassachusetts Society of AnesthesiologistsMichigan Society of AnesthesiologistsMinnesota Society of AnesthesiologistsOhio Society of AnesthesiologistsOld Pueblo Anesthesia GroupPennsylvania Society of AnesthesiologistsSociety of Cardiovascular Anesthesiologists
Contributing Sponsor ($750 to $1,999)Academy of AnesthesiologyAffiliated Anesthesiologists, Inc.American Society of Critical Care AnesthesiologistsJ. Jeffrey Andrews, MDAnesthesia Associates of Northwest Dayton, Inc.Anesthesia Services of BirminghamArkansas Society of AnesthesiologistsAssociation of Anesthesia Program DirectorsCapital Anesthesiology Association
Frederick W. Cheney, MDConnecticut State Society of AnesthesiologistsJeffrey B. Cooper, PhDDavid M. Gaba, MDJohn H. Eichhorn, MDIllinois Society of AnesthesiologistsKentucky Society of AnesthesiologistsThomas J. Kunkel, MDRodney C. Lester, CRNAEdward R. Molina-Lamas, MDMadison Anesthesiology ConsultantsMaine Society of AnesthesiologistsMaryland Society of AnesthesiologistsMembers of the Academy of AnesthesiologyMichiana Anesthesia CareMissouri Society of AnesthesiologistsRobert C. Morell, MDNebraska Society of AnesthesiologistsJohn B. Neeld, MDNevada State Society of AnesthesiologistsNew Mexico Anesthesia ConsultantsNorthwest Anesthesia PhysiciansNeshan Ohanian, MDOklahoma Society of AnesthesiologistsOregon Anesthesiology GroupOregon Society of AnesthesiologistsPhysician Anesthesia ServicePittsburgh Anesthesia AssociatesSociety of Academic Anesthesia ChairsSociety for Ambulatory Anesthesia Society of Neurosurgical Anesthesia & Critical CareSociety for Pediatric AnesthesiaSouth Carolina Society of AnesthesiologistsSouth Dakota Society of AnesthesiologistsTennessee Society of AnesthesiologistsTexas Society of AnesthesiologistsWashington State Society of AnesthesiologistsWest Jersey Anesthesia Associates, PAWisconsin Society of Anesthesiologists
Sponsor ($100 to $749)Anesthesia Associates of BoiseAnesthesia Associates of Chester CountyAnesthesia Associates of St. CloudSusan Bender, CRNAPaul E. Burke, MDCalifornia Society of AnesthesiologistsRobert A. Caplan, MDCardiovascular Anesthesia, LLCCHMC Anesthesia FoundationMelvin A. Cohen, MDStuart M. Cohen, MDColorado Society of AnesthesiologistsCommonwealth Anesthesia AssociatesPaula A. Craigo, MDGlenn E. DeBoerWalter C. Dunwiddie, MDNorig Ellison, MDJan Ehrenwerth, MDBarry J. Friedberg, MDJoseph Gartner, MDGeorgia Anesthesia AssociatesBarry M. Glazer, MDGriffin Anesthesia AssociatesPeter Hendricks, MDJames S. Hicks, MDDr. and Mrs. Glen E. HolleyVictor J. HoughIdaho Society of AnesthesiologistsIndependence Anesthesia, Inc.Sharon Rose JohnsonRobert E. Johnstone, MDDaniel J. Klemmedson, DDS, MDKansas Society of AnesthesiologistsRoger W. Litwiller, MDThomas T. McGranahan, MDMedical Anesthesiology Consultants CorporationMississippi Society of AnesthesiologistsRoger A. Moore, MDErvin Moss, MD
Joseph J. Naples, MDNew Hampshire Society of AnesthesiologistsNew Jersey State Society of AnesthesiologistsNew Mexico Society of AnesthesologistsBeverly K. Nichols, CRNAL. Charles Novak, MDDenise O’Brien, RNJill Oftebro, CRNANewton E. PalmerPhysician’s Accounts ReceivableMukesh K. Patel, MDGaylon K. Peterson, MDPhysician Specialists in AnesthesiaRichard C. Prielipp, MDDebra D. Pulley, MDRhode Island Society of AnesthesiologistsSanford Schaps, MDMuthia Shanmugham, MDSociety for Technology in AnesthesiaSouthern Tier Anesthesiologists, PCSouth County Anesthesia AssociationThe Woodlands Anesthesia AssociationUniversity of Maryland Anesthesiology AssociatesUtah Society of AnesthesiologistsVermont Society of AnesthesiologistsVirginia Society of AnesthesiologistsDrs. Mary Ann and Mark A. Warner, MDPamela K. Webb, PhDMatthew B. Weinger, MDWest Virginia Society of AnesthesiologistsDr. and Mrs. Wetchler, MDLawrence Wobbrock, JDWaterville Anesthesia AssociatesWest River Anesthesiology Consultants
In MemoriamIn memory of Gale E. Dryden, MD (friends of the
Dryden family)In memory of Walter H. Mannheimer (Texas
Society of Anesthesiologists)
Note: Donations are always welcome. Send to APSF; c/o 520 N. Northwest Highway, Park Ridge, IL 60068-2573 (Donor list current through June 21, 2005)

APSF NEWSLETTER Summer 2005 PAGE 41
Fatigue SwallowsUp VigilanceTo the Editor:
I am writing in response to the topic of fatigueand the practice of anesthesiology. It has been saidthat common sense cannot be taught in schools.Fatigue and performance are negatively correlated,as we all know from the admonishments to get agood night’s rest before exams. Don’t patientsdeserve even more consideration? Overworked doc-tors and medical errors have been a flashpoint fordiscussion ever since I was a resident 18 years ago.And we are still doing research to find out howmany medical errors are committed while fatigued.
Why do we need more studies to prove this? Doyou really think that the true incidence of death orpermanent injury will be discovered this way with-out exposing individuals, administrators, and hos-pitals to liability? I’ve learned all I need to knowabout vigilance as a truck driver. Vigilance is neces-sary to prevent accidents. Fatigue swallows up vigi-lance. But there’s more. Fatigue depletes ourcognitive power, diminishes our ability to retrievecritical information, and betrays our best intentions.We fail to see the obvious treatment and anestheticoptions when fatigued. And even if we do, theenergy to act on the knowledge of the best treat-ment plan is gone.
I find no reason for this continuing dialogue –fatigue and what to do about it other than an eco-nomic one: it costs more to hire additional people.Yet the economic costs of decreased productivityfrom injury due to medical errors is in the billionsof dollars. Until our leadership recognizes that thisis money we pay for as a society, which eventuallyimpacts on our health care costs and our compensa-tion, this cognitive dissonance will continue. As amatter of conscience, I as an individual will managemy fatigue in a way that occurs commonly, ifcovertly. I will not relieve my colleagues for breakson certain occasions, nor will I accept responsibilityto conduct an anesthetic for their ASA class IVpatient just to facilitate the OR schedule. I will takemy time to answer my pages. I will not move anyfaster to do endoscopy cases just because someonehas just decided to add on 3 more cases to analready full schedule. Without the element of risk,we can all be the good Samaritans that we imaginedourselves to be when we applied to medical school.With risk, everything changes. Let us stand up andfight to protect our patients instead of finding yetanother way to bend over and accommodate anoverly demanding system, because the next bend-ing over may just break our backs.
Herb Lee, MDNorth Brunswick, NJ
Epidurals for LaborAre Labor IntensiveTo the Editor:
I read the recent APSF edition regarding fatigueand sleep deprivation with great interest as I myselfstruggled to stay awake one morning after call. Itoccurred to me that in my 20 years of practice thatby far the greatest cause of fatigue, stress, and sleepdeprivation to me has been the escalating and inces-sant demands of obstetrical anesthesia and specifi-cally labor epidurals. The evolving standard of“every woman in labor deserves an epidural uponrequest” has enabled a small subgroup of patientsto consume a disproportionately large amount ofavailable anesthesia manpower. What was once aprivilege of a few has become an entitlement to alland a tremendous drain on anesthesia resources.
I would estimate that labor epidurals representless than 5% of patient volume and reimbursementto us nationwide but account for greater than 50%of the demand for after hour anesthesia services.
If we, as a specialty, are serious about address-ing the problem of fatigue caused by sleep depriva-tion, the obvious place to start would be tore-evaluate our professional obligation to performthese underfunded and non-essential proceduresafter hours.
The standards set for us by hospital administra-tors, obstetricians, and our own ASA, regardingprovision of labor epidural analgesia are not feasi-ble in hospitals where anesthesia providers mustwork the next day following call. Total ablation oflabor pain is a noble goal, but the cost to anesthesiaproviders in monetary and physical expenditure farexceeds the reimbursement. We should not have to“burn the candle at both ends” in order to appeaseone overly demanding group of patients by nightand risk detriment to others who are entitled to ourbest efforts by day. Those of us in small groups whotoil under these conditions could use some relief. Ihope ASA and APSF policy makers are listeningand can help in this regard.
Sincerely,TH Parker, Jr., MDMemorial HospitalBainbridge, Georgia
Letters to the Editor: AnesthesiaTechnicians AreProfessionals TooTo the Editor:
I would like to clarify for the readers of thispublication who may have been offended by thecomment made in response to an article in theWinter 2004-2005 issue of your newsletter, “ReaderCalls for Professionalism.” I quote, “I would like tothink that we are all professionals and not justtechnicians.” The definition of a technician is: a) of,relating to, or characteristic of a profession; b)engaged in one of the learned professions; c) char-acterized by or conforming to the technical or ethi-cal standards of a profession.
Why would a reader feel the need to respond tothe comment about “being a professional and notjust a technician”? The APSF Newsletter is read bymany anesthesia technicians who wish to enhancetheir knowledge in their profession of anesthesia.The need for anesthesia technicians in the field ofanesthesia has grown tremendously, and as it con-tinues to grow, the skills must continue to improvein order to provide the safest environment for theproviders and the patients who rely on the profes-sionals in the field of anesthesia. “Just a technician”implies that technicians are not a valuable asset tothe anesthesia team. This was clearly not the intentof the writer. I would like to think that the reasonfor reading this publication is to further our knowl-edge in our profession, thereby eliminating the pos-sibility of repetitive, career-ending mistakes, andgaining the knowledge needed to give patients thebest and safest care possible while their lives are inour hands.
I will continue to increase my knowledge as ananesthesia technician by reading this publicationand any other publication that may benefit my pro-fession. After all, this is what a technician must do:to be a professional!
Daniel A. Clark, Cert. A.T.Jacksonville, FL
Editor’s Note:
We would like to apologize for any negativeconnotation to Mr. Clark and to the manyprofessional anesthesia technicians whocontribute their important skills and effort topatient care.
Improved
APSF website
www.apsf.org

APSF NEWSLETTER Summer 2005 PAGE 42
Letters to the Editor:
To the Editor:
I am not a constant reader of the APSF Newslet-ter so perhaps I've missed the APSF’s position onthis topic; nevertheless, I think it represents a sub-ject worthy of APSF attention. As a supposed“authority” on the clinical use of neuromuscularblocking agents (NMBA), I still come across clini-cians who opine, “I haven't used a peripheralnerve stimulator (PNS) in 20 years and I see noreason to start now.” On a recent visit to a wellrespected academic medical center, the anesthesi-ologist in charge of pediatric anesthesia told methat he never uses PNS units since they “don'twork in kids.”
While a recent editorial opinion (Anesthesiology2003;98:1037-9) certainly does not support theseideas, I am unaware of any published clinicalguidelines by organizations such as the APSF orthe ASA on the subject. I think the time has comefor these societies to clearly state that the adminis-tration of nondepolarizing relaxants in the absenceof neuromuscular monitoring represents substan-dard care.
In a letter to a correspondent, I noted in part. . .
"I agree that there are only limited outcome data(Acta Anaesthesiol Scand 1997;41:1095-1103) to sug-gest that patients who arrive in the PACU with TOFratios of 0.50, for example, have a significantlyincreased morbidity or mortality compared to indi-
viduals who have attained a TOF ratio > 0.80. Toprove this thesis would require a rather massiveproject that is not likely to be funded. However,anesthesiology as a specialty has been lauded forthe drop in anesthesia risk, which has been docu-mented over the last 20 years. Improvements inmonitoring have been cited as a major determinantof this perceived improvement in outcome. Never-theless, there is little evidence-based data thatclearly show that pulse oximetry or capnography infact reduces overall morbidity. Yes, anecdotalreports abound, but the same can be said for the useof objective neuromuscular monitoring.
"When I was a resident (over 40 years ago) wedid not have or routinely use electrocardiography,pulse oximetry, capnography, anesthetic agentmonitors, or cerebral-function physiologic moni-tors. Nor did we miss them. Now I would feelnaked without them. Do I use the TOF-Watch or theDatex M-NMT module in every case where nonde-polarizing blocking drugs are administered? No.However, I sincerely believe that this monitoringmodality should be routinely available to the anes-thesiologist. My experience suggests that it is agreat pedagogical tool. What it teaches is that clini-cal judgment is often wrong.”
Aaron F. Kopman, MD New York, NY
Silenced AlarmResults in“Near-Miss”To the Editor:
I read with interest the deliberations regardingthe use and abuse of alarms in the anesthetic envi-ronment in the Winter 2004-05 issue of the Newslet-ter. During my residency training I observed a nearmiss where a resident had silenced all monitoringalarms during a coronary artery bypass graft proce-dure. The resident disconnected the breathing cir-cuit while the surgeon incised the sternum. He thenforgot to reconnect it. It was only when I walkedinto the OR and asked why the pulse oximeter wasreading 20% that he realized what had happened.Frantic efforts ensued and fortunately the patientcame to no harm. But it was a salutary lesson forboth of us.
I routinely use all monitors available. Duringmy preoperative check of the anesthetic machine, Ialso check and activate all monitoring alarms.Some anesthetic machines and monitors are setautomatically to default settings that are not appro-priate. For example, monitors that have been in userecently in our hospital set the default lower oxy-gen saturation alarm to 88%. Following the recom-mendation of a colleague I set mine higher andnow use 95% as the lower limit of oxygen satura-tion that I will accept. This gives early warningwhile there is still time to react.
In my practice the use of pulse oximeter tone isessential. I am continually amazed to see senior col-leagues switch this off and rely on the single beat ofthe EKG monitor. Residents working in our teamare routinely taught to use pulse oximeter tone atall times, and we stress all the information this pro-vides: oxygen saturation, the presence of sinusrhythm or arrhythmias, and indication of cardiacarrest . We continually emphasize the importance of“tuning in their ears to the tone.” Its absence orchange should spark immediate investigation, par-ticularly when they are away from the “anestheticend of the table.”
Robert N. Norton, BSc, MBChB, FRCAKent, UK
Noise Pollution ObscuresPulse Ox ToneTo the Editor:
While I agree that the pulse oximeter tone,alarms, and so forth should be audible and that thepulse oximeter tone should reflect the patient's oxy-gen saturation, it is often VERY difficult to hearthese sounds over the 80-90 decibel sound pressurelevel of the music being blasted by the surgeons(and, unfortunately, now the anesthesia teams).
We need a limit on the volume of the “music”that is played in the OR. Often, when I am doing acase where I have had to place a temporary pace-maker (like a pacemaker-dependent patient havinga mastectomy overlying the generator), many of thesurgeons play music loudly enough that I have toturn it down myself.
It is only a matter of time before someone (thepatient) gets hurt.
Marc A. Rozner, PhD, MDHouston, TX
SUPPORT YOUR APSFYour contribution is
appreciated!
Monitoring NeuromuscularBlockade Often Overlooked

APSF NEWSLETTER Summer 2005 PAGE 43
Representatives from Absorbent Manufacturing join with APSF to explore safety considerations of absorbent dessication on April 27th, 2005 in Chicago, IL. Participants are (top row,left to right) Jeffrey Mack; Randall Ostroff, MD; Jonathan Deutsche, MD; Juergen-Ralf Lange; Christoph Manegold; Robert Stoelting, MD (APSF President); (bottom row, left to right)Michael Olympio, MD; Mike Holder; Dr. Michael Clarke; Dr. Ciarán Magee; Michael Mitton, CRNA.
Dr. Ganesh is Assistant Professor of Anesthesia atthe Department of Anesthesiology and Critical CareMedicine, The Children’s Hospital of Philadelphia, PA.
Dr. Saubermann is Frances F. Foldes Professor andChairman of the Department of Anesthesiology, AlbertEinstein College of Medicine, Montefiore MedicalCenter, NY.
Dr. Nicolson is Professor of Anesthesia, AssociateAnesthesiologist-in-Chief and Director of the Divisionof Cardiothoracic Anesthesiology, Department of Anes-thesiology and Critical Care Medicine, The Children’sHospital of Philadelphia, PA.
Reference
1. Larach MG, Rosenberg H, Gronert GA, Allen GC.Hyperkalemic cardiac arrest during anesthesia ininfants and children with occult myopathies. Clin Pedi-atr (Phila) 1997;36:9-16.
More Photos From the Absorbent Conference (Article on Front Page)
Dr. Edmond I Eger, II, MD, addresses participants at Absorbent Conference.
MHAUS Reports“MHAUS,” From Page 31

Anesthesia Patient Safety FoundationBuilding One, Suite Two8007 South Meridian StreetIndianapolis, IN 46217-2922
NONPROFIT ORG.U.S. POSTAGE
PAIDWILMINGTON, DEPERMIT NO. 1387
APSF NEWSLETTER Summer 2005 PAGE 44
Inside: • Report on APSF Conference on Safety Concerns ofDessicated Carbon Dioxide Absorbents
• MHAUS Reports 3 Unique Cases of HyperkalemicCardiac Arrest
• Dear SIRS Explores Descending Bellows
• Syringe Reuse Transmits Infections
• JCAHO Standards Have Safety Implications
Thanks to all of our readers, supporters anddonors for making patient safety a high priority.
Inside:
MH News ..............................
..Pages 30-31
Descending Bellows
(Dear SIRS)..............................
Page 34
Syringe Reuse
Transmits Infection ..............Page 37
Safety Implications of
JCAHO Standards..................Page 38
Donors ..............................
............Page 39
NEWSLETTER
Volume 20, No. 2, 25-44
Circulation 75,648
Summer 2005
www.apsf.org The Official Journal of the Anesthesia Patient Safety Foundation
by Michael A. Olympio, MD
There is increasing evidence that exposure of
volatile anesthetics to desiccated carbon dioxide
absorbents may result in exothermic reactions lead-
ing to fires in anesthetic breathing circuits and pro-
duction of toxic products (e.g., carbon monoxide,
compound A, methanol, formaldehyde). Although
fires have only been reported in association with
sevoflurane exposed to desiccated Baralyme®
(Allied Healthcare/Chemetron, withdrawn from the
market), there is significant evidence that potentially
toxic products can be produced upon exposure of
volatile anesthetics to other desiccated absorbents
containing strong bases, particularly potassium and
sodium hydroxide. In some cases this may lead to
sub-clinical carbon monoxide exposure.
In view of these continued anesthesia patient
safety concerns, the Anesthesia Patient Safety Foun-
dation invited medical experts and industry repre-
sentatives (manufacturers of carbon dioxide
absorbents, anesthesia machines, and volatile anes-
thetics) to attend a conference entitled Carbon Diox-
ide Absorbent Desiccation: APSF Conference on Safety
Considerations on April 27, 2005, in Chicago, IL. In
addition to medical experts and industry represen-
tatives (Table 1), APSF invited several organiza-
tions, including the American Society of
Anesthesiologists and the American Association of
Nurse Anesthetists to send observers to the confer-
ence (Table 2). The conference was funded by the
Anesthesia Patient Safety Foundation with the sup-
port of unrestricted educational grants from the 10
industry cosponsors.
The format of the conference included formal
presentations by the 4 medical experts as well as pre-
sentations by representatives of industry. Following
reports generated from small group break-out ses-
sions there was general discussion among all atten-
dees and development of a consensus statement to
reflect the stated goal of the conference, which was
“to develop a consensus statement to share with
anesthesia professionals on the use of carbon dioxide
absorbents so as to reduce the risk of adverse inter-
actions with volatile anesthetic drugs.”
Summary of Expert Medical
and Industry Representative
Presentations
Jerry A. Dorsch, MD, speaking on Anesthesia
Machine Characteristics That Promote Absorbent
Desiccation:
The retrograde flow of fresh gas through the
absorber can desiccate the absorbent. This may be
affected by a number of factors, including the
design of the anesthesia breathing system, the pres-
ence or absence of the reservoir bag, whether the
APL valve is open or closed, the relative resistance
through the components of the breathing circuit,
the fresh gas flow rate, I:E ratio, use of heat and
moisture exchangers, and scavenger suction. With
conventional breathing system design, removing
the bag, opening the APL valve, and occluding the
Y-piece all enhance retrograde flow and desicca-
tion. The effects of these maneuvers in newer, more
modern machines are variable, complex, and may
have the opposite effect. Furthermore, we do not
know of published data that describe the flow of
gas under these various conditions. Unfortunately,
the flow of gas in these breathing systems has not
been well studied.
®
See “Absorbents,” Page 27
Carbon Dioxide Absorbent Desiccation
Safety Conference Convened by APSF
Left to right, Drs. Dorsch, Olympio, Kharasch, Woehlck, Stoelting, and Eger speak at the APSF Conference on Safety
Considerations of Carbon Dioxide Absorbents on July 27, 2005, in Chicago, IL.
Evan D. Kharasch, MD, PhD, speaking on Heat,
Fire, and Smoke: Shining Light on the Issue of Carbon
Dioxide Absorbents and Anesthetic Degradation:
The chemical breakdown to compound A can
occur in moist, as well as desiccated absorbent, but
the potential for highly exothermic reactions and