sumj - volume 3 - issue 1
DESCRIPTION
ÂTRANSCRIPT


Acting Editor for this Issue: Kevin Barr [Year 3 Mental Health Nursing Student; University of Dundee
School of Nursing & Midwifery]
Editor-In-Chief: Laura Fraser [Year 5 Medical Student; University of Dundee Medical School]
Deputy Editor: Kevin Barr [Year 3 Mental Health Nursing Student; University of Dundee School of
Nursing & Midwifery]
IT Manager: Naomi McIlvenny [Year 5 Medical Student; University of Dundee Medical School]
Head Reviewer: Rebecca Grant [Year 1 Medical Student; University of St Andrews Medical School]
Features Commissioner: Lauren Copeland [BMSc Year Medical Student; University of Dundee Medical
School]
National PR Representative: James Millar [Academic Foundation Doctor; NHS Grampian]
Dr David Booth: General Practitioner & Doctors Patients and Communities Facilitator; University of
Dundee
Prof Jeremy Hughes: Consultant Nephrologist, NHS Lothian; Reader in Nephrology, University of
Edinburgh
Dr Hannah Lord: Consultant Oncologist; Ninewells Hospital & Medical School
Lloyd Hughes: Year 5 Medical Student, University of Dundee Medical School; Editor-In-Chief 2011-2013
John Jungpa Park: Editor-In-Chief of Res Medica 2012/2013; Medical Student, University of Edinburgh
Dhairya Lakhani: Vice President, Medical Students’ Association of India; Year 3 MBBS, Sumandeep
Vidyapeeth University

[Editorial] PP. 4-5
K. Barr (Guest Editor for this Issue)
A Career Involving Clinical Research – Potential Tracks to Success PP. 6-9
J. Iredale
Critical Appraisal of a Research Paper PP. 10-17
A. MacInnes & T. Lamont
Acute Stroke – Diagnosis and Management PP. 18-27
G. Smith
Stroke Rehabilitation PP. 28-36
G. Smith
What is the Scope of Autonomy in Medical Practice? PP. 37-42
S. Falahati
Public Health Challenges in India PP. 43-46
D. Lakhani, S. Kumar, S. Gohel, S. Kumar
Electroencephalography – An Overview PP. 47-53
H. Duncan, K. Spillane, I. Morrison
Frailty: What does it mean for Clinical Care Provision? PP. 54-64
C. Reynaud, T. McHugh, R. Romero-Ortuno

The Autonomous Practitioner (Editorial)
Kevin Barr (Year 3 Mental Health Nursing Student, University of Dundee)
Deputy Editor – Scottish Universities Medical Journal
Guest Editor for this Issue
As Acting Editor for this issue, I would like to take this opportunity to welcome you to the first
issue in the third volume of the Scottish Universities Medical Journal (SUMJ). It is with great
pleasure and pride that we present to you a wealth of literature detailing modern concerns
within the medical arena, and we have articles in this issue which should cater for our entire
readership.
The issue of autonomy in contemporary health care has produced great discussion in recent
years1, but what happens when management and clinical policy limits the autonomy of health
care professionals? Falahati2 addresses this in the article ‘What is the Scope of Autonomy in
Medical Practice’2, whereby the weight of autonomy is pitted alongside other ethical principles.
It is true that if we are to be autonomous practitioners we must make effective decisions, but
how do the decisions we make affect our ability to practise ethically? Falahati examines this
argument in detail, thus presenting an effective and successful article.
In this issue we present two articles by Dr Gemma Smith, who examines the ways in which
available tools can help in the assessment and management of those suffering from a
suspected stroke. Smith does this by inspecting the mortality and morbidity rates associated
with stroke3, therefore looking at ways to treat the condition, such as anti-coagulant therapy
and blood pressure control. In her article ‘Secondary Prevention and Rehabilitation after a
Stroke’4, Smith goes further by looking at the risks of recurring strokes, making suggestions on
possible interventions which can be made for stroke management. Indeed, Smith asserts that
the rehabilitation process should involve input from the multi-disciplinary team, leading to the
question of whether or not multi-disciplinary working limits autonomy and independent
practice in contemporary health care.
This issue of the SUMJ also includes an article by Professor John Iredale which looks at the
potential tracks to success in a career involving clinical research5. Iredale offers tips to medical
students who intend to pursue a career as a clinical academic by examining the ways in which
students can access such courses. He finishes by stating that PhD funding has never been
better; indeed, the Wellcome Trust has almost doubled the number of PhD opportunities
available for UK medical graduates5. Therefore, if you are interested in developing a career in
clinical academia, Professor Iredale’s article is both informative and inspiring.

In this issue of the SUMJ we are once again delighted to publish articles from a wide range of
disciplines, spanning myriad levels of experience and knowledge. The SUMJ continues to pride
itself on publishing the work of Doctors, Consultants, Clinical Lecturers, Medical Students,
Nursing Students and all other health professionals, and it is the time and effort of these
individuals which ensures the journal goes from strength to strength.
We would like to thank all of the contributors who continue to submit articles, and to once
again clarify that all submitted articles are taken into consideration by the committee.
I would like to finish by thanking all of my fellow committee members for their support and
assistance throughout my time as Deputy Editor of the SUMJ. Throughout the year I have been
given opportunities to expand my knowledge and improve my practice, and working for the
journal has provided me with great pleasure and satisfaction. As this is the last issue under my
editorship, I would like to thank the committee and our readership. Most importantly, I would
like to wish good luck to the future SUMJ committee, and I hope that the journal continues to
improve under the new committee which will be elected in the near future.
Thank you.
References
1. SAKHANI, D., and COULTER, I. (2009). ‘The Politics of Inter-Professional Working and the
Struggle for Autonomy in Nursing’. Social Science and Medicine, 68, PP. 1221-1228.
2. FALAHATI, S. (2014). ‘What is the Scope of Autonomy in Medical Practice?’ Scottish
Universities Medical Journal, 3(1).
3. SMITH, G. (2014). ‘Acute Stroke – Diagnosis and Management’. Scottish Universities
Medical Journal, 3(1).
4. SMITH, G. (2014). ‘Secondary Prevention and Rehabilitation after a Stroke’. Scottish
Universities Medical Journal, 3(1).
5. IREDALE, J. (2014). ‘A Career Involving Clinical Research – Potential Tracks to Success’.
Scottish Universities Medical Journal, 3(1).

A Career Involving Clinical Research – Potential Tracks to Success
Professor John Iredale DM, FRCP, FMedSci, FRSE (Professor of Medicine; Dean of Clinical
Medicine Director of MRC/UoE Centre for Inflammation Research)
Correspondence – John Iredale: [email protected]
In whatever branch of medicine we work as clinicians, research rightly underpins and informs
what we say, do and deliver in our practice. It is therefore axiomatic that all doctors need to be
research aware and UK Medical Schools have an extraordinarily strong tradition of introducing
research opportunities and projects to medical students. Indeed, Medical Schools can be seen
as a major engine of medical research in the UK, research which is acknowledged to be at the
forefront internationally. These opportunities vary from vacation projects to intercalated BScs
embedded within the medical curriculum. But importantly, medical progress and innovation
additionally depend on the UK generating and maintaining a cohort of doctors who as juniors
and seniors spend a significant part of their working week engaged in research – medical
academics. Their research may be orientated to deliver improvements in care, novel treatments
or enhanced understanding of disease pathogenesis. For my money, this job – that of the
medical academic or clinician scientist - offers the most exciting, challenging and stimulating of
careers and establishes a lifetime flush with opportunities, intellectual challenge and
achievement.
On a UK basis, the last 20 years have been characterised by a renaissance in basic, clinical and
translational research. Driven by the rapid developments of key technologies in, for example
the field of genetics, this renaissance has also been the result of concerted efforts by Medical
Schools, research funders including the Medical Research Council and the Wellcome Trust, the
NHS, the NIHR and Chief Scientists Office, NHS Education Scotland (NES) and the Academy of
Medical Sciences, to establish robust career pathways for doctors interested in becoming
clinician scientists. In turn, this career focus has driven the development of structured
programmes orientated to support junior doctors interested in research and developing their
careers as clinician scientists to achieve their goals and develop their research pedigree
alongside their clinical competences, leadership skills and other aspects of their professional
development. This model career pathway in England and Wales links academic FY programs
with academic clinical fellowships (or ACFs) from which candidates can emerge into specialist
training and/or PhD research before going on to become clinical lecturers and position
themselves for more senior research funding. This structure resulted from two National
reports; The Savill report commissioned by the Academy of Medical Sciences in 2000 and the so
called “Walport Report” delivered in March 2005.
The Universities and NHS in Scotland responded in a slightly different way to the Savill and
Walport reports, establishing a parallel but distinct career structure. In Scotland academic
training falls under the umbrella of SCREDS (The Scottish Clinical Research Excellence
Development Scheme) which is steered and diverted by representation from NES and the
Scottish Universities. Under the aegis of SCREDS, each Scottish medial school has established an
academic career track (with relatively subtle variations from one school to another) which
provides a fertile environment for clinical academic careers. Most importantly each of these
schemes provides support and mentorship – vital for sustaining career enthusiasm and
direction whilst juggling the twin challenges of clinical and academic training. Termed clinical
academic tracks or CATs, these programmes link academic FY ( and non-academic FY) schemes
with core and specialist training (ST) opportunities and support to obtain funding for PhD
studies at the ST stage in addition to providing postdoctoral SCREDS/NES funded clinical
lectureships. More detailed information on each of these schemes is available on the individual
websites of the Scottish Universities listed below.
How then does a medical student interested in developing a career as a clinical academic
negotiate their way through the clinical academic training schemes to success? The first major
milestone in such a career is to establish ones credentials as motivated and interested in
research. This might take the form of undertaking an Intercalated BSc; or for those who can’t
make such a commitment, contributing to research projects as an undergraduate and the early
phases of clinical training is invaluable as a means of gaining experience and building the
academic component of one’s CV.
Each of the Scottish Universities, collaboratively with their local Health Board and NES, now
offer an academic FY scheme. These vary in their configuration but provide the trainee with the
opportunity to undertake some research and, in some cases, formal research training in specific
methodologies such as statistics. The rich eco system of differently composed academic FY
programmes offers a range of research experience for medical graduates. However, not all
candidates may be able to access such positions or there may those who (like the author) were
“late developers” and realised that they have an interest in research after this stage, perhaps in
core training or specialist training.
It is important to recognise that not getting a place on an academic FY scheme does not close
the door to an academic career. Indeed, some of the most impressive individuals that I’ve
interviewed for national schemes have come from non-academic FY and ST positions. But a
characteristic feature of these individuals is long standing engagement and delivery of research
even while undertaking busy clinical training jobs (see my comments above). The secret to
success at both the FY and ST stages, whether in an academic or non-academic position, is good
mentorship. Seek the support of a successful academic in your institution who understands the
system and can offer you advice as you make critical choices. Such an individual is also well
equipped to steer you to research opportunities and other researchers that may support and
assist you as you develop your career.
Just as with academic FY positions, in creating Clinical Academic Tracks at the core and
specialist training stages, the differences in approaches between the individual Scottish
Universities and Medical Schools have created a landscape rich and varied with respect to
opportunities; opportunities that will suit the range of aspirations and requirements that
individual trainee clinician scientists require. In broad terms, each University teaching hospital
has core training and opportunities linked with academic clinical groups and specialties. My
personal view is that the aspiring academic should place emphasis on gaining a specialist
training (ST) position. Because it is generally during ST training that individuals are best placed
to take the next major step in an academic career; that of taking an out of programme
experience to undertake a PhD. The PhD is the essential building block of an academic career
and one which should remain the focus of the aspiring academic clinician scientist. Additionally,
all Universities have been allocated SCREDS/NES funded clinical lectureships which allow those
who have completed a PhD to complete their higher specialist training combining academic
endeavour with their further clinical training and thereby ensuring that clinical competences
are complimented by the development of a strong academic pedigree that will position the
doctor to apply for future research grants and if appropriate further fellowships.
It is impossible in a brief summary such as this to describe in detail the various schemes and
opportunities. It is suggested the reader uses the web based material listed below. But
examples of the variation in approach developing clinical academic tracks include the focus in
Glasgow on a series of core training positions that have been grouped to provide research
opportunities, mentorship and support under the GATE scheme. Edinburgh has a portfolio of
Wellcome Trust funded PhDs that are advertised and deployed to provide doctoral
opportunities for successful trainees. In Edinburgh these have been linked with clinical
lectureships to provide a form of “run-through” academic training (ECAT lectureships) so that
the successful doctoral student exits to a lectureship and can complete training in their
competencies together with accruing critical academic experience to reach the next stage in
their career.
Whilst working towards and achieving funding for a PhD may seem somewhat distant and
daunting at this stage, it is an eminently achievable goal for the keen, motivated and tenacious.
There has never been a better time to apply. Key funders have significantly enhanced PhD
funding in the last 10 years. For example, through their portfolio and national schemes, the
Wellcome Trust has doubled the number of PhD opportunities available for UK medical
graduates. Additionally investment by the Medical Research Council and other major charities

including Cancer Research UK has enhanced the available PhD opportunities for medial
graduates.
So what are the take home messages from this, necessarily, brief synopsis of academic tracks in
Scotland? For the medical students and young junior doctors interested in an academic career,
the key issues are to demonstrate a commitment to research and academic endeavour; become
involved in research projects and relish the chance that a busy clinical job provides not only for
clinical experience but to provide research questions and opportunities. Retain a focus on your
ambition and career and understand that the key building block over the 5 to 7 years after you
qualify will be obtaining funding for and delivering a PhD. Don’t be daunted by the idea of
working towards and obtaining funding for a PhD; there has never been a better time to do so
in terms of the funding opportunities or, arguably a more exciting time to become involved in
research, given the wealth of technologies that can now be applied to clinical questions.
Finally and most importantly seek and exploit mentorship. The value of high quality mentorship
at all stages of a clinical career, but particularly as you emerge from medical school into the
professional clinical arena, cannot be underestimated.
Websites for Scottish Academic Career Track Programmes
Aberdeen - http://www.abdn.ac.uk/acat
Dundee - http://medicine.dundee.ac.uk/dcat
Edinburgh - http://www.ecat.ed.ac.uk
Glasgow - http://www.gla.ac.uk/colleges/mvls/graduateschool/academicandclinicaltraining/

Critical Appraisal of a Research Paper
Andrew MacInnes, BDS (Hons.) MFDS, RCPS (Glasgow), Senior House Officer1
Thomas Lamont, BDS, MFDS, RCPS (Glasgow), Clinical Research Fellow/Honorary Restorative StR2
1Dundee Dental Hospital
2University of Dundee
Correspondence - Andrew MacInnes: [email protected]
ABSTRACT
Whether studying for your professional examinations or planning the care of your patients, critical
appraisal is a vital skill for healthcare professionals. Evidence based healthcare involves the integration
of the best available evidence, clinical experience and patient preference when making decisions related
to patient care. Research papers provide information on current practice and new developments in the
diagnosis, prevention and treatment of disease. It is a fundamental skill to be able to identify and
appraise the best available evidence in order to integrate it with your own clinical experience and
patients values. In this article we hope to provide you with a robust and simple process for assessing the
trustworthiness of articles and assessing their value to your clinical practice.
Key Words: Evidence-Based Medicine, Critical Appraisal and Research Design
Introduction
Whether studying for your professional examinations or planning the care of your patients, critical
appraisal is a vital skill for healthcare professionals. Evidence based healthcare involves the integration
of the best available evidence, clinical experience and patient preference when making decisions related
to patient care. Research papers provide information on current practice and new developments in the
diagnosis, prevention and treatment of disease. It is a fundamental skill to be able to identify and
appraise the best available evidence in order to integrate it with your own clinical experience and
patients values. During the final years of Dental school and early years as a graduate part of our roles
has been to discuss with patients their diagnoses and treatment options in an evidence-based manner.
This requires up to date and accurate knowledge of the available evidence. Critical Appraisal is a method
of carefully and systematically examining articles to assess their value and their place in the literature. In
this article we hope to provide you with a robust and simple process for assessing the trustworthiness of
articles and assessing their value to your clinical practice.
Background
Once an article is identified, critical appraisal involves a structured approach to examining evidence to

assess its value and clinical relevance to modern practice. This allows practitioners to recognise studies
which are biased or poorly designed and therefore ensure only the most reliable information is
incorporated into clinical practice. As the medical profession evolves, undergraduate and junior
practitioners are increasingly expected to be aware of current develo
outlines the three important components in providing evidence based healthcare.
Figure 1 – Providing evidenced based healthcare
An important part of the process is an understanding of the
Figure 2, below, highlights the differing study designs and their relative robustness and reliability.
Evidence from meta-analysis of randomised control trials, such as systematic reviews carried out by the
Cochrane Collaboration, are considered to be the gold standard in evidence. These involve the
aggregation of the highest quality studies available with careful appraisal and statistical analysis of the
findings. These, in turn, may form the basis for evidence b
aid the translation of best available evidence into clinical practice
and the prerequisite body of evidence needed, in many areas of healthcare these are not available and
alternate study designs are utilised.
Clinical Expericance
assess its value and clinical relevance to modern practice. This allows practitioners to recognise studies
are biased or poorly designed and therefore ensure only the most reliable information is
incorporated into clinical practice. As the medical profession evolves, undergraduate and junior
practitioners are increasingly expected to be aware of current developments in patient care.
outlines the three important components in providing evidence based healthcare.
Providing evidenced based healthcare – three important components
An important part of the process is an understanding of the differing levels of the evidence hierarchy.
Figure 2, below, highlights the differing study designs and their relative robustness and reliability.
analysis of randomised control trials, such as systematic reviews carried out by the
ane Collaboration, are considered to be the gold standard in evidence. These involve the
aggregation of the highest quality studies available with careful appraisal and statistical analysis of the
findings. These, in turn, may form the basis for evidence based clinical practice guidelines that serve to
aid the translation of best available evidence into clinical practice2. Due to the nature of these studies
and the prerequisite body of evidence needed, in many areas of healthcare these are not available and
alternate study designs are utilised.
Evidence Based
Healthcare
Best Available Evidence
Patient Preference
assess its value and clinical relevance to modern practice. This allows practitioners to recognise studies
are biased or poorly designed and therefore ensure only the most reliable information is
incorporated into clinical practice. As the medical profession evolves, undergraduate and junior
pments in patient care. Figure 1
differing levels of the evidence hierarchy.
Figure 2, below, highlights the differing study designs and their relative robustness and reliability.
analysis of randomised control trials, such as systematic reviews carried out by the
ane Collaboration, are considered to be the gold standard in evidence. These involve the
aggregation of the highest quality studies available with careful appraisal and statistical analysis of the
ased clinical practice guidelines that serve to
. Due to the nature of these studies
and the prerequisite body of evidence needed, in many areas of healthcare these are not available and
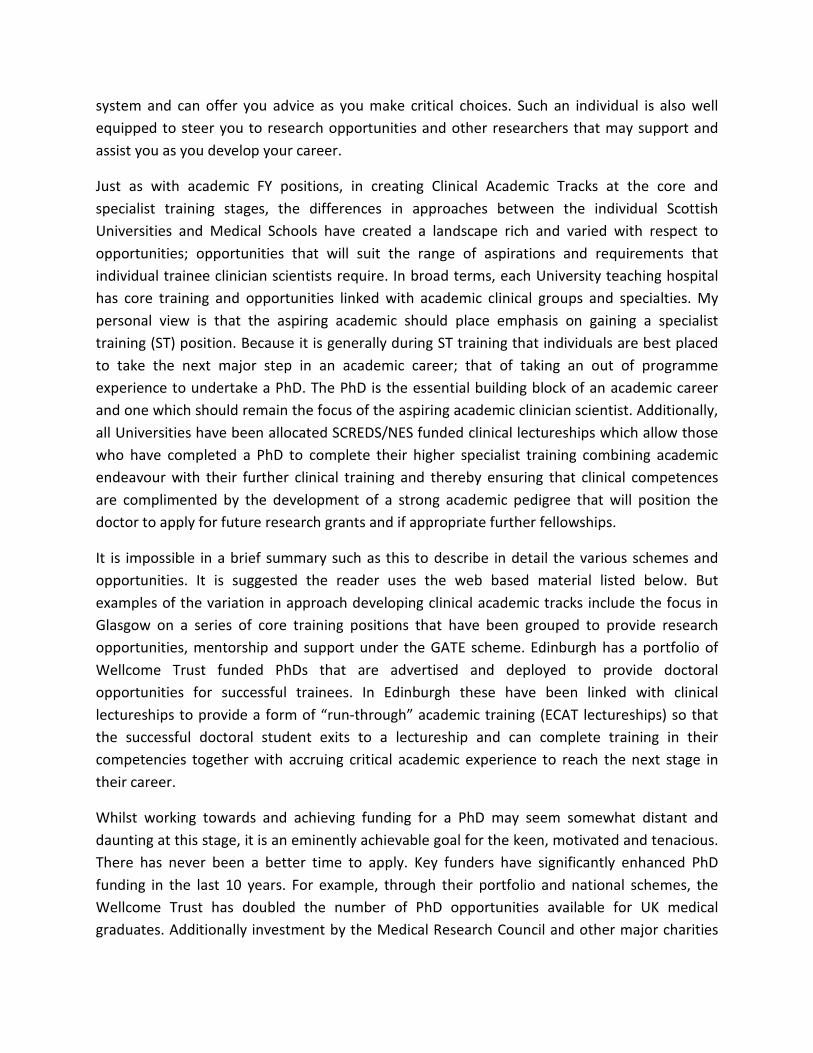
Although assessment of the level of evidence is a significant aspect of critical appraisal, it is essential to
note that studies utilising designs recognised as one of the lower level
value to the profession and increase the body of evidence available, e.g. case, correlation or
comparative studies may be a precursor to assess a hypothesis before a randomised control trial can be
designed. Therefore, different critical appraisal tools may be utilised to assess the varying study designs
available. Additionally, some study questions may preclude themselves to a particular study design
a double blind, randomised control trial of parachutes may not be app
the most appropriate study design to answer the different type of questions being asked.
Figure 3 –
Ia•Evidence from meta
Ib•Evidence from at least one RCT
IIa
•Evidence from at least one well designed, controlled trial which is not randomised
IIb•Evidence from at least one well designed experimental trial
III•Evidence from case, correlation and comparitive studies
IV•Evidence from a panel of experts
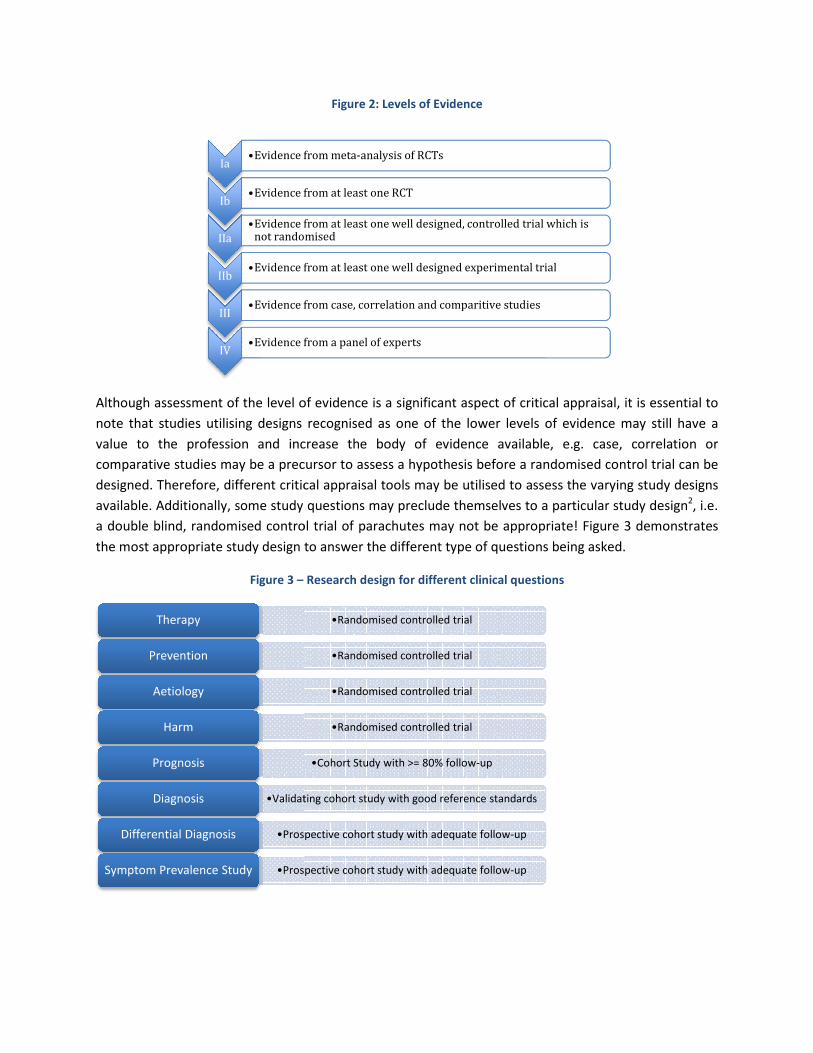
Therapy
Prevention
Aetiology
Harm
Prognosis
•Validating cohort study with good reference standardsDiagnosis
•Prospective cohort study with adequate followDifferential Diagnosis
•Prospective cohort study with adequate followSymptom Prevalence Study
Figure 2: Levels of Evidence
Although assessment of the level of evidence is a significant aspect of critical appraisal, it is essential to
note that studies utilising designs recognised as one of the lower levels of evidence may still have a
value to the profession and increase the body of evidence available, e.g. case, correlation or
comparative studies may be a precursor to assess a hypothesis before a randomised control trial can be
ent critical appraisal tools may be utilised to assess the varying study designs
available. Additionally, some study questions may preclude themselves to a particular study design
a double blind, randomised control trial of parachutes may not be appropriate! Figure 3 demonstrates
the most appropriate study design to answer the different type of questions being asked.
Research design for different clinical questions
Evidence from meta-analysis of RCTs
Evidence from at least one RCT
Evidence from at least one well designed, controlled trial which is not randomised
Evidence from at least one well designed experimental trial
Evidence from case, correlation and comparitive studies
Evidence from a panel of experts
•Randomised controlled trial
•Randomised controlled trial
•Randomised controlled trial
•Randomised controlled trial
•Cohort Study with >= 80% follow-up
Validating cohort study with good reference standards
Prospective cohort study with adequate follow-up
Prospective cohort study with adequate follow-up
Although assessment of the level of evidence is a significant aspect of critical appraisal, it is essential to
s of evidence may still have a
value to the profession and increase the body of evidence available, e.g. case, correlation or
comparative studies may be a precursor to assess a hypothesis before a randomised control trial can be
ent critical appraisal tools may be utilised to assess the varying study designs
available. Additionally, some study questions may preclude themselves to a particular study design2, i.e.
ropriate! Figure 3 demonstrates
the most appropriate study design to answer the different type of questions being asked.

Carrying out Critical Appraisal
Critical appraisal may be carried out utilising various assessment tools. These involve the evaluation of
different aspects of the paper and, in turn, highlight important characteristics of the paper and study
design used. A useful resource to aid the assessment of the multiple study designs employed is the
critical skills assessment programme (CASP)
Critical Skills Appraisal Programme (CASP)
Founded in 1993 the CASP program is a non-profit entity that provides resources, learning and
development opportunities to support critical appraisal skills development in the UK1. It provides critical
appraisal checklists for different types of study designs to enable comprehensive and robust protocols
for critically appraising a research paper. This section breaks critical appraisal down to assess 7 main
points of a research paper. Similar to the CASP methodology we will assess the important features of
any research paper and highlight key points that should be evaluated.
Initial Assessment
The initial assessment of a research paper involves a generalised look at the details of the article and the
publication it is appearing in. It may be of value to look at the year the article was published in and
ascertain if new evidence has been added to the literature since this publication. Conversely, it is also
important to note that seminal papers may have been published a significant time ago and, although the
studies are old, these may still be of significance to modern practice.
The presence of a peer review process in journal acceptance protocols also adds robustness to the
assessment criteria for research papers and hence would indicate a reduced likelihood of publication of
poor quality research. Other areas to consider may include authors declarations of interest and potential
market bias.
Problem
Appraisal of the paper hypothesis and problem addressed by the study is a crucial facet of critical
appraisal. For a study to have value it must address a significant or relevant problem within healthcare
and usually provide new or meaningful results. A useful structure for assessing the problem addressed in
the article is the Problem Intervention Comparison Outcome (PICO) method. This involves identifying if
the research has a focused question (problem), appropriate and clearly stated management strategy
(intervention), a suitable control or alternative (comparison) and that the desired results or patient
related consequences have been identified (outcomes). The current literature should have been
reviewed and commonly will support the hypothesis, which should be clearly stated.
Methodology
The study design of the research is fundamental to the usefulness of the study. Several types of study
design, noted in Figure 4, are available and each has their advantages and disadvantages. Suboptimal
study design can incorporate bias into the study and subsequently skew results.

Assessment of the data collection tool and its relevance to the problem is important, i.e. if the problem
involved assessment or measurement of a disease is the method of doing this appropr
sensitive. The data collection of a study should be objective and the results reproducible. Additionally, it
is important to consider if the amount of time allocated for data collection was appropriate and
relatable to the clinical course of the disease or intervention being studied.
Figure 4. Different Study Designs
Participants/Sample Population
Analysis of the sample population utilised in the research will give an indication as to the relevance of
the study results to individual clinical practice. To minimise any bias within a study the sample
population should be representative of the populatio
should be allocated randomly within the study. It is also imperative to consider the sample size in the
study and identify if the study is adequately powered to produce statistically significant results
values quoted are <0.05.
Data Analysis and Results
The results of the study should be presented in a suitable manner with the main result, whether it
supports or opposes the paper hypothesis, clearly demonstrated. The use of charts and graphs sho
highlight the data collected and facilitate analysis of the outcomes.
Correct statistical analysis of results is crucial to the reliability of the conclusions drawn from the
research paper. Depending on the study design and sample selection method emp
or inferential statistical analysis may be carried out on the results of the study. It is important to identify
if this is appropriate for the study.
Conclusion of Paper
Analysis of the conclusions drawn from the study involves assess
the results and an overall general assessment of study outcome. When critically appraising the
Study Designs
Descriptive
- Cross sectional
- Case report
- Case series
- Survey
Assessment of the data collection tool and its relevance to the problem is important, i.e. if the problem
involved assessment or measurement of a disease is the method of doing this appropr
sensitive. The data collection of a study should be objective and the results reproducible. Additionally, it
is important to consider if the amount of time allocated for data collection was appropriate and
se of the disease or intervention being studied.
Analysis of the sample population utilised in the research will give an indication as to the relevance of
the study results to individual clinical practice. To minimise any bias within a study the sample
population should be representative of the population being studied as a whole and, ideally, participants
should be allocated randomly within the study. It is also imperative to consider the sample size in the
study and identify if the study is adequately powered to produce statistically significant results
The results of the study should be presented in a suitable manner with the main result, whether it
supports or opposes the paper hypothesis, clearly demonstrated. The use of charts and graphs sho
highlight the data collected and facilitate analysis of the outcomes.
Correct statistical analysis of results is crucial to the reliability of the conclusions drawn from the
research paper. Depending on the study design and sample selection method employed, observational
or inferential statistical analysis may be carried out on the results of the study. It is important to identify
Analysis of the conclusions drawn from the study involves assessment of the author’s interpretation of
the results and an overall general assessment of study outcome. When critically appraising the
Study Designs
Analytical
Observational
- Case Control
- Cohort Studies
Experimental
- Randomised control trial
Assessment of the data collection tool and its relevance to the problem is important, i.e. if the problem
involved assessment or measurement of a disease is the method of doing this appropriately specific and
sensitive. The data collection of a study should be objective and the results reproducible. Additionally, it
is important to consider if the amount of time allocated for data collection was appropriate and
Analysis of the sample population utilised in the research will give an indication as to the relevance of
the study results to individual clinical practice. To minimise any bias within a study the sample
n being studied as a whole and, ideally, participants
should be allocated randomly within the study. It is also imperative to consider the sample size in the
study and identify if the study is adequately powered to produce statistically significant results, i.e. p
The results of the study should be presented in a suitable manner with the main result, whether it
supports or opposes the paper hypothesis, clearly demonstrated. The use of charts and graphs should
Correct statistical analysis of results is crucial to the reliability of the conclusions drawn from the
loyed, observational
or inferential statistical analysis may be carried out on the results of the study. It is important to identify
ment of the author’s interpretation of
the results and an overall general assessment of study outcome. When critically appraising the

conclusions of a study it is vital to consider if the results are precise enough to infer a conclusion and
also whether the data was shown to be statistically significant, i.e. p value <0.05.
Appraisal of the conclusions should also ensure recommendations stated were appropriate for the
results achieved and also within the scope of the study. The authors should also address shortcomings in
the study and discuss how this may have affected the results and recommendations proposed.
Overall Assessment
After careful analysis of the different aspects of the research paper the final stage of critically appraising
a research paper is assessing the relevance of its findings to the profession. The reported outcomes of
the diagnostic, preventative or treatment intervention should be assessed focusing on the balance of
potential benefits and drawbacks when compared to accepted alternatives.
Summary
In conclusion, critical appraisal is a fundamental skill in modern practice for assessing the value of
research papers and providing an indication of their relevance to the profession. As the medical
profession evolves and studies providing information on the diagnosis, prevention and treatment of
diseases are published it is crucial to be able to discern the best available evidence. Practitioners are
then able to, through systematic reviews or guidelines, synthesise the available evidence in order to
identify if a change in practice is indicated. Critical appraisal is a skills-set developed throughout a
professional career that facilitates this and, through integration with clinical experience and patient
preference, permits the practice of evidence based medicine and dentistry.
References
1Critical Appraisal Skills Programme, About CASP, http://www.casp-uk.net/about-casp/
2Richards, D., et al. (2008). Evidence-Based Dentistry: Managing Information for Better Practice, Quintessence
Publishing Company, Incorporated.
3Centre For Evidence Based Dentistry, http://www.cebd.org/
4David L Sackett, William M C Rosenberg, J A Muir Gray, R Brian Haynes, and W Scott Richardson. Evidence based
medicine: what it is and what it isn’t. BMJ 1996; 312: 71-72
5Richards, D. and Lawrence, A. Evidence-based dentistry (personal view). British Dental Journal 1995 Oct 7; 179(7):
270-3. (PDF)

Acute Stroke – Diagnosis and Management
Dr Gemma Smith (Specialty Trainee in Elderly Care and Stroke Medicine)
Correspondence - Gemma Smith: [email protected]
ABSTRACT
Stroke (noun): a sudden disabling attack… caused by an interruption in the flow of blood to the brain,
especially through thrombosis.
Stroke is a considerable cause of mortality and morbidity in the UK. The field of stroke medicine has
changed considerably in recent years with the development of hyper-acute treatments such as
thrombolysis, specialist stroke units and a better understanding of secondary prevention. Mortality
rates may have decreased but diagnostics have become more sensitive and it is not clear whether
incidence of stroke is falling overall. It is predominantly a problem of advancing age and many of those
suffering a stroke will be from the older age bracket. This often raises interesting challenges in the
diagnosis and management process due to the complex needs of the patient in the bed.
This article will review the tools available to assist in the systematic assessment and treatment of people
with a suspected stroke.
Key Words: stroke; imaging; thrombolysis
Background
Stroke is a considerable cause of mortality and morbidity in the UK. The field of stroke medicine has
changed considerably in recent years with the development of hyper-acute treatments such as
thrombolysis, specialist stroke units and a better understanding of secondary prevention. Mortality
rates may have decreased2
but diagnostics have become more sensitive and it is not clear whether
incidence of stroke is falling overall3,4
. It is predominantly a problem of advancing age and many of those
suffering a stroke will be from the older age bracket. This often raises interesting challenges in the
diagnosis and management process due to the complex needs of the patient in the bed.
This article will review the tools available to assist in the systematic assessment and treatment of people
with a suspected stroke. The change in stroke services has meant that acute events are now often
admitted directly to acute stroke units as these are proven to provide optimal care in the acute and sub-
acute phases5. In some cases this means that they are omitted from the experience of the acute general
medical take. They remain however, an important general medical emergency.
Recognition and Diagnosis

Rapid diagnosis of a stroke is the first step to instigating appropriate treatment. In the case of
thrombolysis, where potent fibrinolytic drugs are given to restore cerebral blood supply, the faster a
stroke is recognised and treated, the better the outcome6. Strokes are not “black and white” clinical
entities however and many “mimics” have similar symptoms that can lead to diagnostic uncertainties.
The symptoms of a stroke are due to the acute interruption of the blood supply to an area of the brain.
This can be through blockage of a blood vessel (infarcts) or haemorrhage. Infarcts can be caused by
emboli, usually from thrombus in the carotid arteries or left atrium, or from in-situ clot formation. In
both haemorrhagic strokes and infarcts the onset is sudden. The vascular territory involved and the
presence of associated symptoms may assist in the diagnosis.
• Anterior circulation – weakness, sensory deficits, dysphasia (expressive and receptive), visual
field defects, dyspraxia and higher cortical dysfunction, contralateral signs.
• Posterior circulation – visual field defects, ataxia and vertigo, inco-ordination, cranial nerve
deficits, ipsilateral signs.
To allow rapid identification of these stroke patterns and to assist in the exclusion of other possible
diagnoses, the following screening tools have been developed.
F.A.S.T.
This stands for Face, Arm, Speech, Time and has been the subject of a national television awareness
campaign. It is used by paramedics and emergency department triage staff to screen for stroke
symptoms and can be up to 81% sensitive7. It prompts assessment for facial asymmetry, arm weakness,
slurred or disordered speech and then rapid transfer to the appropriate acute care setting for further
assessment. FAST is not infallible and is particularly prone to missing posterior circulation events.
R.O.S.I.E.R8.
This tool is for Recognition of Stroke in the Emergency Room. It was developed to help emergency
department staff assess possible stroke patients and provides some tools for screening out mimics such
as hypoglycaemia, seizures and syncope. It has a sensitivity of 93% and specificity of 83%8. See Table 1.
Table 1 – ROSIER score
Is the blood glucose above 3.5mmol? If not, treat and re-assess.
1. Has there been loss of consciousness or syncope? Yes (-1) No (0)
2. Has there been seizure activity? Yes (-1) No (0)
3. Is there NEW ACUTE onset (or on awakening from sleep) of:
• Asymmetrical face weakness Yes (+1) No (0)
• Asymmetrical arm weakness Yes (+1) No (0)
• Asymmetrical leg weakness Yes (+1) No (0)
• Speech disturbance Yes (+1) No (0)
• Visual field defect Yes (+1) No (0)
Score >0 suggests a stroke diagnosis.

Paramedic teams trained in the use of FAST screening will often refer patients directly to acute stroke
units. Use of the ROSIER scale in emergency departments and medical admissions units allows self-
presenting patients or those admitted via GPs to be assessed rapidly so that appropriate admission
pathways and investigations can be instigated promptly.
Following assessment with screening tools, patients with suspected strokes should have a thorough
history taken and a comprehensive neurological examination. This may need to be simultaneous with
the ordering of investigations such as CT imaging if the patient may be a candidate for thrombolysis as
will be discussed later.
History and Examination
Timing is a crucial point when taking a patient’s history of a suspected stroke. The onset of symptoms is
usually sudden, with all deficits occurring together, as opposed to a “marching” or progressive deficit.
The time of onset is vital, especially when considering patients for thrombolysis that must be initiated
within 4.5 hours of symptom onset9. It is necessary to clearly determine when the patient was last well.
Often patients wake up with symptoms however they may have got up in the night or spoken to their
partner in the early hours of the morning and the time they were last well can still be identified.
It is useful when reviewing neurological symptoms to consider them as positive or negative. Positive
symptoms involve gaining a quality such as extra movements or shaking, added sensations such as
prickling or burning and extra visual signs such as flashing lights. Negative symptoms describe the loss of
a normal function such a weakness, loss of sensation, loss of comprehensible and useful speech, loss of
vision (full or partial) or incoordination. Strokes generally produce negative symptoms. The presence of
positive symptoms can sway the assessing physician towards a diagnosis of a mimic. The negative
symptom of loss consciousness is rarely a feature of stroke (Table 2).
Table 2- Positive and negative features on examination and stroke mimics
Positive symptom Stroke Mimic
Flashing lights and colours in vision. Migraine
Shaking or jerking limbs. Seizures (focal or generalized).
Tingling / prickling sensation. Radiculopathy, herpes zoster infection.
Negative symptom Stroke Mimic
Loss of consciousness Syncope, seizures.
Associated symptoms mainly have a role in identifying mimics or increasing the suspicion of an intra-
cerebral haemorrhage. Haemorrhagic strokes may present with headache, nausea and vomiting, which
are otherwise uncommon in strokes but may also be present in migraine. Confusion and agitation can
occur with intra-cranial haemorrhages or non-stroke diagnoses such as infection or hypoglycaemia. A
medication history is also important, particularly if patients are taking antiplatelet or anticoagulant
therapy.

When considering the diagnosis of a stroke it is useful to look at the vascular risk factors of the patient.
This provides a guide to the probability of a stroke but also as a target for future secondary prevention.
Hypertension, diabetes, smoking, hyperlipidaemia, family history, male gender, age and other
vasculopathies are potent indicators of stroke risk however strokes are still possible in those without
these factors.
Each patient with a suspected stroke should have a thorough neurological examination including
assessment of motor and sensory modalities and cerebellar function. Pronator drift is an excellent sign
of subtle motor weakness. Higher cortical function such as speech and praxis should be assessed.
Speech quality, fluency and word finding skills can be assessed throughout taking the history. Providing
simultaneous stimuli to bilateral visual fields or sensory pathways can identify inattention. The inability
to identify when both sides are stimulated suggests cortical dysfunction. Cranial nerve examinations
should differentiate between upper and lower motor neuron facial weakness and should include an
assessment of visual fields. Neurological examination findings can be applied to the National Institute
for Health Stroke Scale (NIHSS) to give a way of communicating and monitoring stroke severity. The
application of this scale in a reproducible way requires training. The examination findings will also allow
the stroke to be classified as per the Bamford Classification10
. This gives some guide of mortality and
morbidity with a total anterior circulation stroke carrying a higher chance of both.
Total anterior circulation stroke (TACS) – All three of the following: 1.Unilateral weakness (and/or
sensory deficit) of face, arm and leg 2. Homonymous hemianopia 3. Higher cerebral dysfunction
(dysphasia, visuospatial disorder).
Partial anterior circulation stroke (PACS) – Two of the following: 1.Unilateral weakness (and/or sensory
deficit) of face, arm and leg 2. Homonymous hemianopia 3. Higher cerebral dysfunction (dysphasia,
visuospatial disorder).
Lacunar stroke (LACS) – One of the following: 1. Unilateral weakness (and/or sensory deficit) of face and
arm, arm and leg or all three. 2. Pure sensory stroke. 3.Ataxic hemiparesis.
Posterior circulation stroke (PoCS) – One of the following: 1. Cerebellar or brainstem syndromes 2. Loss
of consciousness3. Isolated homonymous hemianopia
Please note that both TACS and PACS involve the anterior and middle cerebral arteries (ACA and MCA),
whilst the PoCS involves the posterior circulation.
Transient Ischaemic Attack
TIAs can present with symptoms in either of the vascular territories described above but resolve entirely
within 24 hours and usually in less than one hour. Amaurosis fugax, described as a curtain coming over

the vision in one eye and resolving rapidly is also a form of TIA. TIAs can generally be managed as an
outpatient and therefore should rarely be seen on medical admission units having been assessed and
referred from GPs or emergency departments.
Following a TIA, the risk of progression to a full stroke within the next 7 days can be predicted by the use
of the ABCD2 score (Table 3).
Once diagnosed with a TIA, with particular emphasis that all symptoms should have resolved entirely,
patients can be commenced on an antiplatelet agent. An ABCD2 score of 4 or less can be referred for
assessment in a TIA clinic. The aim of this service is to identify modifiable risk factors, in particular
carotid stenosis that may be amenable to surgical intervention, and atrial fibrillation for which oral
anticoagulants may be appropriate. TIA clinics are often run five or even seven days a week to allow
rapid access. A score greater than 4 carries a very significant risk of progressing to a stroke and these
cases should be assessed within 24 hours with carotid imaging, as should patients presenting with
crescendo TIAs (more than one episode in a week). In centres without seven-day TIA clinics this may
require admission to hospital.
Investigations
Once a stroke is suspected clinically, the appropriate investigation should be pursued urgently to allow
optimal treatment.
Laboratory tests
A blood glucose level is necessary to exclude hypoglycaemia as a stroke mimic and this can usual be
done as a bedside finger prick test. Blood tests should be sent for full blood count and biochemistry. A
coagulation screen should be sent particularly if a bleed is suspected, if the patient is anti-coagulated or
if thrombolysis is being considered. In the days after a stroke, thyroid function tests, lipid profile and ESR
are also useful investigations.
Table 3 – ABCD2 score
A – age > 60 (1 point)
B – blood pressure >140/90 (1 point)
C – clinical picture:
Unilateral weakness (2 points)
Speech disturbance (1 point)
D – Duration
>60 minutes (2 points)
1-59 minutes (1 point)
D – Diabetes (1 point)
Total out of max. 7

Imaging and their common appearances
CT remains the mainstay in acute radiological investigation in suspected stroke. This should happen
urgently, within 1 hour, in cases being considered for thrombolysis and those cases with a low Glasgow
come score (GCS), signs of meningism or a high suspicion of intra-cerebral bleed11
. All strokes should
have imaging within 24 hours of presenation11,12
.
The role of CT in the immediate phase is mainly to exclude the presence of intracranial haemorrhage.
Intra-cerebral, subarachnoid, subdural and extradural bleeds have a characteristic appearance on CT.
Intra-cerebral haemorrhages are generally rounded, well-circumscribed lesions within the brain
parenchyma (Figure 1). They may have surrounding oedema or extend into the ventricles.
Infarcted cerebral tissue appears unchanged on CT scans in the first few hours. The changes seen later
develop at a range of 2-3 Hounsfield units per hour. The human eye can only detect a difference in
contrast of over 6 Hounsfield units so a clinically apparent stroke will only become radiological apparent
after a few hours.
There are patterns on CT that can indicate cerebral infarction, particularly when applied with the
suspected vascular territory. There may be a loss of differentiation between grey and white matter.
When this occurs in the insular region it is referred to as the insular ribbon sign. Loss of differentiation
may also occur between structures such as the basal ganglia and internal capsule. There may be sulcal
effacement due to underlying oedema. Clot may be visible in the proximal middle cerebral artery,
“dense MCA” sign (Figure 2) or as a “dot sign” if a more distal branch has been occluded. In the posterior
circulation, a hyper-dense basilar artery may be visible (Figure 3) and a high suspicion of impending
occlusion is necessary in patients presenting with nausea and vertigo and posterior circulation signs.
Cerebellar and brainstem strokes are poorly imaged on CT and may require MRI if the diagnosis is in
doubt.
Figure 1: CT of an intra-cranial bleed
Figure 2: Dense MCA Sign

Figure 3: Hyper
Images used with permission from (Fig1) www.radiologysigns.tumblr.com
(Fig 3) www.bjcardio.co.uk
MRI has become a useful tool in stroke diagnosis in recent years. This is primarily due to the use of
diffusion weighted imaging (DWI). Acute infarcts will appear bright on DWI for up to fourte
detailed images produced with MRI, as well as the superior imaging of the posterior intra
structures makes this modality useful when a PoCS is suspected or if the diagnosis or vascular territory is
in doubt. Other MRI modalities such a
The availability of MRI, particularly out of hours, means that it does not have a place in the hyper
phases of stroke management and is unlikely to replace CT in the near future however it remains a
useful adjunct.
Figure 3: Hyper-dense basilar artery
www.radiologysigns.tumblr.com (Fig 2) ww.med-ed.virginia.edu/courses/rad/headct/infection9.html
MRI has become a useful tool in stroke diagnosis in recent years. This is primarily due to the use of
diffusion weighted imaging (DWI). Acute infarcts will appear bright on DWI for up to fourte
detailed images produced with MRI, as well as the superior imaging of the posterior intra
structures makes this modality useful when a PoCS is suspected or if the diagnosis or vascular territory is
in doubt. Other MRI modalities such as gradient echo can identify microhaemorrhages.
The availability of MRI, particularly out of hours, means that it does not have a place in the hyper
phases of stroke management and is unlikely to replace CT in the near future however it remains a
ed.virginia.edu/courses/rad/headct/infection9.html
MRI has become a useful tool in stroke diagnosis in recent years. This is primarily due to the use of
diffusion weighted imaging (DWI). Acute infarcts will appear bright on DWI for up to fourteen days. The
detailed images produced with MRI, as well as the superior imaging of the posterior intra-cranial
structures makes this modality useful when a PoCS is suspected or if the diagnosis or vascular territory is
s gradient echo can identify microhaemorrhages.
The availability of MRI, particularly out of hours, means that it does not have a place in the hyper-acute
phases of stroke management and is unlikely to replace CT in the near future however it remains a

Imaging of the cerebral blood supply, particularly at a carotid level, can assist in identifying the
pathophysiology of embolic strokes. Plaque formation causing stenosis in the internal carotid arteries
leads to thrombus formation that then embolises to more distal cerebral vessels. This imaging can be
done by Doppler measurements in the acute phase after stroke so decisions can be made about carotid
endarterectomy. The use of CT angiography is becoming increasingly popular as new hyper-acute
treatments including intra-arterial thrombolysis and mechanical clot retrieval are investigated. These
interventions rely on early and detailed imaging of the cerebral blood supply. It is also useful in cases of
suspected carotid or vertebral dissection. CT angiography is often not routinely available out of normal
working hours and its use is at the discretion of stroke physicians and radiologists.
Cardiac investigations
The aim of cardiac investigations in stroke patients is to identify atrial fibrillation as a source of cardiac
emboli. In the acute phase, this can be done with a bedside 12 lead ECG. In time, patients with embolic
strokes will need further cardiac investigations to guide secondary prevention measures.
Treatment and Management
In the acute phase, there are several important areas of stroke care to consider including treatment of
the acute event and prevention of complications. Haemorrhagic strokes may need discussion with the
neurosurgeons.
Apart from thrombolysis or antiplatelet measures, the management of these cases has many similarities
to cerebral infarcts and is discussed below. For cerebral infarcts, specific treatment options need to be
considered.
Acute Treatment Options
Thrombolysis
All stroke patients presenting with a suspected cerebral infarction and a time of onset within 4.5 hours
should be considered for thrombolysis. This requires the urgent exclusion of haemorrhage and
discussion with a stroke consultant. Thrombolysis has been shown to improve functional outcome
though it has no effect on mortality. It involves the giving of an intravenous fibrinolytic agent
(recombinant tissue plasminogen activator).
Thrombolysis is licensed for adults of all ages and benefit has been confirmed in the elderly beyond the
age of 80 years9. Treatment is most effective when the “door to needle” time is shortest. The primary
risk of treatment is haemorrhage, either intra- or extra-cranial. Asking about contraindications can
minimise this risk.
Contraindications include a time of onset greater than 4.5 hours prior to treatment, blood pressure
>180mmHg systolic or > 110mmHg diastolic, blood glucose >22 or <2.8mmol, abnormal clotting or
known anti-coagulation, thrombocytopenia, established infarct on CT, history of haemorrhage, recent
surgery, previous strokes in patients with diabetes, seizure activity at any time in the presentation and
pre-existing significant disability. Some contraindications are relative where others absolute. Some may
be modifiable, such as blood pressure. The issue of pre-existing disability relates to the aim of
thrombolysis to improve the chances of good functional recovery, this requires a reasonable premorbid
level of function.
Stroke physicians will review each case on an individual basis and balance the risks and benefits. The
counselling undertaken before thrombolysis can be complex and emotional for patients and relatives.
After thrombolysis patients require intensive monitoring in a specialist unit and repeat scan after 24
hours to exclude haemorrhagic transformation. Following this they can be started on high dose aspirin.
Antiplatelet and anticoagulant therapy
For those patients not having thrombolysis but in whom a haemorrhage has been excluded, the
mainstay of treatment is high dose aspirin (300mg daily). This is continued for fourteen days after the
initial event with the aim of reducing the risk of a further embolic event. Long-term antiplatelet therapy
is with clopidogrel.
Anticoagulant therapy is usually omitted for fourteen days post-stroke. In those on anticoagulants at the
time of infarction the decision to continue or stop may be taken by the stroke consultant and depends
on the infarct size and risks involved.
Blood pressure control
Blood pressure levels often rise around the time of an acute stroke. The risk of allowing blood pressure
to rise is that intra-cerebral haemorrhage may expand and cerebral infarcts may develop haemorrhagic
transformation. Lowering blood pressure in the acute phase after a stroke is contentious as it may be
that the rise seen is a physiological response to maintain cerebral perfusion. Ideally blood pressures
should be kept below 180mmHg but advice should be taken from a stroke specialist.
Nutrition and hydration
Many stroke patients will have an unsafe swallow in the early phases after the event. A ward based
swallow assessment should be completed as soon as possible. In those with an unsafe swallow,
medication should be reviewed and either suspended or given via an alternative route (rectal,
intravenous or topically). Intravenous fluids can be given and artificial feeding should be considered
within the first 24 hours by a nasogastric tube. Aspiration pneumonia is a common complication of
stroke and a low threshold for treatment should be maintained.
Thrombo-embolism prophylaxis
Thrombo-embolic events are an important cause of death following stroke. Routine prophylaxis with
low molecular weight heparin carries risks. It is contra-indicated in acute haemorrhagic stroke and can

increase the risk of haemorrhagic transformation in cerebral infarction. Graduated compression
stockings have been shown to cause more harm than benefit including pressure damage in stroke
patients and are now contraindicated13
. Recent research suggests the use of intermittent pneumatic
compression stockings can be used to reduce thrombo-embolic risk14
and the case for using low
molecular weight heparin can be discussed on a case-by-case basis dependent on the individual risk.
Review of patients with acute strokes
All stroke patients should be transferred to the acute stroke unit as soon as possible after admission.
They should be seen within the next 24 hours by a stroke consultant or associate specialist and within 72
hours by the multidisciplinary team therapists.
The Next Step
The aim of all management in stroke is two fold, to restore as much function as possible to the individual
and to reduce the chance of future similar events. The former relies on rehabilitation and the skills of
the multidisciplinary team. The latter has grown from an evidence base that can then be tailored to each
individual patient’s needs. These issues will be reviewed in the next article on stroke care.
References
1. Oxford English Dictionary http://www.oxforddictionaries.com/definition/english/stroke
2. Lee S et al. UK stroke incidence, mortality and cardiovascular risk management 1999–2008: time-trend
analysis from the General Practice Research Database. BMJ Open 2011;1:e000269 doi:10.1136/bmjopen-
2011-000269
3. Wolf P A et al. Secular trends in stroke incidence and mortality. The Framingham Study. Stroke.1992; 23:
1551-1555
4. Brown RD et al. Stroke incidence, prevalence, and survival: secular trends in Rochester, Minnesota,
through 1989. Stroke; a Journal of Cerebral Circulation [1996, 27(3):373-380]
5. Indredavik B et al. Benefit of a Stroke Unit: A randomized controlled trial Stroke 1991;20:1026-1031.
6. Hack W et al. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS,
and NINDS rt-PA stroke trials. Lancet. 2004;363:768–774.
7. Whiteley WN et al. Clinical Scores for the identification of stroke and transient ischaemic attack in the
emergency department: a cross-sectional study. Neurol Neurosurg Psychiatry. 2011 Sep;82(9):1006-10.
doi: 10.1136/jnnp.2010.235010. Epub 2011 Mar 14.
8. Nor AM et al. The Recognition of Stroke in the Emergency Room (ROSIER) scale: development and
validation of a stroke recognition instrument. Lancet Neurol. 2005 Nov;4(11):727-34.
9. P Sandercock et al. The benefits and harms of intravenous thrombolysis with recombinant tissue
plasminogen activator within 6 h of acute ischaemic stroke (the third international stroke trial [IST-3]): a
randomised controlled trial. Lancet. 2012 June 23; 379(9834): 2352–2363.
10. Pittock SJ et al. The Oxfordshire Community Stroke Project classification: correlation with imaging,
associated complications, and prediction of outcome in acute ischemic stroke. J Stroke Cerebrovasc Dis.
2003 Jan;12(1):1-7.
11. http://guidance.nice.org.uk/CG68/QuickRefGuide/pdf/English CG68: Stroke.
12. http://www.sign.ac.uk/pdf/qrg108.pdf Guideline 108: Management of patients with stroke or TIA:
assessment, investigation, immediate management and secondary prevention
13. The CLOTS trial collaboration. Effectiveness of thigh-length graduated compression stockings to reduce
the risk of deep vein thrombosis after stroke (CLOTS trial 1): a multicentre, randomised controlled trial.
The Lancet, Volume 373, Issue 9679, Pages 1958 - 1965, 6 June 2009

14. The CLOTS trial collaboration. Effectiveness of intermittent pneumatic compression in reduction of risk of
deep vein thrombosis in patients who have had a stroke (CLOTS 3): a multicentre randomised controlled
trial. The Lancet, Volume 382, Issue 9891, Pages 516 - 524, 10 August 2013

Secondary Prevention and Rehabilitation after a Stroke
Dr Gemma Smith (Specialty Trainee in Elderly Care and Stroke Medicine)
Correspondence - Gemma Smith: [email protected]
ABSTRACT
After an acute stroke, consideration of secondary prevention and rehabilitation should start as soon as
possible. The risk of recurrent stroke is high but it can be reduced by pharmacological or even surgical
interventions. Stroke rehabilitation concentrates on addressing neurological deficits, preventing
complications, maintaining health and addressing the psychological impact the event may have had.
Stroke management in this phase of care requires multidisciplinary team input and may take place over
days, weeks, months or even years. The interventions required should be personalised for the
individual’s needs.
Key Words: stroke; rehabilitation; prevention
Introduction
After an acute stroke, consideration of secondary prevention and rehabilitation should start as soon as
possible. The risk of recurrent stroke is high but it can be reduced by pharmacological or even surgical
interventions. Stroke rehabilitation concentrates on addressing neurological deficits, preventing
complications, maintaining health and addressing the psychological impact the event may have had.
Stroke management in this phase of care requires multidisciplinary team input and may take place over
days, weeks, months or even years. The interventions required should be personalised for the
individual’s needs.
Secondary Prevention
The risk of recurrent stroke following a first event is significant1 (fig 1). Thus, the task of secondary
prevention should start immediately. This includes clot prevention, blood pressure and cholesterol
control, specific therapies around carotid or cardiac disease and lifestyle measures. The implementation
of any secondary prevention measure should be balanced with the needs of the individual and patients
should understand the goals of these therapies to encourage future concordance.

Figure 1: Risk of Stroke Recurrence prior to optimal treatment
Time from first stroke. Risk of recurrence.
30 days 3-10%
1 year 5-14%
5 years 25-40%
Clot Prevention
In the first fourteen days following an ischaemic stroke, high dose aspirin (300mg daily) is most effective
at preventing further events. It inhibits platelet aggregation and therefore clot formation. After this
time, aspirin can be stopped and clopidogrel 75mg commenced. Previously, aspirin was used in
conjunction with dipyridamole and this regimen is still used when clopidogrel is not tolerated due to
allergy. All antiplatelet regimens carry an increased risk of bleeding.
Antiplatelet agents aim to prevent in situ thrombus formation or embolic events arising from carotid
artery disease. Alternative agents are required for stroke occurring from cardio-embolic disease. Atrial
fibrillation carries an increased risk of stroke due to the development of thrombus within the left atrial
appendage. All patients should be screened for atrial fibrillation following a stroke with ambulatory ECG
monitoring. For young patients with no cardiac history this can be completed over twenty-four hours
however older patients or those with structurally abnormal hearts may benefit longer periods of
monitoring2, 3
. An echocardiogram can inform the risk of atrial fibrillation by looking for atrial
enlargement and valvular disease.
The CHA2DS2Vasc score4
was developed to help guide treat patients who had atrial fibrillation, and has
superseded the CHADS2 score in some centres. The components of this scale and points tally are as
follows:
Congestive heart failure – 1 point
Age ≥75 years – 2 points / 65-74 - 1 point
Diabetes Mellitus 2 – 1 point
Gender – female 1 point / male 0 points
Hypertension consistently above 140/90 mmHg (or treated hypertension) – 1 point
Previous stroke or TIA – 2 points
Vascular disease (such as peripheral vascular disease) – 1 point
The total score correlates with the annual risk of a stroke, and can help guide treatments of atrial
fibrillation (Fig 2).

Figure 2: CHA2DS2Vasc score and the annual risk of stroke in patients with atrial fibrillation
Patients scoring 2 or more should be considered for oral anticoagulant therapies. Historically this has
been coumarin therapy, usually warfarin, monitored with international normalised ratio (INR)
measurements (target range 2-3). In recent years, other anticoagulants have emerged. Dabigatran is a
direct thrombin inhibitor and Rivaroxaban and Apixaban are direct factor Xa inhibitors. These drugs
require no monitoring and data suggest a reduced likely of bleeding complications5, 6,7
. However if
bleeding does occur they are do not have a specific antidote. The risk of bleeding can be quantified to
some extent using the HAS-BLED8 score but other factors such as co-morbidities, dependency and falls
may play a role in rationalising therapy and decisions should be individualised. In some patients
conversations with stroke physicians may be advisable. Anticoagulant therapy is usually commenced 14
days after an acute stroke.
Echocardiograms carried out to look for cardiac sources of emboli occasional identify patent foramen
ovale (PFO). This is not uncommon in the general population and the role of these lesions in stroke is not
entirely clear. The possibility of paradoxical embolus, emboli arising from thrombus in the deep venous
circulation and crossing the atrial septum to reach the arterial circulation, must be considered. In the
absence of confirmed venous thrombus, antiplatelet rather than anticoagulant therapy is the mainstay
of secondary prevention and the role of closing these PFOs is unclear. Valvular lesions seen on
echocardiogram may also need specialist intervention and the guidelines above for atrial fibrillation
relate to non-valvular disease.
Blood Pressure
In the acute phase following a stroke, control of hypertension is guarded as cerebral perfusion may rely
on a degree of systemic hypertension. Levels above 180 / 110mmHg however, may carry an increased
risk of enlargement of an intra-cerebral haemorrhage or haemorrhagic transformation of an infarct and
should be addressed. Long-term blood pressure control should be aimed at maintaining readings at
CHA2DS2-VASc Score Annual Stroke
Risk %
0 0
1 1.3
2 2.2
3 3.2
4 4.0
5 6.7
6 9.8
7 9.6
8 6.7
9 15.2

<140/90mmHg, or <130/80mmHg for those patients with diabetes or chronic kidney disease and has
been shown to reduce the risk of further events9, 10
. The choice of antihypertensive agent is probably not
important, it is the lowering of blood pressure that is significant, however often other indications for
specific agents may exist. Selection of hypertensive agents is usually selected based upon national or
local guidelines. The benefit of lowering blood pressure is seen in older age groups though over-
treatment of hypertension may increase the risk of orthostatic hypotension and falls.
Cholesterol
The role of hyperlipidaemia on the pathogenesis of vascular disease, include stroke, is well documented
and there is good evidence that statin therapy reduces stroke risk11
. LDL cholesterol is a more specific
target for reduction than total cholesterol though both can be used to guide therapy. An LDL level
<2.0mmol and total cholesterol <3.5mmol is ideal. Patients sometimes wish to try dietary measures to
reduce cholesterol before starting treatment. If statin therapy is not tolerated, other lipid lowering
agents can be used, such as ezetimibe, though the evidence base is less clear. In haemorrhagic strokes,
the role of statins is contentious.
Carotid Disease and Intervention
In patients suffering an ischaemic stroke or TIA, the source of embolus may be atherosclerotic disease in
the internal carotid artery. If this disease causes significant stenosis then surgery may be indicated in the
form of carotid endarterectomy (CEA). This significantly reduces the chance of further strokes,
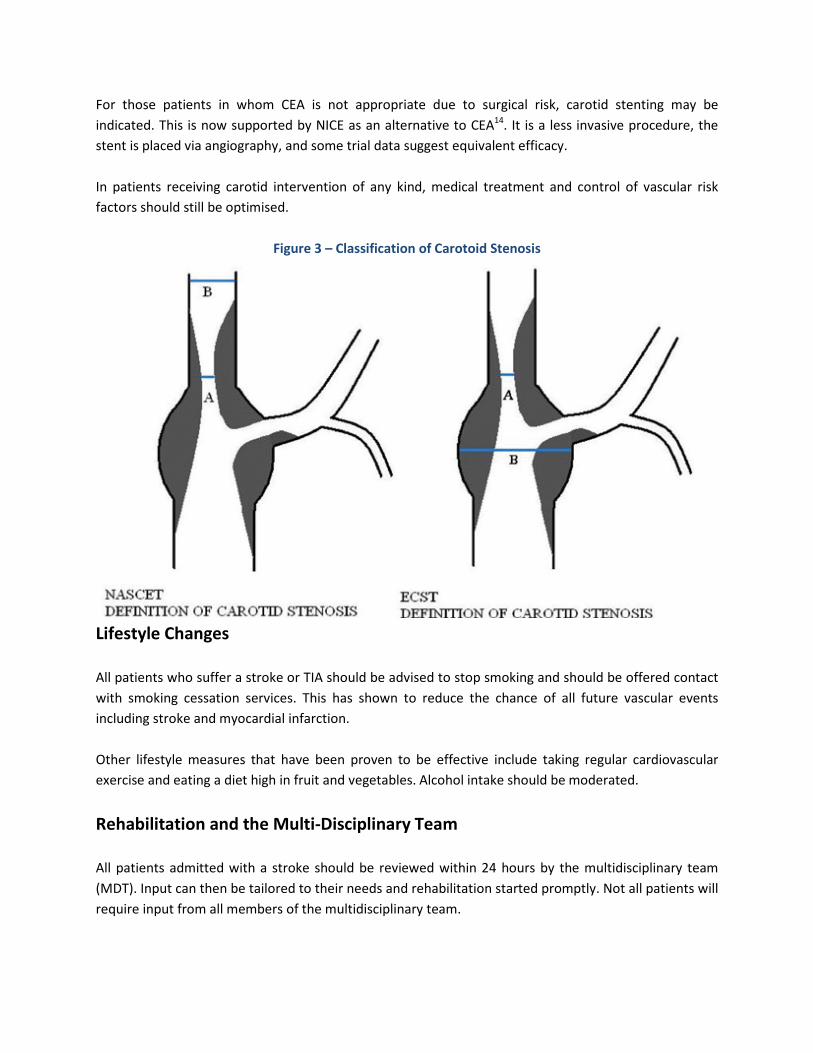
particularly in the higher degrees of stenosis (>70% by NASCET criteria)12
. Carotid stenosis is routinely
assessed by doppler ultrasound. Two systems exist (fig 3)13
, the North American Symptomatic Carotid
Endarterectomy Trial (NASCET) and the European Carotid Surgery Trialists' Collaboration group (ECST).
These take different measurements for comparison to the stenosed area. NASCET compares the normal
distal lumen, ECST uses the diameter of the carotid bulb. A NASCET measurement of 50-99% stenosis or
ECST measurement of 70-99% stenosis is an indication for surgery to be considered. Carotid imaging and
referral to the appropriate vascular surgical team should take place within one week of symptom onset
and surgery should take place within two weeks of symptom onset if it is to go ahead. In cases where
the internal carotid artery is completely occluded there is no role for CEA.
Carotid surgery is a major undertaking and many people who experience a stroke or TIA have significant
other co-morbidities that make them unfit for surgery. The aim of CEA is to prevent future disabling
strokes. For this reason, people who are already significantly disabled, by their stroke or other
conditions, to do not stand to gain the same benefit as those with good functional status. This must be
judged carefully on an individual basis. The difference between surgery on the carotid artery of the
dominant or non-dominant cerebral hemisphere may be significant. Incidental stenosis of the
asymptomatic carotid is not an uncommon finding on doppler ultrasound but currently there is no role
for routine surgery on these lesions.
For those patients in whom CEA is not appropriate due to surgical risk, carotid stenting may be
indicated. This is now supported by NICE as an alternative to CEA14
. It is a less invasive procedure, the
stent is placed via angiography, and some trial data suggest equivalent efficacy.
In patients receiving carotid intervention of any kind, medical treatment and control of vascular risk
factors should still be optimised.
Figure 3 – Classification of Carotoid Stenosis
Lifestyle Changes
All patients who suffer a stroke or TIA should be advised to stop smoking and should be offered contact
with smoking cessation services. This has shown to reduce the chance of all future vascular events
including stroke and myocardial infarction.
Other lifestyle measures that have been proven to be effective include taking regular cardiovascular
exercise and eating a diet high in fruit and vegetables. Alcohol intake should be moderated.
Rehabilitation and the Multi-Disciplinary Team
All patients admitted with a stroke should be reviewed within 24 hours by the multidisciplinary team
(MDT). Input can then be tailored to their needs and rehabilitation started promptly. Not all patients will
require input from all members of the multidisciplinary team.

MDT input can happen on the acute stroke unit, in a rehabilitation centre or at the patient’s own home.
It should continue as long the patient is receiving benefit and making progress but should not persist
when there is no hope of further improvement as this can be psychologically distressing.
Physiotherapy
The role of physiotherapy following a stroke does not just centre around increasing strength and
assisting mobility. Following a stroke, patients may suffer from a range of problems which have a motor
component. They may have weakness, in co-ordination and imbalance, spasticity, pain and marked
functional impairment. They may also require physiotherapy involvement for respiratory secretions
following pneumonia.
The speed at which neurological motor deficits resolve depends on numerous factors such as age, pre-
morbid health and cognition. Lower limbs tend to improve more quickly than upper limbs as the area of
motor cortex which supplies the legs has some dual blood supply from both the anterior and middle
cerebral arteries. Patients with expressive or receptive dysphasia may struggle to communicate with
physiotherapists. Higher cortical function such as inattention can make it difficult for a patient to
identify one side of their body and therefore use those muscles in exercise. Fatigue and depression may
limit a patient’s interaction with therapy. This can be an extremely prominent component in some
patients.
Spasticity can develop over time following a stroke. This can restrict function and be painful and
disabling. If spasticity is left untreated it can lead to permanent muscle shortening and contractures.
These can interfere with activities of daily living; a hand with fixed finger flexion may be difficult to clean
and long nails may cause trauma to the skin. Physiotherapy will identify spasticity early and work at
preventing progression. This can be with active or passive stretching exercises. In more severe cases,
splinting or applying plaster casts can help the affected limb to assume an appropriate position. Patients
with spasticity may respond to medical therapies such as baclofen and tizanidine, though these are not
without side effects. In selected cases botulinum toxin can be injected into the muscle. Increased tone
can occasionally be used to a patients advantage. A leg with increased tone may make transferring from
a chair to bed easier than it would be with a flaccid leg.
Often the goal most important to patients following a stroke is regaining the ability to walk. This is a
complex task requiring rehabilitation of strength, balance and cognition. It is a gradual process,
progressing from using aids to help reach a standing position to walking a few steps with assistance and
then walking with increasing independence and the use of mobility aids such a wheeled walking frames
or sticks. Orthoses may be required to treat specific problems such as foot drop. Regaining balance
requires first the ability to sit and then stand and correct posture to compensate from external forces.
Once mobility is regained, the chance of returning to independent living is greatly increased.
Goal setting and standardised measurements are useful in rehabilitation. Reducing a large goal into
smaller goals can make the journey appear more manageable for patients and maintain their
motivation. Objective scales to measure strength, balance and function allow progress to be recorded

and reviewed, even when staff change between rehabilitation sessions. Power can be recorded using
the Medical Research Counsil 0-5 scale, angles of flexion and extension can be objectively measured,
balance can be assessed with the Tinnetti scale. Overall function is measured on the modified Rankin
scale but changes between grades may mask smaller degrees of improvement.
Occupational Therapy
The role of the occupational therapist is to rehabilitate patients to their activities of daily living. This
includes any activity important to the individual at their stage of life and may go beyond the basic tasks
of washing, dressing and eating.
Activities of daily living often require adequate motor function but also rely on higher cognitive function.
Following a stroke, patients may have issues with praxis (planning and executing complex tasks) and
communication, including expressive and receptive dysphasia. Concentration on the task in hand and
the ability to recall which stages have already been completed is important, as is the ability to attend to
both sides of the body and the immediate environment. Deficits in many of these areas may co-exist,
making a previously simple task challenging.
Occupational therapy enables tasks to be broken down into composite parts that can later be pieced
back together to formulate the complete process. The various stages may benefit from the use of aids to
support patients to pursue the task independently; for example, a plate guard can allow a patient with a
single functioning upper limb to feed themselves from a plate. Technology is playing an increasing role
in occupational therapy rehabilitation and many “apps” are available for use on tablet platforms to
increase concentration, planning and attention.
Cognitive assessment after a stroke often falls within the remit of occupational therapy. All stroke
patients should have a cognitive assessment post-stroke even if no obvious deficit exists. Subtle
problems may be present and may have a significant impact on a person’s ability to live independently
and safely. This cognitive assessment can be challenging, particularly in patients with speech problems.
The Montreal Cognitive Assessment tool (MoCA) is well validated but requires adjustment for those with
expressive dysphasia. Following a stroke, many patients will have a persistent cognitive deficit, labelled
as Vascular Cognitive Impairment (VCI). This is distinct to vascular dementia which is a progressive
process and may occur without evidence of clinical stroke disease but it is possible for someone with VCI
to develop vascular dementia as many of the risk factors are the same.
The most recognised role of occupational therapy is to assist the discharge of a patient by reviewing
their home environment and providing aids and assistance to make that environment appropriate for
their new needs. Despite the best rehabilitation, many patients are left with some residual difficulties
following a stroke and many of these patients are pre-morbidly older and frail with multiple co-
morbidities impacting on their ability to self-care. An assessment of the home environment will often be
carried out before discharge, sometimes with the patient themselves. Areas of attention are access in
and out of the building, enabling mobility around the house, including stairs, and transfer in and out of
bed or bath. Toileting needs may require the provision of a commode. The height of light switches,

electrical points or work surfaces may need to be adjusted if patients are now required to use a
wheelchair. Speaking aids may assist patients with dysphasia. Alarms fitted to beds and doors may alert
carers to the movements of a patient who is confused or at risk of falls.
Speech and Language Therapy
There are two main roles to speech and language therapy following stroke. Patients require assessment
and review of their ability to swallow safely. They may also need assessment of their ability to speak and
understand as even a subtle deficit could have a significant impact on their approach to rehabilitation.
Swallowing ability is usually assessed immediately post-stroke by ward nursing staff. Even people
presenting with presumed mild deficits may have difficulty swallowing safely and may be at risk at
aspiration. Swallowing is a complex task and each stage needs to happen safely to prevent aspiration.
Initial deficits in swallow function can be approached in two ways. Either diet can be adapted by
thickening fluids and providing soft or pureed diet or, in the case of entirely unsafe swallowing, artificial
enteral feeding via naso-gastric tube may be attempted. In some cases unsafe swallowing mechanisms
may persist and discussions may be had regarding long term feeding via a percutaneous endoscopic
gastrostomy (PEG) tube.
Speech is a function of the dominant cerebral hemisphere. In most right handed people this is the left
hemisphere and in a slightly smaller majority of left handed people it is the right hemisphere. Strokes
affecting the dominant hemisphere can cause issues with both the understanding of speech (receptive
dysphasia), the formation of speech (expressive dysphasia) or both. Speech changes are also possible in
non-dominant hemisphere strokes but may present with increased verbosity or conversely the inability
to speak due to apraxia rather than dysphasia.
The loss of speech and understanding can be a very emotional and frustrating issue for patients
following a stroke. Communication can be facilitated in numerous ways using picture and letter cards,
digital speech tools and gestures. The participation in conversation, though frustrating, is therapeutic to
improving speech overall. It requires time and patience but can be provided by untrained family, friends
and carers under the guidance and review of speech and language therapists. Dysphasia may impact on
mental capacity if a patient is unable to communicate their wishes.
Psychological Support
A stroke, whatever the magnitude of the neurological deficit, can have an enormous impact on the
psychological wellbeing of the person. There are numerous issues to contend with including the
acceptance of fallibility and mortality, coming to terms with possible on-going physical problems and the
need to depend on others. There may be a loss of role within society, such as that of carer or wage
earner and concerns for the future, particularly whether a further stroke will occur. In addition to these
issues of adjustment, post-stroke depression is a well-recognised phenomenon that has a neurochemical
basis. Ischaemic damage to neurones disrupts serotonergic and dopaminergic pathways that can lead to

a biological cause of depression. Depression can impact on a patient’s ability to rehabilitate. It may lead
to poor sleep, impaired appetite and subsequent low energy levels and low motivation.
Formal psychological support is of limited availability within hospital medicine as a whole. Ideally,
patients with psychological issues following a stroke would have access to assessment and therapy with
clinical psychologists. In the absence of these services there are other routes that can be pursued.
Listening, explaining and reassuring are tools that any healthcare professional can provide and the
importance of these processes should not be under-estimated. An awareness of what this event means
to the individual and not attempting to minimise these feelings is essential. Education as to the cause of
strokes and future risks following secondary prevention may provide some reassurance and the process
of rehabilitation can restore hope and the idea of a future. The Stroke Association is a charitable
organisation that can provide other forms of support including group sessions or the provision of a
“buddy” who has previously been through similar events or comes from a similar background. In some
cases, post-stroke depression requires pharmacological intervention. This is usually in the form of
selective serotonin re-uptake inhibitors. This may be short-term in nature and can be reviewed at a later
date.
Conclusion
A stroke can be a devastating event and the subsequent recovery can be a long process. Life after a
stroke may involve coping with a new disability, physical or cognitive, and with new medications.
Prompt treatment in the acute phase followed by holistic rehabilitation gives patients the best chance of
returning to independent living. Secondary prevention gives the best chance of not having to experience
the same challenge again in the future.
References
1. http://www.stroke.org/site/DocServer/NSAFactSheet_RecurrentStrokerevised.pdf?docID=998
2. Higgins P et al. Noninvasive Cardiac Event Monitoring to Detect Atrial Fibrillation After Ischemic Stroke: A
Randomized, Controlled Trial. Stroke 2013; 44: 2525-2531
3. Raymond C S et al. Prolonged Rhythm Monitoring for the Detection of Occult Paroxysmal Atrial Fibrillation
in Ischemic Stroke of Unknown Cause. Circulation. 2011; 124: 477-486
4. Hohnloser H et al. Prevention of stroke in patients with atrial fibrillation: current strategies and future
directions. Eur Heart J Suppl September 1, 2008 vol. 10 no. suppl H H4-H10
5. Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, et al. Dabigatran versus warfarin in
patients with atrial fibrillation. N Engl J Med. 2009;361:1139–1151.
6. Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, et al. Rivaroxaban versus warfarin in
nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883–891.
7. Granger CB, Alexander JH, McMurray JJ, Lopes RD, Hylek EM, Hanna M, et al. Apixaban versus warfarin in
patients with atrial fibrillation. N Engl J Med. 2011;365:981–992.
8. Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY. A novel user-friendly score (HAS-BLED) to
assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest. 2010;
138: 1093–1100.
9. PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure lowering regimen
among 6105 individuals with previous stroke or transient ischaemic attack. Lancet. 2001; 358: 1033–1041.
10. Chobanian AV et al. National Heart, Lung, and Blood Institute Joint National Committee on Prevention,

Detection, Evaluation, and Treatment of High Blood Pressure, National High Blood Pressure Education
Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention,
Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003; 289: 2560–
2572.
11. Amarenco P et al. Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators.
High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006; 355: 549–559.
12. Benefit of Carotid Endarterectomy in Patients with Symptomatic Moderate or Severe StenosisHenry
J.M et al for the North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med
1998; 339:1415-1425.
13. Swinnen J et al. carotid duplex ultrasound after carotid stenting. AJUM August 2010; 13 (3):20-22
14. Carotid artery stent placement for symptomatic extracranial carotid stenosis (IPG389) National Institute
for Health and Clinical Excellence. April 2011. www.guidance.nice.org.uk

What is the Scope of Autonomy in Medical Practice?
S. Falahati (University of Glasgow)
Correspondence – S. Falahati: [email protected]
ABSTRACT
Autonomy, literally meaning self-rule, is an essential ethical principle, especially within the field of
medicine. An individual with autonomy can make decisions on the basis of reflection and deliberation
[1]. In general philosophy, autonomy is thought of as “the ability to be one's own person, to live life
according to rationale and purpose that are taken as one's own and not the consequence of controlling
or distorting outside forces” [2]. Individual autonomy is a notion that cultivates both self-ownership and
self-governance and is based on ‘respect for persons‘, which states that all persons have the right “to
make their own choices and develop their own life plans” [3]. The scope of autonomy reflects how far-
reaching autonomy is, and what its boundaries are. This paper analyses the scope of autonomy in order
to achieve greater clarity, and asks if this ethical principle should be superior to the three other
principles (beneficence, non-maleficence and justice) rather than just “prima facie”.[4] Indeed, if there
were to be a single overriding principle at all, should it definitely be autonomy rather than any of the
other three? These questions will be dealt with and explored with the aid of medical ethical scenarios
which help illustrate the points raised. We will identify what the limitations of autonomy are, and how
far-reaching it is, all within the medical context.
Key Words: autonomy; medicine; independence
Introduction
Respect for autonomy is widely accepted as imperative in medical ethics within the Western world.
Although there are cultural differences on the importance of autonomy, it is on the whole the scope of
autonomy where the conflict lies. Certain medical cases can be sources of dilemma for doctors. This
raises the question whether autonomy is only truly respected on the condition that it is the overall
absolute principle to be adhered to, or whether respect for autonomy can remain intact without it being
a conclusive concept. In order to answer this question, the issue needs to be looked at from different
angles. Two aspects in dealing with this subject are in an action-based as well as a situation-based
approach [4].
Principlism is an action-based approach that is based on the development of the four principles by
Beauchamp and Childress [4]. It applies four prima facie principles [5] (‘prima facie’ meaning that the
principles are binding unless conflicting with another principle) - respect for autonomy, beneficence,
non-maleficence, and justice. Beneficence takes into account the patient’s best interests, non-

maleficence (literally meaning “to do no harm”) considers the risks and benefits to the patient, and
finally justice is doing what is fair for the patient. Beauchamp and Childress state that these four
principles can be used as a starting point in order to justify and make an ethical decision, where all the
principles are balanced against each other in order to determine which has the most weight in each
case. Casuistry is a situation-based approach where different cases impact on the moral principles
chosen, and not the other way round. Therefore, unlike principlism, the starting point for making ethical
decisions is to look at other similar cases, and from those, learn how to best handle the situation at
hand. Generally, in medical ethics principlism is preferred to casuistry. This tends to be due to the fact
that in medicine every case will be unique in its own way. Even cases that are similar in many respects
can have different outcomes due to one small difference between them. Principlism is also preferred in
cases where time is an issue, and a decision needs to be made quickly and other cases cannot be looked
upon.
Both systems of thought, however, are open to critique. The main disparagement of principlism is the
inability of choosing one principle over the other when dispute arises between principles. One could
argue that when trying to balance the principles, in the style Beauchamp and Childress advise, the
principles become open to interpretation and can become nothing more than principles that can be
manipulated to justify a hidden agenda. This lack of solid defining criteria can leave the four-principle
approach vulnerable to those with ill intentions. The same can be said of casuistry.
WD Ross [5] makes an effort to give a clearer idea of how to come to a decision when there is conflict
between two principles by mixing both the ideas of casuistry and principlism. He asserts that in times
where more than one prima facie principle is involved in a situation, the case should be analysed as
thoroughly as possible until an opinion is formed where one principle is “more incumbent” than the
other. Even with this method, a person’s idea of what is “more incumbent” is influenced by any pre-
existing judgements or prejudices that they already have.
Scope of Autonomy with Ethical Case Studies
Various ideas of autonomy have evolved from the many philosophical stances on respect for autonomy.
From Immanuel Kant [6] to John Stuart Mill [7], the intricacies of respect for autonomy differ depending
on whose model you read. The scope is even further widened when culture is brought into play. A whole
nation’s outlook on autonomy can differ vastly from that of another. In one country you may find that
autonomy is strongly based on the rights of the individual, whereas in another you may struggle to see if
respect for autonomy really exists at all. Therefore, in instances where these cultures clash, an area of
conflict can arise. Here is a possible case which highlights an example of this conflict in dealing with
respect for autonomy:
A known Jehovah’s Witness arrives in A&E, unconscious, with heavy bleeding from a road-traffic
accident. He needs an urgent blood transfusion, as without it the prognosis could be fatal. This

particular case touches upon both cultural medicine and capacity. These are concepts that deserve
being scrutinized in detail separately; however, they will be briefly discussed here.
It is against the religious belief of Jehovah’s Witnesses to undergo blood transfusions. However, there
are many factors that come into play for this individual case as well as religion. If the patient was
conscious and was verbally communicating to the doctors that he does not wish to have a blood
transfusion, then a quick decision would need to be made to determine whether the patient has the
capacity to make that choice. Kant [6] believed that autonomy does not embrace those who lack reason.
This can be a point of critique, as it narrows the scope of autonomy by eliminating all those without any
rational way of thinking. Nevertheless, the respect for an individual‘s autonomy should still be
maintained even if he lacks capacity. Assuming this patient was conscious and had capacity, it could be
argued that the patient indeed has no autonomy at all, as he is no longer self-determining and is being
led by his beliefs and religion. On the other hand, yielding your autonomy is indeed an autonomous
action in itself. This could be partial or complete, from allowing a doctor to make a decision on your
behalf, to allowing relatives to take medical custody of you, or indeed as it is in this case, to giving
yourself wholly to a higher religious power. This patient is unconscious which automatically makes him
lack capacity at that time, and although we know that he is a Jehovah’s Witness, it would be foolish to
make assumptions that if he were awake he would definitely refuse a blood transfusion. If there was
enough time, relatives could be questioned, and past notes could be studied, to build a clearer picture
as to what the patient would want. If time was an issue, then the doctor would have to make a decision
based on the four principles.
Autonomy looks to be compromised as it can only be an assumption of what the doctor believes the
patient would want. If non-maleficence is thought of, then what actually would be “not to do harm”? Is
it doing harm not to give a transfusion and let the patient die, or would it be more harmful to do so and
later find out that the patient did not wish this and will have to live with the spiritual consequences of
the doctor’s action? Beneficence and justice can also be justified either way. Beauchamp and Childress
[4] declare that when trying to balance out the principles, a degree of instinct is inevitable, and in a case
such as this a person’s own intuition will possibly be the true decision maker, and will leave the
balancing act of the principles effectively redundant.
The demand for, and refusal of, treatment are also closely bound to autonomy. The following two cases
present the issues that can arise due to this. The first case deals with the refusal of treatment that will
lead to the death of the patient, and the second considers a demand for treatment in fear of dying.
Dax Cowart was an American pilot who suffered a terrible accident in 1973 where most of his body was
severely burned by a propane explosion. The burns had severely disabled Dax, blindness and the loss of
his hands being the two most traumatic disabilities. On his way to the hospital he had refused any
medical treatment, wanting to die as he believed he would never become his normal self again. He
continued to tell the doctors that he did not want any treatment, however the doctors rejected this and
forced treatment upon Dax. He was an in-patient for 10 years, and Dax begged his doctors to let him die,
however they continued to force treatment upon him which caused him pain and suffering. Dax went on

to obtain a law degree, speaking publicly on the right to be allowed to die and still believes that at the
time of his accident the doctors should have granted him his wish.
This case occurred in the USA forty years ago. Current GMC guidance [8] in the UK states that if a patient
has capacity then he or she has the right to refuse treatment even if it results in death. In Dax’s case he
was deemed to be lacking in capacity in order to make that decision. His doctors’ justification was that
he was in too much pain to make a rational choice, yet patients like this are in pain for considerable
amounts of time. Should that necessarily mean their autonomy should be compromised because of the
pain? Dax’s doctors believed that ultimately the ends justified the means. This standpoint can be
interpreted as the doctors taking an action in order to satisfy their own moral convictions and not to do
what is in the patient’s best interest. Kant [6] believed that patients should be treated as ends in
themselves, and this gives power in restoring a balance between doctor and patient, by reducing the
natural paternalism and inequality in place.
Another possible case is that of a 28 year old female who had a family history of breast cancer. Her
mother died of breast cancer, as well as her older sister. She asked doctors for a mastectomy, and did
not want to go through any kind of screening or genetic testing. She didn’t see the point in going
through those kinds of rituals because she “knew” that she had breast cancer, and was tired of living in
fear of finding a lump in her breasts. The doctors refused to do a mastectomy without her going through
the initial procedures first.
Mill’s [7] version of autonomy is directed towards the wishes and requests of the individual. So from
that alone, it could be said that demanding various treatments is within the rights of an individual. In our
patient’s case her request for a mastectomy was not without any reason and logical thinking, so it is
hard from that to deem that she lacks capacity. However, her downright refusal and lack of compromise
with the doctors in figuring out a way to solve her problem led to an impasse for the operation she
seeks. So does autonomy allow negotiation? After all, the doctors were not against giving the patient
the operation, but only on the prerequisite that she undergoes initial tests to see if it is clinically
indicated.
Once more, this falls under Kant’s [6] idea of treating patients as ends in themselves and not merely
means. Even if the viewpoint is taken that the surgery requested was nothing more than an elective
surgery, and not a certain life-threatening situation, what is it that makes this case different from
someone who wishes to have cosmetic surgery done to his/her nose to make themselves feel better? If
the patient has full capacity, then both autonomy and beneficence would be fulfilled if the procedure
was to be done, giving the patient peace of mind and respecting her wishes. Conversely, non-
maleficence and justice can be argued to be compromised if the patient’s request was granted. As with
any surgery, there are risks involved in a mastectomy. In this case, the risks could not be assumed to
outweigh the benefits since there is no clinical evidence to indicate the need for surgery. In terms of
justice and fairness, whether or not to provide a female patient such as this with the resources available
for surgery can be questioned when there are other cases for which the need for surgery are clinically
indicated, not only for breast cancer, but various other diseases as well.

As stated above, John Stuart Mill’s [7] vision of autonomy was firmly based on the liberties and desires
of the individual. A unique case of autonomy that is distinct from others is that of the pregnant woman.
Cases of respect for autonomy involving pregnant women can be tricky to deal with, taking into account
that it is effectively the autonomy of both a female and an unborn child that is at hand. John Stuart Mills
[7] declared that self-determination was valid only on the condition that it does not cause harm to
others.
This is a necessary factor in autonomy, as an individual’s autonomy cannot be adhered to if it is causing
direct harm to another or several other human beings. Therefore, let us think of the case of a pregnant
woman who refuses to have a C-section recommended by her doctors. She has been told that if she
does not have a Caesarean, and continues to go into labour naturally, there is a significant likelihood
that her baby could have severe disability and mental retardation. Under current guidance
recommended by the GMC [9], a pregnant woman is allowed to refuse treatment that would be
beneficial to the unborn child and the rights of the unborn child are not established until it is an
independent entity from the mother (ie – until it is born). Using Mill’s attitude towards autonomy and
the requirement of respecting others to make individual autonomy valid, an argument could be made
for a change in guidelines. Of course, the standpoint of those who favour women having the right to
choose abortion is that the foetus should not be treated as a human being, rather only as something
that has the potential to become one, and so should not be allowed the same rights as a human being.
However, in this particular scenario of the mother refusing a C-section, it is not a question of
termination, as this potential has turned into a certainty. So does that mean that the mother’s
autonomy should be denied, due to the fact she is putting her unborn child at harm? The fact is that if
GMC guidance were to allow the pregnant woman’s autonomy to be infringed, this could set the
precedent for evolution to further possible restrictions as well.
It is obvious that the well-being of the mother and her unborn child are intimately tied to each other,
and even though current guidelines states that the unborn child has no rights, this is not to say that
respect for autonomy should imply that a decision is made without taking into consideration the effects
on the child. In fact some believe that morally, we have duties to those close to us, and therefore
believe that relational autonomy [10], as opposed to individual autonomy, is more justified.
Conclusion
So indeed, what is the scope of autonomy in medical practice? We have explored methods of thought
such as principlism and casuistry, different ideologies on autonomy and several specific medical ethics
cases in order to be able to answer this question. We can now see that autonomy is indeed extremely
far-reaching and has many boundaries, but what is most interesting of all is that it is the same things
that make autonomy far-reaching which can equally limit it. From a legal, cultural, and humanitarian
perspective, these are the factors which enable as well as limit autonomy. We saw that in the case of
the pregnant woman, that the principles of guidance from a governing body such as the GMC were

facilitating her autonomy, adding strength to her choice which she may not have had if those guidelines
were not there. However, in the case of the woman requesting a mastectomy, she had no right to
demand to have that procedure from a legal position or from any documented regulatory authority like
the GMC, even if she had reasons that justified her wishes. Culturally, depending on the part of the
world you are from, your autonomy can be viewed at the highest esteem, or indeed it may be an issue
not even worth discussing. Medical procedures are done on humane grounds to help alleviate the
patient’s illnesses whilst respecting his/her autonomy. In the case of Dax Cowart, it was considered
humane to treat the patient against his wishes in order to keep him alive, despite the pain he was in,
hence compromising his autonomy. Humanitarianism is also rightly considered as a boundary for
autonomy whenever it causes harm to another individual. The scope of autonomy consists of all these
concepts which give will to power to individuals, whilst simultaneously setting in place limitations.
In terms of the four principles, it could be posited that autonomy should be regarded at a higher
standard to the other three principles and be the principle that guides the others in order to make a
decision. In a doctor-patient relationship, the balance of power is naturally shifted towards the doctor. If
this position of power was to be abused and the patient’s autonomy disrespected then this can damage
the doctor-patient relationship and give the patient a sense of distrust towards the doctor. If this
attitude was to become widespread, then this would lead to a general lack of trust in the medical
profession as a whole, undermining the health care system, and reflecting badly on those who try their
best to ensure autonomy is maintained. That is why if the autonomy of a patient is held in a high regard,
to the extent that it is leading the other three principles, but not in an absolute sense, the balance in the
doctor-patient relationship can be restored, giving a greater sense of equality to the patient. Using this
approach doctors could have a clear idea of the first principle that should be looked at, and from there
relate autonomy to the other principles. It is often said that there is no right and wrong answer when it
comes to ethics, and this at times can make the process of coming to a suitable resolution all the more
challenging
References
1. Gillon, R, Medical ethics: four principles plus attention to scope, BMJ, Volume 309, Number 6948>309:184, July
1994.
2. Christman, J, Autonomy in Moral and Political Philosophy, The Stanford Encyclopaedia of Philosophy.
3. Garrett T, Baillie W, Garret R, Health Care Ethics (5th Edition).
4. Beauchamp, T, Childress, J, Principles of Biomedical Ethics (7th Edition). Oxford University Press, 2012.
5. Ross, WD, The Right and the Good, Hackett Pub Co Inc, July 1988
6. Secondary source: Parker M. Dickinson D. The Cambridge Medical Ethics workbook. CUP, 2001
Primary source: Kant, I. Groundwork of the Metaphysics of Morals.

7. Secondary source: Parker M. Dickinson D. The Cambridge Medical Ethics workbook.
CUP, 2001
Primary source: Mill, JS. Utilitarianism: On Liberty.
8. Re B (Adult, refusal of medical treatment) [2002] 2 All ER 449 Right of a patient who has capacity to refuse life-
prolonging treatment.
9. St George's Healthcare Trust v S (No 2). R v Louise Collins & Others, Ex Parte S (No 2) [1993] 3 WLR 936.10.
Parker M. Dickinson D. The Cambridge Medical Ethics workbook. CUP, 2001.
10. Parker M. Dickinson D. The Cambridge Medical Ethics workbook. CUP, 2001
Public Health Challenges in India 2013
Dhairya Lakhani (3rd
M.B.B.S.), Dr. Sunil Kumar (M.D.), Shruti Gohel (3rd
M.B.B.S.) & Dr. Supriya Kumar
(M.D.)
Correspondence - Dhairya Lakhani: [email protected]
COMMENTARY PIECE
Key Words: Health, India, Vision 2020, public private partnership
Background
In the din of a slowing economy, falling rupee, rampaging inflation, and incessant political
manoeuvrings, India’s list of challenges continues to grow. Of all these challenges, there is one that
seems insurmountable already, and worse, could soon end up becoming a calamity, aggravating the
suffering of hundreds of millions of Indians. This challenge relates to the provision of affordable,
accessible, and accountable healthcare to every single citizen of India. (1)
On just about every single measurable indicator of healthcare infrastructure, India is rapidly
deteriorating. It is easy to mistake the gleaming glass façade of modern hospitals that have come up in
the top 15-20 cities of India as a sign of India’s improving healthcare infrastructure. It is easier to get
carried away by the frequent appearance of a few celebrity doctors in the newspapers and assume that
the nation’s healthcare is in good hands. Unfortunately, the facts don’t bear this out. (2) Only 48 per
cent of the 1.35 million beds are functional and relevant and about 65 per cent of these are located in
the top 20 cities. (1)
Stark Ground Reality
It is anyone’s guess as to how many qualified doctors the country has. The most optimistic estimates put
this number at less than 5 lakh. More than 65 per cent of the operational beds are in the private sector,
and more than 80 per cent of the spending on healthcare in India is accounted for by the private sector
even though over 65 per cent of India’s population is below the poverty line or living just on its fringes.
No wonders that on an all-India basis, an Indian has to travel an average of 77 km to access basic
secondary care services. (3)
The above challenges are exacerbated by the fact that while the country is still struggling to bring
infectious diseases under control, the incidence of non-communicable diseases is also on the rise. . First,
with increasing life expectancy the epidemiological transition points towards greater incidence of non-

communicable or lifestyle diseases. This goes hand in hand with a continuing serious problem of
communicable and preventable diseases. Second, there is a lot of variation in the public provisioning of
health care - a state subject. Poor states are hard pressed for funds. Third, India is an exception across
countries in that nearly four-fifths of its health care expenditure is out-of pocket. Coupled with the
burgeoning growth of unregulated private sector care-givers, this has serious implications. These three
issues open up a number of policy questions on access to, utilisation and quality of health care.
However, the most important among them is the one, which will specifically address the concerns of the
poor and the sick. Heart diseases, diabetes, and cancer are expected to show a combined average
decadal growth of 47 per cent in future. This will add to the demand for diagnostic, therapeutic and
research facilities in tertiary care specialties. (4)
Considering some of the anticipated trends of population and trained manpower deficits in healthcare
delivery, India needs strategies that are customised to address its needs and in alignment with the
financial resource available. This calls for rigorous participation from both the public and the private
sectors. (5)
The Path Ahead
One such promising solution — though one that has performed below expectation so far — is the Public
Private Partnership (PPP) model. If implemented efficiently, it has the potential to plug many gaps in
the access to basic healthcare. PPP models should be planned and executed to leverage the expertise of
private partners in infrastructure design, strong process orientation and ‘safe’ care delivery methods.
The training of paramedical staff and doctors on specific care protocols and patient safety practices can
be devised and deployed with the support of private healthcare groups and NGOs. Medical equipment
firms can join hands with the government in provisioning IT-enabled point-of-care data management
systems for better disease prevention and immunisation tracking. Diagnostic services at all
district/identified government hospitals can be improved by engaging private players to develop
processes for effective utilisation. (2)
Information technology is one area which, if put to optimal use, can bring immense improvements in
the way we diagnose and treat medical conditions. There are many innovative interventions in the field
of mobile and electronic healthcare that have been successful in other developing markets that could be
replicated in India. New concepts like doctor on web/phone are increasingly gaining ground and can go a
long way in primary and secondary healthcare delivery. (4)
There is also an urgent need to relook at the business models that hospitals have adopted so far. The
temptation to set up world-class tertiary and quaternary multi-specialty hospitals is understandable —
and India does need them — but then how you prioritise the allocation of the available capital is also
important. (5)

Fortunately, there are many promising initiatives in the right direction — in setting up low cost, single
specialty or even a single micro — specialty primary and upgraded secondary care facilities, and setting
up of low capital day-care centres.
Providers are waking up to the need of investing in healthcare facilities that are asset-light, low on
investment and manpower requirements, and easy to scale up and replicate. Corporate players which
have so far concentrated mainly on achieving high occupancies in large multi-specialty hospitals are
venturing into formats that involve lower in-patient hospital stay, higher bed turnover and lower
operational costs. (4)
Role of Government
The government, on its part, needs to support these efforts by providing subsidies on land, and medical
equipment and tax benefits to professionals working in such organisations, especially in rural areas. It
should also take a cue from such low-cost models and consider setting up short stay medical centres at
the district/identified government hospitals that would relieve the pressure on some of the key nodal
hospitals and allow minor surgical procedures to be carried out on time and perhaps reduce the cost of
delivering care as well.
The public sector can take a slew of other measures to strengthen primary healthcare infrastructure.
Here are some pointers. Pharmacies in all government hospitals should stock generics and supply chains
should be re-vitalised to prevent stock-outs that force patients to buy medicines from private
pharmacies. There can be measures to integrate primary health centres with district hospitals to allow
for continuity of care. Child care and women’s care services should be strengthened by enhancing the
availability of trained professionals at primary care clinics and district hospitals. Nodal hospitals of the
government should be identified and equipped with strong emergency services for timely critical care.
The number of medical and paramedical colleges in under-served areas should be increased.
Another probable solution, though mired in controversy, is bringing changes in the training of
healthcare manpower and staffing patterns in hospitals. This should be directed to reduce the number
of crises that require a doctor’s intervention. Hospitals can benefit from a broad range of training
programmes to create workers with a wider array of skills such as physician assistants, nurse
practitioners and diagnostic medical sonographers. This will not only help tackle the issue of the
shortage of trained doctors, but also free up doctors to devote their skill to more complex tasks.
Interventions along these lines have been undertaken in some states like Tamil Nadu where nurses were
trained by the government and the number of positions for them increased in primary health centres.
However, such examples are sporadic and need more vigour to be duplicated in other states.
Deepening connectivity and sharing knowledge can help reduce medical errors and improve care
quality, for example through drug interaction alerts, greater use of evidence-based care protocols and
new capabilities in managing population care, which increase the potential for preventive and low cost
care for chronic conditions. (1)

Conclusion
As a formidable global economic power, accessible quality healthcare can be a key competitive strength
for India. There are three milestones on the journey towards connected healthcare which need to be
achieved – Healthcare IT adoption, Health Information Exchange and Insight-driven Healthcare. It is
imperative for the nation to relook at the current budget outlays, policies and the commitment to
deliver on this comprehensively.
References
1. R.Srinivisan-Health care In India Vision 2020.
2. Katherine E.Bliss-Key Players in Global Health-How Brazil Russia India China and South Africa are
influencing the game A report of the CSIS Global Health Policy Centre
3. Five years of NRHM 2005-2010, Ministry of Health & Family Welfare
4. Annual Report of Ministry of Human Resource Development (MHRD), 2009-10.
5. Morbidity, Health Care and The Condition of the Aged, NSS 60th Round, March 2006

Electroencephalography – An Overview
Holly Duncan (University of Dundee), Kate Spillane (PhD, MRCP), Ian Morrison (PhD, FRCP)
Correspondence – Holly Duncan: [email protected]
ABSTRACT
EEGs are commonly requested by physicians in medical wards for patients with altered conscious levels
and also in the outpatient setting for investigation of seizures. This article seeks to explain how EEG is
performed and explore the correct indications for its use.
Key Words: Electroencephalography; EEG; Indications
Electroencephalography
Electroencephalography (EEG) is the electrical study of brain activity. It was first used on humans by the
German psychiatrist, Hans Berger, in 1929 to examine electrical activity within the brain’s cortical grey
matter1 and it was later discovered that aberrant cortical activity is seen in many neuro-pathologies. It is
especially relevant in seizure disorders, in particular epilepsy. It is a non-invasive, painless procedure
that can be performed in both outpatient and inpatient settings, and usually lasts a minimum of 35-45
minutes2.
EEG & Loss of Consciousness
EEGs have a relatively low sensitivity for diagnosing epilepsy at 25-56%. In a study of over 13,000
military personnel with no history of significant illness or head injury and normal physical examinations,
0.5% had frankly epileptiform discharges on EEG. Only one of these men went on to develop clinical
epilepsy3.
Sam et al reported that epileptic EEG discharges can be seen in up to 12.3% of the community who had
no history of unprovoked seizure or epilepsy. Many of these patients had an underlying acute or
progressive cerebral disorder4, and this highlights that epileptiform discharges are present in a number
of pathologies other than epilepsy. Likewise, abnormal cortical activity is relatively common, especially
in the elderly, migraine patients, those with psychotic illness and those on psychotropic medication5.
To add further confusion, a normal EEG does not exclude a diagnosis of epilepsy. Definite epileptiform
abnormalities are seen in only 29-38% of adults with epilepsy on their first EEG recording5.

The EEG should not therefore be used in isolation to diagnose epilepsy, where history is most important,
nor should it be used to diagnose unexplained losses of consciousness. Performing the investigation in
cases of probable syncope in particular incurs the risk of a false positive result and subsequent
misdiagnosis6.
Specific Indications for EEG in Epilepsy
Classification of Epilepsy
Classification of seizure type is essential for offering prognosis and planning the correct treatment. In
particular, it is helpful to distinguish between generalised and focal onset epilepsies, where certain
medications (e.g. carbamazepine) are usually avoided in generalised epilepsies but not focal onset
epilepsies7.
Furthermore, EEG can facilitate the localisation of an epileptogenic focus and indicate localised
structural pathology underlying the seizure disorder, which is helpful if the patient is being considered
for resective surgery to cure their epilepsy1, 5, 8, and 9
.
Triggers
If stress testing during the EEG identifies photosensitive epilepsy, the patient can manage their
condition by avoiding triggers such as strobe lighting1.
Use of EEG in Intensive Care
The use of continuous EEG (cEEG) recording in Intensive Care Units (ICU) can now provide prompt and
therapeutically important data regarding cerebral function in a cohort of patients who may have only
subtle or no clinical signs10, 11
.
Investigating Periods of Altered Consciousness
EEG is important in the management of convulsive status epilepticus: for monitoring seizure activity and
assessing the response to IV treatment. This is particularly important in intensive care where
convulsions may be masked by sedation, paralysis and antiepileptic drugs5, 8, 10, and 12
.
Whilst convulsive status epilepticus should be clinically evident, a prolonged period of altered
consciousness could be due to non-convulsive status epilepticus (NCSE), which can be difficult to
distinguish from other confusional states. Privitera et al urge that all patients with persistent,
unexplained, altered consciousness receive immediate EEG13
to exclude NCSE and, where appropriate,
allow the prompt initiation of appropriate treatment8. Hirsch reports that the difference in mortality
between NCSE diagnosed at 30 minutes compared with delays of over 24 hours soars from 36% to 75%,
respectively14
.

Other Indications for EEG
There are many reported indications for EEG, including prognosticating head trauma, diagnosis of
encephalitis and dementia, measuring the depth of sedation and predicting the outcome and
management of patients in a coma of other reasons2, 10
. However, the EEG is not specific in many of
these conditions and should only be used to support diagnosis8.
Procedure
Electrodes are positioned on the scalp in an arrangement called a montage. They are placed according
to the International 10/20 System, which is based on the identification of anatomical landmarks such as
nasion and inion and the preauricular points. Electrodes are then placed at consecutive intervals fixed
distances from these points in steps of 10 or 20%; thereby allowing for variations in head size15
. These
points are labelled as Frontal pole (Fp), Frontal (F), Central (C), Parietal (P), Occipital (O) and Temporal
(T). Odd numbers denote points over the left hemisphere and even numbers the right, whilst ‘z’ denotes
zero and identifies electrodes in the midline16
. The potential difference recorded between pairs of
electrodes is amplified and displayed on a monitor2, 17, and 18
. The recorded activity is measured in
microvolts18
and represents the postsynaptic potentials of vertically orientated pyramidal cells within
the cerebral cortex17
.
Routine EEGs now commonly include so-called activation procedures to enhance the diagnostic
sensitivity. During activation, EEG recordings are made when a patient undergoes hyperventilation or
exposure to flashing lights at various frequencies (photic simulation). Binnie et al report that a waking
EEG of at least 30 minutes duration, with hyperventilation and photic stimulation, will demonstrate
inter-ictal epileptiform discharges (IEDs) in about 50% of adults with epilepsy8.
National Institute for Clinical Excellent (NICE) guidelines on the diagnosis and management of epilepsy
recommends that photic stimulation and hyperventilation should remain part of the standard EEG
assessment. The patient must however be warned that such procedures may induce a seizure and they
have a right to refuse6.
Sleep and sleep deprivation can also increase the likelihood of IEDs being recorded as some wave-forms
are more evident during sleep, and tiredness can trigger seizures. Sleep recordings are helpful in
identifying epileptiform discharges in patients who have normal EEGs in the waking state, and so can aid
epilepsy classification8. In particular, there is evidence that sleep deprivation activates IEDs in idiopathic
generalised epilepsies1.
NICE recommend that a sleep EEG is performed when routine EEG has not contributed to a diagnosis or
classification of epilepsy6.

Interpreting EEG Results
Alpha
Waves
8-13Hz rhythm is seen symmetrically and posteriorly when the eyes are closed, this activity is
attenuated in drowsiness and is blocked with eye opening. Alpha waves are normal in adults2, 17 and 18
.
Beta Waves
>13Hz activity is seen symmetrically and frontally in healthy adults. This is unaffected by eye opening
but may be absent of reduced in areas of cortical damage16
.
Theta Waves
4-7Hz rhythm is normal in children up to 13 years of age16
. It is a normal finding in drowsy adults and
becomes more apparent in light sleep. Presence of theta waves in an alert adult can indicate brain
dysfunction20
.
Delta Waves
<4Hz rhythm is normal in infants under 1 year16
. They are only normal in adults in moderate to deep
sleep and their presence in an alert adult suggests brain dysfunction20
.
Theta and delta rhythms are both seen in children and young adults with frontal and temporal
predominance and usually disappear in adulthood.
Generalised spike-wave activity is commonly seen in patients with typical absence epilepsy and may also
be seen in some generalised epilepsy syndromes, whereas focal IEDs are suggestive of partial seizure
FIGURE 3: waveforms seen on EEG. Reproduced with permission from: Medscape Reference. Jan
2013, available at: http://emedicine.medscape.com/article/1139332-overview19.

disorders such as temporal lobe epilepsy17
. Binnie et al observed that hyperventilation provokes spike-
wave activity in patients with absence seizures so consistently that the lack of this finding in an
untreated person who hyperventilates efficiently must cast doubt on the diagnosis8.
Other changes often seen on EEG include generalised slowing, indicating an encephalopathic state, and
focal excess slow activity indicating a unilateral structural lesion.
Conclusion
EEG is a commonly ordered investigation in hospital settings, often for the wrong reasons5. This leads to
misdiagnosis with potentially significant adverse outcomes. It is important that patients are only
referred for EEG in the correct clinical context i.e. to confirm clinical findings from thorough history and
examination.
Learning Points
• EEG is used to monitor cortical activity
• Activation procedures increase the diagnostic sensitivity of EEG
• When used in the correct context, EEG can be used to support a clinical diagnosis of epilepsy, classify
some seizure syndromes and identify epileptogenic foci
• It should not be used in isolation to diagnose epilepsy (in cases of suspected seizure or unexplained
loss of consciousness)
• EEG can be useful in the diagnosis and management of encephalopathies, status epilepticus and
confusional states
References
1. Smith S.J.M., EEG in the diagnosis, classification and management of patients with epilepsy. J Neurol Neurosurg
Psychiatry 2005; 76(2):ii2-ii7
2. EEG. Updated 2012 Jan 26th, cited 2012 October 15th. Available from
http://www.nhs.uk/conditions/EEG/Pages/Introduction.aspx
3. Gregory R. P., Oates T., Merry R. T. G. Electroencephalogram epileptiform abnormalities in candidates for
aircrew training. Electroencephalogr clin neurophysiol. 1992;86(1993):75-77
4. Sam M. C., So E. L. Significance of epileptiform discharges in patients without epilepsy in the community.
Epilepsia. 2001;42(10):1273-1278
5. Fowle A. J., Binnie C. D. Uses and Abuses of the EEG in Epilepsy. Epilepsia. 2000.41(3):S10-S18

6. National Institute for Health and Clinical Excellence. The epilepsies: the diagnosis and management of the
epilepsies in adults and children in primary and secondary care. 2012. London: National Institute for Health and
Clinical Excellence. CG137
7. Joint Formulary Committee. British National Formulary (online) London: BMJ Group and Pharmaceutical Press,
http://www.medicinescomplete.com, Accessed on 05/11/2012
8. Binnie C. D., Stefan H. Modern electroencephalography: its role in epilepsy management. Clin Neurophysiol.
1999;110(1999):1671-1697
9. Noachtar S., Rémi J. The role of EEG in epilepsy: A critical review. Epilepsy Behav. 2009;15(2009):22-33
10. Kennedy J. D., Gerard E. E. Continuous EEG Monitoring in the Intensive Care Unit. Curr Neurol Neurosci Rep.
2012;12:419-428
11. Scheuer M. L. Continuous EEG Monitoring in the Intensive Care Unit. Epilepsia. 2002;43(3):114-127
12. Bleck T. P., Faam F.C.C.M. Status Epilepticus and the Use of Continuous EEG Monitoring in the Intensive Care
Unit (Review). Continuum (Minneap Minn).2012;18(3):560-578
13. Privitera M. D., Strasburg R. H. Electroencephalographic monitoring in the emergency department. Emerg Med
Clin North Am. 1994;12(4):1089-1100
14. Hirsch L. J. Continuous EEG Monitoring in the Intensive Care Unit: An Overview. J Clin Neurophysiol.
2004;21(5):332-340
15. Herwig U., Satrapi P., Schönfeldt-Lecuona C. Using the International 10-20 EEG System for Positioning of
Transcranial Magnetic Stimulation. Brain Topogr 2003;16(2):95-99
16. EEG: Introduction. Cited 2012 Oct 15th. Available from
http://www.medicine.mcgill.ca/physio/vlab/biomed_signals/EEG_n.htm
17. Hauser S., Kasper D. Harrison’s Neurology in Clinical Medicine. USA: McGraw-Hill, 2006
18. Lindsay W., Bone I., Fuller G. Neurology and Neurosurgery Illustrated 5th Edition. London: Churchill Livingstone,
2010
19. Waveforms seen on EEG. Cited Jan 2013, Available at: http://emedicine.medscape.com/article/1139332-
overview
20. Recording EEGs. Cited 2012 Oct 15th. Available from http://www.ebme.co.uk/arts/eegintro/eeg5.htm
21. Scottish Intercollegiate Guidelines Network. April 2003. Diagnosis and Management of Epilepsy in Adults: SIGN
Guideline 70, Edinburgh: Scottish Intercollegiate Guidelines Network
22. Ginsberg L. Neurology Lecture Notes 8th Edition. UK: Blackwell Publishing 2005
23. Scheepers B., Clough P., Pickles C. The misdiagnosis of epilepsy: findings of a population study. Seizure.
1998(7): 403-406
24. Kumar and Clark’s Clinical Medicine. 7th Edition. UK: Saunders Elservier 2009

25. Oommen K.J., Gilson G. E., Nelson J. W., Couch J. R. A study to determine the accuracy of a computerized
algorithm for interpretation of EEGs. J Okla State Med Assoc. 2001 Sept. 94(9):400-402
26. Bonnett L. J., Tudur-Smith C., Williamson P. R., Marson A. G. Risk of recurrence after a first seizure and
implications for driving: further analysis of the Multicentre study of early Epilepsy and Single Seizures. BMJ.
2010;341:c6477
27. Muniz J., Benbadis S. R. Repeating video/EEG monitoring: Why and with what results? Epilepsy Behav.
2010;18(2010):472-473
28. Zivin L., Marsan C. A. Incidence and prognostic significance of “epileptiform” activity in the EEG of non-epileptic
subjects. Brain. 1968;91(4):751-778
29. EEG and EP Lab. Updated 2012 Sept 6th; cited 2012 Oct 15th. Available from
http://www.medicine.virginia.edu/clinical/departments/neurology/facilities/outpatient/EEG_EP_lab-page
30. Salinsky M., Kanter R., Dasheiff R. M. Effectiveness of multiple EEGs in supporting the diagnosis of epilepsy: an
operational curve. Epilepsia. 1987;28(4):331-334
31. Doppelbauer A., Zeitlhofer J., Zifko U., Baumgartner C., Mayr N., Deecke L. Occurrence of epileptiform activity
in the routine EEG of epileptic patients. Acta Neurol Scand. 1993;87(5):345-352
32. History: From EEG to Quantitative EEG (QEEG). Accessed 2012 Oct 18th. Available from
http://www.brainclinics.com/history-of-the-eeg-and-qeeg
33. Tips on reading and reporting the EEG. Accessed 2012 Oct 18th. Available from
http://elsevierhealth.com/media/us/samplechapters/9780750674768/9780750674768.pdf
34. Rijsdijkl M., Leijten F.S.S., Slooter A.J.C. Continuous EEG monitoring in the Intensive Care Unit. Neth J Crit Care.
2008;12(4):157-162
35. Abend N.S., Dlugos D.J., Hahn C.D., Hirsch L.J., Herman S.T. Use of EEG Monitoring and Management of Non-
Convulsive Seizures in Critically Ill Patients: A Survey of Neurologists. Neurocrit Care. 2010;12:382-389
36. Praline J. et al. EEG d’urgence : indications réelles et résultats Emergency EEG: actual indications and results.
Neurophysiologie clinique. 2004 ;34:175-181
37. Young G.B., Campbell V.C. EEG monitoring in the intesive care unit : pitfalls and caveats. J Clin Neurophysiol.
1999;16(1):40-45
38. Vespa P.M., Nenov V., Nuwer M.R. Continuous EEG monitoring in the intensive care unit: early findings and
clinical efficacy. J Clin Neurohysiol. 1999;16(1):1-13
39. Deyne C.D., Struys M., Decruyenaere J., Creupelandt J., Hoste E., Colardyn F. Use of continuous bispectral EEG
monitoring to assess depth of sedation in ICU patients. Intensive Care Med. 1998;24(12):1294-1298
40. Velly L., Pellegrini L., Brude N. EEG en réanimation : quelles indications, quel matériel? Ann Fr Anesth Reanim.
2012 ;31(6) :e145-e153

Frailty: What does it mean for Clinical Care Provision?
Ciarán Reynaud (Year 3 MB BCh BAO, Trinity College Dublin), Tomás McHugh (Year 3 MB BCh BAO,
Trinity College Dublin), Román Romero-Ortuño (Lic Med, MSc, MRCP (UK), PhD; Department of
Medical Gerontology, Trinity College Dublin)
Correspondence – Román Romero-Ortuño: [email protected]
ABSTRACT
This article forms part of the Approaching Geriatric Patient series. Speaking to medical and nursing
students, it is common to see and be asked to assess frail older adults on medical and surgical wards.
However, there is great uncertainty about how these older adults should be managed. It is common that
students ask what aspects of frail patients’ care should and could be different compared to other
patients to improve quality of life and optimise clinical care for this increasing patient group. The
objectives of this review are: (1) to briefly outline the main operationalisations of frailty that are suitable
for clinical care provision; (2) to review the use of frailty tools in ‘aggressive’ therapeutic areas such as
surgery and oncology; (3) to review the evidence for the role of frailty in the assessment of traditional
cardiovascular risk factors and the more appropriate prescribing of medications; and (4) to make a case
for frailty as a screening tool for access to evidence-based comprehensive geriatric assessment (CGA)
services.
Key words: Frail elderly; risk assessment; individualized medicine; evidence-based medicine.
Introduction
‘Frailty’ is a commonly used term outside and inside Medicine. The definition of frail adjective from the
Cambridge Advanced Learner’s Dictionary & Thesaurus
(http://dictionary.cambridge.org/dictionary/british/) is:
‘Weak or unhealthy, or easily damaged, broken, or harmed’
Indeed, frailty is about vulnerability to poor resolution of homoeostasis after a stressor event and is a
consequence of cumulative decline in many physiological systems during a lifetime.1
Campbell & Buchner defined frailty as ‘a condition or syndrome which results from a multi-system
reduction in reserve capacity to the extent that a number of physiological systems are close to, or past,
the threshold of symptomatic clinical failure; and as a consequence the frail person is at increased risk of
disability and death from minor external stresses’.2

In the context of clinical care provision, frail older adults represent a challenge to clinicians because they
usually present with an increased burden of symptoms, are medically complex, and less able to tolerate
interventions of any kind (more prone to complications). In addition, patients who are frail have more
subtle signs and symptoms that can be easily overlooked.
In clinical care provision, some interventions can be more ‘aggressive’ than others and hence be more
complication-prone. Frail (vulnerable) adults are more likely than ‘robust’ adults to suffer complications
from a given medical intervention. While ‘fit’ people are resilient and ‘frail’ people are vulnerable,
chronological age per se cannot tell where a person is along the ‘fitness-frailty’ spectrum3, 4
, due to the
great biological heterogeneity of the population of older people.5 Frailty more closely relates to the
biological than to the chronological age of individuals.6, 7
The measurement of frailty as a surrogate for vulnerability in healthcare delivery is therefore of utmost
importance in a current world characterised by an ageing population and continuing efforts to not only
prevent and minimise iatrogenic events, but also concentrate the use of public resources in
interventions for older people that are effective and evidence-based.
The objectives of this review are: (1) to briefly outline the main operationalisations of frailty that are
suitable for clinical care provision; (2) to review the use of frailty tools in ‘aggressive’ therapeutic areas
such as surgery and oncology; (3) to review the evidence for the role of frailty in the assessment of
traditional cardiovascular risk factors and the more appropriate prescribing of medications; and (4) to
make a case for frailty as a screening tool for access to evidence-based comprehensive geriatric
assessment (CGA) services.
As an intuitive concept, frailty (i.e. vulnerability) is well recognised clinically. However, the objective
measurement (i.e. operationalisation) of the concept is still a matter of debate and there is no agreed
gold standard. Instead, there are several definition approaches, two of the most popular being the
frailty phenotype (i.e. frailty as a syndrome) and the frailty index (i.e. frailty as a state). Rather than being
competitive or mutually exclusive, both approaches are actually complementary and suitable for
different purposes or scenarios.8
A Common Operationalisation of Frailty: The Frailty Phenotype
According to the phenotypic approach, frailty is defined as a clinical syndrome in which three or more of
the following criteria are present: unintentional weight loss, self-reported exhaustion, weakness, slow
walking speed, and low physical activity.9, 10
This approach defines two additional states: pre-frail (i.e.
one or two criteria present) and non-frail (i.e. none of the criteria present). According to the biological
theory underpinning the frailty phenotype, co-morbidity is a risk factor for frailty, and frailty is a
precursor of disability.11
The original validation of this approach by Fried et al. included significant
associations with incident disease, hospitalization, falls, disability and mortality, independently of

chronological age.10
Table 1 shows the original frailty phenotype criteria as defined in the Cardiovascular
Health Study.10
Table 1. Phenotypic frailty criteria.10
Positive for frailty phenotype: ≥3 criteria present; intermediate
or prefrail: 1 or 2 criteria present. Robust or non-frail: no criteria present.
• Weight loss: unintentional weight loss of more than 10 pounds (4.5 Kg) in the last year.
• Exhaustion: for at least 3 days in the last week, “I felt that everything I did was an effort” and/or
“I could not get going”.
• Physical Activity: Based on the short version of the Minnesota Leisure Time Activity
questionnaire.12
Men: Those with Kcals of physical activity per week <383 are frail by this criterion.
Women: Those with Kcals per week <270 are frail by this criterion.
• Walk Time, stratified by gender and height:
Men Cut-off for Time to Walk 15 feet (4.6 m) criterion for frailty
Height ≤173 cm ≥7 seconds
Height >173 cm ≥6 seconds
Women
Height ≤159 cm ≥7 seconds
Height >159 cm ≥6 seconds
• Grip Strength, stratified by gender and body mass index (BMI) quartiles:
Men Cut-off for grip strength (Kg) criterion for frailty
BMI ≤24 ≤29
BMI 24.1–26 ≤30
BMI 26.1–28 ≤30
BMI >28 ≤32
Women
BMI ≤23 ≤17
BMI 23.1–26 ≤17.3
BMI 26.1–29 ≤18
BMI >29 ≤21
Because surrogates for individual frailty phenotype criteria are possible 13
, there have been attempts to
provide healthcare practitioners with phenotypic frailty assessment tools that do not require post-hoc
calculations and can be scored immediately after an individual assessment. An example is the Frailty
Instrument for Primary Care of the Survey of Health, Ageing and Retirement in Europe (SHARE-FI) 14
. This
tool is based on a modified phenotypic approach and includes two web-based frailty calculators (one for
each gender) that are freely accessible on BMC Geriatrics (http://www.biomedcentral.com/1471-
2318/10/57/additional). Their use is intended for community-dwelling adults aged 50 and over.

Translated versions of the calculators can be accessed on https://sites.google.com/a/tcd.ie/share-frailty-
instrument-calculators/. SHARE-FI has been validated against incident disability 15
and mortality.16
In an
observational study, a recent study showed that people identified as frail by SHARE-FI had worse
physical performance scores, more history of falls, more medication burden, and were more often
referred for ongoing assessment and rehabilitation 17
. An advantage of SHARE-FI is that, on average, it
takes about 6.5 minutes to administer (http://www.uakron.edu/dotAsset/8b117eba-ec49-4e57-9495-
fe41fcfbd995.pdf).
Another Common Operationalisation of Frailty: The Frailty Index
A way to operationalise frailty is by considering it as a state and counting in an individual the number of
deficits that he/she has accumulated from a given list (of usually 30 or more potential deficits). Deficits
are widely defined as symptoms, signs, diseases and disabilities that accumulate with age.18
The
number of counted deficits divided by the number of deficits considered results in a score called frailty
index (FI), which ranges from 0 (none of the deficits present) to 1 (all deficits present).
The construct validity of the FI is examined through its relationship to chronological age, and its criterion
validity is examined in its ability to predict mortality 19
, and in relation to other predictions including
disability and use of healthcare resources 20
. Table 2 and Figure 1 exemplify a 40-item FI validated in the
Survey of Health, Ageing and Retirement in Europe (SHARE).20
Table 2. 40 items for a frailty index in SHARE.20
Difficulties:
bathing or
showering
Difficulties: lifting
or carrying weights
Moderate or
vigorous physical
activity: hardly ever,
or never
High blood pressure Hip or femoral
fracture
Difficulties: dressing
Difficulties:
shopping for
groceries
Diminution in the
desire for food
and/or eating less
than usual
Heart attack
Impaired orientation
to date, month, year
and day of week
Difficulties:
getting up from
chair
Difficulties:
doing work around
the house or garden
Poor
self-perceived
health
Stroke Body mass index
(Kg/m2) deficit
Difficulties:
walking across a
room
Difficulties:
preparing a hot
meal
Long-term illness Cancer Breathlessness
Difficulties:
eating, cutting up
food
Difficulties:
taking medications Fatigue Diabetes Falls

Difficulties: reaching
or extending arms
above shoulder
Difficulties:
managing money Sad or depressed Arthritis Fear of falling
Difficulties:
using the toilet
Difficulties:
walking 100 metres Lack of enjoyment Chronic lung disease
Dizziness, faints or
blackouts
Difficulties: climbing
one flight of stairs
Difficulties:
getting in or out of
bed
Hopelessness Osteoporosis Grip strength (Kg)
deficit
Figure 1: Association of the SHARE frailty index with mortality (mean follow up: 2.4 years) by age decade
and tenth of FI, in SHARE wave 1 (men and women combined, total N = 20,547). The number on each
coloured cell represents the mortality rate (%) for that cell.
In terms of individual risk stratification, the FI is a continuous variable and primarily does not classify
people as frail or non-frail but rather assigns a score based on health status. However, Rockwood et al.
proposed FI cut-off points to define phenotypical population subgroups with increasing levels of frailty.
For example, in one of their studies they proposed FI ≤ 0.08 as ‘non-frail’, FI ≥ 0.25 as ‘frail’, and the rest

as ‘pre-frail’.21
In another of their studies, they proposed FI ≤ 0.03 as ‘relatively fit’, 0.03 < FI ≤ 0.10 as
‘less fit’, 0.10 < FI ≤ 0.21 as ‘least fit’, 0.21 < FI ≤ 0.45 as ‘frail’, and FI ≥ 0.45 as ‘most frail’.22
Age-specific
FI cut-offs have also been proposed.23
Frailty in Surgery
Surgeons and anaesthetists accept that working with frail patients is a common but challenging
scenario.24
Current surgical decision-making can be subjective (‘eyeball’25
) and often misjudges a
patient’s physiologic state.26
As a marker of low physiological reserve and vulnerability, frailty has
emerged as an independent predictor of morbidity and mortality after surgery.27-29
Crucially, frailty
improves the predictive power of ‘conventional’ surgical risk scores.30-32
To date, frailty tools have been
successfully validated (as more accurate approaches to risk stratification) in many types or surgery,
including cardiac32-35
, thoracic36
, gastrointestinal37-40
, vascular41, 42
, head and neck43
, kidney transplant44
,
and orthopaedic45
. Objective frailty assessment tools may have implications in preoperative decision
making in selecting patients who optimally benefit from surgery46
, and may prove beneficial when
weighing the risks and benefits of surgery, allowing objective data to guide surgical decision-making and
patient counselling.47
Frailty in Oncology
Frailty has also emerged as a potential aid in the vulnerability assessment of older patients undergoing
oncology (e.g. chemotherapy) treatments. Indeed, a comprehensive geriatric assessment (CGA)
approach, which also evaluates elements of frailty, may be of great interest for those oncologists who
want to identify older patients likely to develop severe toxicity and severe side effects in response to
aggressive treatment.48, 49
The use of ‘frail-friendly’ (i.e. less aggressive) chemotherapy regimens (i.e.
aimed at control of further disease progression rather than maximum tumour shrinkage) may benefit
the more vulnerable patients, lowering their rates of premature withdrawal, complications and early
mortality50
, in addition to improving their quality of life. In that light, oncology trials tailored for the
elderly or frail are needed51
, and examples of frailty-tailored oncology treatment approaches are already
available in lymphoma52
colorectal cancer53
, and gynaecologic oncology54
.
Frailty as a Framework for re-thinking ‘traditional’ Medical Risk Factors
In non-frail adults, a substantial body of evidence has provided substantial insight into the epidemiology
and risk factors of cardiovascular disease.55
However, the study of these ‘traditional’ risk factors in frail
populations is providing very interesting paradoxes. For example, recent evidence suggests that
hypertension may be beneficial in frail people older than 85 years 56
. A study showed that the
association between BP and mortality varies by walking speed: among faster walkers, those with
elevated systolic BP (>/= 140 mm Hg) had a greater adjusted risk of mortality compared with those

without, but among slower walkers, neither elevated systolic nor diastolic BP (>/= 90 mm Hg) was
associated with mortality; in participants who did not complete the walk test, elevated BP was strongly
and independently associated with a lower risk of death.57
Low walking speed, inability to walk, or recurrent falling, can all be markers of frailty and underlying
complex systems.58
Another recent study showed that antihypertensive medications were associated
with an increased risk of serious fall injuries, particularly among those with previous fall injuries and
multiple chronic conditions.59
The Leiden 85-plus study has shown that a decreasing trend in systolic blood pressure (SBP) between 85
and 90 years is associated with increased mortality, and that 90-year-olds with SBP of 150 mmHg or less
had increased mortality risk, independent of the SBP trend in preceding years.60
Furthermore, it has
been shown that in patients aged 85 or more with impaired cognitive functioning, higher SBP is
associated with reduced risk of stroke.61
A careful review of the epidemiology suggests that, in the oldest
old, and especially in the frail, hypertension is not an attributable risk factor for stroke, and
hypercholesterolemia has little effect on stroke risk overall.62
Another example in the area of diabetes management are the recently published evidence-informed
guidelines for treating frail older adults with Type 2 Diabetes Mellitus (T2DM),63
which recommend more
liberalised targets (HbA1c ≥ 8%), treatment simplification, and less monitoring. In patients with long-
standing T2DM and at high risk for cardiovascular events, intensive BP control and fibrate therapy in the
presence of controlled low-density lipoprotein cholesterol levels did not produce a measurable effect on
cognitive decline at 40 months of follow-up; furthermore, intensive BP control was associated with
greater decline in total brain volume at 40 months relative to standard therapy.64
Frailty for more Appropriate Prescribing
Frail older people have been grossly underrepresented in clinical trials, and many day-to-day treatment
decisions are still based on evidence extrapolated from more robust patient groups with fewer
physiological deficits.65
There is very limited evidence on the safety and efficacy of medicines in older
adults, particularly in the frail, who often have multiple co-morbidities and functional impairments.66
The risk of adverse drug reactions (ADRs) increases with increasing patient frailty, and since all
physicians are likely to provide care for this group of vulnerable patients, understanding the concept of
frailty may help to optimise medication prescribing for older people. The incorporation of frailty
measures into future clinical studies of drug effects and pharmacokinetics is important if we are to
improve medication use and guide drug doses for fit and frail older people.65
Furthermore,
individualised prescribing could reduce the risk of adverse drug reactions in at-risk frail older patients.67
Specific guidelines for the management of common conditions will be developed tailored to the
biological age or frailty status of older persons 68
.

Frailty as an Indication for Comprehensive Geriatric Assessment (CGA)
Importantly, the emerging evidence base for the frail is not only about reducing interventions (e.g.
saving the patient – and the health care system – from tight blood pressure and glycaemic controls), but
also about proactively intervening. The most notable example is the Cochrane systematic review on
Comprehensive Geriatric Assessment (CGA) for older adults admitted to hospital 69
. This review showed
that CGA (a multidimensional, interdisciplinary diagnostic process to determine the medical,
psychological and functional capabilities of a frail elderly person in order to develop a co-ordinated and
integrated plan for treatment and long-term follow up) increases a patient's likelihood of being alive and
in their own home at up to 12 months 69
.
Conclusion
In clinical care provision, frailty assessment tools are likely to help clinicians assess vulnerability in
specific clinical scenarios. With high degree of probability, there is presently no other area of Medicine
where such an exciting evidence gap has emerged concerning a sizeable and growing sector of the
population, with simultaneous potential to improve patient outcomes, reduce healthcare expenditure in
ineffective (and potentially harmful) interventions, and help focus resources on new, proactive and
effective CGA-based models of specialist care. The frailty paradigm demands an even greater degree of
involvement at the individual patient level, and will pave the way towards a much more personalised
medicine in old age.
References
1. Clegg A, Young J, Iliffe S, Rikkert MO and Rockwood K. Frailty in elderly people. Lancet. 2013; 381: 752-62.
2. Campbell AJ and Buchner DM. Unstable disability and the fluctuations of frailty. Age and ageing. 1997; 26: 315-
8.
3. Romero Ortuno R and Formiga F. [Fitness or frailty? Does age matter? New horizons in geriatrics]. Revista
espanola de geriatria y gerontologia. 2013; 48: 207-8.
4. Romero-Ortuno R and O'Shea D. Fitness and frailty: opposite ends of a challenging continuum! Will the end of
age discrimination make frailty assessments an imperative? Age and ageing. 2013; 42: 279-80.
5. Lloyd-Sherlock P, McKee M, Ebrahim S, et al. Population ageing and health. Lancet. 2012; 379: 1295-6.
6. Mitnitski AB, Graham JE, Mogilner AJ and Rockwood K. Frailty, fitness and late-life mortality in relation to
chronological and biological age. BMC geriatrics. 2002; 2: 1.
7. Schuurmans H, Steverink N, Lindenberg S, Frieswijk N and Slaets JP. Old or frail: what tells us more? The journals
of gerontology Series A, Biological sciences and medical sciences. 2004; 59: M962-5.
8. Cesari M, Gambassi G, van Kan GA and Vellas B. The frailty phenotype and the frailty index: different
instruments for different purposes. Age and ageing. 2014; 43: 10-2.
9. Bandeen-Roche K, Xue QL, Ferrucci L, et al. Phenotype of frailty: characterization in the women's health and
aging studies. The journals of gerontology Series A, Biological sciences and medical sciences. 2006; 61: 262-6.
10. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. The journals of
gerontology Series A, Biological sciences and medical sciences. 2001; 56: M146-56.
11. Fried LP, Ferrucci L, Darer J, Williamson JD and Anderson G. Untangling the concepts of disability, frailty, and
comorbidity: implications for improved targeting and care. The journals of gerontology Series A, Biological sciences
and medical sciences. 2004; 59: 255-63.
12. Taylor HL, Jacobs DR, Jr., Schucker B, Knudsen J, Leon AS and Debacker G. A questionnaire for the assessment
of leisure time physical activities. Journal of chronic diseases. 1978; 31: 741-55.
13. Eckel SP, Bandeen-Roche K, Chaves PH, Fried LP and Louis TA. Surrogate screening models for the low physical
activity criterion of frailty. Aging clinical and experimental research. 2011; 23: 209-16.
14. Romero-Ortuno R, Walsh CD, Lawlor BA and Kenny RA. A frailty instrument for primary care: findings from the
Survey of Health, Ageing and Retirement in Europe (SHARE). BMC geriatrics. 2010; 10: 57.
15. Romero-Ortuno R, O'Shea D and Kenny RA. The SHARE frailty instrument for primary care predicts incident
disability in a European population-based sample. Quality in primary care. 2011; 19: 301-9.
16. Romero-Ortuno R. The Frailty Instrument of the Survey of Health, Ageing and Retirement in Europe (SHARE-FI)
predicts mortality beyond age, comorbidities, disability, self-rated health, education and depression. European
geriatric medicine. 2011; 2: 323-6.
17. Ntlholang O, Kelly RE, Romero-Ortuno R, et al. The role the frailty syndrome can play in advocacy and resource
allocation for our ageing population – findings in a Dublin day hospital. The Journal of Frailty & Aging. 2013; in
press.
18. Searle SD, Mitnitski A, Gahbauer EA, Gill TM and Rockwood K. A standard procedure for creating a frailty index.
BMC geriatrics. 2008; 8: 24.
19. Theou O, Brothers TD, Mitnitski A and Rockwood K. Operationalization of frailty using eight commonly used
scales and comparison of their ability to predict all-cause mortality. Journal of the American Geriatrics Society.
2013; 61: 1537-51.
20. Romero-Ortuno R. Frailty Index in Europeans: Association with determinants of health. Geriatrics &
gerontology international. 2013.
21. Song X, Mitnitski A and Rockwood K. Prevalence and 10-year outcomes of frailty in older adults in relation to
deficit accumulation. J Am Geriatr Soc. 58: 681-7.
22. Rockwood K, Song X and Mitnitski A. Changes in relative fitness and frailty across the adult lifespan: evidence
from the Canadian National Population Health Survey. CMAJ. 183: E487-94.
23. Romero-Ortuno R. An alternative method for Frailty Index cut-off points to define frailty categories. European
geriatric medicine. 2013; 4.
24. Kitchen R, Patel R, French G and Faull C. How do surgeons and anaesthetists make decisions about surgery for
patients who are frail, and what factors influence these decisions? BMJ supportive & palliative care. 2014; 4 Suppl
1: A37-8.
25. Rodes-Cabau J and Mok M. Working toward a frailty index in transcatheter aortic valve replacement: a major
move away from the "eyeball test". JACC Cardiovascular interventions. 2012; 5: 982-3.
26. Revenig LM, Canter DJ, Master VA, et al. A prospective study examining the association between preoperative
frailty and postoperative complications in patients undergoing minimally invasive surgery. Journal of endourology /
Endourological Society. 2014; 28: 476-80.
27. Partridge JS, Harari D and Dhesi JK. Frailty in the older surgical patient: a review. Age and ageing. 2012; 41:
142-7.
28. Robinson TN, Wu DS, Pointer L, Dunn CL, Cleveland JC, Jr. and Moss M. Simple frailty score predicts
postoperative complications across surgical specialties. American journal of surgery. 2013; 206: 544-50.
29. Farhat JS, Velanovich V, Falvo AJ, et al. Are the frail destined to fail? Frailty index as predictor of surgical
morbidity and mortality in the elderly. The journal of trauma and acute care surgery. 2012; 72: 1526-30; discussion
30-1.

30. Makary MA, Segev DL, Pronovost PJ, et al. Frailty as a predictor of surgical outcomes in older patients. Journal
of the American College of Surgeons. 2010; 210: 901-8.
31. Singh M, Rihal CS, Lennon RJ, Spertus JA, Nair KS and Roger VL. Influence of frailty and health status on
outcomes in patients with coronary disease undergoing percutaneous revascularization. Circulation Cardiovascular
quality and outcomes. 2011; 4: 496-502.
32. Afilalo J, Mottillo S, Eisenberg MJ, et al. Addition of frailty and disability to cardiac surgery risk scores identifies
elderly patients at high risk of mortality or major morbidity. Circulation Cardiovascular quality and outcomes. 2012;
5: 222-8.
33. Sundermann SH, Dademasch A, Seifert B, et al. Frailty is a predictor of short- and mid-term mortality after
elective cardiac surgery independently of age. Interactive cardiovascular and thoracic surgery. 2014.
34. Bagnall NM, Faiz O, Darzi A and Athanasiou T. What is the utility of preoperative frailty assessment for risk
stratification in cardiac surgery? Interactive cardiovascular and thoracic surgery. 2013; 17: 398-402.
35. Green P, Woglom AE, Genereux P, et al. The impact of frailty status on survival after transcatheter aortic valve
replacement in older adults with severe aortic stenosis: a single-center experience. JACC Cardiovascular
interventions. 2012; 5: 974-81.
36. Tsiouris A, Hammoud ZT, Velanovich V, Hodari A, Borgi J and Rubinfeld I. A modified frailty index to assess
morbidity and mortality after lobectomy. The Journal of surgical research. 2013; 183: 40-6.
37. Reisinger KW, van Vugt JL, Tegels JJ, et al. Functional Compromise Reflected by Sarcopenia, Frailty, and
Nutritional Depletion Predicts Adverse Postoperative Outcome After Colorectal Cancer Surgery. Annals of surgery.
2014.
38. Keller DS, Bankwitz B, Nobel T and Delaney CP. Using frailty to predict who will fail early discharge after
laparoscopic colorectal surgery with an established recovery pathway. Diseases of the colon and rectum. 2014; 57:
337-42.
39. Lasithiotakis K, Petrakis J, Venianaki M, et al. Frailty predicts outcome of elective laparoscopic cholecystectomy
in geriatric patients. Surgical endoscopy. 2013; 27: 1144-50.
40. Tan KY, Kawamura YJ, Tokomitsu A and Tang T. Assessment for frailty is useful for predicting morbidity in
elderly patients undergoing colorectal cancer resection whose comorbidities are already optimized. American
journal of surgery. 2012; 204: 139-43.
41. Ganapathi AM, Englum BR, Hanna JM, et al. Frailty and risk in proximal aortic surgery. The Journal of thoracic
and cardiovascular surgery. 2014; 147: 186-91 e1.
42. Karam J, Tsiouris A, Shepard A, Velanovich V and Rubinfeld I. Simplified frailty index to predict adverse
outcomes and mortality in vascular surgery patients. Annals of vascular surgery. 2013; 27: 904-8.
43. Adams P, Ghanem T, Stachler R, Hall F, Velanovich V and Rubinfeld I. Frailty as a predictor of morbidity and
mortality in inpatient head and neck surgery. JAMA otolaryngology-- head & neck surgery. 2013; 139: 783-9.
44. Garonzik-Wang JM, Govindan P, Grinnan JW, et al. Frailty and delayed graft function in kidney transplant
recipients. Archives of surgery. 2012; 147: 190-3.
45. Krishnan M, Beck S, Havelock W, Eeles E, Hubbard RE and Johansen A. Predicting outcome after hip fracture:
using a frailty index to integrate comprehensive geriatric assessment results. Age and ageing. 2014; 43: 122-6.
46. Tegels JJ, de Maat MF, Hulsewe KW, Hoofwijk AG and Stoot JH. Value of geriatric frailty and nutritional status
assessment in predicting postoperative mortality in gastric cancer surgery. Journal of gastrointestinal surgery :
official journal of the Society for Surgery of the Alimentary Tract. 2014; 18: 439-46.
47. Revenig LM, Canter DJ, Taylor MD, et al. Too frail for surgery? Initial results of a large multidisciplinary
prospective study examining preoperative variables predictive of poor surgical outcomes. Journal of the American
College of Surgeons. 2013; 217: 665-70 e1.
48. Ferrucci L, Guralnik JM, Cavazzini C, et al. The frailty syndrome: a critical issue in geriatric oncology. Critical
reviews in oncology/hematology. 2003; 46: 127-37.

49. Aaldriks AA, van der Geest LG, Giltay EJ, et al. Frailty and malnutrition predictive of mortality risk in older
patients with advanced colorectal cancer receiving chemotherapy. Journal of geriatric oncology. 2013; 4: 218-26.
50. Basso U, Tonti S, Bassi C, et al. Management of Frail and Not-Frail elderly cancer patients in a hospital-based
geriatric oncology program. Critical reviews in oncology/hematology. 2008; 66: 163-70.
51. Schmoll HJ. Do we need oncology trials tailored for the elderly or frail? Lancet. 2011; 377: 1725-7.
52. de Barros Pontes L, Todaro J, Karnakis T, et al. Treatment of a frail older patient with diffuse large B-cell
lymphoma on maintenance dialysis: attenuated immunochemotherapy and adapted care plan. Case reports in
oncology. 2013; 6: 197-203.
53. Seymour MT, Thompson LC, Wasan HS, et al. Chemotherapy options in elderly and frail patients with
metastatic colorectal cancer (MRC FOCUS2): an open-label, randomised factorial trial. Lancet. 2011; 377: 1749-59.
54. Courtney-Brooks M, Tellawi AR, Scalici J, et al. Frailty: an outcome predictor for elderly gynecologic oncology
patients. Gynecologic oncology. 2012; 126: 20-4.
55. Mahmood SS, Levy D, Vasan RS and Wang TJ. The Framingham Heart Study and the epidemiology of
cardiovascular disease: a historical perspective. Lancet. 2014; 383: 999-1008.
56. Lipsitz LA. A 91-year-old woman with difficult-to-control hypertension: a clinical review. JAMA. 2013; 310:
1274-80.
57. Odden MC, Peralta CA, Haan MN and Covinsky KE. Rethinking the association of high blood pressure with
mortality in elderly adults: the impact of frailty. Archives of internal medicine. 2012; 172: 1162-8.
58. Nowak A and Hubbard RE. Falls and frailty: lessons from complex systems. Journal of the Royal Society of
Medicine. 2009; 102: 98-102.
59. Tinetti ME, Han L, Lee DS, et al. Antihypertensive Medications and Serious Fall Injuries in a Nationally
Representative Sample of Older Adults. JAMA internal medicine. 2014.
60. Poortvliet RK, de Ruijter W, de Craen AJ, et al. Blood pressure trends and mortality: the Leiden 85-plus Study.
Journal of hypertension. 2013; 31: 63-70.
61. Sabayan B, van Vliet P, de Ruijter W, Gussekloo J, de Craen AJ and Westendorp RG. High blood pressure,
physical and cognitive function, and risk of stroke in the oldest old: the Leiden 85-plus Study. Stroke; a journal of
cerebral circulation. 2013; 44: 15-20.
62. Byatt K. Overenthusiastic stroke risk factor modification in the over-80s: Are we being disingenuous to
ourselves, and to our oldest patients? Evidence-based medicine. 2014.
63. Mallery LH, Ransom T, Steeves B, Cook B, Dunbar P and Moorhouse P. Evidence-Informed Guidelines for
Treating Frail Older Adults With Type 2 Diabetes: From the Diabetes Care Program of Nova Scotia (DCPNS) and the
Palliative and Therapeutic Harmonization (PATH) Program. J Am Med Dir Assoc. 2013.
64. Williamson JD, Launer LJ, Bryan RN, et al. Cognitive function and brain structure in persons with type 2 diabetes
mellitus after intensive lowering of blood pressure and lipid levels: a randomized clinical trial. JAMA internal
medicine. 2014; 174: 324-33.
65. Hubbard RE, O'Mahony MS and Woodhouse KW. Medication prescribing in frail older people. European journal
of clinical pharmacology. 2013; 69: 319-26.
66. Hilmer SN, Gnjidic D and Le Couteur DG. Thinking through the medication list - appropriate prescribing and
deprescribing in robust and frail older patients. Australian family physician. 2012; 41: 924-8.
67. McMillan GJ and Hubbard RE. Frailty in older inpatients: what physicians need to know. QJM : monthly journal
of the Association of Physicians. 2012; 105: 1059-65.
68. Muller M, Smulders YM, de Leeuw PW and Stehouwer CD. Treatment of Hypertension in the Oldest Old: A
Critical Role for Frailty? Hypertension. 2013.
69. Ellis G, Whitehead MA, O'Neill D, Langhorne P and Robinson D. Comprehensive geriatric assessment for older
adults admitted to hospital. Cochrane Database Syst Rev. 2011: CD006211.