substance use problems and the older adult
TRANSCRIPT

Substance Use Problems and the Older Adult
Suzanna Waters Castillo, PhD, MSSWDistinguished Faculty AssociateContinuing Studies – Programs on Aging and Geriatric Mental HealthUniversity of Wisconsin at [email protected] 263 3174www.WGPI.wisc.edu
SUBSTANCE USE PROBLEMS AND THE OLDER ADULT
•Topics today
• Our aging population
• Our Brain on Drugs
• SUDs and MI
• Gambling and Nicotine
• Alcohol Consumption and Older Adults
• Medication Misuse
• Screening Substances
• SBIRT

3Source: U.S. Bureau of the Census. (2000). Population projections of the United States by age, sex,
race and hispanic origin: 1995- 2050, Current Population Reports, P25-1130.
46.0
53.7
62.6
70.3
39.735.0
0
10
20
30
40
50
60
70
80
90
2000 2010 2015 2020 2025 2030
Nu
mb
er
in M
illio
ns
65+ Population Will Double: 35-70 Million Over the Next 25 Years

Aging in Wisconsin

Women Live Longer
Source of data: U.S. Census Bureau, State Interim Population Projections by Age and Sex: 2004-2030, 2005.
Age 65+
Female50.9%
Female58.8%
Male41.2%
Age 85+
Female71.1%
Male28.9%

Housing Characteristics of the 65+
@5.0% live in NFs
66% live with others.
28% live alone in households.
66%
28%
@5.0
%

7
OLDER ADULTS WITH MENTAL ILLNESS WILL DOUBLE FROM 2000 TO 2030.
Projected Growth of 65 and Over Population with Mental Disorders:
2000 to 2030
14
10.8
8 7
0
2
4
6
8
10
12
14
16
2000 2010 2020 2030
Nu
mb
er
in M
illio
ns
Sources: U.S. Department of Health and Human Services, Mental Health: A Report of the
Surgeon General (Rockville, MD: 1999).
U.S. Bureau of the Census. (2000). Population projections of the United States by age, sex, race
and hispanic origin: 1995-2050, Current Population Reports, P25-1130.

Substances
• Baby Boom Generation• Different hypothesis
• We know that baby boomers consume high levels of alcohol
• First cohort group w/high incidence of illicit drug use
• Increased consumption of wine and social acceptance and does not show a decline w/age
• First cohort group socialized into drinking and drug use during a time of increasing consumption
• What there be a cohort effect for this generation of aging adults?
Source: M Gilhooly, Addiction Research and Theory, 2005 (pg 267-280).

Substances
Admissions Aged 50 or Older, by Age Group and Primary
Substance of Abuse: DAIS Report, 2005

Substances: Alcohol, Medication, Illicit Drugs, Tobacco
• Use resulting in declining physical/ social function
• Use in risky situations
• Continued use despite adverse social or personal consequences
Abuse by Patient
• Use resulting in tolerance or withdrawal symptoms
• Unsuccessful attempts to stop or control use
• Preoccupation with attaining or using the drug
Dependence
(Source: DSM IV)

SUDS and Your Brain

SUDS and Your Brain
Addiction Involves Multiple Factors

How Drugs Work
Interact with nerve circuits, centers, and chemical messengers
Results
I Feel Good – Euphoria & Reward
I Feel “Better” – Reduce negative feelings
This Feels “Normal”
I’m craving it, tolerating its effects,
withdrawing and feeling sick

How Drugs Work
Cognitive Deficits Memory problems – short-term loss
Impaired abstraction
Perseveration using failed problem-solving strategies
Loss of impulse control
These deficits are similar to
those with brain damage

How Drugs Work: Video

Suds and MI

SUDS and MI
•Co-occurring Mental Illness with SUDS
Mood Disorder+: 24-40% have a co-occurring SUDS
Alcoholism+: 65% of females and 44% of male alcoholics have co-occurring mental health disorder(s)
THE MAJOR ONE = DEPRESSION19% of female alcoholics, 4x the rate for men
Gambling and Elderly
• Chronic and Late Life
• Seniors are fastest growing gambling population
• Grief Gambling
• Escape, loneliness, regrets, depression, pain etc.

Gambling Studies

Nicotine and Elderly
• Elderly use = 8.4%
• 2-3 times increase in use for SUDS and MI
• Higher rates of CAD and CA
• Dependence:
• Nicotine Dependence is a behavior that an individual is unable to stop use, despite knowledge about damage to health.
• Nicotine is a mood altering substance
• Mildly pleasant

The Challenge
• Society• Ageism
• Lack of awareness
• Disregard
• Lack of education
• Culture of AODA
The Challenge
• Providers• Ageism
• Many providers uncomfortable asking
• Chronic illess and cognitive impairment may mask SUD
• Lack of screening tools and skills
• Lack of knowledge regarding late life AODA

The Challenge
• Older adults• Denial
• Shame
• Fear
• Self-dx
• Unsure of who can help
• Life-long pattern
• Lack of social and family support
• Lack of education and prevention

Alcohol
at-risk
drinking
15%
general
population
85%
• Alcohol is the most common substance misused/abused by older adults• 1-15% at risk drinking
• Complicated by:• Mental Illness• RX Medications• Over the Counter
medications

30 Day Binge Drinking of Wisconsinites
Age and Region

Alcohol
• Older women
• Heightened response to OTC and prescriptions medications
• Have less lean muscle mass than men and less able to metabolize alcohol and this increases w/age
• Increased risk for osteoporosis = bone loss and fracture
• Liver enzymes that metabolize alcohol become less effective w age

Alcohol
• Older Women
• 11% of women 59+ are addicted to prescription medications
• 1% get approprite help
• Alcohol and prescription drugs are the main substance abuse disorders among women

Late vs. Early Onset Alcohol problems
• Late onset - generally defined as onset after age 50
• Up to 50% of elderly alcohol abusers experience the onset of problem drinking later in life
• Early onset patients experience more emotional problems and drop out of treatment at a higher rate.
• Late onset patients tend to be more psychologically stable, remain in treatment longer, have their problem resolved without treatment

Alcohol
Caterogies1. USE
Following prescribed guidelines
2. MIS-USE – 1 in 5 older adultsRisky drinkingPattern maintained will lead to abuse
Unsafe use of medicationsNot taking on timeNot taking proper doseMixing with alcohol and other drugs
3. ABUSEChronicHeavyBinge

Alcohol
• How is use Different with Aging?•Metabolize alcohol more slowly•Metabolize RX and OTC medications slowly•At least one chronic illness•Prone to falls, accidents•More likely to drink alone and at home• Isolation•Prescription drug misuse•Too much or too little or mixing•Multiple medications•ADRs plus alcohol

Alcohol
• Physical Changes of Aging that affect how Alcohol is processed
• Lean body mass decreases
• Fat increases
• Total body waters decreases
• Decrease in stomach ability to metabolize alcohol
• Renal changes
• Decrease in liver function
• Neurotransmitter/brain related changes

Alcohol
• Protective Factors
• Female
• Higher Religiosity
• Fewer Mental/Physical Health Problems
• Positive Coping Styles
• More Social Supports

Alcohol
• When is drinking a problem for older adults?
• Pouring a glass of:
• Wine
• Spirits
• Sherry
• Liqueur

Alcohol

Alcohol
•Drinking Guidelines• No more than 1 standard drink per
day
• No more than 2-3 drinks on any drinking day (binge drinking)
• Limits for older women should be somewhat less than for oldermen

Alcohol3
6

Alcohol
• Excuses people make to use/misuse alcohol
• Improve mood
• Continue a pattern
• Mask depression
• For sleep
• Manage loneliness or boredom
• Socialize
• Manage pain

Video: Alcohol Abuse and Elderly

Mental Illness
Risk Factors Chronic physical health condition(s)
Multiple losses
Death of a loved one
Caregiving stress
Social isolation/lack or loss of social support
Significant loss of independence
History of mental health problems
SUDs
Head trauma with loss of consciousness

Mental Illness
•Alcohol abuse increase risk of:
• Depression
• Anxiety
• Cognitive Processing
• Memory
• Problem solving
• Judgement

Alcohol Abuse
• Medical Conditions• Liver disease
• Cardiovascular disease
• Risk of stroke
• Diabetes
• Ulcers
• GI problems
• Sleep problems
• Gait Disorders
• Bone density and fractures
• Cancer of stomach, larynx, pancreas, liver or esophagus

Alcohol and Medication Misuse

Alcohol
Medication Misuse:
1 in 5 older adults may be affected by combined difficulties with alcohol and medication misuse.
Alcohol-medication interactions may be a factor in at least 25% of ER admissions (NIAAA, 1995).

Alcohol
• Identifying High Risk Older Adults
• Use of certain medications (e.g., warfarin, digoxin, diuretics, psychoactive meds, analgesics)
• 4 or more medications
• Certain chronic conditions (e.g., diabetes)
• Evidence of medication misuse
• Chronic alcohol use

Alcohol
• Dangers•Aspirin and alcohol can increase possibility of
bleeding
• Sleepiness w/alcohol and cold and/or allergy medications
• Cough syrups w/high alcohol content
•Alcohol w/painkillers e.g., acetaminophen can damage liver.

Alcohol
•Dangerous RX
• Benzodiazepines i.e., Valium, Ativan or Centrax
• Sleeping Medications i.e., Ambien
• Pain Medications i.e., Codeine, Percoset
• Antipsychotic Medications
• Antiseizure Medications
• Antihistamines both otc and RX

Alcohol
• “Symptoms”of Medication-Related Problems Due to Misuse/Abuse• Confusion
• Depression
• Delirium
• Insomnia
• Parkinson’s-like symptoms
• Incontinence
• Weakness or lethargy
• Loss of appetite
• Falls
• Changes in speech

Alcohol
• Do not mix with alcohol• Anti depressant
• Anti anxiety medication
• Pain medication of any type
• Sleeping medication of any typeSource: National Council on Aging

Alcohol
• Alcohol and Medications Warning Signs• Physical
• Blackout
• Falls, bruises, burns
• Incontinence (not baseline)
• Poor hygiene
• Strange response to medications
• Poor nutrition i.e., eating junk food only
• Sleep problems or daytime drousiness

Alcohol
• Alcohol and Medication Warning Signs
• Medications
• Unclear about nature of prescription and use
• Confusion about prescription and alcohol use
• Multiple medications
• Previous ADRs
• Lack of Adherence

Alcohol
• Alcohol and Medication Warning Signs
• Physical
• Mood swings
• Anxiousness
• Depression and/or anxiety
• Memory or thinking problems
• Shakes or tremors
• Slurred speech
• Morning drinking
• Vomitting, bloating, indigestion

Alcohol
• Alcohol and Medication Warning Signs
• Behavioral
• Problems w police
• Frequent ER visits
• Does not pay bills or is erratic
• Does not care for home, plants, pets
• Isolates self
• Poor hygiene
• Eviction
• Increased anger and agitation

Alcohol
• Risk Factors for Alcohol Abuse
• Emotional and Social
• Losses (death, finance, family, function, property, status)
• Grief
• Male
• Higher SES
• Retirement
• Social isolation/Low Social Support
• Lack of Purpose/Boredom

Alcohol
• Risk Factors (contd.)
• Medical Problems
• Chronic illness
• Terminal illness
• ADL and IADL problems
• Sensory problems
• Sleep Disorder
• Mood problems
• Psychiatric Illness

Alcohol
• Risk Factors (contd.)
• History
• Family patterns
• Life long problem/chronic
• Cultural i.e., Wisconsin
• Minority Status
• Suicide ideation and/or attempts
• Using Substances to cope
Video: Alcohol and Medication Misuse

Alcohol
•SCREENING

Alcohol
• Special Screening Concerns• Judgement
• Shame
• Fear
• Denial
• Uncertainty
• Outcome
•Rapport• Build trust at screening time
• Develop understanding of who this person is• Culture
• Beliefs
• Values
• Know their lifetime use patterns

Screening for Depresssion
PHQ-9: Patient Health Questionnaire
Over the last 2 weeks, how often have you
been bothered by any of the following?
Not at all
(0)
Several days
(1)
More than
half the
days
(2)
Nearly every
day
(3)
1. Little interest or pleasure in doing things?
2. Feeling down, depressed, or hopeless? x
3. Trouble falling or staying asleep or sleeping
too much?
x x
4. Feeling tired or having little energy? x
5. Poor appetite or over eating? x
6. Feeling bad about yourself-or that you are a
failure or have let yourself or your family
down?
x
7. Trouble concentrating on things, such as
reading the newspaper or watching TV?
x
8. Moving or speaking so slowly that other
people could have noticed? Or the opposite-
being so fidgety or restless that you have been
moving around a lot more than usual?
x
9. Thoughts that you would be better off dead
or of hurting yourself in some way?
x
Column Scores
Severity Score:

Screening for Depression
Geriatric Depression Scale/short FormAdapted from Yesavage JA, Brink TL, Rose TL, et al.
Choose the best answer that you have felt over the past 2 weeks
May ask directly or have someone fill it out
Yes/No
1 Are you basically satisfied with your life?
2 Have you dropped many of you’re activities and interests?
3 Do you feel that your life is empty?
4 Do you often get bored?
5 Are you in good spirits most of the time?
6 Are you afraid that something bad is going to happen to you?
7 Do you feel happy most of the time?
8 Do you often feel helpless?
9 Do you prefer to stay at home?
10 Do you feel that you have more problems with memory than most?
11 Do you think it is wonderful to be alive now?
12 Do you feel worthless the way you are now?
13 Do you feel full of energy?
14 Do you feel that your situation is hopeless?
15 Do you think that nmost people are better off than you are?
Scoring: Assign 1 point if you answer accordingly. 5 or more points indicates a possible depression.
Numbers 2, 3, 4, 6, 8,9, 10, 12, 14, 15 = YES
Numbers 1, 5, 7, 11, 13 = NO

Screening for Generalized Anxiety Disorder GAD-7
Spitzer RL. Arch Intern Med 2006;166:1092-1097.
TOTAL
SCORE
Provisional
Diagnosis
0-4 Minimal anxiety
5-9 Mild anxiety
10-14 Moderate anxiety
15-21 Severe anxiety
• Self rated• Specific for GAD but
useful to detect an anxiety disorder in depression
• Can be used to monitor treatment progress
*GAD-2 is the first 2 questions of the GAD-7

Alcohol• SMAST- G• Short Michigan Alcoholism Screening Test–Geriatric Version (SMAST-G)
• © The Regents of the University of Michigan, 1991.
• Source: University of Michigan Alcohol Research Center. Reprinted with permission.
• Yes (1) No (0)
• 1. When talking with others, do you ever underestimate how much you drink?
• 2. After a few drinks, have you sometimes not eaten or been able to skip a meal because
• you didn’t feel hungry?
• 3. Does having a few drinks help decrease your shakiness or tremors?
• 4. Does alcohol sometimes make it hard for you to remember parts of the day or night?
• 5. Do you usually take a drink to relax or calm your nerves?
• 6. Do you drink to take your mind off your problems?
• 7. Have you ever increased your drinking after experiencing a loss in your life?
• 8. Has a doctor or nurse ever said they were worried or concerned about your drinking?
• 9. Have you ever made rules to manage your drinking?
• 10. When you feel lonely, does having a drink help?
• TOTAL SMAST-G-SCORE (0-10) _____________
• SCORING: 2 OR MORE “YES” RESPONSES IS INDICATIVE OF AN ALCOHOL PROBLEM.
• For further information, contact Frederic C. Blow, PhD, Director, Serious Mental Illness Treatment Research and Evaluation Center (SMITREC),
• Department of Veterans Affairs, Senior Associate Research Scientist, Associate Professor, Department of Psychiatry, University of Michigan.

Alcohol

Alcohol
• Screening Tool: Determine Your Nutritional Health• I have an illness or condition that made me change the kind
or amount of food I eat
• I eat fewer than two meals each day
• I eat few fruits or vegetables or milk products
• I have three or more alcoholic drinks almost every day
• I have tooth or mouth problems that make it hard for me to eat

Alcohol
• Screening Tool: Determine Your Nutritional Health • I don’t always have enough money to buy the food I need
• I eat alone most of the time
• I take three or more different prescribed or over-the-counter medicines a day
• Without wanting to do so, I have lost or gained 10 pounds in the last 6 months
• I am not always physically able to shop, cook, and/or feed myself

Alcohol
• Michigan Alcoholism Screening TestAnswering 2 or more w/yes indicates a possible problem.
1. When talking w others do you ever underestimate how much you actually drink?
2. After a few drinks, have you sometimes not eaten or been able to skip a meal because you didn’t feel hungry?
3. Does having a few drinks help decrease your shakiness or tremors?4. Does alcohol sometimes make it hard for you to remember parts of the day
or night?5. Do you drink to take your mind off your problems?6. Do you drink to relax or calm your nerves?7. Have you ever increased your drinking after experiencing a loss in your life?8. Has a doctor or nurse ever said they were worried or concerned about your
drinking?9. Have you ever made rules to manage your drink 10. When you feel lonely, does having a drink help?

MOCA

Substances
• Tobacco Use
• Illicit Drug Use

Wisconsin Treatment Admissions
Age 50+ by Substance

Illicit Drugs and Older Adults

Substance/Medication-Induced Anxiety Disorder
• Examples of Substances that can cause anxiety:
• Alcohol
• Caffeine
• Cannabis
• Phencyclidine
• Other Hallucinogens
• Inhalant
• Opioid
• Sedative, hypnotic or anxiolytic
• Amphetamine
• Cocaine

Substances
• Illicit Drugs
• National Survey on Drug Use 2006
• Street drugs
• Increase in elderly
• More exist than was expected
• Projections for 2020 age 50+ of about 3.3 million
• Underdiagnosed and undiagnosed problem
Substances and Misuse - Abuse

Treatment
•SBIRT - Evidence Based• Screening
• Brief Intervention
• Referral
• Treatment

Screening, Brief Intervention, Referral and Treatment Evidence-Based Screening Tool that works for Older Adults

Goal
The primary goal of SBIRT is to identify and effectively intervene with those who are at moderate or high risk for psychosocial or health care problems related to their substance use.

SBIRT Settings
Aging/Senior Services Inpatient
Behavioral Health Clinic Primary Care Clinic
Community Health Center Psychiatric Clinic
Community Mental Health Center School-Based/Student Health
Drug Abuse/Addiction Services Trauma Centers/Trauma Units
Emergency Room Urgent Care
Federally Qualified Health Center Veterans Hospital
Homeless Facility Other Agency Sites
Hospital
SBIRT Is a Highly Flexible Intervention

SBIRT

Drinks Per week
DrinksPer day
Men 14 4
Women 7 3 All age
>65 7 3
Categories of drinking
0cm 1 2 3 4 5 6 7 8 9 10
III
IV
ILow risk or
Abstain: 78%
Dependent: 5%
II
Harmful: 8%
Risky: 9%
SBIRT READINESS RULER
Low-risk
drinking limits
• “If it’s okay with you, let’s take a minute to talk about the annual screening form you’ve filled out today.”
Raise the subject
• “As your doctor, I can tell you that drinking (drug use) at this level can be harmful to your health and possibly responsible for the health problem you came in for today.”
Provide feedback
“On a scale of 0-10, how ready are you to cut back your use?”• If >0: “Why that number and not a ____ (lower one)?” •If 0: “Have you ever done anything while drinking (using drugs) that you later regretted?”
Enhance motivation
• “What steps can you take to cut back your use?”• “How would your drinking (drug use) have to impact your life
in order for you to start thinking about cutting back?”
Negotiate plan
I Low risk/Abstain
AUDIT: 0–7 DAST: 0
II RiskyAUDIT: 8–15 DAST: 1-2
III HarmfulAUDIT: 16-19 DAST: 3-5
IV DependentAUDIT: 20+ DAST: 6+
Not at all
Very
SA
MH
SA
Re
ferr
al H
elp
line
1-8
00
-66
2-H
EL
P

SBIRT
• Funding:• Title III-D of the Older American’s Act is
Disease Prevention and Health Promotion. As of this year, due to a change in the appropriations language, these funds are required to be used on only evidence-based DPHP programs. These include programs such as PEARLS, Healthy IDEAS, BRITE, or any other any other behavioral health program that meets at least AoA’s minimal criteria.

Alcohol
Watch Video:
SBIRT for Alcohol use: Older Man

Case Study
• Arthur is 76 year old Korean War Veteran who has post stroke (left side paralysis)cardiovascular disease. He is also diabetic, has symptoms of depression, sleep problems ( can not fall asleep), memory impairment and may be mis-using alcohol.
• Medications are:
• Statin, Anti hypertensive, Insulin, Ambien (sleep), Anti coagulant, aspirin

Substance
Abuse/
Misuse
Social Issues:
More free time to use
Norms for drinking:
-different communities
-peer pressures
Changes in
relationships
Grief, boredom
Undue pessimism
Personality/personal Issues:
Norms for drinking-
at different ages
Prior use of illicit drugs
Underreporting
Denial/minimization
Guilt/shame/hopelessness
Psychiatric Issues:
Chronic anxiety
Recurrent depression, mania
Cognitive impairment-secondary
Alcohol: early- vs. late-onset
Nicotine; Caffeine; Narcotics
Increased rate of spontaneous
remission
Medical Issues:
Chronic pain
Chronic fatigue
Chronic insomnia
Decreased tolerance, falls
Mimic other illnesses
Excess impairment
Medication Issues:
Narcotic analgesics; hypnotics
Sedatives; stimulants
Interactions with Rx,
over-the-counter (OTC) meds

Case Study
• Pair up w/one other person
• What are his possible risk factors?
• How is his problem different d/t age?
• How will you screen for problems?
• What approach to screening will you take?
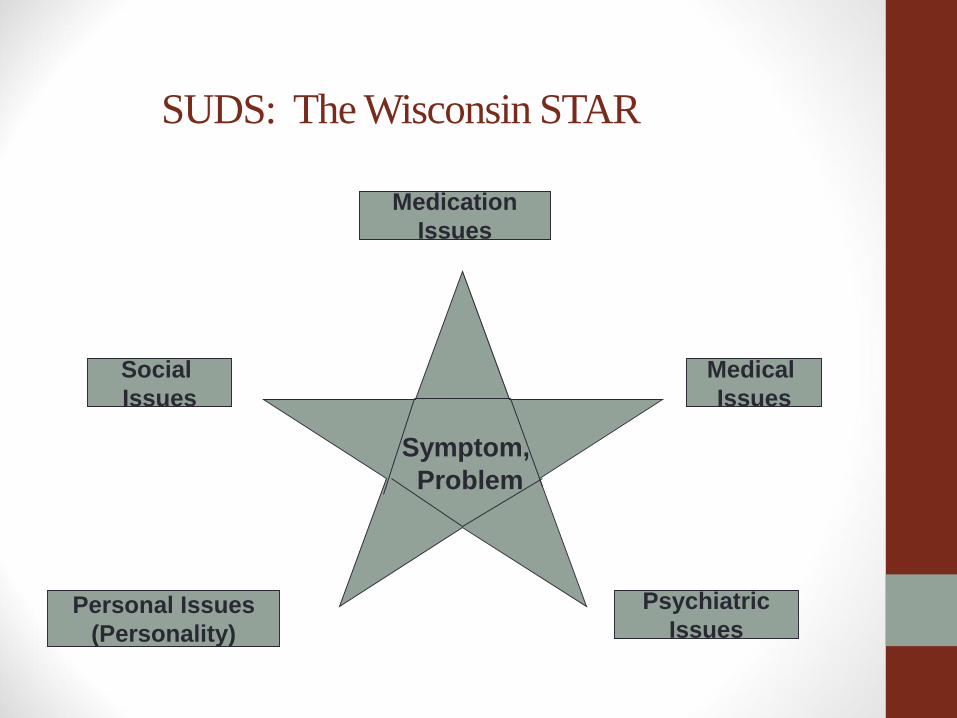
SUDS: The Wisconsin STAR
Symptom,
Problem
Medication
Issues
Social
Issues
Personal Issues
(Personality)
Psychiatric
Issues
Medical
Issues

Substance use Problems and the Older Adult
•References• Journal of Aging Health, Illicit and Non Medical Drug Use
Among Older Adults, Blazer and SU, April 23 (3), 2012.
• SAMHSA – Substance Abuse and Mental Health Services Administrations
• US Census Bureau
• Wisconsin DHS Demographic Report
• Wisconsin Academy State Profile 2012
• Wisconsin STAR – Timothy Howell, MD