suboxone report
TRANSCRIPT

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 1/20
1May 2016
Mov ng Towar s Improve Access for
vidence-Based Opioid Addicton Caren Br s Co um a
Recommenda ons from the Bri sh Columbia Node of
the Canadian Research Ini a ve on Substance Misuse
ay 2016

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 2/20
2May 2016
Execu ve Summary The declaration of a public health emergency in response to the recentrise in illicit drug overdose deaths in British Columbia underscores theimportance of developing a coordinated, evidence-based provincialstrategy to address the harms related to pharmaceutical and illicitopioids. A key component of this strategy is the delivery of healthsystem interventions that optimize engagement, care and treatmentof individuals with opioid addiction. This report brie y describes thescope of the provincial opioid crisis; how regulatory systems for opioidaddiction treatment have evolved in BC, Canada, and internationally;and makes several recommendations that support the eliminationof current barriers to accessing buprenorphine/naloxone, a safe ande ective alternative to methadone for treatment of opioid addictionthat is currently underutilized in BC.

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 3/20
3May 2016
Moving towards improved access for evidence- based opioid addic on care in Bri sh Columbia
The declaration of a public health emergency inresponse to the recent rise in overdose deaths inBritish Columbia underscores the importanceof developing a coordinated, evidence-basedprovincial strategy to address the harms relatedto pharmaceutical and illicit opioids. One keycomponent of this strategy is the delivery of healthsystem interventions that optimize engagement,care and treatment of individuals with opioiduse disorder. Recent changes to BC PharmaCarethat expand coverage to include buprenorphine/ naloxone (e.g., Suboxone® ) as a rst-line treatmentfor opioid use disorder (e.g., patients are no longerrequired to try methadone rst) o er a promising
step forward in reducing fatal overdoses, addictionand other severe harms related to opioid use in BC. In addition, in coming months it is anticipated thatthe College of Physicians and Surgeons of BritishColumbia (CPSBC) may eliminate prescriberrestrictions on buprenorphine/naloxone, which will further improve access to evidence-based carefor all British Columbians. These changes presentan opportunity to highlight remaining barriersto buprenorphine/naloxone access that persistdespite clear research evidence of its safety ande ectiveness.
This document brie y describes: the scope of theprovincial opioid crisis; how regulatory systemsfor opioid addiction treatment have evolved inBC, Canada, and internationally; and the evidencebase supporting elimination of barriers to accessingbuprenorphine/naloxone in BC. Specifically, thebest available evidence strongly supports a potentialmove by the CPSBC to remove the requirementthat BC physicians must hold an exemption undersection 56 of the Controlled Drugs and Substances Act (e.g., a “methadone exemption”) in order toprescribe buprenorphine/naloxone. In addition, the
evidence supports primary care and community-based physicians having a more prominent rolein prescribing buprenorphine/naloxone for thetreatment of opioid use disorder, and adoption
of the dosing recommendations from the drug’sproduct monograph in provincial opioid agonisttreatment program regulations and guidance.
Scope of the Problem. Surveillance data from theBC Coroners Service spanning 2006–2015 show asubstantial increase in overdose deaths attributableto illicit drugs, including non-prescribedprescription opioid medications and heroin (Figure1). In 2015, 480 illicit drug overdoses were reportedacross BC, representing a 31% increase from 2014. This translates to a mortality rate of 10.2 deaths per100,000 population. Similarly high rates have notbeen observed since the 1990s during the heightof the intravenous heroin epidemic in Vancouver. ,
Although all provincial health regions showed anincrease in overdose deaths, those outside of metroVancouver were hit hardest, with the Interior andFraser Health Authorities reporting a 30% and 50%increase in fatalities in the past year, respectively. These trends have continued into early 2016. In themonth of January alone, 76 overdose deaths werereported in the province—the largest number ofdeaths in a single month in almost a decade.
In response to the significant rise in illicitdrug-related overdoses, and projections that
approximately 700–800 overdose deaths areexpected this year if trends continue unabated,provincial health officer Dr. Perry Kendall hasdeclared a public health emergency. This is thefirst time a provincial health officer has servednotice under the Public Health Act to exerciseemergency powers, re ecting the severity of thecurrent situation and the urgent need for collectiveaction. BC is the only province in Canada to takethis action to address the illicit drug overdosecrisis, which will allow medical health officersthroughout the province to collect robust, real-time
information on overdoses to immediately identifylocalized patterns of risk, permitting immediateintervention to prevent serious harms and deathsamong people who use drugs.

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 4/20
4May 2016
The recent emergence of fentanyl in the illicit drugmarket has contributed to the rise in overdosedeaths, and is a pressing public health concern.Specifically, this highly potent synthetic opioidhas been increasingly used to replace and/or“cut” heroin, oxycodone, and other illicit opioids.Fentanyl can be 50–100 times more toxic thanmorphine and is often ingested unknowingly, posingsubstantially higher risks of overdose-related harmsand death than heroin or other illicit opioids. Preliminary data suggest that the proportion ofillicit drug overdose deaths involving fentanyl (aloneor in combination with other drugs) has rapidlyincreased from 5% in 2012 to approximately 30%in 2015. Of the 200 overdose deaths that occurredfrom January 1 to March 31 of this year, fentanyl hasbeen detected in 98 cases (49%).
While not all people who use opioids meet thecriteria for opioid use disorder (i.e., addiction), it iscritically important to expand access to addiction
care and treatment for high-risk opioid users, inorder to reduce overdose deaths in the province,and to target emerging threats to public safety suchas the fentanyl trade.
Regulation of Treatment Options for OpioidUse Disorder. There are currently two rst-linepharmaceutical options available in BC for thetreatment of opioid use disorder: methadoneand buprenorphine/naloxone (e.g., Suboxone®).Methadone is a long-acting synthetic opioid thatacts as a mu (μ) opioid receptor agonist. In BC, it isadministered as an oral solution (e.g., Methadose®).When administered at a therapeutic dosage,
methadone prevents opioid withdrawal, reducesopioid craving, blocks the euphoric e ects of otheropioids, and reduces mortality. Methadone has beenavailable in Canada for treating opioid use disordersince the 1960s, although regulations were initially
very restrictive. Federal regulations for methadone were relaxed in the 1990s, expanding access totreatment in an e ort to reduce drug-related harmsand HIV-transmission associated with injectionopioid use, which had reached epidemic levelsin Vancouver’s Downtown Eastside. Currently,methadone is classified as a controlled drug in
accordance with section 56 of the ControlledDrugs and Substances Act, requiring physicians tobe authorized to prescribe the medication via anexemption from the Federal Department of Health
0
100
200
300
400
500
N u m
b e r o
f D e a t h s
0
2
4
6
8
10
14
12 D e a t h
R a t e p er 1
0 0 , 0 0 0 P
o p ul a
on
Deaths
Rate
1989 • • • • • • • • • • • • •1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 2013 2015
64 117 354 217 300 236 236 190 230 202 201 292 33080 162 308 301 400 236 172 183 229 183 211 274 366 480
2.0 3.5 9.9 5.7 7.6 6.8 5.8 4.6 5.5 4.7 4.6 6.5 7.22.4 4.7 8.4 7.8 10.0 5.8 4.2 4.4 5.4 4.2 4.7 6.0 7.9 10.2
Number of deaths and mortality rate a ributed toillicit drug use in Bri sh Columbia, 1989–2015.
Figure 1
Source: Illicit Drug Overdose Deaths in BC, January 1 2007–April 30 2016. Office of the Chief Coroner of BC. Released May 3, 2016.

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 5/20
5May 2016
Canada. BC has bene ted from a well-establishedmethadone maintenance program for the treatmentof opioid use disorder, which is stewarded by anappointed panel of the CPSBC.
In recent years, buprenorphine/naloxone hasemerged as viable alternative to methadone fortreating opioid use disorder. Health Canadafirst approved buprenorphine/naloxone for thetreatment of opioid dependence in adults in 2007.Buprenorphine/naloxone is a combined formulationof buprenorphine, a partial mu-receptor agonist,and naloxone, an opioid antagonist, which isadministered as a sublingual tablet. Buprenorphineacts to prevent opioid withdrawal and craving,
while the inclusion of naloxone is intended todeter non-medical injection and diversion. Whenbuprenorphine/naloxone is taken as directed in
sublingual form, its naloxone component hasnegligible bioavailability and the therapeutice ect of buprenorphine predominates. However,if diverted for injection use via subcutaneous,intramuscular, or intravenous routes, sufficientnaloxone is absorbed to induce some withdrawalsymptoms in active opioid users. Physicianrequirements to prescribe buprenorphine/naloxoneare determined at the provincial level, typicallyby the College of Physicians and Surgeons oran equivalent provincial licensing body. In BC,recommendations regarding buprenorphine/ naloxone administration are under the purview of
the CPSBC. As full y outl ined in Tables 1 and 2 in theappendices, there is considerable variability acrossCanadian provinces in regulatory and educationalrequirements for physicians to prescribebuprenorphine/naloxone, and several key issues areevident on review of the national situation. First,prescriber restrictions and requirements have notbeen systematically described or scrutinized inan evidence-informed manner. Second, in somecases, this has led to provincial program decisionsthat are based on existing infrastructure (i.e.,
Provincial Methadone Maintenance Programs),incomplete information, and/or apparent lack ofknowledge about relative safety of methadone
versus buprenorphine/naloxone. Third, practice and
policy for buprenorphine/naloxone administrationurgently needs to be updated to re ect the bestavailable science. Prioritizing implementation ofevidence-based policy for buprenorphine/naloxoneadministration in BC will provide patients and
families access to a wider range of safe and e ectivecare options, and will have a more meaningfulpopulation-level impact on the provincialopioid crisis. With the anticipated changes tobuprenorphine/naloxone prescriber restrictions, BC will join several other provinces in Canada that haveadopted less restrictive, evidence-based prescribingregulations (Appendix Table 1).
Research evidence clearly supports the role ofbuprenorphine/naloxone as a rst-line treatmentoption for opioid use disorder. Clinical trialsand systematic reviews consistently demonstrate
that buprenorphine/naloxone offers comparabletreatment outcomes, with fewer side effectsand drug interactions, lower health risks ofdiversion (i.e., use by individuals who do not havea prescription), and signi cant safety advantagesin comparison to methadone. Buprenorphine/ naloxone also demonstrates significant efficacyand favorable safety and tolerability in specificpopulations, including youth and prescriptionopioid-dependent individuals. However,buprenorphine/naloxone remains criticallyunderutilized in BC (Figure 2) for a number ofreasons, including: a lack of skilled addiction careproviders and evidence-based clinical practice
guidelines for treatment of opioid use disorder;and traditionally, restrictions on who can prescribethis medication. Historically, only a small subset ofBC physicians have been authorized to prescribebuprenorphine/naloxone, as per requirements set bythe CPSBC that prescribers must hold a methadoneexemption. In coming months, it is expected therequirement that physicians must hold a Section 56exemption to prescribe buprenorphine/naloxone will be eliminated by the CPSBC. This changeis well supported by research evidence, as will be
detailed below, as well as considerable public healthbene ts achieved in other jurisdictions that haveadopted buprenorphine/naloxone as a first-linetreatment for opioid use disorder.

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 6/20
6May 2016
In recent years, concerted e orts have been madeto address gaps in the provision of evidence-based treatment and care for substance usedisorders, including the ongoing developmentof comprehensive addiction medicine trainingprograms and the dissemination of theVancouver Coastal Health/Providence HealthCare Guidelines for the Clinical Management ofOpioid Use Disorder to clinical sites across theprovince. As well, as mentioned above, inclusionof buprenorphine/naloxone as a rst-line treatmenteligible for PharmaCare coverage will improveaccess and provide individualized options for
treating opioid use disorder. These achievementsbring focus to remaining barriers within theprovince, and an opportunity for continued
advancement through upcoming changes tobuprenorphine/naloxone prescriber restrictions.
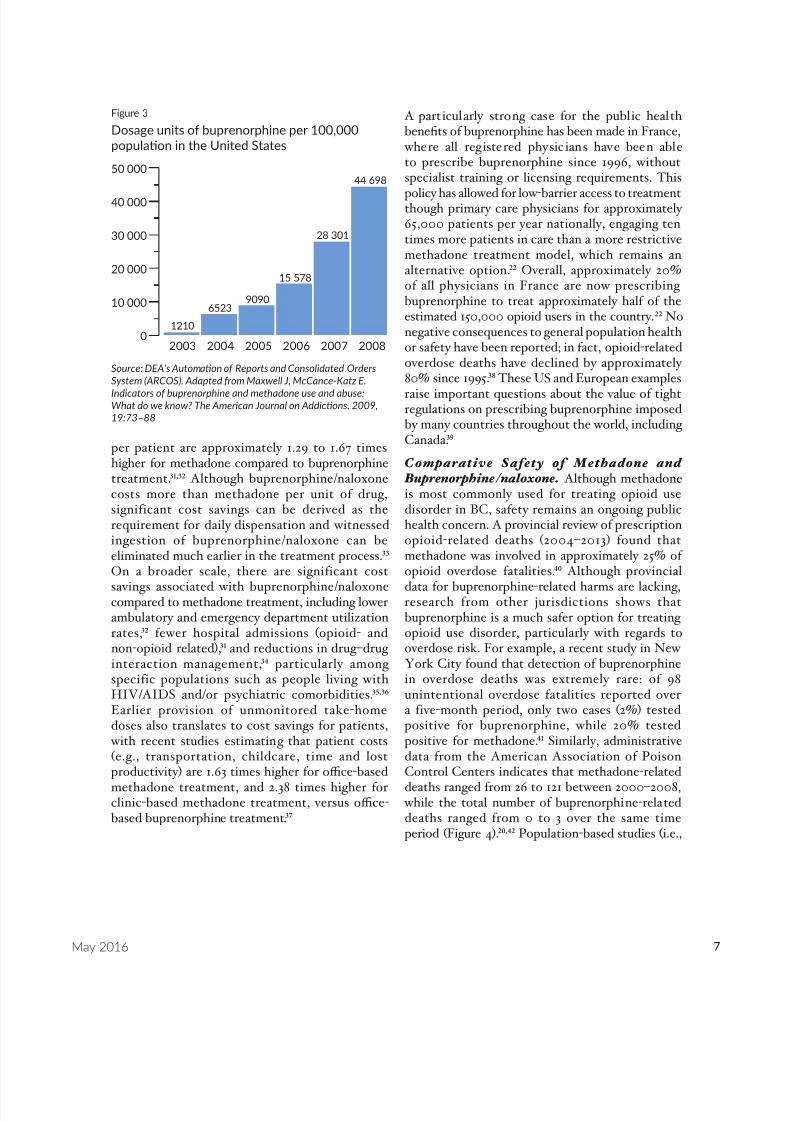
Experience from Other Jurisdict ions where Buprenorphine/naloxone is Widely Prescribed. Although not yet widely used across Canada,buprenorphine * use in the US has rapidly expandedover the past decade. Between 2003 and 2008,there was an approximately 35-fold increase in thenumber of buprenorphine dosage units distributedto US pharmacies (Figure 3). In parallel, between2006 and 2010, there was an approximately ve-fold increase in the number of individuals receivingbuprenorphine prescriptions on an outpatient basisfrom primary care or office-based physicians. , This transition has largely been driven by “TheDrug Addiction Treatment Act” (2000), whichenabled all primary care physicians to administer
buprenorphine following completion of a shortonline training course, effectively mobilizingphysicians to become active partners in thediagnosis and treatment of opioid use disorder.Increased uptake of buprenorphine for treatmentof opioid use disorder has subsequently beenassociated with considerable public health bene ts,in the US and beyond, including: reductions inopioid-related overdose deaths; , decreased illicitopioid and other drug use; – and decreased HIVrisk behaviours. , In addition, the ability to treatopioid use disorder in primary care settings hasbeen shown to improve other health outcomes such
as the identi cation and treatment of other chronicmedical conditions.
Th e emp hasis on prioriti zing access tobuprenorphine for treating opioid use disorder hasresulted in considerable health system cost-savingsin the US. Studies have demonstrated that over the
rst six months of treatment, total healthcare costs* Note: In the US and other jurisdictions, buprenorphinemonotherapy (e.g., Subutex ® ) is an approved treatment for opioidaddiction, although the combined formulation of buprenorphine/ naloxone is predominantly used for this indication. In thisdocument, the term “buprenorphine” represents data for bothproducts unless otherwise speci ed. In Canada, buprenorphine
monotherapy is not approved for the treatment of opioidaddiction and is only available through the Special AccessProgramme, which provides access to non-marketed drugs fortreating patients with serious or life-threatening conditions whenconventional therapies have failed, are unsuitable, or unavailable.
0
2 000
4 000
6 000
8 000
10 000
12 000
14 000
16 000 Methadone
Buprenorphine
2010/2011
2011/2012
2012/2013
2013/2014
12 664 13 856 14 800 15 418338 995 1481 2000
C u
m u
l a v
e P a e n t C o u
n t
MethadoneBuprenorphine
Figure 2
Number of pa ents prescribed methadone orbuprenorphine in Bri sh Columbia, 2010–2014.
Source: BC Opioid Subs tu on Treatment System PerformanceMeasures, 2013/2014. Office of the Provincial Health Minister,Bri sh Columbia Ministry of Health. Released July 2015.
8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 7/20
7May 2016
per patient are approximately 1.29 to 1.67 timeshigher for methadone compared to buprenorphinetreatment. , Although buprenorphine/naloxonecosts more than methadone per unit of drug,significant cost savings can be derived as therequirement for daily dispensation and witnessedingestion of buprenorphine/naloxone can beeliminated much earlier in the treatment process. On a broader scale, there are significant cost
savings associated with buprenorphine/naloxonecompared to methadone treatment, including lowerambulatory and emergency department utilizationrates, fewer hospital admissions (opioid- andnon-opioid related), and reductions in drug–druginteraction management, particularly amongspecific populations such as people living withHIV/AIDS and/or psychiatric comorbidities. , Earlier provision of unmonitored take-homedoses also translates to cost savings for patients,
with recent studies estimating that patient costs(e.g., transportation, childcare, time and lostproductivity) are 1.63 times higher for o ce-basedmethadone treatment, and 2.38 times higher forclinic-based methadone treatment, versus o ce-based buprenorphine treatment.
A particularly strong case for the public healthbene ts of buprenorphine has been made in France,
where all registered physicians have been ableto prescribe buprenorphine since 1996, withoutspecialist training or licensing requirements. This
policy has allowed for low-barrier access to treatmentthough primary care physicians for approximately65,000 patients per year nationally, engaging tentimes more patients in care than a more restrictivemethadone treatment model, which remains analternative option. Overall, approximately 20%of all physicians in France are now prescribingbuprenorphine to treat approximately half of theestimated 150,000 opioid users in the country. Nonegative consequences to general population healthor safety have been reported; in fact, opioid-relatedoverdose deaths have declined by approximately80% since 1995. These US and European examplesraise important questions about the value of tightregulations on prescribing buprenorphine imposedby many countries throughout the world, includingCanada.
Comparative Safety of Methadone and Buprenorphine/naloxone. Although methadoneis most commonly used for treating opioid usedisorder in BC, safety remains an ongoing publichealth concern. A provincial review of prescriptionopioid-related deaths (2004–2013) found thatmethadone was involved in approximately 25% ofopioid overdose fatalities. Although provincial
data for buprenorphine-related harms are lacking,research from other jurisdictions shows thatbuprenorphine is a much safer option for treatingopioid use disorder, particularly with regards tooverdose risk. For example, a recent study in NewYork City found that detection of buprenorphinein overdose deaths was extremely rare: of 98unintentional overdose fatalities reported overa five-month period, only two cases (2%) testedpositive for buprenorphine, while 20% testedpositive for methadone. Similarly, administrativedata from the American Association of PoisonControl Centers indicates that methadone-relateddeaths ranged from 26 to 121 between 2000–2008, while the total number of buprenorphine-relateddeaths ranged from 0 to 3 over the same timeperiod (Figure 4). , Population-based studies (i.e.,
Figure 3
Dosage units of buprenorphine per 100,000popula on in the United States
0
10 000
20 000
30 000
40 000
50 000
1210
65239090
15 578
28 301
44 698
2003 2004 2005 2006 2007 2008
Source: DEA’s Automa on of Reports and Consolidated OrdersSystem (ARCOS). Adapted from Maxwell J, McCance-Katz E.
Indicators of buprenorphine and methadone use and abuse:What do we know? The American Journal on Addic ons. 2009,19:73–88

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 8/20
8May 2016
including individuals receiving treatment andthe general public) from Australia and the UKhave found a four- and six-fold higher risk offatal overdose for methadone compared tobuprenorphine, respectively. ,
In terms of non-fatal safety risks, a recentUS study reported that the number of callsto Poison Control for methadone-relatedissues was 6.7 times higher than calls forbuprenorphine-related issues. Of these,nearly double the proportion of methadone-related calls were associated with major life-threatening events or events requiring medicalattention compared to buprenorphine (46.8% versus 25.8%) . Overall, buprenorphine-related emergency department (ED) visitsrepresent a small proportion of all drug-related ED visits in the US, and are mostcommonly associated with self-managementof withdrawal symptoms, – attempts to ceaseillicit drug use, and/or non-serious adverseevents shortly after initiation of treatment(e.g., precipitated withdrawal).
These pa tterns of increased ri sk withmethadone are largely driven by theincreased propensity for methadone totrigger respiratory depression. Specifically,methadone doses that exceed the threshold
lethal dose for opioid-naïve adults areroutinely prescribed to opioid-tolerantpatients in opioid agonist treatment programsto adequately control withdrawal symptoms.In comparison, the standard therapeuticbuprenorphine/naloxone dose is generally wellbelow the threshold lethal dose and confersa much lower risk of respiratory depressionand fatal overdose. As well, methadone hasa higher potential for dangerous interactions
with alcohol and many common medications(e.g., antibiotics, antifungals, antidepressants,antiretroviral drugs), as well as increasedrisk of cardiac arrhythmias as a result of QTprolongation compared to buprenorphine/ naloxone. While relatively less common,buprenorphine/naloxone-related overdosefatalities are most often the result ofcombined use with other central nervous
system depressants, such as alcoholand benzodiazepines, – or in thecontext of intentional self-harm(e.g., suicide attempts where supra-therapeutic doses are intentionallytaken). Taken together, this
research evidence, and the datadepicted in Figure 3 and Figure4, demonstrate the negligiblee ects of increased buprenorphineprescribing on rates of mortalityand other harms, which must bebalanced alongside proven publichealth benefits, and the relativerisks associated with methadone.
Contributing to safety risksassociated with opioid agonisttreatment is the potential for
diversion, that is, consumptionby an individual without aprescription. For example, a UK- wide analysis of methadone-related
Figure 4
Number of methadone and buprenorphine deathsreported to US poison control centres.
Source: Na onal Poison Data System, American Associa on of PoisonControl Centers. Adapted from Maxwell J, McCance-Katz E. Indicatorsof buprenorphine and methadone use and abuse: What do we know?The American Journal on Addic ons. 2009, 19:73–88
0
30
60
90
120
150
Buprenorphine
Methadone
BuprenorphineMethadone
026
035
058
044
275
184
3108
1121
2103
2000 2001 2002 2003 2004 2005 2006 2007 2008
N u
m b e r o f d e a t h
s

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 9/20
9May 2016
deaths found that only 36% were among individualsknown to be receiving methadone treatment. Thisis consistent with reports from Australia, Europe,and the US, which have found that up to 50% ofoverdose deaths involving methadone are the result
of diversion., ,
These deaths are a function ofthe high potency and toxicity of methadone whenused outside of a closely monitored setting, as wellas its known street value. Although diversion is stilla concern with buprenorphine, the fact that it is apartial opioid agonist, and is typically prescribed inCanada in the combined formulation with naloxone,
greatly limits risks.
Prior research also indicates that most people whouse diverted or street-obtained buprenorphine/ naloxone are opioid users primarily intending toself-medicate withdrawal symptoms rather thanseeking euphoric e ects. , , – Strong predictorsof buprenorphine/naloxone diversion includeinability to access opioid agonist therapy programsand suboptimal dosing for those who are engaged incare. , – Of note, there is no evidence that tightercontrols or dose monitoring reduce diversion, as illustrated by a recent study of all opioidagonist treated patients in Finland that foundunsupervised take-home buprenorphine doses werenot associated with increased risk of diversion toothers. In fact, studies have found that patients
with prior use of non-prescribed buprenorphine are
more likely to enter addiction treatment and havesigni cantly higher odds of remaining in treatmentcompared to patients who are buprenorphine-naïve upon treatment entry. Therefore, e orts tominimize diversion must take this evidence baseinto consideration and avoid undermining thepositive patient and public health bene ts that canbe gained from expanded treatment access.
Nevertheless, to address concerns regardingbuprenorphine/naloxone diversion, there aremechanisms that prescribing physicians canroutinely employ, and that regulatory agencies
(e.g., CPSBC) can help enforce, including periodicurine drug screens to confirm the presence ofbuprenorphine and other illicit drugs to assesspatient stability, as well as closely monitoring
buprenorphine/naloxone use via unannounced pillcounts to assess for and limit potential for diversion.
Growing consensus among experts andopinion leaders has culminated in high-levelrecommendations that buprenorphine/naloxoneshould be routinely considered as a first-linepharmacotherapy option for opioid use disorder,
given its superior safety profile with respect tooverdose risk compared to methadone. – Thiscumulative safety evidence has also led to recentrevisions to the buprenorphine/naloxone productmonograph that remove the requirement for atwo-month period of daily witnessed ingestion,thereby allowing provision of take-home dosingat the judgment of the treating physician (e.g.,as soon as the patient has demonstrated clinicalstability and ability to safely store buprenorphine/
naloxone at home). The CPSBC has not yet revisedtheir current recommendation that patients mustundergo at least two months of daily witnessedingestion before take-home doses are permitted.To our knowledge, no other Canadian jurisdictionhas enforced take-home dosing restrictions thatare inconsistent with the updated Health Canada-approved product monograph or that mirror thoseof methadone. In light of this, the CPSBC shouldconsider revising guidance to remove this additionalbarrier to accessing care, permitting take-homedoses at the discretion of the treating physician.
Recommendations. Collective action is neededto address increasing rates of serious harms anddeaths associated with opioid use in BC. In lightof the public health emergency declaration, it ismore important than ever before to accelerate thetransfer of research evidence into systemic policyand practice change. BC has shown leadershipin several priority areas related to preventingopioid-related harms, including establishment ofsupervised injection sites and take-home naloxoneprograms, and the addition of buprenorphine/ naloxone to the PharmaCare formulary. Theanticipated deregulation of buprenorphine/
naloxone prescribing provides an opportunity toshow continued leadership, through expansion ofphysician and patient access to a medication withproven safety and effectiveness in treatment of

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 10/20
10May 2016
opioid use disorder. To optimize impact, educationefforts that build or enhance professional andpublic knowledge of the comparative risks andbene ts of this medication should be prioritized,as should dissemination of evidence-based practice
guidelines. As has been demonstrated in otherjurisdictions, expanding buprenorphine/naloxoneprescribing to primary care and community-basedphysician practices can lead to considerable publichealth benefits due to proven safety advantagesand lower risks of diversion relative to methadone.Based on the above evidence, it is recommendedthat:
1. Buprenorphine/naloxone should be routinelyo ered as a rst-line pharmacotherapy option(as an alternative to methadone) for opioiduse disorder, given its superior safety pro le
with respect to overdose risk compared tomethadone.
2. The requirement that BC physicians must holda methadone exemption in order to prescribebuprenorphine/naloxone should be eliminated.This review fully supports the CPSBC in itsdeliberations to remove this requirement.In lieu of the methadone exemption, it isrecommended that prescribers should bedirected to complete the existing onlinetraining module on buprenorphine/naloxoneprescribing, but not required, in order tooptimize the number of prescribing physiciansin the province.
3. Evidence-based guidelines for buprenorphine/ naloxone treatment that are tailored to clinicalpractice in BC, such as the Vancouver CoastalHealth/Providence Health Care Guidelinefor the Clinical Management of Opioid
Addiction, should be widely disseminated and
implemented to support best practices amongnew physician prescribers.
4. Publ ic and profess ional educat ioncampaigns designed to increase knowledgeof buprenorphine/naloxone as a first-linetreatment option for opioid use disorder,and the risks and bene ts of this medicationrelative to methadone, should be prioritized.
5. Provincial recommendations for take-homedosing of buprenorphine/naloxone shouldbe identical to those on the buprenorphine/ naloxone product monograph: the requirementfor a two-month period of daily witnessedingestion should be removed from provincialOAT program guidelines, allowing provisionof take-home dosing at the judgment of thetreating physician.
6. Research and education aimed at reducing thediversion of opioid agonist therapies should besupported. The development of educationalresources and programmatic strategies thatsupport prescribers in assessment, riskreduction and prevention of opioid agonistdiversion should be prioritized.
British Columbia is at a critical juncture inour approach to preventing, identifying andtreating opioid use disorder. Removing barriersto accessing proven safe and e ective treatmentsis a key component of a broader strategy tocombat the opioid crisis. Supporting anticipatedregulatory changes and implementing the aboverecommendations has the potential to substantiallyimprove patient and provider access to much-needed options for care, and would likely have ameaningful impact on the health and well-being ofthe many British Columbians a ected by opioid usedisorders.
8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 11/20
11May 2016
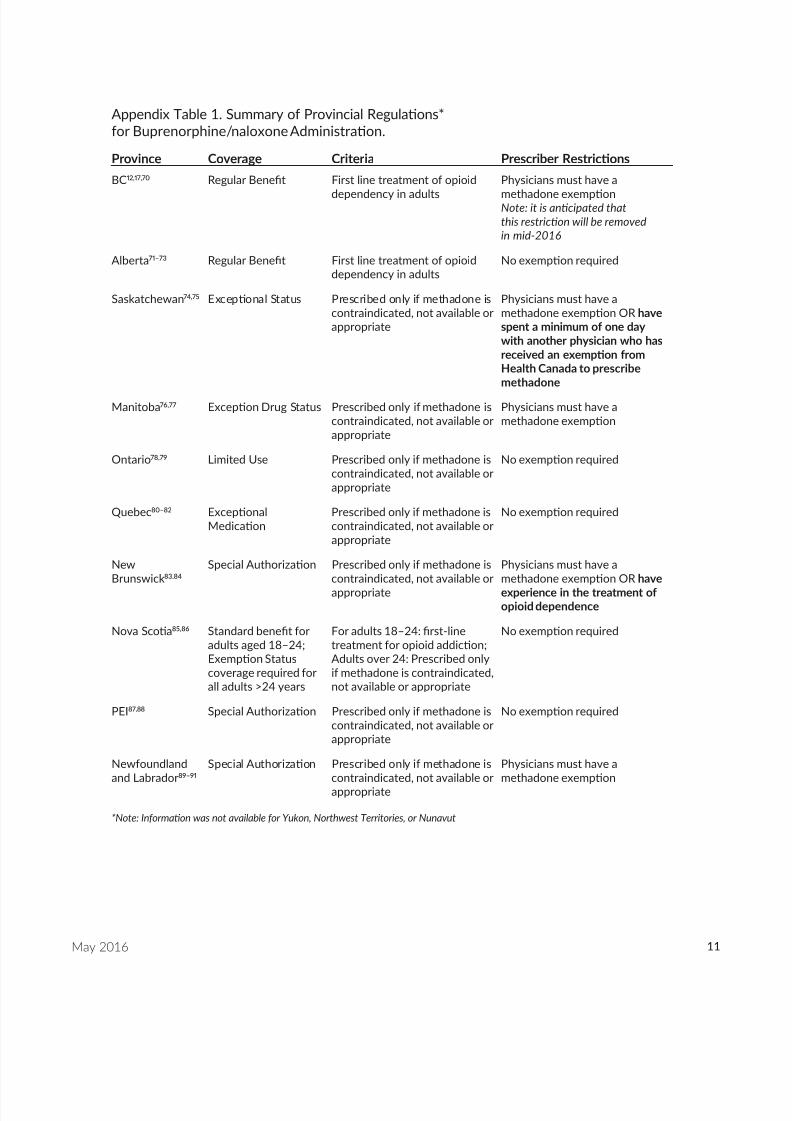
Appendix Table 1. Summary of Provincial Regula ons*for Buprenorphine/naloxone Administra on.
Province Coverage Criteria Prescriber Restric ons
BC12,17,70 Regular Bene t First line treatment of opioid
dependency in adults
Physicians must have a
methadone exemp onNote: it is an cipated thatthis restric on will be removedin mid-2016
Alberta 71–73 Regular Bene t First line treatment of opioiddependency in adults
No exemp on required
Saskatchewan 74,75 Excep onal Status Prescribed only if methadone iscontraindicated, not available orappropriate
Physicians must have amethadone exemp on OR havespent a minimum of one daywith another physician who hasreceived an exemp on fromHealth Canada to prescribemethadone
Manitoba 76,77 Excep on Drug Status Prescribed only if methadone iscontraindicated, not available orappropriate
Physicians must have amethadone exemp on
Ontario 78,79 Limited Use Prescribed only if methadone iscontraindicated, not available orappropriate
No exemp on required
Quebec 80–82 Excep onalMedica on
Prescribed only if methadone iscontraindicated, not available orappropriate
No exemp on required
NewBrunswick 83,84
Special Authoriza on Prescribed only if methadone iscontraindicated, not available orappropriate
Physicians must have amethadone exemp on OR haveexperience in the treatment ofopioid dependence
Nova Sco a 85,86 Standard bene t foradults aged 18–24;Exemp on Statuscoverage required forall adults >24 years
For adults 18–24: rst-linetreatment for opioid addic on;Adults over 24: Prescribed onlyif methadone is contraindicated,not available or appropriate
No exemp on required
PEI87,88 Special Authoriza on Prescribed only if methadone iscontraindicated, not available orappropriate
No exemp on required
Newfoundlandand Labrador 89–91
Special Authoriza on Prescribed only if methadone iscontraindicated, not available orappropriate
Physicians must have amethadone exemp on
*Note: Informa on was not available for Yukon, Northwest Territories, or Nunavut

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 12/20
12May 2016
Appendix Table 2. Summary of Provincial Educa onal and Training Requirements*to Prescribe Buprenorphine/naloxone.
Province Educa on & Prac ce Requirements
Bri shColumbia 12,17
• The physician must hold a methadone exemp on to prescribe buprenorphine/naloxonefor opioid use disorder
• The current requirements for obtaining an authoriza on to prescribe methadone for opioiduse disorder are: ◦ a endance at the Methadone 101 Workshop sponsored by the College ◦ familiariza on with the Methadone Maintenance Program: Clinical Prac ce Guideline ◦ a preceptorship sa sfactory to the Methadone Maintenance Program ◦ an acceptable review of your prescrip on pro le from the PharmaNet database ◦ an interview with a member of the registrar sta ◦ an agreement to undertake a minimum of 12 hours of con nuing medical educa on
(CME) in addic on medicine each year ◦ an agreement to provide a er-hours contact informa on regarding your methadone
maintenance pa ents ◦ an agreement to undergo a prac ce assessment of your methadone maintenance
prac ce within the rst year• Addi onal requirements for obtaining an authoriza on to prescribe
buprenorphine/naloxone for opioid use disorder are: ◦ Physicians must have completed the online educa on module by Schering-Plough
Canada available at www.suboxonecme.ca. Comple on of this module is based on anhonour system, and will not be veri ed except in unusual circumstances
◦ Buprenorphine/naloxone must be prescribed on a duplicate prescrip on pad
Alberta 72,73 • The physician does not need to hold a methadone exemp on to prescribebuprenorphine/naloxone for opioid use disorder
• The current requirements for obtaining an authoriza on to prescribebuprenorphine/naloxone for opioid use disorder: ◦ Ini a on: Comple on of accredited buprenorphine course: www.suboxonecme.ca,
CAMH Opioid Dependence Treatment Core course or other equivalent courseapproved by CPSA. Physician must provide con rma on of course comple on to theCPSA. Must have experience in trea ng opioid use disorder: (postgraduate training,ODT experience, professional cer ca on with CSAM/ASAM or equivalent approvedby CPSA)
◦ Maintenance: Comple on of accredited buprenorphine course: www.suboxonecme.ca, the CAMH Opioid Dependence Treatment Core course or other equivalent courseapproved by CPSA. Physician must provide con rma on of course comple on to theCPSA. Must have a rela onship with a physician experienced in trea ng opioid usedisorder (postgraduate training, ODT experience, cer ca on with CSAM/ASAM orequivalent approved by CPSA)
◦ Temporary prescribing for hospital/incarcerated pa ents: Temporary buprenorphineprescribing physicians will be permi ed to maintain the same buprenorphine dosewithout comple on of a buprenorphine prescribing course. A temporary prescribingphysician must consult with a physician experienced in the treatment of opioiddependency for any dose changes. Must have a rela onship with physician experiencedin treatment of opioid use disorder (postgraduate training, ODT experience,cer ca on with CSAM/ASAM or equivalent approved by CPSA)

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 13/20
13May 2016
Saskatchewan 75 • The physician must hold a methadone exemp on to prescribe buprenorphine/naloxonefor opioid use disorder or have spent a minimum of one day with another physician whohas received an exemp on from Health Canada to prescribe methadone.
• The current requirements for obtaining an authoriza on to prescribe methadone for opioiduse disorder are: ◦ Physician must have license to prac ce medicine in Saskatchewan ◦ Ini a on:
▪ Comple on of MMT workshop/course recognized by CPSS ▪ Direct training (2 days) with experienced, CPSS approved ini a ng physician ▪ Documenta on of clinical competence ▪ College approved mentorship for rst two years of prac ce
▪ Must pursue ongoing educa on relevant to MMT▪ Must access PIP viewer prescribing database ▪ An interview with a member of the registrar sta ▪ Must have access to laboratory services and a pharmacy ▪ Must be limited to 50 pa ents un l rst audit
◦ Maintenance:▪ Comple on of MMT workshop/course recognized by the CPSS▪ Must have an ongoing associa on with experienced ini a ng physician▪ Must access PIP viewer prescribing database ▪ An interview with a member of the registrar sta
◦ Temporary Prescribing:▪ Must consult CPSS if ini a ng physician is not available ▪ Must only prescribe for dura on of pa ents hospital admission ▪ Must not prescribe carried doses ▪ Prior to pa ent discharge, temporary prescribing physician must collaborate with
ini a ng or maintaining physician.• Addi onal requirements for prescribing buprenorphine/naloxone for opioid use disorder
include: ◦ Comple on of the online educa on module — www.suboxonecme.ca ◦ Physicians must have training and interest in addic on medicine ◦ Buprenorphine/naloxone prescrip ons must be wri en on the physician’s personalized
prescrip on pad/CPSS approved electronic prescribing
Manitoba 76 • The physician must hold a methadone exemp on to prescribe buprenorphine/naloxonefor opioid use disorder
• The current requirements for obtaining an authoriza on to prescribe methadone for opioiduse disorder are:◦ Comple on of CAMH Course: Opioid Dependence Treatment Core Course ◦ A one day clinical observership of opioid dependency prac ce
◦ Comple on of several supervised shi s in a methadone/buprenorphine clinic(minimum of 4 half days)
◦ Alterna vely, extensive experience in methadone/buprenorphine addic on prac ce inanother province
• Addi onal Requirements for prescribing buprenorphine/naloxone for opioid use disorderinclude:◦ Comple on of CAMH course: Buprenorphine-Assisted Treatment of Opioid
Dependence: An Online Course for Front-Line Clinicians ◦ Comple on of buprenorphine/naloxone Educa on Program Online course
www.suboxonecme.ca
8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 14/20
14May 2016
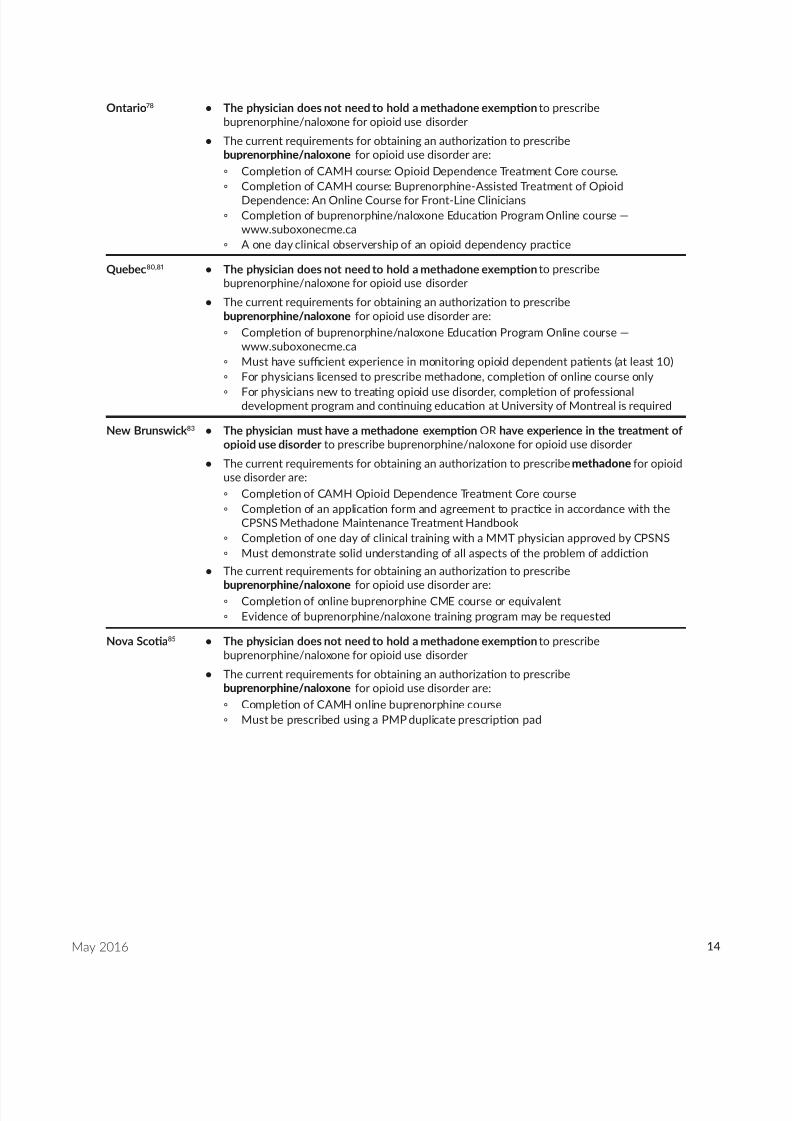
Ontario 78 • The physician does not need to hold a methadone exemp on to prescribebuprenorphine/naloxone for opioid use disorder
• The current requirements for obtaining an authoriza on to prescribebuprenorphine/naloxone for opioid use disorder are:◦ Comple on of CAMH course: Opioid Dependence Treatment Core course.◦ Comple on of CAMH course: Buprenorphine-Assisted Treatment of Opioid
Dependence: An Online Course for Front-Line Clinicians ◦ Comple on of buprenorphine/naloxone Educa on Program Online course —
www.suboxonecme.ca ◦ A one day clinical observership of an opioid dependency prac ce
Quebec 80,81 • The physician does not need to hold a methadone exemp on to prescribebuprenorphine/naloxone for opioid use disorder
• The current requirements for obtaining an authoriza on to prescribebuprenorphine/naloxone for opioid use disorder are: ◦ Comple on of buprenorphine/naloxone Educa on Program Online course —
www.suboxonecme.ca ◦ Must have su cient experience in monitoring opioid dependent pa ents (at least 10) ◦ For physicians licensed to prescribe methadone, comple on of online course only
◦ For physicians new to trea ng opioid use disorder, comple on of professionaldevelopment program and con nuing educa on at University of Montreal is required
New Brunswick 83 • The physician must have a methadone exemp on OR have experience in the treatment ofopioid use disorder to prescribe buprenorphine/naloxone for opioid use disorder
• The current requirements for obtaining an authoriza on to prescribe methadone for opioiduse disorder are:◦ Comple on of CAMH Opioid Dependence Treatment Core course ◦ Comple on of an applica on form and agreement to prac ce in accordance with the
CPSNS Methadone Maintenance Treatment Handbook ◦ Comple on of one day of clinical training with a MMT physician approved by CPSNS
◦ Must demonstrate solid understanding of all aspects of the problem of addic on• The current requirements for obtaining an authoriza on to prescribe
buprenorphine/naloxone for opioid use disorder are: ◦ Comple on of online buprenorphine CME course or equivalent
◦ Evidence of buprenorphine/naloxone training program may be requested
Nova Sco a 85 • The physician does not need to hold a methadone exemp on to prescribebuprenorphine/naloxone for opioid use disorder
• The current requirements for obtaining an authoriza on to prescribebuprenorphine/naloxone for opioid use disorder are: ◦ Comple on of CAMH online buprenorphine course
◦ Must be prescribed using a PMP duplicate prescrip on pad

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 15/20
15May 2016
PEI 87,88 • The physician does not need to hold a methadone exemp on to prescribebuprenorphine/naloxone for opioid use disorder
• The current requirements for obtaining an authoriza on to prescribebuprenorphine/naloxone for opioid use disorder are: ◦ An unrestricted license for independent prac ce in the province of Prince Edward
Island, in good standing with no relevant condi ons or restric ons ◦ No current inves ga ons with regard to prescribing opioids or record keeping ◦ No previous ndings of professional misconduct or previous legal ndings with regard
to opioids or record keeping ◦ Ongoing educa on relevant to prescribing buprenorphine for opioid dependency
including:▪ Comple on of Buprenorphine/naloxone Educa on Program available online —
www.suboxonecme.ca ▪ Comple on of a recognized course on the fundamentals of addic on medicine
within rst two years of commencing prescribing ▪ Comple on of a minimum of 20 hours of formal CME in some aspect of addic on
medicine every ve years ▪ Comple on with signature of form en tled Commitment by Physicians who
Undertake Buprenorphine Treatment for Opioid Dependency
Newfoundlandand Labrador 89,90
• The physician must have a methadone exemp on to prescribe buprenorphine/naloxonefor opioid use disorder
• The current requirements for obtaining an authoriza on to prescribebuprenorphine/naloxone for opioid use disorder are: ◦ Obtain Methadone Exemp on according to Sec on 56 of Controlled Drugs and
Substances Act◦ Comple on of Buprenorphine prescrip on training program approved by college ◦ Par cipa on in con nuing medical educa on in opioid-dependence treatment ◦ Comple on of minimum one-day clinical observership at the Opioid Treatment Centre
in province
*Note: Informa on was not available for Yukon, Northwest Territories, or Nunavut

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 16/20
16May 2016
References1. British Columbia Ministry of Health. “BC increases access
to addiction treatment Suboxone.” BC Government News,October 13, 2015. Available at: https://news.gov.bc.ca/09543.(Accessed April 26 2016).
2. Suboxone (bupreno rphine and naloxon e) product
monograph. Indivior UK Limited: Berkshire, UK. ControlNo. 178168. 2015.3. BC Ministry of Justice, BC Coroners Service. “Illicit Drug
Overdose Deaths in BC, 2006–2015.” Released January 6,2015. Burnaby, BC: O ce of the Chief Coroner.
4. BC Ministry of Justice, BC Coroners Service. “Illicit DrugOverdose Deaths in BC, January 1 2007–April 30 2016.”Released May 3 2016. Available at http://www2.gov.bc.ca/ assets/gov/public-safety-and-emergency-services/death-investigation/statistical/illicit-drug.pdf. (Accessed May2016).
5. Fischer B, Popova S, Rehm J, Ivsins A. Drug-relatedoverdose deaths in British Columbia and Ontario, 1992-2004. Can J Public Health. 2006;97(5):384-387.
6. Province of British Columbia. “Provincial health o cerdeclares public health emergency.” BC Government News, April 14, 2016. Available at: https://news.gov.bc.ca/10694.(Accessed April 26 2016).
7. BC Ministry of Justice, BC Coroners Service. “BC CoronersService warns of deaths related to illicit fentanyl use.”Released January 4, 2014. Available at http://www2.news. gov.bc.ca/news_releases_2013-2017/2014jag0150-000766 .htm. (Accessed April 26 2016).
8. BC Ministry of Justice, BC Coroners Service. “Fentanyl-Detected in Illicit Drug Overdose Deaths, January 1,2012 to March 31, 2016.” Released May 10 2016. Availableat http://www2.gov.bc.ca/assets/gov/public-safety-and-emergency-services/death-investigation/statistical/fentanyl-detected-overdose.pdf. (Accessed May 26 2016).
9. British Columbia Node of the Canadian Research Initiativeon Substance Misuse. Together, we can do this: Strategiesto Address British Columbia’s Prescription Opioid Crisis.November 2015. Available at: http://www.cfenet.ubc.ca/ sites/default/files/uploads/news/releases/opioid-safety-news_release_nov-19-2015.pdf (Accessed Feb 15 2016).
10. Fischer B. Prescriptions, power and politics: The turbulenthistory of methadone maintenance in Canada. J PublicHealth Pol. 2000;21(2):187-210.
11. Strathdee SA, Patrick DM, Currie SL, et al. Needleexchange is not enough: Lessons from the Vancouverinjecting drug use study. AIDS. 1997;11(8):F59-F65.
12. College of Physicians and Surgeons of British Columbia.Methadone Maintenance Program: Clinical PracticeGuideline. 2014. Available at: https://www.cpsbc.ca/ les/ pdf/MMP-Clinical-Practice-Guideline.pdf. (Accessed May17 2016).
13. Chiang CN, Hawks RL. Pharmacokinetics of the
combination tablet of buprenorphine and naloxone. Drug Alcohol Depend. 2003;70(2 Suppl):S39-47.14. Bigelow GE, Preston KL, Liebson IA. Abuse liability
assessment of buprenorphine-naloxone combinations.NIDA Res Monogr. 1987;76:145-149.
15. Mattick RP, Breen C, Kimber J, Davoli M. Buprenorphinemaintenance versus placebo or methadone maintenance foropioid dependence. Cochrane Database Syst Rev. 2014(2):CD002207. doi: 10.1002/14651858.CD002207.pub4.
16. Connery HS. Medication-assisted treatment of opioid use
disorder: review of the evidence and future directions. HarvRev Psychiatry. 2015;23(2):63-75.
17. College of Physicians and Surgeons of British Columbia.Suboxone. 2015. Available at: https://www.cpsbc.ca/ programs/bc-methadone-program/suboxone. (AccessedMay 17 2016).
18. St. Paul’s Goldcorp Addiction Medicine Fellowship. Training the Next Generat ion of Physician Leaders.St. Paul’s Hospital, Vancouver, BC, Canada. http:// addictionmedicinefellowship.org.
19. Vancouver Coastal Health and Providence Health CareOpioid Use Disorder Treatment Guideline Committee.Guideline for the Clinical Management of Opioid Addict ion. 2015. Available at: http: //www.vch.ca/media/ Opioid-Addiction-Guideline.pdf. (Accessed May 17 2016).
20. Maxwell JC, McCance-Katz EF. Indicators ofbuprenorphine and methadone use and abuse: what do weknow? Am J Addict. 2010;19(1):73-88.
21. Lofwall MR, Walsh SL. A review of buprenorphine diversionand misuse: the current evidence base and experiences fromaround the world. J Addict Med. 2014;8(5):315-326.
22. Auriacombe M, Fatséas M, Dubernet J, Daulouède JP,Tignol J. French eld experience with buprenorphine. Am J Addict. 2004;13 Suppl 1:S17-28.
23. Schwartz RP, Gryczynski J, O’Grady KE, et al. Opioidagonist treatments and heroin overdose deaths inBaltimore, Maryland, 1995-2009. Am J Public Health.2013;103(5):917-922.
24. Mattick RP, Kimber J, Breen C, Davoli M. Buprenorphinemaintenance versus placebo or methadone maintenancefor opioid dependence. Cochrane Database Syst Rev.
2008(2):CD002207. doi: 10.1002/14651858.CD002207.pub3.25. Woody GE, Poole SA, Subramaniam G, et al. Extended
vs shor t-term buprenorphine-naloxone for treatmentof opioid-addicted youth: a randomized trial. JAMA.2008;300(17):2003-2011.
26. Potter JS, Dreifuss JA, Marino EN, et al. The multi-siteprescription opioid addiction treatment study: 18-monthoutcomes. J Subst Abuse Treat. 2015;48(1):62-69.
27. Weiss RD, Potter JS, Gri n ML, et al. Long-term outcomesfrom the National Drug Abuse Treatment Clinical TrialsNetwork Prescription Opioid Addiction Treatment Study.Drug Alcohol Depend. 2015;150:112-119.
28. Kumar MS, Mudaliar S, Thyag arajan SP, Kumar S,Selvanayagam A, Daniels D. Rapid assessment and responseto injecting drug use in Madras, south India. Int J DrugPolicy. 2000;11(1-2):83-98.
29. Sullivan LE, Moore BA, Chawarski MC, et al.Buprenorphine/naloxone treatment in primary care isassociated with decreased human immunode ciency virusrisk behaviors. J Subst Abuse Treat. 2008;35(1):87-92.

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 17/20
17May 2016
30. Rowe TA, Jacapraro JS, Rastegar DA. Entry into primarycare-based buprenorphine treatment is associated withidentification and treatment of other chronic medicalproblems. Addict Sci Clin Pract. 2012;7:22.
31. Baser O, Chalk M, Fiellin DA, Gastfriend DR. Cost andutilization outcomes of opioid-dependence treatments. Am
J Manag Care. 2011;17 Suppl 8:S235-248.32. Barnett PG. Comparison of costs and utilization amongbuprenorphine and methadone patients. Addiction.2009;104(6):982-992.
33. Rosenheck R, Kosten T. Buprenorphine for opiateaddiction: potential economic impact. Drug AlcoholDepen. 2001;63(3):253-262.
34. Roncero C, Domínguez-Hernández R, Díaz T, et al.Management of opioid-dependent patients: comparisonof the cost associated with use of buprenorphine/naloxoneor methadone, and their interactions with concomitanttreatments for infectious or psychiatric comorbidities. Adicciones. 2015;27(3):179-189.
35. Moody DE. Metabolic and toxicological considerationsof the opioid replacement therapy and analgesic drugs:
methadone and buprenorphine. Expert Opin Drug MetabToxicol. 2013;9(6):675-697.36. Meemken L, Hanho N, Tseng A, Christensen S, Gillessen
A. Drug-Drug Interactions With Antiviral Agents in PeopleWho Inject Drugs Requiring Substitution Therapy. AnnPharmacother. 2015;49(7):796-807.
37. Jones ES, Moore BA, Sindelar JL , O’Connor PG,Schottenfeld RS, Fiellin DA. Cost analysis of clinic ando ce-based treatment of opioid dependence: Results withmethadone and buprenorphine in clinically stable patients.Drug Alcohol Depend. 2009;99(1-3):132-140.
38. Lepère B, Gourarier L, Sanchez M, et al. [Reduction inthe number of lethal heroin overdoses in France since1994. Focus on substitution treatments]. Ann Med Interne(Paris). 2001;152 Suppl 3:IS5-12.
39. Fatseas M, Auriacombe M. Why buprenorphine is sosuccessful in treating opiate addiction in France. CurrPsychiatry Rep. 2007;9(5):358-364.
40. Gladstone EJ, Smolina K, Morgan SG. Trends and sexdifferences in prescription opioid deaths in BritishColumbia, Canada. Inj Prev. 2015.
41. Paone D, Tuazon E, Stajic M, et al. Buprenorphineinfrequently found in fatal overdose in New York City.Drug Alcohol Depend. 2015;155:298-301.
42. Dasgupta N, Bailey EJ, Cicero T, et al. Post-marketingsurveillance of methadone and buprenorphine in theUnited States. Pain Med. 2010;11(7):1078-1091.
43. Bell JR, Butler B, Lawrance A, Batey R, Salmelainen P.Comparing overdose mortality associated with methadoneand buprenorphine treatment. Drug Alcohol Depend.2009;104(1-2):73-77.
44. Marteau D, McDonald R, Patel K. The relative risk offatal poisoning by methadone or buprenorphine withinthe wider population of England and Wales. BMJ Open.2015;5(5):e007629.
45. Substa nce Abuse and Mental Health Ser vices Administ ration (SAMHSA). Cente r for Behavio ra lHealth Statistics and Quality. January 29, 2013. The Drug Abuse Warning Network (DAWN) Report: EmergencyDepartment Visits Involving Buprenorphine. Rockville,MD.
46. Bazazi AR, Yokell M, Fu JJ, Rich JD, Zaller ND. Illicituse of buprenorphine/naloxone among injecting andnoninjecting opioid users. J Addict Med. 2011;5(3):175-180.
47. Furst RT. Suboxone misuse along the opiate maintenancetreatment pathway. J Addict Dis. 2013;32(1):53-67.
48. Gwin Mitchell S, Kelly SM, Brown BS, et al. Uses ofdiverted methadone and buprenorphine by opioid-addicted individuals in Baltimore, Maryland. Am J Addict.2009;18(5):346-355.
49. Schuman-Olivier Z, Albanese M, Nelson SE, et al. Self-treatment: illicit buprenorphine use by opioid-dependenttreatment seekers. J Subst Abuse Treat. 2010;39(1):41-50.
50. Luty J, O’Gara C, Sessay M. Is methadone too dangerousfor opiate addiction? BMJ. 2005;331(7529):1352-1353.
51. Chou R, Weimer MB, Dana T. Methadone overdose and
cardiac arrhythmia potential: ndings from a review ofthe evidence for an American Pain Society and College onProblems of Drug Dependence clinical practice guideline. J Pain. 2014;15(4):338-365.
52. Häkkinen M, Launiainen T, Vuori E, Ojanperä I.Benzodiazepines and alcohol are associated with casesof fatal buprenorphine poisoning. Eur J Clin Pharmacol.2012;68(3):301-309.
53. Häkkinen M, Vuori E, Ojanperä I. Prescription opioidabuse based on representative postmortem toxicology.Forensic Sci Int. 2014;245C:121-125.
54. Wikner BN, Ohman I, Selden T, Druid H, Brandt L,Kieler H. Opioid-related mortality and lled prescriptionsfor buprenorphine and methadone. Drug Alcohol Rev.2014;33(5):491-498.
55. Pelissier-Alicot AL, Sastre C, Baillif-Couniou V, et al.Buprenorphine-related deaths: unusual forensic situations.Int J Legal Med. 2010;124(6):647-651.
56. Heinemann A, Iwersen-Bergmann S, Stein S, Schmoldt A,Püschel K. Methadone-related fatalities in Hamburg 1990-1999: implications for quality standards in maintenancetreatment? Forensic Sci Int. 2000;113(1-3):449-455.
57. Degenhardt L, Larance BK, Bell JR, et al. Injection ofmedications used in opioid substitution treatment in Australia after the introduction of a mixed partial agonist-antagonist formulation. Med J Aust. 2009;191(3):161-165.
58. Genberg BL, Gillespie M, Schuster CR, et al. Prevalenceand correlates of street-obtained buprenorphine use amongcurrent and former injectors in Baltimore, Maryland. Addict Behav. 2013;38(12):2868-2873.
59. Hakansson A, Medvedeo A, Andersson M, Berglund M.Buprenorphine misuse among heroin and amphetamineusers in Malmo, Sweden: purpose of misuse and route ofadministration. Eur Addict Res. 2007;13(4):207-215.

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 18/20
18May 2016
60. Monte AA, Mandell T, Wilford BB, Tennyson J, Boyer EW.Diversion of buprenorphine/naloxone coformulated tabletsin a region with high prescribing prevalence. J Addict Dis.2009;28(3):226-231.
61. Lofwall MR, Havens JR. Inability to access buprenorphinetreatment as a risk factor for using diverted buprenorphine.
Drug Alcohol Depend. 2012;126(3):379-383.62. Richert T, Johnson B. Long- term self-treatment with
methadone or buprenorphine as a response to barriers toopioid substitution treatment: the case of Sweden. HarmReduct J. 2015;12:1.
63. Yokell MA, Zaller ND, Green TC, Rich JD. Buprenorphineand buprenorphine/naloxone diversion, misuse, and illicituse: an international review. Current Drug Abuse Rev.2011;4(1):28-41.
64. Launonen E, Alho H, Kotovirta E, Wallace I, Simojoki K.Diversion of opioid maintenance treatment medicationsand predictors for diversion among Finnish maintenancetreatment patients. Int J Drug Policy. 2015;26(9):875-882.
65. Monico LB, Mitchell SG, Gryczynski J, et al. PriorExperience with Non-Prescribed Buprenorphine: Rolein Treatment Entry and Retention. J Subst Abuse Treat.2015;57:57-62.
66. American Society of Addict ion Medicine. The ASAMNational Practice Guideline for the Use of Medicationsin the Treatment of Addiction Involving Opioid Use.2015. Available at: http://www.asam.org/quality-practice/ gu idel ines -a nd-consensus-documents/npg/compl ete - guideline (Accessed May 18 2016).
67. Center for Substance Abuse Treatment. Clinical Guidelinesfor the Use of Buprenorphine in the Treatment of Opioid Addiction. Treatment Improvement Protocol (TIP) Series40. DHHS Publication No. (SMA) 04-3939. Rockville,MD: Substance Abuse and Mental Health Services Administration, 2004.
68. Handford C, Kahan M, Srivastava A, Cirone S, Sanghera S,Palda V. Buprenorphine/naloxone for opioid dependence:clinical practice guidelines. Toronto, ON: CAMHKnowledge and Innovation Support Unit. 2012.
69. Kolodny A, Courtwright DT, Hwang CS, et al. Theprescription opioid and heroin crisis: a public healthapproach to an epidemic of addiction. Annu Rev PublicHealth. 2015;36:559-574.
70. British Columbia PharmaCare Formulary Search. UpdatedFeb 2 2016. Available at: https://pcbl.hlth.gov.bc.ca/ pharmacare/bene tslookup/. (Accessed Feb 15 2016).
71. Alberta Drug Bene t List (ADBL). Updated February 15,2016. Available a t: http://www.health.alberta.ca/services/ drug-bene t-list.html. (Accessed Feb 15 2016).
72. College of Physicians and Surgeons of Alberta. AlbertaMethadone Maintenance Treatment: Standards andGuidelines for Dependence. 2014. Available at: http://cpsa.ca/wp-content/uploads/2015/06/alberta-mmt-standards- guidelines.pdf?8563c4 (Accessed May 18 2016).
73. College of Physicians and Surgeons of Alberta. PhysicianPrescribing Practices Program (P4). BuprenorphinePrescribing. Available at: http://www.cpsa.ca/physician-prescribing-practices/buprenorphine-prescribing/.(Accessed Feb 15 2016).
74. Saskatchew an Online Formulary Database. Updated
January 28, 2015. Available at: http:// formulary.drugplan .health.gov.sk.ca/. (Accessed Feb 15 2016).75. College of Physicians and Surgeons of Saskatchewan.
Methadone Guidelines and Standards for the Treatment ofOpioid Addiction/Dependence. March 2015. Available at:https://www.cps.sk.ca/Documents/Programs%20and%20Services/Methadone/SK-Methadone-Guidelines-2015-Mar-FINAL.pdf. (Accessed Feb 15 2016).
76. College of Physicians and Surgeons of Manitoba.Manitoba Methadone & Buprenorphine MaintenanceGuidelines: Recommended Practice. Revised July 2014. Availab le at: http:/ /mpha. in1 touch.org/up loaded/web/ Guidelines/CPSM%20Manitoba%20Methadone%20&%20Buprenorphine%20Maintenance%20-%20Recommended%20Practice%20.pdf. (Accessed Feb 15
2016).77. Manitoba Pharmacare Program Drug Benefits &Interchangeability Formulary. Updated January 18 2016. Available at: http://web22.gov.mb.ca/eFormulary/. (AccessedFeb 15 2016).
78. College of Physicians & Surgeons of Ontario. MethadoneMaintenance Treatment Program Standards and ClinicalGuidelines. 2011. Available at: https://www.cpso.on.ca/ uploadedFiles/members/MMT-Guidelines.pdf. (AccessedFeb 15 2016).
79. Ontario Drug Benefit Formulary/Compar ative DrugIndex. Updated January 28 2016. Available at: https://www.healthinfo.moh.gov.on.ca/formulary/. (Accessed Feb 152016).
80. College des Medecins du Quebec. Utilisation de laméthadone dans le traitement de la toxicomanie auxopiacés (1999). Modi cations aux lignes directrices (2004).The Use of Methadone in the Treatment of Opiate Addiction: - February 2000. Available at: http://www.cmq.org/publications-pdf/p-1-1999-10-01-fr-utilisation-methadone-traitement-toxicomanie-aux-opiaces.pdf. 2000.(Accessed Feb 15 2016).
81. Collège des médecins du Québec and Ordre despharmaciens du Québec. La buprénorphine dans letraitement de la dépendance aux opioïdes. Available at:http://www.opq.org/cms/Media/808_38_fr-CA_0_ld_ buprenorphone.pdf. (Accessed Feb 15 2016).
82. Regie de l’assurance maladie Quebec. List of Medications.Updated January 11 2016. Available at: https://www.prod.ramq.gouv.qc.ca/DPI/PO/Commun/PDF/Liste_Med/Liste_ Med/liste_med_2016_02_08_en.pdf (Accessed Feb 15 2016).
83. College of Physicians and Surgeons of New Brunswick.Treatment of Opioid Addiction. June 2015. Availablea t : h t tps : / /www.cpsnb .org /engl i sh /Guide l ines / TreatmentofOpioidAddiction.htm. (Accessed Feb 15 2016).

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 19/20
19May 2016
84. New Brunswick Drug Plans Formulary. Februar y2016. Available at: http://www2.gnb.ca/content/ dam/gnb/Departments/h-s/pdf/en/NBDrugPlan/ NewBrunswickDrugPlansFormulary.pdf. (Accessed Feb 152016).
85. College of Physicians and Surgeons of Nova Scotia.CPSNS Methadone Maintenance Treatment Handbook.May 2012. Available at: http://www.cpsns.ns.ca/Portals/0/ PDFprograms/Methadone%20Main tenance%20Treatment%20Handbook.pdf. (Accessed Feb 15 2016).
86. Nova Scotia Formulary. February 2016. Available at: http:// novascotia.ca/dhw/pharmacare/documents/formulary.pdf.(Accessed Feb 15 2016).
87. College of Physicians and Surgeons of Prince EdwardIsland. Prescribing Buprenorphine Treatment for OpioidDependency. Approved January 27, 2014. Availableat: http://cpspei.ca/wp-content/uploads/2014/02/ BUPRENORPHINE-Treatment-for-Opioid-Dependency- Jan-2714.pdf. (Accessed Feb 15 2016).
88. Health PEI. PEI Pharmacare Formulary. Updated January2016. Available at: http://healthpei.ca/formulary. (AccessedFeb 15 2016).
89. The College of Physicians and Surgeons ofNewfoundland and Labrador. Guideline - PrescribingBuprenorphine. Available at: http://www.cpsnl.ca/default.asp?com=Policies&m=340&y=&id=63. (Accessed Feb 152016).
90. The College of Physicians and Surgeons of Newfoundlandand Labrador. Methadone Maintenance TreatmentStandards and Guidelines. May 2013. Available at:http://www.cpsnl.ca/userfiles/file/Methadone%20Maintenance%20Treatment%20Standards%20and%20Guidelines%20-%20CPSNL%20-%20March%2014,%202013%20-%20Final.pdf. (Accessed Feb 15 2016).
91. Newfoundland and Labrador Prescription Drug Program(NLPDP). Updated February 15 2016. Available at: http:// www.health.gov.nl.ca/health/prescription/newformulary.asp(Accessed Feb 15 2016).

8/16/2019 Suboxone report
http://slidepdf.com/reader/full/suboxone-report 20/20
20May 2016
Authors and ContributorsKeith Ahamad , MD, CCFP, CISAM Family and Addiction Medicine Physician, Providence Health Care / Vancouver Coastal Health Research Scientist, BC Centre for Excellence in HIV/AIDS Clinical Assistant Professor, Faculty of Medicine, UBC
Thomas Kerr , PhDDirector, Urban Health Research Initiative, BC Centre for Excellence in HIV/AIDS Professor, Faculty of Medicine, UBC
Seonaid Nolan , MD, FRCPC, Dip ABAM Internal Medicine and Addiction Medicine Physician, Providence Health Care Research Scientist, Urban Health Research Initiative, BC Centre for Excellence in HIV/AIDS Clinical Assistant Professor, Faculty of Medicine, UBC
Evan Wood , MD, PhD, ABIM, FRCPC Professor of Medicine, Canada Research Chair in Inner City Medicine, UBC Medical Director, Community Addiction Services, Vancouver Coastal Health / Providence Health Care Principal Investigator, British Columbia Node of the Canadian Research Initiative in Substance Misuse (CRISM)
Con icts of InterestThe authors of this report have no con icts of interest to declare.
Speci cally, the authors con rm that they have no a liations with or involvement in any privatecorporation or entity, and have no nancial interests (i.e., have not received any honoraria; educational
grants; membership, employment, consultancies, stock ownership, or other equity interest; experttestimony or patent-licensing arrangements) in any private corporation or entity that would undulyin uence the content or recommendations made in this report.
AcknowledgementsWe wish to acknowledge Emily Wagner for research and writing assistance in preparing this document.We also wish to thank Cheyenne Johnson, James Nakagawa, Zoe O’Neill, Diane Pépin, Lianlian Ti,Peter Vann, and Pauline Voon for editorial and administrative assistance.
This work was supported, in part, by the Canadian Institutes of Health Research through the CanadianResearch Initiative in Substance Misuse (SMN–139148) and the Canada Research Chairs programthrough a Tier 1 Canada Research Chair in Inner City Medicine which supports Dr. Evan Wood. TheBC Node of CRISM is supported by the BC Centre for Excellence in HIV/AIDS.