subdural haematoma: presentation and diagnosis …hemianaesthesia and hemianopia. these signs were...
TRANSCRIPT

Postgrad. med. J. (October 1968) 44, 785-791.
Subdural haematoma: presentation and diagnosis on medical wards
M. E. WALKERM.A., M.B. Cantab., M.R.C.P.
Neurological Registrar
MICHAEL ESPIRM.A., M.B. Cantab., M.R.C.P.
Department ofNeurology, Leicester AreaConsultant Neurologist
R. H. SHEPHARDF.R.C.S.
Consultant Neurosurgeon, Regional Neurosurgical Unit, Derby
SummaryThe twenty-two adult patients with subacute and
chronic subdural haematoma seen in Leicester dur-ing the last 7 years have been reviewed. The clin-ical manifestations and results of investigations aredescribed. The diagnostic difficulties which mayconfront physicians are discussed, with specialreference to cases with no history of head injurymasquerading as strokes. Stress is laid on the pointswhich help with the differentiation.
IntroductionThe diagnosis of subdural haematoma (SDH)
does not usually present much difficulty for theneurosurgeon, as once this possibility isconsidered, it can be readily confirmed by burr-hole exploration, which also allows definitivetreatment to be started. However, in patients admit-ted in the first place to general medical rather thanneurosurgical wards, and particularly when a his-tory of head injury is lacking, the correct diagnosismay not be suspected initially. In such cases, thedifferential diagnosis may cover a wide variety ofconditions, and the role of the physician is toconsider the possibility of SDH and select thesuitable cases for investigation and surgical treat-ment. We have, therefore, reviewed the adultpatients with proven SDH in Leicester over thelast 7 years, and in this paper report our exper-iences with special reference to the diagnosticproblems encountered.SDH are now usually classified into acute, sub-
acute and chronic, but the limits of each groupvary (McKissock, Richardson & Bloom, 1960; Gil-martin, 1964). We have regarded SDH as acute ifoperation is performed within 3 days after injury,subacute-more than 3 days but within 3 weeks,and chronic-more than 3 weeks or without anyhistory of head injury (Rosenbluth et al., 1962;Alexander, 1964).
Patients with acute SDH will not be discussed,as they are usually admitted directly to accidentor general surgical wards, and deterioration orfailure to improve following the recent head in-jury is a well-recognized indication for burr-holeexploration. Severe brain damage is frequentlyfound coincidentally, and evacuation of the SDHmay make little difference to the ultimate outcome.On the other hand, with subacute and chronic
SDH the correct diagnosis is often not obvious andyet most vital, as these patients often have relativelylittle associated brain damage and timely surgicaltreatment is much more rewarding.
In this paper we first describe the clinical mani-festations and preliminary investigation of thepatients with subacute and chronic SDH to indic-ate the common features which can be applied tohelp with the diagnosis of the difficult cases. Thislatter group will then be discussed separately inorder to illustrate the particular diagnostic diffi-culties and emphasize their distinguishing features.
Clinical manifestationsThere were twenty-two patients in this series,
nine with subacute and thirteen with chronic SDH.All recovered after surgical treatment, except twoof the chronic cases. Table 1 shows that in thirteencases (eight subacute and five chronic) there wasa clear-cut relation to a head injury before thediagnosis was established by burr-holes, but in theremaining nine cases (eight chronic and one sub-acute) no such history was obtained, or a previoushead injury was either trivial, remote or of doubt-ful significance, so that the diagnosis of SDH wasnot obvious and not suspected initially.
Predisposing factorsThe liability of alcoholics to develop SDH is
well known (Brain, 1962), and this has also beenreported in epileptics (Feldman, Pincus &
Protected by copyright.
on February 2, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.44.516.785 on 1 O
ctober 1968. Dow
nloaded from
M. E. Walker, Michael Espir and R. H. Shephard
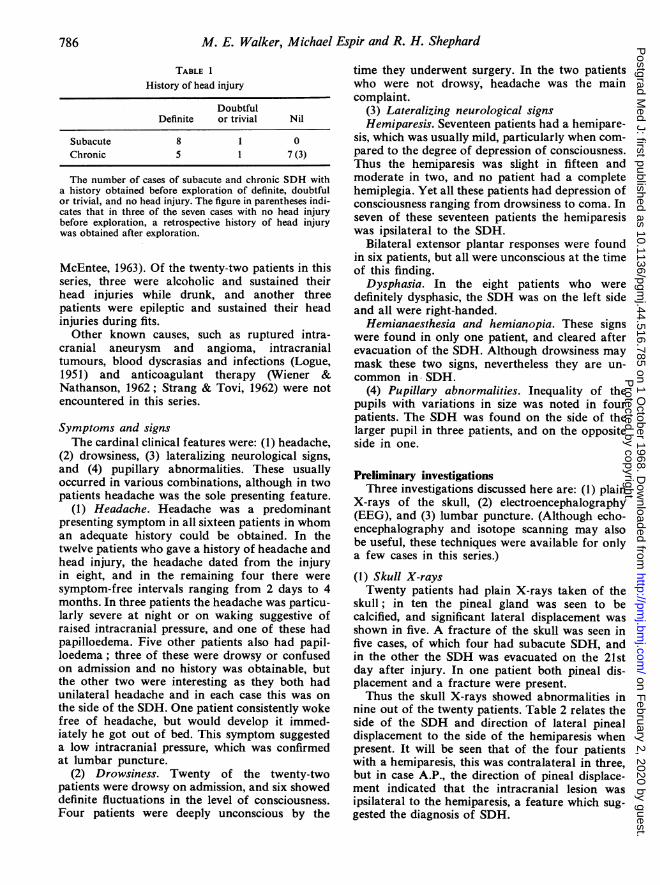
TABLE 1
History of head injury
DoubtfulDefinite or trivial Nil
Subacute 8 1 0Chronic 5 1 7 (3)
The number of cases of subacute and chronic SDH witha history obtained before exploration of definite, doubtfulor trivial, and no head injury. The figure in parentheses indi-cates that in three of the seven cases with no head injurybefore exploration, a retrospective history of head injurywas obtained after exploration.
McEntee, 1963). Of the twenty-two patients in thisseries, three were alcoholic and sustained theirhead injuries while drunk, and another threepatients were epileptic and sustained their headinjuries during fits.
Other known causes, such as ruptured intra-cranial aneurysm and angioma, intracranialtumours, blood dyscrasias and infections (Logue,1951) and anticoagulant therapy (Wiener &Nathanson, 1962; Strang & Tovi, 1962) were notencountered in this series.
Symptoms and signsThe cardinal clinical features were: (1) headache,
(2) drowsiness, (3) lateralizing neurological signs,and (4) pupillary abnormalities. These usuallyoccurred in various combinations, although in twopatients headache was the sole presenting feature.
(1) Headache. Headache was a predominantpresenting symptom in all sixteen patients in whoman adequate history could be obtained. In thetwelve patients who gave a history of headache andhead injury, the headache dated from the injuryin eight, and in the remaining four there weresymptom-free intervals ranging from 2 days to 4months. In three patients the headache was particu-larly severe at night or on waking suggestive ofraised intracranial pressure, and one of these hadpapilloedema. Five other patients also had papil-loedema; three of these were drowsy or confusedon admission and no history was obtainable, butthe other two were interesting as they both hadunilateral headache and in each case this was onthe side of the SDH. One patient consistently wokefree of headache, but would develop it immed-iately he got out of bed. This symptom suggesteda low intracranial pressure, which was confirmedat lumbar puncture.
(2) Drowsiness. Twenty of the twenty-twopatients were drowsy on admission, and six showeddefinite fluctuations in the level of consciousness.Four patients were deeply unconscious by the
time they underwent surgery. In the two patientswho were not drowsy, headache was the maincomplaint.
(3) Lateralizing neurological signsHemiparesis. Seventeen patients had a hemipare-
sis, which was usually mild, particularly when com-pared to the degree of depression of consciousness.Thus the hemiparesis was slight in fifteen andmoderate in two, and no patient had a completehemiplegia. Yet all these patients had depression ofconsciousness ranging from drowsiness to coma. Inseven of these seventeen patients the hemiparesiswas ipsilateral to the SDH.
Bilateral extensor plantar responses were foundin six patients, but all were unconscious at the timeof this finding.
Dysphasia. In the eight patients who weredefinitely dysphasic, the SDH was on the left sideand all were right-handed.
Hemianaesthesia and hemianopia. These signswere found in only one patient, and cleared afterevacuation of the SDH. Although drowsiness maymask these two signs, nevertheless they are un-common in SDH.
(4) Pupillary abnormalities. Inequality of thepupils with variations in size was noted in fourpatients. The SDH was found on the side of thelarger pupil in three patients, and on the oppositeside in one.
Preliminary investigationsThree investigations discussed here are: (1) plain
X-rays of the skull, (2) electroencephalography(EEG), and (3) lumbar puncture. (Although echo-encephalography and isotope scanning may alsobe useful, these techniques were available for onlya few cases in this series.)
(1) Skull X-raysTwenty patients had plain X-rays taken of the
skull; in ten the pineal gland was seen to becalcified, and significant lateral displacement wasshown in five. A fracture of the skull was seen infive cases, of which four had subacute SDH, andin the other the SDH was evacuated on the 21stday after injury. In one patient both pineal dis-placement and a fracture were present.Thus the skull X-rays showed abnormalities in
nine out of the twenty patients. Table 2 relates theside of the SDH and direction of lateral pinealdisplacement to the side of the hemiparesis whenpresent. It will be seen that of the four patientswith a hemiparesis, this was contralateral in three,but in case A.P., the direction of pineal displace-ment indicated that the intracranial lesion wasipsilateral to the hemiparesis, a feature which sug-gested the diagnosis of SDH.
786P
rotected by copyright. on F
ebruary 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.44.516.785 on 1 October 1968. D
ownloaded from
Subdural haematoma
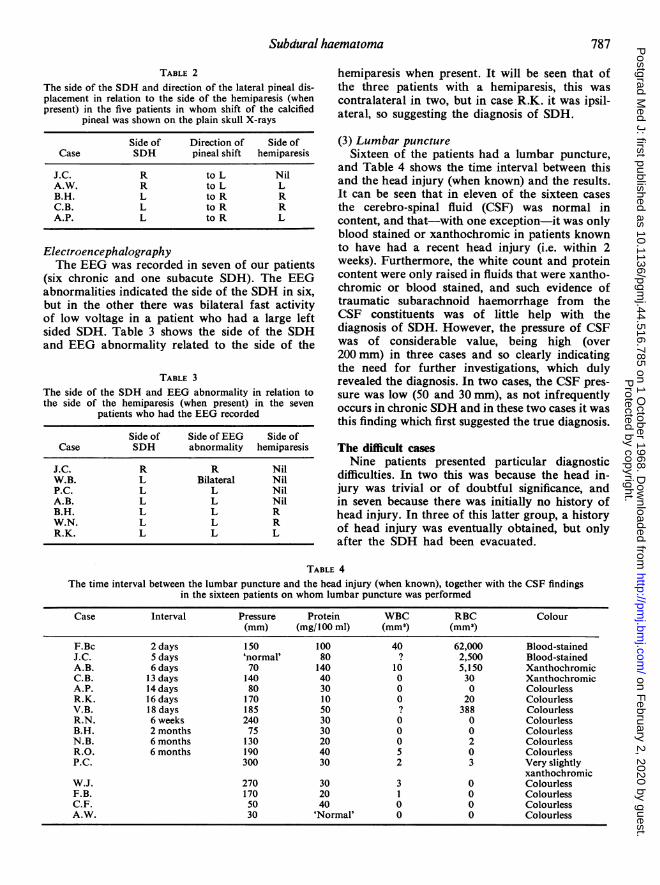
TABLE 2The side of the SDH and direction of the lateral pineal dis-placement in relation to the side of the hemiparesis (whenpresent) in the five patients in whom shift of the calcified
pineal was shown on the plain skull X-rays
Side of Direction of Side ofCase SDH pineal shift hemiparesis
J.C. R to L NilA.W. R to L LB.H. L to R RC.B. L to R RA.P. L to R L
ElectroencephalographyThe EEG was recorded in seven of our patients
(six chronic and one subacute SDH). The EEGabnormalities indicated the side of the SDH in six,but in the other there was bilateral fast activityof low voltage in a patient who had a large leftsided SDH. Table 3 shows the side of the SDHand EEG abnormality related to the side of the
TABLE 3The side of the SDH and EEG abnormality in relation tothe side of the hemiparesis (when present) in the seven
patients who had the EEG recorded
Side of Side of EEG Side ofCase SDH abnormality hemiparesis
J.C. R R NilW.B. L Bilateral NilP.C. L L NilA.B. L L NilB.H. L L RW.N. L L RR.K. L L L
hemiparesis when present. It will be seen that ofthe three patients with a hemiparesis, this wascontralateral in two, but in case R.K. it was ipsil-ateral, so suggesting the diagnosis of SDH.
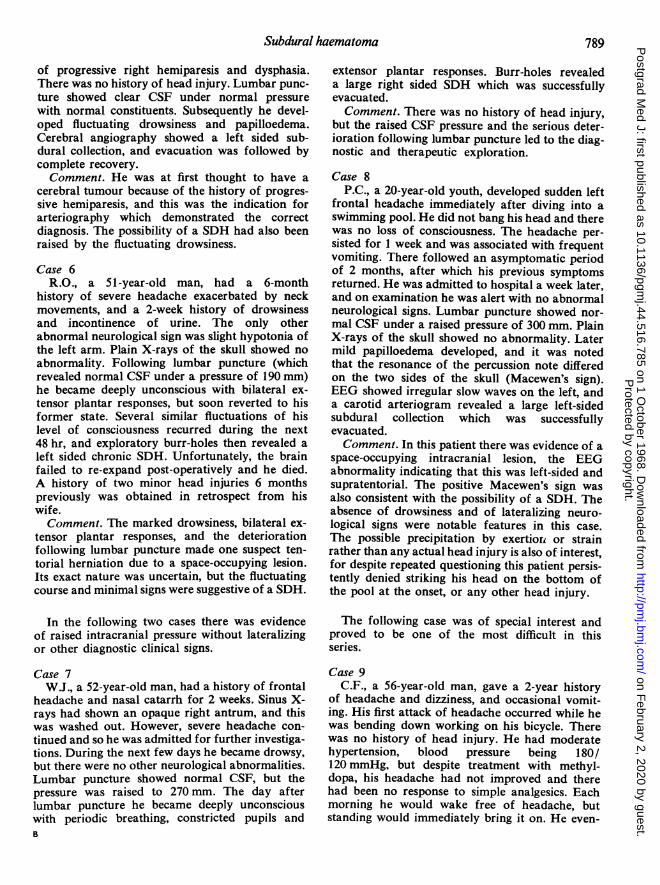
(3) Lumbar punctureSixteen of the patients had a lumbar puncture,
and Table 4 shows the time interval between thisand the head injury (when known) and the results.It can be seen that in eleven of the sixteen casesthe cerebro-spinal fluid (CSF) was normal incontent, and that-with one exception-it was onlyblood stained or xanthochromic in patients knownto have had a recent head injury (i.e. within 2weeks). Furthermore, the white count and proteincontent were only raised in fluids that were xantho-chromic or blood stained, and such evidence oftraumatic subarachnoid haemorrhage from theCSF constituents was of little help with thediagnosis of SDH. However, the pressure of CSFwas of considerable value, being high (over200 mm) in three cases and so clearly indicatingthe need for further investigations, which dulyrevealed the diagnosis. In two cases, the CSF pres-
sure was low (50 and 30 mm), as not infrequentlyoccurs in chronic SDH and in these two cases it wasthis finding which first suggested the true diagnosis.
The difficult casesNine patients presented particular diagnostic
difficulties. In two this was because the head in-jury was trivial or of doubtful significance, andin seven because there was initially no history ofhead injury. In three of this latter group, a historyof head injury was eventually obtained, but onlyafter the SDH had been evacuated.
TABLE 4The time interval between the lumbar puncture and the head injury (when known), together with the CSF findings
in the sixteen patients on whom lumbar puncture was performed
Case Interval Pressure Protein WBC RBC Colour(mm) (mg/100 ml) (mm') (mm')
F.Bc 2 days 150 100 40 62,000 Blood-stainedJ.C. 5 days 'normal' 80 ? 2,500 Blood-stainedA.B. 6 days 70 140 10 5,150 XanthochromicC.B. 13 days 140 40 0 30 XanthochromicA.P. 14 days 80 30 0 0 ColourlessR.K. 16 days 170 10 0 20 ColourlessV.B. 18 days 185 50 ? 388 ColourlessR.N. 6 weeks 240 30 0 0 ColourlessB.H. 2 months 75 30 0 0 ColourlessN.B. 6 months 130 20 0 2 ColourlessR.O. 6 months 190 40 5 0 ColourlessP.C. 300 30 2 3 Very slightly
xanthochromicW.J. 270 30 3 0 ColourlessF.B. 170 20 1 0 ColourlessC.F. 50 40 0 0 ColourlessA.W. 30 'Normal' 0 0 Colourless
787P
rotected by copyright. on F
ebruary 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.44.516.785 on 1 October 1968. D
ownloaded from

M. E. Walker, Michael Espir and R. H. Shephard
The following case histories illustrate some of theproblems encountered. In the first four cases astroke was the initial diagnosis.
Case 1V.B., a 57 year-old-woman, fell at the bottom of
some stairs and injured her head, losing conscious-ness for just a few minutes. During the next 2weeks she had intermittent stiffness of her rightupper limb and slight difficulty with her speech.She was then admitted to hospital, and later thatday became disorientated with a right hemiparesisand bilateral extensor plantar responses. Shebecame increasingly drowsy and the right pupilbecame fixed and dilated. Lumbar punctureshowed colourless CSF under pressure of 185 mm,there were 388 red cells and the protein was 50 mg/100 ml. Plain X-rays of the skull showed no abnor-mality, but a left carotid arteriogram revealed a leftsided subdural collection, which was successfullyevacuated.Comment. In this case the significance of the
head injury was initially uncertain, and it seemedpossible that the fall and subsequent signs resultedfrom cerebro-vascular insufficiency. However, thebilateral extensor plantar responses, deepeningcoma and later the dilated and fixed right pupilsuggested tentorial herniation rather thanunilateral cerebral ischaemia, and the true signifi-cance of the head injury then became clear. How-ever, post-operatively her dysphasia did not clearcompletely, and a right homonymous hemianopiawas noted; it seems possible that she may have infact sustained a cerebro-vascular lesion at the on-set, leading to her fall and the development ofthe SDH.
Case 2N.B., a 56-year-old man, had a previous history
of both cerebral and myocardial infarctions. Sevendays before admission he developed severe head-ache associated with weakness of the right lowerlimb. These symptoms increased and on the dayof admission he also developed weakness of theright arm and dysphasia. Lumbar puncture showedclear CSF under normal pressure with normalconstituents. Plain X-rays of his skull showed noabnormality. He later became increasingly drowsywithout any increase in the hemiparesis, and itwas this that raised the possibility of a SDH. Burr-holes were performed and a large left-sided SDHwas successfully evacuated. Subsequently it waslearnt that he had sustained a minor head injury6 months previously.Comment. Taking into account his past history,
it was thought-not unnaturally-that he hadsuffered a further cerebral infarct. However, the
following points were more in favour of SDH thancerebral infarction: (a) the headache was severeand persistent, (b) the hemiparesis started and wasmore marked in the lower limb, (c) his symp-toms increased over a period of 7 days, and (d)finally there was increasing drowsiness withoutincrease in the hemiparesis, which is a characteris-tic feature of SDH.
Case 3B.H. a 71-year-old man, was admitted in a con-
fused and drowsy state with no available history.Examination revealed a mild right hemiparesiswith dysphasia, and left cerebral infarction was theinitial diagnosis. Lumbar puncture showed clearCSF under normal pressure with normal constitu-ents. EEG showed generalized slowing-with lowervoltage on the left. However, pineal displacement tothe right was noted on the plain skull X-rays andburr-holes were therefore advised. These revealeda left-sided SDH which was removed, leading tocomplete recovery. Only afterwards was it learntthat the patient had suffered a minor headinjury at work 2 months previously.Comment. This patient also exhibited marked
drowsiness with only a slight hemiparesis, and inaddition the pineal was displaced.Case 4A.W., a 66-year-old man, developed episodes of
dizziness and headache with slight left hemiparesis.After approximately 48 hr he lapsed into uncons-ciousness, and as his general practitioner thoughtthat he had a stroke he was nursed at home for thenext 5 days. His admission to hospital was thenrequested for terminal care, and on examinationhe was deeply unconscious and moribund. Lumbarpuncture revealed clear CSF under a low pressureof 30 mm with normal constituents. The possibilityof a SDH was queried because of the low CSFpressure, and arrangements were made for him tohave plain X-rays taken of the skull followed byburr-holes. These revealed a right sided chronicSDH which was evacuated, and he eventuallyrecovered completely.Comment. His skull X-rays in fact showed that
the pineal gland was calcified and displaced to theleft, but the decision had been made to proceedwith exploratory burr-holes before the radiolog-ical findings were known, because of the low CSFpressure. Questioned carefully in retrospect, he hadno recollection of any head injury.
In the following two cases, an intracranialtumour was the initial diagnosis.Case 5
F.B., a 60-year-old man, had 1 month's history
788P
rotected by copyright. on F
ebruary 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.44.516.785 on 1 October 1968. D
ownloaded from
Subdural haematoma
of progressive right hemiparesis and dysphasia.There was no history of head injury. Lumbar punc-ture showed clear CSF under normal pressurewith normal constituents. Subsequently he devel-oped fluctuating drowsiness and papilloedema.Cerebral angiography showed a left sided sub-dural collection, and evacuation was followed bycomplete recovery.Comment. He was at first thought to have a
cerebral tumour because of the history of progres-sive hemiparesis, and this was the indication forarteriography which demonstrated the correctdiagnosis. The possibility of a SDH had also beenraised by the fluctuating drowsiness.
Case 6R.O., a 51-year-old man, had a 6-month
history of severe headache exacerbated by neckmovements, and a 2-week history of drowsinessand incontinence of urine. The only otherabnormal neurological sign was slight hypotonia ofthe left arm. Plain X-rays of the skull showed noabnormality. Following lumbar puncture (whichrevealed normal CSF under a pressure of 190 mm)he became deeply unconscious with bilateral ex-tensor plantar responses, but soon reverted to hisformer state. Several similar fluctuations of hislevel of consciousness recurred during the next48 hr, and exploratory burr-holes then revealed aleft sided chronic SDH. Unfortunately, the brainfailed to re-expand post-operatively and he died.A history of two minor head injuries 6 monthspreviously was obtained in retrospect from hiswife.Comment. The marked drowsiness, bilateral ex-
tensor plantar responses, and the deteriorationfollowing lumbar puncture made one suspect ten-torial herniation due to a space-occupying lesion.Its exact nature was uncertain, but the fluctuatingcourse and minimal signs were suggestive of a SDH.
In the following two cases there was evidenceof raised intracranial pressure without lateralizingor other diagnostic clinical signs.
Case 7W.J., a 52-year-old man, had a history of frontal
headache and nasal catarrh for 2 weeks. Sinus X-rays had shown an opaque right antrum, and thiswas washed out. However, severe headache con-tinued and so he was admitted for further investiga-tions. During the next few days he became drowsy,but there were no other neurological abnormalities.Lumbar puncture showed normal CSF, but thepressure was raised to 270 mm. The day afterlumbar puncture he became deeply unconsciouswith periodic breathing, constricted pupils andB
extensor plantar responses. Burr-holes revealeda large right sided SDH which was successfullyevacuated.Comment. There was no history of head injury,
but the raised CSF pressure and the serious deter-ioration following lumbar puncture led to the diag-nostic and therapeutic exploration.
Case 8P.C., a 20-year-old youth, developed sudden left
frontal headache immediately after diving into aswimming pool. He did not bang his head and therewas no loss of consciousness. The headache per-sisted for 1 week and was associated with frequentvomiting. There followed an asymptomatic periodof 2 months, after which his previous symptomsreturned. He was admitted to hospital a week later,and on examination he was alert with no abnormalneurological signs. Lumbar puncture showed nor-mal CSF under a raised pressure of 300 mm. PlainX-rays of the skull showed no abnormality. Latermild papilloedema developed, and it was notedthat the resonance of the percussion note differedon the two sides of the skull (Macewen's sign).EEG showed irregular slow waves on the left, anda carotid arteriogram revealed a large left-sidedsubdural collection which was successfullyevacuated.Comment. In this patient there was evidence of a
space-occupying intracranial lesion, the EEGabnormality indicating that this was left-sided andsupratentorial. The positive Macewen's sign wasalso consistent with the possibility of a SDH. Theabsence of drowsiness and of lateralizing neuro-logical signs were notable features in this case.The possible precipitation by exertiori or strainrather than any actual head injury is also of interest,for despite repeated questioning this patient persis-tently denied striking his head on the bottom ofthe pool at the onset, or any other head injury.
The following case was of special interest andproved to be one of the most difficult in thisseries.
Case 9C.F., a 56-year-old man, gave a 2-year history
of headache and dizziness, and occasional vomit-ing. His first attack of headache occurred while hewas bending down working on his bicycle. Therewas no history of head injury. He had moderatehypertension, blood pressure being 180/120 mmHg, but despite treatment with methyl-dopa, his headache had not improved and therehad been no response to simple analgesics. Eachmorning he would wake free of headache, butstanding would immediately bring it on. He even-
789P
rotected by copyright. on F
ebruary 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.44.516.785 on 1 October 1968. D
ownloaded from

M. E. Walker, Michael Espir and R. H. Shephard
tually developed intermittent drowsiness, with hic-coughs and frequent vomiting, although when hewas admitted to hospital there were no other neuro-logical abnormalities. Plain X-rays of the skullwere normal, and lumbar puncture showed normalCSF but a low pressure of 50 mm. Carotid angio-grams revealed bilateral subdural collections. Un-fortunately the brain failed to re-expand afterthese had been evacuated, and the patient died.Comment. The low pressure state was the salient
feature suggesting the diagnosis of SDH in thiscase. In retrospect it seemed possible that the strainfrom bending down when working on his bicycleprecipitated the haemorrhage.
DiscussionThe case histories cited above illustrate certain
characteristic features of SDH, some of which canbe correlated with the pathological processes in-volved. The initial incident may be the rupture ofone or more of the veins traversing the subduralspace between the cerebral hemisphere and thesuperior sagittal sinus. Such an event seems morelikely to occur in patients with cerebral atrophy,or in those subject to frequent head injuries (e.g.epileptics and alcoholics). In many cases a headinjury is known to be the precipitating cause, butin most series there is a group of patients fromwhom no history of head injury can be obtained.Although in such cases a trivial head injury mayhave been forgotten, it seems possible that SDHcan occasionally result from just coughing, strain-ing or exertion. It has also been suggested that inthe absence of any known history of head injury,spontaneous bleeding and haematoma formationmay occur intradurally, i.e. between the inner andouter layer of the dura, possibly due to a congenitaldiathesis (Jewesbury & Josse, 1964).The haematoma overlying the cerebral cortex
may enlarge as a result of an osmotic mechanism(Gardner, 1932). It may then cause the percussionnote of the skull to be flatter on the affected side(Macewen's sign), although this may be difficultto elicit and is not pathognomonic of SDH. Insome cases the haematoma is of maximal thicknessin the parasagittal region, so that the hemiparesismay start and be most severe in the lower limb,as described in one of our cases. Although thismay also result from infarction in the territoryof the anterior cerebral artery, this is relativelyrare compared with infarction in the distributionof the middle cerebral artery, when the upperlimb is mainly affected. Furthermore with super-ficial parietal lesions, hemianaesthesia and hemian-opia would not be expected, whereas they are ofcourse common in cerebral infarction and othermore deeply situated lesions.
SDH occasionally become calcified or ossified(Jackson & Clare, 1965), sometimes they may re-gress spontaneously (Bender, 1960; Ambrosetto,1962; Lancet, 1962), but the majority graduallyexpand, compressing the underlying brain and itsvenous drainage. Eventually this may cause themedial part of the ipsilateral temporal lobe toherniate through the tentorial hiatus. The thirdnerve may thus be compressed, and inequality withfluctuation in size of the pupils is a well-knownsign in SDH. At the same time, the opposite cere-bral peduncle may be compressed against thetentorial edge, causing a hemiparesis on the sameside as the SDH. In this series the frequency withwhich the hemiparesis was ipsilateral to the SDHhas been mentioned. Although this phenomenonmay also occur in some intracranial tumours (e.g.meningioma), nevertheless this is of diagnosticvalue in the differentiation of SDH from cerebralinfarction. Pre-operative evidence regarding thelateralization of the SDH may be obtained by not-ing lateral pineal displacement on the plain skullX-rays, and/or predominantly unilateral EEGabnormalities. Although the EEG is usuallyabnormal and may be helpful, particularly if theabnormality is ipsilateral to the hemiparesis, never-theless the EEG is of relatively limited value sothat if not readily available this should not lead toany undue delay of other necessary measures.The clinical, radiological and EEG findings may
thus indicate the correct diagnosis and lateraliza-tion. However, as far as treatment is concerned, asSDH may be bilateral whether or not lateralizingsigns are present, and even if SDH is found andevacuated from one side, burr-hole explorationshould always be done on both sides.As with other intracranial space-occupying
lesions, the manifestations of SDH result fromboth its local effects on underlying cerebral tis-sues and its general effects on intracranialdynamics. However, because the clot is extra-cerebral and often exerts its effects over a widearea of cerebral cortex, symptoms and signs oflocal pressure (e.g. hemiparesis) tend to berelatively slight, whereas those of generalized dis-turbance of intracranial dynamics (e.g. headache,drowsiness or coma) tend to be severe. Thesefeatures contrast sharply with those of cerebralinfarction, when a lesion of sufficient magnitudeto produce drowsiness is usually associated with adense hemiplegia, and often hemianaesthesia andhemianopia as well.The main difficulties in diagnosis occur when
there is no known history of head injury, or whenthe significance of a minor or remote head injuryis uncertain. In these patients the initial diagnosisis usually cerebral infarction or tumour. The sus-
790P
rotected by copyright. on F
ebruary 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.44.516.785 on 1 October 1968. D
ownloaded from
Subdural haematoma 791
picion of cerebral tumour usually merits furtherinvestigations, so that the correct diagnosis isrevealed. However, this does not hold true in sus-pected stroke. This problem frequently arises inthe elderly (Bedford, 1957; Stuteville & Welch,1958; Perlmutter, 1961; Spencer, 1964), in whommental changes tend to be attributed to arterioscler-osis and when falls and minor head injuries arecommonplace, so that even if there is a historyof such an injury its true significance may not beappreciated. Furthermore, because of old age,arteriosclerosis or hypertension, cerebral angio-raphy may be withheld, and thus the true diagnosismay not even be revealed by chance. It is clearlyimpracticable and undesirable to perform burr-holes or arteriograms on all cases of suspectedstroke, but the features which we have discussedmay indicate the necessity for proceeding withthese investigations.
ConclusionsAlthough this is a small series of cases, we feel
justified in emphasizing that the diagnosis of SDH,especially in the difficult cases with no history ofhead injury, should be considered:
(a) When there is drowsiness or coma, orevidence of raised intracranial pressure withoutany other obvious signs or cause, particularly inan epileptic or alcoholic.
(b) In suspected cerebral infarction: (1) whenthere is severe or persistent headache, (2) whenthe level of consciousness and physical signs fluctu-ate in severity, (3) when depression of conscious-ness is marked with only a slight hemiparesis, (4)when the hemiparesis affects the leg more thanthe arm, (5) when there is inequality and fluctua-tion in size of the pupils, (6) when the percussionnote of the skull differs on the two sides, (7) whenthe pressure at lumbar puncture is abnormally lowor high, (8) when plain skull X-rays show a fractureor pineal shift, and (9) when plain skull X-rays(echo-encephalography if available), and/or EEGindicate an intracranial lesion on the same sideas the hemiparesis.
Proof of the diagnosis of SDH and successfultreatment are dependent on timely burr-hole ex-ploration, and although arteriography may also bea most valuable diagnostic aid, yet these proceduresdemand valid indications. When they are readily
fulfilled the prognosis should be excellent, but indifficult cases the indications for these proceduresmay depend upon paying attention to the detailsdiscussed, and recovery may then result from anotherwise hopeless situation.
AcknowledgmentsWe wish to acknowledge with thanks the collaboration of
our colleagues who have helped with the management of thecases reported.
ReferencesALEXANDER, J.B. (1964) Chronic subdural haematoma, as
seen by the internist. N.Carolina med. J. 25, 95.AMBROSETTO, C. (1962) Post-traumatic subdural haematoma:
further observations on non-surgical treatment. Arch.Neurol. 6, 287.
BEDFORD, P.D. (1957) Intracranial haemorrhage-diagnosisand treatment. Proc. R. Soc. Med. 51, 209.
BENDER, M.B. (1960) Recovery from subdural haematomawithout surgery. J. Mt Sinai Hosp. N. Y. 27, 52.
BRAIN, LORD (1962) Diseases of the Nervous System, Sixthedition, p. 309. Oxford University Press, London.
FELDMAN, R.G., PINCUS, J.H. & McENTEE, W.J. (1963)Cerebrovascular accident or subdural fluid collection?Arch. intern. Med. 112, 966.
GARDNER, W.J. (1932) Traumatic subdural haematoma:with particular reference to the latent interval. Arch.Neurol. 27, 847.
GILMARTIN, D. (1964) Arteriography in diagnosis of sub-dural haematoma. Lancet, i, 1061.
JACKSON, F.E. & CLARE, F. (1965) Ossified subdural haema-tomas of the cerebral convexities. J. Amer. med. Ass. 191,598.
JEWESBURY, E.C.O. & JOSSE, S.E. (1964) Arteriography indiagnosis of subdural haematoma. Lancet, i, 1277.
Lancet (1962). Annotation, ii, 1154.LoGUE, V. (1951) Chronic subdural effusions. Modern
Trends in Neurology (Ed. by A. Feiling), p. 363. Butter-worth, London.
McKISSOCK, W., RICHARDSON, A. & BLOOM, W.H. (1960)Subdural haematoma: A review of 389 cases. Lancet, i,1365.
PERLMUTTER, I. (1961) Subdural haematoma in older patients.J. Amer. med. Ass. 176, 212.
ROSENBLUTH, P.R., ARIAS, B., QUARTETTI, E.V. & CARNEY,A.L. (1962) Current management of subdural haematoma:analysis of 100 consecutive cases. J. Amer. med. Ass. 179,759.
SPENCER, W. (1964) Problems in diagnosis of intracranialdisease among the aged. J. Mt Sinai Hosp. N. Y. 31, 17.
STRANG, R.R. & TovI, D. (1962). Subdural haematomascomplicating anticoagulant therapy. Brit. med. J. i, 845.
STUTEVILLE, P. & WELCH, K. (1958) Subdural haematomain the elderly person. J. Amer. med. Ass. 168, 1445.
WIENER, L.M. & NATHANSON, M. (1962) The relationship ofsubdural haematoma to anticoagulant therapy. Arch.Neurol. 6, 282.
Protected by copyright.
on February 2, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.44.516.785 on 1 O
ctober 1968. Dow
nloaded from