subarachnoid hemorrhage
TRANSCRIPT
Subarachnoid
HEMORRHAGE
DR RAJESH T EAPEN
ATLAS HOSPITAL
MUSCAT
Definition
• Subarachnoid haemorrhage is
defined as bleeding into the
subarachnoid space within the
intracranial vault.
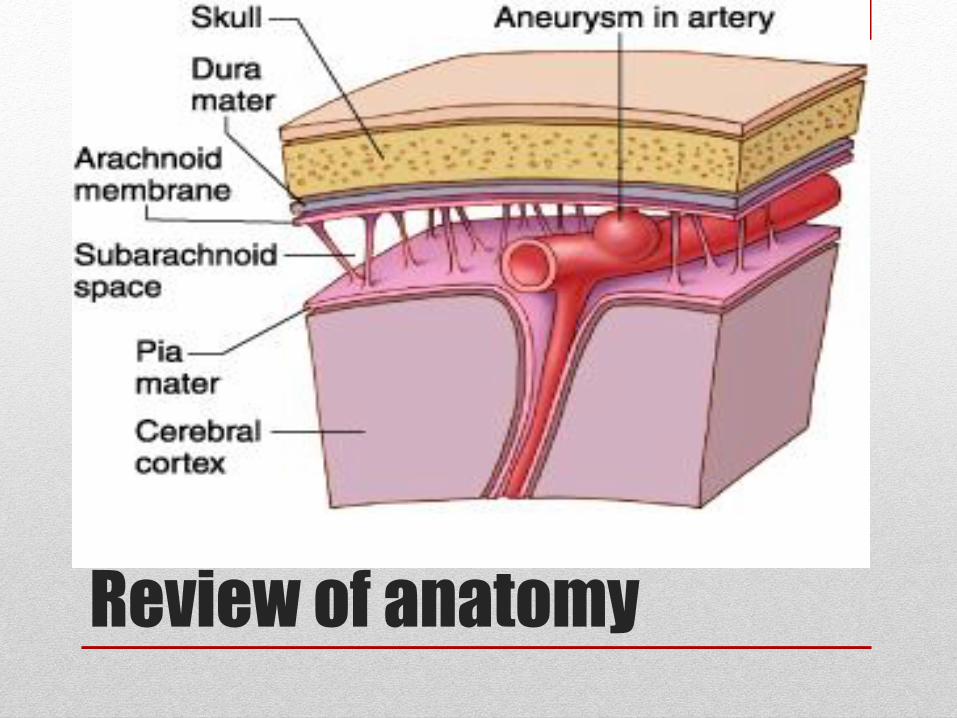
Review of anatomy
Incidence
• The incidence of subarachnoid haemorrhage is 9.1 per
100,000 annually.
• Risk increases in older age 60% higher in age above 80
• Risk of SAH is relatively higher in women over 55 years
than men

Risk factors
• Race
• Sex
• Age
• Genetics
• Smoking
• Alcohol
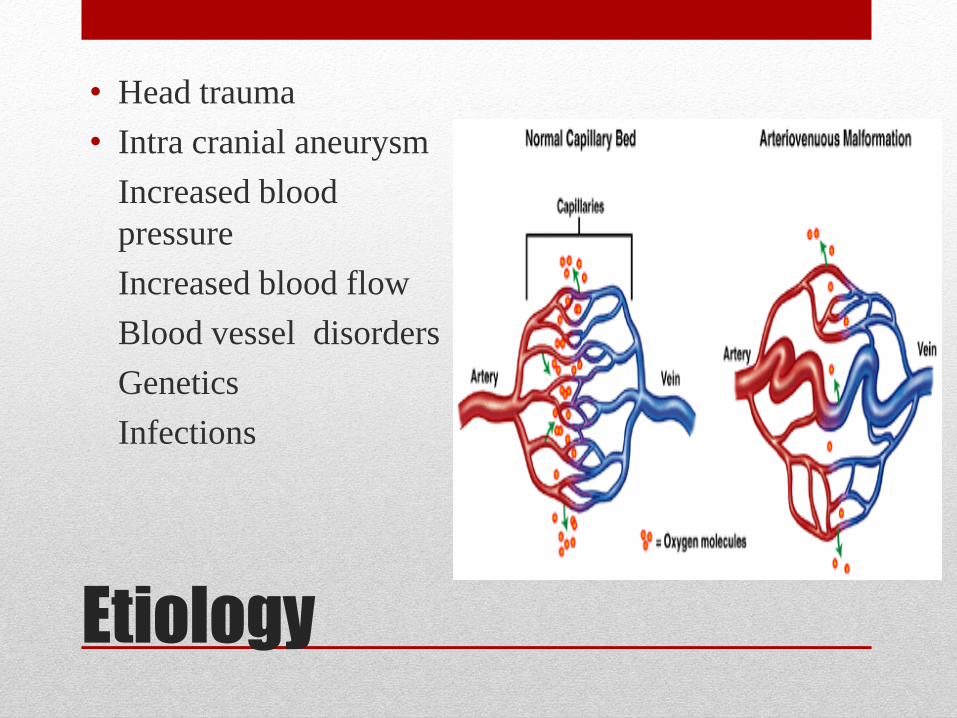
Etiology
• Head trauma
• Intra cranial aneurysm
Increased blood
pressure
Increased blood flow
Blood vessel disorders
Genetics
Infections
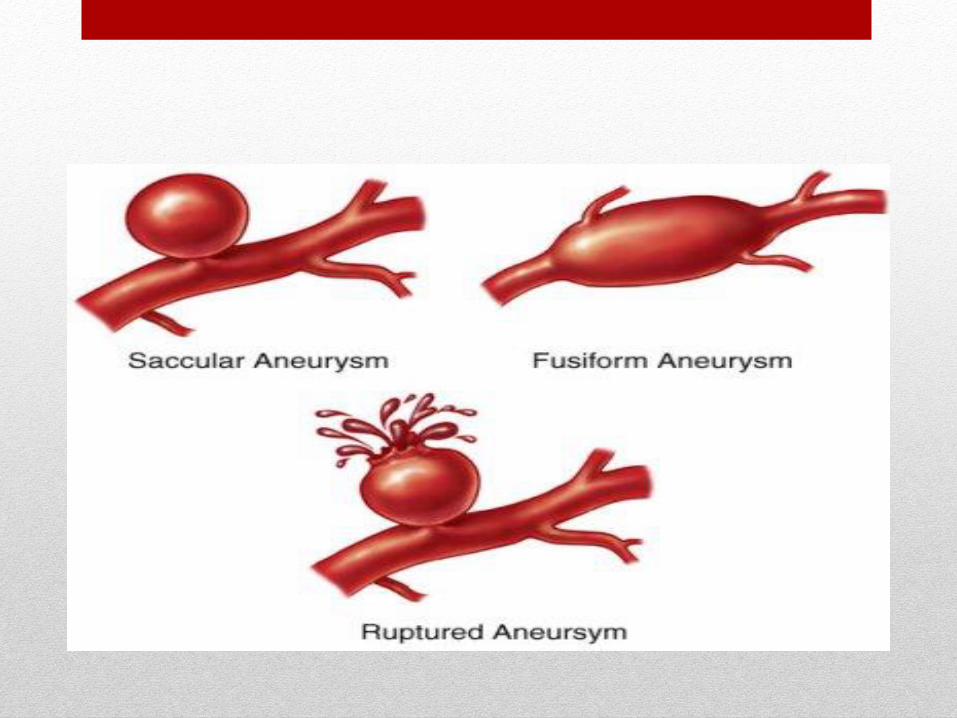
Types of aneurysm
• Berry (saccular)aneurysm
• Giant (fusiform) aneurysm
• Mycotic aneurysm
• Charcot –Bouchard aneurysm
• Traumatic aneurysm
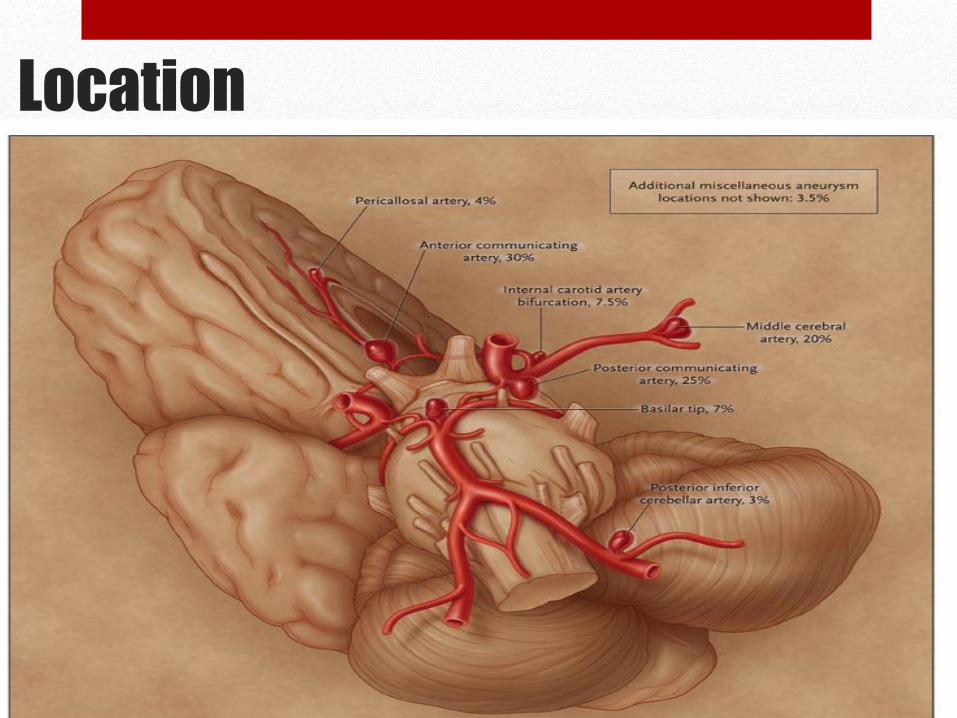
Location
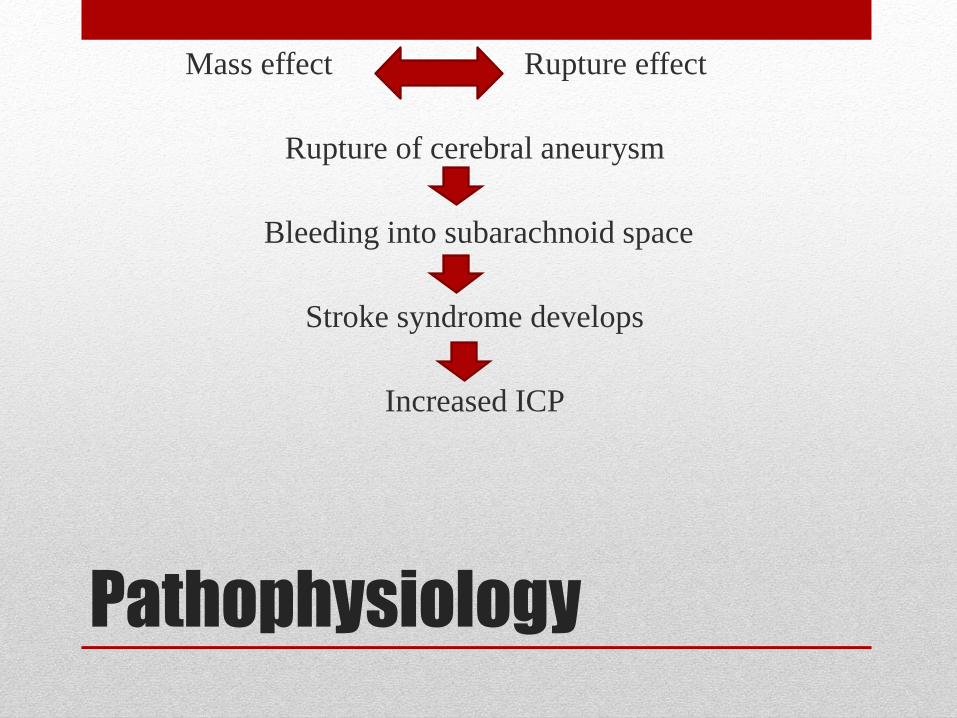
Pathophysiology
Mass effect Rupture effect
Rupture of cerebral aneurysm
Bleeding into subarachnoid space
Stroke syndrome develops
Increased ICP
Risk Factors • Behavioral
• Hypertension
• Smoking
• Alcohol Abuse
• Drug Abuse
• Stress
• Low BMI
• Non-Behavioral
• Female Sex
• History of previous SAH
• Family history
• Polycystic Disease
• Age
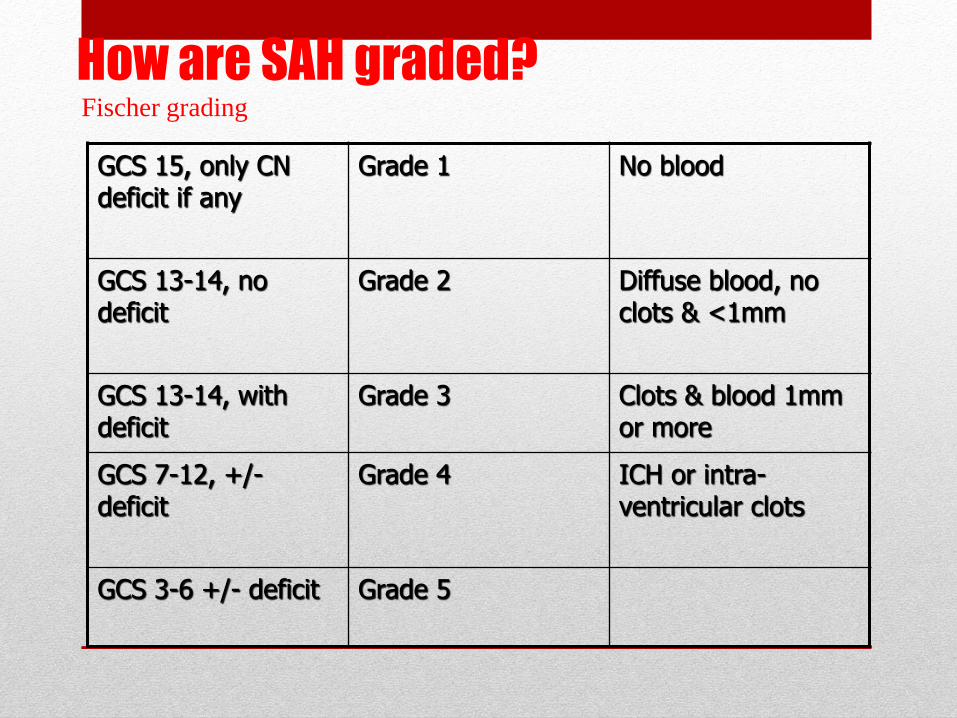
How are SAH graded?
GCS 15, only CN deficit if any
Grade 1 No blood
GCS 13-14, no deficit
Grade 2 Diffuse blood, no clots & <1mm
GCS 13-14, with deficit
Grade 3 Clots & blood 1mm or more
GCS 7-12, +/- deficit
Grade 4 ICH or intra-ventricular clots
GCS 3-6 +/- deficit Grade 5
Fischer grading
Clinical Presentation • “The worst headache of my life”
• Sudden, severe onset with or without LOC (loss of
consciousness)
• Generally associated with nausea and vomiting, stiff neck,
photophobia, restlessness and agitation
• Seizures may occur (most commonly in first 24 hours)
• Typically asymptomatic until rupture occurs
Some times low back pain and bilateral radicular leg pain.
Signs
• Neck stiffness
• Impaired level of consciousness in some patients
• Subhyaloid haemmorhage on optic funduscopy
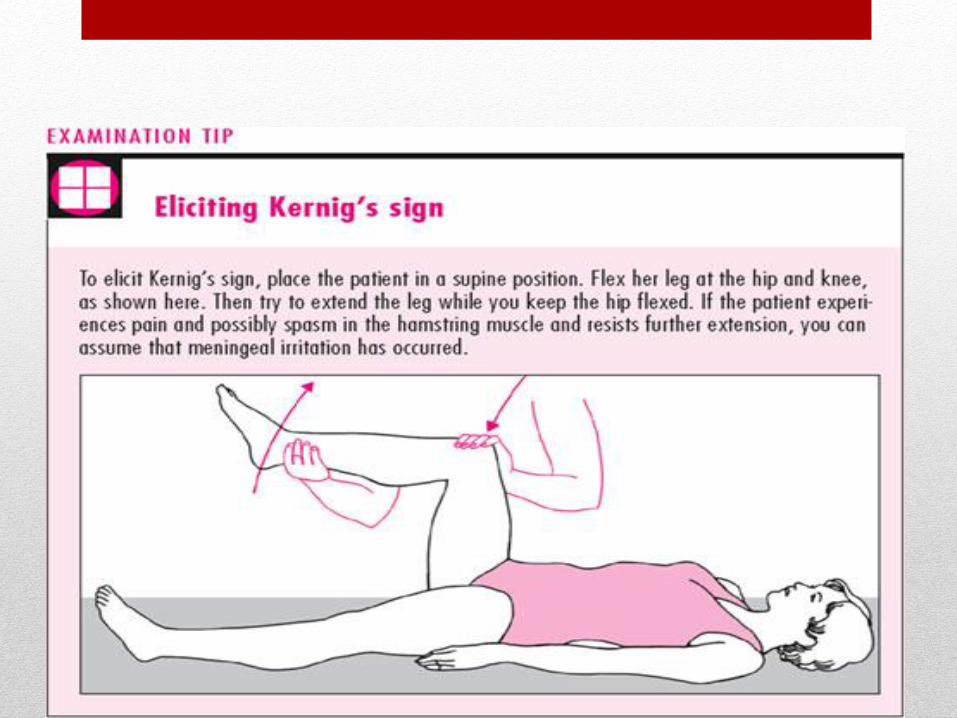
Kernigs sign
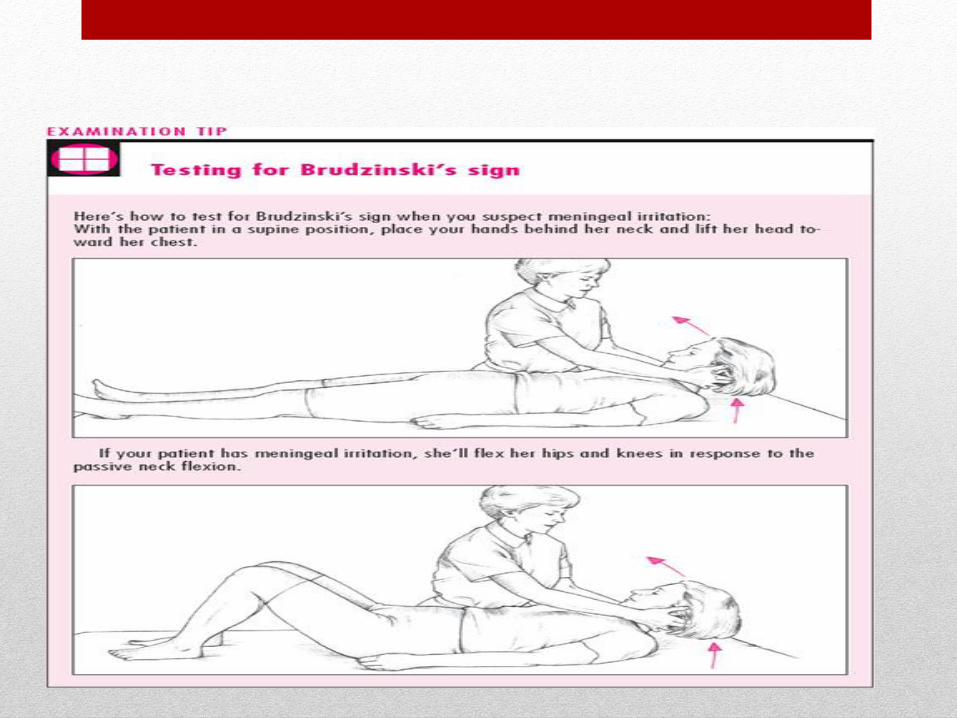
Brudzinskis sign
Grading of SAH
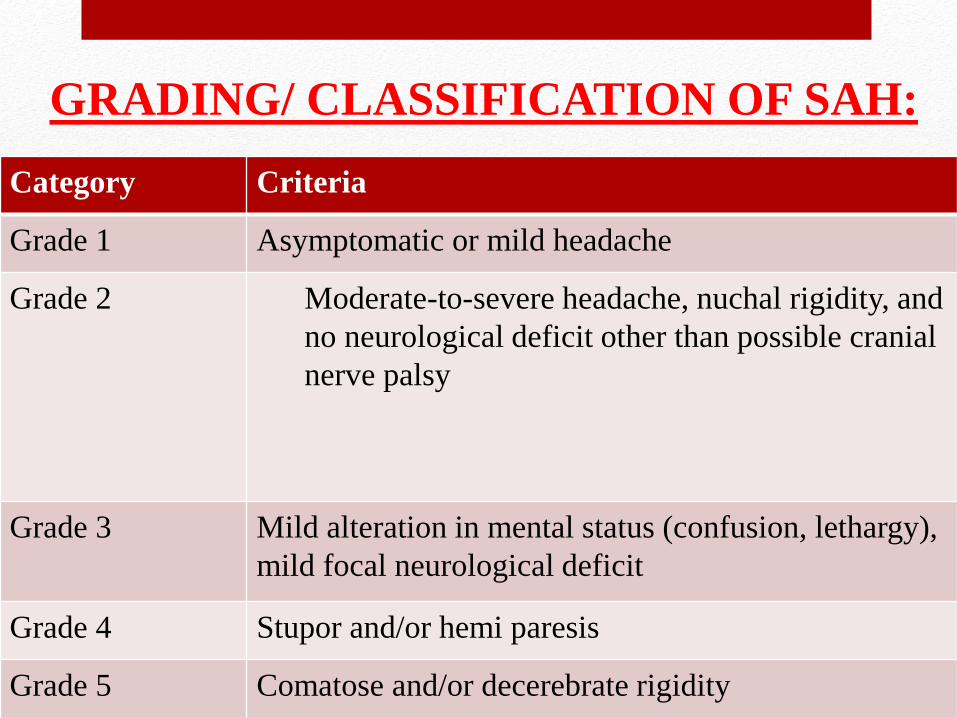
Hunt-Hass classification
Category Criteria
Grade 1 Asymptomatic or mild headache
Grade 2 Moderate-to-severe headache, nuchal rigidity, and
no neurological deficit other than possible cranial
nerve palsy
Grade 3 Mild alteration in mental status (confusion, lethargy),
mild focal neurological deficit
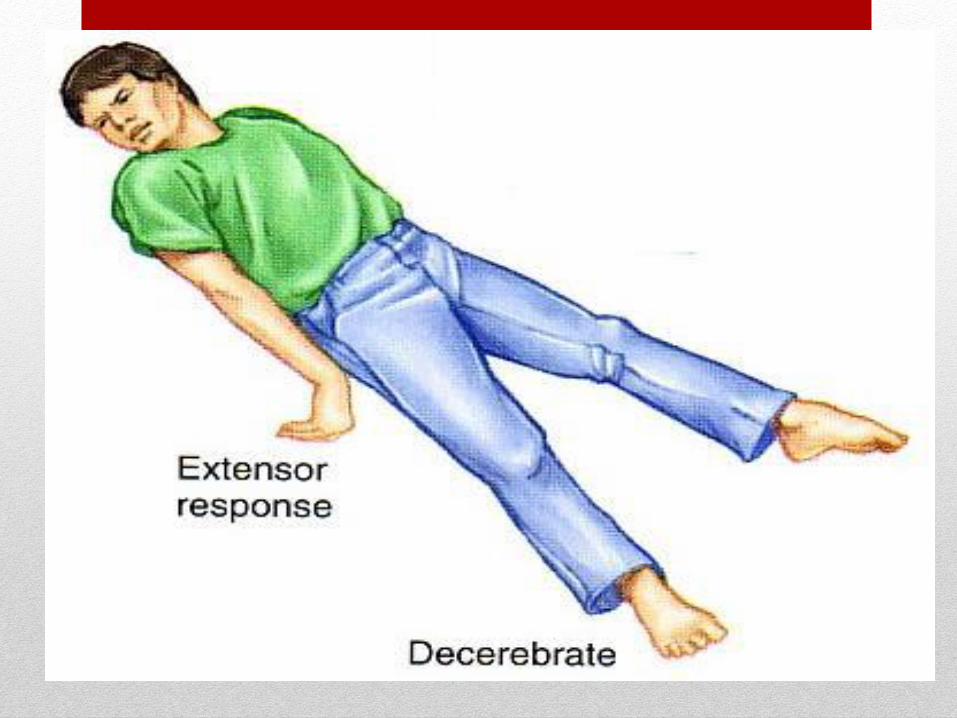
Grade 4 Stupor and/or hemi paresis
Grade 5 Comatose and/or decerebrate rigidity
GRADING/ CLASSIFICATION OF SAH:
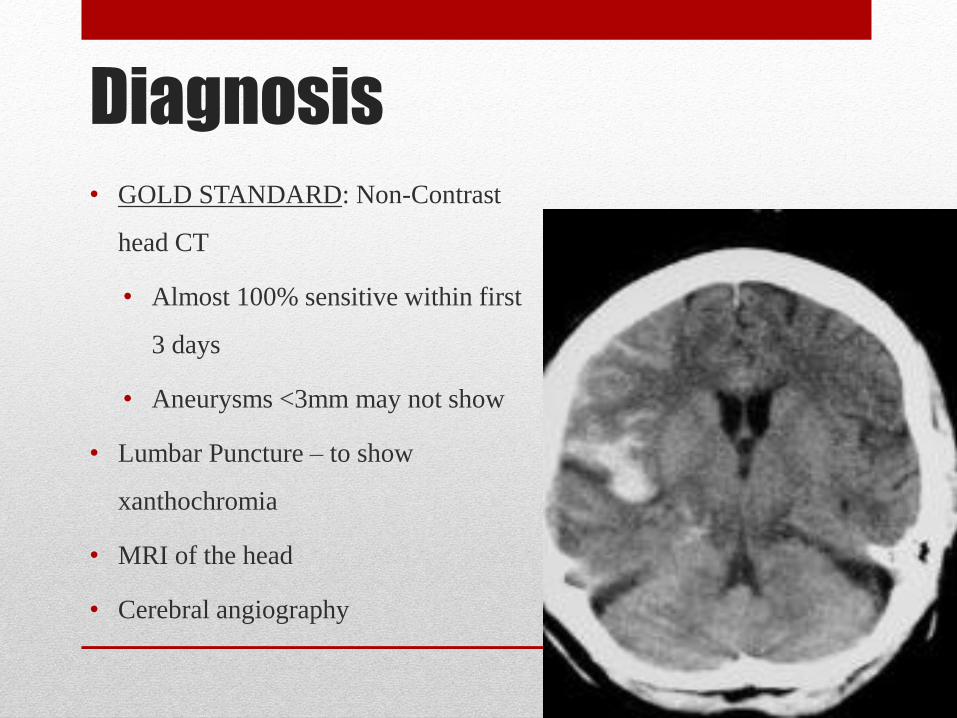
Diagnosis • GOLD STANDARD: Non-Contrast
head CT
• Almost 100% sensitive within first
3 days
• Aneurysms <3mm may not show
• Lumbar Puncture – to show
xanthochromia
• MRI of the head
• Cerebral angiography
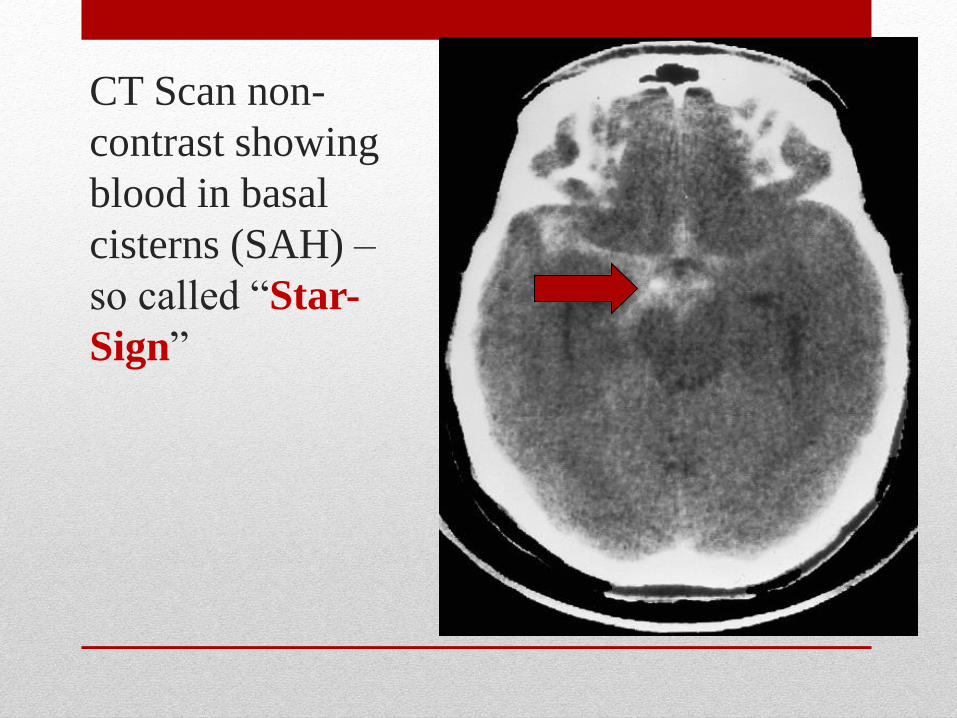
CT Scan non-
contrast showing
blood in basal
cisterns (SAH) –
so called “Star-
Sign”

Management
Medical management
• Acute care
• If patient is comatose ventilator assistance
• ABG analysis
• Emergency CT scan
• Cardiac monitoring
• Pain management
• The goal of treatment is to prevent re bleeding and
cerebral vasospasm
• Re bleeding
• Bed rest
• Recombinant activator factor VII
• Calcium channel blocker
• Smooth muscle relaxants
• Triple H therapy
Hypervolumia
Hypertension
Hemodilution
• Steroids
• Antihypertensive
• Antipyretics
• Anticonvulsants
• Analgesics
• Sedatives
• Stool softeners
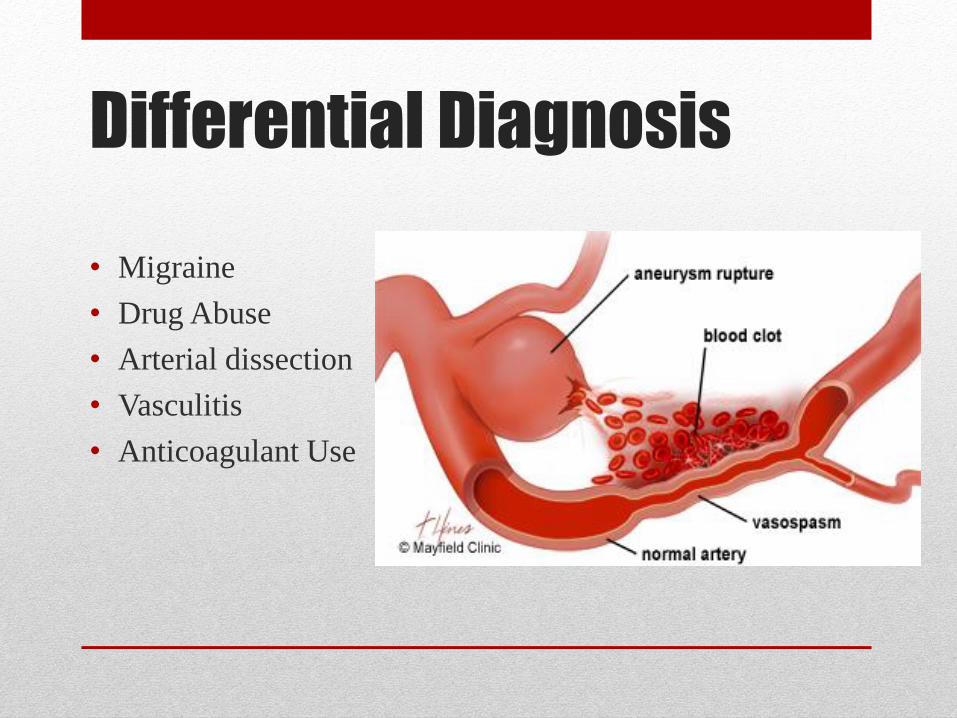
Differential Diagnosis
• Migraine
• Drug Abuse
• Arterial dissection
• Vasculitis
• Anticoagulant Use
Pharmacological Treatment
• Monitor CVP (Central Venous Pressure) – if <7 0.9% NS bolus
• Maintain SBP 90-140mmHg until aneurysm is secured (clipping or
coiling)
• If non-traumatic – control vasospasms with Nimodipine 60mg q4h
X 21 days or 30mg q2h X21 days
• Prevent seizures – levetiracetam 500mg IV Q12h
• Control blood glucose levels
Nimodipine (Nimotop®)
• Indication: Subarachanoid Hemorrhage (Hunt & Hess 1-V)
• MOA: Calcium channel blocker – prevents calcium entry into
smooth muscle cells during depolarization which inhibits
vasoconstriction
• Dose: 30mg PO q2h for 21 days OR 60mg PO q4h for 21 days
• Interactions: CYP3A4 Inhibitors and Inducers
• Pharmacokinetics: 95% protein bound, hepatic metabolism
• Monitoring: BP, HR, Neurological improvement
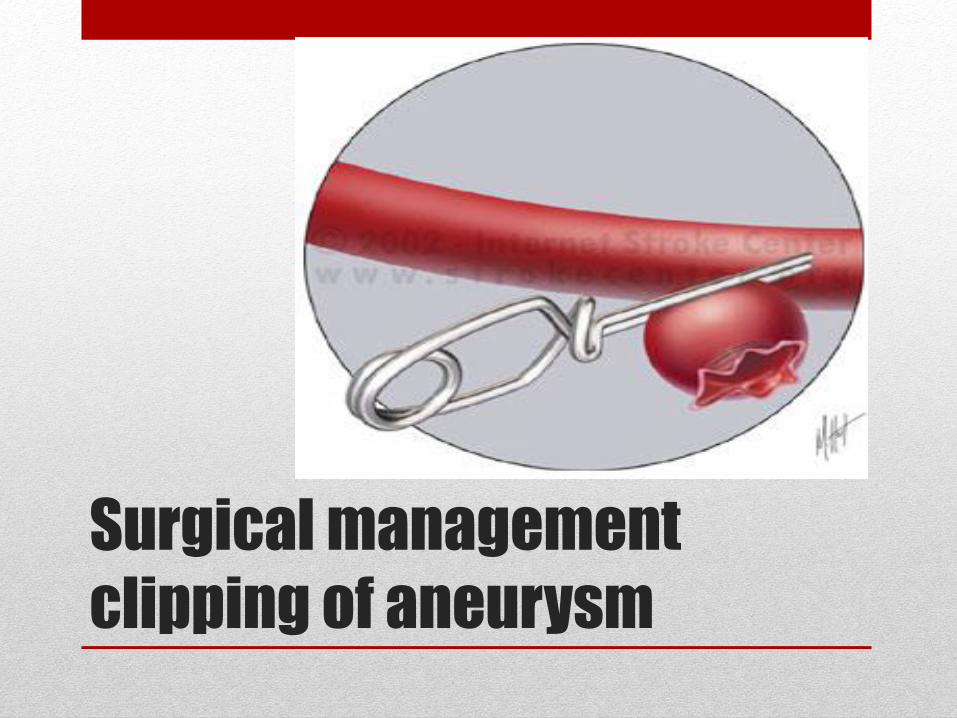
Surgical management
clipping of aneurysm
22/02/2015© 2009, American Heart Association. All rights reserved.
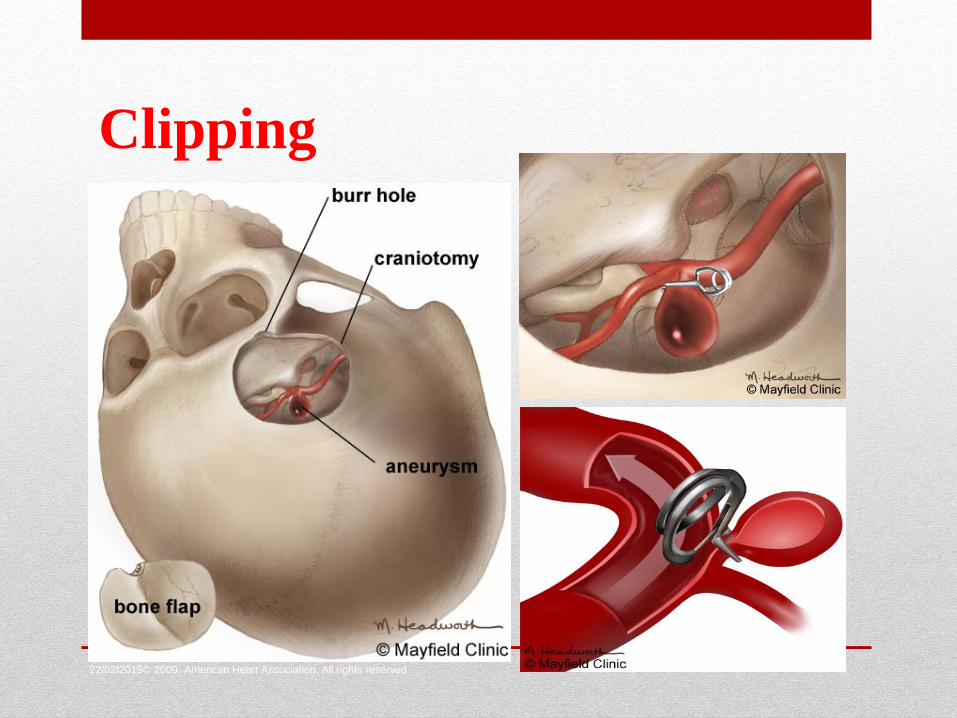
Clipping
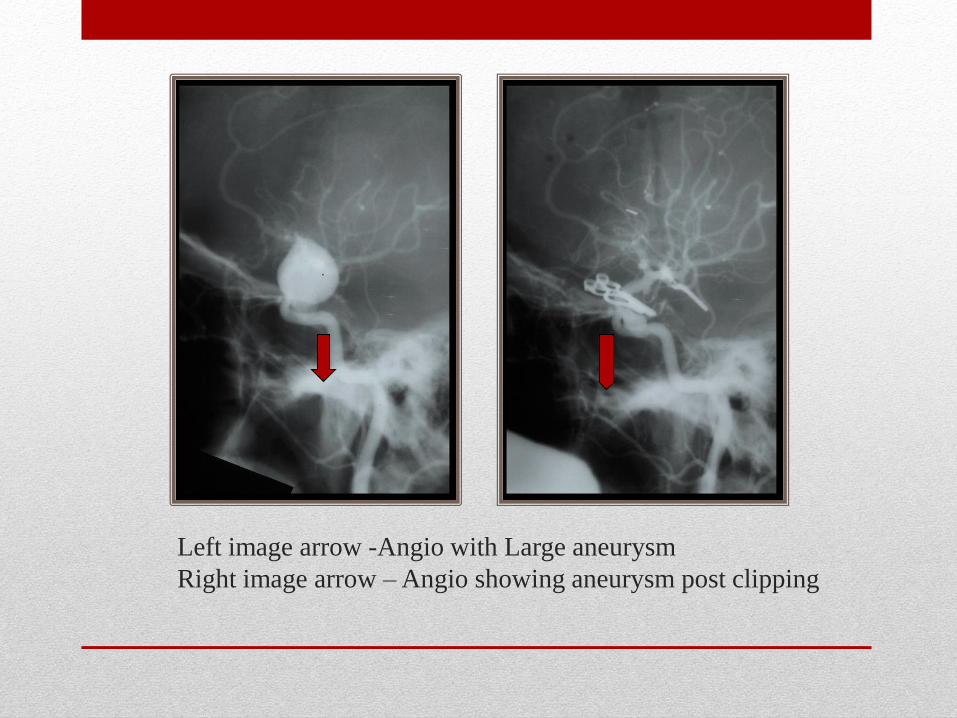
Left image arrow -Angio with Large aneurysm
Right image arrow – Angio showing aneurysm post clipping
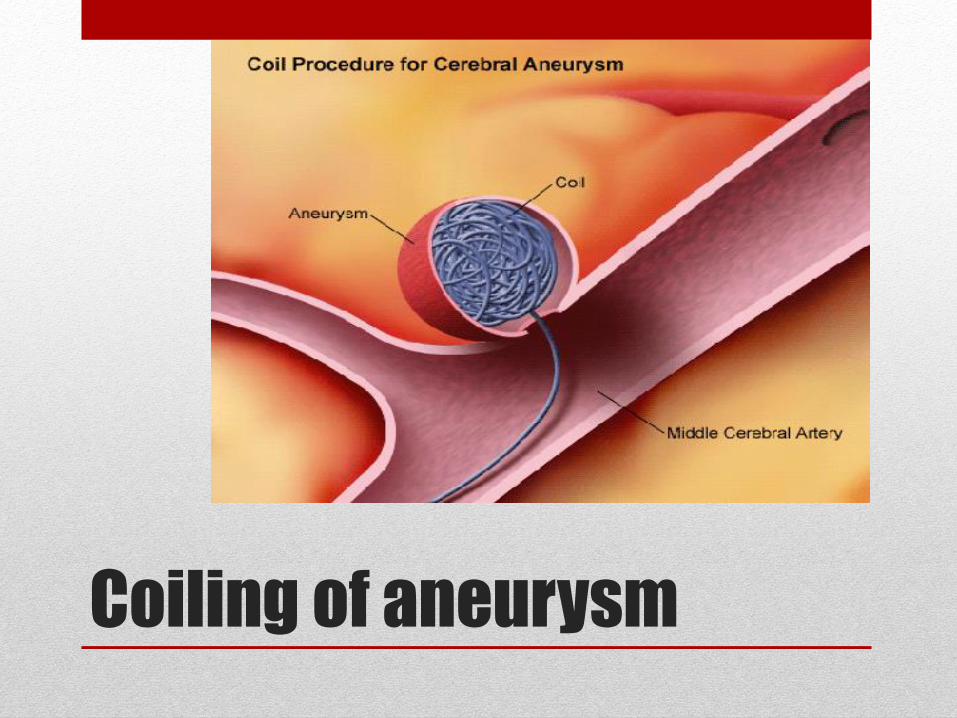
Coiling of aneurysm
22/02/2015© 2009, American Heart Association. All rights reserved.
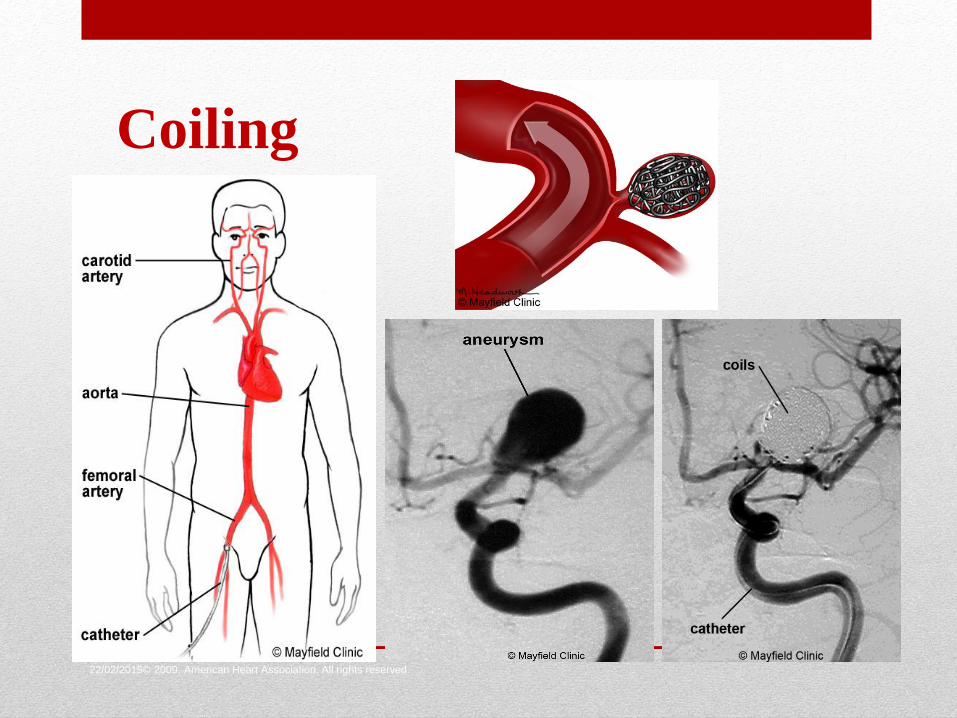
Coiling
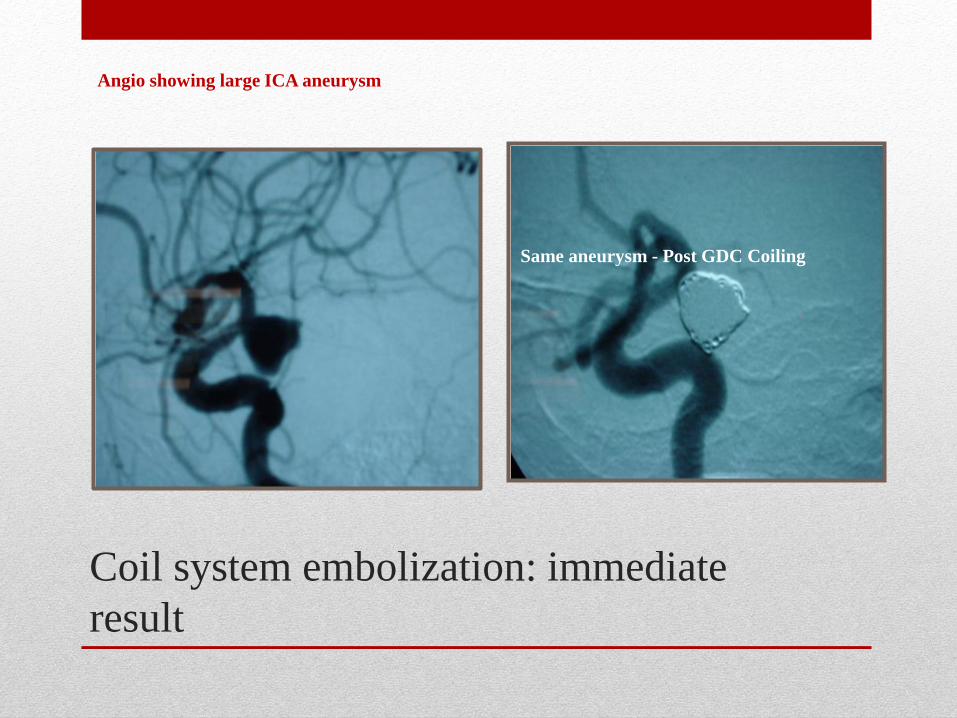
Coil system embolization: immediate
result
Angio showing large ICA aneurysm
Same aneurysm - Post GDC Coiling
Infectious problems in SAH patients
• important to distinguish saccular aneurysms from mycotic (frequently post-bacteremic) aneurysms
• postoperative infections
• postoperative meningitis may be aseptic, but this is a diagnosis of exclusion
• particularly a problem in the SAH patient because the hemorrhage itself causes meningeal reaction
• complications of critical illness
• complications of steroid use
Seizures in SAH patients
• about 6% of patients suffer a seizure at the time of the
hemorrhage
• distinction between a convulsion and decerebrate posturing
may be difficult
• postoperative seizures occur in about 1.5% of patients despite
anticonvulsant prophylaxis
• remember to consider other causes of seizures (e.g., alcohol
withdrawal)
Seizures in SAH
patients
• patients developing delayed ischemia may seize
following reperfusion by angioplasty
• late seizures occur in about 3% of patients
Seizure management in
SAH
• seizures in patients with unsecured aneurysms may
result in rebleeding, so prophylaxis (typically
phenytoin) is commonly given
• even a single seizure usually prompts a CT scan to
look for a change in the intracranial pathology
• additional phenytoin is frequently given to raise the serum
concentration to 20+ ug/mL
• lorazepam to abort serial seizures or status epilepticus
Nursing management
• Altered neurological function related haemorrhage from
cerebral aneurysm
• Pain due to cerebral haemorrhage
• Sensory input distortion related to meningeal irritation
• Potential for seizure related to cerebral irritation
• Potential for neurological deterioration related to re
bleeding or cerebral vasospasm
Complication
• Rebleeding
• Hydrocephalus
• Intraventricular haemorrhage
• Increased intracranial pressure
• Intracerebral haemorrhage
• Seizures
• Cerebral vasospasm
COMPLICATIONS
• Respiratory complication
• Venous complication
• Cardiovascular complication
• Fluid and electrolyte disturbance
• Gastrointestinal complication
Complications with SAH • Vasospasm
• Blood vessel goes into spasm causing ischaemia - stroke
• To prevent keep them filled with at least 3L fluid day & nimodipine IV/PO & insert central line to monitor central venous pressure – aiming for 8-10
• Suspected with deteriorating GCS/new neurological deficit
• Treatment – Urgent CT brain to rule out a bleed as a cause of the deterioration then urgent angiogram to diagnose & treat vasospasm
• Greatest risk of vasospasm is days 4-7 but significant risk for first 3 weeks after bleed, therefore must use preventive measures for at least 3 weeks
Complications with SAH • Hyponatraemia
• Susceptible due to being fluid loaded & cerebral salt wasting
• Cerebral salt wasting = renal loss of sodium due to intracranial pathology ? Cause. Loss of water & salt (whereas SIADH is loss of salt & retention of water)
• Treat with normal or hypertonic saline
• If refractory may need a mineralocorticoid e.g. fludrocortisone to stimulate renal reabsorption – but this should only be used under instructions from consultant endocrinologist
Complications with SAH • Seizures
• A seizure is a disturbance of sensation, movement or consciousness
• All seizures originate from the surface of the brain – cortex
• Blood is an irritant to the cortex
• Prophylaxis with phenytoin or levetiracetam
• Ensure phenytoin levels are therapeutic
• Treat as seizure from any cause & suspect re-bleed
Complications with
SAH
• Venous Thrombo Embolism
• On bed rest
• TEDS (Thrombo Embolism Deterrent Stockings)
• Prophylactic enoxaparin as soon as consultant sees fit
• Always keep VTE in the back of your mind
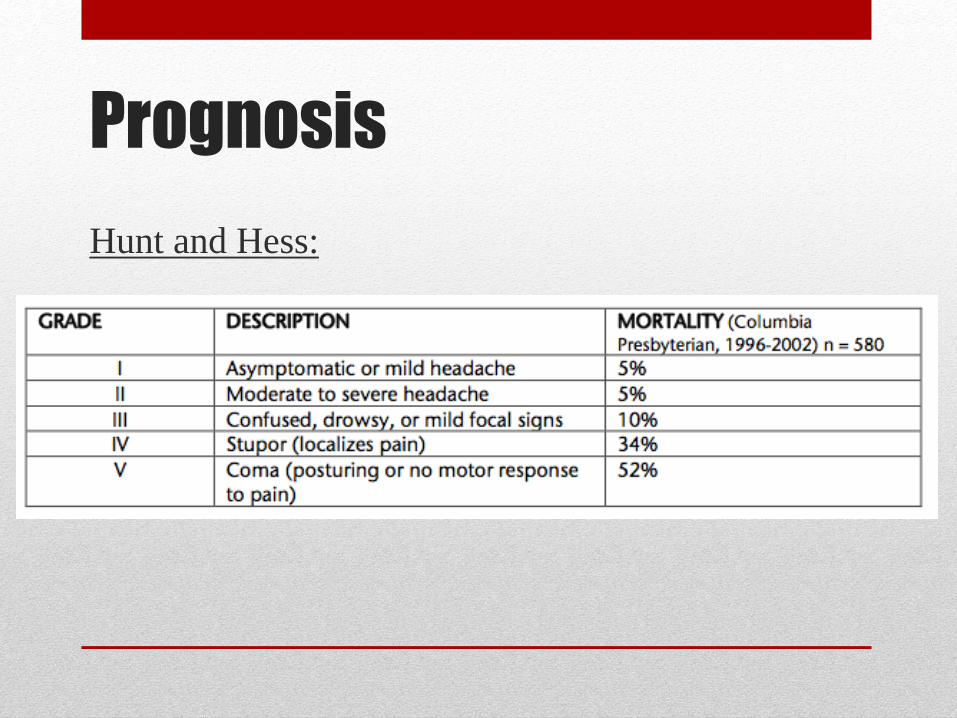
Prognosis
Hunt and Hess:
