su1134 comparative efficacy of biologic therapy in the management of biologic-naive patients with...
TRANSCRIPT
AG
AA
bst
ract
s
* indicate reference categories for multivariate analysis
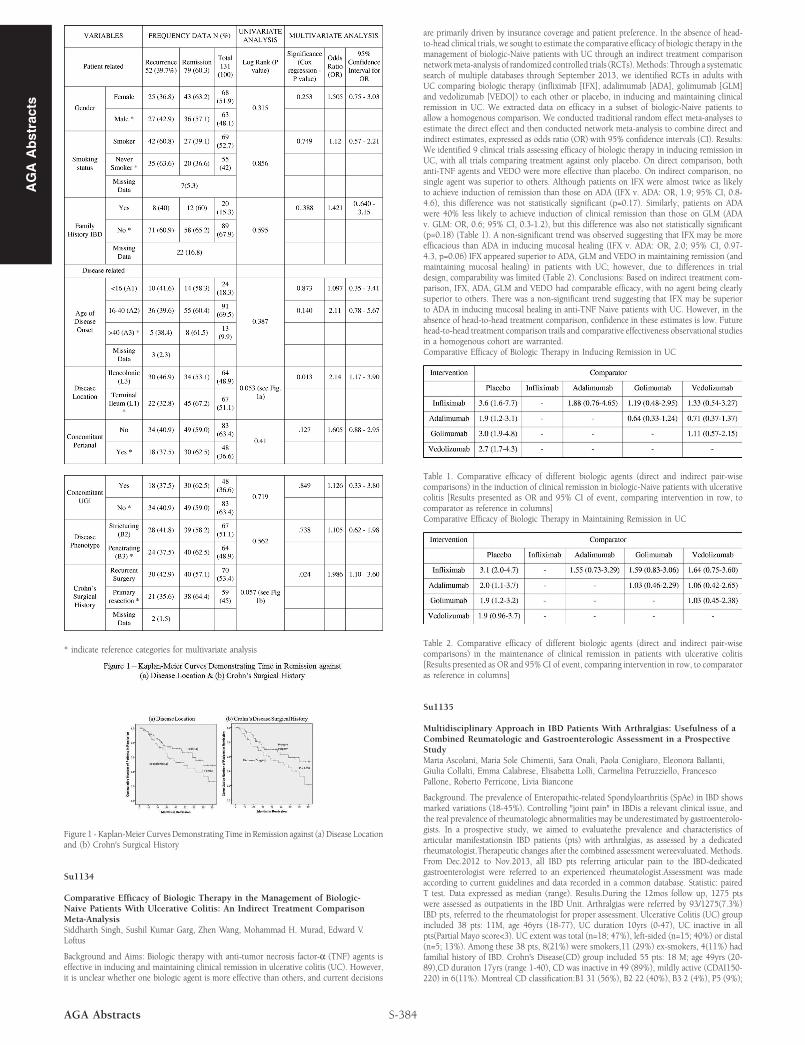
Figure 1 - Kaplan-Meier Curves Demonstrating Time in Remission against (a) Disease Locationand (b) Crohn's Surgical History
Su1134
Comparative Efficacy of Biologic Therapy in the Management of Biologic-Naive Patients With Ulcerative Colitis: An Indirect Treatment ComparisonMeta-AnalysisSiddharth Singh, Sushil Kumar Garg, Zhen Wang, Mohammad H. Murad, Edward V.Loftus
Background and Aims: Biologic therapy with anti-tumor necrosis factor-α (TNF) agents iseffective in inducing and maintaining clinical remission in ulcerative colitis (UC). However,it is unclear whether one biologic agent is more effective than others, and current decisions
S-384AGA Abstracts
are primarily driven by insurance coverage and patient preference. In the absence of head-to-head clinical trials, we sought to estimate the comparative efficacy of biologic therapy in themanagement of biologic-Naive patients with UC through an indirect treatment comparisonnetwork meta-analysis of randomized controlled trials (RCTs). Methods: Through a systematicsearch of multiple databases through September 2013, we identified RCTs in adults withUC comparing biologic therapy (infliximab [IFX], adalimumab [ADA], golimumab [GLM]and vedolizumab [VEDO]) to each other or placebo, in inducing and maintaining clinicalremission in UC. We extracted data on efficacy in a subset of biologic-Naive patients toallow a homogenous comparison. We conducted traditional random effect meta-analyses toestimate the direct effect and then conducted network meta-analysis to combine direct andindirect estimates, expressed as odds ratio (OR) with 95% confidence intervals (CI). Results:We identified 9 clinical trials assessing efficacy of biologic therapy in inducing remission inUC, with all trials comparing treatment against only placebo. On direct comparison, bothanti-TNF agents and VEDO were more effective than placebo. On indirect comparison, nosingle agent was superior to others. Although patients on IFX were almost twice as likelyto achieve induction of remission than those on ADA (IFX v. ADA: OR, 1.9; 95% CI, 0.8-4.6), this difference was not statistically significant (p=0.17). Similarly, patients on ADAwere 40% less likely to achieve induction of clinical remission than those on GLM (ADAv. GLM: OR, 0.6; 95% CI, 0.3-1.2), but this difference was also not statistically significant(p=0.18) (Table 1). A non-significant trend was observed suggesting that IFX may be moreefficacious than ADA in inducing mucosal healing (IFX v. ADA: OR, 2.0; 95% CI, 0.97-4.3, p=0.06) IFX appeared superior to ADA, GLM and VEDO in maintaining remission (andmaintaining mucosal healing) in patients with UC; however, due to differences in trialdesign, comparability was limited (Table 2). Conclusions: Based on indirect treatment com-parison, IFX, ADA, GLM and VEDO had comparable efficacy, with no agent being clearlysuperior to others. There was a non-significant trend suggesting that IFX may be superiorto ADA in inducing mucosal healing in anti-TNF Naive patients with UC. However, in theabsence of head-to-head treatment comparison, confidence in these estimates is low. Futurehead-to-head treatment comparison trails and comparative effectiveness observational studiesin a homogenous cohort are warranted.Comparative Efficacy of Biologic Therapy in Inducing Remission in UC
Table 1. Comparative efficacy of different biologic agents (direct and indirect pair-wisecomparisons) in the induction of clinical remission in biologic-Naive patients with ulcerativecolitis [Results presented as OR and 95% CI of event, comparing intervention in row, tocomparator as reference in columns]Comparative Efficacy of Biologic Therapy in Maintaining Remission in UC
Table 2. Comparative efficacy of different biologic agents (direct and indirect pair-wisecomparisons) in the maintenance of clinical remission in patients with ulcerative colitis[Results presented as OR and 95% CI of event, comparing intervention in row, to comparatoras reference in columns]
Su1135
Multidisciplinary Approach in IBD Patients With Arthralgias: Usefulness of aCombined Reumatologic and Gastroenterologic Assessment in a ProspectiveStudyMarta Ascolani, Maria Sole Chimenti, Sara Onali, Paola Conigliaro, Eleonora Ballanti,Giulia Collalti, Emma Calabrese, Elisabetta Lolli, Carmelina Petruzziello, FrancescoPallone, Roberto Perricone, Livia Biancone
Background. The prevalence of Enteropathic-related Spondyloarthritis (SpAe) in IBD showsmarked variations (18-45%). Controlling "joint pain" in IBDis a relevant clinical issue, andthe real prevalence of rheumatologic abnormalities may be underestimated by gastroenterolo-gists. In a prospective study, we aimed to evaluatethe prevalence and characteristics ofarticular manifestationsin IBD patients (pts) with arthralgias, as assessed by a dedicatedrheumatologist.Therapeutic changes after the combined assessment wereevaluated. Methods.From Dec.2012 to Nov.2013, all IBD pts referring articular pain to the IBD-dedicatedgastroenterologist were referred to an experienced rheumatologist.Assessment was madeaccording to current guidelines and data recorded in a common database. Statistic: pairedT test. Data expressed as median (range). Results.During the 12mos follow up, 1275 ptswere assessed as outpatients in the IBD Unit. Arthralgias were referred by 93/1275(7.3%)IBD pts, referred to the rheumatologist for proper assessment. Ulcerative Colitis (UC) groupincluded 38 pts: 11M, age 46yrs (18-77), UC duration 10yrs (0-47), UC inactive in allpts(Partial Mayo score<3). UC extent was total (n=18; 47%), left-sided (n=15; 40%) or distal(n=5; 13%). Among these 38 pts, 8(21%) were smokers,11 (29%) ex-smokers, 4(11%) hadfamilial history of IBD. Crohn's Disease(CD) group included 55 pts: 18 M; age 49yrs (20-89),CD duration 17yrs (range 1-40), CD was inactive in 49 (89%), mildly active (CDAI150-220) in 6(11%). Montreal CD classification:B1 31 (56%), B2 22 (40%), B3 2 (4%), P5 (9%);