student no. e10739 september 2016 a dissertation submitted
TRANSCRIPT

What are the similarities and differences between TCM and Ayurveda?
Student No. E10739
September 2016
A dissertation submitted in partial fulfilment of the Licentiate in Acupuncture.
Word count: 3741
Submitted: 10th May, 2019

i
Abstract
Traditional Chinese Medicine (TCM) and Ayurveda are two forms of traditional Asian
medicine that are still in practice and have spread through the world, under the
umbrella of Complementary and Alternative Medicine (CAM) in countries where the
mainstream practice is allopathic medicine.
This paper reviews the existing literature that compares TCM and Ayurveda, starting
with their historical development and cross pollination between both systems. It then
examines their view on energetic physiology, where both systems coincide in their
consideration of a life force (Qi/Prana) and its effects on the homeostasis of the body
through a dynamic Five Element/Tridosha model. TCM, however, has a concept of
Yin/Yang which has no direct correspondence in Ayurveda. Diagnostic tools such as
pulse taking and tongue examination are similar in each system, and both TCM and
Ayurveda have a prominent herbal medicine component. Massage, exercise and
acupuncture/marma points are also important in terms of maintenance of optimal
health and disease prevention. Since TCM and Ayurveda are often used alongside
allopathic medicine in the treatment of complex diseases, this paper aims to provide
TCM practitioners with an overview of Ayurveda in relationship to TCM which can
inform their practice.

ii
Table of Contents Introduction......................................................................................................................1
Methods............................................................................................................................2
Results..............................................................................................................................3
1. Historicalcontextandcrosspollination..............................................................................3
2. Energeticphysiology..........................................................................................................5
2.1QiandPrana............................................................................................................................5
2.2FiveElements,TridoshaandYin/Yang.....................................................................................6
3. Healingmodalities.............................................................................................................9
3.1HerbalmedicinesinAyurvedaandTCM..................................................................................9
3.2Acupunctureandyoga...........................................................................................................10
3.2.1FurthercommentaryonQi/Pranameasurements.......................................................................11
3.3Acupunctureandchakras......................................................................................................12
4. Bioinformatics..................................................................................................................13
Discussion.......................................................................................................................15
Conclusion.......................................................................................................................20
References......................................................................................................................21
AppendixA......................................................................................................................25

iii
Acknowledgements
To my dear husband, Keith Pritchard, who encouraged me to enroll in this course and
has selflessly supported this endeavor for the last three years.
To my yoga teachers Hamish Hendry and Ruth Westoby who patiently try to educate
me in yoga philosophy and Ayurveda.
To my acupuncture mentors, Suky Bains Miller and Michelle Austen-Marriott, who
have given invaluable advice throughout my study of acupuncture.

1
Introduction
Traditional Chinese Medicine (TCM) and Ayurveda are the two most globalised forms
of traditional Asian medicine. TCM has a philosophical background of Daoism and
Ayurveda of Vedic philosophy (Kim, Pham, & Koh, 2011).
Both systems place the patient within the context of a universe made up of a
combination of elements: Wood, Fire, Earth, Metal and Water in TCM and Ether, Air,
Fire, Water and Earth in Ayurveda (Patwardhan, Warude, Pushpangadan, & Bhatt,
2005). They also share the concept of a “life energy” that flows through the body,
called Qi in TCM and Prana in Ayurveda, which must flow unimpeded for health or can
lead to disease when blocked (Rosch, 2009).
Another common feature is that they are both patient-centric as opposed to the
allopathic medicine’s disease-centric view. The patient is examined and their
constitution and symptoms are assessed, and with this a specific therapeutic
treatment will be prescribed. This means that the same disease in two different people
might be treated with different herbal formulations or therapeutic methods (Kim, Pham,
& Koh, 2011).
TCM and Ayurveda are widely used in their country of origin, with TCM accounting for
40% of all healthcare delivered in China and 77% of Indian households using
Ayurvedic products. Within the context of Complementary and Alternative Medicine
(CAM), both are also growing rapidly outside China and India, motivated by concern
about adverse effect of drugs and a search for gentler means of managing chronic
diseases in countries with increasingly longer life expectancy (The Economic Times,
2018; World Health Organization, 2002).
As a soon to be practitioner of TCM and a long-term student of yoga, I have an interest
in both medicines although my expertise in Ayurveda is only superficial. This
dissertation has enabled me to understand the underpinning concepts of Ayurveda
and how they relate to TCM, and spurred an interest in the areas that have not been
fully covered by research yet.

2
Methods
The following search query on the Cambridge University Library was used:
Title contains TCM Ayurveda
OR Title contains Chinese medicine Ayurveda
OR Title contains Chinese Ayurveda
This search attempted to capture the literature where both systems were mentioned.
It returned 18 results, out of which 5 were of restricted access or broken links and thus
excluded from this review.
The advanced search in Google Scholar did not allow for building complex queries;
instead the search query was set to:
find articles with all the words ‘TCM’ and ‘Ayurveda’ that occur in the title of the
article
It returned three articles, one of which was excluded as its focus was on Traditional
Arabic and Islamic Medicine.
Expanding the term “TCM” into “Traditional Chinese Medicine” in Google Scholar
returned 46 results; most of these, however, were citations and the rest had already
been acquired by the earlier searches, but it did return a dissertation on the
comparison between the two medicines as a new result.
The same search in Pubmed did not return any new results.
The rest of the literature was acquired by following references in the search results.

3
Results
1. Historicalcontextandcrosspollination
TCM and Ayurveda are the two most ancient still practiced traditional medicine
systems in the world. The earliest manuscripts for medical practice in China are found
in the Historical Memoirs (Shi Ji), about 500 B.C., which discusses pulse study, tongue
inspection and patient questioning as diagnostic tools, as well as acupuncture,
moxibustion, massage, remedial exercise and plant medicine as therapeutic
modalities. For Ayurveda, while Vedic healing is recorded in the Atharva Veda as a
manual of magic, the first recording of empirical medicine is the Charaka Samhita1
dated between the 8th and 10th centuries B.C. (Svoboda & Lade, 1995).
Frawley, Ranade & Lele (2003, p.9) attribute Ayurveda’s initial influence on TCM to
Bodhidharma (500 – 600 A.D.), a Buddhist monk who is traditionally credited as the
transmitter of Chan Buddhism to China and who initiated the physical training of the
monks of Shaolin Temple2, which led to the creation of Shaolin kungfu. Part of the
warrior training included knowledge of marmas, points on the body that can be used
specifically for the diagnosis and treatment of disease or generally for promoting health
1 “Compendium of Charaka” (Charaka being considered the “Indian father of medicine”), describes
ancient theories on the human body, etiology, symptomology and therapeutics for a wide range of
diseases.
2 built around 300 A.D. in the Hohan province of China to accommodate monks travelling from India to
China

4
and longevity. Frawley et al. (2005) relate these marma points to acupuncture points
in Ayurveda and Marma Therapy, but don’t go into any comparative detail.
As Buddhism thrived in China under the Tang dynasty, the number of Buddhist
monasteries and temples increased rapidly and many canonical Ayurvedic works were
translated into Chinese. An example is the Neng qing yijie yanjibing doloni jing, “A
classic on a spell to cure all eye diseases” by Amoghavajra3 (Takakusu & Watanabe,
2000)., which touches upon the standard etiology of eye diseases as defined by the
Tridosha theory of Ayurveda (Deshpande, 2008).
An area where there was a healthy exchange of ideas in both directions is
pharmacology. China imported hemp, sandalwood, cardamom, cinnamon and other
herbs from India while India imported rhubarb, licorice, gingseng, mugwort and tea
from China (Svoboda & Lade, 1995). All of these were used medicinally in both
systems.
The blocking of the Silk Road due to Muslim invasions and the decline of Buddhism in
India and China meant that from the 10th century A.D. onward, TCM and Ayurveda
were essentially isolated from each other. The introduction of European medicine to
China and India from the 18th century A.D. signified the decline of both traditional
medicines until their current resurgence.
3 Amoghavajra (अमोघव&) was a prolific translator acknowledged as one of the Eight Patriarchs of the
Doctrine in Shingon Buddhism.
5
2. Energeticphysiology
Neither TCM nor Ayurveda based their mapping of human physiology on internal
anatomical study. This is because in both cultures, dissection was considered a
profanity. In China, it was believed that it would interfere with the Po4 and its capacity
to return to the earth. In India, any damage to the corpse before its cremation was
thought to continue onto the soul’s next incarnation (Svoboda & Lade, 1995, p. 93).
2.1QiandPrana
Both systems posit the existence of a life force called Qi in TCM and Prana in
Ayurveda, which travels through TCM’s meridians and Ayurveda’s 72,000 nadis
(Greenwood, 2006). Gasseholm (2012) identifies this commonality and likens it to
Wilhelm Reich’s orgone, a biological or cosmic energy that can be concentrated using
insulated Faraday cages called orgone accumulators5 (Turner, 2011, pp. 222-223).
But while Reich’s orgone experiments were dismissed by Albert Einstein (Reich, 1953)
and ultimately led to Reich’s incarceration, modern attempts to measure Qi and/or
Prana aim to legitimize TCM and Ayurveda in the world of allopathic medicine, which
is skeptical about non-measurable attributes.
Narayanan, Korotkov, & Srinivasan (2018) propose a Unified System of Medicine that
uses electro photonic imaging (EPI) to measure “communication energy”, “normalized
4 The soul of the Yin, associated with the Lungs 5 Sean Connery is said to have owned an orgone accumulator (Turner, 2011, July 08). There seem to
be others in existence (Figure 3, Appendix A).

6
area” and “entropy”. They claim that EPI can measure communication in the meridians
(TCM) or nadis (Ayurveda) by taking these three measurements in the ten fingers of
the hands. However, the “organ systems” that they list (endocrine, pituitary, pancreas,
coccyx) are not part of the medical model of either TCM or Ayurveda.
2.2FiveElements,TridoshaandYin/Yang
Svoboda & Lade (1995), Gasseholm (2012) and Kim et al. (2011) all comment that
TCM and Ayurveda have a theory of Five Elements: Wood, Fire, Earth, Metal and
Water in TCM and Ether, Air, Fire, Water and Earth in Ayurveda. But the strength of
TCM’s Five Elements theory resides in their assisting and controlling relationships,
while Ayurveda’s five elements are quite static and the subtle energies that govern all
life are better represented by the Tridosha theory.
The three doshas (Vatta, Pitta, Kapha) are present in all living beings and their relative
strength to each other determines the individual’s constitution. They need to be in
balance for health; any imbalance in one dosha will cause disharmony between the
other two and will over time cause disease.
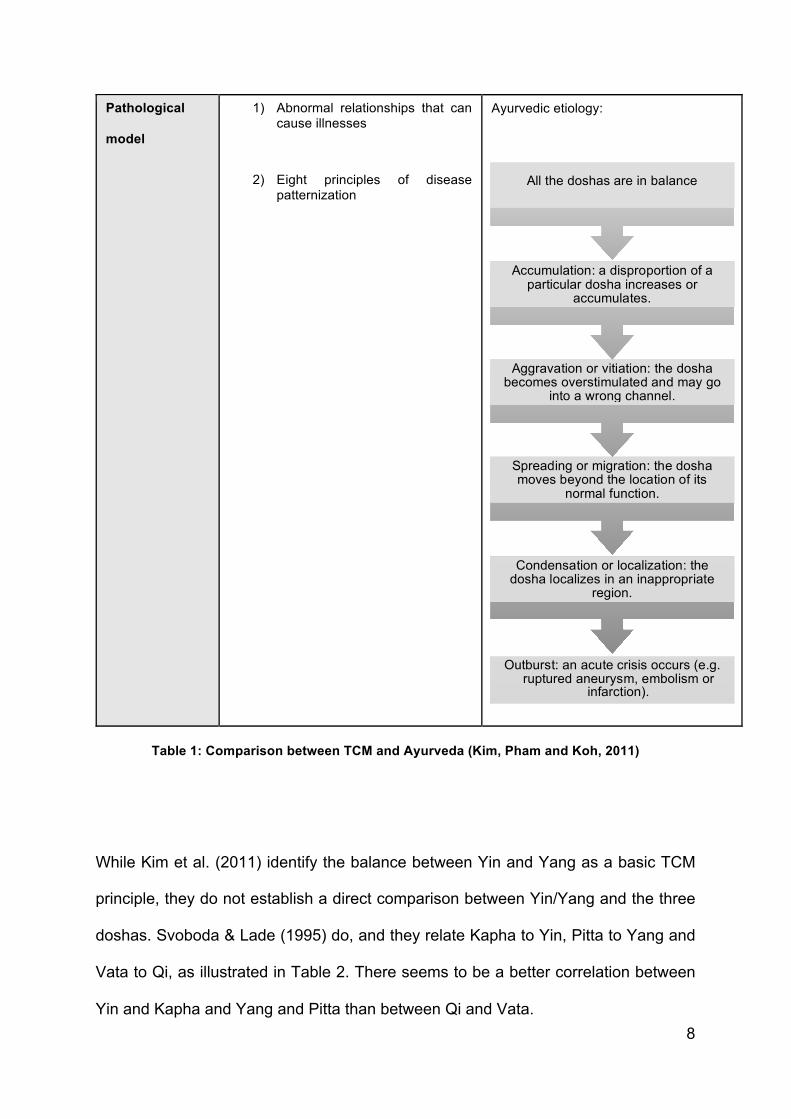
Table 1 represents the physiological equilibrium and pathological model of TCM and
Ayurveda respectively according to Kim et al. (2011). TCM posits abnormal
relationships/balance between Yin and Yang or the Five Elements as the cause of
pathologies that then can be categorized according to different theories (Eight
Principles, Five Elements, Six Divisions, etc.) For Ayurveda, they present a
chronological perspective of disease progression that starts with a disproportionate
accumulation of a specific dosha and as the imbalance increases can ultimately result
in acute crisis (e.g. embolism or infarction).

7
TCM Ayurveda
Philosophical
background
Taoism Vedic philosophy
Approach to
patient
Syndrome-based medicine Constitution-based medicine
Basic principles Ying/Yang theory
Five Elements
Tridoshas
Five Elements
Physiological
equilibrium
model
1) Balance between Yin and Yang (follows the principle of waxing and waning, mutual restraining and mutual nourishing of Ying and Yang)
2) Balance among the Five Elements
Balance among the Tridoshas where all
the doshas are functioning correctly in
appropriate proportions to each other
and in the right positions.
8
Pathological
model
1) Abnormal relationships that can cause illnesses
2) Eight principles of disease patternization
Ayurvedic etiology:
Table 1: Comparison between TCM and Ayurveda (Kim, Pham and Koh, 2011)
While Kim et al. (2011) identify the balance between Yin and Yang as a basic TCM
principle, they do not establish a direct comparison between Yin/Yang and the three
doshas. Svoboda & Lade (1995) do, and they relate Kapha to Yin, Pitta to Yang and
Vata to Qi, as illustrated in Table 2. There seems to be a better correlation between
Yin and Kapha and Yang and Pitta than between Qi and Vata.
Outburst: an acute crisis occurs (e.g. ruptured aneurysm, embolism or
infarction).
Condensation or localization: the dosha localizes in an inappropriate
region.
Spreading or migration: the dosha moves beyond the location of its
normal function.
Aggravation or vitiation: the dosha becomes overstimulated and may go
into a wrong channel.
Accumulation: a disproportion of a particular dosha increases or
accumulates.
All the doshas are in balance

9
Ayurveda Qualities TCM Qualities
Vata Dry, cold, light, unstable,
clear, rough, subtle
Qi Both material and immaterial, can be
translated as energy, ether, matter,
matter-energy, vital force, life force.
Pitta Oily, hot, intense, light,
fluid, malodorous, mobile
Yang Active, brightness, sunshine, fire,
hardness, male, dryness, hot, restless
Kapha Oily, cold, heavy, stable,
viscid, smooth, soft
Yin Passive, darkness, earth, water,
softness, female, moisture, night time,
slowness, cold, docile
Table 2: Doshas vs Qi, Yin and Yang (Svoboda & Lade, 1995)
3. Healingmodalities
3.1HerbalmedicinesinAyurvedaandTCM
TCM and Ayurveda have extensive herbal pharmacopoeias, with 7815 herbal
substances recorded in Zhong Hua Ben Cao , Chinese Materia Medica and
about 7000 species in India’s The National Medicinal Plants Board (Jaiswal, Liang, &
Zhao, 2016). The authors propose comparative investigation of both pharmacopoeias
to gain deeper insights into their respective ancient medical texts, but also to
understand which plants from the other traditional medicine can be substituted in case
of deforestation or environmental disaster.

10
While in both systems different plants can be used for the same therapeutic purposes6,
there are several species commonly used in TCM and Ayurveda for different aims.
One example is turmeric whose stem is said to break up blood stasis, promote the
flow of Qi, stimulate menstruation, and relieve pain as per TCM but Ayurveda uses the
whole plant for respiratory diseases, rheumatism, inflammation, menstrual problems,
cold, cough, and skin allergies7.
Jaiswal, Liang, Ho, Chen, & Zhao (2014) performed a comparative tissue-specific
metabolite analysis and determination of protodioscin content in Asparagus species
used in TCM and Ayurveda and concluded that the differences in their quality are
based upon their protodioscin content, and these species can be used as a substitute
for each other for similar therapeutic benefits in TCM and Ayurveda.
3.2Acupunctureandyoga
Sharma, Hankey, Meenakshy, Nagendra, & Nagilla (2014) describe the increase of
prana as the mechanism by which yoga practices increase wellbeing. They ran a study
that measured the changes in electrodermal resistance at the Jing Well points of the
body brought by yoga practices including yoga asana (postures), vegetarian diet and
meditation practices. Sharma et al. (2014) claim that this electrodermal resistance can
6 For example, Amomum kravanh in TCM and Amomum tsaoko in Ayurveda are used to improve
digestion.
7 One could argue a correspondence between these, for example Ayurveda’s inflammation might
relate to Blood stasis or Qi stagnation in TCM.

11
be used as a measure of qi and by extension, of prana. Their study on a small group
of 33 participants showed a “decrease in meridian bioimpedance corresponding to
increased meridian energy levels” suggesting that yoga practices increase prana
levels in the body.
3.2.1FurthercommentaryonQi/Pranameasurements
As mentioned in 2.1QiandPrana, there are criticisms of the use of electrical devices
to detect and monitor acupuncture points. Bioimpedance measures exogenic current
when an external electric source is applied to a biologic organism. This is different
from bioelectricity, the measure of electrical currents associated with life processes
(Ahn & Martinsen, 2007). While Sharma et al. (2014) took great measures to ensure
consistency of readings in their study by using the same points and following the same
steps in a specific process, there are still complicating factors such as tissue hydration
and the presence of sweat ducts that can adversely impact readings from these
devices.
However, Ahn, Schnyer, Conboy, Laufer, & Wayne (2009) later performed a study on
a small number of participants (n=14) to determine if electrodermal measures at Jing
Well points would be linked to clinical measures in adolescent women with chronic
pelvic pain, and found significant associations between the electrodermal measures
and clinical outcome even after adjusting for treatment designation.

12
3.3Acupunctureandchakras
Greenwood (2006) identifies the lack of literature about chakras in relationship with
acupuncture. Chakras are the energy centres of the subtle body which are located
along the spine (Frawley, Ranade, & Lele, 2005). He highlights a symmetry in the
classification of the seven main chakras into lower, middle and upper where each
group contains specific chakras that reflect the principles of the void (Tao),
individuation (Yang) and connection (Yin). In this comparison, the lower three chakras
reflect these themes in relationship to the personal or individual ego, while the upper
three chakras relate to the transpersonal.
From here, he builds a correspondence between the chakras and their TCM
equivalents in the shape of TCM Five Elements and acupuncture points (see Table 3).
In his view, the journey from the lower three chakras to the ones related to the
transpersonal can be compared to the passage through the Golden Gate described in
TCM (Jarrett, 1994).

13
Sanskrit name English Ayurvedic element
Acupuncture points Chinese element
Muladhara Root Support Earth REN-1, DU-1 Water
Swadhisthana Your own dwelling
or origin
Water REN-4, REN-5, REN-6 Earth
(Water)
Manipura The city of the
shining jewel
Fire REN-12, DU-6, DU-8 Wood
Anahata That which is
never new
Air REN-17, DU-11 Fire
Vishuddha Purification Space REN-22, ST-9 Metal
Ajna Command No element REN-24.5, DU-14 No element
Sahasrara Universal
selfhood
No element REN-20 No element
Table 3: Chakras and their TCM correspondences (Greenwood, 2006)
4. Bioinformatics
The technological advances of the last 20 years, particularly in terms of data
connectivity and storage, have allowed medical research to adapt Google’s mission
statement “organise the world’s information and make it universally accessible and

14
useful” to their own domain. Bioinformatics8 is attracting interest both from research
organization and venture capital (Saviotti, deLooze, Michelland, & Catherine, 2000).
Ikram, Ghani, & Abdullah (2015) highlight medical informatics as the field that
processes medical information such as electronic medical records, clinical decision
support systems, imaging processing systems, telemedicine and many more and set
out to compare the state of the art in several traditional medicines, including TCM and
Ayurveda.
TCM is leading the way, with the use of artificial intelligence such as a Clinical Data
Warehouse to support TCM knowledge discovery, but also databases of specific
chemical protocols and specific gene and disease information to facilitate the
interactional effects of both Western medicine and TCM. They have adopted ISO
Standards to help this aim of integrating these two systems.
The bioinformatics efforts for Ayurveda include assessment help systems for
practitioners, expert systems that provide diet, exercise and prevention practices for
patients, and a government backed system to assimilate and interpret Ayurvedic texts
into a Decision Support System.
8 The use of computer software to understand biological data.
15
Discussion
Direct comparison of TCM vs Ayurveda is not a hugely popular research topic, most
likely because both medical systems are vast and it takes many years of study and
practice to become a proficient practitioner in either one of them. They are also more
commonly part of a treatment plan alongside allopathic medicine, so it makes more
sense for practitioners of TCM to educate themselves in this field instead of Ayurveda,
and vice versa.
Literature on the history and development of both systems with relationship to each
other mostly concentrates on the exchange of ideas between the sixth and tenth
centuries A.D., where the expansion of Buddhism in both China and India favoured a
healthy flow of information in both directions, although scholars from each country tend
to emphasize their own export of knowledge.
A potential research area would be the evolution of TCM and Ayurveda after the tenth
century when their usage was contained within their respective countries, and the
efforts later made to modernize them. The early years (1950s) of the People’s
Republic of China saw a governmental effort to standardize Chinese Medicine
zhongyi, into what is currently known as TCM xueyuanpai, (Hsu, 2008).
Meanwhile, the late 19th and early 20th centuries witnessed a revival of Ayurvedic
medicine through the All India Ayurvedic Congress (A.I.A.C.) in 1907, a professional
interest group of Ayurvedic practitioners, also influenced by British Orientalism9. It
would be interesting to compare how these two different groups (government vs
practitioners) worked towards standardization of their respective medical system.
TCM and Ayurveda are considered “energy medicine” in that both posit the existence
of a life force (Qi/Prana), whose disruption will lead to illness, and both systems
9 “a set of ideas and practices inaugurated under Warren Hastings, Governor-General of Bengal from
1773 to 1785 that sought to know and understand the languages and culture of India as a key step
toward good governance.” (Hsu, 2008)
16
categorize the body’s functions according to a theory of five elements, but while TCM’s
five elements are dynamic and their interrelationships are central to health or absence
of it, Ayurveda’s focus is on the Tridosha model. Some efforts have been made to
compare TCM’s Five elements and Tridosha. Further research into this area might
inform their respective uses of herbal medicines and possibly the creation of a
compendium of commonalities. It would also be interesting to research why Ayurveda
doesn’t have a similar concept to TCM’s Yin/Yang, particularly since it also works in
several continuums of hot/cold, light/dark, slow/fast…
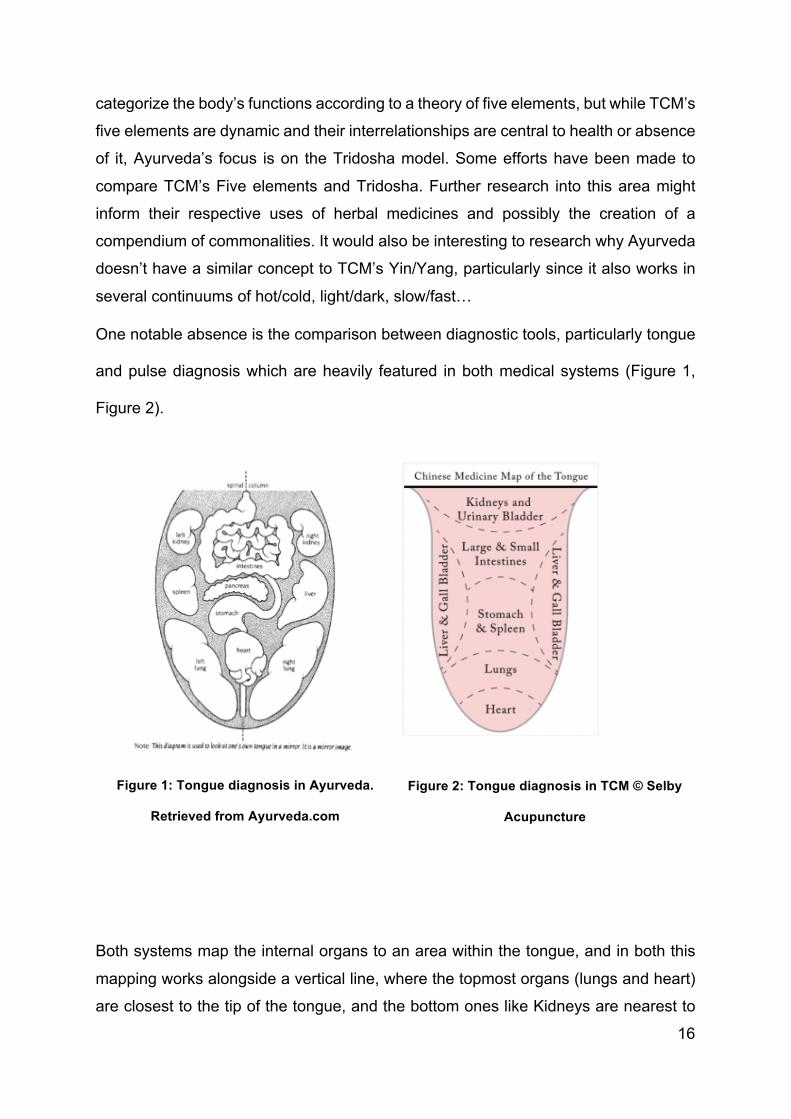
One notable absence is the comparison between diagnostic tools, particularly tongue
and pulse diagnosis which are heavily featured in both medical systems (Figure 1,
Figure 2).
Figure 1: Tongue diagnosis in Ayurveda.
Retrieved from Ayurveda.com
Figure 2: Tongue diagnosis in TCM © Selby
Acupuncture
Both systems map the internal organs to an area within the tongue, and in both this
mapping works alongside a vertical line, where the topmost organs (lungs and heart)
are closest to the tip of the tongue, and the bottom ones like Kidneys are nearest to

17
the root. There are some differences, for example TCM places the diagnostic area of
the heart at the tip while Ayurveda maps it further up, surrounded by the lungs.
The other pillar of diagnosis in both systems is pulse reading, which is very
sophisticated in both and can take practitioners many years to master.
Both TCM and Ayurveda observe four basic characteristics of the pulse that can be
detected on both wrists and all positions and depths: speed, strength, regularity and
depth. Ayurveda also measures temperature and the consistency of the vessel wall
(rough/elastic/thickened).
They also assign organ correspondences to the three pulse positions (cun, guan, chi)
and two depths. Ayurveda distinguishes seven levels of depth and the organ
correspondences sit in the first and seventh level. Table 4 illustrates the comparison.
There is a close correlation in both systems except for the pulses for Stomach/Spleen
and Gallbladder/Liver, which TCM places on the right wrist and Ayurveda on the left.

18
Position TCM Ayurveda
Right distal
Large Intestine
Lungs
Large Intestine
Lungs
Right middle Stomach
Spleen
Gallbladder
Liver
Right proximal Triple Burner
Pericardium
Pericardium
Circulation
Left distal Small Intestine
Heart
Small Intestine
Heart
Left middle Gallbladder
Liver
Stomach
Spleen
Left proximal Kidneys Bladder
Kidney
Table 4: Organ pulses comparison TCM vs Ayurveda (Flaws, 2012; Lad, 2006).
Research into therapeutic modalities in TCM and Ayurveda in relationship to each
other is inconsistent. Efforts are being made in herbal medicine, assisted by
technological advances and partly motivated by environmental concerns and
globalisation. But while herbal medicine is a substantial part of TCM and Ayurveda,
there are other prominent therapies who seem to have a counterpart in the opposite
system:
19
• Tui Na vs Ayurvedic massage
• Acupuncture vs marma points
• Tai Chi/Qi Gong vs yoga
These might be potential areas for future research.
On evaluation of the literature found on the comparisons between TCM and Ayurveda,
one could think that this is a purely academic interest without real world application for
the practitioner of either system who is not a scholar or a pharmaceutical corporation
trying to commercialize compounds found in traditional herbal medicine. But with the
advent of globalisation and the increased interest outside China or India in their
traditional medical systems, it is not rare for a patient to combine treatments from both
and allopathic medicine, for example someone could be seeing an Ayurvedic
practitioner for help with digestive issues with the aim to discontinue the use of
antacids, and at the same time see an acupuncturist for lower back pain. Therefore,
an understanding of the basics of Ayurveda as a TCM practitioner and vice versa
would add value to a practitioner of either, helping them understand their diagnosis or
being able to consult with the practitioner of the opposite system.
20
Conclusion
TCM and Ayurveda are the most globalised systems of traditional medicine still in
practice. They are both patient centric and centered on the body’s energy and its
composition as a reflection of the wider Universe. TCM calls this energy Qi and
Ayurveda Prana, which relates to the functional aspects of life in terms of Five
Elements (TCM) and Three Doshas (Ayurveda). In addition, TCM relies heavily on its
concept of Yin and Yang, for which there doesn’t seem to be an Ayurvedic equivalent.
Herbal medicine is a foundational therapy in both systems and the interest in its
similarities and differences is currently experiencing a resurgence, aided by data
storage and artificial intelligence technology.
Another area of current research is the attempt to measure Qi/Prana, possibly with the
intention to legitimize these medical systems in the eyes of allopathic medicine and
continue their worldwide expansion.
Research into comparative massage, movement therapies and acupuncture/marma
points has been limited so far and could yield further insights into how these
therapeutical modalities assist with the flow of Qi/Prana or the balance of the Five
Elements and Three Doshas.
Given the global trend of increased interest in both medical systems due to their
perception as gentler forms of medicine that can assist with complex conditions that
allopathic medicine does not have a full answer to, it could be of benefit to practitioners
of TCM and Ayurveda to understand the basics of the opposite system and how they
compare to each other.
21
References
Acupuncture - definition (n.d.). Retrieved February 3, 2019, from
https://www.evidencebasedacupuncture.org/acupuncture/acupuncture-definition/
Ahn, A. C., & Martinsen, Ø G. (2007). Electrical Characterization of Acupuncture
Points: Technical Issues and Challenges. The Journal of Alternative and
Complementary Medicine, 13(8), 817-824. doi:10.1089/acm.2007.7193
Ahn, A. C., Schnyer, R., Conboy, L., Laufer, M. R., & Wayne, P. M. (2009).
Electrodermal Measures of Jing-Well Points and Their Clinical Relevance in
Endometriosis-Related Chronic Pelvic Pain. The Journal of Alternative and
Complementary Medicine, 15(12), 1293-1305. doi:10.1089/acm.2008.0597
Bauer, M., LAc. (2006, February 01). The Role of Taoist Spirituality in Chinese
Medicine, Part One: The Gate of All Wonders. Acupuncture Today. Retrieved
February 28, 2019, from
https://www.acupuncturetoday.com/mpacms/at/article.php?id=30308
Deshpande, V. J. (2008). Glimpses of Ayurveda in medieval Chinese medicine.
Indian Journal of History of Science, 43(2), 137-161.
Flaws, B. (2012). The secret of Chinese pulse diagnosis. Boulder, CO: Blue Poppy
Press.
Frawley, D. (2003). Ayurvedic healing: A comprehensive guide. Delhi: Motilal
Banarsidass.
Frawley, D., Ranade, S., & Lele, A. (2005). Ayurveda & marma therapy: Energy
Points in Yogic Healing:. Delhi: Chaukhamba Sanskrit Pratishthan.
Greenwood, M., MB (MD). (2006). Acupuncture And The Chakras. Medical
Acupuncture, 17(3), 27-32.
Harper, D. J. (1998). Early Chinese medical literature: The Mawangdui medical
manuscripts. London: Kegan Paul International.

22
Hinrichs, T. (2001). Early Chinese Medical Literature: The Mawangdui Medical
Manuscripts (review). Bulletin of the History of Medicine 75(1), 121-123. Johns
Hopkins University Press. Retrieved February 26, 2019, from Project MUSE
database.
Hsu, E. (2008). The History of Chinese Medicine in the Peoples Republic of China
and its Globalization. East Asian Science, Technology and Society, 2(4), 465-484.
doi:10.1215/s12280-009-9072-y
Ikram, R. R., Ghani, M. K., & Abdullah, N. (2015). An analysis of application of health
informatics in Traditional Medicine: A review of four Traditional Medicine Systems.
International Journal of Medical Informatics, 84(11), 988-996.
doi:10.1016/j.ijmedinf.2015.05.007
Jaiswal, Y., Liang, Z., Ho, A., Chen, H., & Zhao, Z. (2014). A Comparative Tissue-
specific Metabolite Analysis and Determination of Protodioscin Content in Asparagus
Species used in Traditional Chinese Medicine and Ayurveda by use of Laser
Microdissection, UHPLC-QTOF/MS and LC-MS/MS. Phytochemical Analysis, 25(6),
514-528. doi:10.1002/pca.2522
Jaiswal, Y., Liang, Z., & Zhao, Z. (2016). Botanical drugs in Ayurveda and Traditional
Chinese Medicine. Journal of Ethnopharmacology, 194, 245-259.
doi:10.1016/j.jep.2016.06.052
Jarrett, L. S. (1994). The Loss and Return of Original Nature: The Law of
Husband/Wife. American Journal of Acupuncture, 22(1).
Kim, J. Y., Pham, D. D., & Koh, B. H. (2011). Comparison of Sasang Constitutional
Medicine, Traditional Chinese Medicine and Ayurveda. Evidence-Based
Complementary and Alternative Medicine, 2011, 1-6. doi:10.1093/ecam/neq052
Koh, T. C. (1981). Chinese medicine and martial arts. The American Journal of
Chinese Medicine, 9(3), pp. 181-6. Retrieved February 3, 2019, from
https://wwww.unboundmedicine.com/medline/citation/6764088/Chinese_medicine_a
nd_martial_arts_

23
Lad, V. (2006). Secrets of the pulse: The ancient art of ayurvedic pulse diagnosis.
Albuquerque, NM: Ayurvedic Press.
Lakshmi-chandra, M., BIMS, PhD, Singh, B. B., PhD, & Dagenais, S., DC. (2001).
Ayurveda: A historical perspective and principles of the traditional healthcare system
in India. Alternative Therapies in Health and Medicine, 7(2), 36-42.
Lele, A., Frawley, D., & Ranade, S. (1999). Secrets of marma: The lost secrets of
Ayurveda: A comprehensive text book of ayurvedic vital points. Delhi: Chaukhamba
Sanskrit Pratishthan.
Materia Medica Editorial Committee (1999). Materia Medica of China. Shanghai:
Shanghai Science and Technology Publishing House
Narayanan, C., Korotkov, K., & Srinivasan, T. (2018). Bioenergy and its implication
for yoga therapy. International Journal of Yoga, 11(2), 157.
doi:10.4103/ijoy.ijoy_54_17
Patwardhan, B., Warude, D., Pushpangadan, P., & Bhatt, N. (2005). Ayurveda and
Traditional Chinese Medicine: A Comparative Overview. Evidence-based
Complementary and Alternative Medicine, 2(4), 465-473. doi:10.1093/ecam/neh140
Prasad, S. (2017). Marma Therapy in Katigraha W.S.R. Low Back Pain. Journal of
Medical Science And Clinical Research, 05(06), 23070-23074.
doi:10.18535/jmscr/v5i6.45
Reich, W. (1953). History of the discovery of the life energy. [Place of publication not
identified]: Orgone Institute.
Rosch, P. J. (2009). Bioelectromagnetic and Subtle Energy Medicine. Annals of the
New York Academy of Sciences, 1172(1), 297-311. doi:10.1111/j.1749-
6632.2009.04535.x
Saviotti, P. P., DeLooze, M., Michelland, S., & Catherine, D. (2000). The changing
marketplace of bioinformatics. Nature. doi:https://doi-
org.ezp.lib.cam.ac.uk/10.1038/82351
24
Sharma, B., Hankey, A., Meenakshy, K., Nagendra, H., & Nagilla, N. (2014). Can
yoga practices benefit health by improving organism regulation? Evidence from
electrodermal measures of acupuncture meridians. International Journal of Yoga,
7(1), 32. doi:10.4103/0973-6131.123477
Svoboda, R., & Lade, A. (1995). Tao and dharma: Chinese medicine and Ayurveda.
Twin Lakes, WI: Lotus Press.
Takakusu, J., & Watanabe, K. (Eds.). (1968). The Taisho Shinshu Daizokyo. Tokyo:
Society for the publication of the Taisho Tripitaka, TT.1324.
The Economic Times (2018, November 23). 77 percent Indian households use
Ayurvedic products: PwC report. Retrieved March 16, 2019, from
https://economictimes.indiatimes.com/industry/healthcare/biotech/healthcare/77-
percent-indian-households-use-ayurvedic-products-pwc-
report/articleshow/66773295.cms
Turner, C. (2011). Adventures in the orgasmatron: Wilhelm Reich and the invention
of sex. [Place of publication not identified]: HarperPress.
Turner, C. (2011, July 08). Wilhelm Reich: The man who invented free love.
Retrieved April 17, 2019, from
https://www.theguardian.com/books/2011/jul/08/wilhelm-reich-free-love-orgasmatron
Unschuld, P. U., Tessenow, H., & Zheng, J. (2011). Huang di nei jing su wen: an
annotated translation of Huang Dis Inner Classic -- Basic Questions. Berkeley:
University of California Press.
Wilhelm Reich. (2019, March 25). Retrieved from
https://en.wikipedia.org/wiki/Wilhelm_Reich#Orgonomy
World Health Organization (2002). Traditional medicine strategy 2002-2005.
Geneva.

25
Appendix A
Figure 3: Orgone accumulator van in North London. Photo by Mark Singleton.