strategy management of risks associated with infection prevention
TRANSCRIPT

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 1 of 26
Strategy
Management of risks associated with infection prevention and control (IPC)
1 Scope
Trust-wide: This document summarises the entire portfolio of infection control measures used by Cambridge University Hospitals NHS Foundation Trust to manage the various risks associated with infection prevention and control.
2 Purpose
To describe the management structures, standards, policies and procedures supporting the prevention and control of infection at Cambridge University Hospitals NHS Foundation Trust.
3 Abbreviations used
CoIC Control of Infection Committee CQC Care Quality Commission DH Department of Health HCAI healthcare associated infections ICT Infection Control Team IPC infection prevention and control MRSA methicillin-resistant Staphylococcus aureus RCA root cause analysis
4 Introduction
The Strategy is approved by Addenbrooke’s Control of Infection Committee and compliance is monitored by the Cambridge University Hospitals NHS Foundation Trust Board of Directors and the Trust’s clinical governance structures. The strategy is based on the criteria contained within The Health and Social Care Act 2008 and the Code of Practice for health and adult social care on the prevention and control of infections and related guidance (DH 16 Dec 2009) and draws on previous and current advice from the Department of Health including:
• Getting Ahead of the Curve • Winning Ways: working together to reduce healthcare associated
infection in England • Towards Cleaner Hospitals and Lower Rates of Infection: a summary
of action
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 2 of 26
• Saving Lives: a delivery programme to reduce healthcare associated infection including MRSA
• Essential Steps to Safe Clean Care: Reducing Healthcare Associated Infection.
• Care Quality Commission (December 2009) Cooperation with Other Providers.
The day-to-day business of infection control is carried out by the Infection Control Team (ICT). The ICT implements a comprehensive annual programme of work covering all the main areas of risk. The content of the annual programme is based on the standards set in the Saving Lives, supported by corporate and local assessments of risk based on surveillance and audit activity. The main business of the ICT is to produce and implement the infection control annual priorities and audit programme and to resolve current infection control problems in the Trust by appropriate action or issue of advice. The team is also responsible for reviewing and implementing the national HCAI strategy and DH policy and initiatives.
5 How this document is structured
The strategy comprises ten criteria taken from the Health and Social Care Act (2008).
Criteria
1 Systems to manage and monitor the prevention and control of infection. These systems use risk assessments and consider how susceptible service users are and any risks that their environment and other users may pose to them.
2 Provide and maintain a clean and appropriate environment in managed premises that facilitates the prevention and control of infections.
3 Provide suitable accurate information on infections to service users and their visitors.
4 Provide suitable accurate information on infections to any person concerned with providing further support or nursing/ medical care in a timely fashion.
5 Ensure that people who have or develop an infection are identified promptly and receive the appropriate treatment and care to reduce the risk of passing on the infection to other people.
6 Ensure that all staff and those employed to provide care in all settings are fully involved in the process of preventing and controlling infection.
7 Provide or secure adequate isolation facilities.
8 Secure adequate access to laboratory support as appropriate.
9 Have and adhere to policies, designed for the individual’s care and provider organisations, that will help to prevent and control infections.
10 Ensure, so far as is reasonably practicable, that care workers are free of and are protected from exposure to infections that can be caught at work and that all staff are suitably educated in the prevention and control of infection associated with the provision of health and social care.
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 3 of 26
The content of this document is informed by a self assessment of compliance with the Code of Practice that has been undertaken using the saving lives balanced scorecard; the self assessment is reviewed quarterly. Cambridge University Hospitals NHS Foundation Trust has registered as fully compliant with the Code of Practice for the purposes of Care Quality Commission HCAI registration.
6 Management, organisation and environment
6.1 Criterion 1: Systems to manage and monitor the prevention and control of infection
These systems use risk assessments and consider how susceptible service users are and any risks that their environment and other users may pose to them. This criterion links with Outcome 6, Regulation 24 cooperating with other providers in the CQC guidance about compliance. Cambridge University Hospitals NHS Foundation Trust has in place:
• A Board level agreement outlining the Board’s collective responsibility for minimising risks of infection and how this is to be achieved.
• A director of infection prevention and control (DIPC) accountable to the chief executive and the Board.
• Mechanisms in place by which the Board ensures sufficient resources are available to secure effective prevention and control of HCAI.
• Measures to ensure that relevant staff, contractors and other persons directly or indirectly concerned with patient care receive suitable and sufficient information, training and supervision in measures required to prevent or minimise HCAI.
• A programme of audit to ensure key policies and practices are being implemented appropriately.
• A policy addressing patient movement between departments, within and between healthcare establishments.
• A designated decontamination lead.
• A designated antibiotic pharmacist and a microbiologist with an antibiotic role.
6.1.1 Risk assessment
The Trust has in place suitable and sufficient assessment of risks to patients receiving healthcare with respect of HCAI. The Trust monitors risks of infection through data collection, audit and review of clinical incident reporting. These findings and a review of current risk assessments are reported to the Control of Infection Committee (CoIC) and the findings are used to inform future actions.
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 4 of 26
Corporate and local HCAI risk assessments are available on the Trust’s Risk Register. The risk rating report for high risks is reviewed on a quarterly basis by the Quality and Risk Committee. Existing control measures and further preventative measures are identified for action. The Trust has a robust incident reporting system through which staff can report adverse incidents such as deviation from a clinical guideline or poor practice that may be detrimental to patient care. A report is submitted every two months detailing infection control incidents and complaints from patients/ visitors. These are reviewed by the ICT and CoIC and common themes identified for action. Each MRSA bacteraemia is subject to a root cause analysis (RCA) and is reported via the incident reporting system. An RCA meeting is held fortnightly within the Trust which is attended by:
• clinicians • members of the infection control team • the PCT lead infection control nurse.
Actions are identified and disseminated at relevant meetings throughout the organisation including reporting to TEF (The Executive Forum) and CoIC. Each MRSA RCA is provided to the Primary Care Trust DIPC via nhs.net. Any deaths occurring as a result of an MRSA bacteraemia are reported as a serious untoward incident. Every patient diagnosed with Clostridium difficile associated diarrhoea is reviewed by an infection control nurse at least daily. The infection control nurses (ICN) assist in the correct placement of the patient. Where possible all cases are placed in the designated isolation ward or are placed in a side room. Staff are supported in their decision making processes by the risk assessment tool for prioritisation of patients who require isolation. Each case has an RCA completed, which includes:
• a review of predisposing antibiotic therapy • the use of proton pump inhibitors • current antibiotic treatment • other predisposing variables.
All cases of C. difficile which result in death, colectomy, or are the result of a cluster/ outbreak are reported as serious untoward incidents. A meeting is held monthly to discuss these cases; learning and action points are disseminated. Daily minuted meetings (Monday to Friday) are held to discuss the management of C. difficile patients and other current infection control issues eg norovirus. These are held in conjunction with Operations Centre staff, Estates and Facilities staff, on-call managers and the ICNs.
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 5 of 26
6.1.2 Infection control management, including the role of the DIPC
The ICT comprises medical and nursing infection control professionals who are responsible for the day-to-day operation of the infection control service including:
• surveillance and mandatory reporting • the provision of policies • a programme of audit to ensure that key policies and practices are
implemented appropriately • provision of advice to clinical and management colleagues including:
o monitoring of infection risks o ongoing staff education and training o appropriate advice in response to major outbreaks of
communicable infections. The infection control nurses have designated areas of responsibility across the organisation and members of the ICT provide a 24 hour on-call service for provision of infection control advice to clinical and management colleagues. The ICT reports to the CoIC and is directly accountable via the infection control doctor and the deputy chief nurse to the DIPC. The DIPC is responsible for leading the Trust’s Infection Control Team and reports directly to the Chief Executive and the Board of Directors (DIPC responsibilities – see appendix 1). The infection control doctor is responsible for day to day management of infection control and liaises closely with the DIPC as required (ICD responsibilities – see appendix 2). The infection control team (ICT) consists of:
• director infection prevention and control • associate medical director for HCAI • non-executive director (infection prevention and control) • consultant microbiologist x5 • consultant virologist x3 • deputy chief nurse • infection control lead nurse • infection control clinical nurse specialist x2 • infection control nurse x2 • surgical site infection surveillance nurses x2 • audit and surveillance nurse • information analyst • clerical assistant.
The CoIC meets every two months. Membership comprises:
• representatives from the ICT • nominated infection control leads from all clinical directorates • representatives from other relevant groups within the Trust.
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 6 of 26
Table 1: CoIC membership • consultant in infectious diseases (chairman) • medical director and director of infection prevention and control (vice chair) • associate medical director HCAI • non-executive director (infection prevention and control) • deputy chief nurse • consultant microbiologist and infection control doctor • infection control lead nurse • consultant in communicable disease control, Cambridgeshire & Peterborough Health
Protection Unit • head of risk and patient safety • sterile services manager • chief pharmacist and decontamination lead • operations managers • consultant in neonatal intensive care (HCAI) • sister neonatal ICU, Rosie Maternity Hospital • consultant in occupational health • theatre manager • estates and facilities manager • consultant virologist • D10 ward manager (Infectious Diseases Unit) • senior clinical nurse, Emergency Admissions Unit • consultant orthopaedic surgeon (HCAI) • senior clinical nurse, surgical services • communications officer.
The CoIC reports to the Quality and Risk Committee and is responsible for supervising the delivery of the annual infection control priorities and audit programme and the infection control annual report, as well as identifying risks relating to infection control via review of risk assessments, incident reports and complaints. Cambridge University Hospitals NHS Foundation Trust has devolved accountability for HCAI to divisional level via the divisional directors and heads of nursing and through nominated infection control leads in each clinical department. The clinical department leads have responsibility for implementing specific infection control practices and achieving key performance targets for their directorates. The infection control leads are responsible for implementing and monitoring infection control policies in their clinical areas with support as required from members of the ICT. Infection control consultant leads report to their divisional directors within the divisional clinical governance framework. The senior clinical nurses and clinical service managers have day to day responsibility and accountability for infection control and delivering a safe and clean care environment. The SCNs/ CSMs report directly to their operations managers. See appendix 3 and appendix 4 for identified roles and responsibilities. The key working structures for infection control are summarised in appendix 5.
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 7 of 26
6.1.3 Assurance framework
Infection control is an integral part of the clinical and corporate governance framework. Infection control is recorded as a risk to patient safety in the Trust’s board assurance framework. This framework identifies the key control measures in place and the means by which the Board of Directors is assured that those controls are operating and the risk is being managed. The main source of board assurance identified in the framework is the monthly performance report to the board showing current infection levels and reporting on actions, initiatives and audits of compliance. The DIPC reports regularly to the Board of Directors on performance against target; key issues and actions relating to MRSA blood stream infections, Clostridium difficile and other infection issues when relevant. The Infection Control Annual Report is produced by the consultant microbiologist and the DIPC for presentation to the Board of Directors and is a public document. This provides an important opportunity for the ICT to highlight any concerns about the resources needed to manage infection related risks in the coming year and for the Board of Directors to explore any concerns they may have about the management of infection control. The monthly infection control reports are available to all Trust staff via Connect and business intelligence tool (QlikView) and are disseminated to key networks following reporting at TEF. The Trust via the deputy chief nurse or infection control lead nurse reports to the PCT monthly or more frequently if required on the incidence of MRSA bacteraemia, Clostridium difficile and any declared outbreaks eg norovirus. The Trust, via the deputy chief nurse, infection control doctor and lead nurse reports to the SHA (Strategic Health Authority) monthly on MRSA bacteraemias and Clostridium difficile and, where there is non-compliance with monthly agreed targets as per the agreed contract, the Trust also reports to Monitor monthly. Divisional directors can raise any concerns relating to infection control issues via The Executive Forum which is attended by members of the Board of Directors and divisional directors. Divisional lead nurses and modern matrons can raise any concerns relating to infection control issues via representation on the Control of Infection Committee and also through the deputy chief nurse to the Board of Directors.
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 8 of 26
6.2 Criterion 2: Provide and maintain a clean and appropriate environment in managed premises that facilitates the prevention and control of infections
This criterion links with Outcome 10, Regulation 15 safety and suitability of premises contained in CQC guidance about compliance. The ICT, in collaboration with the Estates and Facilities Team and the decontamination lead, monitors standards of cleanliness within the Trust and promotes best practice by ensuring the following.
• The Trust has a cleaning strategy developed by the Estates and Facilities Team in collaboration with the ICT and approved by the Control of Infection Committee.
• The provision of policies for
o the maintenance of the environment o provision of cleaning services o linen, laundry and dress o decontamination.
• Staff are suitably trained and hold adequate competencies for their roles.
• There are designated managers for the cleaning of the environment
and the cleaning and decontamination of equipment. • Lead nurses are included in all aspects of cleaning services, including
contract negotiations and service delivery at ward level. • Senior clinical nurses have personal responsibility for delivering a safe
and clean environment. The nurse in charge of any patient area has direct responsibility for ensuring that cleanliness standards are maintained throughout the shift, including use of appropriate escalation procedures where necessary.
• Ensuring, through audit and ward visits that all parts of the premises
are suitable for the purpose, kept clean and maintained in good physical repair and condition. The audit results are fed back to the wards and incorporated into the nursing quality metric report which provides information monthly by ward and division.
• Patient Environmental Audit Team (PEAT) visits are undertaken and
the findings and recommendations are actioned. • The cleaning arrangements detail the standards of cleanliness
required in each part of the premises and that cleaning schedules and frequencies are publicly available.
• There is adequate provision of suitable handwashing facilities and
antibacterial hand rubs, including risk assessments of placement of alcohol hand gels.
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 9 of 26
• Correct procedures are in place for the delivery of food services,
including food hygiene and food brought into the organisation by patients, staff and visitors.
• Advising on waste disposal. All waste is treated as hazardous
therefore there is no need for segregation. There is a clinical waste incineration facility on site with an associated ‘energy from waste’ heat recovery system. This facility is compliant with the EA permitted waste incineration directive.
• There is a programme of planned, preventative maintenance,
including pest control and the management of potable and non-potable water supplies.
• Advising on the audit of the Trust professional dress code and uniform
policy, which is undertaken on an annual basis. The policy states that uniforms are expected to be clean and fit for purpose and includes the ‘bare below the elbow’ guidance (DH, 2007).
• Ensuring the supply and provision of linen and laundry including
uniforms which reflects health service guidance HSG(95)18 hospital laundry arrangements for used and infected linen.
• Ensuring the Trust has effective arrangements for the appropriate
decontamination of instruments and other equipment. The Trust is fully compliant with HBN/13 and has registration under MDD93/42/EEC.
• There is a designated decontamination lead with responsibility for
ensuring that the decontamination policy is implemented in relation to the organisation and takes account of national guidance.
• Appropriate procedures are followed for acquisition and maintenance
of decontamination equipment. • A monitoring system is in place to ensure decontamination processes
are fit for purpose and meet required standards: o risk assessment o weekly water testing and feedback of results o machine checks o maintenance with available records.
• A monitoring system is in place to ensure safe and adequate
equipment cleaning in line with High Impact Intervention No. 8 Decontamination of Equipment.
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 10 of 26
6.3 Criterion 3: Provide suitable accurate information on infections to service users and their visitors.
This criterion links with Outcome 1, Regulation 17 Reporting and involving services users contained in CQC guidance about compliance.
Local statistics on the rate of HCAI for key organisms including MRSA and Clostridium difficile are included in the infection control annual report. The annual report also contains information on the incidence of infections in orthopaedic joint replacements and voluntary surveillance of surgical site infection rates for selected categories of interventions.
Patients experiencing HCAI caused by MRSA, Clostridium difficile and other significant organisms receive an information leaflet which contains information about the organism and explains any precautions required both in the hospital and in the community post discharge. Information is also available for visitors. Specific patient, staff and public information is regularly posted on the public website, including:
• the latest incidence rates for MRSA and Clostridium difficile • information on specific organisms or infection risks eg Norovirus,
influenza. These include information for patients, relatives and visitors on reporting areas of concern. General information on the Trust’s HCAI performance is available via the publication of the Board of Governor minutes. Infection control advice leaflets are available in various languages for patients, visitors and health care workers. Infection control information on MRSA and C. difficile are an obligatory field on electronic medical records and discharge/ transfer documentation.
6.4 Criterion 4: Provide suitable accurate information on infections to any person concerned with providing further support or nursing/medical care in a timely fashion.
This criterion links with Outcome 6, Regulation 14 cooperating with other providers contained in CQC guidance about compliance. The movement of patients within the Trust is included in key policy documents such as the admission and discharge policies and the patient transfer policy. The ICT works jointly with bed managers, Operations Centre staff and with Estates and Facilities services in planning patient admissions, transfers, discharges and movements between departments and other healthcare facilities. The Trust uses transfer documentation which communicates the patient’s infection status to the receiving team or PCT provider organisation. Compliance with Trust policies is monitored through complaints and incident reporting as well as audit. Monthly data on bed moves for infection control
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 11 of 26
purposes is included as a key performance indicator in the Trust infection control report. The Trust’s electronic medical record (eMR) and discharge record include infection status as a mandatory field for both MRSA and C. difficile. The Trust has developed in collaboration with the PCT an MRSA care pathway (care of patient with methicillin-resistant staphylococcus aureus); this is a patient held record which is transferred into the community on discharge of the patient. Local Trust infection control policies require information on potential infection hazards to be forwarded to other institutions before patients are transferred out of the Trust. The acute Trust works with the PCT to provide a comprehensive whole health economy approach to the management of HCAI. A review of progress is undertaken quarterly at the Cambridge PCT Strategic Infection Control Committee meeting and at the Clinical Quality Monitoring Group. The Infection Control Team liaises with the Discharge Planning Team and infection control information is included in all documentation. The ICT is part of a region-wide planning and implementation forum for dealing with gastrointestinal infection management.
6.5 Criterion 5: Ensure that people who have or develop an infection are identified promptly and receive the appropriate treatment and care to reduce the risk of passing on the infection to other people
Cambridge University Hospitals NHS Foundation Trust is able to demonstrate that responsibility for infection prevention and control is effectively devolved to all professional groups by means of inclusion in all job descriptions and mandatory inclusion in appraisal documentation including for medical staff. Compliance with mandatory training and completion of appraisal are reported monthly in the corporate balanced scorecard. The Trust is compliant with national MRSA screening guidance, including the screening of all emergency patients. Compliance is audited and reported monthly in the infection control report. Nursing documentation audits are undertaken weekly across all inpatient areas including compliance with the MRSA ICP and C. difficile care record. Point prevalence audits of compliance with antibiotic prescribing are undertaken and reported regularly by the antibiotic pharmacist. The Trust monitors compliance with the appropriate isolation of patients, including time to isolation. This is reported monthly in the infection control report.
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 12 of 26
6.6 Criterion 6: Ensure that all staff and those employed to provide care in all settings are fully involved in the process of preventing and controlling infection
The Trust as far as is reasonably practicable ensures that its staff and contractors and others involved in the provision of healthcare cooperate so far as is necessary to enable the Trust to meet its obligations under the code of practice for the prevention and control of healthcare associated infections. The Trust works across the health economy on infection prevention and control measures, including working with the Health Protection Unit, Health Protection Agency, PCT, SHA and Regional Epidemiology Unit. The Trust has the ability to cohort patients where necessary including in the event of a cluster or outbreak of a specific organism. The decision to classify the incidence of any infectious disease as an outbreak is taken by the Infection Control Team in consultation with the infection control doctor or on duty microbiologist/ virologist. Broadly, an outbreak can be defined as:
• an incident in which two or more people experiencing a similar illness are linked in time/ place
• a greater than expected rate of infection compared with the usual background rate for the place and time where the outbreak has occurred
• a single case for certain rare diseases such as: o diphtheria o botulism o rabies o viral haemorrhagic fever o polio.
Refer to the Trust’s generic outbreak protocol. The Trust has in place infection control training programmes for all staff including external contractors. Training programmes are identified through the use of infection control training needs analysis.
6.7 Criterion 7: Provide or secure adequate isolation facilities
The Trust recognises the need to maintain and expand facilities for patient isolation for infectious purposes, while recognising the need to provide single room facilities for patients requiring privacy for other reasons. To assist staff the Trust has an isolation policy and organism-specific policies detailing the need for isolation. Staff are also assisted in their decision-making through the provision of a risk assessment tool for prioritisation of patients who require isolation. Failure to observe recommended isolation procedures results in the generation of an incident report and if appropriate, emergency control measures as outlined by the Infection Control Team and/or the local consultant in communicable disease control (CCDC).
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 13 of 26
6.8 Criterion 8: Secure adequate access to laboratory support as appropriate
The local Trust Microbiology Department has full CPA (UK) clinical pathology accreditation, which requires the provision of appropriate protocols and standard operating procedures. The microbiology services are provided by the Health Protection Agency (HPA) although the department, which is the HPA Regional Microbiology Laboratory for the East of England, is fully integrated into the Trust. There is provision of seven day laboratory working and 24 hour access to microbiology and virology advice.
7 Clinical care protocols
5.1 Criterion 9: Have and adhere to policies, designed for the individual’s care and provider organisations, that will help to prevent and control infections.
A comprehensive infection control document section is available via the Trust’s document library, which identifies all infections and infectious conditions which require isolation or specific infection control management and describes any specific precautions required. The infection control documents also identify clinical situations where isolation precautions may be required before any infection risk has been confirmed (eg patients with pyrexia of unknown origin from abroad). In the event of a failure of the electronic library a master copy of all infection control policies and procedures is kept in the Operations Centre. The folders are updated regularly and audited six-monthly. The ICT is responsible for the maintenance and updating of the infection control policies, procedures and guidance documents. There are currently a number of infection control documents which are evidence based and reflect national guidance documents. Approval for such documents is via the CoIC and ratification is via the Quality and Risk Committee. The antimicrobial prescribing policy is the joint responsibility of the consultant microbiologist and antibiotic pharmacist and is approved by the Joint Drugs and Therapeutics Committee. The decontamination policies and procedures are the responsibility of the decontamination lead. All infection control polices carry a two yearly review date, or sooner in the light of new evidence. The review schedule is monitored within the annual infection control programme and by the Trust documents administrator.
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 14 of 26
Compliance with key policies is audited according to a schedule included in the annual programme. Infection control documents include the following:
Policies Cleaning and disinfectionHand hygieneDisinfectants and antiseptics Safe disposal of sharp objects Aseptic procedures and use of treatment rooms Isolation (includes standard universal precautions) Clostridium difficile infectionSharps injury and other exposures to blood, including guidance for use of post-exposure prophylaxis (PEP) against blood-borne viruses (BBV)MRSA: Guidelines for the management of methicillin resistant Staphylococcus aureus (MRSA), including screening and decolonisation Safe handling of food for ward kitchensManagement of gastroenteritis outbreaks on hospital wardsCare of patients and staff infected or colonised with Lancefield group A streptococci Care of the infested patientManagement of patients with glycopeptide-resistant enterococci (GRE)care of the patient with a urinary catheter Personal protective equipmentInfection control and management guidelines for patients with mycobacterium tuberculosis (TB)Infectious diseases: Ward N2 and Ward D10 operational policyvenepunctureManagement of multi-drug resistant (MDR) Acinetobacter baumanii (MRAB)cases of chickenpox and zoster (shingles) occurring in hospitalCare of patients with known or suspected Creutzfeldt-Jakob disease (CJD) or variant Creutzfeldt-Jakob disease (vCJD)LegionellaDecontamination of reusable medical devicesSingle use/ limited itemsStaff immunisation and infection screeningIncident reporting and investigationEast of England serious untoward incidents policyWaste Disposal Policy
Procedures Aseptic non touch technique (ANTT) for the administration of intravascular drugs and fluids Incident reporting and investigationCare of infected bodies on general wardsLast offices (adults only)Waste Disposal Procedure
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 15 of 26
Guidelines Antibiotics: A guide to antibiotic therapy in adult patientsGuidelines for the prevention of infection associated with enteral feedingDecontamination of equipment, fixtures and fittings prior to the decommissioning or vacating of wards Prevention of sepsis after splenectomy
Protocols Major incident protocolClosure of wards, departments and premises to new admissions - see specific alert organism policies and the generic outbreak protocol. Packaging, labelling and transport of specimens within the TrustViral haemorrhagic fevers (VHF): management of patients with suspected VHFCollection of clinical specimens
Influenza Pandemic Escalation Plan
Decontamination documents The ICT also collaborates with others such as the Central Venous Access Team in developing guidelines such as the Central venous access devices (CVAD) – criteria for referral to the Vascular Access Team (VAT).
8 Health care workers
8.1 Criterion 10: Ensure, so far as is reasonably practicable, that care workers are free of and are protected from exposure to infections that can be caught at work and that all staff are suitably educated in the prevention and control of infection associated with the provision of health and social care.
This criterion links with: • Outcome 12, Regulation 21 requirements relating to workers • Outcome 11, Regulation 16 safety, availability and suitability of
equipment • Outcome 10, Regulation 15 safety and suitability of premises • Outcome 6, Regulation 14 cooperating with other providers contained
in CQC guidance about compliance. Staff are protected from the risk of infection through a comprehensive portfolio of policies addressing:
• induction training of new staff • annual training of existing staff • occupational health measures.
All staff have access to occupational health advice and out of hours access to medical advice in the event of exposure to a blood borne virus or an alert organism.
Strategy for management of risks associated with IPC Version 6; Approved May 2010
Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 16 of 26
There is a screening and immunisation programme which is in accordance with national guidance, specifically ‘immunisation against infectious diseases’; including pre-employment screening and ongoing health screening for communicable diseases where indicated. The Trust is working towards reducing occupational exposure to blood borne viruses including the prevention of sharps injuries by the purchase of safer sharps products where available including the blood culture sampling system and intravenous cannulae.
8.1.1 Induction, training programmes and ongoing education
• All clinical staff including bank nursing staff are required to participate in induction and mandatory annual infection control training currently provided by the ICT and infection control link nurses. This includes hand hygiene and standard isolation precautions based on national guidelines.
• The Trust has implemented an infection control elearning programme to support the mandatory training programme already in place.
• All new clinical and support staff receive the principles of infection prevention and control training including hand hygiene as part of the induction process. All new staff are provided with a hand hygiene guide.
• Senior and junior medical staff receive detailed infection control training including:
o isolation policy o antimicrobial prescribing o blood culture guidance o management of exposure to blood borne viruses.
• In addition FY1, FY2 and SpRs undergo a practical assessment in the care of patients with infections.
• Infection control training for locum/ agency staff is available in the form of a training pack.
• Clinical directorates are required to include audit of compliance with basic infection control policies as part of clinical governance programme. This is monitored by the ICT.
• Compliance with induction training, mandatory training and appraisal is reported quarterly in the Trust’s operational balanced scorecard and presented to TEF.
• The Infection Control Team and line manager are notified of non-attenders at induction and mandatory training. It is the responsibility of the line manager to ensure that non-attenders are followed up and complete their training.
• Fit testing for RPE (respiratory protective equipment) is undertaken for all staff in high risk areas on induction.
Strategy for management of risks associated with IPC Version 6; Approved May 2010
Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 17 of 26
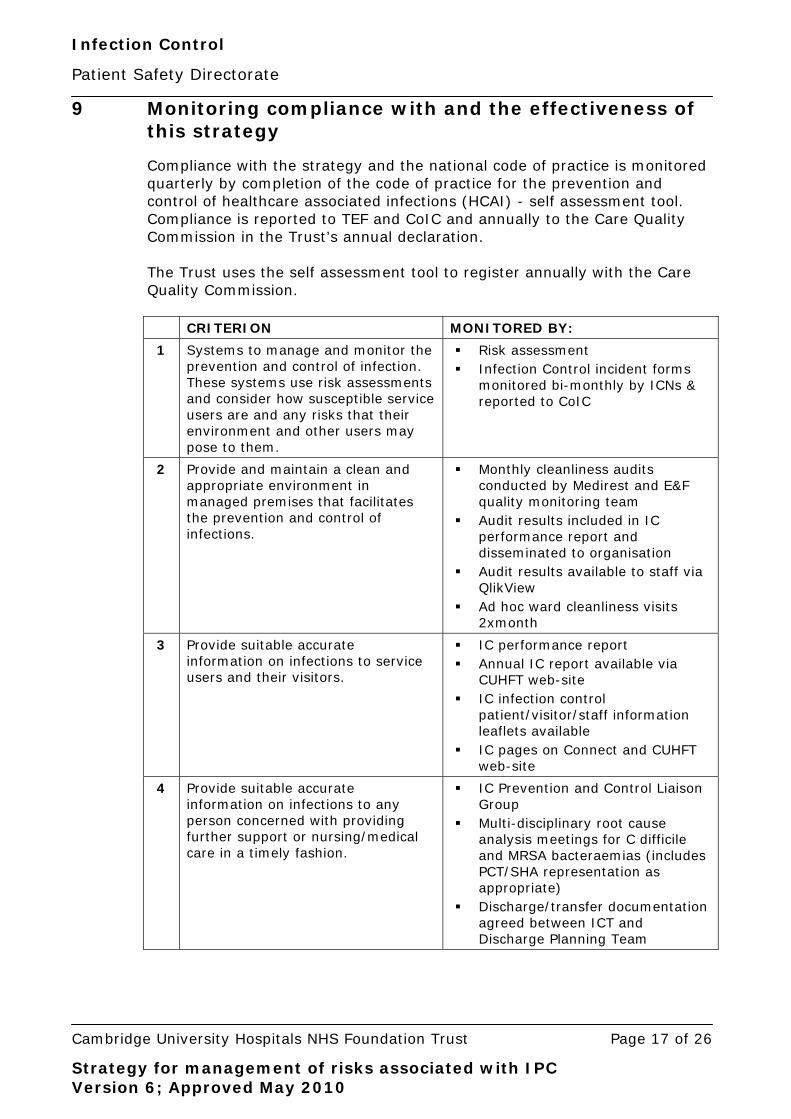
9 Monitoring compliance with and the effectiveness of this strategy
Compliance with the strategy and the national code of practice is monitored quarterly by completion of the code of practice for the prevention and control of healthcare associated infections (HCAI) - self assessment tool. Compliance is reported to TEF and CoIC and annually to the Care Quality Commission in the Trust’s annual declaration. The Trust uses the self assessment tool to register annually with the Care Quality Commission.
CRITERION MONITORED BY:
1 Systems to manage and monitor the prevention and control of infection. These systems use risk assessments and consider how susceptible service users are and any risks that their environment and other users may pose to them.
Risk assessment Infection Control incident forms
monitored bi-monthly by ICNs & reported to CoIC
2 Provide and maintain a clean and appropriate environment in managed premises that facilitates the prevention and control of infections.
Monthly cleanliness audits conducted by Medirest and E&F quality monitoring team
Audit results included in IC performance report and disseminated to organisation
Audit results available to staff via QlikView
Ad hoc ward cleanliness visits 2xmonth
3 Provide suitable accurate information on infections to service users and their visitors.
IC performance report Annual IC report available via
CUHFT web-site IC infection control
patient/visitor/staff information leaflets available
IC pages on Connect and CUHFT web-site
4 Provide suitable accurate information on infections to any person concerned with providing further support or nursing/medical care in a timely fashion.
IC Prevention and Control Liaison Group
Multi-disciplinary root cause analysis meetings for C difficile and MRSA bacteraemias (includes PCT/SHA representation as appropriate)
Discharge/transfer documentation agreed between ICT and Discharge Planning Team
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 18 of 26
CRITERION MONITORED BY:
5 Ensure that people who have or develop an infection are identified promptly and receive the appropriate treatment and care to reduce the risk of passing on the infection to other people.
Alert organism surveillance daily by ICT
IC representation at daily operational meetings
6 Ensure that all staff and those employed to provide care in all settings are fully involved in the process of preventing and controlling infection.
IC mandatory training included in induction and refresher training
IC e-learning package available HCAI competency package for all
clinical staff Medical student and qualified
doctor OSCE assessments undertaken
7 Provide or secure adequate isolation facilities.
IC involvement in new builds and refurbishments
Isolation policy in place with regular audit and feedback
Aspects of isolation included in IC performance report
8 Secure adequate access to laboratory support as appropriate.
Laboratory has HPA Accreditation and undertakes 7-day working
9 Have and adhere to policies, designed for the individual’s care and provider organisations, that will help to prevent and control infections.
Policies and procedures reviewed and updated two-yearly or as required
All policies/procedures available via Connect
Compliance monitored as stated in individual policies
10 Ensure, so far as is reasonably practicable, that care workers are free of and are protected from exposure to infections that can be caught at work and that all staff are suitably educated in the prevention and control of infection associated with the provision of health and social care.
Occupational Health monitoring of staff well-being
Provision of vaccination to staff as appropriate with feedback of uptake
OLM attendance at mandatory IC training is monitored with recall for non-attenders via managers
10 References
Department of Health (2003) Winning Ways Working together to reduce Healthcare Associated Infection in England. Report from the Chief Medical Officer.
The Health and Social Care Act 2008: Code of Practice for health and adult social care on the prevention and control of infections and related guidance. (Dec. 2009)
Care Quality Commission (December 2009) Cooperation with Other Providers.
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 19 of 26
11 Associated documents
• care of patient with methicillin-resistant staphylococcus aureus ICP • generic outbreak protocol • risk assessment tool for prioritisation of patients who require isolation • patient transfer policy • Trust professional dress code and uniform policy
Equality and diversity statement This document complies with the Cambridge University Hospitals NHS Foundation Trust service equality and diversity statement.
Disclaimer It is your responsibility to check against the electronic library that this printed out copy is the most recent issue of this document.
Document management Approval: Control of Infection Committee, 20 May 2010 Owning department: Infection Control Author(s): Angela Thompson, Cheryl Trundle, Nicholas Brown, Ann Alderton, Geraldine
Martell, Helen Howe, Andrew Lever File name: Strategy for management of risks associated with IPC Version 6 May 2010.doc Supersedes: Version 5, July 2009 Version number: 6 Review date: May 2013 Local reference: Media ID: 3506
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 20 of 26
Appendix 1: Director of infection prevention and control responsibilities
• Being responsible for the ICT
• Overseeing the maintenance, development and implementation of the infection
control policies and their implementation
• Being a full member of the ICT, regularly attending infection control meetings
• Reporting directly to the chief executive, Board of Directors and Quality and Risk
Committee on infection control matters
• Ensuring that poor infection control practices in the Trust are identified and
challenged, including clinical hygiene practice and inappropriate antibiotic
prescribing
• Ensuring that the impact of all existing and new policies on HCAI are assessed and
to make recommendations for change
• Being an integral member of the Quality and Risk Committee and having director
responsibility for patient safety
• Producing an annual infection control report which is released publicly.
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 21 of 26
Appendix 2:
Role description: Infection control doctor/ consultant medical microbiologist lead for infection control
General
The infection control doctor is a medical consultant who is expected to provide leadership for and maintain an overview of infection control and act as an infection control specialist within the Trust. The role would normally be performed by a consultant medical microbiologist, with other medical microbiology consultants deputising during periods of absence to ensure that 24 hour cover is provided. The consultant is accountable for this role to the medical director/ DIPC.
Role • to advise and support the DIPC on all aspects of infection control in the hospital
and on implementation of agreed policies • to act as the medical lead for the infection control team and advise and support
the infection control nurses in day-to-day activities • to investigate outbreaks of hospital infection as described in the NHS Executive
(1995) Hospital infection Control: Guidance on the control of Infection in hospitals. Close liaison with the consultant for communicable disease control (CCDC) will be necessary as detailed in this guidance
• to advise and support executive directors, divisional directors, clinical directors, service managers as appropriate about infection control issues
• to serve as a specialist adviser (with colleagues as appropriate) on all matters relating to hospital infection control
• to be an active member of the Trust Control of Infection Committee • to advise and contribute to the planning and implementation of relevant
activities required to achieve the Trust’s aims and objectives, NHS standards and the compliance criteria under the Health and Social Care Act (2008)
• to contribute to the planning, delivery and implementation of standards required to achieve NHSLA to a level appropriate to the Trust
• to prepare and update policies, together with other relevant personnel, in relation to hospital infection control
• to be involved in the planning and upgrading of hospital facilities • to be involved in the setting of quality standards with regard to hospital
infections and in audits of infection • to support and contribute to the training of medical students, medical and
nursing staff and other health care workers of all grades • to liaise with other infection control doctors and CsCDC /consultants in health
protection in developing PCT and SHA-wide infection control programmes
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 22 of 26
Appendix 3:
Role description: Clinical department lead for infection control
General For prevention and control of infection to be effective, infection control activities have to be embedded into everyday practice and applied consistently by everyone. All staff should demonstrate good infection control and hygiene practice. Individual divisions need to have ownership of infection control in their areas of practice and infection control must be considered as an essential component of clinical governance. The clinical department lead for infection control is a medical consultant who is expected to provide leadership for, maintain an overview of and act as a contact point for the collection, dissemination and use of relevant infection control data. The lead is not expected to be an infection control specialist. Although the remit of the clinical department lead is for infection control throughout the clinical department, it is expected that the primary role will be to relate to medical staff, although this will vary dependent on the nature of the unit. For the predominately ward based clinical departments, the senior clinical nurses and senior sisters/ charge nurses already have infection control responsibilities and many areas have infection control link nurses.
Role 1. to act as the first point of contact for infection control related issues
within the division 2. to promote good infection control practice within the division 3. to liaise with the infection control doctor [consultant microbiologist] and
Infection Control Team, divisional director, clinical director and service manager as appropriate about infection control issues
4. to receive Trust data, advice, policies, alerts etc relevant to their division,
and to disseminate this information appropriately within the division and to present it as appropriate to divisional meetings
5. to establish infection control training needs within the division, and to act
as a resource for relevant training opportunities.
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 23 of 26
Appendix 4:
Role description: Senior charge nurse (SCN)/ clinical service manager (CSM) lead for infection control
General For prevention and control of infection to be effective, infection control activities have to be embedded into everyday practice and applied consistently by everyone. All staff should demonstrate good infection control and hygiene practice. Individual divisions need to have ownership of infection control in their areas of practice and infection control must be considered as an essential component of clinical governance.
The senior clinical nurse/ clinical service manager is accountable for the infection control practicess and standards of cleanliness on their wards/ clinical areas. The SCN/CSM lead for infection control is expected to provide leadership for, maintain an overview of, and act as a contact point for the collection, dissemination and use of relevant infection control data. The lead is not expected to be an infection control specialist.
Although the remit of the lead is for infection control throughout the clinical department, it is expected that the primary role will be to relate to nursing staff, although this will vary dependent on the nature of the unit. Senior sisters/ charge nurses also have infection control responsibilities and many areas have infection control link nurses who have a training and education remit.
Role 1. act as the first point of contact for infection control related issues within
the division
2. promote good infection control practice within the clinical department
3. liaise with the infection control doctor (consultant microbiologist) and infection control team, divisional director, clinical director and service manager as appropriate about infection control issues
4. receive Trust data, advice, policies, alerts etc relevant to their clinical
department, and to disseminate this information appropriately within the clinical department, presenting it as appropriate to clinical department meetings and managing the implementation
5. in conjunction with the clinical department lead, establish infection control
training needs within the clinical department, ensuring that infection control is included in a ward induction programme for all new staff including medical staff and to act as a resource for relevant training opportunities in collaboration with the Infection Control Team
6. be responsible for establishing a clear structure for infection control within
the directorate
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 24 of 26
7. be responsible for the performance management of poor infection control
practices by challenging practice in the clinical area, utilising the appraisal system and progressing, where necessary, to the use of the capability/ disciplinary process
8. participate in and/or to chair the infection prevention and control group for
their directorates
9. be responsible for leading the discussion regarding all reports relating to infection control and actioned through the group, all methicillin-resistant Staphylococcus aureus (MRSA) bacteraemias and cases of C. difficile, including the findings of RCA (root cause analysis) should be discussed along with follow-up actions
10. facilitate meetings on all wards focusing on clinical safety including
infection control issues such as • MRSA screening, • correct patient placement of infectious patients, • barrier nursed patients, • catheter care and cannula care.
Spot checks are to be carried out by the SCN/ CSM at an agreed frequency
11. be responsible for reporting on infection control issues such as: • weekly hand hygiene audits, • cleaning scores, • infection control reports and • quality metrics at audit and clinical governance meetings
12. be responsible with the consultant in charge of patient care and the
Infection Control Team to undertake, review and action a root cause analysis for cases of MRSA bacteraemia and clostridium difficile
13. monitor and act on any problems regarding ward cleanliness.
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 25 of 26
Appendix 5: key working arrangements day-to-day
SENIOR CLINICAL
NURSES/CSMs (IC LEADS)
DEPUTY MEDICAL
DIRECTOR
MEDICAL DIRECTOR/
DIPC
DEPUTY
CHIEF NURSE
CHIEF EXECUTIVE
INFECTION
CONTROL TEAM
DIVISIONAL INFECTION
CONTROL LEADS
INFECTION CONTROL DOCTOR
The above chart indicates key working arrangements for day-to-day for infection control purposes and does not replace the management structure. No existing line management arrangements are changed. The hospital Control of Infection Committee (CoIC) retains its functions as before:
• to foster an environment within the Trust in which infection control is an integral part of all working practices
• to advise and support the Infection Control Team (ICT)
• to draw the attention of the chief executive (CE), either through the ICT or, if necessary, directly, to any serious problems or hazards relating to infection control
• to consider reports on infections and infection control problems including national reports and initiatives
Strategy for management of risks associated with IPC Version 6; Approved May 2010

Infection Control
Patient Safety Directorate
Cambridge University Hospitals NHS Foundation Trust Page 26 of 26
• to discuss and endorse a plan for the management of outbreaks in the hospital and monitor its implementation
• to discuss and endorse a plan for the hospital response to major outbreaks in the community – the major incident (outbreak) plan – and monitor its implementation
• to: o discuss and endorse the annual infection prevention and control
programme, which will be submitted for approval to the CE, o review the progress of the programme, o assist in its effective implementation, and o review the final results
• to advise on the most effective use of resources available for implementation of the programme and for contingency requirements
• to advise on and approve infection control policies before their submission for the CE’s approval, and review their implementation
• to promote and facilitate the education of all grades of hospital staff in infection control procedures
• to encourage communication among the different disciplines involved. The minutes of the committee meetings should be widely circulated and made accessible to senior medical and nursing staff and appropriate committees
• to review and advise on infection control initiatives undertaken by members of the Trust with the Infection Control Team
• To receive and advise on infection control programmes undertaken by the Occupational Health Department.
The CoIC reports via the director of Infection Prevention and Control to the Quality and Risk Committee. The structure in the Trust is in accordance with Department of Health recommendations described in Winning Ways, action area six: management and organisation.
Strategy for management of risks associated with IPC Version 6; Approved May 2010