strategies for success: strengthening rural partnerships · 7/18/2018 · not leadership speech...
TRANSCRIPT

Strategies for Success:
Strengthening Rural Partnerships
JULY 18, 2018
LCDR Fred Butler Jr MBA MPH
Senior Advisor for Integration and Quality
Quality Improvement and Innovation Group
Center for Clinical Standards and Quality
Centers for Medicare and Medicaid Services
U.S. Department of Health & Human Services

2
For your hard work & commitment
For your leadership and contributions to rural health
For the strategic thinking of everyone in the room
For being part of the continued evolution and
innovation of community-based healthcare

3
Purposes of Session
Share Powerful Leadership and Management Models & Mindsets
Net Forward Energy
Accountability for Bold Goals
Change Management
Resilience
Choice
Real Work, Requests, Offers, Networking, Deal-making & Action
Review potential opportunities for Community-Based Organizations
Generating Results to Address the Opioid Crisis
QIO 11th and 12th Scopes of Work
Gain your perspectives, insights and feedback

4CMS has established large-scale, action-focused networks
to spread quality improvement and generate results on a
national scale
Partnership for Patients
4,000+ Hospitals
Transforming Clinical Practices Initiative
120,000+ Clinicians
End Stage Renal Disease Networks
6,000 Dialysis Facilities
Quality Innovation Networks –Quality Improvement Organizations
390+ Communities
12,000+ Nursing Homes
3,800 Home Health Organizations
300 Hospice
1,700 Pharmacies
MACRA and Quality Payment Program - Small, Underserved, Rural Support (SURS)
Up to 200,000 Clinicians

CMS Strategic GoalsTHE CMS STRATEGY WILL BE BUILT ON ONE MAIN GOAL:
PUT PATIENTS FIRST

6
Centers for Medicare and Medicaid Services:
Strategic Goals
1. Empower patients and doctors to make decisions about their
health care.
2. Usher in a new era of state flexibility and local leadership.
3. Support innovative approaches to improve quality,
accessibility, and affordability.
4. Improve the CMS customer experience.

7A Continuum of Energy, Thoughts,
Statements
Positive (+) | Negative (-)
What Works What Doesn’t Work
Good Stories Bad Stories
Opportunities Problems
What We Can Do What We Can’t Do
What I Do Have What I Don’t Have
Acting Analyzing, Wishing
Taking Responsibility Blame

8Cultivating a Mindset of Net
Forward Energy

Assertions
Declarations
Requests & Offers
Acknowledgements
“Yes, and”
Effective Questions
Leadership Happens Through Language-- Leadership Speech Acts --

Gossip
Complaints
Worries
Frets
Ineffective Questions
Not Leadership Speech Acts

11
11
“I believe that this nation should commit itself to achieving the
goal, before this decade is out, of landing a man on the moon
and returning him safely to the earth.”
--- President John F. Kennedy,
Delivered in person before a joint session of Congress
May 25, 1961
Bold Aims Create Systems; Systems Create Results

12Partnership for Patients
Focused on 2 Breakthrough Aims

13National Hospital-Acquired Conditions (HACs) Rate:
HACs per 1,000 Discharges
145 142132
121 121
9894
90
0
20
40
60
80
100
120
140
160
2010 2011 2012 2013 2014 2015 2016*
Historical Trend 2014 Rebaselined HAC Rate*preliminary
data
Source: AHRQ, National HAC Scorecard 2014 and 2016
14National Results on Patient Safety:
Substantial Progress Thru 2015
Source: Agency for Healthcare Research & Quality. “Saving Lives and Saving Money: Hospital-Acquired
Conditions Update. Interim Data From National Efforts To Make Care Safer, 2010-2014.” December 1, 2015.
125,000 lives saved
$28B in cost savings
3.1M fewer harms
15Pause for Reflection
and Discussion
1. What is your main insight from this
material so far?
2. What are some of your own
experiences with these kinds of
leadership and management
approaches?

167 Key Goals of CMS Transforming
Clinical Practice Initiative
1
6

1791% of 22,656 Enrolled TCPI Practices are small, rural or operating in medically underserved areas
17
DesignationNumber of Practices
Percent of Total Enrollment
Medically Underserved Areas 11,913 52.58%
Rural Areas 3,872 17.09%
Small Practices 17,420 76.88%
Small, Rural, OR Medically
Underserved Practices20,642 91.11%
Small, Rural, AND Medically
Underserved Practices1,997 8.81%

18
CCWV Service
Area by zip code
(shaded area)• 15 Health Centers
• 1 Dental Clinic
• 8 Pharmacies
• Behavioral Health
• Pain Management
• 50 School-Based Centers

19Framing the Opioid Problem for
a High Performing Practice in WV
In 2016, the five states with the highest rates of death due to drug overdose were:
• West Virginia (52.0 per 100,000)
• Ohio (39.1 per 100,000)
• New Hampshire (39.0 per 100,000)
• Pennsylvania (37.9 per 100,000)
• Kentucky (33.5 per 100,000)

20Community Care of WV’s Integrated Pain Care model
All patients with pain complaints are welcomed at any practice location
1. Patients are assessed and a determination is made if opioid prescriptions in excess of 30 days is a likely treatment path.
2. CDC guidelines are considered.
3. The patient receives education about the integrated program and a sample controlled substances contract is discussed with the patient.
4. Internal referral to our “specialty” program is made.
5. Patients are contacted by the pain management clinic to begin pre-visit planning including Opioid Risk Assessments, PDMP education, SDoH, SBIRT, psychiatric assessments for comorbidities, etc.
6. The PCP and pain management team develop a shared care plan for treatment after the patient is assessed by the chronic pain team.

21
The opioid program data that CCWV does know
Program Result
Patients entering the program since 2013 2692
Active users today 1057
Overdoses from our program users 0

39% of the total hospitals are identified as rural/CAH

23Hospital Improvement Innovation
Network—Minnesota

24Hospital Association of New York State
HIIN: Improvement in Sepsis

25
We were taught….
That People Are
Resistant to Change

26
In fact…
People Are Not Resistant to Change
27
In fact…
People Are Not Resistant to Change
We Change All the Time!

28
In fact…
People Are Not Resistant to Change
We Change All the Time!
However…
People Are Resistant to Being Changed.

29Lead Change by Helping People
Invent Their Own Changes
What is working?
What is causing it to work?
What is our objective here?
What could we do…More of?
Better?
Differently?

30Pause for Reflection
and Discussion
1. What is your main insight from this latest
material?
2. What are some of your own experiences
opioids and change management?

31
“Real Work” is:
• Making Commitments
• Delivering on Commitments
• Securing Commitments from others

32
Work is not…
Talking About Commitments
33
Together, Doing Real Work,
We Can Make the World Turn
200 people at the Rural Health Care Improvement Collaboration Meeting
engage repeatedly in making requests and offers….say, 5-10 commitments
each:
That could be 1,000 to 2,000 commitments!
What we ask of you:
Embrace Change!
Seek Out Innovation, New Experiences, New Partners!
Think About Data Differently!
33

“The antidote to exhaustion
…is wholeheartedness.”
-- David Whyte
“Crossing the Unknown Sea”
Fostering Resilience in
Ourselves and Others
35
What Are the Sources of Resilience?
Wholeheartedness
Purpose
Embracing Change; Leading Change
Partners
Choice
Perspective

A Powerful Model
Stimulus Response

Choice: The Most Powerful Model
Stimulus CHOICE Response

Viktor E. Frankl
Made Extraordinary Choices
Seminal Book:
Man’s Search for
Meaning
39
Pause for Reflection and Discussion
As a leader, what might you do more
of, better or differently today, and
going forward?

40Our “Way” of
Operating to Achieve Results
Bold, Clear Aims -- Implemented at Scale
Focus on Results
Do More of What Works
Make Best-In-Class Performance, Common
Performance
Tight About the “What” Outcome; Flexible on
the “How”
Foster and Foment Joy in Work

41Emerging Key Priority Areas to Guide
Our Improvement Work Through 2024
Opioids & Behavioral Health Nursing Home Quality
Burden Reduction Supporting Patients Through Care Transitions
Patient Safety Chronic Disease Management/Self-Management
Rural Health, Vulnerable Populations and
Patient & Family Engagement
are Cross-cutting Priorities
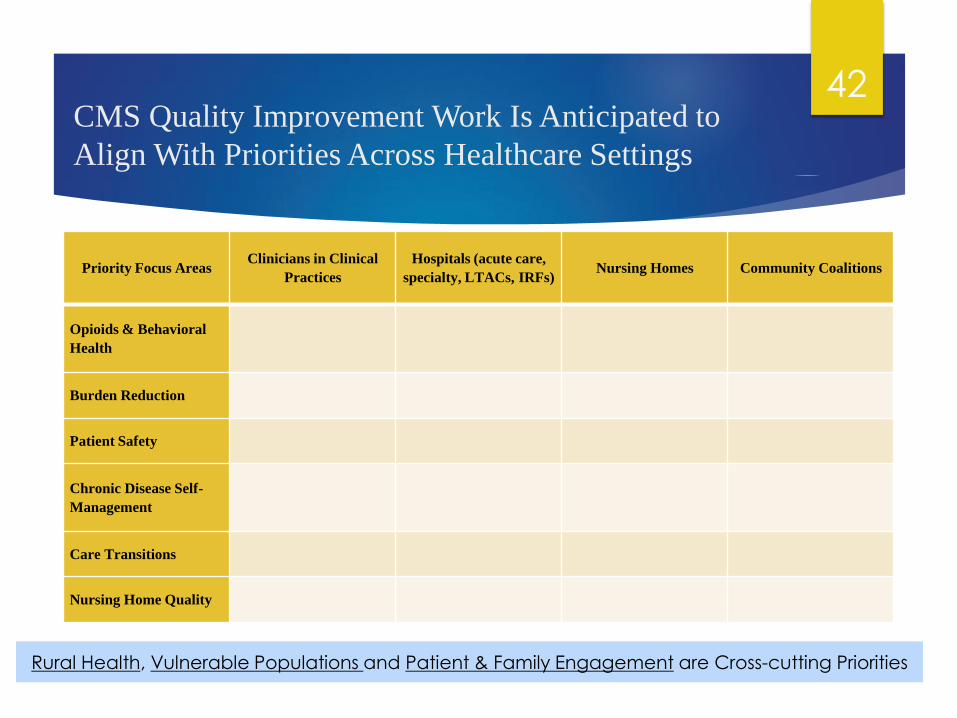
42CMS Quality Improvement Work Is Anticipated to
Align With Priorities Across Healthcare Settings
Priority Focus AreasClinicians in Clinical
Practices
Hospitals (acute care,
specialty, LTACs, IRFs)Nursing Homes Community Coalitions
Opioids & Behavioral
Health
Burden Reduction
Patient Safety
Chronic Disease Self-
Management
Care Transitions
Nursing Home Quality
Rural Health, Vulnerable Populations and Patient & Family Engagement are Cross-cutting Priorities

43
Intended Approach
Less reporting, fewer deliverables, and more
improvement work
Maximize competition
Continue testing promising innovations through
the Strategic Innovation Engine
Advance and scale up promising innovations from
innovation projects and other successful
initiatives on the front lines
Sustain and expand continuous quality
improvement based on data from Beneficiary and
Family Centered Care functions
Reward Value
Use of CMS datasets for impact evaluation
Be flexible on the “how” methods and tight on the
“what” outcomes
Perform work at National Scale across all key
healthcare settings, including: clinical practices,
hospitals, nursing homes and communities
Work in close partnership with both patients &
providers – put patients over paperwork
Align with Administration priorities, other federal
programs/agencies, and team with private partners
Align with and implement CMS Meaningful
Measures: fewer, more important measures with a
focus on outcomes/results
Strong use of self-reported QI data, with validation, to
drive improvement work
44Questions for Discussion & Feedback
What are your insights and reactions to these
CMS priorities?
What opportunities does this work potentially
create for HRSA rural partners?
What else?

45
Thank you!
LCDR Fred Butler Jr MBA MPH
Senior Advisor for Integration and Quality
Quality Improvement Innovation Group
Centers for Clinical Standards and Quality
Centers for Medicare and Medicaid Services