stop taking the piss luke burman stoppit queensland autumn symposium may 2015
TRANSCRIPT

Stop taking the piss
Luke BurmanSTOPPIT
Queensland Autumn Symposium May 2015
18mo boy fevers 1/7

No significant history otherwise
Vaccinations UTD
18mo boy fevers 1/7

No significant history otherwise
Vaccinations UTD
18mo boy fevers 1/7T39.1RR20HR100SpO2
98%CRT <2Alert
No significant history otherwise
Vaccinations UTD
18mo boy fevers 1/7T39.1RR20HR100SpO2
98%CRT <2Alert
Looks very well, smiling, iPhone+

No significant history otherwise
Vaccinations UTD
18mo boy fevers 1/7T39.1RR20HR100SpO2
98%CRT <2Alert
Looks very well, smiling, iPhone+
Neither focus nor concern on detailed systems exam
No significant history otherwise
Vaccinations UTD
18mo boy fevers 1/7T39.1RR20HR100SpO2
98%CRT <2Alert
Looks very well, smiling, iPhone+
Neither focus nor concern on detailed systems exam
Past his bed timeGrumpy
pa(re)nts

No significant history otherwise
Vaccinations UTD
18mo boy fevers 1/7T39.1RR20HR100SpO2
98%CRT <2Alert
Looks very well, smiling, iPhone+
Neither focus nor concern on detailed systems exam
Past his bed timeGrumpy
pa(re)nts
He’s been in ED 35mins

No significant history otherwise
Vaccinations UTD
18mo boy fevers 1/7T39.1RR20HR100SpO2
98%CRT <2Alert
Looks very well, smiling, iPhone+
Neither focus nor concern on detailed systems exam
Past his bed timeGrumpy
pa(re)nts
He’s been in ED 35mins
What do you do next?


24

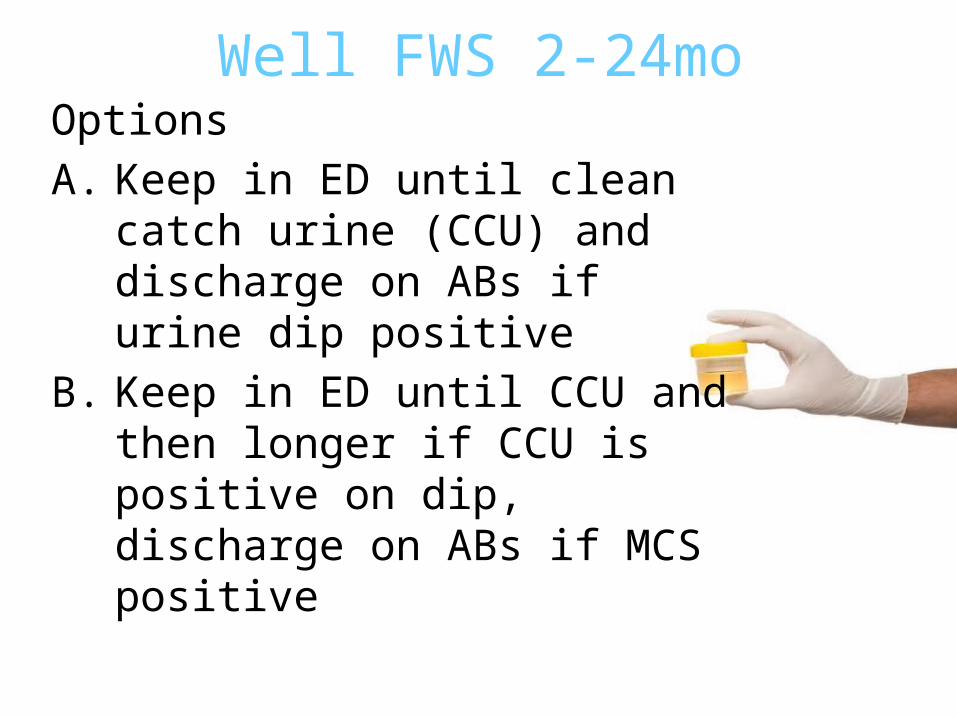
Well FWS 2-24mo

Well FWS 2-24moOptions

Well FWS 2-24moOptionsA. Keep in ED until clean catch urine
(CCU) and discharge on ABs if urine dip positive
Well FWS 2-24moOptionsA. Keep in ED until clean catch urine
(CCU) and discharge on ABs if urine dip positive
B. Keep in ED until CCU and then longer if CCU is positive on dip, discharge on ABs if MCS positive

Well FWS 2-24moOptionsA. Keep in ED until clean catch urine
(CCU) and discharge on ABs if urine dip positive
B. Keep in ED until CCU and then longer if CCU is positive on dip, discharge on ABs if MCS positive
C. Discharge now, no further work-up

Well FWS 2-24moOptionsA. Keep in ED until clean catch urine
(CCU) and discharge on ABs if urine dip positive
B. Keep in ED until CCU and then longer if CCU is positive on dip, discharge on ABs if MCS positive
C. Discharge now, no further work-upD. Discharge now, some other
approach

So why do we take the piss…?

So why do we take the piss…?
? Because we always do? Because guidelines say so
So why do we take the piss…?
? Because we always do? Because guidelines say so? To identify UTI…..so that
we can treat it!!

So why do we take the piss…?
? Because we always do? Because guidelines say so? To identify UTI…..so that
we can treat it!!? To prevent pyelonephritis

So why do we take the piss…?
? Because we always do? Because guidelines say so? To identify UTI…..so that
we can treat it!!? To prevent pyelonephritis? To prevent renal scarring

So why do we take the piss…?
? Because we always do? Because guidelines say so? To identify UTI…..so that
we can treat it!!? To prevent pyelonephritis? To prevent renal scarring? To prevent urosepsis and DEATH

So why do we take the piss…?
? Because we always do? Because guidelines say so? To identify UTI…..so that
we can treat it!!? To prevent pyelonephritis? To prevent renal scarring? To prevent urosepsis and DEATH? To prevent CKD and hypertension

So why do we take the piss…?
? Because we always do? Because guidelines say so? To identify UTI…..so that
we can treat it!!? To prevent pyelonephritis? To prevent renal scarring? To prevent urosepsis and DEATH? To prevent CKD and hypertension? To decrease symptoms



Anals of Emergency Medicine
n


UTI in kids – big deal?

UTI in kids – big deal?8% of girls and 2% of boys are diagnosed with at
least one UTI by the age of seven years.
UTI in kids – big deal?8% of girls and 2% of boys are diagnosed with at
least one UTI by the age of seven years.= a “thing”
UTI in kids – big deal?8% of girls and 2% of boys are diagnosed with at
least one UTI by the age of seven years.
Incidence in febrile children<3mo
girl 7.5% boy 8.7%
3-12mo girl 8.3% boy 1.7%
12-24 mo girl 2.1% boys????

UTI in kids – big deal?8% of girls and 2% of boys are diagnosed with at
least one UTI by the age of seven years.
Incidence in febrile children<3mo
girl 7.5% boy 8.7%
3-12mo girl 8.3% boy 1.7%
12-24 mo girl 2.1% boys???? Shaikh N, Morone NE, Bost JE, et al. Prevalence of urinary tract infection in childhood: a meta-analysis. Pediatr Infect Dis J. 2008;27:302-308.

Will this well child get septic?
Will this well child get septic?
and
DIE!!!

Will this well child get septic?
How common is paediatric urosepsis?
and
DIE!!!

Will this well child get septic?
How common is paediatric urosepsis?
Older children and teens (<19yo): 0.56/1000/year
<28d: 3.6/1000/year
70% of uroseptics were neonatal
and
DIE!!!
Will this well child get septic?
Evidence that paediatric urosepsis, especially outside neonatal age is RARE
and
DIE!!!
Will this well child get septic?
Evidence that paediatric urosepsis, especially outside neonatal age is RARE
60% due to bacteraemia and respiratory causes
and
DIE!!!

Will this well child get septic?
Evidence that paediatric urosepsis, especially outside neonatal age is RARE
60% due to bacteraemia and respiratory causes
Evidence that paediatric urosepsis is LESS FATAL than sepsis from other sources
and
DIE!!!
Will this well child get septic?
Evidence that paediatric urosepsis, especially outside neonatal age is RARE
60% due to bacteraemia and respiratory causes
Evidence that paediatric urosepsis is LESS FATAL than sepsis from other sources
Case fatality rate of 3.7% v.~10%
and
DIE!!!

Will this well child get septic?
Evidence that paediatric urosepsis, especially outside neonatal age is RARE
60% due to bacteraemia and respiratory causes
Evidence that paediatric urosepsis is LESS FATAL than sepsis from other sources
Case fatality rate of 3.7% v.~10%
Not just a modern finding. Developed world and work-up from pre-1970s papers do not identify a higher rate of urosepsis in the absence of advanced medicine
and
DIE!!!

Will this well child get septic?
No evidence about rate of progression of simple UTI to sepsis and nothing in historical literature to suspect that this rate would be high.
and
DIE!!!

Will this well child get septic?
No evidence about rate of progression of simple UTI to sepsis and nothing in historical literature to suspect that this rate would be high.
Paediatric UTI frequently presents as a prolonged fever >2/7 without other localizing symptoms
and
DIE!!!

Will this well child get septic?
No evidence about rate of progression of simple UTI to sepsis and nothing in historical literature to suspect that this rate would be high.
Paediatric UTI frequently presents as a prolonged fever >2/7 without other localizing symptoms
Late presentation is not clearly associated with sepsis
and
DIE!!!

Will this well child get septic?
Paediatric urosepsis is:
Rare
Not particularly fatal
Unlikely to rapidly progress from uncomplicated UTI
and
DIE!!!
Will this well child get septic?
Probably not…
and
DIE!!!

Phew, but what about scarring ?
Phew, but what about scarring ?
? Does UTI progress to pyelonephritis
? Does UTI progress to scarring
Phew, but what about scarring ?
? Does UTI progress to pyelonephritis47%
? Does UTI progress to scarring15%

Phew, but what about scarring ?
? Does UTI progress to pyelonephritis47%
? Does UTI progress to scarring15%
Yes&
Yes

DONE!Causes
scarring: test and
treat

Hang on…is scarring bad?

Hang on…is scarring bad?
Old guidelines based on 2 studiesGill et al. 1976. Chart Review. N=100 children with hypertension. Reflux nephropathy believed to be the cause in 14. No long-term follow up.
Shore and Gorelick 1999. A review of several very small studies. Many were of children with abN IVU. Suggestion of decreased GFR

Hang on…is scarring bad?
Multiple other studies since 2000Prospective, controlled, largeLong-term follow-upConfirm rate of scarring with paediatric UTINo clinically or statistically significant increased rate of CKD or decreased GFREpidemiological data also

Hang on…is scarring bad?
Scarring sounds bad…

But we got the BOMB!

Do antibiotics even work?
UTIPyelonephritisScarringSepsisSymptoms
Do antibiotics even work?
UTIPyelonephritisScarringSepsisSymptoms

Do antibiotics even work?
UTIPyelonephritisScarringSepsisSymptoms
Natural HistoryNo good data!!!!?1908 German study – can’t find it!

Do antibiotics even work?
UTIPyelonephritisScarringSepsisSymptoms
Natural HistoryUnpublished prospective cohort study
presented at 2000 Pediatric Academic Societies Annual Meeting.n= 3066 infants 0-3mo T 38°Cmanaged per physicians whimsome investigated, sent home, some admitted, some treated
Statistical trickery~54 UTIs never received treatment2 infants subsequently diagnosed UTI Neither bacteremic; both treated and recovered uneventfully.

Do antibiotics even work?
UTI (?)PyelonephritisScarringSepsisSymptoms

Do antibiotics even work?
UTI (?)PyelonephritisScarringSepsisSymptoms

Do antibiotics even work?
UTI (?)PyelonephritisScarringSepsisSymptoms
Lots of recent studies including a Cochrane review of IV v PO
No data on whether ABs modify progression to pyelonephritis
Do antibiotics even work?
UTI (?)Pyelonephritis (?)ScarringSepsisSymptoms

Do antibiotics even work?
UTI (?)Pyelonephritis (?)ScarringSepsisSymptoms
Do antibiotics even work?AAP guidelines:Cites a chart review and a
retrospective study suggest early ABs decrease scarring
Several other retrospective audits also suggest reduced scarring, especially with early antibiotics
UTI (?)Pyelonephritis (?)ScarringSepsisSymptoms

Do antibiotics even work?AAP guidelines:Cites a chart review and a
retrospective study suggest early ABs decrease scarring
Several other retrospective audits also suggest reduced scarring, especially with early antibiotics
Recent prospective studies: several, good sized studies. Nearly all: no relation between timing of ABs and scarring. Only 1 study showed +ve association if ABs delayed >4.5 daysLatest: 287 children. No difference between early (<12h) AB
and delayed (up to 5h) AB groups
UTI (?)Pyelonephritis (?)ScarringSepsisSymptoms
Do antibiotics even work?
UTI (?)Pyelonephritis (?)Scarring (-)SepsisSymptoms

Do antibiotics even work?
UTI (?)Pyelonephritis (?)Scarring (-)SepsisSymptoms

Do antibiotics even work?
UTI (?)Pyelonephritis (?)Scarring (-)SepsisSymptoms
PreventionUrosepsis rare in kidsAntibiotic complications common
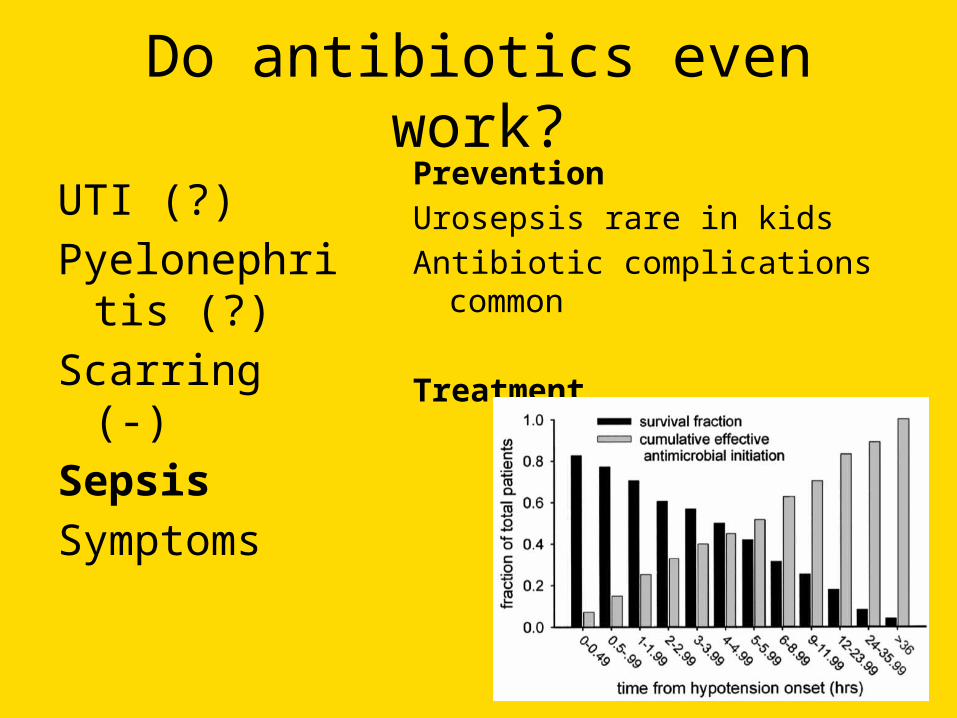
Do antibiotics even work?
UTI (?)Pyelonephritis (?)Scarring (-)SepsisSymptoms
PreventionUrosepsis rare in kidsAntibiotic complications common
Treatment

Do antibiotics even work?
UTI (?)Pyelonephritis (?)Scarring (-)Sepsis (+/-)Symptoms

Do antibiotics even work?
UTI (?)Pyelonephritis (?)Scarring (-)Sepsis (+/-)Symptoms

Do antibiotics even work?
UTI (?)Pyelonephritis (?)Scarring (-)Sepsis (+/-)Symptoms
Surpise! No data.
Do antibiotics even work?
UTI (?)Pyelonephritis (?)Scarring (-)Sepsis (+/-)Symptoms (?)

What?! No bug killers?

What?! No bug killers?
Otitis mediaTonsillitisPharyngitisSinusitisDrained abscessValvulopathy & dental proceduresOther minor infectionOther minor infection

First do no harm…
AnaphylaxisAntibiotic associated diarrhoeaPseudomembranous colitisDrug eruptionsAntimicrobial resistance

First do no harm…
AnaphylaxisAntibiotic associated diarrhoeaPseudomembranous colitisDrug eruptionsAntimicrobial resistance
MEDICALISATION OF MILD ILLNESS
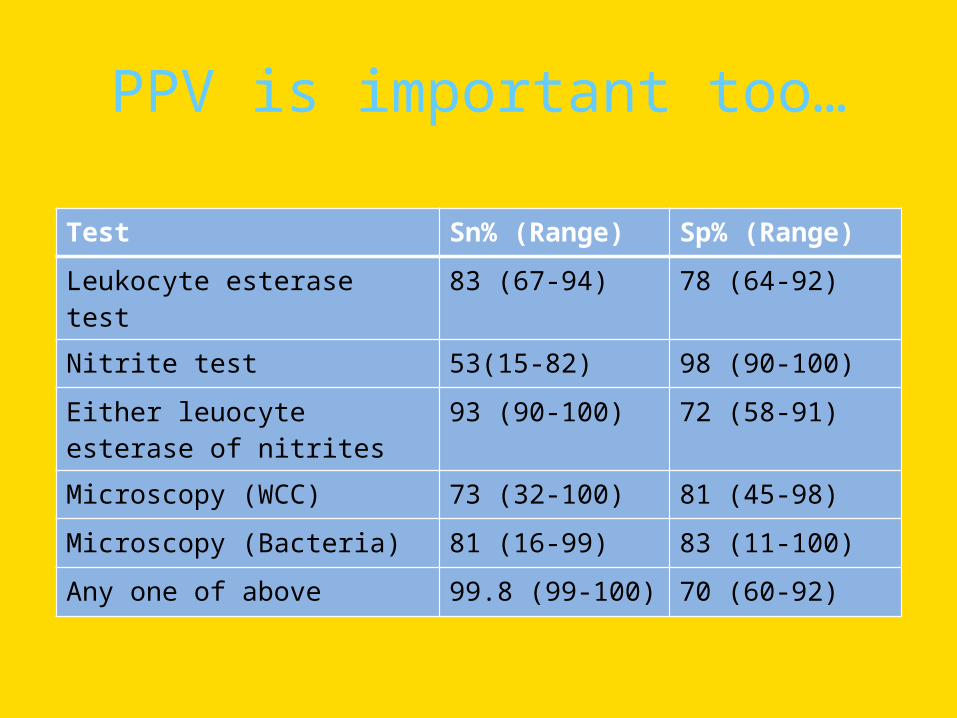
PPV is important too…
Test Sn% (Range) Sp% (Range)
Leukocyte esterase test 83 (67-94) 78 (64-92)
Nitrite test 53(15-82) 98 (90-100)
Either leuocyte esterase of nitrites
93 (90-100) 72 (58-91)
Microscopy (WCC) 73 (32-100) 81 (45-98)
Microscopy (Bacteria) 81 (16-99) 83 (11-100)
Any one of above 99.8 (99-100) 70 (60-92)

PPV is important too…
+ PPV = 58%

PPV is important too…
+ =

PPV is important too…
Sterile pyuria: common
Asymptomatic bacteruria– VARIABLE BETWEEN 0.5 AND 4% BOYS <<<<<girls– Usually cited as 2%

So, what’re you saying?

So, what’re you saying?
Stop giving antibiotics to kids with UTI????????

So, what’re you saying?
Stop giving antibiotics to kids with UTI????????
Stop getting urine samples when UTI suspected???????

So, what’re you saying?
Stop giving antibiotics to kids with UTI????????
Stop getting urine samples when UTI suspected???????
NO

What I am saying

What I am saying
The evidence is such that the role of antibiotics in uncomplicated paediatric UTI should be questioned with good quality RCTs. Until
then, antibiotics for all paediatric UTI remain a standard of care.

What I am saying
The evidence is such that the role of antibiotics in uncomplicated paediatric UTI should be questioned with good quality RCTs. Until
then, antibiotics for all paediatric UTI remain a standard of care.
The evidence is such that aggressive policies demanding same day urinary collection in low risk, well infants and small children with FWS, outside the neonatal period, have no basis in
evidence and can be ignored.
What I am saying
The evidence is such that the role of antibiotics in uncomplicated paediatric UTI should be questioned with good quality RCTs. Until
then, antibiotics for all paediatric UTI remain a standard of care.
The evidence is such that aggressive policies demanding same day urinary collection in low risk, well infants and small children with FWS, outside the neonatal period, have no basis in
evidence and can be ignored.STOPPIT

What I am saying
The evidence is such that the role of antibiotics in uncomplicated paediatric UTI should be questioned with good quality RCTs. Until
then, antibiotics for all paediatric UTI remain a standard of care.
The evidence is such that aggressive policies demanding same day urinary collection in low risk, well infants and small children with FWS, outside the neonatal period, have no basis in
evidence and can be ignored.STOPPITKEEP ITFOR
NOW

4 weeks old + fever
12mo 3x UTIs FWS

Documented VUR

16mo multiple congenital abnormalities

CRT 4s
Looks unwell

Acquired immunodeficiency

On chemo

2mo – 2 yearsFever < 4 daysFWS on detailed surveyWell by senior opinionMinimal SxNo PHx UTINo risk factorsLives within cooeeAccess to follow upCapable parents
STO
P T
AK
ING
TH
E P
ISS
STO
P T
AK
ING
TH
E P
ISS
LET THEM GO HOMEHome clean catchStore in fridge >4hClear TCB adviceOpen door policyEnsure follow up
2mo – 2 yearsFever < 4 daysFWS on detailed surveyWell by senior opinionMinimal SxNo PHx UTINo risk factorsLives within cooeeAccess to follow upCapable parents