steroids in acute bacterial online meningitis author
TRANSCRIPT

Steroids in acute bacterial meningitis
Javier Garau, MD, PhDUniversity of Barcelona
SpainESCMID Summer School, Porto , July 2009ESCMID Online Lectu
re Library
© by author

Dexamethasone treatment in childhood bacterial meningitis in Malawi: a randomised controlled trial.
• Double-blind, placebo controlled trial; 598 children with pyogenic meningitis admitted to the Queen Elizabeth Central Hospital, Blantyre, Malawi. Neurological, developmental, and hearing assessments at 1 and 6 months after discharge.Primary outcome: overall death. Secondary outcomes: sequelae, in-hospital deaths, and death after discharge. Analysis was done by intention to treat.
• FINDINGS: Of the 598 children, 307 (51%) were assigned to DXM and 295 (49%) to placebo. 338 (40%) had Streptococcus pneumoniae, 170 (28%) Haemophilus influenzae type b, 66 (11%) Neisseria meningitidis, and 29 (5%) Salmonella spp. The number of overall deaths was the same in the two treatment groups (RR 1.00 [95% CI 0.8-1.25], p=0.93). At final outcome, sequelae were identified in 84 (28%) of children on steroids and in 81 (28%) on placebo (RR 0.99 [95% CI 0.78-1.27], p=0.97).
• INTERPRETATION: Steroids are not an effective adjuvant treatment in children with acute bacterial meningitis in developing countries.
Molyneux EM et al. Lancet 2002;360:211-8
ESCMID Online Lecture Library
© by author

IDSA Recommendations for use of adjuntive dexamethasone (DXM) in meningitis. Children
• At present, insufficient data to make a recommendation on the use of DXM in neonates with bacterial meningitis.
• Despite some variability in result of published trials, we believe the available evidence supports the use of adjunctive DXM in infants and children with H. influenzae type b meningitis (A-I).
• DXM should be given 10–20’ prior to, or at least concomitant with, the first antimicrobial dose, at 0.15 mg/kg every 6 h for 2–4 days.
• In infants and children with pneumococcal meningitis, there is controversy concerning DXM (C-II).
IDSA Guidelines for the Management of Bacterial Meningitis. Clin Infect Dis 2004; 39:1267–84
ESCMID Online Lecture Library
© by author

Glycerol and/or Dexamethasone in Childhood BacterialMeningitis: A Randomized, Double-Blind, Placebo-Controlled Trial
• Glycerol, a naturally occurring trivalent alcohol, an essential compound of the human cell membrane, a hyperosmolar agent, and an osmotic diuretic, long used in neurosurgery, neurology, and ophthalmology to reduce raised tissue pressure
• The first systematic trial was performed in Finland during the period 1987–1991. Glycerol appeared to reduce profound hearing loss and persistent neurological abnormalities as efficaciously as dexamethasone, but the series was too small for definitive conclusions.
• Prospective, randomized, double-blind trial comparing adjuvant dexamethasone or glycerol with placebo in children aged from 2 months through 16 years in Latin America.
• Primary end points were death, severe neurological sequelae, or deafness, with the first 2 end points forming a composite end point.
Peltola H et al, Clin Infect Dis 2007; 45:1277–86
ESCMID Online Lecture Library
© by author

Peltola H et al, Clin Infect Dis 2007; 45:1277–86
IV ceftriaxone, 80–100 mg/kg/once daily for 7–10 days.DXM, 0.15 mg/kg/q6h, for 48 h, the first dose 15 min prior to administration of ceftriaxone (if possible).Oral 85% glycerol, given for 48 h, 1.5 g (1.5 mL)/kg/q6h. The first dose 15 min prior to ceftriaxoneNo fluid restriction was used
ESCMID Online Lecture Library
© by author

ESCMID Online Lecture Library
© by author

a Determined by x2 test between 4 groups (for heterogeneity).b Severe neurological sequelae included blindness (7 patients), quadriplegia (8), hydrocephalus requiring a shunt (4), or severe psychomotor retardation (26), with each child counted only once.c Hearing threshold of 80 dB for the better ear.
ESCMID Online Lecture Library
© by author

ESCMID Online Lecture Library
© by author

ESCMID Online Lecture Library
© by author

• No adjuvant therapy significantly affected death or deafness.• In contrast, glycerol and dexamethasone plus glycerol reduced
severe neurological sequelae, compared with placebo; the ORs were 0.31 (95% CI, 0.13–0.76; P<.010) and 0.39 (95% CI, 0.17–0.93; P<.033), respectively.
• For neurological sequelae and death, the ORs were 0.44 (95% CI, 0.25–0.76; P<.003) and 0.55 (95% CI,0.32–0.93; P<.027), respectively.
• Dexamethasone therapy prevented deafness in patients with H. influenzae type b meningitis only if patients were divided grossly into dexamethasone recipients and nonrecipients and if timing between dexamethasone and ceftriaxone administration was not taken into account (OR, 0.27; 95% CI,0.09–0.77; P<.014).
Peltola H et al, Clin Infect Dis 2007; 45:1277–86
ESCMID Online Lecture Library
© by author

ACUTE BACTERIAL MENINGITISADULTS
ESCMID Online Lecture Library
© by author
DEXAMETHASONE IN ADULTS WITH BACTERIAL MENINGITIS
• Prospective, randomized, double-blind trial of adjuvant treatment with DXM as compared with placebo in acute bacterial meningitis.
• DXM (10 mg/q6h/4 days) and placebo administered 15-20 minutes before or with the first dose of antibiotic (Amoxicillin, 2 G/q4h) and given q6h x 4 days.
• The primary outcome measure was the score of The Glasgow Outcome Scale at eight weeks
De Gans, J, et al, NEJM 2002;347:1549-1556
ESCMID Online Lecture Library
© by author

OUTCOMES EIGHT WEEKS AFTER ADMISSION, ACCORDING TO CULTURE RESULTS
Jean de Gans et al, NEJM 2002
ESCMID Online Lecture Library
© by author

OUTCOMES EIGHT WEEKS AFTER ADMISSION, ACCORDING TO CULTURE RESULTS
Jean de Gans et al, NEJM 2002
ESCMID Online Lecture Library
© by author

OUTCOMES EIGHT WEEKS AFTER ADMISSION, ACCORDING TO CULTURE RESULTS
Jean de Gans et al, NEJM 2002
ESCMID Online Lecture Library
© by author

OUTCOMES EIGHT WEEKS AFTER ADMISSION, ACCORDING TO CULTURE RESULTS
Jean de Gans et al, NEJM 2002
ESCMID Online Lecture Library
© by author

OUTCOMES EIGHT WEEKS AFTER ADMISSION, ACCORDING TO CULTURE RESULTS
Jean de Gans et al, NEJM 2002
ESCMID Online Lecture Library
© by author

Jean de Gans et al, NEJM 2002
* *
* RR 0,48 CI95%, 0.24-0.96
ESCMID Online Lecture Library
© by author

IDSA Recommendations for use of adjuntive dexamethasone (DXM) in meningitis
• Adjunctive DXM should be initiated in all adult patients with suspected pneumococcal meningitis.
• DXM should only be continued if the CSF Gram stain reveals gram-positive diplococci,or if blood or CSF cultures are positive for S. pneumoniae.
• DXM should not be given to adult patients who have already received antimicrobial therapy, because administration of DXM in this circumstance is unlikely to improve patient outcome (A-I).
• The data are inadequate to recommend adjunctive DXM to adults with meningitis caused by other bacterial pathogens, although some authorities would initiate dexamethasone in all adults.
• In patients with suspected pneumococcal meningitis who receive adjunctive DXM,addition of rifampin to the empirical combination of vancomycin plus a third-generation cephalosporin may be reasonable pending culture results and in vitro susceptibility testing (B-III).
IDSA Guidelines for the Management of Bacterial Meningitis. Clin Infect Dis 2004; 39:1267–84
ESCMID Online Lecture Library
© by author

DEXA METHASONE IN ADULT BACTERIAL MENINGITIS
Recent experience
ESCMID Online Lecture Library
© by author

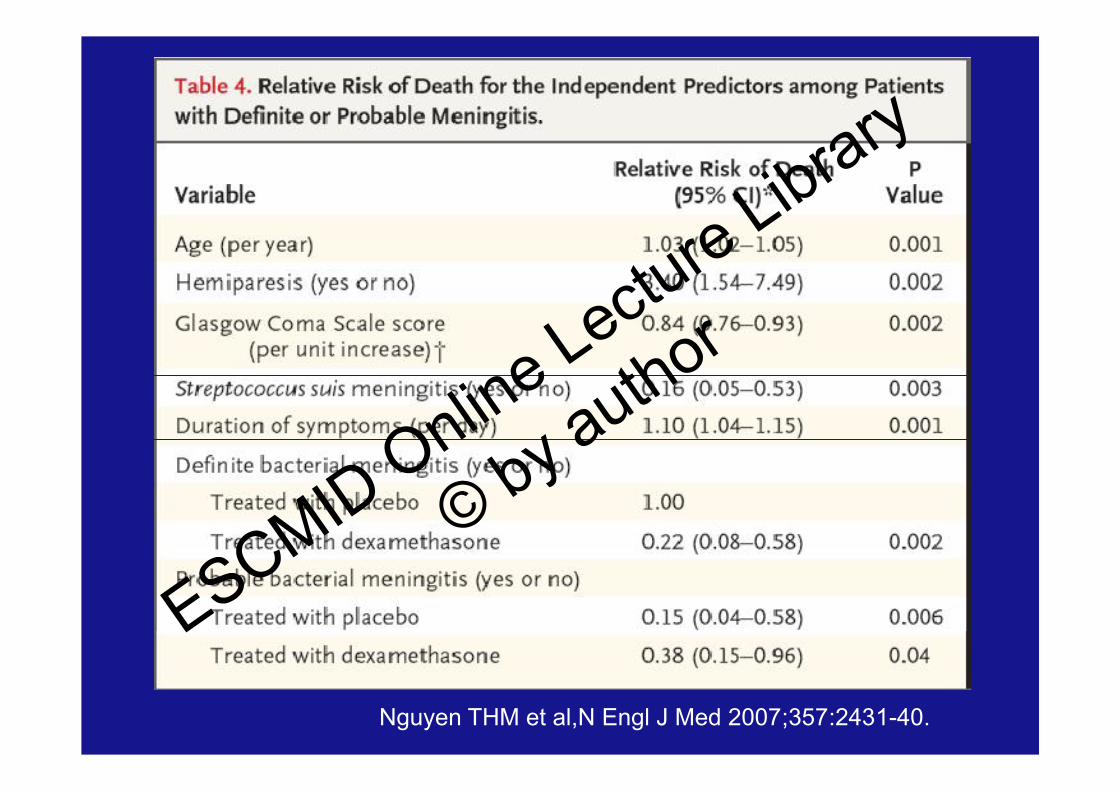
Dexamethasone in Vietnamese Adolescents and Adultswith Bacterial Meningitis
• Randomized, double-blind, placebo-controlled trial of dexamethasone in 435 patients over the age of 14 years who had suspected bacterial meningitis.
Results• An ITT analysis of all the patients showed that DXM was not associated with a
significant reduction in the risk of death at 1 month (RR, 0.79; 95% CI, 0.45 to 1.39) or the risk of death or disability at 6 months (OR, 0.74; 95% CI, 0.47 to 1.17).
• In patients with confirmed bacterial meningitis, however, there was a significant reduction in the risk of death at 1 month (RR, 0.43; 95% CI, 0.20 to 0.94) and in the risk of death or disability at 6 months (OR, 0.56; 95% CI, 0.32 to 0.98).
Conclusions• Dexamethasone does not improve the outcome in all adolescents and adults with
suspected bacterial meningitis• A beneficial effect is confined to patients with microbiologically proven disease,
including those who have received prior treatment with antibiotics.
Nguyen THM et al,N Engl J Med 2007;357:2431-40.
ESCMID Online Lecture Library
© by author
Nguyen THM et al,N Engl J Med 2007;357:2431-40.
ESCMID Online Lecture Library
© by author

Corticosteroids for Bacterial Meningitis in Adults in Sub-Saharan Africa
• In sub-Saharan Africa, bacterial meningitis is common and is associated with a high mortality.
• Adjuvant therapy with corticosteroids reduces mortality among adults in the developed world, but it has not been adequately tested in developing countries or in the context of advanced HIV infection
• Randomized, double-blind, placebo-controlled trial of DXM (16 mg twice daily for 4 days) and an open-label trial of IM vs. IV ceftriaxone (2 g twice daily for 10 days) in adults with an admission diagnosis of bacterial meningitis in Blantyre, Malawi
Scarborough M et al. N Engl J Med 2007;357:2441-50.
ESCMID Online Lecture Library
© by author

ESCMID Online Lecture Library
© by author

Scarborough M et al N Engl J Med 2007;357:2441-50.
ESCMID Online Lecture Library
© by author

DXM IN MENINGITISCONCLUSIONS
• Overall, corticosteroids significantly reduce mortality, severe hearing loss and neurological sequelae. In adults with community-acquired bacterial meningitis, corticosteroid therapy should be administered in conjunction with the first antibiotic dose. In children, data support the use of adjunctive corticosteroids in children in high-income countries. No beneficial effect of corticosteroids found for children in low-income countries (Cochrane Database Syst Rev. 2007 Jan 24;(1):CD004405)
• In children, GLY seriously challenges the position of DXM as adjuvant medication. Severe neurological sequelae are relieved by GLY, whereas no current medication prevents hearing impairment.
• The same can be said of adults with similar baseline characteristics. • Patient selection on the basis of host and pathogen genotype may
improve the outcome.
ESCMID Online Lecture Library
© by author

Levels of Vancomycin in CSFof Adult Patients Receiving Adjunctive Corticosteroids
to Treat Pneumococcal Meningitis• Observational open multicenter study, adult patients
admitted to ICU because of suspected pneumococcal meningitis
• IV cefotaxime (200 mg per kg of body weight per day), vancomycin (administered as continuous infusion of 60 mg per kg of body weight per day after a loading dose of 15 mg per kg of body weight)
• Adjunctive therapy with dexamethasone (10 mg/q6h).• Vancomycin levels in CSF were measured on day 2 or
day 3 of therapy and were correlated with protein levels in CSF and vancomycin levels in serum (determined at the same time as levels in CSF).
Ricard JD et al, Clin Infect Dis 2007;44:250-5
ESCMID Online Lecture Library
© by author

ESCMID Online Lecture Library
© by author

Correlation between levels of vancomycin in serum and CSF in patients with meningitis. The bold arrow indicates the patient who was eventually determinedto have meningitis due to Neisseria meningitidis.
Ricard JD et al, Clin Infect Dis 2007:44:250-5
ESCMID Online Lecture Library
© by author

Correlation between the concentration of protein in CSF and the ratio of vancomycin concentration in CSF to vancomycin concentration in serum. Positive correlation confirms that meningeal permeability, partly induced by meningeal inflammation, affects the rate of vancomycin penetration into the CSF. The bold arrow indicates the patient with severe hypoproteinemia
ESCMID Online Lecture Library
© by author

Mean levels of VAN in CSF, compared with mean levels of VAN in serum, in experimental and clinical studies. There was a strong positive correlation between serum and CSF levels of VAN. Open circles, clinical studies that used dexamethasone, including our study (arrow); open squares, experimental studies with dexamethasone; solid circles, clinical studies in which treatment did not include use of dexamethasone; solid squares, experimental studies without dexamethasone.
ESCMID Online Lecture Library
© by author

DEXAMETHASONE AND VANCOMYCIN
• Adjunctive therapy (10 mg every 6 h) for two days.
• Appropriate concentrations of vancomycin in CSF may be obtained even when concomitant steroids are used.
• Dexamethasone can, therefore, be used without fear of impeding vancomycin penetration into the CSF of patients with pneumococcal meningitis, provided that vancomycin dosage is adequate
Ricard JD et al, Clin Infect Dis 2007
ESCMID Online Lecture Library
© by author

Management algorithm for adults with suspected bacterial meningitis.“Stat” indicates that the intervention should be done emergently.e Dexamethasone and antimicrobial therapy should be administered immediately after CSF is obtained.
IDSA Guidelines for the Management of Bacterial Meningitis. Clin Infect Dis 2004; 39:1267–84
ESCMID Online Lecture Library
© by author

Kaplan Meier Survival curve of 187 patients with S.pneumoniae meningitis in Denmark 1999–2000 according to the focus of the infection. Otogenic focusvs. pneumonic focus, sinusitic focus, other foci, and no primary infection focus: Log rank test: P = 0.0002, 0.008,<0.0001, and 0.03, respectively. Other foci vs. no primaryinfection focus: P = 0.01.
ESCMID Online Lecture Library
© by author

PNEUMOCOCCAL MENINGITISEMPIRICAL ANTIBIOTIC TREATMENT
Prevalence of penicillin resistance
- No invasive strains with Cefotaxime MIC >1 mg/L reported:
Cefotaxime, 200 mg/Kg/day, - Invasive strains with cefotaxime MIC > 1 mg/L:
Cefotaxime, 300 mg/Kg/dayPLUS
Vancomycin*
*Continuous infusion of 60 mg/kg/day after a loading dose of 15 mg/kgMean levels of vancomycin in serum and CSF, 25.2 and 7.2 mg/L, respectively (Ricard JD et al, Clin Infect Dis 2007)
ESCMID Online Lecture Library
© by author

PNEUMOCOCCAL MENINGITISDIRECTED THERAPY
- If pen MIC < 0.1 mg/LPenicillin G, 250.000 U/24h
- If pen MIC 0.1 to 4 mg/L (CEF MIC, 0,1-1 (2 ?)Cefotaxime, 200-350 mg/Kg/dayCeftriaxone, 4 grams/day
- Allergic to penicillinVancomycin + rifampin
- Cefotaxime MIC > 2 mg/LAs aboveESCMID Online Lectu
re Library
© by author

ESCMID Online Lecture Library
© by author

Fernández-Viladrich P et al, AAC 1996
ESCMID Online Lecture Library
© by author

CSF bacterial counts at 0 h and bacterial killing rates at 6, 24 and 26 h after antimicrobial therapy in experimental pneumococcal meningitis caused by the highly cephalosporin-resistant ATCC 51916 strain
Evaluation of ceftriaxone, vancomycin and rifampicin alone andcombined in an experimental model of meningitis
Ribes S et al, JAC 2005: 56, 979–982
ESCMID Online Lecture Library
© by author

Evaluation of ceftriaxone, vancomycin and rifampicin alone and combined in an experimental model of meningitis caused by highly cephalosporin-resistant
Streptococcus pneumoniae ATCC 51916
Ribes, S et al, JAC 2005
ESCMID Online Lecture Library
© by author