status asthmaticus
TRANSCRIPT
Status Asthmaticus in Children
Soumya Ranjan ParidaBasic B.Sc. Nursing 4th year
Sum Nursing College

� Chronic inflammatory disorder of the medium and small airways.
� These airways are hypersensitive to certain “triggers” in the environment.
� Intermittent and recurrent episodes of...– Wheezing– Shortness of breath – Chest tightness– Cough - night, early morning
� Usually reversible
� Asthma cannot be cured but its symptoms can be controlled with proper environmental changes and medication.
What is Asthma ?

Status Asthmaticus in Children
� Definition: Status Asthmaticus is a life threatening form of asthma defined as “a condition in which a progressively worsening attack is unresponsive to the usual appropriate therapy with adrenergic drugs and that leads to pulmonary insufficiency.”
� Epidemiology� Pathophysiology� Presentation and Assessment� Treatment
Topics Covered
Risk factors for fatal asthma� Medical
– Previous attack with rapid/severe deterioration or respiratory failure or seizure/loss of consciousness
� Psychosocial– Denial, non-compliance– Depression or other psychiatric disorder– Dysfunctional family
: Epidemiology: Epidemiology
Status Asthmaticus in Children� Epidemiology� Pathophysiology
– Cytokines– Airway pathology– Autonomic nervous system– Pulmonary mechanics– Cardiopulmonary interactions– Metabolism
� Presentation and assessment� Treatment

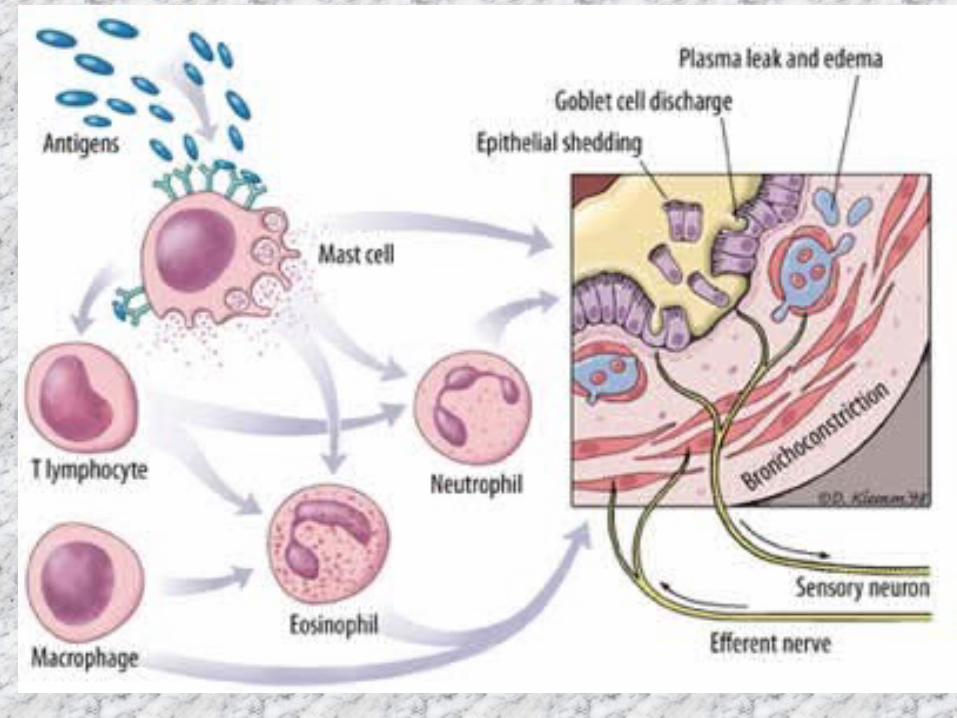
Pathophysiology� Asthma is primarily an
inflammatory disease
Mucous pluggingMucous plugging
Smooth muscle Smooth muscle spasmspasm Airway edemaAirway edema

Inflammatory cytokines
� Activated mast cells and lymphocytes produce pro-inflammatory cytokines (histamine, leukotrienes, PAF,PGD2), which are increased in asthmatics’ airways and bloodstream
:: Pathophysiology Pathophysiology
Airway� The irritable and inflamed airway is
susceptible to obstruction triggered by– Allergens– Infections– Irritants including smoke– Exercise– Emotional stress– GE reflux– Drugs– Other factors
Pathophysiology
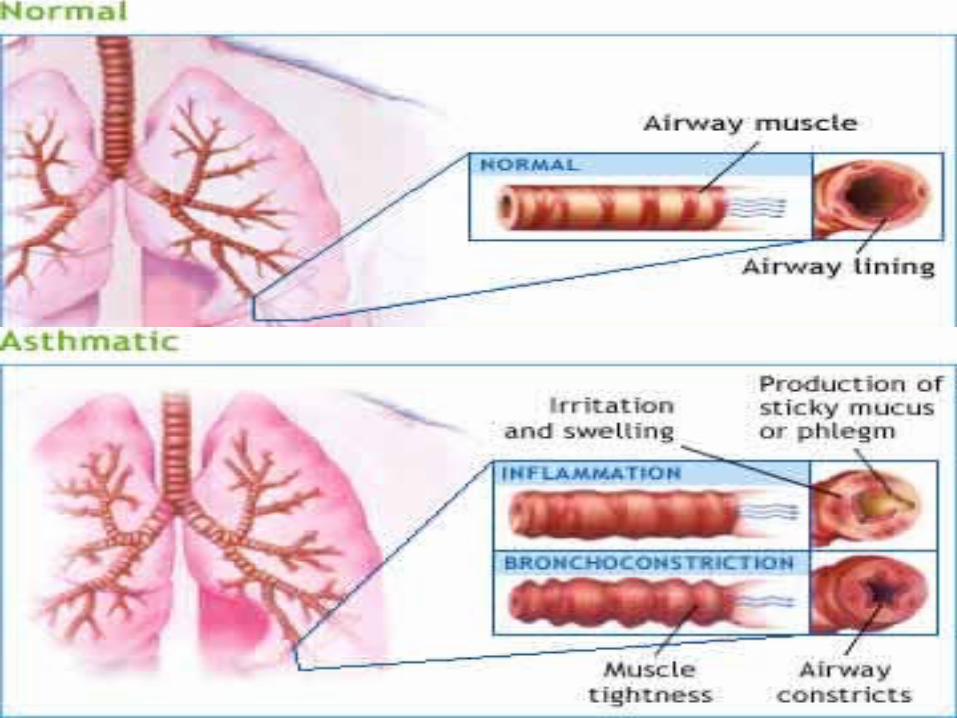

Irritable and damaged airway
HypersecretionHypersecretion
Epithelial damage with exposed nerve endingsEpithelial damage with exposed nerve endings
Hypertrophy of goblet cells and mucus glandsHypertrophy of goblet cells and mucus glands
Pathophysiology
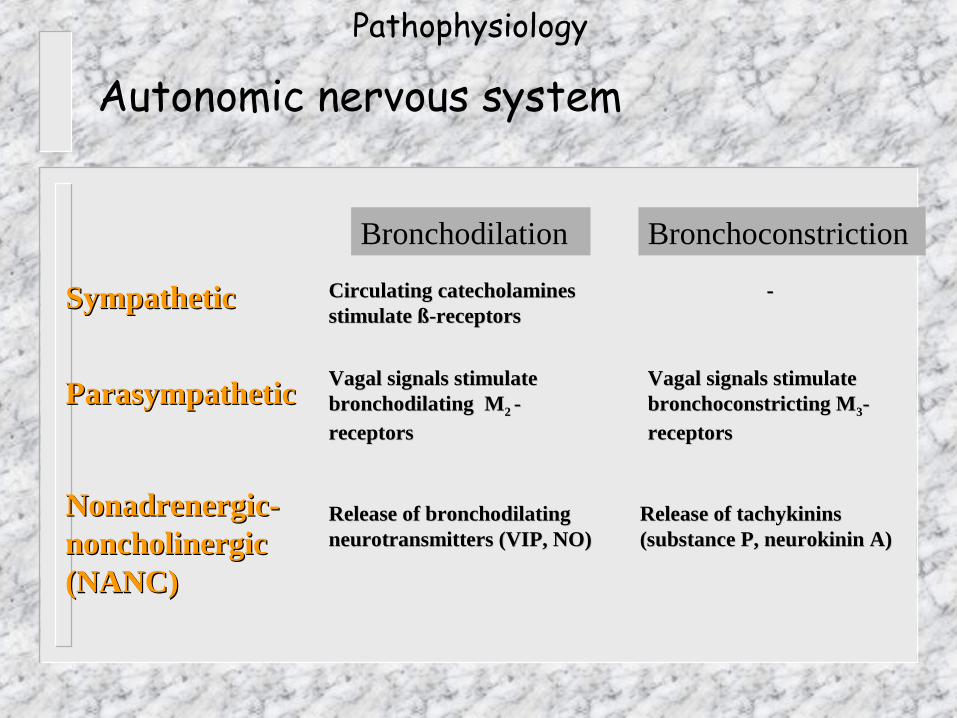
Autonomic nervous system
Bronchodilation Bronchoconstriction
SympatheticSympathetic Circulating catecholamines Circulating catecholamines stimulate ß-receptorsstimulate ß-receptors
--
ParasympatheticParasympathetic Vagal signals stimulate Vagal signals stimulate bronchodilating Mbronchodilating M2 2 - - receptorsreceptors
Vagal signals stimulate Vagal signals stimulate bronchoconstricting Mbronchoconstricting M33--receptorsreceptors
Nonadrenergic-Nonadrenergic-noncholinergic noncholinergic (NANC)(NANC)
Release of bronchodilating Release of bronchodilating neurotransmitters (VIP, NO)neurotransmitters (VIP, NO)
Release of tachykinins Release of tachykinins (substance P, neurokinin A)(substance P, neurokinin A)
Pathophysiology
Lung mechanics
� Hyperinflation– Obstructed small airways cause
premature airway closure, leading to air trapping and hyperinflation
� Hypoxemia– Inhomogeneous distribution of affected
areas results in V/Q mismatch, mostly shunt
Pathophysiology
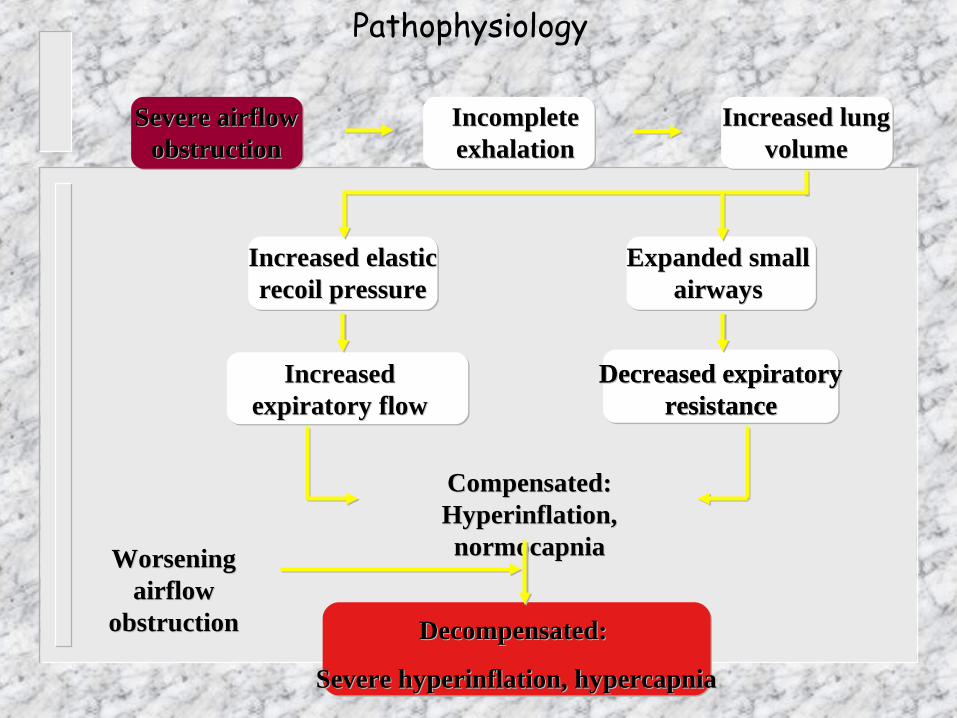
Severe airflow Severe airflow obstructionobstruction
Incomplete Incomplete exhalationexhalation
Increased lung Increased lung volumevolume
Increased elastic Increased elastic recoil pressurerecoil pressure
Increased Increased expiratory flowexpiratory flow
Expanded small Expanded small airwaysairways
Decreased expiratory Decreased expiratory resistanceresistance
Compensated:Compensated:Hyperinflation, Hyperinflation, normocapnianormocapnia
Decreased expiratory Decreased expiratory resistanceresistance
Decompensated: Decompensated:
Severe hyperinflation, hypercapniaSevere hyperinflation, hypercapnia
Worsening Worsening airflow airflow
obstructionobstruction
Pathophysiology
Cardiopulmonary interactions
� Left ventricular load– Spontaneously breathing children
with severe asthma have negative intrapleural pressure (as low as -35 cmH2O) during almost the entire respiratory cycle
– Negative intrapleural pressure causes increased left ventricular afterload, resulting in risk for pulmonary edema
Pathophysiology
Cardiopulmonary interactions� Right ventricular load
– Hypoxic pulmonary vasoconstriction and lung hyperinflation lead to increased right ventricular afterload
Pathophysiology
Cardiopulmonary interactions
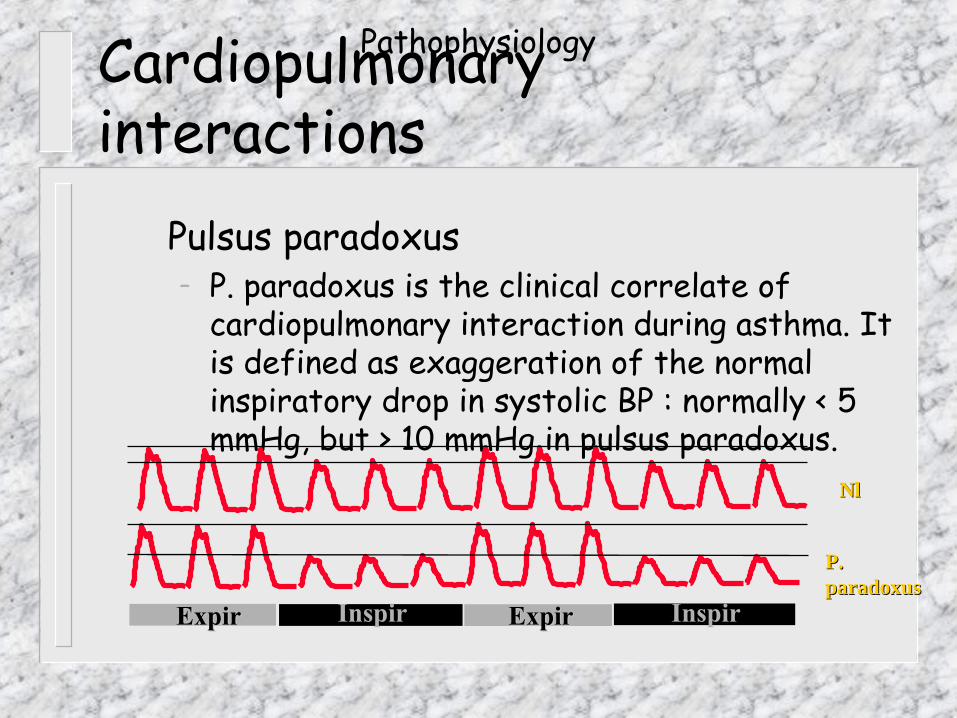
� Pulsus paradoxus– P. paradoxus is the clinical correlate of
cardiopulmonary interaction during asthma. It is defined as exaggeration of the normal inspiratory drop in systolic BP : normally < 5 mmHg, but > 10 mmHg in pulsus paradoxus.
ExpirExpir Inspir
NlNl
P. P. paradoxusparadoxus
InspirExpirExpir
Pathophysiology

Pulsus paradoxus correlates with severity
� All patients who presented with FEV1 of < 20% (of their best FEV1
while well) had pulsus paradoxus
Pathophysiology
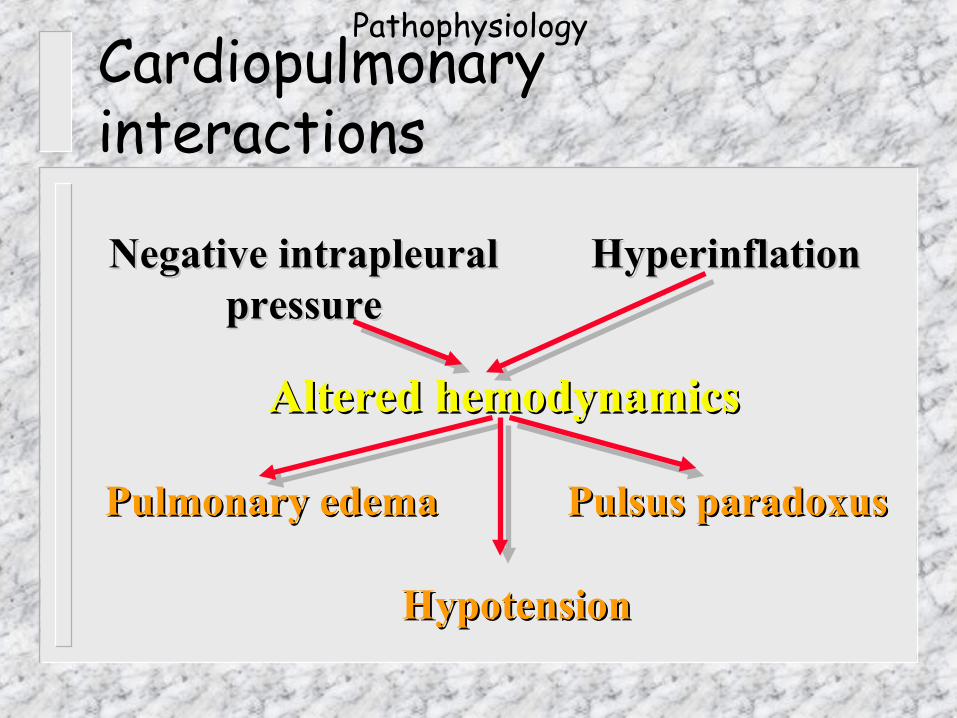
Cardiopulmonary interactions
Negative intrapleuralNegative intrapleuralpressurepressure
Pulmonary edemaPulmonary edema Pulsus paradoxusPulsus paradoxus
HyperinflationHyperinflation
HypotensionHypotension
Altered hemodynamicsAltered hemodynamics
Pathophysiology
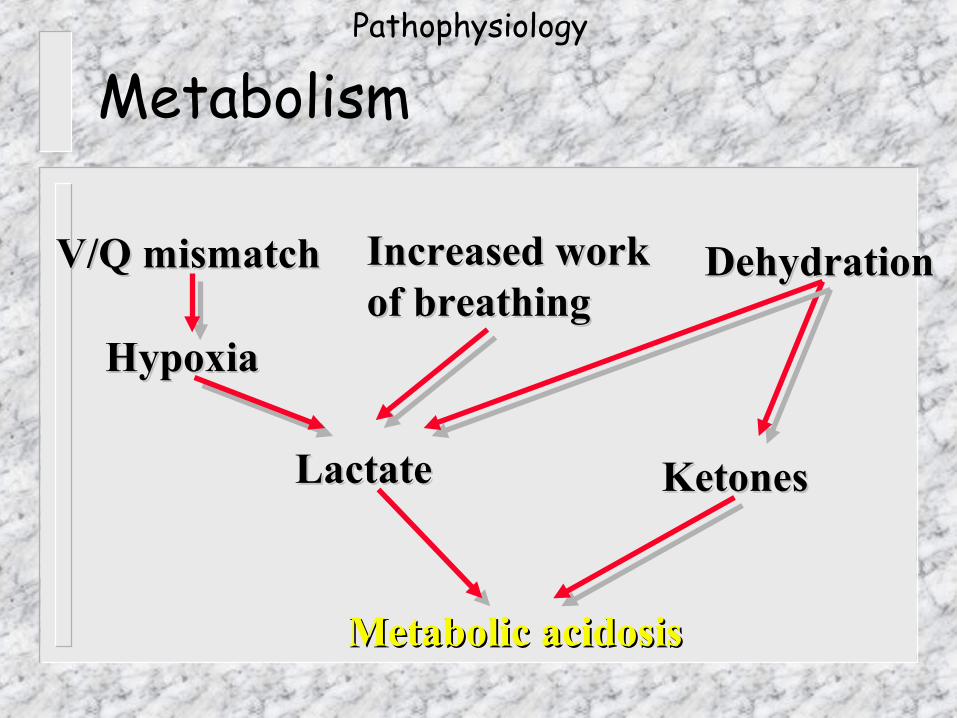
Metabolism
V/Q mismatchV/Q mismatch
HypoxiaHypoxia
DehydrationDehydration
LactateLactate KetonesKetones
Metabolic acidosisMetabolic acidosis
Increased workIncreased workof breathingof breathing
Pathophysiology
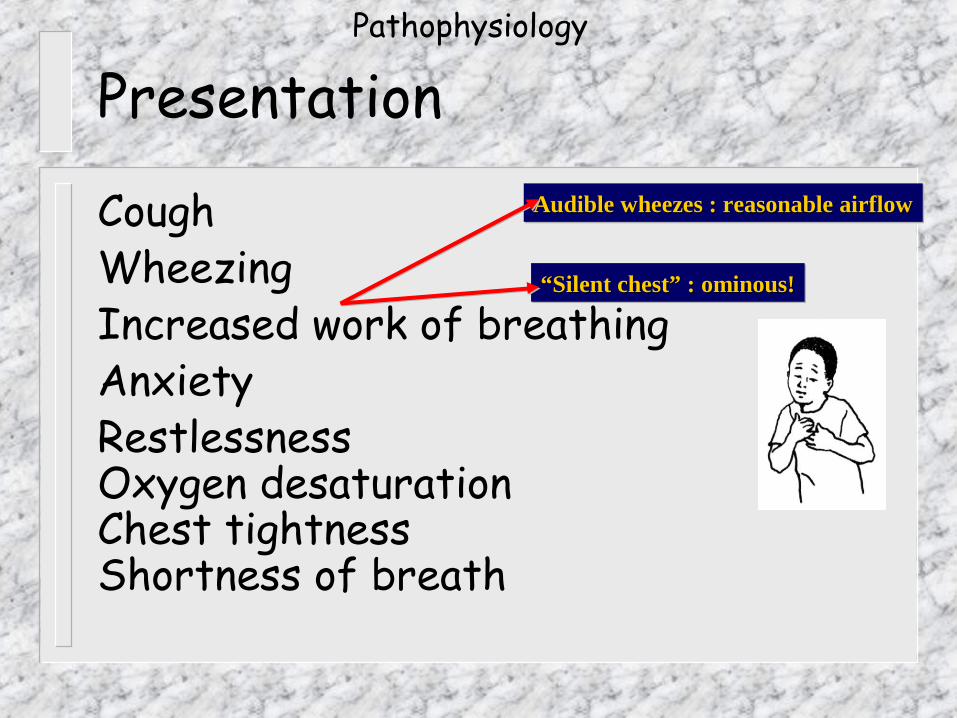
Presentation
Cough Wheezing Increased work of breathingAnxiety RestlessnessOxygen desaturation Chest tightnessShortness of breath
Audible wheezes : reasonable airflowAudible wheezes : reasonable airflowAudible wheezes : reasonable airflowAudible wheezes : reasonable airflow
““Silent chest” : ominous!Silent chest” : ominous!““Silent chest” : ominous!Silent chest” : ominous!
Pathophysiology
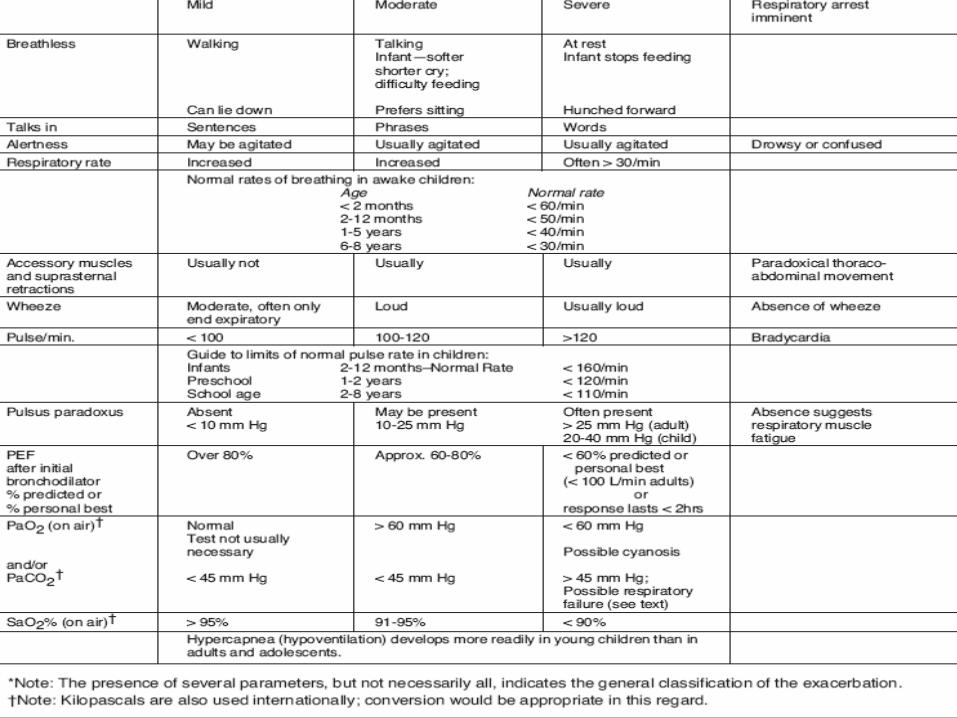
Assessment
� Findings consistent with impending respiratory failure:– Altered level of consciousness– Inability to speak– Absent breath sounds– Central cyanosis– Diaphoresis– Inability to lie down– Marked pulsus paradoxus
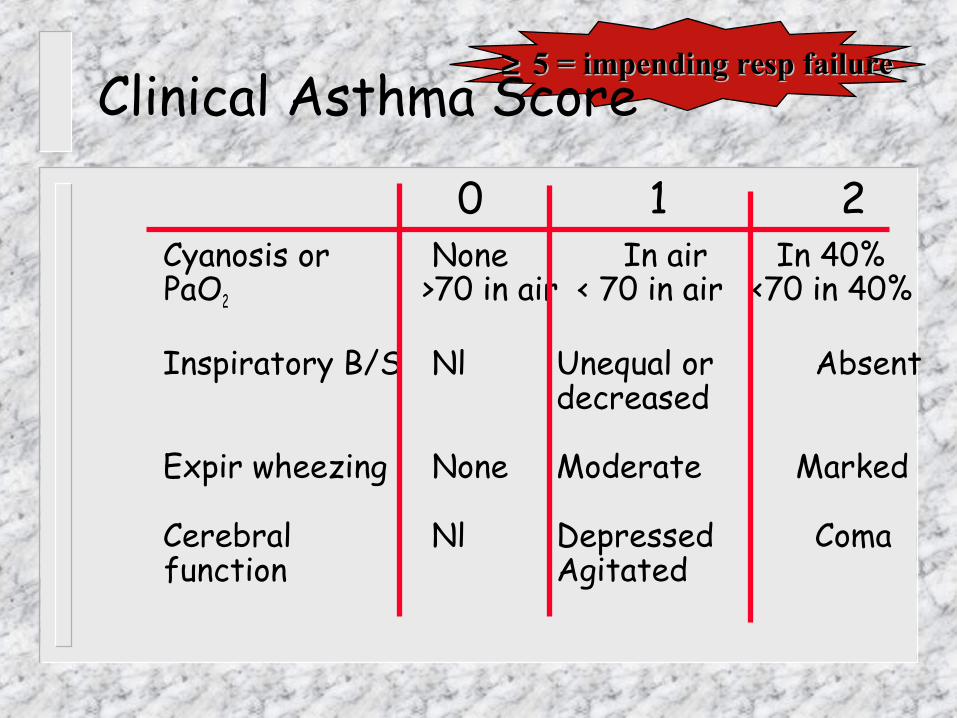
Clinical Asthma Score
0 1 2� Cyanosis or None In air In 40% PaO2 >70 in air < 70 in air <70 in 40%
� Inspiratory B/S Nl Unequal or Absent decreased
� Expir wheezing None Moderate Marked
� Cerebral Nl Depressed Coma function Agitated
≥ ≥ 5 = impending resp failure5 = impending resp failure
Chest X-Ray
– Not routinely indicated– Exceptions:
� Patient is intubated/ventilated� Suspected barotrauma� Suspected pneumonia� Other causes for wheezing are being
suspected
Assessment
ABG
– Early status asthmaticus: hypoxemia, hypocarbia
– Late: hypercarbia– Decision to intubate should not depend
on ABG, but on clinical assessment– Frequent ABGs are crucial in the
ventilated asthmatic
Assessment
Differential Diagnosis of wheezing� Bronchiolitis � Pneumonia-viral, bacterial, atypical � Congenital abnormalities: larnygotrachelmalacia, vocal cord
paralysis, tracheal or bronchial stenosis, gastro-esophageal reflux, vascular ring.
� Enlarged lymph nodes from infection or tumor � Foreign bodies in trachea, bronchus, or esophagus � Cystic Fibrosis � Aspergillus � Anaphylaxis � Toxic fume exposure

Oxygen
� Deliver high flow oxygen, as severe asthma causes V/Q mismatch (shunt)
� Oxygen will not suppress respiratory drive in children with asthma
Treatment

Fluid
� Judicious use of IV fluid necessary– Most asthmatics are dehydrated on
presentations - rehydrate to euvolemia– Overhydration may lead to pulmonary
edema– SIADH may be common in severe asthma
Treatment
Antibiotics
� Most infections precipitating asthma are viral
� Antibiotics are not routinely indicated
??
Treatment
ß-Agonists
� ß-receptor agonists stimulate ß2-receptors on bronchial smooth muscle and mediate muscle relaxation
� Epinephrine� Isoproterenol� Terbutaline� Albuterol
Relatively ßRelatively ß22 selective selective
Significant ßSignificant ß11 cardiovascular cardiovascular effectseffects
Treatment
ß-Agonists
� Less than 10% of nebulized drug reach the lung under ideal conditions
� Drug delivery depends on– Breathing pattern– Tidal volume– Nebulizer type and gas flow
Treatment
ß -Agonists
� Delivery of nebulized drug– Only particles between
0.8 - 3 mm are deposited in alveoli
– Correct gas flow rate is crucial
– Most devices require 10-12 L/min gas flow to generate correct particle size
Treatment
•ß -Agonists
� Continuous nebulization superior to intermittent nebulization –More rapid improvement–More cost effective–More patient friendly
Treatment
ß -Agonists
� Dosage– Intermittent nebulization
� O.1-2.5mg (0.5% solution), dilute with NS to 3 ml
� High dose: use up to undiluted 0.5% solution– Continuous nebulization
� 0.5mg/kg/hr� High dose: up to undiluted 5% solution (≈ 150
mg/hr)
Treatment
ß -Agonists
� Intravenous ß - Agonist– Consider for patients with severe air
flow limitation who remain unresponsive to nebulized albuterol
– Terbutaline is i.v. ß-agonist of choice – Loading dosage :10mcg/kg in 10 min– Maintenance Dosage: 0.5 – 5.0
mcg/kg/min
Treatment
ß -Agonists
� Side effects� Tachycardia� Agitation, tremor� Hypokalemia
Treatment
ß -Agonists
� Cardiac side effects– Myocardial ischemia known to occur with
i.v. isoproterenol– No significant cardiovascular toxicity
with i.v. terbutaline (prospective study in children with severe asthma)
– Tachycardia (and tremor) show tachyphylaxis, bronchodilation does not
Treatment

Steroids
� Asthma is an inflammatory disease
� Steroids are a mandatory element of first line therapy regimen (few exceptions only)
Treatment
Steroids
� Hydrocortisone 4-8 mg/kg x 1, then 2-4 mg/kg q 6°� Methylprednisolone 2 mg/kg x1, then 0.5-1 mg/kg q 4-6°
Treatment
Steroids� Significant side effects
– Hyperglycemia– Hypertension – Acute psychosis– Unusual or unusually severe
infections� Steroids contraindicated with
active or recent exposure to chickenpox
– Allergic reaction� Reported with
methylprednisolone, hydrocortisone and prednisone*
Treatment
Anticholinergics - Ipratropium
� Quaternary atropine derivative� Not absorbed systemically� Thus minimal cardiac effects� (may find a fixed/dilated pupil if the nebulizer mask slips
over an eye!)
Treatment
Anticholinergics
� Change in FEV1 is significantly greater when ipratropium was added to ß-agonists (199 adults)� Highly significant improvement in pulmonary function when ipratropium was added to albuterol (128 children). Sickest asthmatics experienced greatest improvement
Treatment
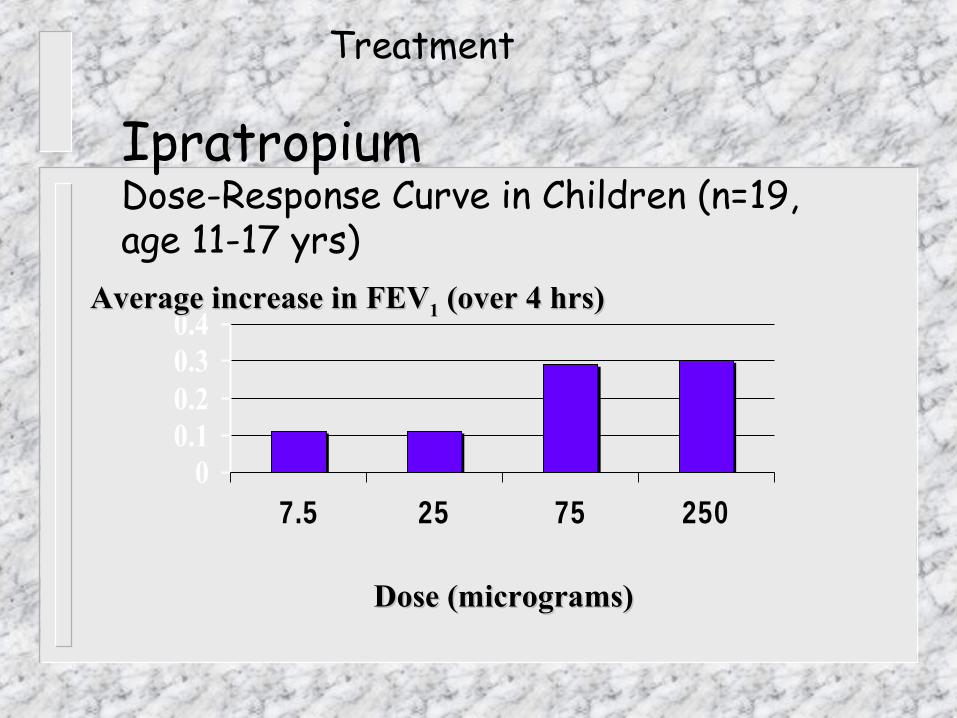
IpratropiumDose-Response Curve in Children (n=19, age 11-17 yrs)
00.10.20.30.4
7.5 25 75 250
Dose (micrograms)Dose (micrograms)
Average increase in FEVAverage increase in FEV11 (over 4 hrs) (over 4 hrs)
Treatment
Ipratropium
� Nebulize 250 - 500 mg every 6 hours
Treatment
Intubation, Ventilation
� Absolute indications:– Cardiac or respiratory arrest– Severe hypoxia– Rapid deterioration in mental state
– Respiratory acidosis does not dictate intubation
Treatment

Why hesitate to intubate the asthmatic child?
� Tracheal foreign body aggravates bronchospasm
� Positive pressure ventilation increases risk of barotrauma and hypotension
� > 50% of morbidity/mortality during severe asthma occurs during or immediately after intubation
Treatment
Intubation
� Preoxygenate, decompress stomach� Sedate (consider ketamine)� Neuromuscular blockade (may avoid
large swings in airway/pleural pressure)
� Rapid orotracheal intubation (consider cuffed tube)
Treatment
Immediately after intubation� Expect hypotension, circulatory
depression� Allow long expiratory time� Avoid overzealous manual breaths� Consider volume administration� Consider pneumothorax� Consider endotracheal tube
obstruction (++ secretions)
Treatment
Mechanical ventilation
� Positive pressure ventilation worsens hyperinflation/risk of barotrauma
� Thoughtful strategies include:– Pressure-limited ventilation, TV 8-12
ml/kg, short Ti, rate 8-12/min (permissive hypercapnia)
– Pressure support ventilation using PS=20-30 cmH2O (may decrease hyperinflation by allowing active exhalation)
Treatment

Ketamine
� Dissociative anesthetic with strong analgesic effect
� Direct bronchodilating action� Useful for induction (2 mg/kg i.v.) as
well as continuous infusion (0.5 - 2 mg/kg/hr)
� Induces bronchorrhea, emergence reaction
Treatment
Inhalational anesthetics
� Halothane, isoflurane have bronchodilating effect
� Halothane may cause hypotension, dysrhythmia
� Requires scavenging system, continuous gas analysis
Treatment
Theophylline
� Role in children with severe asthma remains controversial
� Narrow therapeutic range� High risk of serious adverse effects� Mechanism of effect in asthma
remains unclear
Treatment

– Loading Dosage :6-7mg/kg – Maintenance Dosage; as per age– 6wk-6mth :0.5mg/kg/hr– 6mth-1yr : 0.7mg/kg/hr– 1yr-9yr : 1mg/kg/hr– 9yr-12yr : 0.9mg/kg/hr– 12yr-ad : 0.7mg/kg/hr
TheophyllineTreatment
Theophylline
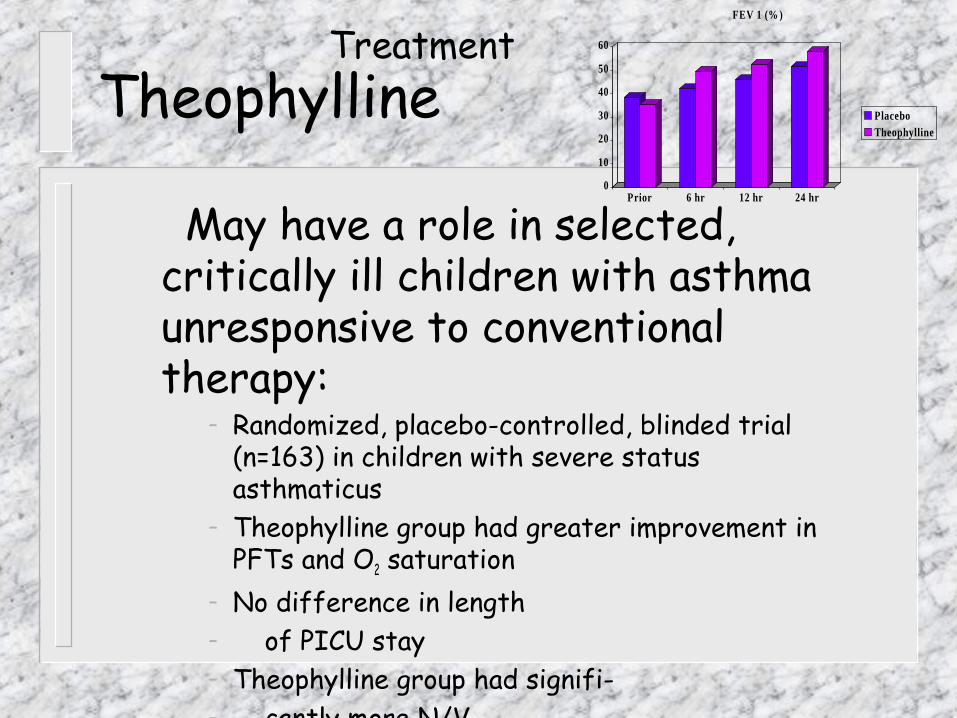
� May have a role in selected, critically ill children with asthma unresponsive to conventional therapy:
– Randomized, placebo-controlled, blinded trial (n=163) in children with severe status asthmaticus
– Theophylline group had greater improvement in PFTs and O2 saturation
– No difference in length – of PICU stay– Theophylline group had signifi-– cantly more N/V
0
10
20
30
40
50
60
Prior 6 hr 12 hr 24 hr
FEV 1 (% )
PlaceboTheophylline
Treatment

Magnesium
� Smooth-muscle relaxation by inhibition of calcium uptake (=bronchodilator)
� Dosage recommendation: 25 - 75 mg/kg i.v. over 20 minutes
Treatment
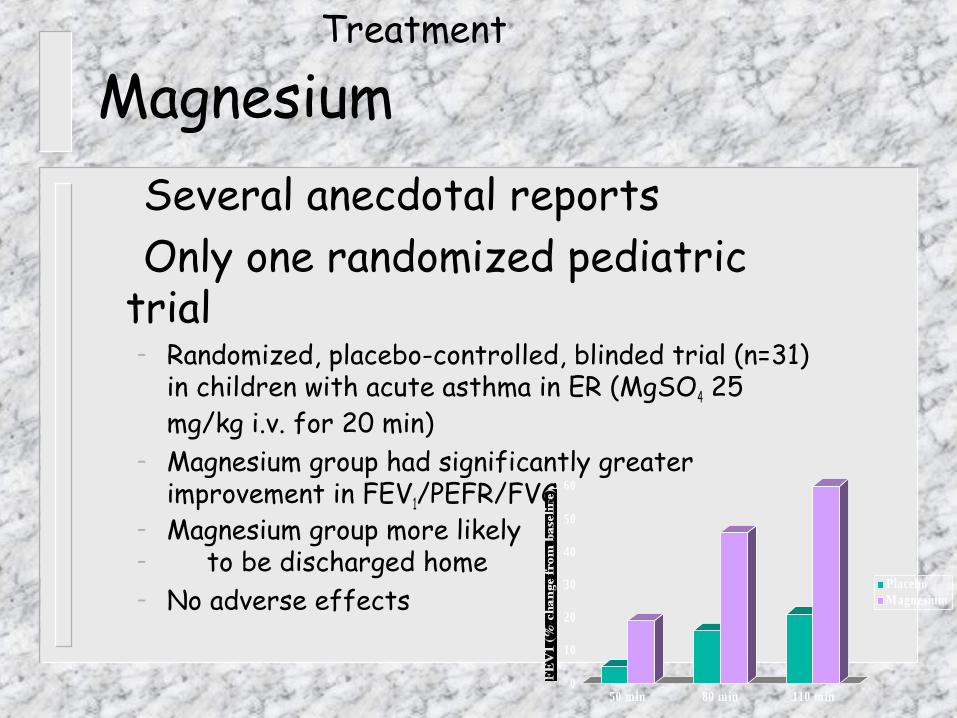
Magnesium � Several anecdotal reports� Only one randomized pediatric trial
– Randomized, placebo-controlled, blinded trial (n=31) in children with acute asthma in ER (MgSO4 25 mg/kg i.v. for 20 min)
– Magnesium group had significantly greater improvement in FEV1/PEFR/FVC
– Magnesium group more likely– to be discharged home– No adverse effects
0
10
20
30
40
50
60
50 min 80 min 110 min
PlaceboMagnesium
Treatment
Helium - Oxygen (Heliox)
� Helium lowers gas density (if at least 60% helium fraction)
� Reduces resistance during turbulent flow
� Renders turbulent flow less likely to occur
Treatment
Heliox
� Helium-oxygen (80:20) decreased pulsus paradoxus and increased PEFR in a controlled trial of adult patients
� Heliox may worsen dynamic hyperinflation
Treatment
Bronchoscopy, bronchial lavage� Marked mucus plugging may render
bronchodilating and anti-inflammatory therapy ineffective
� “Plastic bronchitis” has been described in asthmatic children
� Combined bronchoscopy/lavage has been used in desperately ill asthmatic children
Treatment

Summary� Severe asthma in children is increasing in
prevalence and mortality� Aggressive treatment with ß-agonist, steroids and
anticholinergic is warranted even in the sick-appearing child
� Avoid intubation if possible� Mechanical ventilation will worsen bronchospasm
and hyperinflation� Use low morbidity approach to mechanical
ventilation

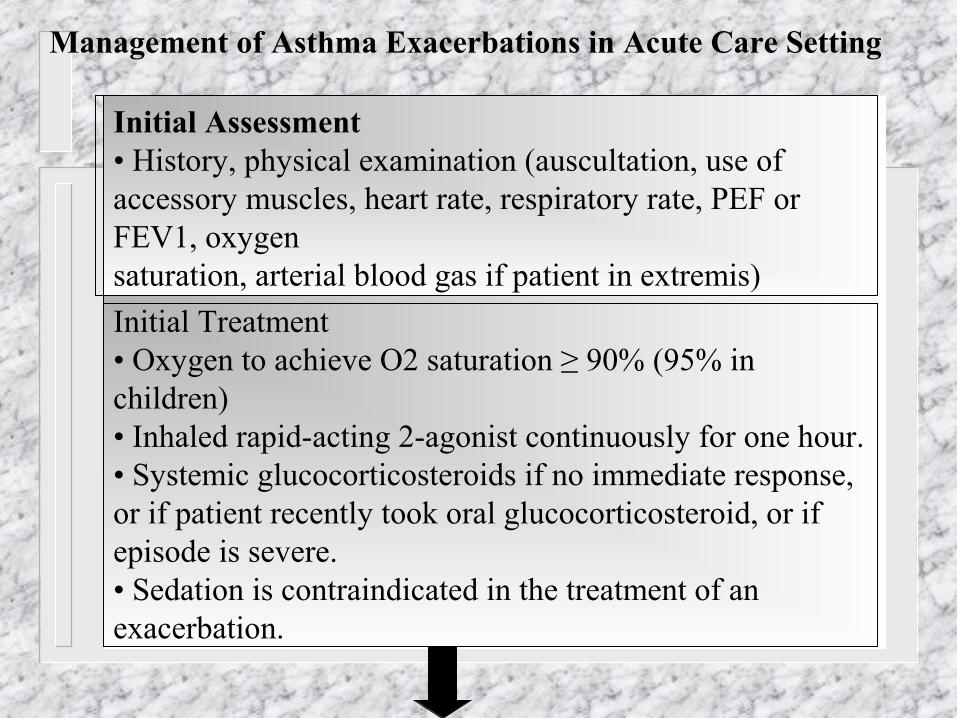
Management of Asthma Exacerbations in Acute Care Setting
Initial Assessment • History, physical examination (auscultation, use of accessory muscles, heart rate, respiratory rate, PEF or FEV1, oxygensaturation, arterial blood gas if patient in extremis)
Initial Treatment• Oxygen to achieve O2 saturation ≥ 90% (95% in children)• Inhaled rapid-acting 2-agonist continuously for one hour.• Systemic glucocorticosteroids if no immediate response, or if patient recently took oral glucocorticosteroid, or if episode is severe.• Sedation is contraindicated in the treatment of an exacerbation.
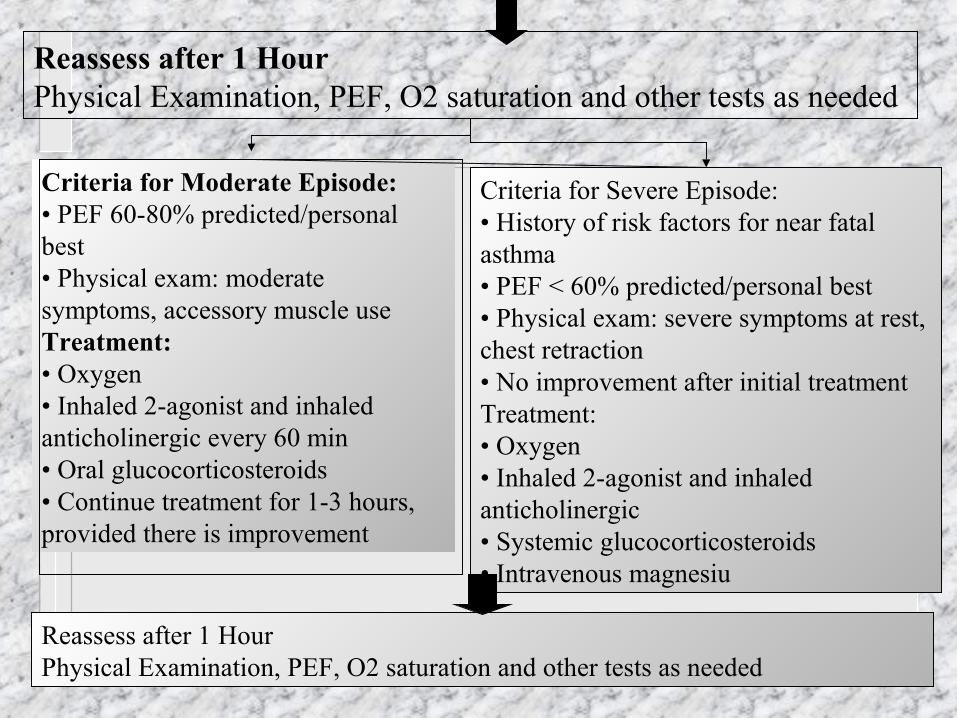
Reassess after 1 HourPhysical Examination, PEF, O2 saturation and other tests as needed
Criteria for Moderate Episode:• PEF 60-80% predicted/personal best• Physical exam: moderate symptoms, accessory muscle useTreatment:• Oxygen• Inhaled 2-agonist and inhaled anticholinergic every 60 min• Oral glucocorticosteroids• Continue treatment for 1-3 hours, provided there is improvement
Criteria for Severe Episode:• History of risk factors for near fatal asthma• PEF < 60% predicted/personal best• Physical exam: severe symptoms at rest, chest retraction• No improvement after initial treatmentTreatment:• Oxygen• Inhaled 2-agonist and inhaled anticholinergic• Systemic glucocorticosteroids• Intravenous magnesiu
Reassess after 1 HourPhysical Examination, PEF, O2 saturation and other tests as needed
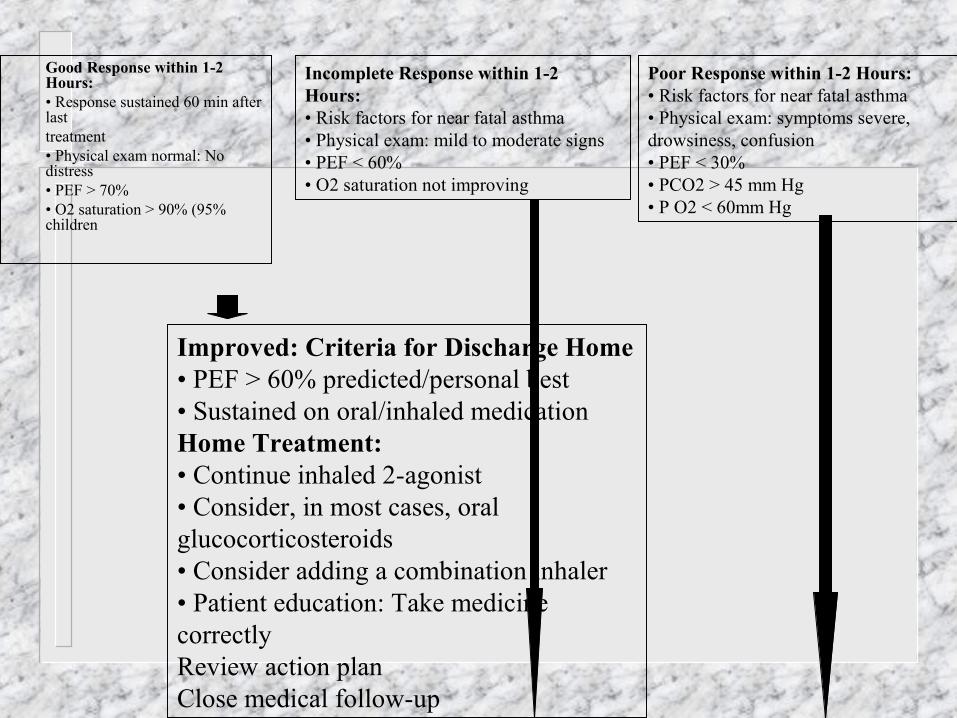
� Good Response within 1-2 Hours:
� • Response sustained 60 min after last
� treatment� • Physical exam normal: No
distress� • PEF > 70%� • O2 saturation > 90% (95%
children
Incomplete Response within 1-2Hours:• Risk factors for near fatal asthma• Physical exam: mild to moderate signs• PEF < 60%• O2 saturation not improving
Improved: Criteria for Discharge Home• PEF > 60% predicted/personal best• Sustained on oral/inhaled medicationHome Treatment:• Continue inhaled 2-agonist• Consider, in most cases, oral glucocorticosteroids• Consider adding a combination inhaler• Patient education: Take medicine correctlyReview action planClose medical follow-up
Poor Response within 1-2 Hours:• Risk factors for near fatal asthma• Physical exam: symptoms severe,drowsiness, confusion• PEF < 30%• PCO2 > 45 mm Hg• P O2 < 60mm Hg
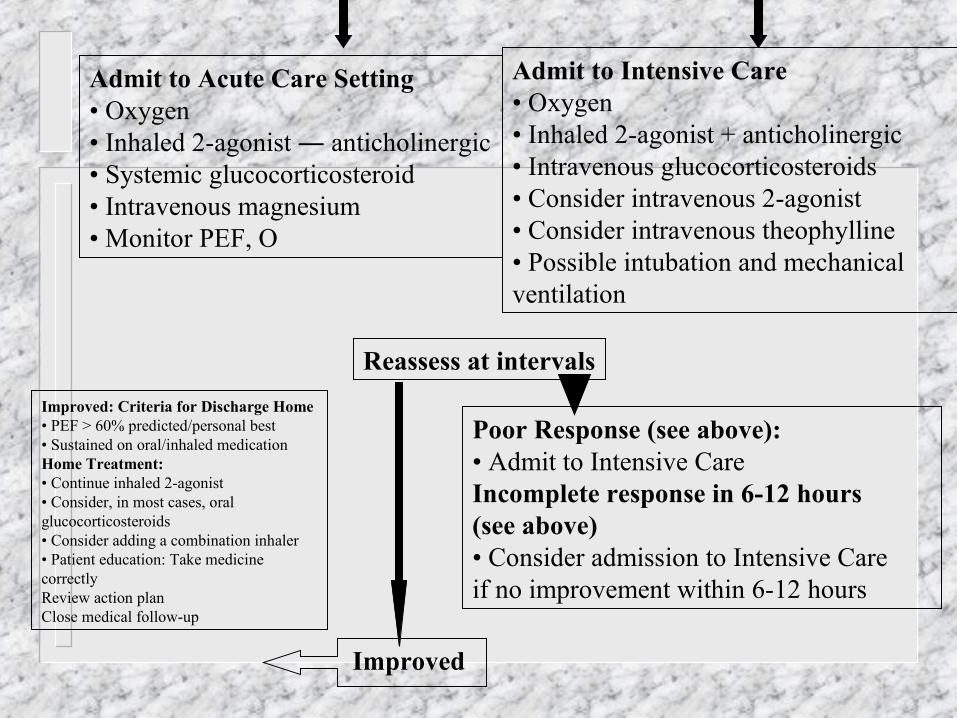
Admit to Acute Care Setting• Oxygen• Inhaled 2-agonist ― anticholinergic• Systemic glucocorticosteroid• Intravenous magnesium• Monitor PEF, O
Admit to Intensive Care• Oxygen• Inhaled 2-agonist + anticholinergic• Intravenous glucocorticosteroids• Consider intravenous 2-agonist• Consider intravenous theophylline• Possible intubation and mechanicalventilation
Reassess at intervals
Poor Response (see above):• Admit to Intensive CareIncomplete response in 6-12 hours(see above)• Consider admission to Intensive Careif no improvement within 6-12 hours
Improved: Criteria for Discharge Home• PEF > 60% predicted/personal best• Sustained on oral/inhaled medicationHome Treatment:• Continue inhaled 2-agonist• Consider, in most cases, oral glucocorticosteroids• Consider adding a combination inhaler• Patient education: Take medicine correctlyReview action planClose medical follow-up
Improved
