statins and cad prevention: rosuvastatin. rising burden of cvd in india (2005) lancet...
TRANSCRIPT

Statins and CAD Prevention:
Rosuvastatin

Rising burden of CVD in India (2005)
Lancet 2005;366:1744-9
Estimated proportions of total deaths and DALYs lost by cause in India (all ages, 2005)

CAD risk factors in Indians
0
10
20
30
40
50
60
36.9 38.8
29.3
59.05
30.97
18.0213.28
%
J Assoc Physicians India. 2004 Feb;52:103-8
Fraction of CAD patients with various risk factors (n=5748)
Dyslipidaemia is a major CVD risk factor in
Indians

Secondary Prevention
NCEP ATP 3. Circulation 2002; 106;3143
“NCEP-ATP III specifies an LDL cholesterol <100 mg/dL as the goal of therapy in
secondary prevention”
LDL-C is the primary target
“NCEP-ATP III identifies the sum of LDL+VLDL [termed non-HDL cholesterol (Total-CL minus HDL-CL)] <130
mg/dL as a secondary target of therapy in persons with high triglycerides (≥200 mg/dL)”
Non-HDL-C as the secondary target
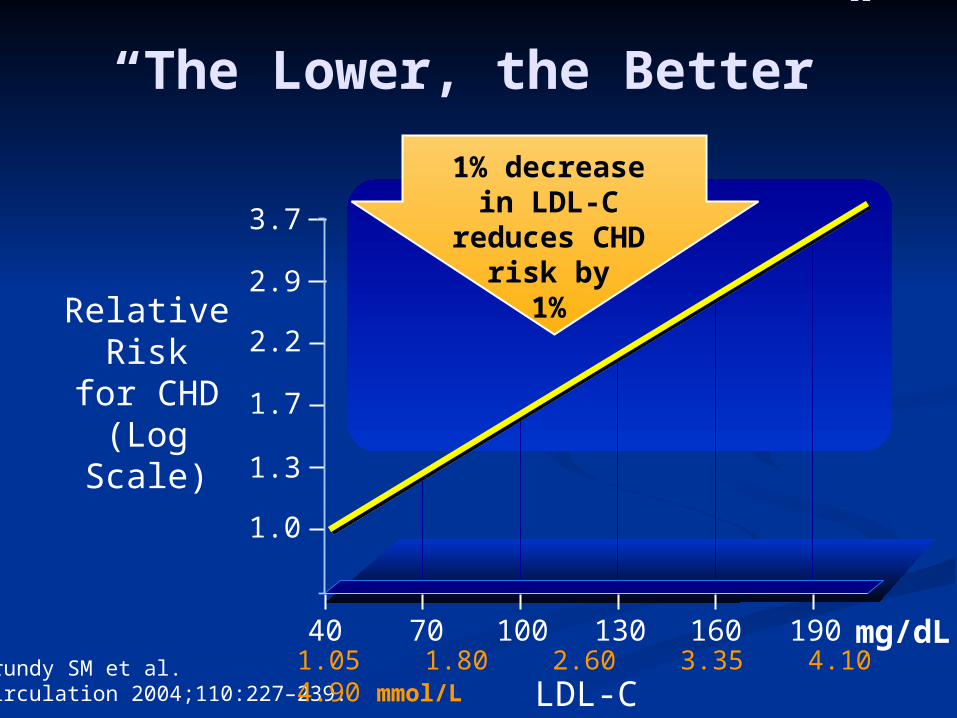
“The Lower, the Better”
RelativeRisk
for CHD (Log Scale)
3.7
2.9
2.2
1.7
1.3
1.0
LDL-C
40 70 100 130 160 190
0
1
Grundy SM et al. Circulation 2004;110:227–239.
mg/dL1.05 1.80 2.60 3.35 4.10 4.90 mmol/L
1% decreasein LDL-C reduces
CHD risk by1%
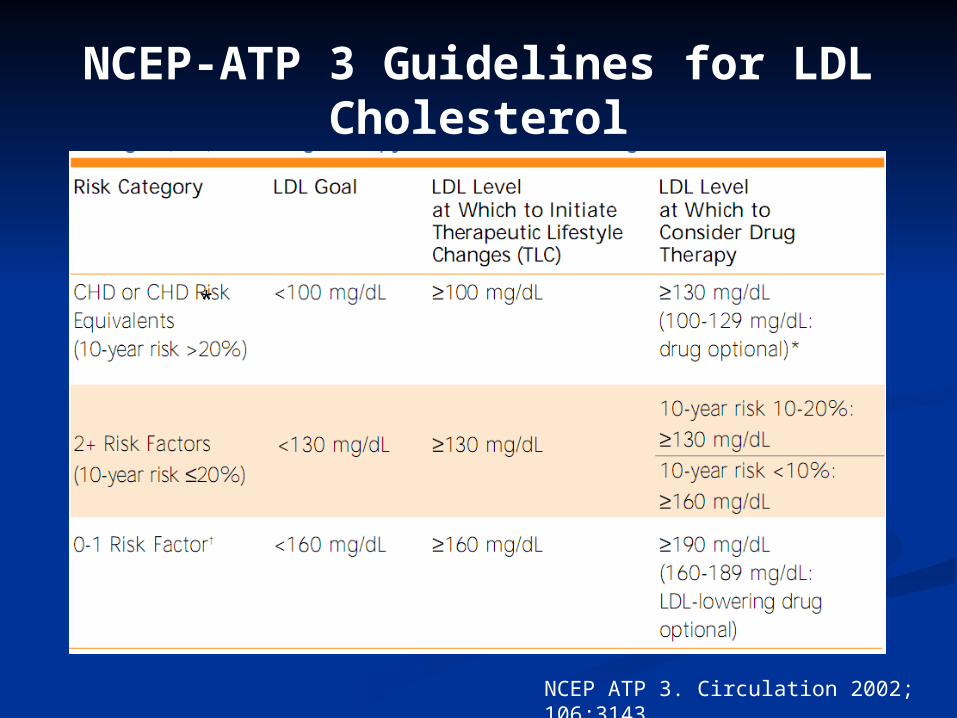
NCEP-ATP 3 Guidelines for LDL Cholesterol
NCEP ATP 3. Circulation 2002; 106;3143
*
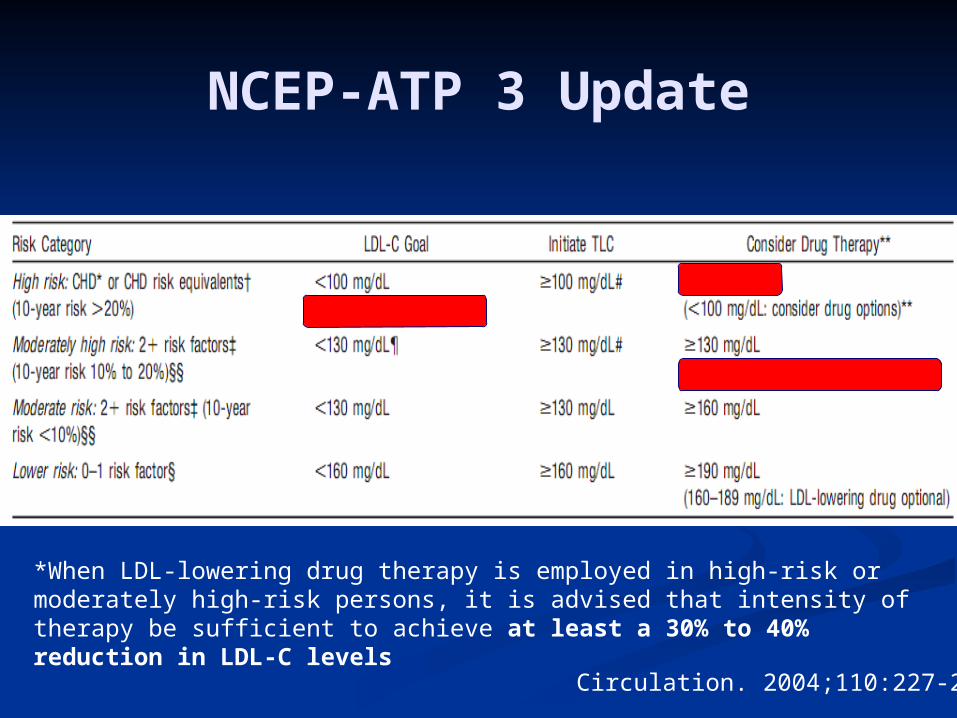
NCEP-ATP 3 Update
Circulation. 2004;110:227-239
*When LDL-lowering drug therapy is employed in high-risk or moderately high-risk persons, it is advised that intensity of therapy be sufficient to achieve at least a 30% to 40% reduction in LDL-C levels
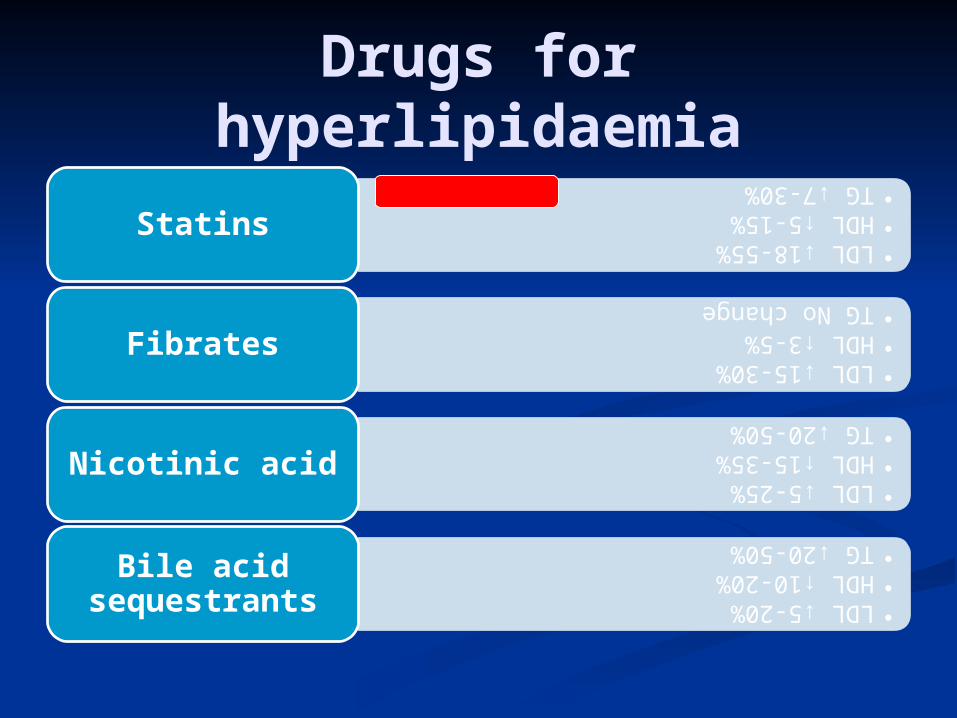
Drugs for hyperlipidaemia
•LDL ↓18-55%
•HDL ↑5-15%
•TG ↓7-30%
Statins
•LDL ↓15-30%
•HDL ↑3-5%
•TG No change
Fibrates
•LDL ↓5-25%
•HDL ↑15-35%
•TG ↓20-50%
Nicotinic acid
•LDL ↓5-20%
•HDL ↑10-20%
•TG ↓20-50%
Bile acid sequestrants

LDL-C goal: an unmet need
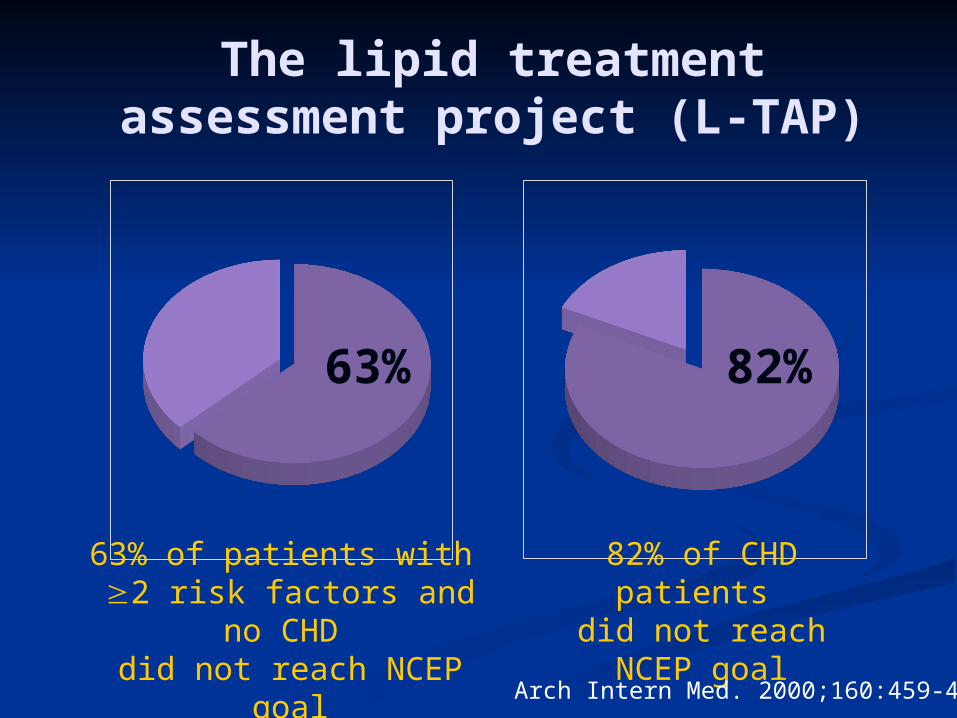
The lipid treatment assessment project (L-TAP)
63% of patients with 2 risk factors and no CHD
did not reach NCEP goal
63% 82%
82% of CHD patients did not reach NCEP
goal
Arch Intern Med. 2000;160:459-467

Many Patients With CHD Fail to Achieve LDL-C and Non-HDL-C Goals Even With
Dose Titration
LDL-C Non-HDL-C0
10
20
30
40
50
60
70
80
90
100Atorvastatin 10 - 80 mg
Simvastatin 10 - 40 mg
Lovastatin 20 - 80 mg
Fluvastatin 20 - 80 mg
Pravastatin 10 - 40 mg
Pat
ien
ts, %
at
go
al
ACCESS STUDY. Ballantyne CM, et al. Am J Cardiol. 2001;88:265-269
n = 2,543†
At Wk 54
GAP
Reasons for the unmet gap
Variations in drug potency
Drug interactions
Variations in drug tolerability
affecting compliance

Rosuvastatin
“Superstatin”

Statins: Comparison of standard doses
† For every doubling of the dose above standard dose, an approximate 6% decrease in LDL-C level can be obtained
Circulation. 2004;110:227-239
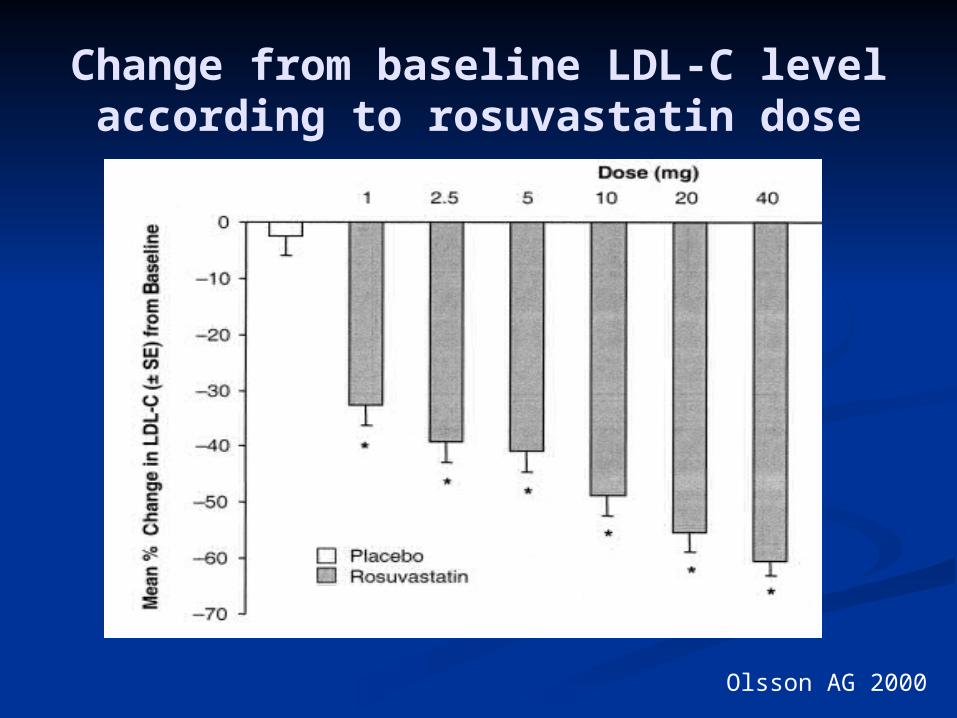
Change from baseline LDL-C level according to rosuvastatin dose
Olsson AG 2000

LDL-C: % Change From Baseline at week 6
Rosuvastatin 10 to 40 mg vs Comparators
-45.87
-52.34-54.96
-36.73
-42.57-47.79
-51.05
-20.13-24.29
-29.67-28.3
-34.98-38.81
-45.78
-70
-60
-50
-40
-30
-20
-10
010 20 40 80
Dose, mg
% c
ha
ng
e f
rom
ba
se
lin
e
Rosuvastatin (n = 156 - 160)Atorvastatin (n = 158 - 165)Pravastatin (n = 158 - 165)Simvastatin (n = 161 - 164)
P <0.001 vs comparators on a mg-to-mg basis. Data presented as means.
http://www.fda.gov/OHRMS/DOCKETS/ac/03/slides/3968S1_01_B-AstraZeneca-Efficacy.ppt#14
STELLAR Study. Am J Cardiol 2003;92:152–160)

Rosuvastatin
“Less drug interactions”
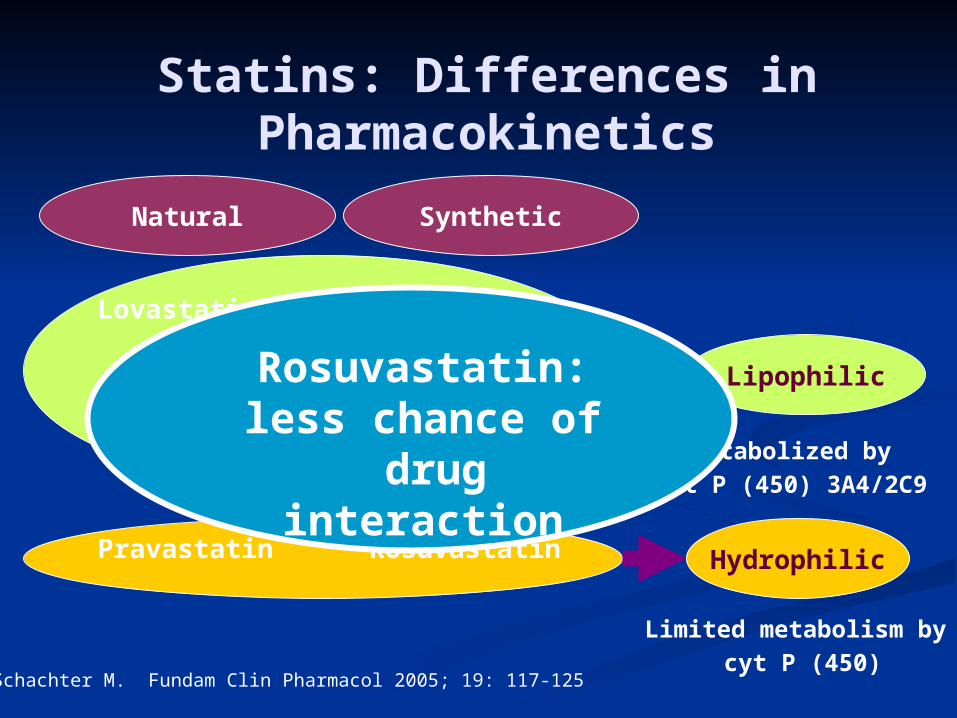
Statins: Differences in Pharmacokinetics
Natural Synthetic
Lovastatin
Simvastatin
Pravastatin
Atorvastatin
Fluvastatin
Rosuvastatin
Lipophilic
Hydrophilic
Metabolized bycyt P (450) 3A4/2C9
Limited metabolism by cyt P (450)
Schachter M. Fundam Clin Pharmacol 2005; 19: 117-125
Rosuvastatin: less chance of
drug interaction
Rosuvastatin
“Ease of administration”
Longer half-life
Hepatic cholesterol synthesis is maximal between midnight and 2:00 A.M
Most statins attain peak plasma concentrations 1-4 hours after oral administration and have a half-life of 1-4 hours requiring them to be administered in the evening
Rosuvastatin has a long half-life like atorvastatin (approximately 20 hrs) which permits it to be administered any time in a day

Rosuvastatin“Effects on other atherogenic lipid
parameters”

Effect on total cholesterol
-33
-27-25
-19
-35
-30
-25
-20
-15
-10
-5
0
Mean
% c
han
ge i
n T
C f
rom
b
ase
lin
e
** p<0.001 vs. other statins
Rosuvastatin 10mg
Atorvastatin 10mg
Simvastatin 20mg
Pravastatin 20mg
n=389 n=393 n=249 n=252
Coron Artery Dis 2004;15:115-23.

Effect on triglycerides
-19-18
-12 -12
-20
-18
-16
-14
-12
-10
-8
-6
-4
-2
0
Mean
% c
han
ge i
n T
G f
rom
b
ase
lin
e
** p<0.001 vs. simvastatin & pravastatin
Rosuvastatin 10mg
Atorvastatin 10mg
Simvastatin 20mg
Pravastatin 20mg
n=389 n=393 n=249 n=252
Am J Cardiol 2003;91(Suppl):3C-10C.
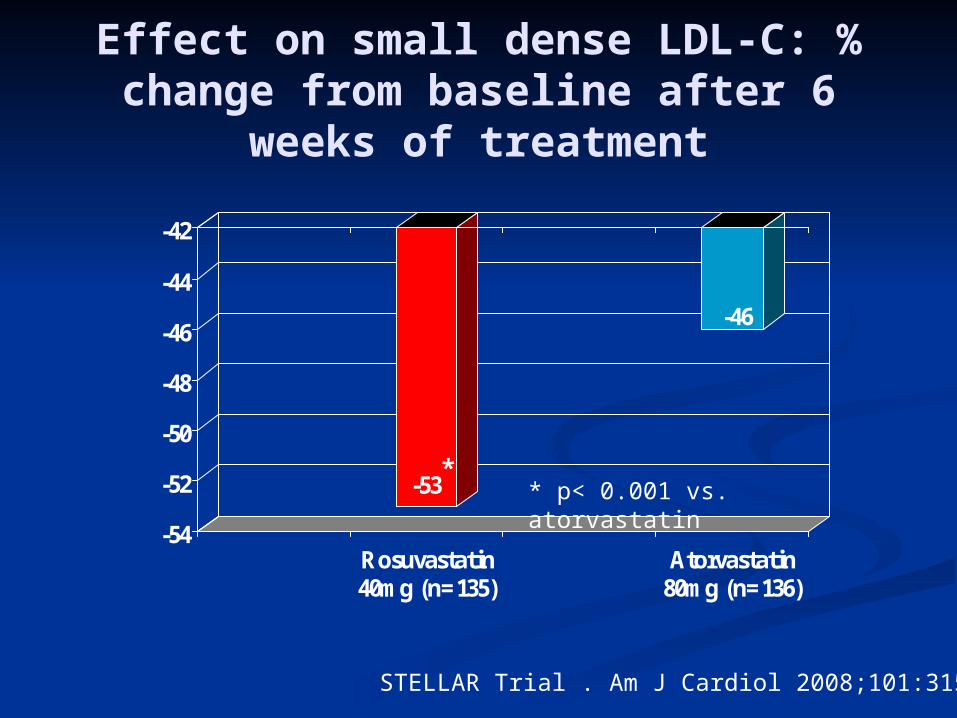
Effect on small dense LDL-C: % change from baseline after 6
weeks of treatment
-53
-46
-54
-52
-50
-48
-46
-44
-42
Rosuvastatin40mg (n=135)
Atorvastatin80mg (n=136)
** p< 0.001 vs. atorvastatin
STELLAR Trial . Am J Cardiol 2008;101:315–318.

Effect on HDL-C: % Change From Baselineat week 6
9.69.5
7.7
2.1
4.44.85.7 5.6
4.53.2
6.8
5.26.0
5.3
0
2
4
6
8
10
12
10 20 40 10 20 40 80 10 20 40 10 20 40 80
Treatment, mg
% c
ha
ng
e f
rom
ba
se
lin
e
Rosuvastatin Atorvastatin
Pravastatin Simvastatin
P < .002 RSV 10 mg vs PRA 10 mg. P < .002 RSV 20 mg vs ATV 20 mg, 40 mg, 80 mg; PRA 20 mg, 40 mg; SIM 40 mg.P < .002 RSV 40 mg vs ATV 40 mg, 80 mg; PRA 40 mg; SIM 40 mg.Data presented as LS means ± SE.
N = 156 160 157 158 155 156 165 160 164 161 165 162 158 163
STELLAR Study. Am J Cardiol 2003;92:152–160)
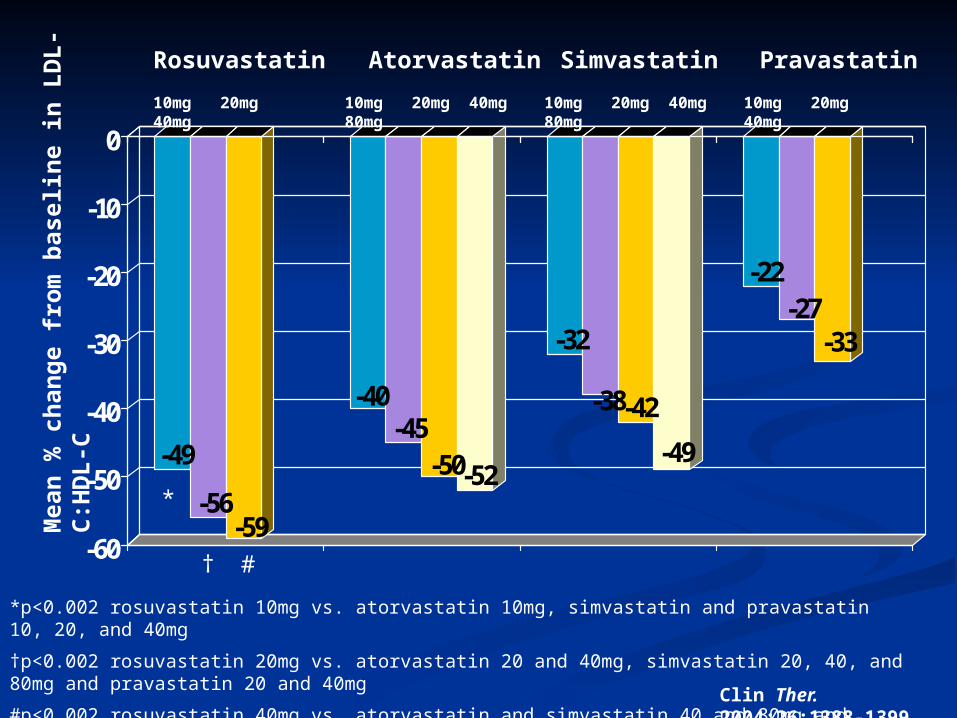
-49
-56-59
-40-45
-50-52
-32
-38-42
-49
-22-27
-33
-60
-50
-40
-30
-20
-10
010mg 20mg 40mg
10mg 20mg 40mg 80mg
10mg 20mg 40mg 80mg
10mg 20mg 40mg
Rosuvastatin Atorvastatin Simvastatin PravastatinM
ean
% c
han
ge f
rom
base
lin
e i
n L
DL
-C
:HD
L-C
*
† #
*p<0.002 rosuvastatin 10mg vs. atorvastatin 10mg, simvastatin and pravastatin 10, 20, and 40mg
†p<0.002 rosuvastatin 20mg vs. atorvastatin 20 and 40mg, simvastatin 20, 40, and 80mg and pravastatin 20 and 40mg
#p<0.002 rosuvastatin 40mg vs. atorvastatin and simvastatin 40 and 80mg and pravastatin 40mg
Clin Ther. 2004;26:1388-1399
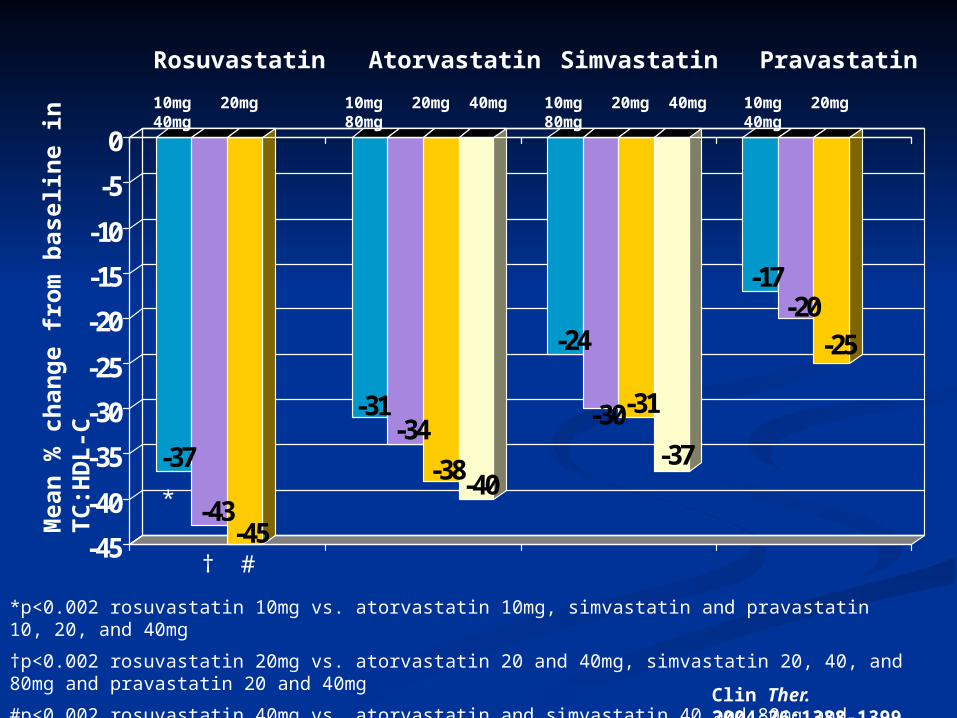
-37
-43-45
-31-34
-38-40
-24
-30-31
-37
-17-20
-25
-45
-40
-35
-30
-25
-20
-15
-10
-5
010mg 20mg 40mg
10mg 20mg 40mg 80mg
10mg 20mg 40mg 80mg
10mg 20mg 40mg
Rosuvastatin Atorvastatin Simvastatin PravastatinM
ean
% c
han
ge f
rom
base
lin
e i
n
TC
:HD
L-C
*
† #
*p<0.002 rosuvastatin 10mg vs. atorvastatin 10mg, simvastatin and pravastatin 10, 20, and 40mg
†p<0.002 rosuvastatin 20mg vs. atorvastatin 20 and 40mg, simvastatin 20, 40, and 80mg and pravastatin 20 and 40mg
#p<0.002 rosuvastatin 40mg vs. atorvastatin and simvastatin 40 and 80mg and pravastatin 40mg
Clin Ther. 2004;26:1388-1399

-46
-52-55
-38-42
-47-48
-29
-36-38
-45
-21-25
-31
-60
-50
-40
-30
-20
-10
010mg 20mg 40mg
10mg 20mg 40mg 80mg
10mg 20mg 40mg 80mg
10mg 20mg 40mg
Rosuvastatin Atorvastatin Simvastatin PravastatinM
ean
% c
han
ge f
rom
base
lin
e i
n N
on
H
DL
-C:H
DL
-C
*
† #
*p<0.002 rosuvastatin 10mg vs. atorvastatin 10mg, simvastatin and pravastatin 10, 20, and 40mg
†p<0.002 rosuvastatin 20mg vs. atorvastatin 20 and 40mg, simvastatin 20, 40, and 80mg and pravastatin 20 and 40mg
#p<0.002 rosuvastatin 40mg vs. atorvastatin and simvastatin 40 and 80mg and pravastatin 40mg
Clin Ther. 2004;26:1388-1399

-41
-46-48
-32
-38-41-42
-26
-30-35
-39
-17
-24-27
-50-45
-40-35
-30-25-20
-15-10
-50
10mg 20mg 40mg
10mg 20mg 40mg 80mg
10mg 20mg 40mg 80mg
10mg 20mg 40mg
Rosuvastatin Atorvastatin Simvastatin PravastatinM
ean
% c
han
ge f
rom
base
lin
e i
n
Ap
oB
:Ap
oA
-1
*
† #
*p<0.002 rosuvastatin 10mg vs. atorvastatin 10mg, simvastatin and pravastatin 10, 20, and 40mg
†p<0.002 rosuvastatin 20mg vs. atorvastatin 20, simvastatin 20, 40, and 80mg and pravastatin 20 and 40mg
#p<0.002 rosuvastatin 40mg vs. atorvastatin and simvastatin 40 and 80mg and pravastatin 40mg
Clin Ther. 2004;26:1388-1399
Rosuvastatin
“Clinical implications”
Earlier achievement of targets
POLARIS study. Atherosclerosis 194 (2007) e154–e164

-0.0014
0.0131
-0.005
0.000
0.005
0.010
0.015• 984 asymptomatic
patients with moderately elevated cholesterol and low risk of CVD acc to NCEP-ATP 3 criteria
• Rosuvastatin 40mg (n=702) Vs Placebo (n=282) for 2 years
Cha
nge
in C
IMT
for
12
Car
otid
Art
ery
site
s (m
m/y
ear)
Change in CIMTChange in CIMT
n = 702
n = 282
p < 0.001
METEOR Trial. ACC 2007METEOR Trial. ACC 2007
Rosuvastatin
Placebo

ASTEROID: Effect on atheroma volume measured by IVUS
Mean % atheroma volume (N = 349)
39.6 38.6
0
35
40
45
50
Baseline 24 months
Mean atheroma volume in most diseased segment
(n = 319)
65.159
0
60
70
80
90
100
Baseline 24 months
Nissen SE et al. JAMA. 2006;295:1556-65.
mm3
P < 0.001 P < 0.001
%
Primary Prevention With LDL-Lowering Therapy
Reduced intakes of saturated fat and
cholesterol
Increased physical activity
Weight control
Statins

JUPITER trial
Justification for the Use of Statins in Primary Prevention: An Intervention Trial Evaluating
RosuvastatinRidker et al, N Engl J Med 2008

JUPITERMulti-National Randomized Double Blind Placebo
Controlled Trial of Rosuvastatin in the Prevention of Cardiovascular
EventsAmong Individuals With Low LDL and Elevated
hsCRP
Ridker et al, Circulation 2003;108:2292-2297.
JUPITERTrial Design
Rosuvastatin 20 mg (N=8901) MIStroke
Unstable Angina
CVD DeathCABG/PTCA
4-week run-in
No Prior CVD or DMMen >50, Women >60
LDL <130 mg/dL hsCRP >2 mg/L
Placebo (N=8901)
0
1
2
3
4
5
hsC
RP
(m
g/L
)
0
20
40
60
80
100
120
140
LD
L (
mg
/dL
)
Months0 12 24 36 48
0
10
20
30
40
50
60
0
20
40
60
80
100
120
140
0 12 24 36 48
TG
(m
g/d
L)
HD
L (
mg
/dL
)
Months
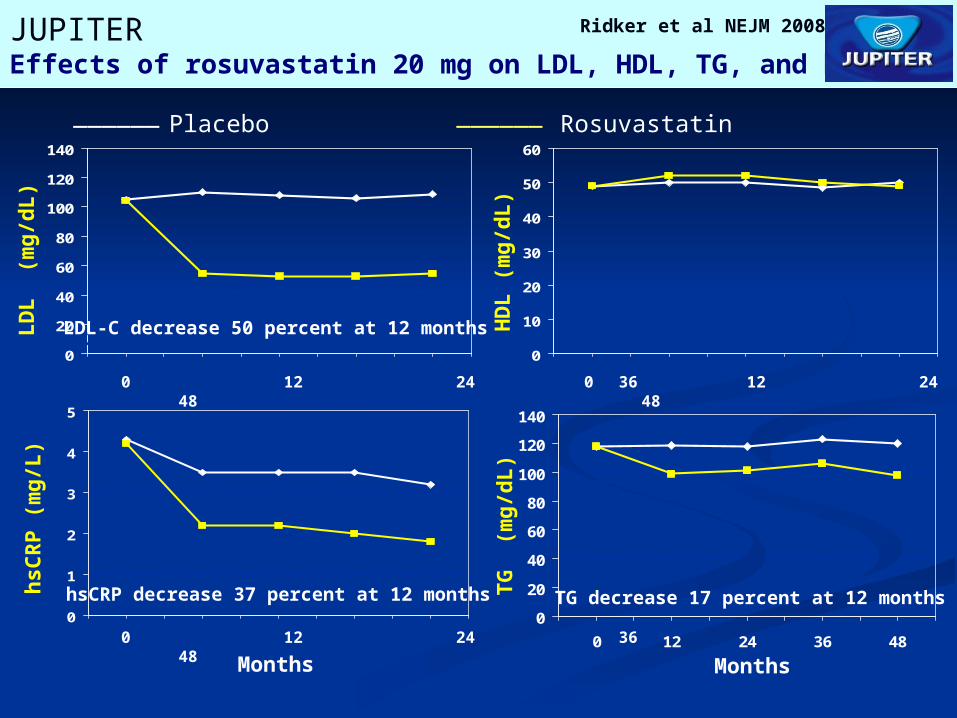
JUPITEREffects of rosuvastatin 20 mg on LDL, HDL, TG, and hsCRP
LDL decrease 50 percent at 12 months
hsCRP decrease 37 percent at 12 months
HDL increase 4 percent at 12 months
TG decrease 17 percent at 12 months
Ridker et al NEJM 2008
0 12 24 36 48
0 12 24 36 48 0 12 24 36 48
______ ______Placebo Rosuvastatin
LDL-C decrease 50 percent at 12 months

JUPITERPrimary Trial Endpoint : MI, Stroke, UA/Revascularization, CV Death
Placebo 251 / 8901
Rosuvastatin 142 / 8901
HR 0.56, 95% CI 0.46-0.69P < 0.00001
- 44 %
0 1 2 3 4
0.0
00
.02
0.0
40
.06
0.0
8
Cu
mu
lati
ve In
cid
ence
Number at Risk Follow-up (years)
Rosuvastatin
Placebo
8,901 8,631 8,412 6,540 3,893 1,958 1,353 983 544 157
8,901 8,621 8,353 6,508 3,872 1,963 1,333 955 534 174
Ridker et al NEJM 2008
Number Needed to Treat (NNT5) = 25

JUPITERSecondary Endpoint – All Cause Mortality
Placebo 247 / 8901
Rosuvastatin 198 / 8901
HR 0.80, 95%CI 0.67-0.97P= 0.02
- 20 %
0 1 2 3 4
0.00
0.01
0.02
0.03
0.04
0.05
0.06
Cu
mu
lati
ve I
nci
den
ce
Number at Risk Follow-up (years)
RosuvastatinPlacebo
8,901 8,847 8,787 6,999 4,312 2,268 1,602 1,192 683 2278,901 8,852 8,775 6,987 4,319 2,295 1,614 1,196 684 246
Ridker et al NEJM 2008

JUPITERPrimary Endpoint – Subgroup Analysis
0.25 0.5 1.0 2.0 4.0
Rosuvastatin Superior Rosuvastatin Inferior
MenWomen
Age < 65Age > 65
SmokerNon-Smoker
CaucasianNon-Caucasian
USA/CanadaRest of World
HypertensionNo Hypertension
All Participants
N P for Interaction
11,001 0.80 6,801
8,541 0.32 9,261
2,820 0.6314,975
12,683 0.57 5,117
6,041 0.5111,761
10,208 0.53 7,586
17,802
Ridker et al NEJM 2008

FDA has approved rosuvastatin to reduce the risk of stroke, MI and arterial revascularization procedures in individuals without clinically evident CHD but with an increased risk of CVD based on age (men
≥50 and women ≥60), hsCRP ≥ 2 mg/L, and the presence of at least one additional CVD risk factor, such as hypertension, low HDL-C, smoking, or a family history of premature coronary heart disease.

AURORA
AURORA Trial. N Engl J Med 2009;360:1395-4074D study. N Engl J Med 2005;353:238-48
• 2776 patients, 50-80 years age, undergoing maintenance hemodialysis
• Rosuvastatin 10 mg Vs placebo
• Median follow-up of 3.8 yrs
• Rosuvastatin lowered LDL-C level but had no significant effect on the composite primary end point of death from cardiovascular causes, nonfatal MI, or nonfatal stroke
• Similar results with atorvastatin observed in 4D study

Rosuvastatin
“Safety”
Adverse events
Equal or even lower risk of myopathy compared to other statins because of the lower dose requirement and option of non-daily dosing
Mild transaminitis might occur – Self limiting
Small but significant increases in the rate of physician-reported diabetes and glycated hemoglobin values noted in JUPITER trial
Hematuria, proteinuria, ARF only in very high doses (≥80mg)
Ann Intern Med. 2009;150:858-868. Am J Cardiol. 2000;85:15E-19E
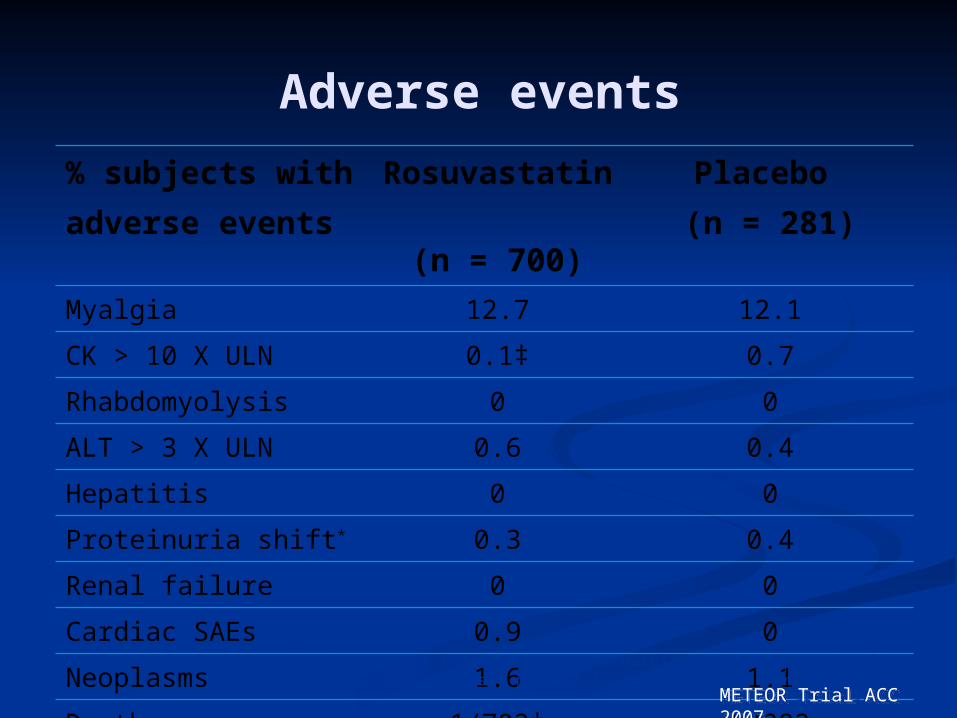
Adverse events
% subjects with adverse events
Rosuvastatin
(n = 700)
Placebo (n = 281)
Myalgia 12.7 12.1
CK > 10 X ULN 0.1‡ 0.7
Rhabdomyolysis 0 0
ALT > 3 X ULN 0.6 0.4
Hepatitis 0 0
Proteinuria shift* 0.3 0.4
Renal failure 0 0
Cardiac SAEs 0.9 0
Neoplasms 1.6 1.1
Deaths 1/702† 0/282*Shift in dipstick urine protein from none/trace at baseline to ≥ 2+ post baseline. †Creutzfeldt-Jakob disease, not related to study treatment. ‡Exercise-associated.
METEOR Trial ACC 2007METEOR Trial ACC 2007
Summary
Lipid abnormalities are proportionately associated with CAD morbidity and mortality
Failure rate in achieving NCEP ATP III goal in CHD patients is very high
Rosuvastatin is more effective in reducing LDL-C and achieving NCEP ATP III goal

Summary Effective in reducing plaque volume,
and hence may be useful for secondary prevention of CAD
May also be useful for primary prevention in select populations
Being a hydrophilic, associated with less chances of drug interactions
Safe and well tolerated



Cost comparison
ZYROVA – Zydus Cadila; 5 mg x 10's (IRP: rupee 90), 10 mg x 10's (IRP: rupee 150), 20 mg x 10's (IRP: rupee 280)
ATORVA – Zydus Cadila; 10 mg x 10's (IRP: rupee 94), 40 mg x 10's (IRP: rupee 190.03)
ORVAS – Systopic; 5 mg x 10's (IRP: rupee 16)10 mg x 10's (IRP: rupee 24.5)20 mg x 10's (IRP: rupee 48)
Source – CIMS (http://cimsasia.com)