static-content.springer.com10.1007... · web view24.miser wf, arakaki r, jiang h, scism-bacon j,...
TRANSCRIPT

Supplementary data tables
Table I: T1DM studies meeting all of the eligibility criteria (all regimens)
Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition
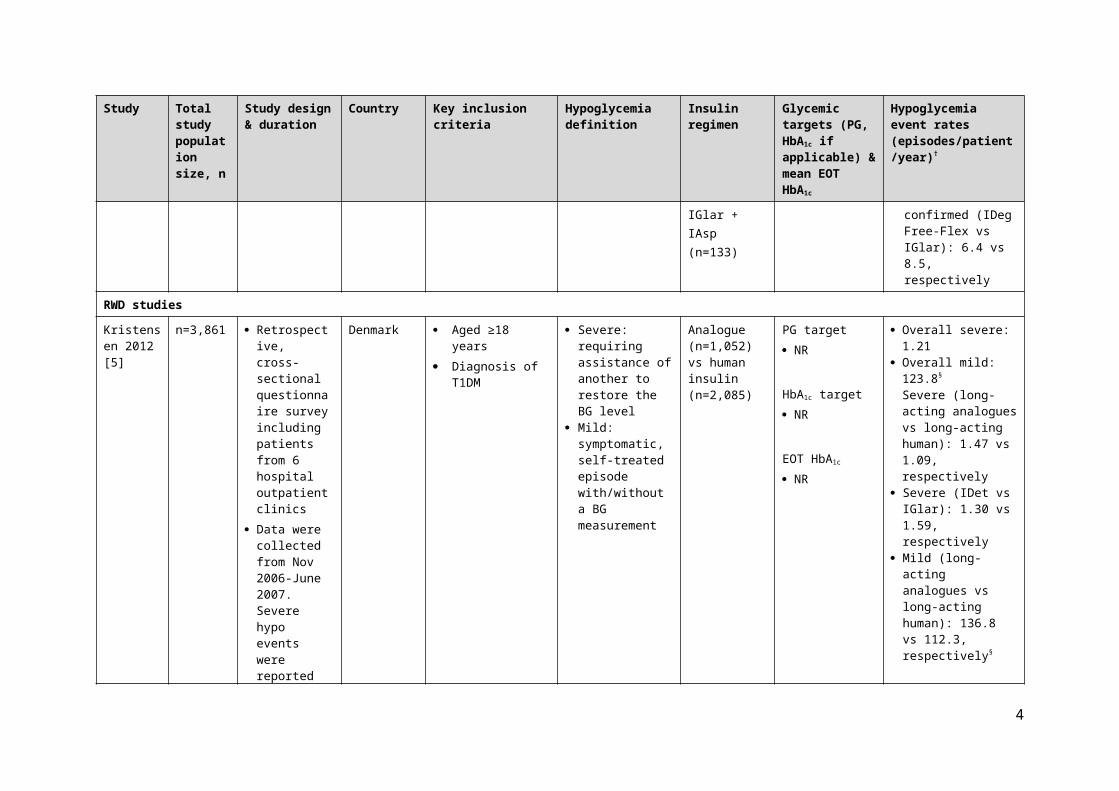
Insulin regimen Glycemic targets (PG, HbA1c if applicable) & mean EOT HbA1c
Hypoglycemia event rates (episodes/patient/year)†
RCTs
Hirsch 2012 [1]
n=548 Phase III, open-label, treat-to-target, multicenter, RCT
26 weeks
Australia, Denmark, France, Israel, Poland, Romania, Russia, UK, USA
Aged ≥18 years Diagnosis of T1DM
for ≥1 year Treated with insulin
(BB, premix, self-mix) for ≥1 year
HbA1c 7.0–10.0% BMI ≤35 kg/m2
Patients with recurrent severe hypoglycemia or hypoglycemic unawareness were excluded.
Confirmed: PG <3.1 mmol/L (regardless of symptoms) or severe episodes requiring assistance
Nocturnal: occurring between midnight and 6:00 hours (inclusive)
Analogue co-formulation vs BB: IDegAsp + IAsp (n=366) vs IDet + IAsp (n=182)
PG target 4–5 mmol/L
HbA1c target <7%
EOT HbA1c
IDeg Asp: 7.6% IDet: 7.6%
Confirmed, including severe (IDegAsp vs IDet + IAsp): 39.17 vs 44.34, respectively
Severe (IDegAsp vs IDet + IAsp): 0.33 vs 0.42, respectively
Nocturnal - confirmed (IDegAsp vs IDet + IAsp):3.71 vs 5.72, respectively
Heller 2012 (BEGIN®: BB T1) [2]
n=629 Phase III, open-label, treat-to-target, non-inferiority, multicenter, RCT
52 weeks
France, Germany, Russia, South Africa, UK, USA
Aged ≥18 years Diagnosis of T1DM
for ≥1 year Treated with BB
therapy for ≥1 year HbA1c ≤10% BMI ≤35 kg/m2
Patients with recurrent severe hypoglycemia or hypoglycemic unawareness were excluded.
Confirmed: PG <3.1 mmol/L or severe episodes requiring assistance
Nocturnal: occurring from 00:01 to 05:59 hours (inclusive)
BB: IDeg + IAsp (n=472) vs IGlar + IAsp (n=157)
PG target 3.9–<5.0
mmol/L
HbA1c target <7%
EOT HbA1c‡
IDeg: 7.3% IGlar: 7.3%
Confirmed, including severe (IDeg vs IGlar): 42.54 vs 40.18, respectively
Severe (IDeg vs IGlar) 0.21 vs 0.16, respectively
Nocturnal - confirmed (IDeg vs IGlar): 4.41 vs 5.86, respectively
1

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition
Insulin regimen Glycemic targets (PG, HbA1c if applicable) & mean EOT HbA1c
Hypoglycemia event rates (episodes/patient/year)†
Bode 2013(BEGIN®: BB T1) [3]
n=469 Open-label, multicenter, extension study of BEGIN® BB T1
52 weeks
France, Germany, Russia, South Africa, UK, USA
Aged ≥18 years Diagnosis of T1DM
for ≥1 year Treated with BB
therapy for ≥1 year HbA1c ≤10% BMI ≤35 kg/m2
Confirmed: PG <3.1 mmol/L or severe episodes requiring assistance
Nocturnal: occurring from 00:01 to 05:59 hours (inclusive)
BB: IDeg + IAsp (n=351) vs IGlar + IAsp (n=118)
PG target 3.9–4.9 mmol/L
HbA1c target <7%
EOT HbA1c
IDeg: 7.4% IGlar: 7.5%
Confirmed: only reported graphically
Severe (IDeg vs IGlar): 0.17 vs 0.15, respectively
Nocturnal - confirmed (IDeg vs IGlar): 3.9 vs. 5.3, respectively
Mathieu 2013 (BEGIN®: Flex T1) [4]
Main trial: n=493
Extension:n=372
Open-label, treat-to-target, non-inferiority RCT
26 weeks with a 26-week extension
Europe, USA Aged ≥18 years On BB therapy HbA1c ≤10% BMI ≤35 kg/m2
Patients with recurrent severe hypoglycemia or hypoglycemic unawareness were excluded.
Confirmed: BG <3.1 mmol/L or severe episodes requiring assistance
Nocturnal: occurring between 00:01 and 05:59 hours (inclusive)
Main trial, BB:
IDeg Forced-Flex + IAsp (IDeg at fixed intervals with 8–40 hrs between doses; n=164) vs IDeg + IAsp (n=165), vs IGlar + IAsp (n=164)
Extension, BB:
IDeg Free-Flex + IAsp (8–40 hrs between doses of IDeg; n=239) vs IGlar + IAsp (n=133)
PG target Basal titration:
4.0–5.0 mmol/L Bolus titration:
<5.0 mmol/L
HbA1c target NR
HbA1c at Week 26‡
IDeg Forced-Flex: 7.3%
IDeg: 7.3% IGlar: 7.1%
HbA1c at Week 52 IDeg Free-Flex:
7.6% IGlar: 7.5%
Weeks 0–26 Confirmed (IDeg
Forced Flex vs IDeg vs IGlar): 82.4 vs 88.3 vs 79.7, respectively
Severe (IDeg Forced Flex vs IDeg vs IGlar): 0.3 vs 0.4 vs 0.5, respectively
Nocturnal - confirmed (IDeg Forced Flex vs IDeg vs IGlar): 6.2 vs 9.6 vs 10.0, respectively
Weeks 0–52 Confirmed (IDeg Free-
Flex vs IGlar): 68.1 vs 63.4, respectively
Severe (IDeg Free-Flex vs IGlar): 0.2 vs 0.4, respectively
Nocturnal - confirmed (IDeg Free-Flex vs IGlar): 6.4 vs 8.5, respectively
2

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition
Insulin regimen Glycemic targets (PG, HbA1c if applicable) & mean EOT HbA1c
Hypoglycemia event rates (episodes/patient/year)†
RWD studies
Kristensen 2012 [5]
n=3,861 Retrospective, cross-sectional questionnaire survey including patients from 6 hospital outpatient clinics
Data were collected from Nov 2006-June 2007. Severe hypo events were reported for the previous year
Denmark Aged ≥18 years Diagnosis of T1DM
Severe: requiring assistance of another to restore the BG level
Mild: symptomatic, self-treated episode with/without a BG measurement
Analogue (n=1,052) vs human insulin (n=2,085)
PG target NR
HbA1c target NR
EOT HbA1c
NR
Overall severe: 1.21 Overall mild: 123.8§
Severe (long-acting analogues vs long-acting human): 1.47 vs 1.09, respectively
Severe (IDet vs IGlar): 1.30 vs 1.59, respectively
Mild (long-acting analogues vs long-acting human): 136.8 vs 112.3, respectively§
Ostenson 2014 [6]
n=1,631 patients with T1DM
Retrospective, questionnaire-based survey
Patients recruited via consumer panels, websites, telephone, and GP clinics
4 weeks
Austria, Denmark, Finland, Norway, Sweden, Switzerland, the Netherlands
Aged ≥15 years Diagnosis of T1DM Current insulin
treatment
Severe: requiring the assistance of another to manage
Non-severe: symptomatic, self-treated, with/without a BG measurement or BG ≤3.1 mmol/L without symptoms and self-managed
Nocturnal: occurring while in bed/asleep
Basal only (n=134), BB (n=1,058), other (n=439)
PG target NR
HbA1c target NR
EOT HbA1c
NR
Mean non-severe: 91.0 Severe: 0.7 Nocturnal – non-
severe: 20.0¶
3
Abbreviations: BB, basal-bolus; BD, twice daily; BG, blood glucose; BMI, body mass index; EOT: end of treatment; HbA1c, glycated hemoglobin; IAsp, insulin aspart; IDeg, insulin degludec; IDegAsp, insulin degludec and insulin aspart co-formulation; IDet, insulin detemir; IGlar, insulin glargine; NR, not reported; OAD, oral anti-diabetic drug; OD, once daily; PG, plasma glucose; RCT, randomized controlled trial; T1DM, type 1 diabetes mellitus.†Event rates are reported as the mean number of episodes per patient per year unless otherwise specified.‡Calculated based on reported baseline values and decreases from baseline.§Rates of mild hypoglycemia are reported in the study as episodes per patient per week. ¶Calculated based on 22% of non-severe hypoglycemic episodes occurring during sleep.
4

Table II: T2DM studies meeting all of the eligibility criteria (basal-oral regimens)
Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition
Insulin regimen Glycemic targets (PG, HbA1c if applicable) & mean EOT HbA1c
Hypoglycemia event rates (episodes/patient/year)†
RCTs
Buse 2011 (DURABLE) [7]
n=2,091 Open-label, multinational, parallel-group RCT
30 months
Argentina, Australia, Brazil, Canada, Greece, Hungary, India the Netherlands, Romania, Spain, USA
Aged 30–80 years Diagnosis of T2DM Insulin naïve HbA1c >7.0% Taking ≥two OADs
(MET, SU, pioglitazone, rosiglitazone) for ≥90 days
Patients with a history of severe hypoglycemia were excluded.
Severe: requiring assistance with oral carbohydrate, IV glucose or glucagon
Confirmed: PG ≤3.9 mmol/L or symptomatic
Nocturnal: occurring after bedtime and before morning meal/insulin dose
Basal-oral: IGlar + OADs (n=1,046)
PG target NR
HbA1c target ≤7.0%
EOT HbA1c
HbA1c for patients who maintained HbA1c goal: 6.5%
HbA1c for patients who did not maintain goal: 7.6%
Overall: 16.4‡
Confirmed (‘documented symptomatic’ with PG ≤3.9 mmol/L): 8.2‡
Severe: 0.07‡
Nocturnal - confirmed: 7.7‡
De Vries 2012 [8]
n=988 Open-label, parallel-group RCT
38 weeks
Belgium, Canada, France, Germany, Italy, the Netherlands, Spain, UK, USA
Aged 18–80 years Diagnosis of T2DM Insulin naïve HbA1c 7.0–10.0%
after treatment with MET for ≥3 months, or HbA1c 7.0–8.5% after treatment with MET and SU for ≥3 months
Minor: PG <3.1 mmol/L and self-treated
Basal-oral: IDet + MET + liraglutide (n=162)
PG target NR
HbA1c target <7.0% ≤6.5%
EOT HbA1c
7.1%
Minor: 0.286
Zinman n=1,030 Open-label, Austria, Aged ≥18 years Confirmed: BG Basal-oral: IDeg PG target Confirmed, including
5

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition
Insulin regimen Glycemic targets (PG, HbA1c if applicable) & mean EOT HbA1c
Hypoglycemia event rates (episodes/patient/year)†
2012 (BEGIN: Once Long) [9]
treat-to-target, non-inferiority, multicenter, parallel-group RCT
52 weeks
Belgium, Canada, Czech Republic, Denmark, Finland, France, Germany, Norway, Serbia and Montenegro, Spain, USA
Diagnosis of T2DM for ≥6 months
Insulin naïve HbA1c 7–10%
(inclusive) BMI ≤40 kg/m2
Treated with unchanged doses of OADs for ≥3 months
Patients with recurrent severe hypoglycemia or hypoglycemic unawareness were excluded.
<3.1 mmol/L or severe episodes requiring assistance
Nocturnal: occurring between 00:01 and 05:59 hours (inclusive)
+ MET (n=773) vs IGlar + MET (n=257)
3.9–4.9 mmol/L
HbA1c target <7.0%
EOT HbA1c
IDeg: 7.1% IGlar: 7.0%
severe (IDeg vs IGlar): 1.52 vs 1.85, respectively
Severe (IDeg vs IGlar): 0.003 vs 0.023, respectively
Nocturnal - confirmed (IDeg vs IGlar): 0.25 vs 0.39, respectively
6

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition
Insulin regimen Glycemic targets (PG, HbA1c if applicable) & mean EOT HbA1c
Hypoglycemia event rates (episodes/patient/year)†
Gough 2013 (BEGIN: Low Volume) [10]
n=460 Open-label, treat-to-target, non-inferiority, multicenter RCT
26 weeks
Canada, France, Ireland, Russia, South Africa, Ukraine, UK, USA
Aged ≥18 years Diagnosis of T2DM
for ≥6 months Insulin naïve HbA1c 7–10%
(inclusive) BMI ≤45 kg/m2
Treated with MET ± additional OADs for ≥3 months
Patients with recurrent severe hypoglycemia (>1 event in last 12 months) or hypoglycemic unawareness were excluded.
Confirmed: BG <3.1 mmol/L or severe episodes requiring assistance
Nocturnal: occurring between 00:01 and 05:59 hours (inclusive)
Basal-oral: IDeg + MET ± DPP-4 inhibitor (n=228) vs IGlar + MET ± DPP-4 inhibitor (n=229)
PG target <5 mmol/L
HbA1c target <7.0%
EOT HbA1c§
IDeg: 7.0% IGlar: 6.9%
Confirmed, including severe (IDeg vs IGlar): 1.22 and 1.42, respectively
Nocturnal - confirmed (IDeg vs IGlar): 0.18 and 0.28, respectively
Meneghini 2013 [11]
n=457 Open-label, treat-to-target, multicenter RCT
26 weeks
Argentina, India, Korea, Puerto Rico, Thailand, USA
Aged ≥18 years Diagnosis of T2DM ≥6
months Treated with MET ± a
second OAD for ≥3 months
HbA1c 7–9% BMI ≤35 kg/m2
Minor: able to self-treat and BG <3.1 mmol/L with/without symptoms
Major: unable to self-treat
Symptomatic: symptoms of hypoglycemia and BG >3.1 mmol/L or no BG measurement
Nocturnal: occurring between 23:00 and 05:59
Basal-oral: IDet + MET (n=228) vs IGlar + MET (n=229)
PG Target ≤5.0 mmol/L
HbA1c target ≤7.0% ≤6.5%
EOT IDet: 7.5% IGlar: 7.1%
All events (IDet vs IGlar): 3.19 vs 4.41, respectively
Minor (IDet vs IGlar): 1.15 vs 1.51, respectively
Symptomatic (IDet vs IGlar): 2.03 vs 2.89, respectively
Major (IDet vs IGlar): 0 vs 0.02, respectively
Nocturnal - confirmed (IDet vs IGlar): 1.11 vs 0.88, respectively
Nocturnal – non-severe (IDet vs IGlar): 0.38 vs
7

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition
Insulin regimen Glycemic targets (PG, HbA1c if applicable) & mean EOT HbA1c
Hypoglycemia event rates (episodes/patient/year)†
hours (inclusive) 0.29, respectively
Meneghini 2013 [12]
n=687 Phase III, open-label, treat-to-target, parallel-group RCT
26 weeks
Argentina, Finland, Hungary, India, Israel, Former Yugoslav Republic of Macedonia, Malaysia, Mexico, Norway, Russia, Serbia and Montenegro, South Africa, Taiwan, UK
Aged ≥18 years Diagnosis of T2DM
for ≥6 months BMI ≤40 kg/m2
Previously treated with OADs (baseline HbA1c 7.0–11.0%) or any basal insulin + OADs (HbA1c 7.0–10.0%)
Patients with recurrent severe hypoglycemia (>1 event in last 12 months) or hypoglycemic unawareness were excluded.
Confirmed: PG <3.1 mmol/L (regardless of symptoms) and severe events requiring assistance
Nocturnal: onset between 00:01 and 05:59 hours (inclusive)
Basal-oral: IDeg Flex (8–40 hrs between doses (n=229) vs IDeg (n=228) vs IGlar (n=230)
PG target 3.9-<5.0 mmol/
L
HbA1c target <7.0%
EOT IDeg Flex: 7.2% IDeg: 7.3% IGlar: 7.1%
Confirmed, including severe (IDeg Flex vs IDeg vs IGlar): 3.6 vs 3.6 vs 3.5, respectively
Nocturnal - confirmed (IDeg Flex vs IDeg vs IGlar): 0.6 vs 0.6 vs 0.8, respectively
Onishi 2013 [13]
n=435 Phase III, open-label, treat-to-target, multicenter, non-inferiority RCT
26 weeks
Hong Kong, Japan, Malaysia, South Korea, Taiwan, Thailand
Aged ≥18 years (≥20 years for Japan)
Diagnosis of T2DM for ≥6 months
Insulin naïve HbA1c 7.0–10.0%
(inclusive) BMI ≤35 kg/m2
Treated with 1–2 OADs at an unchanged dose for ≥3 months
Confirmed: PG <3.1 mmol/L (regardless of symptoms) or severe requiring assistance
Nocturnal: onset between 00:01 and 05:59 hours (inclusive)
Basal-oral: IDeg + ≥1 OAD (n=289) vs IGlar + ≥1 OAD (n=146)
PG target 3.9-<5.0 mmol/
L
HbA1c target <7.0% ≤6.5%
EOT IDeg: 7.2% IGlar: 7.1%
Confirmed, including severe (IDeg vs IGlar): 3.0 vs 3.7, respectively
Nocturnal - confirmed (IDeg vs IGlar): 0.8 vs 1.2, respectively
8

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition
Insulin regimen Glycemic targets (PG, HbA1c if applicable) & mean EOT HbA1c
Hypoglycemia event rates (episodes/patient/year)†
Philis-Tsimikas 2013 [14]
n=458 Open-label, multicenter RCT
26 weeks
Argentina, Canada, India, Mexico, South Africa, Turkey, USA
Aged ≥18 years Diagnosis of T2DM
for ≥6 months Insulin naïve HbA1c 7.5–11.0%
(7.5–10% for Argentina)
BMI ≤40 kg/m2
Treated with 1–2 OADs at an unchanged dose for ≥3 months
Confirmed: plasma glucose <3.1 mmol/L (regardless of symptoms) or severe requiring assistance
Nocturnal: onset between 00:01 and 05:59 hours (inclusive)
Basal-oral: IDeg + OADs (n=229)
PG target <5.0 mmol/L
HbA1c target <7.0%
EOT 7.2%
Confirmed, including severe: 3.07
Severe: 0.01 Nocturnal - confirmed:
0.52
Rodbard 2013 [15]
n=1,023 Open-label, treat-to-target, multinational RCT
52 week extension of BEGIN®: Once Long study
Austria, Belgium, Canada, Czech Republic, Denmark, Finland, France, Germany, Norway, Serbia and Montenegro, Spain, USA
Aged ≥18 years Diagnosis of T2DM
for ≥6 months HbA1c 7–10%
(inclusive) BMI ≤40 kg/m2
Treated with unchanged doses of OADs for ≥3 months
Confirmed: BG <3.1 mmol/L or severe episodes requiring assistance
Nocturnal: occurring between 00:01 and 05:59 hours (inclusive)
Basal-oral: IDeg + OADs (n=551) vs IGlar + OADs (n=174)
PG target 3.9–4.9
mmol/L
HbA1c target <7.0%
EOT IDeg: 7.0% IGlar: 6.9%
Confirmed, including severe (IDeg vs IGlar): 1.72 vs 2.05, respectively
Severe (IDeg vs IGlar): 0.006 vs 0.021, respectively
Nocturnal - confirmed (IDeg vs IGlar): 0.27 vs 0.46, respectively
Buse 2014(DUAL II) [16]
n=413 Phase III, parallel-group, double-blind RCT
26 weeks
Bulgaria, Denmark, Hungary, India, Slovenia, Switzerland, USA
Aged ≥18 years HbA1c 7.5–10.0%
(inclusive) BMI ≥27 kg/m2
Treated with basal insulin at a stable dose (20–40 units/day [±10%]) for ≥90 days + OADs
Confirmed: PG <3.1 mmol/L (regardless of symptoms) and severe requiring assistance
Nocturnal: Confirmed hypoglycemia with onset between
Basal-oral: IDeg + MET (n= 199) vs IDegLira + MET (n=199)
PG target NR
HbA1c target <7.0% ≤6.5%
EOT
Confirmed – including severe (IDeg vs IDegLira): 2.6 vs 1.5, respectively
Nocturnal – confirmed (IDeg vs IDegLira): 0.32 vs 0.22, respectively
9

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition
Insulin regimen Glycemic targets (PG, HbA1c if applicable) & mean EOT HbA1c
Hypoglycemia event rates (episodes/patient/year)†
00:01 and 05:59 hours (inclusive)
IDeg: 8.0% IDegLira: 6.9%
RWD studies
Tsai 2011 (FINE) [17]
n=2,921 Prospective, multinational, observational
6 months
Bangladesh, China, Hong Kong, India, Indonesia, Korea, Pakistan, Singapore, Taiwan, Thailand, Vietnam
Aged ≥20 years Patients with T2DM
on OADs HbA1c ≥8% Required initiation of
basal insulin based on the judgement of their treating physician
Mild/moderate: asymptomatic with BG <3.9 mmol/L, or symptomatic with/without a BG measurement
Severe: BG <3.9 mmol/L requiring assistance
Basal +/- oral regimen: IDet (n=61), IGlar (n=2,016) or NPH +/- OADs (n=589)
PG target NR
HbA1c target <7.0%
EOT§
Overall: 7.7% IGlar: 7.5% IDet: 9.1% NPH: 8.2%
IGlar (mild-moderate vs severe): 0.224 vs 0.003, respectively
IDet (mild-moderate vs severe): 0.361 vs 0.000, respectively
NPH (mild-moderate vs severe): 0.458 vs 0.031, respectively
Home 2011 [18]
n=66,726 Non-interventional, prospective, international, observational
24 weeks
Africa, Asia, Europe, Latin America
Diagnosis of T2DM Minor: BG <3.1 mmol/L, with/without symptoms and able to self-manage
Major: symptomatic, requiring assistance and BG <3.1 mmol/L or reversal of symptoms following food intake, or glucagon or IV glucose
Nocturnal: symptomatic, occurring during
Insulin detemir:Insulin naïve n=12,078Prior insulin user n=3467
PG target NR
HbA1c target <7.0%
EOTNR
Insulin naïve: Overall: 1.33 Minor: 1.33 Major: 0.00 Nocturnal: 0.38
Prior insulin: Overall: 1.83 Minor: 1.83 Major: 0.01 Nocturnal: 0.47
10

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition
Insulin regimen Glycemic targets (PG, HbA1c if applicable) & mean EOT HbA1c
Hypoglycemia event rates (episodes/patient/year)†
sleep between bedtime after the evening insulin injection and before getting up
Verges 2012 (LIGHT) [19]
n=2,541 Longitudinal, prospective, multicenter, observational
3 months
France Aged >40 years Diagnosis of T2DM Insulin naïve HbA1c >7% Receiving OADs
Minor (diurnal or nocturnal): patient reported
Severe: requiring assistance and BG <2.8 mmol/L and relief of symptoms following food intake, glucagon or IV glucose
Insulin analogue (IDet or IGlar)
PG target NR
HbA1c target <7.0%
EOT Overall: 7.5% IDet: 7.5% IGlar: 7.5%
Overall: 5.6 Nocturnal: 1.04 Severe: 0.12
Khunti 2012 (SOLVE) [20]
n=17,374 Prospective, open-label, observational
24 weeks
Canada, China, Germany, Israel, Italy, Poland, Portugal, Spain, Turkey, UK
Diagnosis of T2DM Receiving ≥1 OAD
Minor: BG <3.1 mmol/L with/without symptoms
Severe: requiring assistance to administer food, glucagon or IV glucose
Basal-oral: IDet + OADs
PG target NR
HbA1c target <7.0%
EOT 7.5%
Minor: 1.832 Severe: 0.005 Nocturnal - non-severe:
0.277
Brod 2012 (GAPP2) [21]
n=3,042 Online, multinational, cross-sectional survey
30 days
Canada, Denmark, Germany, Japan, UK, US
Aged ≥40 years Received a diagnosis
of T2DM >40 years of age
Receiving insulin therapy (excluding
Self-treated (diurnal or nocturnal)
Basal (n=1,460) PG target NR
HbA1c target NR
Overall basal¶: 35.3 Diurnal basal¶: 23.1 Nocturnal basal¶: 13.4
11

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition
Insulin regimen Glycemic targets (PG, HbA1c if applicable) & mean EOT HbA1c
Hypoglycemia event rates (episodes/patient/year)†
premix, bolus only or pumps)
EOT NR
Echtay 2013 [22]
n=2,155 Multinational, prospective, observational
24 weeks
Israel, Jordan, Lebanon, Pakistan
Diagnosis of T2DM Previously treated
with ≥1 OAD or newly diagnosed starting IDet ± OAD therapy
Minor: self-treated with/without symptoms and BG <3.1 mmol/L
Major: symptomatic and requiring assistance or reversal of symptoms following glucagon or IV glucose administration
Nocturnal: symptomatic occurring during sleep, after evening insulin injection
Basal ± OAD: IDet
PG target NR
HbA1c target <7.0% ≤6.5%
EOT IDet: 7.6%
Overall: 1.37 Minor: 1.30 Major: 0.02 Nocturnal: 0.39
Ostenson 2014 [6]
n=2,196 Retrospective, questionnaire based survey
Patients recruited via consumer panels, websites, telephone, and GP clinics
4–7 weeks
Austria, Denmark, Finland, Norway, Sweden, Switzerland, the Netherlands
Aged ≥15 years Diagnosis of T2DM Current insulin
treatment
Non-severe: symptomatic self-treated, with/without a BG measurement or BG ≤3.1 mmol/L without symptoms, self-managed
Severe: requiring assistance to manage
Nocturnal: occurring while in bed/asleep
Basal PG target NR
HbA1c target NR
EOT NR
Non-severe: 20.3 Severe: 0.1 Nocturnal – non-
severe††: 6.5
12

Abbreviations: BG, blood glucose; BMI, body mass index; EOT, end of treatment; HbA1c, glycated hemoglobin; IDet insulin detemir; IDeg, insulin degludec; IGlar, insulin glargine; IV, intravenous; MET, metformin; NPH, neutral protamine Hagedorn; NR, not reported; OAD, oral anti-diabetic drug; PG, plasma glucose; RCT, randomized controlled trial; SU, sulphonylurea; T2DM, type 2 diabetes mellitus.†Event rates are reported as the mean number of episodes per patient per year unless otherwise specified.‡For all non-severe hypoglycemia, values were calculated at endpoint for the period between the previous office visit and endpoint office visit. For severe hypoglycemia, incidence and rate were calculated over the entire study duration due to the rare occurrence of severe hypoglycemia.§Calculated based mean change from baseline.¶Calculated based on the rates of events per patient per 30 days.††Calculated based on the percentage of non-severe hypoglycemic events reported during sleep.
13

Table III: T2DM studies meeting all of the eligibility criteria (basal-bolus regimens)
Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition Insulin regimen
HbA1c target (if applicable) & EOT levels (mean, SD)
Hypoglycemia event rates (episodes/patient/year)†
RCTs
Jain 2010 [23]
n=484 Randomized, open-label, active-controlled RCT
36 weeks
Australia, Canada, France, Greece, India, Republic of Korea, Mexico, Russian Federation, Spain
Aged 30–80 years Diagnosis of T2DM Insulin naïve HbA1c 7.5–12.0% BMI ≤40 kg/m2
Taking ≥2 OADs for ≥90 days
Capable and willing to use insulin injections and SMPG
Excluded if recent history of severe hypoglycemia
Confirmed: symptomatic or BG <3.9 mmol/L (regardless of symptoms)
Severe: symptomatic and requiring assistance with either BG <2.8 mmol/L or prompt recovery after oral carbohydrate, glucagon or IV glucose
Nocturnal: occurring between bedtime and waking
Basal-bolus: IGlar + insulin lispro (n=242)
PG target NA
HbA1c target ≤7.0% <7.0% ≤6.5%
EOT IGlar:
7.50%
Overall: 26.6‡
Miser 2010 [24]
n=744 Open-label, parallel-group, non-inferiority intensification sub study of the DURABLE RCT
6 months
Argentina, Australia, Brazil, Canada, Greece, Hungary, India, the Netherlands, Puerto Rico, Romania, Spain
Aged 30–80 years Diagnosis of T2DM Insulin naïve HbA1c >7.0% Treated with ≥2
OADs for 90 days
Excluded if recent history of severe hypoglycemia
Confirmed: plasma glucose ≤3.9 mmol/L§ or symptomatic
Severe: requiring assistance
Nocturnal: events occurring after bedtime and before the morning meal or insulin dose
Basal-bolus: IGlar + ILis + OADs (n=370)
PG target NA
HbA1c target ≤7.0% ≤6.5%
EOT Arm A and
B: 8.1% and 8.2%, respectively
Overall (Arm A and B): 11.2 and 12.1, respectively
Nocturnal IGlar (Arm A and B): 3.0 and 2.4, respectively
Garber n=1,006 Phase III, Bulgaria, Aged ≥18 years Confirmed: BG Basal bolus: PG target Confirmed, including
14

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition Insulin regimen
HbA1c target (if applicable) & EOT levels (mean, SD)
Hypoglycemia event rates (episodes/patient/year)†
2012 (BEGIN®: BB T2) [25]
randomized. open-label, treat-to-target, parallel-group, non-inferiority
52 weeks
Germany, Hong Kong, Ireland, Italy, Romania, Russia, Slovakia, South Africa, Spain, Turkey, USA
Diagnosis of T2DM for ≥6 months
HbA1c 7.0–10.0% (inclusive)
BMI ≤40.0 kg/m2
Treated with any insulin regimen for ≥3 months
<3.1 mmol/L (irrespective of symptoms)
Severe: requiring assistance
Diurnal: occurring between 06:00 and 00:00
Nocturnal: occurring between 00:01 and 05:59 hours (inclusive)
IDeg + IAsp (n=755) vs IGlar + IAsp (n=251)
NR
HbA1c target <7.0%
EOT††
IDeg: 7.2% IGlar: 7.2%
severe (IDeg vs IGlar): 11.09 vs 13.63, respectively
Diurnal (IDeg vs IGlar): 9.28 vs 11.39, respectively
Nocturnal - confirmed (IDeg vs IGlar):1.39 vs 1.84, respectively
Severe (IDeg vs IGlar): 0.06 vs 0.05, respectively
Bowering 2012 [26]
n=426 Randomized open-label, multinational, active-controlled, parallel RCT
48 weeks
Australia, Brazil, Canada, China, India, South Korea, Mexico
Aged 30–80 years Diagnosis of T2DM HbA1c ≥7% and
<11.0% Taking OADs without
insulin for ≥90 days
Excluded if recent history of severe hypoglycemia
Overall: symptomatic or BG <3.9 mmol/L (regardless of symptoms)
Severe: symptomatic and requiring assistance with either BG <2.8 mmol/L, or prompt recovery after oral carbohydrate, glucagon or IV glucose
Nocturnal: any event occurring between bedtime and waking
Basal bolus: IGlar + ILis with OAD (n=212)
PG target NR
HbA1c target <7.0% ≤6.5%
EOT 7.3%
Overall¶: 23.85 Nocturnal¶: 10.34
RWD studies
15

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition Insulin regimen
HbA1c target (if applicable) & EOT levels (mean, SD)
Hypoglycemia event rates (episodes/patient/year)†
Home 2011 [18]
n=66,726 Non-interventional, prospective, international, observational
24 weeks
Africa, Asia, Europe, Latin America
Diagnosis of T2DM Minor: BG <3.1 mmol/L, with/without symptoms and able to self-manage
Major: symptomatic, requiring assistance and BG <3.1 mmol/L or reversal of symptoms following food intake, or glucagon or IV glucose
Nocturnal: symptomatic, occurring during sleep between bedtime after the evening insulin injection and before getting up
Basal-bolus: Insulin naïve n=1593Prior insulin user n=2512
PG target NR
HbA1c target <7.0%
EOT NR
Insulin naïve: Overall: 2.95 Minor: 2.95 Major: 0.00 Nocturnal: 0.42
Prior insulin: Overall: 4.08 Minor: 4.08 Major: 0.001 Nocturnal: 0.95
Brod 2012 (GAPP2) [21]
n=3,042 Online, multinational, cross sectional survey
30 days
Canada, Denmark, Germany, Japan, UK, US
Aged ≥40 years Diagnosis of T2DM Currently on insulin
treatment (excluding premix, bolus only or pumps)
Self-treated (diurnal or nocturnal)
Basal-bolus (n=1,582)
PG target NR
HbA1c target NR
EOT NR
Overall¶: 38.9 Diurnal¶: 30.4 Nocturnal¶: 8.5
Ostenson 2014 [6]
n=2,196 Retrospective, questionnaire-based survey
4–7 weeks
Austria, Denmark, Finland, Norway, Sweden, Switzerland, the Netherlands
Aged ≥15 years Diagnosis of T2DM Currently on insulin
treatment
Severe: requiring assistance to manage
Non-severe: symptomatic self-treated, with/without a BG measurement or BG ≤3.1 mmol/L without symptoms, self-managed
Nocturnal: occurring
Basal-bolus PG target NR
HbA1c target NR
EOT NR
Non-severe: 35.4 Severe: 0.2 Nocturnal – non-
severe‡‡: 7.8
16

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition Insulin regimen
HbA1c target (if applicable) & EOT levels (mean, SD)
Hypoglycemia event rates (episodes/patient/year)†
while in bed/asleep
Abbreviations: BID, twice daily; BG, blood glucose; BMI, body mass index; EOT, end of treatment; HbA1c, glycated hemoglobin; IAsp, insulin aspart; IDet insulin detemir; IDeg, insulin degludec; IGlar, insulin glargine; ILis, insulin lispro; IV, intravenous; NR, not reported; OAD, oral anti-diabetic drug; OD, once daily; PG, plasma glucose; QD, four times daily; RCT, randomized controlled trial; SU, sulphonylurea; T2DM, type 2 diabetes mellitus.†Event rates are reported as the mean number of episodes per patient per year unless otherwise specified.‡Hypoglycemia rates are reported in the study as episodes per patient per week. § Converted from mg/dL to mmol/L¶Hypoglycemia rates are reported in the study as episodes per 30 days. †† Calculated based on the mean change from baseline.‡‡ Calculated based on the percentage of non-severe hypoglycemic events reported during sleep.
17

Table IV: T2DM studies meeting all of the eligibility criteria (premix regimens)
Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition Insulin regimen
HbA1c target (if applicable) & EOT levels (mean, SD)
Hypoglycemia event rates (episodes/patient/year)†
RCTs
Jain 2010 [23]
n=484 Randomized, open-label, active-controlled RCT
36 weeks
Australia, Canada, France, Greece, India, Republic of Korea, Mexico, Russian Federation, Spain
Aged 30–80 years Diagnosis of T2DM Insulin naïve HbA1c 7.5–12.0% BMI ≤40 kg/m2
Taking ≥2 OADs for ≥90 days
Confirmed: symptomatic or BG <3.9 mmol/L (regardless of symptoms)
Severe: symptomatic and requiring assistance with either BG <2.8 mmol/L or prompt recovery after oral carbohydrate, glucagon or IV glucose
Nocturnal: occurring between bedtime and waking
Premix: Insulin lispro mix 50/50
PG target NR
HbA1c target ≤7.0% <7.0% ≤6.5%
EOT 7.58%
All events¶: 19.1
Miser 2010 [24]
n=744 Open-label, parallel-group, non-inferiority intensification sub study of the DURABLE RCT
6 months
Argentina, Australia, Brazil, Canada, Greece, Hungary, India, the Netherlands, Puerto Rico, Romania, Spain
Aged 30–80 years Diagnosis of T2DM Insulin naïve HbA1c >7.0% Treated with ≥2
OADs for 90 days Excluded if recent
history of severe hypoglycemia
Confirmed: plasma glucose ≤70 mg/dL or symptomatic
Severe: requiring assistance
Nocturnal: events occurring after bedtime and before the morning meal or insulin dose
Premix: insulin lispro mix 75/25 (Arm A) (n=200) or insulin lispro 50/50 (Arm B) (n=174)
PG target NR
HbA1c target ≤7.0% <7.0%
EOT Arm A:
8.0% Arm B:
8.2%
Arm A (insulin lispro 75/25) Overall: 10.1 Nocturnal - confirmed:
2.5Arm B (insulin lispro 50/50) Overall: 11.1 Nocturnal - confirmed:
2.5
18

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition Insulin regimen
HbA1c target (if applicable) & EOT levels (mean, SD)
Hypoglycemia event rates (episodes/patient/year)†
Rosenstock 2010 [27]
n=677 Randomized, open-label, parallel-group RCT
52 weeks
Argentina, Brazil, Canada, Chile, Mexico, Poland, Russia, Spain, UK, USA
Aged 18–80 years Diagnosis of T2DM HbA1c >7.0% and
≤11.0% BMI ≤40 kg/m2
Taking any standard insulin regimen of 2 or 3 injections daily
Required <1.4 U insulin per kg bodyweight
Non-smoking for ≥6 months
FEV1 and DLco ≥70% Total lung capacity
≥80%
Excluded if experienced ≥2 episodes of hypoglycemia or related admission to hospital within 6 months
Mild/moderate: symptomatic and BG ≤3.5 mmol/L; symptoms in the absence of BG measurements that are relieved by carbohydrate administration; or BG >2.0 mmol/L or ≤2.7 mmol/L with/without symptoms
Severe: BG ≤2 mmol/L or symptomatic requiring assistance and BG <2.7 mmol/L. In the absence of BG measurement, symptoms to be reversed by oral carbohydrates or SC glucagon
Premix: Biphasic IAsp 70/30 (n=316)
PG target NR
HbA1c target ≤7.0%
EOT§
8.0%
Mild/moderate: 7.08††
Severe: 0.26‡‡
Overall: 7.32††
Buse 2011 (DURABLE) [7]
n=2,091 Randomized, open-label, multicenter, parallel-group RCT
30 months
Argentina, Australia, Brazil, Canada, Greece, Hungary, India the Netherlands, Puerto Rico, Romania,
Aged 30–80 years Diagnosis of T2DM Insulin naïve HbA1c >7.0% Taking two or more
OADs (Met, SU, pioglitazone, rosiglitazone) for ≥90 days
Excluded if history of
Severe: requiring assistance with oral carbohydrate, IV glucose or glucagon
Confirmed: plasma glucose ≤3.9 mmol/L or symptomatic
Nocturnal: occurring after bedtime and before morning
Premix: lispro mix 75/25 + OADs (n=1,045)
PG target NR
HbA1c target ≤7.0%
EOT 7.1%
Overall, including severe: 18.6
Severe: 0.03 Nocturnal - confirmed:
5.9
19

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition Insulin regimen
HbA1c target (if applicable) & EOT levels (mean, SD)
Hypoglycemia event rates (episodes/patient/year)†
Spain, USA severe hypoglycemia meal/insulin dose
Bowering 2012 [26]
n=426 Randomized, open-label, active-controlled, parallel RCT
48 weeks
Australia, Brazil, Canada, China, India, South Korea, Mexico
Aged 30–80 years Diagnosis of T2DM HbA1c ≥7% and
<11.0% Taking OADs without
insulin for ≥90 days
Confirmed: symptomatic or BG <3.9 mmol/L (regardless of symptoms)
Severe: symptomatic and requiring assistance with either BG <2.8 mmol/L, or prompt recovery after oral carbohydrate, glucagon or IV glucose
Nocturnal: occurring between bedtime and waking
Premix: insulin lispro mix 75/25
PG target NR
HbA1c target <7.0% ≤6.5%
EOT 7.1%
Overall¶: 20.8 Nocturnal¶: 8.15
RWD studies
Berntorp 2011 [28]
n=1,154 Prospective, observational, multicenter study in routine clinical practice
6 months
Sweden Diagnosis of T2DM Insulin naïve Treating physician
decision to initiate biphasic IAsp30
Major: requiring assistance and either plasma glucose <3.1 mmol/L or reversal of symptoms upon glucose/glucagon administration
Nocturnal: symptomatic occurring after bedtime and before the morning determination of fasting plasma glucose/insulin injection
Premix: Biphasic IAsp30
PG target NR
HbA1c target ≤7%
EOT 7.2%
Overall event : 4.1 Nocturnal: 0.9
Home 2011 [18]
n=66,726 Non-interventional, prospective, international,
Africa, Asia, Europe, Latin America
Diagnosis of T2DM Minor: BG <3.1 mmol/L, with/without symptoms and able to self-manage
Major: symptomatic,
Premix: Insulin naïve n=27,591
PG target NR
Insulin naïve: Overall: 1.04 Minor: 1.04
20

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition Insulin regimen
HbA1c target (if applicable) & EOT levels (mean, SD)
Hypoglycemia event rates (episodes/patient/year)†
observational 24 weeks
requiring assistance and BG <3.1 mmol/L or reversal of symptoms following food intake, or glucagon or IV glucose
Nocturnal: symptomatic, occurring during sleep between bedtime after the evening insulin injection and before getting up
Prior insulin user n=13,318
HbA1c target <7.0%
EOT NR
Major: 0.00 Nocturnal: 0.20
Prior insulin: Overall: 2.35 Minor: 2.34 Major: 0.02 Nocturnal: 0.55
Makela 2012 [29]
n=493 Non-randomized, non-interventional, prospective, open-label, observational study in primary care
26 weeks
Finland Diagnosis of T2DM Insulin naïve or
previously treated with basal-only insulin and requiring improved glycemic control as judged by the treating physician
Minor: BG <3.1 mmol/L or symptomatic with BG ≥3.1 mm/L
Major: requiring assistance to administer carbohydrate, glucagon, or IV glucose
Nocturnal: occurring after bedtime and before getting up in the morning
Premix: Biphasic IAsp30 (insulin naïve: 215. prior insulin: 342)
PG target NR
HbA1c target <7.0%
EOT Insulin
naïve: 7.1% Prior
insulin: 7.5%
Major: Insulin naïve: 0.2 Prior insulin: 0.13
Minor: Insulin naïve: 6.45 Prior insulin: 8.58
Nocturnal – non-severe Insulin naïve: 1.25 Prior insulin: 2.56
Pirags 2012 [30]
n=1,139 Prospective, observational, multicenter study
12 months
10 countries in Africa, Asia, and Europe
Aged ≥18 years Diagnosis of T2DM BMI <40 kg/m2
Prior treatment with ≥1 OADs for ≥3 months
Requirement of a premixed insulin to achieve metabolic control as judged by
Severe: requiring assistance to administer carbohydrate, glucagon, or other resuscitative actions and BG <3.9 mmol/L or prompt recovery after restoring normoglycemia
Premix: insulin lispro 25/75 or biphasic IAsp 30/70
PG target NR
HbA1c target <7.0% ≤6.5%
EOT
Severe: 0.04
21

Study Total study population size, n
Study design & duration
Country Key inclusion criteria Hypoglycemia definition Insulin regimen
HbA1c target (if applicable) & EOT levels (mean, SD)
Hypoglycemia event rates (episodes/patient/year)†
the treating physician
7.3%
Ostenson 2014 [6]
n=2,196 Questionnaire based survey
Patients recruited via consumer panels, websites, telephone, and GP clinics
4–7 weeks
Austria, Denmark, Finland, Norway, Sweden, Switzerland, the Netherlands
Aged ≥15 years Diagnosis of T2DM Currently on insulin
treatment
Severe: requiring assistance to manage
Non-severe: symptomatic self-treated, with/without a BG measurement or BG ≤3.1 mmol/L without symptoms, self-managed
Nocturnal: occurring while in bed/asleep
Other, including mixed insulin
PG target NR
HbA1c target NR
EOT NR
Non-severe§§: 27.0 Severe§§: 0.2 Nocturnal – non-
severe§§: 7.3
Abbreviations: BG, blood glucose; BMI, body mass index; DLco, diffusing capacity of the lungs for carbon monoxide; EOT, end of treatment; FEV1, forced expiratory volume in 1 second; HbA1c, glycated hemoglobin; IAsp, insulin aspart; IV, intravenous; MET, metformin; NR, not reported; OAD, oral anti-diabetic drug; OD, once daily; PG, plasma glucose; RCT, randomized controlled trial; SC, subcutaneous; SU, sulphonylurea; T2DM, type 2 diabetes mellitus.†Event rates are reported as the mean number of episodes per patient per year unless otherwise specified.§ Calculated based on the mean change from baseline.¶Hypoglycemia rates are reported in the study as episodes per 30 days. ††Hypoglycemia rates are reported in the study as episodes per patient per month. ‡‡Severe hypoglycemia rates are reported in the study as episodes per 100 patient months. §§ Calculated based on the percentage of non-severe hypoglycemic events reported during sleep.
22

References1. Hirsch IB, Bode B, Courreges JP, Dykiel P, Franek E, Hermansen K, et al. Insulin degludec/insulin aspart administered once daily at any meal, with
insulin aspart at other meals versus a standard basal-bolus regimen in patients with type 1 diabetes: a 26-week, phase 3, randomized, open-label, treat-to-target trial. Diabetes Care. 2012 Nov;35(11):2174-81.
2. Heller S, Buse J, Fisher M, Garg S, Marre M, Merker L, et al. Insulin degludec, an ultra-longacting basal insulin, versus insulin glargine in basal-bolus treatment with mealtime insulin aspart in type 1 diabetes (BEGIN Basal-Bolus Type 1): a phase 3, randomised, open-label, treat-to-target non-inferiority trial. Lancet. 2012 Apr 21;379(9825):1489-97.
3. Bode BW, Buse JB, Fisher M, Garg SK, Marre M, Merker L, et al. Insulin degludec improves glycaemic control with lower nocturnal hypoglycaemia risk than insulin glargine in basal-bolus treatment with mealtime insulin aspart in Type 1 diabetes (BEGIN Basal-Bolus Type 1): 2-year results of a randomized clinical trial. Diabet Med. 2013 May 26;30(11):1293-7.
4. Mathieu C, Hollander P, Miranda-Palma B, Cooper J, Franek E, Russell-Jones D, et al. Efficacy and Safety of Insulin Degludec in a Flexible Dosing Regimen vs Insulin Glargine in Patients With Type 1 Diabetes (BEGIN: Flex T1): A 26-Week Randomized, Treat-to-Target Trial With a 26-Week Extension. J Clin Endocrinol Metab. 2013 Mar;98(3):1154-62.
5. Kristensen PL, Hansen LS, Jespersen MJ, Pedersen-Bjergaard U, Beck-Nielsen H, Christiansen JS, et al. Insulin analogues and severe hypoglycaemia in type 1 diabetes. Diabetes Res Clin Pract. 2012 Apr;96(1):17-23.
6. Ostenson CG, Geelhoed-Duijvestijn P, Lahtela J, Weitgasser R, Markert Jensen M, Pedersen-Bjergaard U. Self-reported non-severe hypoglycaemic events in Europe. Diabet Med. 2014 Jan;31(1):92-101.
7. Buse JB, Wolffenbuttel BH, Herman WH, Hippler S, Martin SA, Jiang HH, et al. The DURAbility of Basal versus Lispro mix 75/25 insulin Efficacy (DURABLE) trial: comparing the durability of lispro mix 75/25 and glargine. Diabetes Care. 2011 Feb;34(2):249-55.
8. DeVries JH, Bain SC, Rodbard HW, Seufert J, D'Alessio D, Thomsen AB, et al. Sequential intensification of metformin treatment in type 2 diabetes with liraglutide followed by randomized addition of basal insulin prompted by A1C targets. Diabetes Care. 2012 Jul;35(7):1446-54.
9. Zinman B, Philis-Tsimikas A, Cariou B, Handelsman Y, Rodbard HW, Johansen T, et al. Insulin Degludec Versus Insulin Glargine in Insulin-Naive Patients With Type 2 Diabetes: A 1-year, randomized, treat-to-target trial (BEGIN Once Long). Diabetes Care. 2012 Oct 5;35: 2464-71.
10. Gough SCL, Bhargava A, Jain R, Mersebach H, Rasmussen S, Bergenstal RM. Low volume insulin degludec 200 U/ml once-daily improves glycaemic control similar to insulin glargine with a low risk of hypoglycemia in insulin-naïve patients with type 2 diabetes: A 26-week, randomized, controlled, multinational, treat-to-target trial: the BEGINTM LOW VOLUME trial. Diabetes Care. 2013;36(9):2536-42.
11. Meneghini L, Kesavadev J, Demissie M, Nazeri A, Hollander P. Once-daily initiation of basal insulin as add-on to metformin: a 26-week, randomized, treat-to-target trial comparing insulin detemir with insulin glargine in patients with type 2 diabetes. Diabetes Obes Metab. 2013 Aug;15(8):729-36.
12. Meneghini L, Atkin SL, Gough SC, Raz I, Blonde L, Shestakova M, et al. The efficacy and safety of insulin degludec given in variable once-daily dosing intervals compared with insulin glargine and insulin degludec dosed at the same time daily: a 26-week, randomized, open-label, parallel-group, treat-to-target trial in individuals with type 2 diabetes. Diabetes Care. 2013 Apr;36(4):858-64.
23

13. Onishi Y, Iwamoto Y, Yoo SJ, Clauson P, Tamer SC, Park S. Insulin degludec compared with insulin glargine in insulin-naive patients with type 2 diabetes: A 26-week, randomized, controlled, Pan-Asian, treat-to-target trial. J Diabetes Investig. 2013 Nov 27;4(6):605-12.
14. Philis-Tsimikas A, Del Prato S, Satman I, Bhargava A, Dharmalingam M, Skjoth TV, et al. Effect of insulin degludec versus sitagliptin in patients with type 2 diabetes uncontrolled on oral antidiabetic agents. Diabetes Obes Metab. 2013 Aug;15(8):760-6.
15. Rodbard HW, Cariou B, Zinman B, Handelsman Y, Philis-Tsimikas A, Skjoth TV, et al. Comparison of insulin degludec with insulin glargine in insulin-naive subjects with Type 2 diabetes: a 2-year randomized, treat-to-target trial. Diabet Med. 2013 Nov;30(11):1298-304.
16. Buse JB, Vilsboll T, Thurman J, Blevins TC, Langbakke IH, Bottcher SG, et al. Contribution of Liraglutide in the Fixed-Ratio Combination of Insulin Degludec and Liraglutide (IDegLira). Diabetes Care. 2014 Nov;37(11):2926-33.
17. Tsai ST, Pathan F, Ji L, Yeung VT, Chadha M, Suastika K, et al. First insulinization with basal insulin in patients with Type 2 diabetes in a real-world setting in Asia. J Diabetes. 2011 Sep;3(3):208-16.
18. Home P, Naggar NE, Khamseh M, Gonzalez-Galvez G, Shen C, Chakkarwar P, et al. An observational non-interventional study of people with diabetes beginning or changed to insulin analogue therapy in non-Western countries: the A1chieve study. Diabetes Res Clin Pract. 2011 Dec;94(3):352-63.
19. Verges B, Brun JM, Tawil C, Alexandre B, Kerlan V. Strategies for insulin initiation: insights from the French LIGHT observational study. Diabetes Metab Res Rev. 2012 Jan;28(1):97-105.
20. Khunti K, Caputo S, Damci T, Dzida GJ, Ji Q, Kaiser M, et al. The safety and efficacy of adding once-daily insulin detemir to oral hypoglycaemic agents in patients with type 2 diabetes in a clinical practice setting in 10 countries. Diabetes Obes Metab. 2012 Dec;14(12):1129-36.
21. Brod M, Rana A, Barnett AH. Impact of self-treated hypoglycaemia in type 2 diabetes: a multinational survey in patients and physicians. Curr Med Res Opin. 2012 Dec;28(12):1947-58.
22. Echtay A, Tsur A, Hasan MI, Abu-Hijleh MO, Al Khatib N, Andari E, et al. Clinical experience with insulin detemir in patients with type 2 diabetes from the near East countries. Diabetes therapy : research, treatment and education of diabetes and related disorders. 2013 Dec;4(2):399-408.
23. Jain SM, Mao X, Escalante-Pulido M, Vorokhobina N, Lopez I, Ilag LL. Prandial-basal insulin regimens plus oral antihyperglycaemic agents to improve mealtime glycaemia: initiate and progressively advance insulin therapy in type 2 diabetes. Diabetes Obes Metab. 2010 Nov;12(11):967-75.
24. Miser WF, Arakaki R, Jiang H, Scism-Bacon J, Anderson PW, Fahrbach JL. Randomized, open-label, parallel-group evaluations of basal-bolus therapy versus insulin lispro premixed therapy in patients with type 2 diabetes mellitus failing to achieve control with starter insulin treatment and continuing oral antihyperglycemic drugs: a noninferiority intensification substudy of the DURABLE trial. Clin Ther. 2010 May;32(5):896-908.
25. Garber AJ, King AB, Del Prato S, Sreenan S, Balci MK, Munoz-Torres M, et al. Insulin degludec, an ultra-long acting basal insulin, versus insulin glargine in basal-bolus treatment with mealtime insulin aspart in type 2 diabetes (BEGIN Basal-Bolus Type 2): a phase 3, randomised, open-label, treat-to-target non-inferiority trial. Lancet. 2012 Apr 21;379(9825):1498-507.
26. Bowering K, Reed VA, Felicio JS, Landry J, Ji L, Oliveira J. A study comparing insulin lispro mix 25 with glargine plus lispro therapy in patients with Type 2 diabetes who have inadequate glycaemic control on oral anti-hyperglycaemic medication: results of the PARADIGM study. Diabet Med. 2012 Sep;29(9):e263-72.
24

27. Rosenstock J, Lorber DL, Gnudi L, Howard CP, Bilheimer DW, Chang PC, et al. Prandial inhaled insulin plus basal insulin glargine versus twice daily biaspart insulin for type 2 diabetes: a multicentre randomised trial. Lancet. 2010 Jun 26;375(9733):2244-53.
28. Berntorp K, Haglund M, Larsen S, Petruckevitch A, Landin-Olsson M. Initiation of biphasic insulin aspart 30/70 in subjects with type 2 diabetes mellitus in a largely primary care-based setting in Sweden. Prim Care Diabetes. 2011 Jul;5(2):89-94.
29. Makela JK, Schmuser C, Askonen K, Saukkonen T. Starting or switching to biphasic insulin aspart 30 (BIAsp 30) in type 2 diabetes: a multicenter, observational, primary care study conducted in Finland. Diabetes Res Clin Pract. 2012 Jan;95(1):10-8.
30. Pirags V, El Damassy H, Dabrowski M, Gonen MS, Racicka E, Martinka E, et al. Low risk of severe hypoglycaemia in patients with type 2 diabetes mellitus starting insulin therapy with premixed insulin analogues BID in outpatient settings. Int J Clin Pract. 2012 Nov;66(11):1033-41.
25