staphy aureus by inhibitory titers and serum bactericidal titers for human subject5 receiving...
TRANSCRIPT

C o n c i s e C o m m u n i c a t i o n s 53
Linezolid showed higher activity (MICgo 4.0 mg/L) against B. jragilis (100 strains) compared to eperezolid (MICgo 16 mg/L). The MIC values (range, MIC50 and MICgo) for the 360 tested strains of linezolid and eperezolid are shown in Table 1. Strains with intrinsic resistance to conventional anti-anaerobe agents, includ- ing three C. d@le strains and one B. jagi l i s strain resistant to clindamycin, seven €3. ,%@is strains resistant to cefoxitin, and one B. splunchnicus resistant to metronidazole, did not show any cross-resistance to the oxazolidinones.
The results of the present study are in accordance with previous reports on in vitro susceptibility to linezolid and eperezolid of anaerobic microorganisms [3]. Oral administration of linezolid (400 mg PO) and eperezolid (1 000 mg PO) to healthy volunteers has earlier been reported to yield peak serum concentra- tions of 12.38 mg/L and 6.28 mg/L, respectively, while the trough concentrations were estimated to be 7.9 mg/L and 1.62 mg/L, respectively [7]. These serum levels of linezolid are well in excess of the MICs €or anaerobic Gram-positive bacteria as well as for many anaerobic Gram-negative microorganisms. Concerning eperezolid, anaerobic Gran-positive bacteria are mainly susceptible to achieved serum levels. Linezolid has been reported to be active versus experimental B. -fiagilis soft tissue infections in mice [XI . Future clinical studies will show the potential of the oxazolidinones in the treatment of anaerobic infections. In conclusion, the new oxazolidinones linezolid and eperezolid have excellent activity against Gram-positive anaerobic
microorganisms, with linezolid also exhibiting activity against Bacteroides spp. These agents may be useful in the treatment and prophylaxis of anaerobic infections.
Acknowledgment This work was supported by Pharmacia & Upjohn Inc., Kalamazoo, MI, USA.
References 1.
3 1.
3.
4.
5
6.
7
8
Ford CW, Hamel JC, Stapert D, et al. Oxazolidinones: new antibacterial agents. Trends Microbiol 1996; 5: 196-200. Jones R N , Johnson DM, Erwin ME. I n vitro antimicrobial activities and spectra of U-100592 and U-100766, two novel fluorinated oxazolidinones. Antimicrob Agents Cheinother 1996; 40: 720-6. Zurenco GE, Yagi BH, Schaadc RD, et al. In vitim activities of U-100592 and U-100766, novel oxazolidinone antibacterial agents. Antiinicrob Agents Chemother 1996; 40: 839-45. Finegold S. Anaerobic infections in humans: an overview. Anaerobe 1995; 1: 3-9. Hedberg M, Nord CE. Antimicrobial-resistant anaerobic bacteria in human infections. Med Microbiol Lett 1996; 5: 295-304. Suinmanen P, Baron E. Citron D, Strong C, Wexler H, Finegold S. Wadsworth anaerobic bacteriology manual, 5th edn. Los Angeles, CA: Veterans Administration Wadsworth Medical Center, 3 993. Schaadt RD, Bates DH, Daley-Yates PT, Pawsey SD, Stalker DJ, Zurenko GE. Seruni inhibitory titers and serum bactericidal titers for human subject5 receiving multiple doses of the antibacterial oxazolidinones eperezolid and linezolid. Diagn Microbiol Infect Dis 1997; 28: 2 0 1 3 . Ford CW, H a n d JC, Wilsoin DM, et al. The in vivo activities of U-100592 and U-100766, novel oxazolidinone antimicrobial agents, against experimental bacterial infections. Antiinicrob Agents Chemother 1996; 40: 1508-13.
Identification of methicillin-resistant Staphy lococcus aureus by latex agglutination kits: performance with epidemic strains (EMRSA) and strains causing problems with latex agglutination methods
Cliri hficrobiol lrtfcct 1999; 5: 53-56
Colirz W B. Walker" mid Derek E J Browti
Clinical Microbiology and Public Health Laboratory, Box 236, Addenbrooke's Hospital, Cambridge CBI' 2QW, UK
*Tel: +44 1223 257035 Fax: +44 1223 242175 E-mail:
Acceuted 22 June 1998
Agglutination kits for the identification of Staphylococcus aweus have been available for a number of years as an alternative to the coagulase test. The tube coagulase
test, which detects the production of free coagulase, was considered to be the standard (sensitivity 95-98%) but it takes 4-34 h for completion [I 4. A more simple
5 4 C l in ica l M i c r o b i o l o g y a n d I n f e c t i o n , V o l u m e 5 N u m b e r 1, J a n u a r y 1999
and widely used test is the detection ofbound coagulase (clumping factor) by a slide agglutination reaction. However, this test is less reliable and has a 10-15% false- negative rate [l]. Rapid commercial agglutination assays based on the detection of clumping factor and protein A became available in the early 1980s, and reports suggested accuracy similar to that of the tube coagulase test [3-51. However, later reports documented false- negative results among methicillin-resistant S. uureus (MRSA) strains, and this has been explained by the absence or low-level production of clumping factor or protein A in some strains [6-111. More recently, some kits have been enhanced to overcome the problems with identification of MRSA by including antibodies to cell surface antigens or capsular polysaccharide, and it is reported that some kits have proved reliable for the identification of MRSA [12-151. These reports suggest that the kits have a sensitivity of 96.9-100%. However, it is unclear how well these new kits perform with epidemic strains of MRSA (EMRSA) described in the UK, and what their reliability is for the identification of strains of MRSA which gave problems with the earlier kit formulations.
MRSA strains were detected soon after the intro- duction of methicillin in 1960 [16]. Reports of their isolation increased in the UK up to a peak of 5% of strains sent to the Staphylococcus Reference Laboratory in 1971 [17]. There followed a fall in the number of isolations of MRSA in the UK and some European countries which has been suggested to be due to the increased use of aminoglycosides [18]. However, in the
1980s there was the recognition of strains described as ‘epidemic’ on the basis of their particular ability to spread and cause infection, while other strains do not behave in this way [19]. EMRSA is defined as affecting two or more patients in two or more hospitals [20]. EMRSA strains were characterized on the basis ofphage typing, antibiogram, protein A and urease production and the presence of toxins. EMRSA-1 was first detected in 198 1 and became progressively more widespread, particularly in the Thames regions, until it began to decline in 1987. Further epidemic strains were described during the late 1980s, and Kerr et a1 described 14 different EMRSA strains in 1990 [21]. The majority of the EMRSA strains have been associated with out- breaks restricted to specific areas of the UK. For example, EMRSA-2 has remained restricted to the South East and South West Thames regions [17]. However, some strains have spread throughout a number of regions and have affected multiple hospitals. These strains include EMRSA-3 (phage type 75/83A), EMRSA-15 (phage type 75) and EMRSA-16 (phage type 29/52/75/77/83A). Currently, EMRSA-3 is the third most common epidemic strain reported and its incidence has remained steady [22 ] . It appeared in the South East Thames region in 1987 and is affecting between 10 and 15 hospitals a month. In contrast, the incidence of strains EMRSA-15 and EMRSA-16 has continued to increase during the period 1993-97, and they currently affect approximately 135 and 125 hospitals a month respectively [22]. Isolates of EMRSA-15 have been reported predominantly from the West Midlands
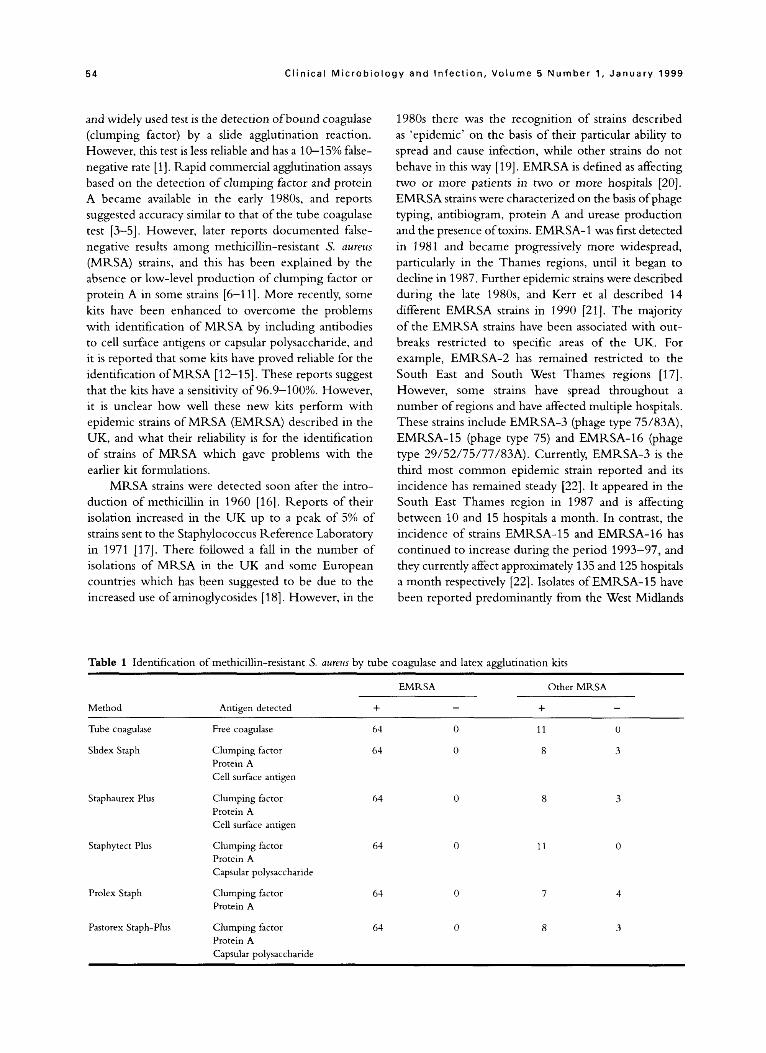
Table 1 Identification of methicillin-resistant S. uureux by tube coagulase and latex agglutination kits
EMRSA
- Method Antigen detected +
~
Other MRSA
Tube coagulase Free coagulase 64
Slidex Staph Clumping factor Protein A Cell surface antigen
Staphaurex Plus Clumping factor Protein A Cell surface antigen
Staphytect Plus Clumping factor Protein A Capsular polysaccharide
Prolex Staph Clumping factor Protein A
64
64
64
64
Pastorex Staph-Plus Clumping factor 64 Protein A Capsular polysaccharide
0
0
11 0
8 3
8
11
7 4
8 3

C o n c i s e C o m m u n i c a t i o n s 55
and North Thames, while EMRSA-16 has been con- centrated in the Thames regions, although both have been isolated throughout the UK.
The epidemic strains have been associated with dfferent infections. EMRSA-3, which is more common in the community, is often isolated from pressure sores and ulcers [23]. EMRSA-15 appears to colonize patients in care of the elderly units and is often isolated from eyes, pressure sores, vaginal swabs and urine [24]. EMRSA-16 tends to be established in hospitals, causing a variety of infections, particularly chest infections [25].
We have tested the ability of several currently available latex agglutination kits to recognize isolates of EMRSA. We have also tested the kits with strains of MRSA which gave problems with identification using earlier latex agglutination kits. Sixty-four strains of E M M A were examined. These included three of type 1, four of type 2, five of type 3, two of type 4, three of type 5, three of type 6, two of type 7, three of type 8, one of type 9, three of type 10, three of type 1 1, three of type 12, three of type 13, three of type 14, one of type 15 and two of type 16. We are grateful to Dr B. Cookson of the Central Public Health Labora- tory, London, UK for supplying these isolates, which were from various hospitals in the UK. Isolates of the same EMRSA type were from different hospitals. An additional 10 isolates of E M M A type 15 and 10 of EMRSA 16 were from different patients at Addenbrooke’s Hospital, Cambridge. Eleven MRSA strains which were not EMRSA but which caused problems with earlier kits were also included [7]. All 75 strains were examined for coagulase production by the tube coagulase test [36] and for agglutination with five commercial latex kits (Slidex Staph, bioM6rieux UK Ltd, Basingstoke, UK; Staphaurex Plus, Murex Biotech Ltd, Dartford, UK; Staphytect Plus, Oxoid Ltd, Basingstoke, UK; Prolex Staph, Pro-Lab Diagnostics, Neston, UK; Pastorex Staph-Plus, Sanofi Pasteur, Guildford, UK).
The identity of all strains of S. aliveus was con- firmed by the tube coagulase test (Table 1). All latex agglutination ki ts proved reliable for the identification of all the EMRSA strains. However, there were problems with the identification of some of the strains which had given problems with the early agglutination kits. The Staphytect Plus was the only kit which was able to identifi all the earlier problematic strains. The Prolex Staph, which detects only clumping factor and protein A, had only one more error than three of the kits which include detection of other cell wall coniponents. Interestingly, different tests gave false-negative results with different strains, and eight strains gave false- negative results with at least one kit. This is probably related to deficiencies in the strains for the particular
components detected by the individual kits. While all the kits correctly identified EMRSA
strains, which account for a large proportion of the isolates currently causing problems in the UK, users should be aware of the possible limitations with some non-epidemic strains.
References 1. Kloos WE, Lambe Jr D T Staphylococcus. In: Balows A, Hausler
Jr. WJ, Hermann KL, Isenberg HD, Shadomy HJ, eds. Manual
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
of clinical microbiology Washington: American Society for Microbioloby, 1991: 221-37. Zarzour JY, Belle EA. Evaluation of three procedures for identification of S/aphylococcus nureus from clinical source?. J Clin Microbiol 1978; 7: 133-b. Doern GV. Evaluation of a commercial latex agglutination test for identification of Staphylococcus auras . J Clin Microbiol 1982;
Essers L, Radebold K. Rapid and reliable identification of Staphylococcus aureiu by a latex agglutination test. J Clin Microbiol 1980; 12: 641-3. Pennell DK, Rott-Petri JA, Kurzynsli TA. Evaluation of three comnirrcial agglutination tests for the identification of Staphylo- coccus aweus. J Clin Microbiol 1984; 20: 614-17. Dickson JS, Marples RR. Coagulase production by strains of Staphylococcus aureus of differing resistance characters: a com- parison of two traditional methods with a latex agglutination system detecting both clumping factor and protein A. J Clin t’athol 1986; 39: 371-5. Coles MAT, Brown DFJ. ‘Staphaurex’ negative, niethicillin resistant Staphylococcus aureus. J Clin Pathol 19%; 39: 13f25. Ruane PJ, Morgan MA, Citron DM, Mulligan ME. Failure of rapid agglutination methods to detect oxacillin-resistant Stnphylu- coccus aurws. J Clin Microbiol 1986; 24: 490-2. Piper J, Hadfield T, McCleskey F, et al. Efficacies of rapid agglutination tests for identification of methicillin-resistant staphylococcal strains as Sfaphylococrus aurcus. J Clin Microbiol
Fournier JM, Boutonnier A, Bouvet A. Staphylococcus uurcw strains which are not identified by rapid agglutination methods are of capyular serotype 5. J Clin Microbiol 1989; 27: 1372-4. Kuusela l‘, Hilden P, Savolainen K, Vuento M, Lyytikainen 0, Vuopio-Varkila J. Rapid detection of methicillin-resistant Staphylococcus auras strains not identified by slide agglutination tests. J Clin Microbiol 1994; 31: 143-7. Tveten Y. Evaluation of new agglutination test for identification of oxacillin-susceptible and oxacillin-resistant Staphylococcus aureus. J Clin Microbiol 1995; 33: 1333-4. I
Luijendijk AD, van Belkum A, Verbrugh H, Kluytmans J. Comparison of five tests for identification of Staphylococcus aweiis from clinical samples. J Clin Microbiol 1996; 34: 2267-9. Kampf G, Weist R, Swidsinski S, Kegel M, Ruden H. Comparison of screening nirthods to identi6 niethicillin- resistant Staphylococcus nureus. Eur J Clin Microbiol Infect Dis 1997; 16: 301-7. Ihvies S. Detection of methicillin-resi?tant Staphylococcus aureus: the evaluation of rapid agglutination methods. Br J Biomed Sci 1997; 54: 13-15. Jevons MI? ‘Ce1benin’-resistant staphylococci. Br Med J 1961; 1: 12.1-5. Marples KK, Reith S. Methicillin-resistant Staphylococcus aweus
in England and Wales. Conimun Dis Rep 1992; 2: K75-9.
15: 416-18.
1988; 26: 1907-9.

56 Clinical Microbiology and Infect ion, Volume 5 Number 1 , January 1999
18. Shanson DC. Antibiotic-resistant Staphylococcus aureus. J Hosp Infect 1981; 2: 11-36.
19. Cookson BD, Phillips I. Epidemic methicillin-resistant Staphylo- coccus aureus. J Antimicrob Chemother 1988; 21: C57-65.
20. Working Party Report. Revised guidelines for the control of methicillin-resistant Staphylococcus aureus infection in hospitals. J Hosp Infect 1998; 39: 253-90.
21. Kerr S, Kerr GE, Mackintosh CA, Marples RR. A survey of methicillin-resistant Staphylococcus aureus affecting patients in England and Wales. J Hosp Infect 1990; 16: 35-48.
22. Anon. Epidemic methicillm resistant Staphylococcus aureus. Commun Dis Rep 1997; 7: 191.
23. Anon. Epidemic methicillin resistant Staphylococcus aureus. Commun Dis Rep 1996; 6: 197.
24. Working Party Report. Guidelines on the control of methicillin- resistant Staphylococcus aureus in the community. J Hosp Infect
25. Cox RA, Conquest C, Mallaghan C, Marples RR. A major outbreak of methicillin-resistant Staphylococcus aureus caused by a new phage type (EMRSA-16). J Hosp Infect 1995; 29: 87-106.
26. Barrow GI, Feltham RKA. Cowan and Steel’s manual for the identification of m e d d bacteria. Cambridge: Cambridge University Press, 1993.
1995; 31: 1-12.