standards in medical informatics dr jeremy rogers md mrcgp senior clinical fellow in health...
TRANSCRIPT

Standards in Standards in Medical InformaticsMedical InformaticsDr Jeremy Rogers MD MRCGPSenior Clinical Fellow in Health InformaticsNorthwest Institute of Bio-Health Informatics

Why Standardise ?Why Standardise ?
How Standards are builtHow Standards are built
Standards BodiesStandards Bodies
HL7HL7

Why Standardise ?Why Standardise ?
Standards Bodies Standards Bodies
How Standards are builtHow Standards are built
HL7HL7

Why Standardise?Why Standardise?
Joseph Whitworth1803-1887
Stanley Grove Care Home (1892)
British Standard Whitworth (BSW)BS 84:1956 : 55º Pitch
Whitworth HospitalDarley Dale (1887)
Whitworth InstituteDarley Dale (1890)

About Standards…About Standards…
DefinitionsDefinitions
Minimum acceptable manufacturing specification, issued by a body that creates such specifications
Concrete example of an item or a specification against which all others may be measured
Common technical specification for competing entities in a market that brings benefits without hurting competition
Conspicuous object used as a rallying point in battle

About Standards…About Standards…
TypesTypes
De jure – followed because you have to
De facto – followed because they’re worth it
Open – publicly availablethough not necessarily royalty free
E.g. 50Hz AC, HTML, POP3
ProprietaryE.g. Sony Memory Stick, VHS/Betamax

About Standards…About Standards…
BenefitsIncreased interoperability of components (in theory)
Reduce duplication of effort
Enable competitive supplier market
PitfallsProprietary ~ supplier lock-in
Open ~ “Embrace, extend and extinguish”
Aka “Copy, corrupt, copyright, circulate, control”
Extinguish = turn and open standard into a proprietary one

'The main reason standards 'The main reason standards are so wonderful is that are so wonderful is that
there are there are so many to choose from'so many to choose from'Anon

Why Standardise ?Why Standardise ?
Standards BodiesStandards Bodies
How Standards are builtHow Standards are built
HL7HL7
Standards BodiesStandards Bodies
ISO
CEN
HL7See also IEEE, ANSI, DICOM, W3C, NCPDP, NCCLS, Corba etc

ISOISO International Organisation for StandardisationInternational Organisation for Standardisation
ISO is acronym for…?
Est 1947
TC 215 – medical informaticsWG1 Health Records and Modelling
WG2 Messaging and Communication
WG3 Health Concept Representation
WG4 Security
WG5 Health Cards

CENCEN
ComitComitéé Europ Europééen de Normalisationen de Normalisation MISSION: to promote voluntary technical harmonization in Europe in conjunction with worldwide bodies and its partners in Europe.
Harmonization:
Diminishes trade barriers
Promotes safety
Allows interoperability of products, systems and services
Promotes common technical understanding
2005 Budget: 11,202,000 Euro (~$13.5m)

CENCENWho is in it?Who is in it?
AustriaBelgiumCyprusCzech RepublicDenmarkEstoniaFinlandFrance
Germany GreeceHungary IcelandIrelandItalyLatviaLithuaniaLuxembourgMalta
The NetherlandsNorwayPolandPortugalSlovakiaSloveniaSpainSwedenSwitzerlandUnited Kingdom
ALL procurements by government or other public bodies from these CEN members MUST comply with all relevant CEN standards

CENCENTC 251 Health InformaticsTC 251 Health Informatics
Website: www.centc251.org
Working GroupsInformation models (WG I)
Terminology and knowledge representation (WG II)
Security, Safety and Quality (WG III)
Technology for Interoperability (WG IV)

HL7HL7Health Level SevenHealth Level Seven
Independent, but ANSI accredited activity, entirely devoted to health
HL7 = level 7 of ISO model for OSI
OSI = Open Systems Interconnection1. The physical layer deals with data at a bit level
2. The data link layer breaks input data into data frames and the receiver returns acknowledgement frames
3. The network layer controls the transmission of packets of data, including routing and control of traffic congestion
4. The transport layer manages data from the session layer, if necessary splitting it into smaller sections
5. The session layer allows machines to communicate, this includes synchronisation of activity
6. The presentation layer manages the syntax and semantics of information, this may also include data compression and encryption
7. The application layer defines file structure and transfer, and manages compatibility between different systems

HL7HL7Raison d’Raison d’êêtretre
‘When two healthcare providers in the USA merge (one buys the other) they often have different computer systems.
To make one business IT system, you need to get the two systems working as one system, if possible. Before HL7 version 2, the whole thing was such a mess that it could easily cost more than a million dollars and take forever. With HL7 version 2 it is estimated that it still costs several hundred thousand dollars and takes months. HL7 version 2 is, therefore, better than nothing but far from ideal. We need to do better (because there are a lot of US healthcare organisations merging right now).
The hope is that connecting two HL7 version 3 systems together might only cost a few tens of thousands of dollars and take a few weeks, because trying to work out how to make the data flow will require even fewer experts and less time. This is because a lot more things that were previously variable or optional in version 2 will now be fixed or compulsory in version 3.’
Dan Russler

HL7HL7Who is in it?Who is in it?
USA origin and primary market
National Groups in:
KoreaLithuaniaThe NetherlandsNew ZealandSouthern AfricaSwitzerlandTaiwanTurkeyUnited Kingdom
ArgentinaAustraliaCanadaChinaCzech RepublicFinlandGermanyIndiaItalyJapan

HL7HL7 OrganisationOrganisation
3 plenary meetings per year
Special Interest Groups
Technical Committeesemail discussions
Arden Syntax
Attachments
Cardiology
Clinical Guidelines
Clinical Genomics
Community Based Health Services
Conformance
Emergency Care
Generation of Anesthesia Standards
Government Project
Health Care Devices
Imaging Integration
Java
Laboratory
Patient Safety
Pediatric Data Standards
Pharmacy
Public Health and Emergency Response
Template
XML
Ballot Task Force
Clinical Statements
Common Message Element Types
Dynamic Model
Harmonization
HL7Terminfo
Services BOF
27 HL7 SIGsTechnical Steering Committee
Architectural Review Board
CCOW
Clinical Decision Support
Education
Electronic Health Record
Electronic Services
Financial Management
Implementation
Infrastructure and Messaging
International Affiliates
Marketing
Medical Records/Information Management
Modeling and Methodology
Orders/Observations
Organization Review Committee
Outreach Committee for Clinical Research
Patient Administration
Patient Care
Personnel Management
Process Improvement
Publishing
Regulated Clinical Research Information Mgmt.
Scheduling and Logistics
Security
Structured Documents
Tooling Committee
Vocabulary
28 HL7 Technical Committees
RIM Harmonisation Committee
Iterative process, final ballot
Why Standardise ?Why Standardise ?
Standards Bodies Standards Bodies
How Standards are builtHow Standards are built
HL7HL7

Building StandardsBuilding Standards Who builds them?Who builds them?
Manufacturers of products
Customers of products
Collectors of tax when one person buys something from another
Competitors with any of the above
Academic experts largely innocent of the above dynamics
CENCEN Development of CEN standardsDevelopment of CEN standards
Influence of members:National standards bodies in each member state
e.g. BSI
Mirror panels of national experts
e.g. NHS IST 35 mirrors CEN TC 251
Nominated expert goes to CEN meetings
CEN Working: Options:Adopt a pre-existing standard
often but not always from ISO
Ask ISO to develop it
the Vienna agreement
Convene a CEN Technical Committee to draft new standard

Building StandardsBuilding Standards How are they built?How are they built?
TC 251Member
Anyone
WorkingGroup
ProposalTC 251Board
Reject
ProjectTeam
InterimReports(INR)
InterimReports(INR)
ShortStrategic
Study
OpenTender
Document
Reject
FirstWorking
Draft(FWD)
FirstWorking
Draft(FWD)
FinalVersion(FFV)
FinalVersion(FFV)
CommentsVotingPre-Standard(ENV)
Pre-Standard(ENV)
Full Standard(EN)
Full Standard(EN)
AbandonAbandon 3 months
3 years

Building StandardsBuilding Standards
The Economic CostThe Economic Cost
$400 Individual Annual Subscription$11000 for company with >$50M turnover
$16000 ~ 3 Meetings per year3 x $700 Transatlantic flight
3 x $900 Hotel for a week
3 weeks physically in attendance
3 weeks consultancy time
StandardsStandards
An ObservationAn Observation
Labour intensive process
Costly to participants
Economic viability:Revenue from process
Revenue from result

DISCUSSION EXERCISEDISCUSSION EXERCISEStandards: friend or foe ?Standards: friend or foe ?
Standards and ProcurementProblems with monolithic MegaCorp
Problems with TinyCorp
Standards and SalesHow do standards create a market?
Can a standard create an acceptable customer lock-in?
Who funds development of competing ‘open’ standards? Why?
Why are emergent standards used in marketing e.g. 811g?

Why Standardise ?Why Standardise ?
Standards BodiesStandards Bodies
How Standards are builtHow Standards are built
HL7HL7

HL7 Standard VersionsHL7 Standard Versions
2.0 (1988) Prototype
2.1 (1990) First standard
2.2 (1994) Widely Adopted
2.3 (1997) In operation
2.3.1 (1999) Approved ANSI standardApproved ANSI standard
2.42.4 (2000) Approved ANSI standard(2000) Approved ANSI standard
2.52.5 (2003)(2003) Current ANSI standardCurrent ANSI standard3.0 In development

Limitations of Version 2.xLimitations of Version 2.x
Implicit information model, not explicit
Events not tightly coupled to profiles
Uncontrolled vocabularies
Limited to a single encoding syntax
No explicit support for object technologies
No explicit support for security functions
Optionality is ubiquitous and troublesome
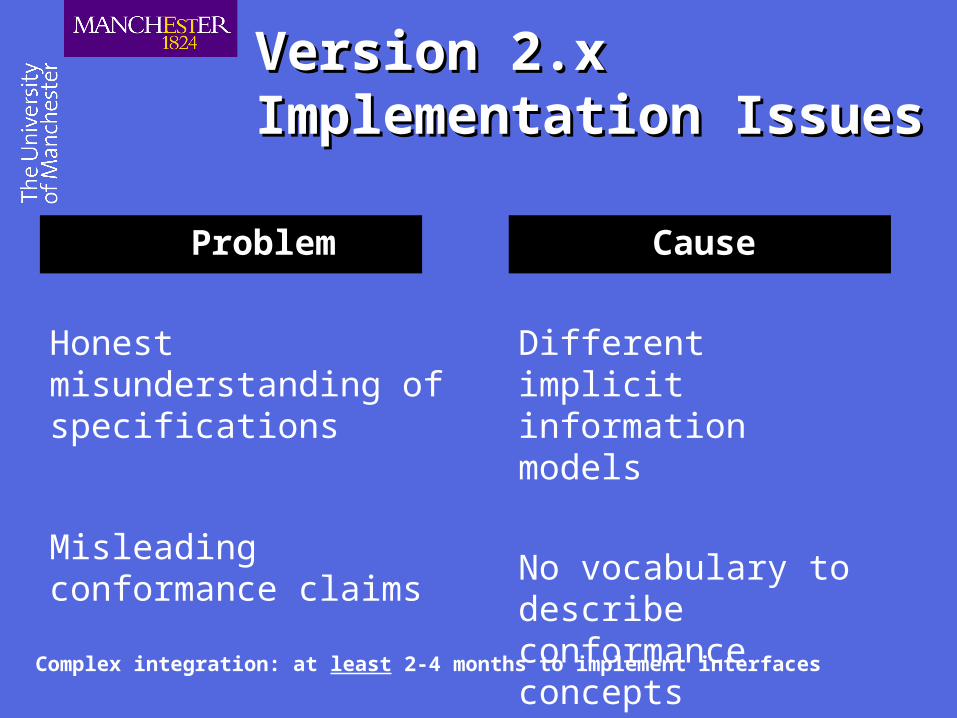
Version 2.x Version 2.x Implementation IssuesImplementation Issues
Complex integration: at least 2-4 months to implement interfaces
Problem
Honest misunderstanding of specifications
Misleading conformance claims
Cause
Different implicit information models
No vocabulary to describe conformance concepts

Other FactorsOther Factors
Increasing pace of business change
Migration toward an evidence-based model
Transition from managing visit to managing cost
Regulatory pressures
Increasing complexity of HIT
HL7 Version 3HL7 Version 3
Clinical Messaging
Clinical Documentation
(Vocabulary)LegLower LimbFemur

HL7 version 3HL7 version 3Main Messaging ComponentsMain Messaging Components
Message Development Framework (MDF)
Reference Information Model (RIM)Large, shared object model representing clinical domain
Message, and ACT life-cycle focus
“An ANSI standard … simple abstract framework which addresses the wildly heterogeneous and interlinked nature of clinical data with only six important classes”
RIM-derived information models DMIM, RMIM
XMLCMET, HMD
Approved Vocabularies
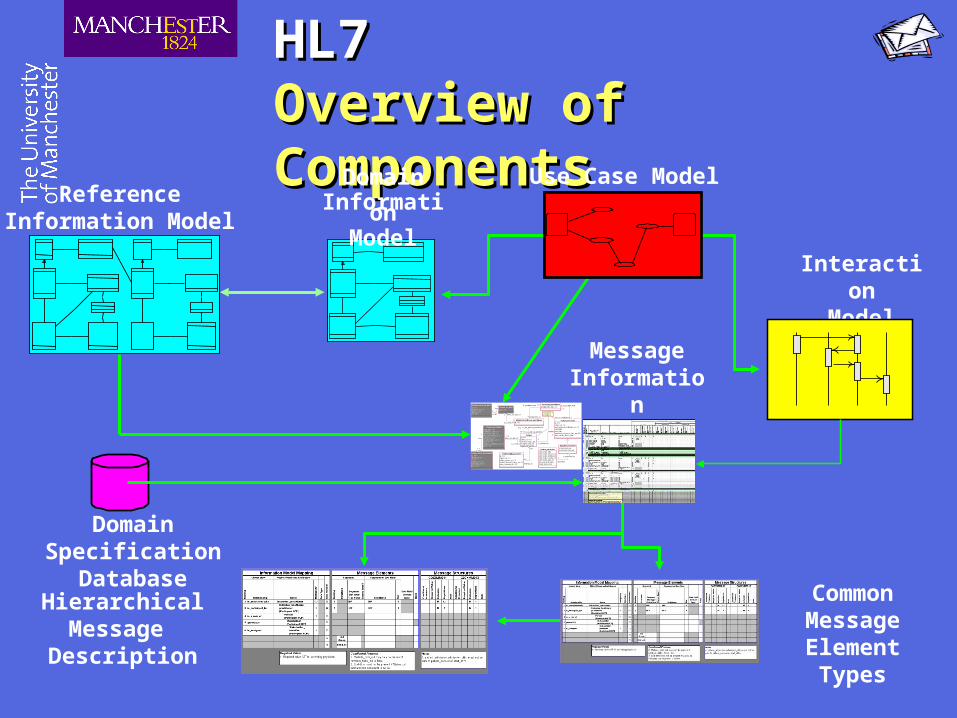
HL7HL7Overview of ComponentsOverview of Components
HierarchicalMessage
Description
CommonMessage ElementTypes
ReferenceInformation Model
MessageInformation
Model
Inpatient_encounter
actual_days_qtyestimated_days_qtyPatient_admission
admission_dttmadmission_reason_cdadmission_referral_cdadmission_source_cdadmission_type_cdpre_admit_test_indreadmission_ind
1
1is_preceded_by
1
preceded
1
Encounter_practitioner
participation_type_cdPerson_as_IHCP
phon : TIL
Person_name_for_IHCP
cd : CVpurpose_cd : CVtype_cd : CVnm : PN
1
1
has1
is_for
1
Patient_billing_account
id : TIIs tatus_cd : CVbilling_status_cd : CVpatient_financial_class_cd : CVprice_schedule_id : TII
Patient_encounter
id : TIIs tatus_cd : CVencounter_classification_cd : CVstart_dttmend_dttmexpected_insurance_plan_qty : NMfirst_similar_illness_dttm
1..*
1
is_associated_with
1..*
has_as_participant 1Individual_healthcare_practitioner
id : TII
0..*
1
is_participant_for 0..*
participates_as1
1
1
is_a_role_of
1
takes_on_role_of1
Patient
id : TIIs tatus_cd : CVnewborn_baby_indmultiple_birth_indorgan_donor_ind
0..1
1
belongs_to
0..1
has1
1
1
involves
1
is_involved_in
1
0..*
0..1
has_a_primary_provider0..*
is_the_primary_provider_for0..1Person_as_Patient
birth_dttm : TSbirthplace_addr : STdeceased_dttm : TSeducation_level_cd : CVgender_cd : CVmarital_s tatus_cd : CVrace_cd : CVreligious_affiliation_cd : CVphon : TIL
1..1
1..1
is_a_role_of
1..1
takes_on_role_of
1..1
Person_name_for_Patient
nm : PNeffective_dt : TScd : CVpurpose_cd : CVtermination_dt : TStype_cd : CV
1
1..*
has
1
is_for1..*
Exactly one occurrence
InteractionModel
Domain SpecificationDatabase
DomainInformation
Model
Use Case Model

HL7 RIMHL7 RIMUltra High Level ViewUltra High Level View
ENTITY
MESSAGE CONTROL
ROLE
STRUCTUREDDOCUMENTS
PARTICIPATIONACT
6 classes:
ACT actions that must be documented as healthcare unfolds
ACT-RELATIONSHIP mutual binding between acts e.g. order and observation
ENTITY physical things of interest or take part in healthcare
ROLE role that entities play in different ACTS
ROLE LINK relationship between roles
PARTICIPATION binds acts to Entities (e.g. who did it, where etc)
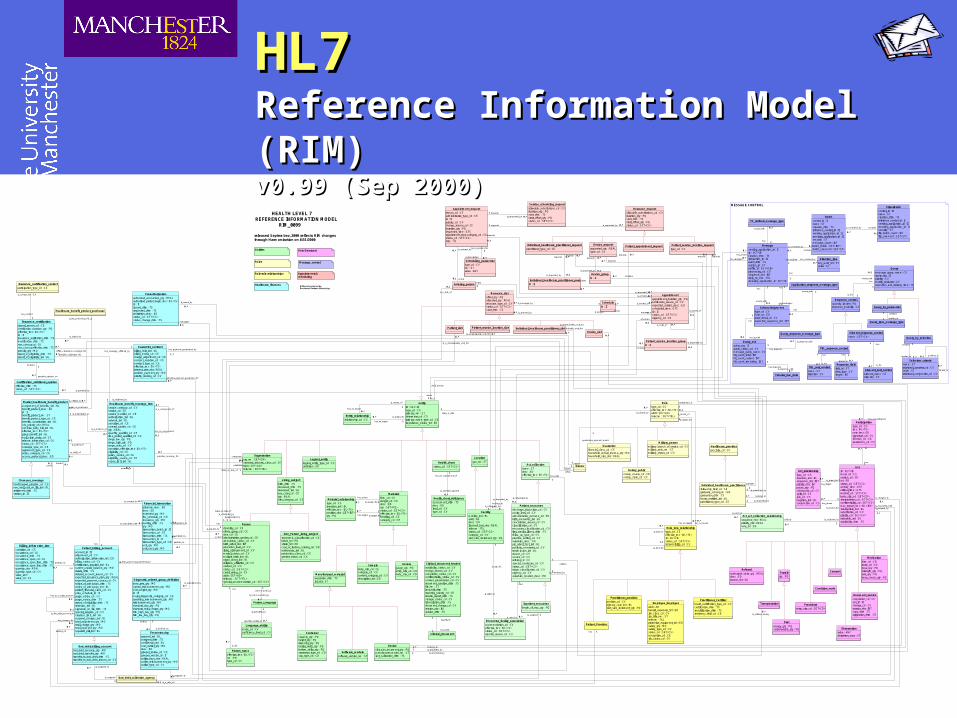
HL7HL7Reference Information Model (RIM)Reference Information Model (RIM)v0.99 (Sep 2000)v0.99 (Sep 2000)
Champus_coverage
handicapped_program_cd : CEnon_avail_cert_on_file_ind : BLretirement_dttm : TSstation_id : II
Referral
authorized_visits_qty : REALdesc : EDreason_txt : ED
Healthcare_finances
Message_control
Acts (Services)
Appointments & scheduling
Roles
HEALTH LEVEL 7 REFERENCE INFORMATION MODEL RIM_0099
released September, 2000 reflects RIM changes through Harmonization on 8/31/2000
Observation
value : ANYderivation_expr : ST
Medication
form_cd : CDroute_cd : CDdose_qty : PQstrength_qty : PQrate_qty : PQdose_check_qty : PQ
Procedure
entry_site_cd : SET<CD>
Supply
qty : PQ
Diet
energy_qty : PQcarbohydrate_qty : PQ
Condition_node
Consent
Enitites
Document_service
completion_cd : CVset_id : IIstorage_cd : CVversion_nbr : INTcopy_dttm : TSorigination_dttm : TS
Billboard produced by:Rochester Outdoor Advertising
Healthcare_provider
specialty_cd : CV
Container
capacty_qty : PQheight_qty : PQdiameter_qty : PQbarrier_delta_qty : PQbottom_delta_qty : PQseperator_type_cd : CDcap_type_cd : CD
Access
gauge_qty : PQentry_site_cd : CDbody_site_cd : CD
Device_slot
Device_request
requested_qty : REALtype_cd : CE
Device_group
id : II
0..*
0..1
requests 0..*
is_requested_by 0..1
Device
slot_size_increment_qty : PQmanufacturer_model_nm : STlast_calibration_dttm : TS
0..*
1
is_scheduleable_unit_for
0..*
is_scheduled_by1
0..*
1
requests0..*
is_requested_by1
0..*
1..*
contains0..*
belongs_to1..*
Notary_public
notary_county_cd : CEnotary_state_cd : CE
Employee_Employer
addr : ADhazard_exposure_txt : EDjob_class_cd : CVjob_title_nm : STtelecom : TELprotective_equipment_txt : EDsalary_qty : MOsalary_type_cd : CVstatus_cd : SET<CS>occupation_cd : CEjob_status_cd : CV
Sample
body_site_cd : CEcategory_cd : CVcontent_category_cd : CVdescription_txt : ED
Living_subject
birth_dttm : TSdeceased_dttm : TSdeceased_ind : BLeye_color_cd : CEqty : REALdiet_category_cd : CS Material_relationship
type_cd : CSinversion_ind : BLeffective_tmr : IVL<TS>position_nbr : LIST<INT>qty : PQ
Material
form_cd : CVdanger_cd : CEdesc : EDqty : SET<PQ>status_cd : SET<CS>effective_tmr : IVL<TS>handling_cd : CEcategory_cd : CE
0..* 1
has_source
0..* is_source_for 1
0..* 1
has_target
0..*
is_target_for
1
Patient_service_location_group
id : II
Patient_service_location_request
type_cd : CV
0..1
0..*
is_requested_by
0..1
requests0..*
Patient_service_location_slot
Facility
mobility_ind : BLaddr : ADdesc : EDlicensed_bed_nbr : REALtelecom : TELstatus_cd : SET<CS>category_cd : CVslot_size_increment_qty : PQ
1..*
0..*
belongs_to
1..*
contains
0..*
1
0..*
is_requested_by
1
requests0..*
0..*
1
is_scheduleable_unit_for 0..*
is_scheduled_by1
Inpatient_encounter
length_of_stay_qty : PQ
Practitioner_provider
position_cd : CVprimary_care_ind : BLslot_size_increment_qty : PQ
Practitioner_Certifier
board_certification_type_cd : CVcertification_dttm : TSrecertification_dttm : TSresidency_field_cd : CE
Military_person
military_branch_of_service_cd : CVmilitary_rank_nm : STmilitary_status_cd : CV
Location
gps_txt : ST
Software_module
software_version_nm : ST
Logical_entity
logical_entity_type_cd : CSdefinition : ED
Bad_debt_billing_account
bad_debt_recovery_qty : MObad_debt_transfer_qty : MOtransfer_to_bad_debt_dttm : TStransfer_to_bad_debt_reason_cd : CV
Encounter_drg
approval_ind : BLassigned_dttm : TSconfidential_ind : BLcost_outlier_qty : MOdesc : EDgrouper_review_cd : CEgrouper_version_id : IIoutlier_days_nbr : REALoutlier_reimbursement_qty : MOoutlier_type_cd : CV
0..*
1
is_assigned_to0..*
is_assigned 1
Language_ability
mode_cd : CVproficiency_level_cd : CV
Manufactured_material
expiration_dttm : TSlot_nbr : ST
Health_chart
status_cd : SET<CS>
Health_chart_deficiency
assessment_dttm : TSdesc : EDlevel_cd : CVtype_cd : CV
1
0..*
has_an_assessment_of1
is_assessed_against
0..*
Bad_debt_collection_agency
0..*
1
is_assigned_to0..*
is_assigned
1
Diagnostic_related_group_definition
base_rate_qty : MOcapital_reimbursement_qty : MOcost_weight_qty : MOid : IImajor_diagnostic_category_cd : CEoperating_reimbursement_qty : MOreimbursement_qty : MOstandard_day_qty : PQstandard_total_charge_qty : MOtrim_high_day_qty : PQtrim_low_day_qty : PQ
1
0..*
defines 1
is_defined_by0..*
Guarantor
financial_class_cd : CEhousehold_annual_income_qty : MOhousehold_size_nbr : REAL
Insurance_certification_contact
participation_type_cd : CE
Healthcare_benefit_product_purchaser
Act_collection
name : STdesc : EDeffective_tmr : IVL<TS>
Organization
org_nm : SET<ON>standard_industry_class_cd : CEaddr : SET<AD>telecom : SET<TEL>
0..1
1
is_a_role_of0..1
takes_on_role_of 1
1..1
0..*
establ ishes
1..1
is_established_by
0..*
Billing_information_item
condition_cd : CEoccurrence_cd : CEoccurrence_dttm : TSoccurrence_span_cd : CEoccurrence_span_from_dttm : TSoccurrence_span_thru_dttm : TSquantity_nbr : REALquantity_type_cd : CVvalue_amtvalue_cd : CE
Guarantor_contract
billing_hold_ind : BLbilling_media_cd : CEcharge_adjustment_cd : CEcontract_duration_cd : CEcontract_type_cd : CEeffective_tmr : IVL<TS>interest_rate_nbr : REALperiodic_payment_qty : MOpriority_ranking_cd : CV
1
1..*
guarantees_payment_under
1
has_payment_guaranteed_by
1..*
Patient_Provider
Act_relationship
type_cd : CSinversion_ind : BLsequence_nbr : INTpriority_nbr : INTpause_qty : PQcheckpoint_cd : CSsplit_cd : CSjoin_cd : CSnegation_ind : BLconjunction_cd : CS
Act_act_collection_relationship
sequence_nbr : REALpriority_nbr : REALnote_txt : ED
1
0..*
has_parts
1
is_part_of
0..*
Patient_billing_account
account_id : IIadjustment_cd : CVauthorization_information_txt : EDbilling_status_cd : CVcertification_required_ind : BLcurrent_unpaid_balance_qty : MOdelete_dttm : TSdeleted_account_reason_cd : CVexpected_insurance_plan_qty : REALexpected_payment_source_cd : CVnotice_of_admission_dttm : TSnotice_of_admission_ind : BLpatient_financial_class_cd : CVprice_schedule_id : IIpurge_status_cd : CVpurge_status_dttm : TSreport_of_eligibility_dttm : TSretention_ind : BLsignature_on_file_dttm : TSspecial_program_cd : CVstoploss_limit_ind : BLsuspend_charges_ind : BLtotal_adjustment_qty : MOtotal_charge_qty : MOtotal_payment_qty : MOseparate_bill_ind : BL
0..*
1pertains_to
0..* has
1
0..1
0..1
is_the_prior_account_for
0..1
has_as_a_prior_account
0..1
0..*
0..*
has_payment_guaranteed_by0..*
provides_payment_guarantee_for
0..*
0..*
1belongs_to
0..*
has 1
Act
id : SET<II>mood_cd : CSservice_cd : CDtxt : EDstatus_cd : SET<CS>activity_time : GTScritical_time : GTSmethod_cd : SET<CV>body_site_cd : SET<CD>interpretation_cd : SET<CS>confidentiality_cd : SET<CV>max_repeat_nmr : IVL<INT>interruptible_ind : BLsubstitution_cd : CVpriority_cd : SET<CV>orderable_ind : BLavailability_dttm : TS
0..* 1
has_source
0..*
is_source_for
1
0..*1
has_target
0..*is_target_for 1
10..*
is_collected_by
1
col lects
0..*
0..*
0..1
is_charged_to
0..*
has_charges_for
0..1
Participation
type_cd : CStmr : IVL<TS>note_text : EDsignature_cd : CVfunction_cd : CDawareness_cd : CV
0..*
1
for0..*
has1
Role_role_relationship
type_cd : CSeffective_tmr : IVL<TS>id : SET<II>status_cd : SET<CS>responsibility_cd : CS
1..1
0..*
is_root_for
1..1
is_leaf_of
0..*
Transportation
Encounter_facility_association
accommodation_cd : CVeffective_tmr : IVL<TS>status_cd : SET<CS>transfer_reason_cd : CV
1
0..*
is_site_for
1
is_sited_at
0..*
Person_Language
0..*
1
specifies_abi lity_in 0..*
is_specified_by1
Person_name
effective_tmr : IVL<TS>nm : PNtype_cd : CV
Patient_appointment_request
Patient_slot
Financial_transaction
alternate_desc : EDdesc : EDextended_qty : MOfee_schedule_cd : CEinsurance_qty : MOposting_dttm : TSqty : MOtransaction_batch_id : IItransaction_cd : CEtransaction_dttm : TStransaction_id : IItransaction_type_cd : CEunit_qty : MOunit_cost_qty : MO
0..1
0..*
categorizes
0..1
is_categorized_by0..*0..*
1
is_associated_with 0..*
has 10..*
1
pertains_to
0..*
is_associated_with
1
Healthcare_benefit_coverage_item
service_category_cd : CVservice_cd : CEservice_modifier_cd : CEauthorization_ind : BLnetwork_ind : BLassertion_cd : CEcovered_parties_cd : CEqty : REALquantity_qualifier_cd : CEtime_period_qualifier_cd : CErange_low_qty : PQrange_high_qty : PQrange_units_cd : CVassertion_effective_tmr : IVL<TS>eligibility_cd : CEpolicy_source_cd : CEeligibility_source_cd : CEcopay_limit_ind : BL
0..1
0..*
has_as_components
0..1
is_a_component_of
0..*
1..*
0..*
is_covered_by
1..*
provides_coverage_for
0..*
Resource_slot
offset_qty : PQallocated_qty : REALresource_type_cd : CVstatus_cd : SET<CS>start_dttm : TS
Schedule
id : II10..*
manages
1is_managed_by0..*
Patient_encounter
discharge_disposition_cd : CVacuity_level_cd : CVadministrative_outcome_txt : EDbirth_encounter_ind : BLcancellation_reason_cd : CVclassification_cd : CVencounter_classification_cd : CVfirst_similar_illness_dttm : TSfollow_up_type_cd : CVpractice_setting_cd : CVvaluables_desc : EDpre_admit_test_ind : BLpublicity_constraint_cd : CVreadmission_ind : BLreason_cd : CVsource_cd : CVreferral_cd : CVspecial_courtesies_cd : CVstatus_cd : SET<CS>triage_classification_cd : CVurgency_cd : CVvaluables_location_desc : ED
0..*
1
is_util ized_during0..*
uti lizes
1
0..*
1
is_used_by 0..*
uses1
Person
disability_cd : CEethnic_group_cd : CErace_cd : CEadministrative_gender_cd : CEambulatory_status_cd : CVbirth_order_nbr : INTeducation_level_cd : CVliving_arrangement_cd : CVmarital_status_cd : CVmultiple_birth_ind : BLorgan_donor_ind : BLreligious_affiliation_cd : CVstudent_cd : CVstatus_cd : SET<CS>credit_rating_cd : CVaddr : SET<AD>telecom : SET<TEL>special_accommodation_cd : SET<CV>
1
0..*
communicates_in
1
is_communicated_by
0..*
1
0..*
has1
is_for
0..*
1
0..*
is_requested_by
1
requests 0..*
0..*
1
is_a_scheduleable_unit_for
0..*
is_scheduled_by
1
0..* 1is_entered_by0..* enters 1
1
0..*
has
1
pertains_to0..*
Resource_request
allowable_substitutions_cd : CVduration_qty : PQstart_dttm : TSstart_offset_qty : PQstatus_cd : SET<CS>
Service_scheduling_request
allowable_substitutions_cd : CVduration_qty : PQstart_dttm : TSstart_offset_qty : PQstatus_cd : SET<CS>
Appointment
appointment_duration_qty : PQnotification_reason_cd : CVexpected_service_desc : EDscheduled_time : GTSid : IIstatus_cd : SET<CS>urgency_cd : CE
0..* 0..*is_reserved_by0..* reserves0..*
1..* 0..*
books
1..* is_booked_in0..*
0..1
0..*
is_parent_of
0..1
is_child_of 0..*
0..1
0..1
is_scheduled_by
0..1
schedules
0..1
Entering_person
0..*
1
is_entered_by0..*
enters
1
1
0..1
takes_on_role_of
1
is_a_role_of
0..1
Scheduling_parameter
type_cd : CVnm : STvalue : ANY
Appointment_request
reason_cd : CEadministrative_type_cd : CEid : IIpriority_cd : CVchange_reason_cd : CEduration_qty : PQrequested_time : GTSappointment_rqst_category_cd : CEstatus_cd : SET<CS>dttm : TS
0..*1 is_requested_by 0..*requests1
1
0..*
requests1
is_requested_by 0..*
0..1
0..*
requests
0..1
is_requested_by0..*
0..1
0..*
enters0..1
is_entered_by0..*
0..*
1
parameterizes 0..*
has_as_parameter1
Query_response_message_type
Tabular_row_data
FileorBatch
control_id : IIname : STcreation_dttm : TSreference_control_id : IIsending_application_id : IIreceiving_application_id : IIsecurity : STfile_batch_count : INTfile_comment : SET<ST>
Application_response_message_type
Query_ack
query_tag : IIquery_status_cd : CVmessage_query_name : CVhit_count_total : INThit_count_current : INThit_count_remaining : INT
1
0..*
has_response
1
is_response_with0..*
1
0..*
has_response
1
is_response_with0..*
Response_control
quantity_limited : PQresponse_modality : CV
Response_field
field_id : STdata_type : CVlength : INT
TBL_response_control
0..*
1
returns_to 0..*
has 1
TBL_sort_control
name : STdirection : CV
1
0..*
has1
is_for0..*
Element_sort_control
element_name : STdirection : CV
Element_response_control
name : SET<CV>
0..*
1
is_for0..*
has1
Query_by_parameter
Query_spec_message_type
1
1
contains1
appl ies_to1
Non_Person_living_subject
taxonomic_classification_cd : CEbreed_txt : EDstrain_txt : EDcoat_or_feather_coloring_txt : EDeuthanasia_ind : BLproduction_class_cd : CEgender_status_cd : CE
MESSAGE CONTROL
Role
type_cd : CSeffective_tmr : IVL<TS>addr : SET<AD>telecom : SET<TEL>
0..*
0..1
has_as_participant0..*
participates_in
0..1
0..*
1
has_as_target0..*
is_target_for1
1
0..*
is_source_of
1
has_as_source0..*
Entity_relationship
relationship_cd : CS
Attention_line
key_word_txt : STvalue : ST
Batch
control_id : IIname : STcreation_dttm : TSreference_control_id : IIsending_application_id : IIreceiving_application_id : IIsecurity : STmessage_count : INTbatch_totals : SET<INT>batch_comment : SET<ST>
0..10..*
contains
0..1
is_contained_by
0..*
TC_defined_message_type
Acknowledgement
type_cd : CVnote_txt : EDerror_detail_cd : CVexpected_sequence_nbr : INT
1
0..1
occurs_with 1
has
0..11
0..1
has
1
occurs_with0..1
Query
message_query_name : CVquery_tag : IIpriority : CVmodify_indicator : CVexecution_and_delivery_time : TS
1
1
has
1
is_for 1
Message
sending_application_id : IIid : SET<II>creation_dttm : TSinteraction_id : IIevent_dttm : TSversion_id : STprofile_id : SET<OID>processing_cd : CVsequence_nbr : INTreply_to_com : TELreceiving_application_id : SET<II>
0..*1
can_accompany
0..*
can_include
1
0..1
0..* contains
0..1is_contained_by
0..*
0..1
1
occurs_with0..1
has1
1..*
1
acknowledges1..*
has 1
0..1
1
occurs_with0..1
has1
0..1
1 occurs_with
0..1has
1
Entity
id : SET<II>type_cd : CSprimary_nm : STdeterminer_cd : CSprimary_name_type_cd : CEimportance_status_txt : ED
10..*
plays_a_role
1
is_played_by
0..*
0..*
1has_as_target
0..* is_target_for
1
1
0..*
is_source_of
1has_as_source
0..*
0..*
1..*
has_recipient0..*
shall_receive
1..*
0..*
1..1
has_sender
0..*
sends
1..1
Query_by_selection
Selection_criteria
name : STrelational_operator_cd : CVvalue : STrelational_conjunction_cd : CV
1
1..*
contains 1
appl ies_to 1..* 0..1
0..*
is_father_to0..1
is_son_of
0..*
Preauthorization
authorized_encounters_qty : REALauthorized_period_begin_tmr : IVL<TS>id : IIissued_dttm : TSrequested_dttm : TSrestriction_desc : EDstatus_cd : SET<CS>status_change_dttm : TS
1
0..1
is_authorized_by1
authorizes
0..1
Insurance_certification
appeal_reason_cd : CEcertification_duration_qty : PQeffective_tmr : IVL<TS>id : IIinsurance_verification_dttm : TSmodification_dttm : TSnon_concur_cd : CEnon_concur_effective_dttm : TSpenalty_qty : MOreport_of_eligibility_dttm : TSreport_of_eligibility_ind : BL
1
1..*
has_contact
1
is_contact_for 1..*
10..*
has_coverage_affi rmed_by
1
affirms_insurance_coverage_for
0..*
0..*
1
provides_validation_for0..*
is_validated_by1
Insurer1
0..*
issues1
is_issued_by
0..*
1
0..*
issues
1
is_issued_by
0..*
Master_healthcare_benefit_product
assignment_of_benefits_ind : BLbenefit_product_desc : EDid : IIbenefit_product_nm : STbenefit_product_type_cd : CEbenefits_coordination_ind : BLcob_priority_nbr : REALcombine_baby_bill_ind : BLeffective_tmr : IVL<TS>group_benefit_ind : BLmail_claim_party_cd : CErelease_information_cd : CEstatus_cd : SET<CS>coverage_type_cd : CEagreement_type_cd : CEpolicy_category_cd : CEaccess_protocol_desc : ED 0..*
0..1
is_child_of
0..*
is_parent_of
0..1
1..1
0..*
is_the_purchaser_of 1..1
has_as_purchaser0..*
0..*
0..1
is_covered_by 0..*
covers0..1
0..*
1
is_a_instance_of
0..*
is_instantiated_as1
0..*
0..*
insures0..*
is_insured_by
0..*
1
0..*
offers
1
is_offered_by 0..*
Clinical_document_header
availability_status_cd : CVchange_reason_cd : CVcompletion_status_cd : CVconfidentiality_status_cd : CVcontent_presentation_cd : CVdocument_creation_dttm : TSfile_nm : STlast_edit_dttm : TSreporting_priority_cd : CEresults_report_dttm : TSstorage_status_cd : CVtranscription_dttm : TSdocument_change_cd : CVversion_nbr : INTversion_dttm : TS
Clinical_document
1
1
is_part_of1
has_parts1
Individual_healthcare_practitioner_slot
Individual_healthcare_practitioner_pool
id : II
Individual_healthcare_practitioner_request
practitioner_type_cd : CE
0..1
0..*
is_requested_by 0..1
requests 0..*
Certification_additional_opinion
effective_dttm : TSstatus_cd : SET<CS>
0..*
1
provides_opinion_on0..*
includes1
Individual_healthcare_practitioner
fellowship_field_cd : CEgraduate_school_nm : ONgraduation_dttm : TSboard_certified_ind : BLpractitioner_type_cd : CE
1
0..*
is_scheduled_by1
is_scheduleable_unit_for
0..*
1..*
0..*
belongs_to1..*
contains
0..*
1
0..*
is_requested_by1
requests 0..*
0..*
1
is_provided_by0..*
provides
1
Role-role relationships

HL7HL7Reference Information Model (RIM)Reference Information Model (RIM)v2.11 (Jul 2005)v2.11 (Jul 2005)
HL7 v3 RIM version 2.1114TH July 2005
ENTITY PARTICIPATION ACT
MESSAGE CONTROL
ROLE
STRUCTUREDDOCUMENTS
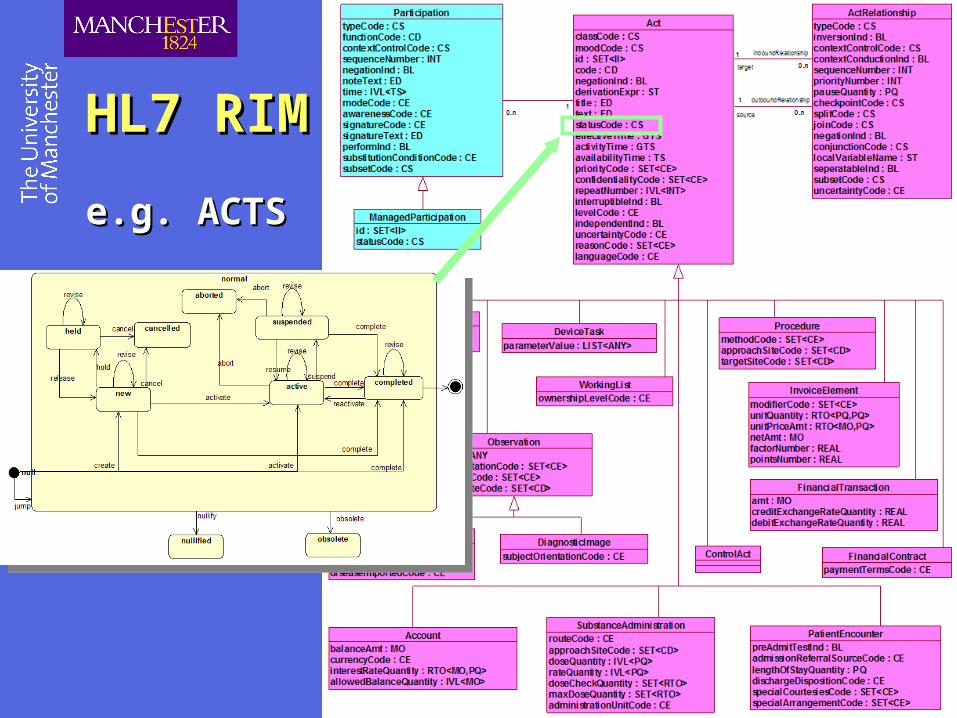
HL7 RIMHL7 RIM e.g. ACTSe.g. ACTS

HL7 RIMHL7 RIM e.g. Message Controle.g. Message Control

EXERCISEEXERCISECompare RIM v0.99 with v2.11Compare RIM v0.99 with v2.11
When was each version released?
List the subtypes of [Role] that an [Entity] may play
Can all subytpes of [Entity] sensibly play all subtypes of [Role]?
What attributes can [Person] take in each version?
Which attributes of [Person] have disappeared since v0.99?

RIM-derivativesRIM-derivatives
Domain Message Information Model (D-MIM)
Makes the abstract RIM specific
Defines the information elements for a specific domain or specialty area
e.g. Prescribing
Refined Message Information Model (R-MIM)
Refines a DMIM to define elements of a family of messages
e.g. Parent Prescribing
Common Message Element Types (CMET)
Reusable DMIM or RMIM components
Hierarchical Message Definition (HMD)
Tabular ordered representation of RMIM elements
? Similar to an XML DTD

Pharmacy DMIM 2003Pharmacy DMIM 2003
Institutional Supply Order(PORX_RM222000)
Supply promise in an institutional setting
0..* subjectCoveragetypeCode*: <= PERTpertainsTo
0..* alerttypeCode*: <= TRIGtriggerFor
0..* formulary
typeCode*: <= INSTdefinition
0..* justifyingObservationIndication
typeCode*: <= RSONreason2
0..* encountertypeCode*: <= COMPcomponentOf1
Note:E.g. radioactive substance mustbe administered in secured location,oral morphine in pharmacy
Note:This Act represents the core of the act ofordering a medication and administering to apatient. It directly holds the route and dosageinstructions.
ObservationIndicationclassCode*: <= OBSmoodCode*: <= EVNid: (used for future maintenance)statusCode: (Complete, Superceded)effectiveTime:confidentialityCode:value*: CE CWE [0..1] <= ObservationValue (e.g. ICD9)targetSiteCode:
FormularyclassCode*: <= SPLYmoodCode*: <= DEFid*: [1..*] (catalogue #)
ObservationCriteriaclassCode*: <= OBSmoodCode*: <= EVN.CRTcode: CE CWE <= ObservationTypetext*:effectiveTime:value:
MedicationAdministrationclassCode*: <= SBADMmoodCode*: <= ActMoodid*:text: (Summary of act)effectiveTime:activityTime:availabilityTime:priorityCode:confidentialityCode: "N"routeCode: <= RouteOfAdministrationapproachSiteCode: <= ActSite (Can't have this without a route)doseQuantity:rateQuantity:doseCheckQuantity: SET<RTO<QTY,QTY>>maxDoseQuantity: SET<RTO<QTY,QTY>>
MedicationSupplyclassCode*: <= SPLYmoodCode*: <= ActMoodid: (defaults to Sub_admin_order.id)code: <= ActPharmacySupplyType (partial, trial, etc. - this would be used to indicate authorizationfor trial/partial dispense)text: (pharm. instructions)effectiveTime: (Earliest/last allowed dispense, frequencyrestrictions, etc.)confidentialityCode:repeatNumber: INT "1" (ie this is issue 3 (of 5))quantity*: [1..1]expectedUseTime: (days supply ordered)
CMET: (COV) A_Coverage
[universal](COCT_MT180000)
CMET: (ALRT) A_Alert
[universal](COCT_MT260000)
CMET: (ENC) A_Encounter
[universal](COCT_MT010000)
CMET: (LOCE) R_LocationLocatedEntity
[universal](COCT_MT070000)
0..* playedRole
CMET: (ASSIGNED) R_AssignedPerson
[universal](COCT_MT090100)
CMET: (LOCE) R_LocationLocatedEntity
[universal](COCT_MT070000)
0..* playedRole
CMET: (ASSIGNED) R_AssignedPerson
[universal](COCT_MT090100)
CMET: (ASSIGNED) R_AssignedPerson
[universal](COCT_MT090100)
CMET: (ASSIGNED) R_AssignedDevice
[universal](COCT_MT090300)
CMET: (ASSIGNED) R_AssignedPerson
[universal](COCT_MT090100)
CMET: (ASSIGNED) R_AssignedDevice
[universal](COCT_MT090300)
0..* locatedEntity
typeCode*: <= DSTdestination
0..* assignedEntity
overseertypeCode*: <= x_ParticipationVrfRespSprfWitmodeCode:signatureCode:signatureText:
0..* participant
author2typeCode*: <= AUTtime*: (time of creation)modeCode:signatureCode:signatureText:
1..* participant *
author2typeCode*: <= AUTtime*: (time of creation)modeCode:signatureCode:signatureText:
0..* assignedEntity
dataEnterertypeCode*: <= ENT
0..* assignedEntity
author1typeCode*: <= AUT
0..* assignedEntity
overseertypeCode*: <= x_ParticipationVrfRespSprfWittime*: (verification or attestation)modeCode:signatureCode:signatureText:
0..* assignedEntity
dataEnterertypeCode*: <= ENT
0..* assignedEntity
author1typeCode*: <= AUT
0..* medication
typeCode*: <= CSMconsumable
1..* aRole *
typeCode*: <= PRDproduct
0..* participant
typeCode*: <= PRFsignatureCode: <= ParticipationSignaturesignatureText:
performer
0..* locatedEntity
typeCode*: <= LOClocation
0..* pertinentCoverage
typeCode*: <= PERTpertinentInformation
0..* locatedEntity
typeCode*: <= ORGorigin
CMET: (ASSIGNED) R_AssignedPerson
[universal](COCT_MT090100)
0..* assignedEntity
typeCode*: <= RCVreceiver
0..* a_SubstanceAdminMaster
typeCode*: <= INSTdefinition
Note:Used to refererencepharmacy protocolsgoverning how a drugshould be prescribed/administered.
A_SubstanceAdminMasterclassCode*: <= SBADMmoodCode*: <= DEFid*: [1..*] (catalogue #)
Pharmacy Domain ModelPORX_DM000000 v11.1
20 March 2003
Updated to Rim 2.02
Note:Eg: Use dose of 50mgif pulse <40bpmorGive medication untilpain relieved
0..* pertinentObservationDx
typeCode*: <= PERTpertinentInformation
Note:Observations that supportthe decision on which medicationor what dose to use.Eg Body weight, Surface Area,Allergies, Medical conditions
CMET: (OBS) A_ObservationDx
[minimal](COCT_MT120104)
CMET: (PAT) R_Patient[universal]
(COCT_MT050000)
1..* patient *
subjecttypeCode*: <= SBJ
Note:The medication ordered or administeredto the patient.Eg Amoxicillin 250mg Tablets.
Will normally be specialised to Kind
Note:The patient who is goingto receive the medication
Note:The header for the visitto the primary care physicianor a particular hospital stay.Includes information on therelevant financial account
Note:The reason for the medfication order.Eg Treatment of bronchitis
Note:Who wrote the order,typically a doctor
Note:Who gave the medicationto the patient, typically unused incommunity and a nurse insecondary care
Note:Who confirmed the order or the admin
Note:Who entered the data sayingfor the order or the admin
Note:Who should be called for clarificationtypically the same as the Author.
Note:Identifies information about an eligibilitycheck or authorization that has beenreceived in relation to an action. It is initiatedfrom the Supply and provides confirmationback to the SubstanceAdministration
Note:Intended to identify problems orwarnings associated with an Actthat have previously been evaluatedand discounted.
This CMET is missing at presentand the mechanism will not work.
Note:Who confirmed the supplytypically a pharmacist
Note:Who entered the data sayingwhat the supply is
Note:Who should be called for clarificationtypically the same as the Author.
Note:Who wrote the supply requesttypically the doctor who wrotethe medication order,but could also be a nurseor ward pharmacist
Note:The formulary which governswhat can be supplied
Note:Who will receive the supply.It may be the patient, a carer.
Note:The medication that is being suppliedeg Amoxil 250mg tables, 56 tablets
Will normally be specialised to instance
Note:For a supply, where the supplycame from and where it was sent to.Eg Pharmacy, Ward
Note:This act represents the act of supplyingmedication to a patient or their representative.It does NOT deal with administering it to the patient.
component / componentOf2
0..* medicationAdministration1
0..* medicationAdministration2
typeCode*: <= COMPNote:Links together a series oforders or administrations that formpart of a series whether scheduledor not or where an order fulfills partof a previous order.
Also used for complex doses, ormultiple routes.
component / componentOf
0..* medicationSupply1
0..* medicationSupply2
typeCode*: <= COMPNote:Links together a series ofsupply acts that formpart of a series whether scheduledor not or where an order fulfills partof a previous order.
0..* participant
typeCode*: <= PRFsignatureCode: <= ParticipationSignaturesignatureText:
performer
Note:Changed fromCOCT_MT070103, but is the the correct CMET?
Note:Need to redo diagnosis code
0..* locatedEntity
typeCode*: <= DSTdestination
0..1 justifiedMedicationAdministration *
0..* justifyingMedicationSupply *
typeCode*: <= RSON
reason1 /reasonOf
inFulfillmentOf
0..* priorMedicationAdministration
typeCode*: <= FLFS
predecessor
0..* priorMedicationAdministration
typeCode*: <= SUCCNote:Allows for modeling revisionof an order
Note:Allows relation of differentmoods of the act.
inFulfillmentOf
0..* priorMedicationSupply
typeCode*: <= FLFS
predecessor
0..* priorMedicationSupply
typeCode*: <= SUCC
Note:Allows for modeling revisionof an order
Note:Allows relation of differentmoods of the act.
AssignedPractitionerOrDevice
AssignedPractitionerOrDevice
Note:See Q&A 31
MedicationAdministrationInstructionsclassCode*: <= SBADMmoodCode*: <= ActMoodtext: (Additional free text instructions)
0..* medicationAdministrationInstructions
typeCode*: <= COMPcomponent1
Community Supply Event(PORX_RM124000)
Supply Event in a community setting
Institutional Combined Order(PORX_RM232000)
Administration and Supply Orderin an institutional setting
Institutional SupplyPromise(PORX_RM223000)
Supply promise in an institutional setting
Institutional Supply Event(PORX_RM224000)
Supply event in an institutional setting
Community Combined Order(PORX_RM132000)
Administration and Supply Orderin a community setting
Institutional Administration Order(PORX_RM212000)
Administration promise in an institutional setting
Institutional Administration Promise(PORX_RM213000)
Administration promise in an institutional setting
Institutional Administration Event(PORX_RM214000)
Administration event in an institutional setting
0..* outcomeObservationCriteria
outcometypeCode*: <= OUTCcheckpointCode:negationInd:conjunctionCode:
0..* observationCriteria
preconditiontypeCode*: <= PRCNcheckpointCode:negationInd:conjunctionCode:
CMET: (MMAT) E_Medication
[universal](COCT_MT231000)
1..1 manufacturedMedication
MedicationclassCode*: <= MANU
1..1 manufacturedMedication
MedicationDispensedclassCode*: <= MANU
CMET: (MMAT) E_Medication
[universal](COCT_MT231000)
Pharmacy DMIM
v11.1 (20.3.2003)

Detail from Pharmacy DMIM
v11.1 (2003)
RouteCode
Ontology of routes?
RouteCode
Ontology of routes?
CMET for encounterCMET for encounter

1..1 patient *
recordTargettypeCode*: <= RCT
ParentPrescriptionclassCode*: <= INFOmoodCode*: <= EVNid*: II [1..1]code*: CD CNE [1..1] <= SnomedCTeffectiveTime*: TS [1..1]
1..1 pertinentCareRecordElementCategory
pertinentInformation2typeCode*: <= PERTtemplateId*: II [1..1] "CSAB_RM-NPfITUK10.pertinentInformation1"
CareRecordElementCategoryclassCode*: <= CATEGORYmoodCode*: <= EVNcode*: CV CNE [1..1] <= CREType
1..* actRef
typeCode*: <= COMP
component
PrescriptionclassCode*: <= SBADMmoodCode*: <= RQOid*: LIST<II> [2..2] (1 Prescription ID, 2 Prescription ID + Check Digit)code*: CD CNE [1..1] <= SnomedCT-AdministrationrepeatNumber: IVL<INT> [0..1]
1..1 participant *
authortypeCode*: <= AUT
contextControlCode*: CS CNE [1..1] <= OPtime*: TS [1..1] (time of creation)
signatureText*: ED [1..1]
0..1 participant
typeCode*: <= LAcontextControlCode*: CS CNE [1..1] <= OP
time*: TS [1..1]signatureText*: ED [1..1]
legalAuthenticator
0..1 participant *
typeCode*: <= PRFcontextControlCode*: CS CNE [1..1] <= OP
performerCMET: (ROL) R_AgentNPFITOrganizationSDS
[universal](UKCT_MT120501UK02)
0..1 pertinentTemporaryExemptionInfo
typeCode*: <= PERTinversionInd*: BL [1..1] "false" (Fixed)contextConductionInd*: BL [1..1] "true" (Fixed)negationInd*: BL [1..1] "false" (Fixed)seperatableInd*: BL [1..1] "true" (Fixed)
pertinentInformation3 TemporaryExemptionInfoclassCode*: <= OBSmoodCode*: <= EVNcode*: CV CNE [1..1] <= PrescriptionAnnotation "EX" (Fixed)effectiveTime*: IVL<TS> [1..1]value*: CV [1..1] <= PrescriptionChargeExemption
ReviewDateclassCode*: <= OBSmoodCode*: <= EVNcode*: CV CNE [1..1] <= PrescriptionAnnotation "RD" (Fixed)effectiveTime*: TS [1..1]
LineItemclassCode*: <= SBADMmoodCode*: <= RQOid*: II [1..1] (item ID)code*: CD CNE [1..1] <= SnomedCT-Administration (Route of and approach site)effectiveTime: GTS (3 times a day etc.)repeatNumber: IVL<INT>doseQuantity: IVL<PQ>rateQuantity: IVL<PQ>
PrescriberEndorsementclassCode*: <= OBSmoodCode*: <= EVNcode*: CV CNE [1..1] <= PrescriptionAnnotation "PE" (Fixed)text: STvalue*: CV [1..1] <= PrescriberEndorsement (Justification)
0..1 pertinentReviewDate
typeCode*: <= PERTinversionInd*: BL [1..1] "false" (Fixed)contextConductionInd*: BL [1..1] "true" (Fixed)negationInd*: BL [1..1] "false" (Fixed)seperatableInd*: BL [1..1] "true" (Fixed)
pertinentInformation11
1..* pertinentLineItem *
typeCode*: <= PERTinversionInd*: BL [1..1] "false" (Fixed)contextConductionInd*: BL [1..1] "true" (Fixed)negationInd*: BL [1..1] "false" (Fixed)seperatableInd*: BL [1..1] "true" (Fixed)templateId*: II [1..1] "CSAB_RM-NPfITUK10.sourceOf2"
pertinentInformation2
RequestedMaterialclassCode*: <= MMATdeterminerCode*: <= KINDcode*: CE CNE [1..1] <= ManufacturedMaterialSnCT
1..1 manufacturedRequestedMaterial
ManufacturedProductclassCode*: <= MANU
1..1 manufacturedProduct *
producttypeCode*: <= PRDcontextControlCode*: CS CNE [1..1] <= ContextControl "OP"
0..* pertinentPrescriberEndorsement
typeCode*: <= PERTinversionInd*: BL [1..1] "false" (Fixed)contextConductionInd*: BL [1..1] "true" (Fixed)negationInd*: BL [1..1] "false" (Fixed)seperatableInd*: BL [1..1] "true" (Fixed)
pertinentInformation3
0..1 priorOriginalItemRef
typeCode*: <= FLFSinversionInd*: BL [1..1] "false" (Fixed)contextConductionInd*: BL [1..1] "false" (Fixed)negationInd*: BL [1..1] "false" (Fixed)seperatableInd*: BL [1..1] "true" (Fixed)templateId*: II [1..1] "CSAB_RM-NPfITUK10.sourceOf1"
inFulfillmentOfOriginalItemRefclassCode*: <= SBADMmoodCode*: <= RQOid*: II [1..1]
0..1 priorOriginalPrescriptionRef
typeCode*: <= FLFSinversionInd*: BL [1..1] "false" (Fixed)contextConductionInd*: BL [1..1] "false" (Fixed)negationInd*: BL [1..1] "false" (Fixed)seperatableInd*: BL [1..1] "true" (Fixed)templateId*: II [1..1] "CSAB_RM-NPfITUK10.sourceOf1"
inFulfillmentOf OriginalPrescriptionRefclassCode*: <= SBADMmoodCode*: <= RQOid*: II [1..1]
ActRefclassCode*: <= ACTmoodCode*: <= ActMoodid*: II [1..1]
Note:Nominated Pharm
Note:Charlie to add effective time tostatement commentary (change name?)
Note:Dose Instructionswill be here in the originaltext part of the CD code
Parent Prescription(PORX_RM132004UK04)
Description
Repeatprescriptionsonly
Constraint:
Repeatprescriptionsonly
Constraint:
Absent for Acute PrescriptionsMandatory otherwise
Constraint: repeatNumber
Relevant only forRepeat Dispensing Prescriptionsabsent otherwise
Constraint:
For RepeatPrescriptions use low and high value,for Repeat dispensing use only high value,for acute do not use.
Constraint: repeatNumber
1..1 pertinentPrescriptionType *
typeCode*: <= PERTinversionInd*: BL [1..1] "false" (Fixed)contextConductionInd*: BL [1..1] "true" (Fixed)negationInd*: BL [1..1] "false" (Fixed)seperatableInd*: BL [1..1] "true" (Fixed)
pertinentInformation4 PrescriptionTypeclassCode*: <= OBSmoodCode*: <= EVNcode*: CV CNE [1..1] <= PrescriptionAnnotation "PT" (Fixed)value*: CV [1..1] <= PrescriptionType
1..1 pertinentPrescriptionTreatmentType *
typeCode*: <= PERTinversionInd*: BL [1..1] "false" (Fixed)contextConductionInd*: BL [1..1] "true" (Fixed)negationInd*: BL [1..1] "false" (Fixed)seperatableInd*: BL [1..1] "true" (Fixed)
pertinentInformation5 PrescriptionTreatmentTypeclassCode*: <= OBSmoodCode*: <= EVNcode*: CV CNE [1..1] <= PrescriptionAnnotation "PTT" (Fixed)value*: CV [1..1] <= PrescriptionTreatmentType
1..1 pertinentPrescription *
typeCode*: <= PERTinversionInd*: BL [1..1] "false" (Fixed)contextConductionInd*: BL [1..1] "true" (Fixed)negationInd*: BL [1..1] "false" (Fixed)seperatableInd*: BL [1..1] "true" (Fixed)templateId*: II [1..1] "CSAB_RM-NPfITUK10.pertinentInformation"
pertinentInformation1
CMET: (ROL) R_AgentNPFITPerson
[universal](UKCT_MT120201UK02)
Note:Add PTT & PT to PrescriptionAnnotation Vocab
Note:As this CMET carries the Patient IDit is a valid according to the CSMP
1..1 participant *
typeCode*: <= RESPcontextControlCode*: CS CNE [1..1] <= OP
responsibleParty
LineItemQuantityclassCode*: <= SPLYmoodCode*: <= RQOcode*: CD CNE [1..1] <= SnomedCT-Supplyquantity*: PQ [1..1]
DaysSupplyclassCode*: <= SPLYmoodCode*: <= RQOeffectiveTime*: IVL<TS> [1..1] (Dispensing window)expectedUseTime*: IVL<TS> [1..1] (Prescription duration)
Mandatory forRepeat Dispensing Prescriptionsabsent otherwise
Constraint: effectiveTime
1..1 pertinentDosageInstructions *
typeCode*: <= PERTinversionInd*: BL [1..1] "false" (Fixed)contextConductionInd*: BL [1..1] "true" (Fixed)negationInd*: BL [1..1] "false" (Fixed)seperatableInd*: BL [1..1] "true" (Fixed)
pertinentInformation4
1..1 pertinentLineItemQuantity *
typeCode*: <= PERTinversionInd*: BL [1..1] "false" (Fixed)contextConductionInd*: BL [1..1] "true" (Fixed)negationInd*: BL [1..1] "false" (Fixed)seperatableInd*: BL [1..1] "true" (Fixed)
pertinentInformation2
0..1 pertinentDaysSupply
typeCode*: <= PERTinversionInd*: BL [1..1] "false" (Fixed)contextConductionInd*: BL [1..1] "true" (Fixed)negationInd*: BL [1..1] "false" (Fixed)seperatableInd*: BL [1..1] "true" (Fixed)
pertinentInformation7
CareEventRefclassCode*: <= ACTmoodCode*: <= ActMoodid*: II [1..1]
1..1 pertinentCareEventRef
typeCode*: <= PERTinversionInd*: BL [1..1] "false" (Fixed)contextConductionInd*: BL [1..1] "false" (Fixed)negationInd*: BL [1..1] "false" (Fixed)seperatableInd*: BL [1..1] "true" (Fixed)templateId*: II [1..1] "CSAB_RM-NPfITUK10.sourceOf1"
pertinentInformation6
Note:PoC Event that resulted in thisprescription being generated
Note:The quantity can beeither days to supplyor amount
optionional butonly for Repeat Dispensing
Constraint: expectedUseTime
CMET: (PAT) R_Patient
[identifiedETP](COCT_MT050012UK04)
0..1 roleName
DosageInstructionsclassCode*: <= OBSmoodCode*: <= EVNcode*: CV CNE [1..1] <= PrescriptionAnnotation "DI" (Fixed)value*: ST [1..1] (Dose Instructions)
AdditionalInstructionsclassCode*: <= OBSmoodCode*: <= EVNcode*: CV CNE [1..1] <= PrescriptionAnnotation "AI" (Fixed)value*: ST [1..1] (Additional Instructions)
0..1 pertinentAdditionalInstructions
typeCode*: <= PERTinversionInd*: BL [1..1] "false" (Fixed)contextConductionInd*: BL [1..1] "true" (Fixed)negationInd*: BL [1..1] "false" (Fixed)seperatableInd*: BL [1..1] "true" (Fixed)
pertinentInformation1
1..1 pertinentDispensingSitePreference *
typeCode*: <= PERTinversionInd*: BL [1..1] "false" (Fixed)
contextConductionInd*: BL [1..1] "true" (Fixed)negationInd*: BL [1..1] "false" (Fixed)
seperatableInd*: BL [1..1] "true" (Fixed)
pertinentInformation1DispensingSitePreferenceclassCode*: <= OBSmoodCode*: <= EVNcode*: CV CNE [1..1] <= PrescriptionAnnotation "DSP" (Fixed)value*: CV [1..1] <= DispensingSitePreference
HL7 RMIMHL7 RMIMe.g. e.g. Parent PrescribingParent Prescribing
Parent Prescribing RMIM v3.1.06 (2004)

Detail fromParent Prescribing RMIM v3.1.06 (2004)
HL7 HL7 Clinical DocumentationClinical Documentation
Clinical Document Architecture (CDA)Exchange model for clinical documents
Leverages XML, HL7 RIM and coded vocabularies
XML Syntax & framework for expressing clinical document semantics
Discharge Summary, Imaging Report, Admission & Physical etc
Minimum version ~ Dublin Core
XML-RIM metadata Header, content not marked up
Level 3 CDA implies extensively marked up content also
ANSI Standard November 2000
HL7 HL7 Clinical DocumentationClinical Documentation
Clinical Context Management Specification (CCOW)Protocol for linking multiple applications
Means to identify common clinical ‘context’ across boundaries
= identity of patient and previous encounters
ANSI Standard September 2000
TemplatesRIM-compliant CDA data structures
Express specific clinical data e.g. BP
May be combined to define template for larger datasets
Embedded data validation rules
(thus,similar to OpenEHR archetypes)

About Standards…About Standards…
SummarySummary
Tool for interoperability
Extensive and costly activity in health informatics
Complex outputChiefly, information models (UML etc)
Cautious industrial buy-in: what’s the migration pathway?
HL7 Predominant body at the moment