standards for medium secure units - royal college of ... standards for medium secure units...
TRANSCRIPT
Charity registration no. 228636
Standards for
Medium Secure Units Quality Network for Medium Secure Units
Edited by Sarah Tucker and Tessa Hughes 1st Edition CRTU 044

1: Relational Security 1
2: Procedural Security 5
3: Physical Security 7
4: Personal Dignity 10
5: Core Interventions 12
6: Workforce Development and Training 14
7: Equality and Diversity 15
8: Workforce, Recruitment, Retention 15
9: Supervision and Support 16
10: Patient Involvement 17
11: Advocacy 17
12: Carer Involvement 17
13:Interagency Working 18
14: Management 18
Appendix 1: References 19
Appendix 2: Advisory Group 22
Appendix 3: Project Team 23
Appendix 4: Acknowledgements 24
Appendix 5: Standards Order Form 30
Appendix 6: Standards Feedback Form 31
Contents

Foreword It is a great pleasure to introduce these Standards for Medium Secure Units and to welcome their implementation by the new Quality Network for Medium Secure Units. These standards specifically for medium secure units are very long-needed. Moreover, their implementation promises to play a key role in assisting pioneer members of the quality network to develop and respond to the objectives identified by the Department of Health’s Standards for Better Health. The Department of Health with specialist commissioners will continue work on refining standards for medium security. This work will be incorporated into the implementation of the standards by the Quality Network for Medium Secure Units in an on-going way. In turn the work of the Quality Network will inform the development of the Department of Health standards. New policy will not lead to improvement unless front-line staff are fully involved in the process of change. This exciting new quality network aims to engage and support front-line staff of all professions. The well-tested quality network model offers frontline staff invaluable opportunities to explore common difficulties and learn from each other, during standards-based peer-review visits. These service standards for medium secure units provide often-isolated individual units the opportunity to speak to commissioners with a united voice about common problems. The changes occurring to commissioning in England and Wales make it timely to engage and involve commissioners with this initiative as the pressing next stage. It seems inevitable that the future will bring about the need for accreditation, and the implementation of these standards promises to prime units to move in this direction. Dr John O’Grady Chair of the Forensic Faculty, Royal College of Psychiatrists


Introduction The Standards for Medium Secure Units (MSUs) include all the Department of Health standards (Health Offender Partnerships, 2004) and extra standards identified by members of the Quality Network for MSUs from a supplementary set. The development of this supplementary set and the editing of the final document is summarised below. Department of Health standards are marked (DH) and supplementary standards are marked (S). 1) The Development of the Supplementary Standards for MSUs 1.1) Literature Review and Development of Draft Standards A bibliography of key documents was compiled from professional bodies, regulators, policy, other quality networks, and experts (see Appendix 1). These were reviewed and standards were identified or derived from guidance and recommendations. A pre-consultation draft of supplementary standards was developed, informed by, and referenced to, the literature. 1.2) Consultation A consultation took place at a stakeholder workshop on 23 January 2006 as part of the Third National Conference on Research and Development in Medium Secure Psychiatric Units at the Institute of Psychiatry (see Appendix 4). The standards consisted of ten sections. Stakeholders worked in five small groups and were asked to comment on two sections each. 1.3) Editing The process of consultation and incorporation of expert comments, staff member and ex-client member comments ensured that the draft standards reflect contemporary medium secure unit practice. 2) Augmentation of the Department of Health Standards for MSUs 2.1) Consultation and Editing The Department of Health Standards for MSUs were numbered and sent out for consultation to members of the Quality Network for MSUs. Members were asked to read through the Department of Health Standards and then identify Supplementary standards which would usefully augment the Department of Health set. The Department of Health Standards for MSUs were therefore augmented, but not changed. 2.2) Standards for Better Health The resulting standards were mapped on to the Department of Health Standards for Better Health (2004) and an identifying code was added in the far right column. This enables members of the Quality Network for MSUs to use local review reports as evidence of compliance with Standards for Better Health. This is required in the Healthcare Commission’s Annual Health Check. Where the column is left blank there is no obvious corresponding standard.


1
1. Relational Security
Relational Security – Admission and Assessment
Source Standards for Better
Health
1.1 Units have systems and processes in place that ensure good quality multi-disciplinary assessment prior to admission
(DH)
1.2
The assessment takes into account relevant history, problems, issues, legal status and risks
(S)
1.3
There is a clearly defined process for the admission of people to the unit
(S)
1.4
There are written referral criteria
(S)
1.5
Staff and patients provide written information about the unit that addresses the needs of prospective patients, referrers and other relevant professionals
(S)
C16
1.6
The information provided contains a clear description of the aims of admission, the current programme and modes of treatment
(S)
C16
1.7
Measures are in place to record and audit refusals, terminated referrals and waiting lists
(S)
1.8
Where patients are refused admission to the service, the reasons for refusal are explained to the person and referrer, and they are informed about alternative options
(S)
1.9
Those presenting as high risk or with more severe conditions are given priority with assessment
(S)
C19
1.10
All patients have an initial treatment plan in place within 24 hours following admission
(DH)
C19
1.11
All patients on admission have an initial risk assessment
(DH)
C7c; C1b

2
Relational Security - Care and Treatment
Source Standards for Better
Health
1.12 All patients are managed within the framework of the CPA process
(DH)
C5a
1.13
The staff team develop a written care pathway in consultation with each patient, within the limits of safety and risk assessment
(S)
C17
1.14
Patients are given a copy of the management or care plan or have ready access to it
(S)
C16
1.15
There is a core day described in each patient's individualised care plan (A description of the core day may also be found elsewhere e.g. in ward programme or individual timetable)
(DH)
C16
1.16
There are regular case reviews in line with good practice ECC/CPA guidelines
(DH)
C5a
Relational Security - Team Composition and Skills
1.17 There are processes in place which demonstrate an evaluated staffing profile to meet the needs of the patients (e.g. skills assessment and needs assessment)
(DH)
C5b; C5c;
C11a
1.18
There are clear and effective systems for communication and handover within staff teams
(DH)
C1b
1.19
There are regular multi-disciplinary team meetings for clinical matters and administration, and the team is consulted on relevant management decisions such as developing and reviewing operational policy
(S)
C5b
1.20
The ratio of Consultant Psychiatrists to medium secure beds is 1: 14
(DH)
1.21
There are multi-disciplinary teams identified as part of the staffing establishment, with each team including psychiatrists, nurses, psychologists, occupational therapists, and social workers
(DH)
1.22
There is at least one nurse holding the RMN qualification on duty at all times
(S)
1.23
At least four staff hold an appropriate qualification on duty per shift and two at night-time (Grade E-H)
(S)

3
Relational Security - Team Composition and Skills cont’d
Source Standards for Better
Health
1.24 A typical unit with 10-12 places includes at least one WTE SpR or equivalent
(S)
1.25
A typical unit with 10-12 places includes at least one level two SHO
(S)
1.26
In a typical unit about one WTE clinical psychologist is provided
(S)
1.27
In a typical unit about one WTE Occupational Therapist is provided
(S)
1.28
1.0 WTE social work input is provided in a typical 10-12 bed unit
(S)
1.29
The unit has access to a substance misuse specialist or dual diagnosis specialist either working as part of an integrated or parallel model
(S)
1.30
The unit has access to a range of practitioners offering psychotherapeutic sessions
(S)
1.31
The unit has access to a range of education professionals which include teachers, a special educational needs co-ordinator, an educational psychologist, and career guidance
(S)
1.32
All staff can demonstrate an understanding of their role in relation to meeting the complex needs of patients
(DH)
1.33
The variance between staff in post and establishment is minimised
(DH)
C11a
1.34
The number of nursing staff on the unit is sufficient to safely meet the needs of the patients at all times
(S)
1.35
Extra nursing cover is available when needed, e.g. there is access to additional on-call staff in emergency
(S)
1.36
The unit is staffed by permanent staff and agency staff are used only in exceptional circumstances
(S)
C11a
1.37
There are published and monitored plans to deliver therapy and treatments in line with planned programmes
(DH)
C5a;C5b

4
Relational Security - Risk and Safety
Source Standards for Better
Health
1.38 The unit provides an annual report on risks and incidents to enable the unit to learn from risks and provide a safer environment
(S)
C1a
1.39
The unit promotes an open, blame-free culture for reporting incidents
(S)
C8a
1.40
There is a policy on clinical risk assessment
(S)
C7c
1.41
The unit keeps records of the following measures concerning risk assessment:
(S)
C7c
1.42
Number of periods of escorted access taken by in-patients
(S)
C7c
1.43
Number of periods of unescorted access taken by in-patients
(S)
C7c
1.44
Number of abscondings from escorted access as percentage of escorted access taken
(S)
C7c
1.45
Number of failures to return from unescorted access as percentage of access
(S)
C7c
1.46
Number of escapes within last 12 months
(S)
C7c
Relational Security - Discharge and Transfer
1.47 The place of discharge is known before admission where possible
(S)
1.48
There is a frequent decision-making forum, e.g. weekly ward rounds rather than monthly reviews, to prevent unnecessary delays to discharge
(S)
1.49
Discharge targets are agreed as part of the discharge planning process
(S)
1.50
When a patient needs to transfer to services for older people, a joint review is undertaken to ensure effective hand-over takes place
(S)
C6
1.51
A CPA meeting is held for all patients to plan discharge
(S)
1.52
Section 117 meetings are held prior to the discharge of all patients detained under a treatment section of the Mental Health Act
(S)

5
2.Procedural Security
Source Standards for Better
Health
2.1 There are relevant, accessible, authorised, up to date policies (no more than 3 years old) and procedures in place to address the areas of practice identified above
(DH)
Procedural Security - Care and Treatment
2.2 There are written admission and discharge procedures
(S)
2.3
There are written policies and procedures that implement the requirements of the Care Programme Approach (CPA)
(S)
2.4
There is a procedure regarding obtaining consent from patients
(S)
C13b
Procedural Security - Risk and Safety
2.5 There is a policy in place on the management of aggression and violence which is compliant with NICE 25
(DH)
C3
2.6
The unit has procedures for the management of bullies and for those who have been bullied
(S)
C14c
2.7
There is a policy in place for the observation and monitoring of patients who are at risk of suicide
(S)
C1b
2.8
The procedure for resuscitation of patients is clearly documented, resuscitation equipment is available and its location is clearly identified
(S)
2.9
There are policies, procedures and guidance for infection control practice
(S)
C4a
2.10
There is a searching policy in relation to patients, visitors, bedrooms, and off ward areas
(DH)
C20a
2.11
There are contingency plans agreed with the police and emergency services (NICE 25) covering as a minimum: hostage taking, serious disorder, riot, escape
(DH)
C1b

6
Procedural Security - Risk and Safety cont’d
Source Standards for Better
Health
2.12 There is a policy on the control of illicit substances covering (a) treatment of substance misuse; (b) education on the dangers of substance abuse; (c) advice to visitors on the dangers of passing illicit/unauthorised substances; (d) a protocol with police for when drugs are discovered; (e) a policy on "searching with cause" for drugs
(DH)
2.13
There is a policy for administering drugs at dosages above BNF recommendations
(S)
2.14
There are clear contingency plans in place which meet NICE Clinical Guideline 25 Systems (including: systems to ensure the management of serious incidents, systems for review (both internal and external to organisation), methods to ensure learning, audit process of actions with time scales following review, and clear lines of responsibility and accountability)
(DH)
C1a
2.15
There is a policy for prompt response to staff alarms
(S)
C1b
2.16
There is a procedure for evacuation in case of fire which is rehearsed at regular intervals
(S)
2.17
There is a procedure in place to ensure that perimeter fence inspection processes are audited
(S)
C20a
2.18
There is a protocol in place for the risk assessment of patient access to telephones, the internet and cameras
(S)
C7c
2.19
Units have in place appropriate procedures to manage the risks created by the movement of patients within the unit and externally (e.g. for hospital/court visits, visitors and staff) proportionate to the level of risk posed, and the effect of those measures on the rights of patients, staff and visitors, and the patients quality of life.
(S)
C7c; C13a
Procedural Security - Responsibilities and Rights
2.20 There is a policy in place to ensure issues of equality and diversity are regularly monitored
(S)
C18
2.21
The unit has a written complaints procedure
(S)
C14a
2.22
The unit holds data in compliance with legislation (including the Data Protection Act 1984, MAPPA, Caldicott Principle) to ensure maintenance of confidentiality
(S)
C9; C13c
7
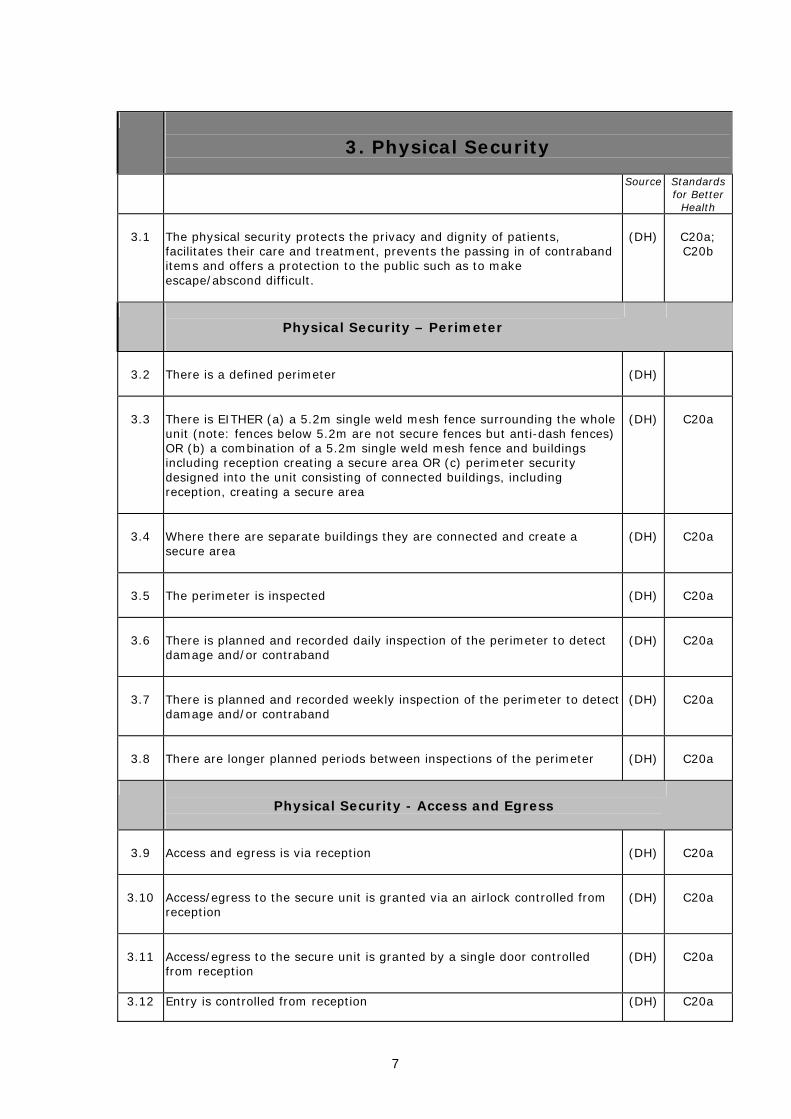
3. Physical Security
Source Standards for Better
Health
3.1 The physical security protects the privacy and dignity of patients, facilitates their care and treatment, prevents the passing in of contraband items and offers a protection to the public such as to make escape/abscond difficult.
(DH)
C20a; C20b
Physical Security – Perimeter
3.2
There is a defined perimeter
(DH)
3.3
There is EITHER (a) a 5.2m single weld mesh fence surrounding the whole unit (note: fences below 5.2m are not secure fences but anti-dash fences) OR (b) a combination of a 5.2m single weld mesh fence and buildings including reception creating a secure area OR (c) perimeter security designed into the unit consisting of connected buildings, including reception, creating a secure area
(DH)
C20a
3.4
Where there are separate buildings they are connected and create a secure area
(DH)
C20a
3.5
The perimeter is inspected
(DH)
C20a
3.6
There is planned and recorded daily inspection of the perimeter to detect damage and/or contraband
(DH)
C20a
3.7
There is planned and recorded weekly inspection of the perimeter to detect damage and/or contraband
(DH)
C20a
3.8
There are longer planned periods between inspections of the perimeter
(DH)
C20a
Physical Security - Access and Egress
3.9
Access and egress is via reception
(DH)
C20a
3.10
Access/egress to the secure unit is granted via an airlock controlled from reception
(DH)
C20a
3.11
Access/egress to the secure unit is granted by a single door controlled from reception
(DH)
C20a
3.12 Entry is controlled from reception (DH) C20a

8
Physical Security - Locking System and Keys
Source Standards for Better
Health
3.13 There is a secure locking system in place
(DH)
C20a
3.14
There is a secure locking system - either manual, electronic, magnetic or a combination of these, with backup replacement in the event of a compromise or failure AND a separate locking suite for doors/locks within the perimeter or providing access to it
(DH)
C20a
3.15
There is a secure locking system - either manual, electronic, magnetic or a combination of these, with a separate locking suite for doors/locks within the perimeter or providing access to it, but with no backup replacement
(DH)
C20a
3.16
Checking of secure keys takes place
(DH)
C20a
3.17
Secure keys are accounted for and reconciled by reception twice daily, normally at end of main shift and at night (Note that reconciliation of keys means that all keys held in reception and issued are accounted for in a single check)
(DH)
C20a
3.18
Secure keys are accounted for and reconciled by reception once daily
(DH)
C20a
3.19
Secure keys are accounted for and reconciled by reception less than once a day
(DH)
C20a
Physical Security – Alarms
3.20
All staff who work in the secure unit are issued with a personal alarm
(DH)
C20a
3.21
There is written evidence that staff personal alarms are regularly tested
(S)
C20a
3.22
There is a way for patients to raise an alarm in an emergency
(S)
C20a

9
Physical Security - Restraint and Seclusion
Source Standards for Better
Health
3.23 The unit operates within the appropriate legal framework in relation to the use of physical restraint
(S)
C5a
3.24
The circumstances and justification for using physical restraint are recorded immediately; every such incident is documented within 24 hours (one working day); the RMO is informed and a report is submitted by the nurse in charge to the Trust management in line with Trust incident reporting policy
(S)
3.25
If seclusion is used, there is a designated seclusion facility available, which is designed to minimise risk of injury and where the patient is continually monitored
(S)
Physical Security- Environment and Facilities
3.26 The unit is well designed and has the necessary facilities and resources for people requiring medium secure care
(S)
C21
3.27
There are areas with clear lines of sight to enable staff to monitor patients who need closer observation
(S)
C20a
3.28
Entrances and exits are designed to enable staff to see who is entering or leaving
(S)
C20a
3.29
Patients have supervised access to computers with relevant risk assessment
(S)
3.30
The unit is managed in line with Health and Safety legislation and guidance
(S)
C20a
3.31
All confidential case materials, e.g. notes, are kept in locked cabinets or locked offices
(S)
C20b
3.32
There is a policy in place for child visiting/contact with children
(DH)
C2

10
4.Personal Dignity
Personal Dignity - Healthcare Access and Provision
Source Standards for Better
Health
4.1 There is good access to primary healthcare services
(DH)
C6
4.2
There is access to good quality physical healthcare and screening
(DH)
C6
4.3
The in-patient team has good access to a range of services, as appropriate to the needs of the patients. These include the following:
(S)
4.4
General practitioner services
(S)
C6
4.5
Laboratory services
(S)
C6
4.6
Neurological, cardiology and dental services
(S)
C6
4.7
Substance and alcohol misuse services
(S)
C6
Personal Dignity - Responsibilities and Rights
4.8 Staff demonstrate respect for patients
(DH)
C13a
4.9
It is explained how complaints may be made without the knowledge and involvement of the person complained of
(S)
C14b
4.10
Staff are made aware of complaints that are relevant to their work and the outcome of the complaints process
(S)
C7b
4.11
Staff ensure basic needs are met to ensure personal dignity (e.g. privacy, clothing etc)
(DH)
C13a
4.12
Patients may sleep in privacy and in areas separate from patients of the opposite sex, within the limits of safety and risk assessment
(S)
C13a; C20b
4.13
The food provided is of a good standard
(S)
C15a
11
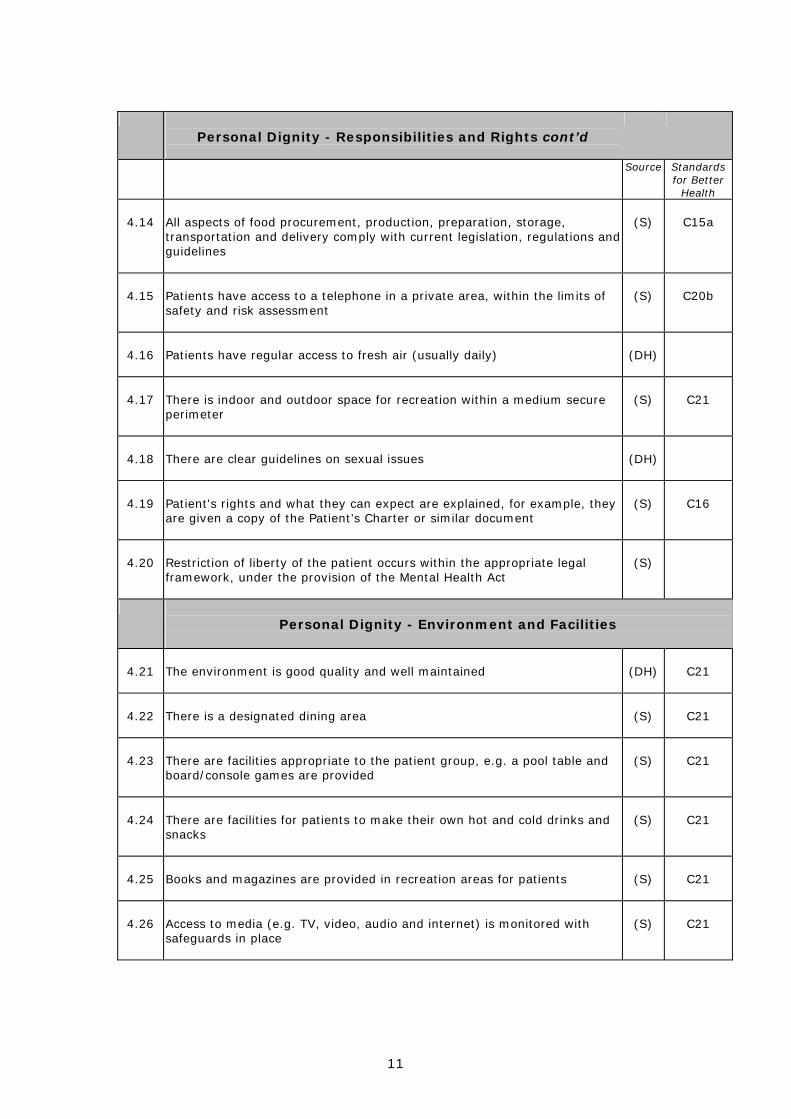
Personal Dignity - Responsibilities and Rights cont’d
Source Standards for Better
Health
4.14 All aspects of food procurement, production, preparation, storage, transportation and delivery comply with current legislation, regulations and guidelines
(S)
C15a
4.15
Patients have access to a telephone in a private area, within the limits of safety and risk assessment
(S)
C20b
4.16
Patients have regular access to fresh air (usually daily)
(DH)
4.17
There is indoor and outdoor space for recreation within a medium secure perimeter
(S)
C21
4.18
There are clear guidelines on sexual issues
(DH)
4.19
Patient's rights and what they can expect are explained, for example, they are given a copy of the Patient’s Charter or similar document
(S)
C16
4.20
Restriction of liberty of the patient occurs within the appropriate legal framework, under the provision of the Mental Health Act
(S)
Personal Dignity - Environment and Facilities
4.21 The environment is good quality and well maintained
(DH)
C21
4.22
There is a designated dining area
(S)
C21
4.23
There are facilities appropriate to the patient group, e.g. a pool table and board/console games are provided
(S)
C21
4.24
There are facilities for patients to make their own hot and cold drinks and snacks
(S)
C21
4.25
Books and magazines are provided in recreation areas for patients
(S)
C21
4.26
Access to media (e.g. TV, video, audio and internet) is monitored with safeguards in place
(S)
C21

12
5.Core Interventions
Core Interventions - Care and Treatment
Source Standards for Better
Health
5.1 There are clear care pathways identified which are reviewed regularly
(DH)
5.2
There is a range of clinically effective treatments, therapies, recreational and life skills training and support available
(DH)
5.3
A structured therapeutic programme is run during weekdays
(S)
5.4
A comprehensive range of treatments is available at the unit. This will depend upon the nature of the group of patients, but is likely to include:
(S)
5.5
Art therapy
(S)
5.6
Behavioural therapy
(S)
5.7
Cognitive therapy (e.g. CBT, brief solution focused therapy, anger management)
(S)
5.8
Drama therapy
(S)
5.9
Drug therapy
(S)
5.10
Family therapy and family work
(S)
5.11
Group therapy
(S)
5.12
Music therapy
(S)
5.13
Occupational therapy
(S)
5.14
Offender related treatments (where these are not part of the core programme units have access to specialist offender programme such as SOTP)
(S)
5.15
Social skills training
(S)
13
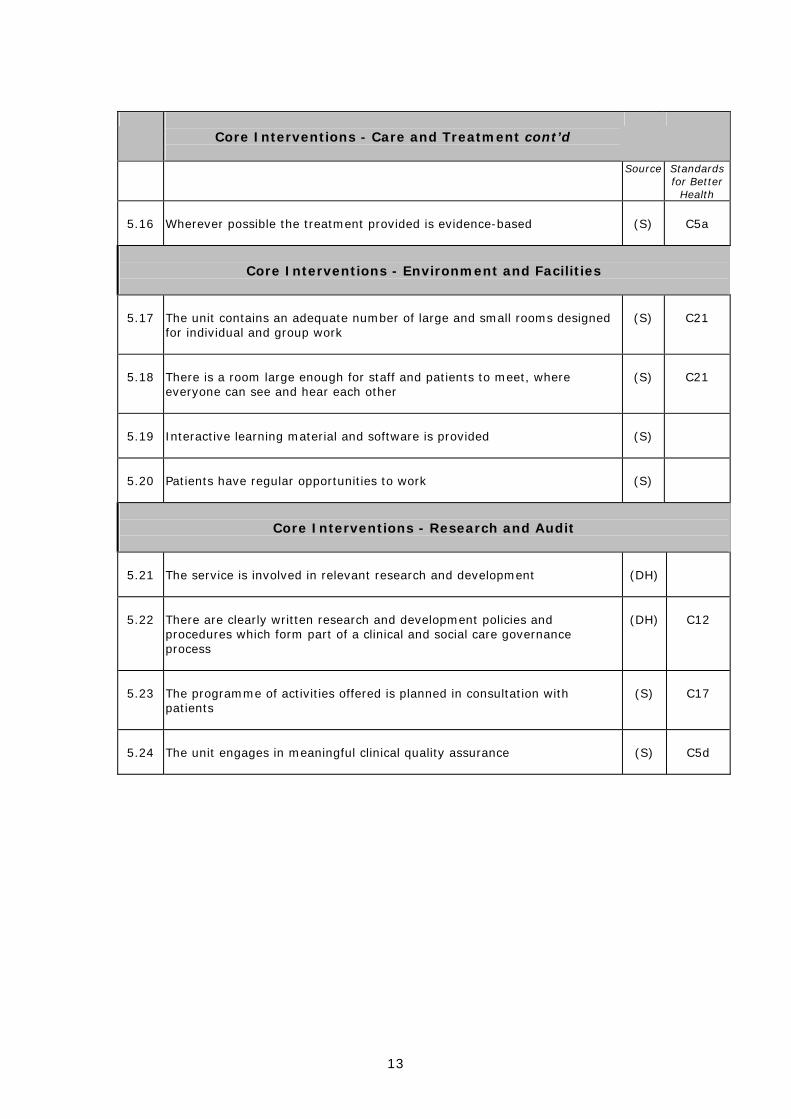
Core Interventions - Care and Treatment cont’d
Source Standards for Better
Health
5.16 Wherever possible the treatment provided is evidence-based
(S)
C5a
Core Interventions - Environment and Facilities
5.17 The unit contains an adequate number of large and small rooms designed for individual and group work
(S)
C21
5.18
There is a room large enough for staff and patients to meet, where everyone can see and hear each other
(S)
C21
5.19
Interactive learning material and software is provided
(S)
5.20
Patients have regular opportunities to work
(S)
Core Interventions - Research and Audit
5.21 The service is involved in relevant research and development
(DH)
5.22
There are clearly written research and development policies and procedures which form part of a clinical and social care governance process
(DH)
C12
5.23
The programme of activities offered is planned in consultation with patients
(S)
C17
5.24
The unit engages in meaningful clinical quality assurance
(S)
C5d

14
6: Workforce Development and Training
Source Standards
for Better Health
6.1
There is a workforce training and development strategy in place
(DH)
C11a
6.2
All staff have an individual personal development plan which is updated annually
(DH)
C8b
6.3
Training has been provided in the following:
(S)
C11a
6.4
Clinical governance
(S)
C7a; C5d;
C11a
6.5
Culturally sensitive practice, disability awareness, and other equality issues
(S)
C7e; C11a
6.6
Legal frameworks such as the Mental Health Act 1983 and the revised Code of Practice
(S)
C11a
6.7
Management of imminent and actual violence, breakaway techniques and restraint measures
(S)
C11a
6.8
Resuscitation
(S)
C11a
6.9
The issue of touching in general and the problem of sexual attraction between staff and patients
(S)
C11a
6.10
Unit managers who are nursing staff have had further training in management and team leadership
(S)
C11a
6.11
Training needs are informed through the skills needed within the unit, staff development plans and supervision systems which have assessed in the last year
(S)
C5c
15
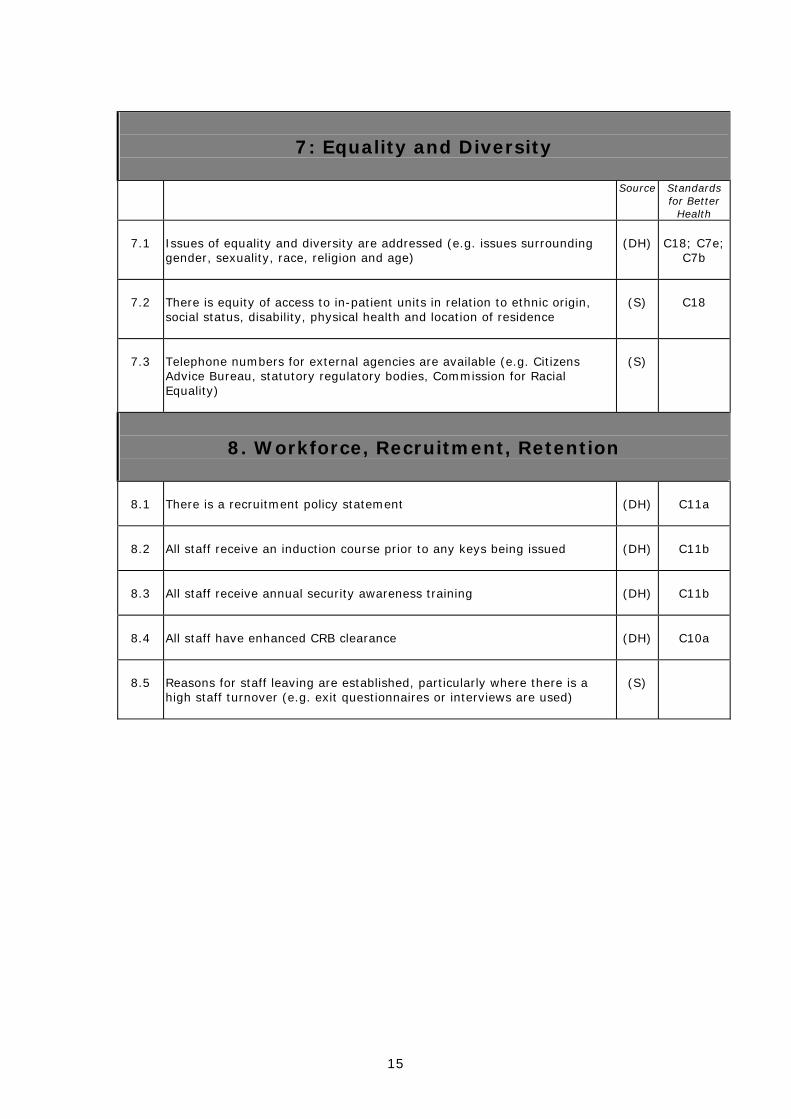
7: Equality and Diversity
Source Standards
for Better Health
7.1
Issues of equality and diversity are addressed (e.g. issues surrounding gender, sexuality, race, religion and age)
(DH)
C18; C7e;
C7b
7.2
There is equity of access to in-patient units in relation to ethnic origin, social status, disability, physical health and location of residence
(S)
C18
7.3
Telephone numbers for external agencies are available (e.g. Citizens Advice Bureau, statutory regulatory bodies, Commission for Racial Equality)
(S)
8. Workforce, Recruitment, Retention
8.1 There is a recruitment policy statement
(DH)
C11a
8.2
All staff receive an induction course prior to any keys being issued
(DH)
C11b
8.3
All staff receive annual security awareness training
(DH)
C11b
8.4
All staff have enhanced CRB clearance
(DH)
C10a
8.5
Reasons for staff leaving are established, particularly where there is a high staff turnover (e.g. exit questionnaires or interviews are used)
(S)

16
9: Supervision and Support
Source Standards
for Better Health
9.1
There is a programme of clinical supervision and support to meet the needs of all staff
(DH)
C5b
9.2
Adequate time is made available to enable staff supervision and support to be delivered
(DH)
C5b
9.3
Staff take up of supervision and support is regularly monitored and audited
(DH)
C5b;C5d
9.4
All staff receive regular supervision totalling at least one hour per month from a person with appropriate experience
(S)
C5b
9.5
Junior staff have regular supervision totalling at least one hour per week and are able to contact a senior colleague as necessary
(S)
C5b
9.6
There are regular forums for all staff to reflect on their experience of the work
(S)
C5b
9.7
There is a regular staff support group, ideally weekly
(S)
17
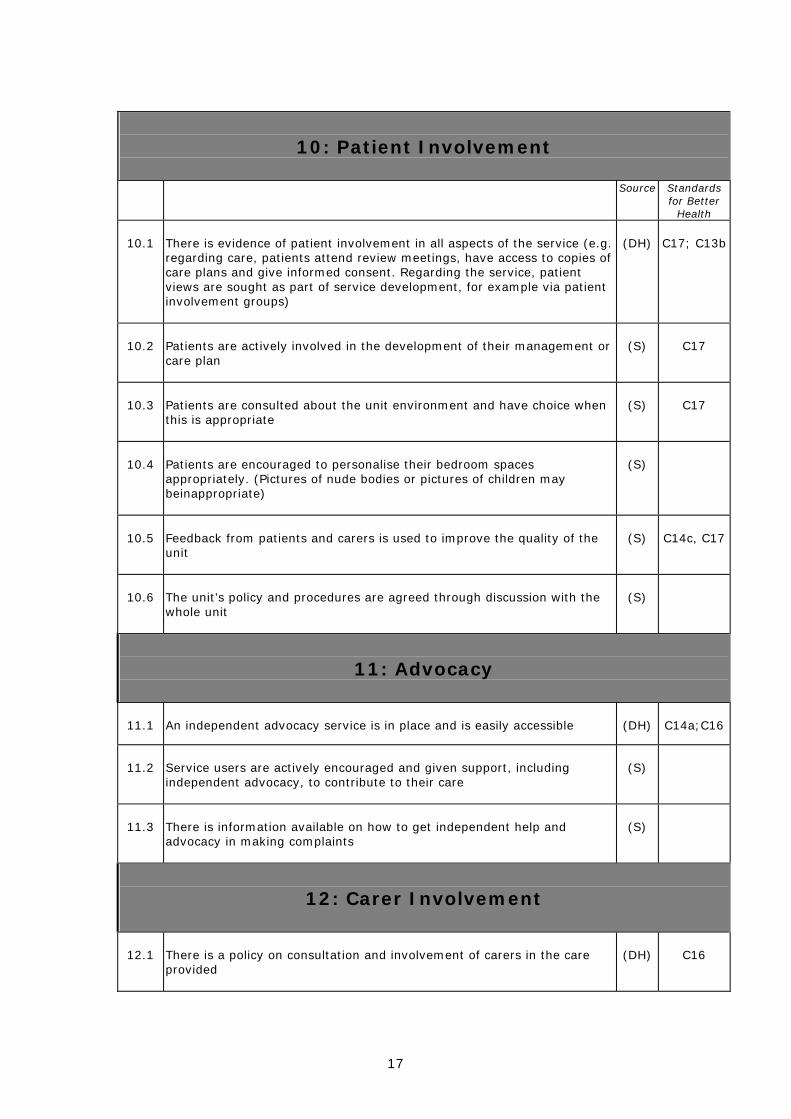
10: Patient Involvement
Source Standards
for Better Health
10.1
There is evidence of patient involvement in all aspects of the service (e.g. regarding care, patients attend review meetings, have access to copies of care plans and give informed consent. Regarding the service, patient views are sought as part of service development, for example via patient involvement groups)
(DH)
C17; C13b
10.2
Patients are actively involved in the development of their management or care plan
(S)
C17
10.3
Patients are consulted about the unit environment and have choice when this is appropriate
(S)
C17
10.4
Patients are encouraged to personalise their bedroom spaces appropriately. (Pictures of nude bodies or pictures of children may beinappropriate)
(S)
10.5
Feedback from patients and carers is used to improve the quality of the unit
(S)
C14c, C17
10.6
The unit’s policy and procedures are agreed through discussion with the whole unit
(S)
11: Advocacy
11.1 An independent advocacy service is in place and is easily accessible
(DH)
C14a;C16
11.2
Service users are actively encouraged and given support, including independent advocacy, to contribute to their care
(S)
11.3
There is information available on how to get independent help and advocacy in making complaints
(S)
12: Carer Involvement
12.1 There is a policy on consultation and involvement of carers in the care provided
(DH)
C16

18
13: Inter Agency Working
Source Standards
for Better Health
13.1
There is inter-agency working (e.g. meeting regularly with other MSUs, drug action teams, the police, community mental health teams, external probation and local community services)
(DH)
C22a
13.2
The Mental Health Act Commission visits are facilitated and co-operated with
(S)
C22a
13.3
There is an identified duty doctor available at all times to attend the unit
(S)
C22a
14. Management
14.1 There are clear governance arrangements for secure services at Board level
(DH)
C7a
14.2
There are finance management systems in place which ensure financial probity
(DH)
C7d
14.3
The management of patient information complies with Caldicott
(DH)
C9; C13c
14.4
There is accurate information which meets the requirements of the MHMDS
(DH)
19
Appendix 1: References 1) Standards for Medium Secure Units – Health Offender Partnerships,
Department of Health (DH) Collins, M. & Davies, S. (2003) Security Needs Assessment Profile Department of Health (1993) NHS Estates Guidelines Department of Health (1994) Guidance on the discharge of mentally disordered people and their continuing care in the community HSG (94) 27 Department of Health (1999) Code of Practice to the Mental Health Act 1983 Department of Health (2000) An organisation with a memory Department of Health (2001) Building a safer NHS for patients – implementing an organisation with a memory Department of Health (2003) Checklist of Recommendations from the Victoria Climbie Inquiry Department of Health (2005) Independent investigation of adverse events in mental health services National Institute of Clinical Excellence (2005) Violence, The short-term management of disturbed / violent behaviour in in-patient settings and emergency departments Royal College of Psychiatrists for the Healthcare Commission (2005) National Audit of Violence 2) Supplementary Standards for Medium Secure Units – Centre for
Quality Improvement, Royal College of Psychiatrists (S) Department of Health (1998) The Patient’s Charter: Privacy and Dignity and the provision of single sex accommodation Department of Health (1999) Code of Practice Mental Health Act 1983 Department of Health (2000) The NHS Plan - Better hospital food, sections 4.16 - 4.18 Department of Health (2001) Adult Mental Health: National Service Framework (and the NHS Plan) Department of Health (2001) Safety First - Five-Year Report of the National Confidential Inquiry into Suicide and Homicide by People with Mental Illness Department of Health (2002) Women’s Mental Health: Into the Mainstream Strategic Development of Mental Health Care for Women.
20
Department of Health (2002) Mental Health Policy Implementation Guide: National Minimum Standards for General Adult Services in Psychiatric Intensive Care Units (PICU) and Low Secure Environments Department of Health (2002), Mental Health Policy Implementation Guide: Adult Acute Inpatient Care Provision Department of Health, National Institute for Mental Health for England, The Sainsbury Centre for Mental Health (2004) The Ten Essential Shared Capabilities – A Framework for the Whole Mental Health Workforce, Roslyn Hope. Department of Health (2004) Organising and Delivering Psychological Therapies Department of Health (2006) Standards for Better Health Faulkner, A. & Morris, B. (2003) User involvement in forensic mental health research and development, NHS National Programme on Forensic Mental Health Research and Development Forensic Mental Health Services Managed Care Network (2005) Care standards for Forensic Mental Health Inpatient Facilities in Scotland (draft for consultation) Healthcare Commission (2004) Assessment for improvement: Understanding the Standards Health and Social Care Advisory Service (2005) Standards for the Quality Improvement Review of Medium Secure Units, Allured and Somekh (eds.) Her Majesty’s Inspector Prisons (2004) Expectations London Development Centre for Mental Health, the King’s Fund and London’s Mental Health Provider Trusts (2004), Acute Care Collaborative Standards London Development Centre for Mental Health (2005) Developing a Personality Disorder Framework for London Mental Health Act Commission (2004) Placed Amongst Strangers., Tenth Biennial Report National Health Service Executive (2000) Safety, privacy and dignity in mental health units: Guidance on mixed sex accommodation for mental health services National Institute for Clinical Excellence (2005) Violence: The short-term management of disturbed/violent behaviour in psychiatric in-patient settings and emergency departments. Clinical Guideline 25 National Institute for Mental Health for England (2003) Policy implementation guidance for the development of services for people with personality disorder - ‘Personality disorder: No longer a diagnosis of exclusion National Institute for Mental Health for England (2004) Mental Health Policy Implementation Guide: Developing Positive Practice to Support the Safe and Therapeutic Management of Aggression and Violence in Mental Health In-patient Settings National Patient Safety Agency (2004) Safer Wards for acute Psychiatry: a review of the available evidence.

21
Royal College of Psychiatrists (1996) Wish you were here? Ethical considerations in the admission of patients to substandard psychiatric units CR50 Royal College of Psychiatrists (1998) 'Not Just Bricks and Mortar': Report of the working group on the size, staffing, structure, siting and security of new acute adult psychiatric in-patient units CR62 Royal College of Psychiatrists (2001) Perinatal maternal mental health services. Recommendations for provision of services for childbearing women. CR88 Royal College of Psychiatrists (2002), Acute in-patient psychiatric care for young people with severe mental illness. Recommendations for commissioners, child and adolescent psychiatrists and general psychiatrists. CR106 Royal College of Psychiatrists (2003) Specialist Secure Psychiatric Care (Forensic Faculty) Royal College of Psychiatrists (2005) Service Standards for Therapeutic Communities, 4th Edition CRTU035 Royal College of Psychiatrists (2005) The Five-Fives Standards for the Commissioning of NHS Therapeutic Communities appendix 1 in Service Standards for Therapeutic Communities, 4th Edition (2005) CRTU035 Royal College of Psychiatrists and National Institute for Mental Health for England (2005) New Ways of Working for Psychiatrists Royal College of Psychiatrists (2006), Service Standards for Acute Psychiatric Wards. CRTU 040 Sainsbury Centre for Mental Health (1997) The National Visit. A one-day Visit to 309 Acute Psychiatric Wards Sainsbury Centre for Mental Health (1998), Acute Problems. A Survey of the Quality of Care in Acute Psychiatric Wards Sainsbury Centre for Mental Health (2002) Breaking the Circles of Fear: A review of the relationship between mental health services and African and Caribbean communities. Sainsbury Centre for Mental Health (2005) Acute Care 2004. A National Survey of Adult Psychiatric Wards in England Sainsbury Centre for Mental Health (2005) CPA care planning for service users who are repeatedly detained under the Mental Health Act Worrall, A (2005) ‘Clinical Governance Standards for Mental Health and Learning Disability Services: Enabling Front-line Staff’ in James A, Worrall A, Kendall T (eds) 2005. Clinical Governance in Mental Health and Learning Disability Services. London: Gaskell

22
Appendix 2: Advisory Group Kate Bailey Consultant Psychologist The Spinney Lorna Duggan Consultant Forensic Psychiatrist, St Andrews Health Care Mike Gatsi Senior Nurse, Three Bridges Regional Secure Unit John O’Grady (Chair) Consultant Forensic Psychiatrist Ravenswood House, Chair of Forensic Faculty, Royal College of Psychiatrists Tessa Hughes Quality Improvement Worker, Quality Network for Medium Secure Units Andrew Johns Consultant Forensic Psychiatrist, Dennis Hill Unit Harry Kennedy Consultant Forensic Psychiatrist, The Central Mental Health Hospital Paul Lelliott Consultant Psychiatrist/Director, College Research & Training Unit David Ndegwa Consultant Forensic Psychiatrist, SLAM Sarah Tucker Programme Manager, Quality Network for Medium Secure Units Roland Woodward Head of PD and Forensic Services, Affinity Healthcare Adrian Worrall Head of Centre for Quality Improvement

23
Appendix 3: Project Team The Quality Network for Medium Secure Units is part of the Royal College of Psychiatrists’ Centre for Quality Improvement: http://www.rcpsych.ac.uk/crtu/centreforqualityimprovement.aspx
John O’Grady Consultant Psychiatrist/Expert Advisor, Quality Network for Medium Secure Units Paul Lelliott Consultant Psychiatrist/Director, College Research & Training Unit Adrian Worrall Head of Centre for Quality Improvement Sarah Tucker Programme Manager, Quality Network for Medium Secure Units Tessa Hughes Quality Improvement Worker, Quality Network for Medium Secure Units

24
Appendix 4: Acknowledgements Particular thanks to Adrian Cree for his contribution to the preparation of the pre-consultation draft of the draft Supplementary Standards. We are also very grateful to the delegates of The Third National Conference on Research and Development in Medium Secure Psychiatric Units (23rd & 24th January 2006) who took part in the consultation workshop on the draft Supplementary Standards for Medium Secure Units.
Dr Ayobami Adekunle Laboratory Scientist Durojaiye Specialist Psychiatric Hospital
Mr Gordon Alderson Forensic Social Worker The John Howard Centre
Miss Victoria Altoft Assistant Psychologist Humber Centre For Forensic Psychiatry
Dr Tim Amos Senior Lectuer in Forensic Psychiatry
University of Bristol
Ms Ruth Ashworth Forensic Social Worker Bracton Centre
Mr Jude Atiyota House Officer Durojaiye Specialist Psychiatric Hospital
Mr John Baines Forensic Mental Health Social Worker
Guild Lodge
Mr David Beattie Cygnet Healthcare Cygnet Clinic Becton
Dr Gillian Bell Consultant Forensic Learning Disabilites Consultant
Northgate Hospital
Dr Richard Bennett Chartered Clinical Psychologist Reaside Clinic
Mr John Blakesley Team Leader Forensic Intensive Psychological Treatment Team
Dr Jennifer Blandford Head of Forensic Inpateint Psychology
Runwell Hospital
Mr Mark Booth Staff Nurse Ravenswood House
Mrs Carol Bowes Clinical Service Manager Fromeside
Mrs Christine Brown Senior Occupational Therapist The Humber Centre for Forensic Psychiatry
Dr Phillip Brown Consultant Forensic Psychiatrist Hutton Centre
Sue Browning Head of Social Work Bracton Centre
Mr Keith Bullivant Head of Nursing Linden House Hospital
Dr Harri Burgess Clinical Psychologist Dene Hospital
Karen Burgess Senior Lecturer in Occupational Therapy
Canterbury Christ Church University
Mr Jerome Burnell Lead Clinical Nurse Wood Lea Clinic
Mr Mick Burns Clinical Leader Yorkshire Centre for Forensic Psychiatry
Dr Walter Busuttil Medical Director and Consultant
Dene Hospital
Mrs Hannah Callum Psycho-Social Therapist Tony Hillis Unit
Ms Joanne Campbell-Antonio
Forensic Social Worker Bracton Centre
Dr Vinceno Cappiellot Psychiatrist Department of Psychiatry
Sinead Carroll Psychology Assistant HMP The Mount
Mrs Jane Carroll Senior Social Worker Ashworth Hospital

25
Dr Dawn Carson Consultant Forensic Psychiatrist Hutton Centre
Mrs Kate Caston Lead for High Secure & DSPD Department of Health
Dr Angelene Chester Psychiatric Registrar King Edward Memorial Hospital
Dr Lorraine Childs Clinical Psychologist St Andrew's Hospital
Dr Tom Clark Consultant Forensic Psychiatrist
Mrs Sheryle Cleave Ward Manager Cuthbert Ward
Mr David Cochrane Service Head Three Bridges Unit
Miss Katy Cogswell Occupational Therapist Countess of Chester Hospital
Dr P Collins Consultant Forensic Psychiatrist Newton Lodge
Mr Michael Collins Senior Nurse Researcher Rampton Hospital
Dr Haley Cooper Clinical Psychologist
Ms Kirsty Craig Deputy Manager Mental Health Team
St Mungos
Ms Lisa Dakin Senior Nurse Manager Bracton Centre
Dr Lisa Davies Chartered Forensic Psychologist
Dene Hospital
Dr Dominic De Souza Specialist Registrar in Forensic Psychiatry
John Howard Centre
Mr Paul Decker Assistant Psychologist Runwell Hospital
Mr Collins Denys Service User Researcher City University
Dr Humayon
Dewan Head of Psychiatry Beech House
Ms Yasmin Dipchan Forensic Social Worker Bracton Centre
Mr Jeremy Dixon Senior Practitioner in Forensic Social Work
Fromeside
Ms Pattie Ducie Social Worker East Kent Substance Misuse Team
Ms Eleanor Duke Team Manager Three Bridges Unit
Mr Chris Dunn Occupational Therapist Evenlode, Oxford Clinic
Mr John Enser Director of Forensic and Prison Services
Bracton Centre
Dr Tim Exworthy Consultant Forensic Psycharist Redford Lodge Hospital
Miss Hannah Farr Assistant Psychologist Bracton Centre
Dr Seena Fazel Senior Research Fellow and Consultant Forensic Psychiatrist
University of Oxford / Warneford Hospital Oxford
Dr Andrew Forrester Consultant Forensic Psychiatrist HMP Brixton
Ms Vanessa Fowler Prison Mental Health Transfer Project Lead
Department of Health
Mr Steven Fuller Service User Researcher City University
Mr Riza Gangoo Ward Manager Chase Farm Hospital
Dr Kay Garvey Consultant Psychologist Ardenleigh Womens Forensic Service
Dr Paul Gilluley Clinical Director Maqle Forensic Services
West London Mental Health NHS Trust
Ms Lucie Goddard Research Assistant Mentally Disordered Offender Policy Research Unit
Miss Caroline Goldstein Assistant Psychologist Runwell Hospital
Ms Amy Gordon Forensic Mental Health Assistant
Fromeside Clinic
Mrs Cristina Gostlow Deputy Unit Nurse Manager St Andrew's Hospital
Ms Kathryn Harney Programme Manager National Forensic Mental Health R&D Programme
26
Ceinwen Haydon Approved Social Worker Forensic Service at Northgate Hospital
Mr Dave Hearn Practice Development Nurse FIPTS Inpatient Service, SLaM
Dr Jayne Henry Clinical Psychologist Eric Shepherd Unit
Prof Bob Heyman Associated Dean for Research City University
Dr S Hill Consultant in Forensic & Clinical Psychology
Adult Forensic
Ms Angela Hoadley Research Associate Sainsbury Centre for Mental Health
Mr John Hoar Regional Director Cygnet Hospital Ealing
Dr Josanne Holloway Consultant Forensic Psychiatrist / Service Director
Bolton, Salford and Trafford mental Health Trust
Andrea Hough Forensic Occupational Therapist
Reaside Clinic
Dr Gareth Hughes Head of Psychological Services Kneesworth House Hospital
Ms Maria Iglesias Mental Health Worker St Mungos
Dr M Iqbal Consultant Psychiatrist SPLD
Maureen Jaimin Approved Social Worker Forensic Service at Northgate Hospital
Amina Jappie Senior Forensic Social Work Practitioner
Runwell Hospital
Nikki Jeffcote Consultant Clinical Psychologist Three Bridges
Dr Johnny John-Kamen
Lead/Consultant Clinical Forensic Psychologist
Humber Centre For Forensic Psychiatry
Mr Terence Jolley Voluntary DSPD Visitor / Carer
Dr Julia Jones Senior Research Fellow City University
Dr O Kareem Consultant Psychiatrist Linden House Hospital
Dr Vivek Khosla Specialist Registrar The Oxford Clinic
Ms Maggie Kiegh Charge Nurse Butler Clinic
Dr Michael Kingham Consultant Forensic Psychiatrist Kent Psychiatry Service
Mr Bryan Kvilums Clinical Nurse Manager - Forensics
Wood Lea Clinic
Dr Chris Lace SpR in Forensic and LD Psychiatry
Kenneth Day Unit
Mr Ray Lancaster Social Work Team Manager Butler Clinic
Ms Fiona Langford Senior Social Worker Ardenleigh Womens Forensic Service
Mrs Geetha Langheit Clinical Psychologist 2 Oakglade
Dr Rachel Lart Senior Lecturer - Social Policy University of Bristol
Dr Kate Law Chartered Forensic Psychologist
Cane Hill Forensic Mental Health Unit
Mrs Barbara Lee Clinical Nurse Manager Langdon Hospital
Ms Jo Leech Associate Director West London Forensic Service
Ms Jacqui Linsey Senior Social Worker Ravenswood House
Ms Jacqui Linsey Senior Social Worker Ravenswood House
Ms Tracey Linton Forensic Social Worker Scott Clinic
Dr Matthew Lister Clinical Psychologist Oxford Clinic
Ms Helen Lockett Research Associate The Sainsbury Centre for Mental Health
Mr Conrad Lohneis Service User Researcher City University
Mr Andy Lucas Head Occupational Therapist The Humber Centre for Forensic Psychiatry
Ms Helen Lycett Occupational Therapist Oxfordshire Mental Health Trust

27
Mrs Natalija Lytrides Quality Co-ordinator Redford Lodge
Miss Sophie MacCulloch Research Fellow St George's Hospital
Mr Jonathan Mason Clinical Psychologist Cedar House
Miss Kathryn Mason Consultant Forensic Occupational Therapist
Marston House
Dr Nigel McKenzie Consultant Psychiatrist Highgate Mental Health Centre
Mr Bernard Mensah Charge Nurse Chase Farm Hospital
Dr Gillian Mezey Reader & Consultant in Forensic Psychiatry
St George's Hospital
Ms Sarah Miller Forensic Psychology Research Fellow
University of Surrey
Dr Thomas Mlele Consultant Psychiatrist Rowan House
Miss Olive Moloney Assistant Psychologist St John's House Hospital
Dr Elizabeth Moody Home Office Mental Health Unit
Miss Jayne Moore Substance Misuse Nurse Oxford Clinic
Mr Gerry Moore Social Work Team Manager Shaftesbury Clinic
Miss Beth Morphey Forensic Community Psychiatric Nurse
Oxford Clinic
Ms Caroline Mortimer Forensic Social Worker Norvic Clinic
Mrs Karen Mulliner Prison Mental Health Transfer Project Assistant
Department of Health
Dr Kevin Murray Associate Medical Director Broadmoor Hospital
Ms Kay Mustard Social Worker Roycroft Clinic
Dr Javiera Navarro Clinical Psychologist Institute of Psychiatry
Dr David Ndegwa Clinical Director Lambeth Forensic Services
Dr Graham Ness Consultant Forensic Psychiatrist Edenfield Centre
Mr Samuel Nkala Charge Nurse Kneesworth House Hospital
Dr William Obomanu Consultant Forensic Psychiatrist Chadwick Lodge
Mr Paul O'Connor Clinical Manager Cygnet Wing
Dr Annemarie
O'Connor Clinical Psychologist Humber Centre For Forensic Psychiatry
Mr Olufemi Olabintan Forensic Social Worker FIPTS Inpatient Service, SLaM
Mr Brendan O'Mahoney Assistant Psychologist Care Perspectives
Seamus O'Reilly Charge Nurse Fromeside Clinic
Mr John Owiti Senior Staff Nurse Centre for Forensic Mental Health
Pauline Palmer Senior Forensic Social Worker Norvic Clinic
Ms Joanne Parker Assistant Psychologist Runwell Hospital
Dr Janet Parrott Clinical Director Bracton Centre
Mr Georgie Parry-Crooke
Senior Lecturer London Metropolitan University
Dr Kiran Patel SpR in Forensic Psychiatry Home Office Suite
Ms Jo Paton Head of Research & Training Safer Custody Group, Health Partnerships
Dr Louise Pearson Clinical Psychologist Reaside Clinic
Mr Matthew Perrynan Charge Nurse Butler Clinic
Miss Cassie Philpin Research Officer University of Surrey
Mr Adam Pickford Senior Practitioner in Forensic Social work
The Hatherton Centre
Nicola Piek Occupational Therapist Camlet Lodge
28
Dr Simon Plunkett Consultant Forensic Psychiatrist Guild Lodge Secure Service
Dr J Poole Consultant Forensic Psychiatrist Department of Forensic Psychiatry
Mr Richard Prior Head of Social Care Fromeside
Mrs Jane Pym Head of Nursing Care Principles
Mr Colman Pyne Assistant Director Camlet 3
Dr Natalie Pyszora Consultant Forensic Psychiatrist Broadmoor Hospital
Mr Reshad Rajabalee Clinical Nurse Leader Thornford Park Hospital
Mr Abdallah Ramankhan Ward Manager Chase Farm Hospital
Dr Abdul Raoof Specialist Registrar Runwell Hospital
Stokely Raphael Services Liasison Manager Cygnet Health Care
Dr James Reed Staff Grade Psychiatrist Ardenleigh Womens Forensic Service
Ms Helen Reeves Forensic Social Worker East Sussex County Council
Dr David Reiss Cosultant Forensic Psychiatrist West London Mental Health NHS Trust
Ms Lisa Reynolds Research Fellow City University
Dr Lauren Richards Chartered Clinical and Forensic Psychologist
Ardenleigh Womens Forensic Service
Ms Sandra Ricketts Ward Nurse Langdon Hospital
Tim Riding
Nicky Runeckles Sales Director Bowden House
Dr Ricardo Sainz-Fuertes
Specialist Registrar Trevor Gibbons Unit
Dr Chiara Samele Head of Research Sainsbury Centre for Mental Health
Mr Malcolm Scoales Research Assistant Mentally Disordered Offender Policy Research Unit
Dr Kishore Seewoon- arain
Clinical Director Runwell Hospital
Miss Sarah Shanahan Assistant Psychologist Reaside Clinic
Dr Drona Sharma Head of Psychiatric Services Linden House Hospital
Dr Shubhinder
Shergill Consultant Psychiatrist Eric Shepherd Unit
Ms Mary Teresa
Sherlock Staff Nurse Eric Shepherd Unit
Mr Andrew Skerritt Barrister & Solicitor Self-employed
Dr Penny Snow Home Office
Prof Keith Soothill Professor of Social Research Lancaster University
Dr Sue Spiers Assistant Programme Manager National Forensic Mental Health R&D Programme
Dr E Stauffen-berg
Consultant Forensic Neuro Psychiatrist
Little Plumstead Hospital
Ms R Steadman-Allen
Forensic Social Worker Trevor Gibbens Unit
Mr Wayne Stockton Chartered Forensic Psychologist
Runwell Hospital
Mr Nigel Stokes Forensic Mental Health Social Worker
Guild Lodge
Ms Pat Sutcliffe
Julie Taylor Senior Lecturer in Allied Health Professions
Canterbury Christ Church University
Miss Michelle Taylor Occupational Therapist Kneedsworth House Hospital
Mrs Ann Teemal Nurse Development Officer Kneesworth House Hospital

29
Dr Vicky Thakordas Head of Psychology HMP The Mount
Mr Jacob Thompson Service User Researcher City University
Miss Melanie Townley Mental Health Assistant Fromside
Dr Ian Treasaden Clinical Director
Dr Christos Tsopelas Consultant Psychiatrist Thriasso Hospital
Mr Kevin Turley Charge Nurse Fromside
Dr Julian Walker Consultant Forensic Clinical Psychologist
Fromside
Dr Pamela Walters Specialist Registrar in Forensic Psychiatry
John Howard Centre
Mr Andy Ward Forensic Modern Matron Runwell Hospital
Dr Fiona Warren Lecturer in Psychology University of Surrey
Sonia Wateridge Senior Practitioner in Forensic Social Work
Dorset Forensic Team
Dr A Welborn Psychiatric Registrar Royal Perth Hospital
Dr Neil West Assistant Director Runwell Hospital
Dr Alison Westman Consultant Child and Adolescent Forensic Psychiatrist
St Nicholas Hospital
Dr Justin Wilson Consultant Psychiatrist Linden House Hospital
Miss Louise Wood Assistant Psychologist Humber Centre for Forensic Psychiatry
Mrs C Wood Community Psychiatric Nurse Ardenleigh Womens Forensic Service
Debra Woolley Service Manager Norvic Clinic

30
Appendix 5: Standards Order Form Further copies of these standards can be obtained by copying and completing this form: I would like to order copies of the Standards for Medium Secure Units at £10 each Title:(Dr, Mr, Mrs, Ms etc.): First name: Surname: Job Title: Organisation Name: Address: Postcode: Tel: Fax/E-mail: Please indicate your preferred method of payment: a) I enclose a cheque for £ made payable to ‘The Royal College of Psychiatrists’ b) Please invoice my organisation for £ Today’s Date:_____/_____/_____ Signed: PLEASE RETURN TO: Quality Network for Medium Secure Units, The Royal College of Psychiatrists’ Research and Training Unit, 4th Floor, Standon House, 21 Mansell Street, London E1 8AA. Tel: 020 7977 6665/6661. Fax: 020 7481 4831. E-mail: [email protected]

31
Appendix 6: Standards Feedback Form We hope you have found the Service Standards for Medium Secure Units useful and would appreciate your feedback. Your comments will be incorporated, with the approval of members of the quality network, into future editions of this publication. 1. Have you found these standards useful? Yes No Comments: 2. Do you have suggestions for new sections/topic areas or new standards or
criteria you would like to see included in future versions? 3. Do you have any general suggestions about this document that would
improve its usefulness? 4. What is your profession? Thank you for taking the time to complete this form. Your comments will be considered carefully. Please photocopy and return to: Quality Network for Medium Secure Units, Royal College of Psychiatrists’ Research Unit, 4th Floor, Standon House, 21 Mansell Street, London E1 8AA. Fax: 020 7481 4831.

32
33
Charity registration no. 228636
Quality Network for Medium Secure Units Royal College of Psychiatrists’ Centre for Quality Improvement
4th Floor, 21 Mansell Street, London E1 8AA
Telephone: 020 7977 6665/6661 Fax: 020 7481 4831
Email:[email protected] Website: http://www.rcpsych.ac.uk/msu