standardizing assessment data: continuity assessment record and evaluation (care) item set presented...
TRANSCRIPT

Standardizing Assessment Data: Continuity Assessment Record and Evaluation (CARE) Item Set
Presented by:
Barbara Gage, PhD
Engelberg Center for HealthCare Reform/The Brookings Institution
Stella Mandl, BSW, BSN, PHN, RN
Center for Clinical Standards & Quality/CMS
Presented to:
The Long Term Care Discussion Group
Wednesday, November 6, 2103

Thinking Ahead: Data Element Standardization
Stella Mandl, RNTechnical AdvisorDivision of Chronic and Post Acute CareCenter for Clinical Standards and QualityCenter for Medicare & Medicaid [email protected]

When we keep in mind the ultimate goal of
and step back to look at the big picture of what’s been done to prepare, it becomes clearer where
the work converges; how much of the work is connected and has already been done to achieve
Data Assessment Elements Goal
3
Achieving Uniformity to Facilitate Effective Communication for Better Care of Individuals and Communities

Assessment Data is:•Standardized•Reusable •Informative
• Communicates in the same information across settings
• Ensures data transferability forward and backward allowing for interoperability
Standardization:•Reduces provider burden•Increases reliability and validity•Offers meaningful application to providers•Facilitates patient centered care, care coordination, improved outcomes, and efficiency
• Fosters seamless care transitions• Evaluates outcomes for patients that traverse
settings• Allows for measures to follow the patient• Assesses quality across settings, and Inform
payment modeling
CARE: Concepts
4
Guiding Principles and Goals:

5
As Is To Be As Is: Multiple Incompatible Data Sources
Uniform Data Elements Across Providers
StandardizedNationally Vetted
Nursing Homes
MDS
Home Health Agencies
OASIS
Inpatient Rehab Facilities
IRF-PAI
Hospitals
No Standard Data Set
Physicians
No Standard Data Set
LTCHS
LTCH CARE Data Set
Outpatient Settings
No Standard Data Set
To Be: Uniform Assessment Data Elements Enable Use/re-use of Data
Exchange Patient-Centered Health Info Promote High Quality Care Support Care Transitions Reduce Burden Expand QM Automation Support Survey & Certification Process Generate CMS Payment
GOAL:
Transition

• Align measures with the National Quality Strategy and Six Measure Domains
• Implement measures that fill critical gaps within the six domains
• Develop parsimonious sets of measures - core sets of measures
• Remove measures that are no longer appropriate (e.g., topped out)
• Align measures with external stakeholders, including private payers and boards and specialty societies
• Continuously improve quality measurement over time• Align measures across CMS programs whenever
and wherever possible
CMS Vision for Quality Measurement
6
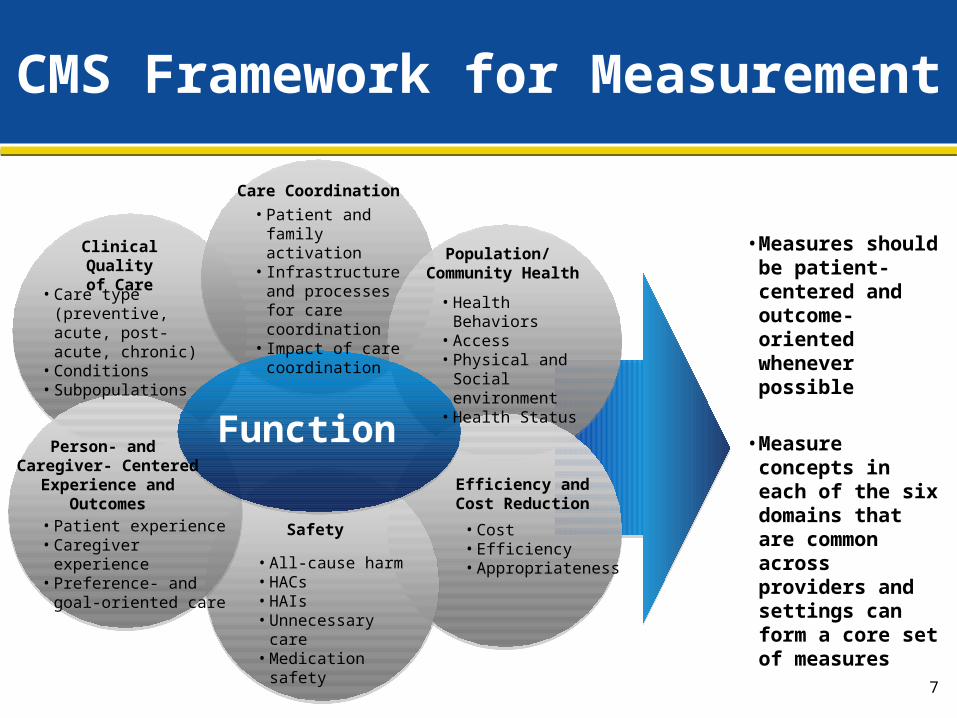
CMS Framework for Measurement
• Measures should be patient-centered and outcome-oriented whenever possible
• Measure concepts in each of the six domains that are common across providers and settings can form a core set of measures
• Patient experience• Caregiver experience• Preference- and goal-
oriented care
Efficiency andCost Reduction
• Cost• Efficiency• Appropriateness
Care Coordination
• Patient and family activation
• Infrastructure and processes for care coordination
• Impact of care coordination
Clinical Qualityof Care
• Care type (preventive, acute, post-acute, chronic)
• Conditions• Subpopulations
Population/ Community Health
• Health Behaviors• Access• Physical and Social
environment• Health Status
• All-cause harm• HACs• HAIs• Unnecessary care• Medication safety
7
Safety
Person- and Caregiver- Centered
Experience and Outcomes
Function

• Assessment Instrument/Data Sets use uniform and standardized items
• Measures are harmonized at the Data Element level• Providers/vendors have public access to standards • Data Elements are easily available with national
standards to support PAC health information technology (IT) and care communication
• Transfer of Care Documents are able to incorporate uniform Data Elements used in PAC settings, if desired
• Measures can evaluate quality across settings and be used for setting comparisons
Building the Future State
8
• Facilities are able to transmit electronic and interoperable Documents and Data Elements
• Provides convergence in language/terminology• Data Elements used are clinically relevant• Care is coordinated using meaningful information that is
spoken and understood by all• Measures can evaluate quality across settings and
evaluate intermittent and long term outcomes• Incorporates needs beyond healthcare system
Keeping in Mind, the Ideal State
9

Standardizing Assessment Data: CARE
Presented by
Barbara Gage, PhD
Phone 202-238-3571
E-mail [email protected]

11
State of the Art in Measuring Patients’ Health Status in Medicare
• Acute Hospitals no standard assessment tool to admit and monitor patients
• Long-Term Care Hospitals newly standardized items for quality reporting
• Inpatient Rehabilitation Facilities IRFPAI required
• Skilled Nursing Facilities MDS required
• Home Health Agencies OASIS required

12
DRA of 2005 called for one uniform tool that could be used to measure patient health status at:
• Acute hospital discharge
• Admission/discharge/interim times for cases using:
• Long Term Care Hospitals
• Inpatient Rehabilitation Facilities
• Skilled Nursing Facilities
• Home Health Agencies

13
Standard Language important for:
• Improving coordination of care – one set of terms to define pressure ulcer severity, functional impairment, cognitive impairment across providers
• Improving data exchangeability – can’t merge inconsistent items; need standard language to transfer information between providers treating the case
13

14
Continuity Assessment Record & Evaluation (CARE) Development
Sponsored by CMS, Office of Clinical Standards and Quality
• Principal Investigator/RTI Team: Barbara Gage, Shula Bernard, Roberta Constantine, Melissa Morley, Mel Ingber
• Co- Principal Investigators: Rehabilitation Institute of Chicago, Northwestern University
• Consultants: Visiting Nurse Services of NY, University of Pennsylvania, RAND, Case Western University
• Input by pilot test participants, including participating acute hospitals, LTCHs, IRFs, SNFs, and HHAs
14

15
15
Consensus Development
• Year 1 of CARE development: Gain input from the providers/research community
» Review existing assessment tools (MDS, IRFPAI, OASIS, LTCH tools, acute items)
» Technical Expert Panels
– Clinical communities from 25 associations, including AHA, AMRPA, NALTH, ALTHA, NAHC, VNAA, AHCA, AAHSA, APTA, AOTA, ASHA, ANA,ARN, CMA, Discharge Planners, Joint Commission, to name a few
– Research/case-mix communities, including DRG, FRG, HHRG, RUG

16
Standardized Assessment Items Should:• Build on current measurement science but also add new
instrument development methodologies, and
• Modify existing assessment instruments to develop a standard assessment instrument that will:
» Measure health and functional status
» Assess service needs
» Evaluate treatment outcomes
» Guide payment policy
» Improve seamless transitions

17
17
Common Domains in Existing Assessment Tools
Administrative Information
Social Support Information
Medical Diagnosis/Conditions
Functional Limitations
» Physical
» Cognitive

18
Differences Across Tools
• Individual items that measure each concept
• Rating scales used to measure items
• Look-back or assessment periods
• Unidimensionality of individual items
18

19
Functional Item Comparisons
Tools
No. of Functional
ItemsScale Levels Assessment Periods
IRFPAI 18 7 Past 3 days
MDS 3.0 12 8 Past 5 days
OASIS 8 varies Assessment day

20
Differences in Item Details• Bathing:
» IRFPAI and OASIS – bathing only
» MDS – bathing and transferring in/out tub/shower
• Dressing:
» IRFPAI and OASIS – 2 items (Upper/Lower)
» MDS – 1 item
• Toileting:
» IRFPAI – level of independence
» OASIS – ability to get to/from
» MDS – ability to use toilet, transfer, change pads
Source: Gage and Green, 2006. Chapter 2. The State of the Art: Current CMS PAC Instruments in Uniform Patient Assessment for Post-Acute Care, CMS Report, Contract #IFMC 500-02IA03.

21
Incomparable Functional Scales
IRF-PAI MDS OASIS
7= Complete independence 0= Independent 0= bathe independent tub/shower
6=Modified (device) 1= Supervision 1= with devices, independent
5=Supervision 2= Limited Asst. (guided maneuvering)
2= with person (reminders, access, reach difficult areas
4=Minimal Assistance 25% 3= Extensive Asst (3+ times/week)
3= participates but req. other person
3= Moderate Assistance 50%
4= Total Dependence 4= unable, bathes in bed/chair
2=Maximal Asst. 25% 8= Activity NA 5= totally bathed by other
1= Total Asst.
0= Activity NA
Unknown

22
CARE Item Development
• Formed 4 Workgroups
» Medical acuity/continuity of care
» Functional impairment
» Cognitive impairment
» Social/Environmental support

23
23
Workgroup Charge:
• Identify critical areas/domains for measuring case-mix acuity, resource use, or outcomes
• Review existing legacy tools (MDS, IRFPAI, OASIS), other leading measurement tools (PROMIS, COCOA-B, VA)
• Propose core set that can be used at hospital discharge and across all PAC settings

24
Issues in Selecting Items
• Identify Standard –
» Measures that applied across severity groups but capture the range of severity
» Scales that do not lead to ceiling or floor effects when measuring severity
» Assessment windows that would allow severity comparisons across settings
• Self-report/performance-based items
• Current Medicare payment methods
• Minimal burden on providers
• Varying technology options across providers

25
Medical Items
• Primary Acute Care Diagnosis
• PAC Diagnosis
• Comorbidities/Complicating Conditions
• Physiologic Factors
• Treatments
• Prognosis/Life Expectancy/Frailty
26
Social/Environmental Items
Physical Living EnvironmentPrior residenceStructural barriers
Social Support and AssistancePrior lives withLives with after dischargeType of caregiverFrequency of Assistance

27
Function Items
• Core Function Items
» All patients, all settings
• Supplemental Function Items
» Based on patient’s functional status (e.g., bedfast, self-care, basic mobility, IADLs)
» Maximize range of patient ability captured (i.e., avoiding floor and ceiling effects)
» Provide sufficient variation to capture improvement in function

28
Core Function Domains• Prior Functional Status
• Need for Assistance
» Eating
» Bed Mobility
» Oral Hygiene
» Toilet Hygiene
» Transfer
» Dressing - Upper Body
» Locomotion
• Function Modifiers
» Weight-bearing
» Sitting Unassisted
» Swallowing

29
Supplemental Function Items
• Bedfast
» Sit to lying, roll left or right, sponge bath
• Self Care
» Lower body dressing, shower/bathe, get in/out of car, curb/1 step, short ramp
• Basic Mobility
» 4 steps-exterior, long ramp exterior, walk longer distance-interior, wheel longer distance-interior, 12 steps-interior

30
Supplemental Function Items
• IADLs
» Laundry, light shopping, make light meal, dishwashing-by hand, dishwashing-machine, telephone-answering, telephone-placing call, medication management-oral meds, medication management-inhalers, medication management injectables
31
Cognitive/Self Report Items• Mental status
» Orientation
» Memory
» Screening for delirium
• Mood/Depression
• Behavioral symptoms
• Pain
• Sensory input
» Vision
» Hearing

32
32
Cognitive Items (cont’d)
• Communication
» Comprehension
» Expression
• Fatigue

33
Reliability of the Standardized CARE Items• Most CARE items based on existing validated items
currently used in the Medicare program; but few items had been used in multiple settings or across different levels of care.
• Two types of reliability tests were conducted to examine whether the items performed consistently across settings and across disciplines
» Traditional Inter-rater Reliability (pairs of assessors rate the same patient similarly)
» Video Reliability (cross disciplinary rating of standard video patients)
33

34
Traditional Inter-rater Reliability Methods
• Paired staff, matched on credential, assessed the same patient
• Tested in subsample of participating PACPRD providers (n = 34)
• Each site collected data on 10-15 patients
• 455 pairs of assessments collected
34

35
IRR Methods: Item Selection and Analysis
• Analyses followed methods used to evaluate existing CMS tools (MDS, OASIS, IRFPAI)
• Reliability scores at least equal to existing tools
» Categorical items: Kappa (for 2 levels), Weighted Kappa (for > 2 levels, Fleiss-Cohen weights)
– Range: 0 poor, 0.01–0.20 slight, 0.21–0.40 fair, 0.41– 0.60 moderate, 0.61–0.80 substantial, and 0.81–1 almost perfect
» Continuous items: Pearson Correlation
36
IRR: Results• Overall, the vast majority of Kappas (weighted and
unweighted) found were above 0.60
• Prior functioning and history of falls: 0.69 - 0.863
• Skin integrity:
» Pressure ulcers – 7 of 8 categorical items 0.67 or higher
» Length and width correlations – approx 0.6
» Major wounds – 0.64 and higher
» Turning Surfaces – 3 of 5 above 0.6, 4 of 5 above 0.5

37
IRR: Results
• Cognitive status and Mood: 26 of 29 above 0.6
• Pain:
» Interview items – all 5 above 0.6, 4 above 0.79
» Observational assessment – 4 of 5 above 0.6

38
IRR: Results• Impairments:
» Bladder and bowel:
– Current status items higher than 0.7
– Prior status items higher than 0.65
» Swallowing signs and symptoms: NPO (0.97), None (0.84), coughing (0.68), loss of liquids and holding food in mouth all low prevalence ranged 0.46-0.56
» All hearing, weight bearing, respiratory and endurance items had kappas above 0.6
39
IRR: Results• Functional status:
(calculated with and without letter codes)
» Core (self-care and mobility including walk and wheel): all above 0.6 except ‘tube feeding’ and ‘walk 150 feet’
» Supplemental Self Care: all above 0.63 except ‘roll left and right’
» Supplemental Mobility: all above 0.63 except ‘walk 50 feet with two turns’ ‘walk 10 feet on uneven surface’ and the wheel long and short ramps

40
40
IRR: Results
• Functional status (cont’d): (calculated with and without letter codes)
» IADLs: all above 0.7 excluding letter codes except ‘laundry’ and ‘light shopping’; all above 0.6 when including letter code, except ‘use public transportation’
• Overall plan of care: above 0.6

41
IRR: Summary
• IRR results indicate substantial to almost perfect agreement for the majority of items evaluated
• The few lower kappa scores tend to be for low prevalence items
• IRR results for CARE items are in line with the majority of IRR results available for equivalent items on MDS, OASIS, and FIM

42
CARE Item Reports• 2 website URLs
» http://cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Post-Acute-Care-Quality-Initiatives/CARE-Item-Set-and-B-CARE.html
» http://cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Post-Acute-Care-Quality-Initiatives/Functional-Measures-.html
• The Development and Testing of the Continuity Assessment Record and Evaluation (CARE) Item Set: Final Report on the Development of the CARE Item Set. Volume 1 of 3 [PDF, 8MB]
• The Development and Testing of the Continuity Assessment Record and Evaluation (CARE) Item Set: Final Report on Reliability Testing. Volume 2 of 3 [PDF, 2MB]
• The Development and Testing of the Continuity Assessment Record and Evaluation (CARE) Item Set: Final Report on the Development of the CARE Item Set and Current Assessment Comparisons. Volume 3 of 3 [PDF, 2MB]
• Continuity Assessment Record and Evaluation (CARE) Item Set: Additional Provider-Type Specific Interrater Reliability Analyses [PDF, 902KB]
• Continuity Assessment Record and Evaluation (CARE) Item Set: Video Reliability Testing. [PDF, 348KB]
» ASPE Report: Analysis of Crosscutting Medicare Functional Status Quality Metrics Using the Continuity and Assessment Record and Evaluation (CARE) Item Set. Final Report [PDF, 2MB]
•

43
On-Going Efforts with standardized CARE Item Set
• Developing setting-agnostic quality measures
• Quality Reporting Programs for IRF, LTCH, and hospice
• E-specification of “Best in Class” by CMS/ONC standards &interoperability groups
44
On-Going Efforts with Standardized CARE Item Set
• Developing Outpatient Therapy Payment Alternatives
– CARE-C: community therapy
– CARE-F: NF therapy
• B-Care (subset of standardized items for Bundled Payment Initiatives)
• LTSS Care Items (add items for long term social support programs)
