standardized assessments /adl - asht assessments /adl ... • visual analog scale • find out: ......
TRANSCRIPT

University of California, Irvine Medical CenterOrange, California
February 24‐26, 2017
Hand Evaluation
Audra Ponci Bado PT, MPT, OCS, CHT
Standardized Assessments /ADL• DASH
• 30 components• ADL Performance and symptoms
• Quick DASH• 11 components derived from original DASH
• MAYO • Elbow and wrist separate evaluation scales• Pain , function, motion, strength
• Oxford• Pain and function• Shoulder and Elbow
Standardized Assessments /ADL• Patient-Rated Wrist Evaluation (PRWE)
• Measures pain & disability in patients with wrist pathology• High test-retest reliability
• UEFS• measures effect of UE disorders on function
• Michigan Hand Questionnaire• 37 items looking at health domains in patients with hand disorders
• ASES Elbow Form• Pain and function questions• High reliability and validity
• ASES Shoulder Form• Pain and function questions• High reliability and internal consistency (Skirven, et al., 2011)
Demographic Information
• Patient History • Age • Handedness • Occupation • Avocation
• Date and History of Injury • Mechanism of Injury• Past Medical History • Medications • Surgery • Pain Assessment • Expectations
Pain• Verbal subjective assessment/Numeric Rating Scales
• 0-10 scale, 0= none, 10/10 = severe • Note pain rating at the time of evaluation, in addition to the recent
(<2-3 days) worst and best
• Pain charts • Visual analog scale
• Find out:• If pain is constant or intermittent.• If pain is during day hours or nightly.• What exacerbates or decreases patient’s pain level.
Observations• Atrophy - muscle wasting• Edema - pitting, brawny• Congruency of bony prominences and musculoskeletal architecture
• Nodules, wrinkles, calluses, contractures, deformities• Cascade of metacarpals• Hematoma/ecchymosis – may be indicative of acute injury or recent
surgery• Skin changes: Shiny, smooth, fragile, mottling
(Skirven, et al., 2011)

Wound/Scar• Location• Size/dimensions: length and width• Color: pink, red, white, yellow, black• Odor• Drainage: bloody, purulent, serous• Scar: hypertrophic, keloid,
adherent, hypersensitive
Trophic changes
• Nail growth: Ridges, grooves, splitting• Nail shape: clubbed, domed, clawed• Nail color: normal-pink, pale-anemic, bluish-vascular
insufficiency• Unusual nail growth may indicate nail matrix damage• Other changes associated with sympathetic dysfunction
(CRPS)
Vasomotor• Affected by general health:
• Smoker• Diabetes• Autoimmune disorder• Cardiac
• Affected by occupational factors: • Cold exposure• Vibratory tools• Repetition of tasks
Vasomotor
• Capillary refill test: Apply pressure to nail or pulp – blanching should occur with pressure and normal color should return when pressure is removed, compare to contralateral side.
• Assess pulses (if applicable)• Subclavian – sternal end of clavicle in scalene • Axillary – center of armpit• Brachial- superior to antecubital fossa, medial to biceps tendon• Radial- just proximal to wrist crease, volar-radial wrist• Ulnar – just proximal to wrist crease, volar-ulnar wrist
Edema• Will affect ROM measurements
(i.e. dorsal hand edema creates MP extension positioning)
• Note if it is brawny – Thick and immobile• Or pitting – Leaves depression with fingertip pressure• Observe for loss of wrinkles, creases, and ROM.
VolumeterStandardized tool, which measures amount of water hand displaces
• Measurements should be taken on both the involved and non-involved sides.
• Exercise has been found to have an effect on volumetrics; therefore, measurements should be performed at the same point in the therapy routine with repeated tests.
• Mild discrepancy when comparing right dominant to left non-dominant hand (~3.4%)
• Water temperature should be room temperature
Volumeter• Follow standardized procedures• Use room temperature water• Remove all jewelry, or document if it is left on• Fill to top of volumeter to the overflow level• Discard extra water and place beaker beneath
volumeter spout• Patient slowly submerges hand with MF/RF
web space split over plastic rod• Water will flow into the beaker• Monitor that position until water flow comes
to a complete stop• Repeat this on contralateral side
Circumferential • Surface measurements are taken with a flexible
tape measure.• Assess both hands• Measurements are taken in centimeters• Due to the variables of placement of tape and
tension applied, this testing is not standardized or reliable.
• Common sites to measure:• P1, P2, and P3• PIP and DIP• Across MPs• Wrist level• Elbow level• 3 inches distal to elbow crease
Figure of Eight• Reliable method with high
correlation between volumeterand figure of 8
• Four landmarks are used and provide a final number in cm
• 1. Begin at distal aspect of ulnar styloid, cross volar wrist to distal aspect of radial styloid
• 2. Diagonally across dorsal aspect of hand to 5th MCP jt.
• 3. Volarly across level of DPC• 4. Tape is taken dorsally across the
hand to the starting point at pisiform
• Sensitivity 99% Specificity 99%
3
1
24
ROM Considerations
• Patient needs to understand the ROM requested
• ASHT recommendations for ROM:• “0” is neutral.• “+” is hyperextension• “-” is an extensor lag
• Measurements should be written as extension/flexion (i.e. 10/85).• Normal ROM and functional ROM are not the same. Functional ROM
reflects the amount of motion a person needs to perform most ADL’s. These numbers are less than normative values.
• Placement of goniometer should be over the dorsal surface of the digits, if this is not possible, then lateral placement is performed
AROM• Reflects Muscle’s ability to move a joint, which correlates to
function• Normal variations from person to person in what is
considered “normal”• Limitations can be due to:
• Adhesions• Denervation• Strength/weakness• Inflammation• Subluxation, dislocation, or bowstringing of tendons• Lack of tendon continuity/ attenuation• Joint restrictions
PROM• Reflects the ability of a joint to be moved through its normal arc of
motion
• It assesses the joint and surrounding soft tissue structures
• Limitations may be associated with • Capsular tightness• Contractures• Joint incongruity• Malunited fractures
• Fixed deformities: limited AROM & PROM (i.e. adhesive capsulitis)
• If PROM>AROM it is usually indicative of tendon insufficiency, muscle weakness or adhesions

TAM and TPM
• Total Active Motion (TAM) and Total Passive Motion (TPM) are calculated by adding the flexion numbers of the MP, PIP, and DIP and subtracting any extension deficits.Example TAM:
• MP 0/90• PIP -10/85• DIP -5/55• TAM = 90 + 85 + 55 - 10 - 5 = 215
• *not accurate if the patient has hypermobile joints.
Fingertips to Distal Palmar Crease
• Distance of the fingertips to
distal palmar crease (DPC) of
each finger
Strength: MMT• MMT: Measures the strength of individual muscles or muscle group• MMT has questionable reliability and validity, however, it remains the
most common strength assessment.• It is not necessary to test each muscle during an examination. A
screening is performed by testing a key muscle innervated by one of the peripheral nerves (median, ulnar and radial)
• Isolated testing is indicated with a peripheral nerve injury• Scale: The 0-5 numerical scale
0 - no evidence of contractibility to 5 - full ROM against resistance • Weakness may indicate a nerve injury, disuse atrophy, pathology, CNS
lesion or pain.• Note any pain with excursion of muscle-tendon unit
(ie. 1st dorsal compartment with DeQuervain’s tendonitis).
Pinch
• Use a Pinchometer (a standardized tool, with standardized instructions)
• Take average of 3 trials for each type of pinch, alternating from one hand to the other
• Positioning: UE should be adducted, elbow at 90 degrees and FA in neutral
Types of PinchTripod Lateral (key) Tip to tip
(3 Jaw Chuck) Thumb against radial side Thumb against IF
Thumb against IF and MF. of IF Anterior interosseusMedian n. injuries or Ulnar N. (add. pollicus or NerveCMC DJD. First dorsal interossei)
Five Position Grip Test
• 3 trials taken bilaterally, alternating hands, at each of the 5 levels.
• Produces a skewed bell-shaped curve.
• A flat curve may indicate a submaximal effort by the patient.
Position Iposition II
IIIIV
V
Grip
• Dynamometer: The handheld dynamometer is a standardized tool, which measures grip strength isometrically.
• Measure both hands and compare • Positioning: Pt seated with UE adducted to
side of body, elbow at 90 degrees, and forearm in neutral
• Dynamometer should be calibrated yearly• Screening: The average of 3 trials is recorded
on level 2
Rapid Alternating Grip
• At the present time, this is not proven to be reliable or valid
• ASHT Clinical Assessment Recommendations:• Use level that produced the maximal grip amount from the
5-rung testing• Exchange the dynamometer from one hand to the other• Repeat for 10-20 grasps per hand• Watch needle to assess grip strength• Observe for any outlier measurement.
Two Point Discrimination
• This test is performed using a discriminator
• Innervation density test• Ability to perceive the
difference of 2 stimuli• The patients hand should be
supported with vision occluded
Two Point Discrimination: Static and Moving
• Points are applied to digital pulps
• Static testing: Performed in a randomized sequence on the digital pulps in a longitudinal fashion with points perpendicular to skin
• Static testing begins at 5 mm of distance between the 2 points• Testing is proximal to distal • Patient responds with “one” or “two”
• Dynamic testing: Begins at 8 mm between the 2 points and the points are across width of the pulps, and traced from proximal to distal
Two Point Discrimination
• Use enough pressure to just blanch the skin.• Make sure points are perpendicular to the skin surface.• Use random order to test• 7/10 correct responses are needed to assess accurate sensation
level.• If no response or inaccurate response is given, the distance between
the ends is increased by 1 mm until 7 of 10 responses are accurate• Compare to contralateral side.• Compression neuropathies can still have a “normal” result.• Sensitivity 32%, Specificity 81%
Two Point Discrimination• Indications for testing:
• Nerve lacerations with repairs or grafts.
• Nerve compressions after surgical releases.
• Long-standing nerve compression with motor changes.
Problems with testing:• No force control.• No inter-rater reliability.• Skin topography can alter
results.• Vibration of examiner’s
hand can alter results.• Difficult to control velocity
of points • Limited repeatability
Two Point Discrimination
• Static norms (for hand): • Normal 0-6mm• Fair 7-10mm • Poor 11-15mm• Non-functional 16+mm
• Dynamic norms (for hand): • Normal 2-3mm• Fair 4-6mm• Poor 7-9mm
Semmes-Weinstein Monofilaments Standardized test
• Correlates the ability to functionally discriminate light touch to deep-pressure
• The test evaluates the cutaneous innervation of the median, ulnar and radial nerves
• Patient is seated with the upper extremity in a comfortable position and vision occluded
• Sensitivity 82%, Specificity 86%
Semmes-Weinstein Monofilaments
Application by standardized methods:• Applied perpendicular to skin for 1.5
seconds and the monofilament bends in a C, and then removed for 1.5 seconds.
• Repeat for 3 trials per monofilament for a positive response with monofilaments 1.65-4.08
• Repeat once for monofilaments 4.17-6.65.
Semmes-Weinstein Monofilaments
• Begin testing with “normal threshold” monofilament, and increase
• Test distal to proximal along nerve pathways
• Randomize sequencing and timing between stimuli, beginning with finer monofilaments and increasing as necessary.
Semmes-Weinstein
• Norms:
• 1.65‐2.83 Normal
• 3.22‐ 3.61 Diminished light touch
• 3.84‐4.31 Diminished protective sensation
• 4.56‐6.65 Loss of protective sensation
• > 6.65 Un‐testable – deep pressure only
• Mini‐kit is used as a screening tool and contains only the 5 threshold levels for each sensibility level.
Sensibility
• There can be a false positive due to nerve anastomoses
• Riche-Cannou: anastamosis is at the hand level between motor branch of the ulnar nerve and the recurrent branch of the median nerve. With high ulnar nerve injuries, the patient will not claw.

Anastomoses
Martin-Gruber: is at the forearm level, and is seen in 15-20% of the population. Generally contains motor fibers only, with the median nerve innervating the ulnar intrinsic muscles that are typically innervated by the ulnar nerve.
Vibration: Tuning forks
• Tuning forks commonly used at 30cps and 256cps.• Vibratory force application not controllable.• Stimulus varies with examiners technique and force
applied.• Strike force cannot be replicated.• Responses from patient are subjective • Studies indicate that end organs have their own
stimulus response that varies with frequency, and therefore instruments of this nature cannot give athorough picture
Wrinkle test
• An objective test is used to demonstrate a lack of wrinkling which correlates with denervated hand.
• Used typically with children and those that cannot cooperate with formal sensory testing methods.
• The hand is placed in warm water for 30 minutes.• If results are positive, the patient will show a lack of skin
wrinkling in a denervated area after hand is pulled from the water.
• Positive results correlate with an absence of sensibility.
Ninhydrin Test• Clean hands; dried with acetone or alcohol• Wait 5-30 min; press onto good quality bond paper• Hold 15 seconds and trace• Remove hand and spray paper with ninhydrin reagent; the
paper is allowed to dry for 24 hours
• A normal print will show discrete sweat gland orifices due to amino acids staining the paper
• A blank print indicates that no sweating has occurred, due to non-functional sweat glands, implying nerve damage
• There is a 0-3 scoring scale. 0 represents no sweating and 3 represents normal sweating.
Stages of Sensory Recovery • Pain/temperature • 30cps vibration • Moving touch• Static touch• 256 vibration• 2-point discrimination• Localization to touch• Stereognosis
Paul Valentine Moved Some Vases 2 Local Storage
CoordinationMinnesota Rate of Manipulation• Timed standardized test, which was valid
and reliable with the original wooden version
• Current models are plastic and validity and reliability have not been established
• There is normative data• A measure of gross coordination• The test includes five different activities,
which involve placing blocks into spaces on a board
CoordinationPurdue Pegboard• Timed Standardized test • Normative data• Test both involved and noninvolved hands• A measure of fine coordination• Patients places a metal peg into a pegboard,
followed by a washer and a collar• Patient completes as many sets as possible in
a limited time
Allen’s Test for radial or ulnar arterial patency
• Palpate radial and ulnar arteries at the wrist, and apply pressure to occlude both.
• Exsanguinate the hand by having the patient open and close fist several times, then open the hand to a relaxed open position.
• Release one of the arteries – Note quality and time for the hand to re-
perfuse or revascularize. – Normal is <3-5 seconds.
• Repeat entire test releasing other artery* Do not perform if patient has had any
surgical vascular repair
Provocative Tests: Intrinsic Tightness Test
• Hold MPJ in hyperextension and passively flex the PIP, note ROM
• Then place MPJ into flexion, and passively flex the PIP, note ROM
• Test is positive if PIP ROM is greater with the MP flexed
Oblique Retinacular Ligament Test• Stabilize the digit with one hand• While holding the PIPJ in extension,
passively flex the DIPJ• Retest DIPJ flexion with the PIP
in flexion• Positive if the DIP has greater PROM with
the PIP flexed• If ROM is limited in both positions, the
patient may have a joint contracture.
Extrinsic Tightness Test- Digital Extensors• Hold MP in extension and passively flex
IPs• Repeat IP flexion with the MP in flexion• Test is “+” if the IP ROM is greater with
the MP in extension vs. flexion• Varying wrist position will affect results• Must rule-out IP limitations prior to
completing this test
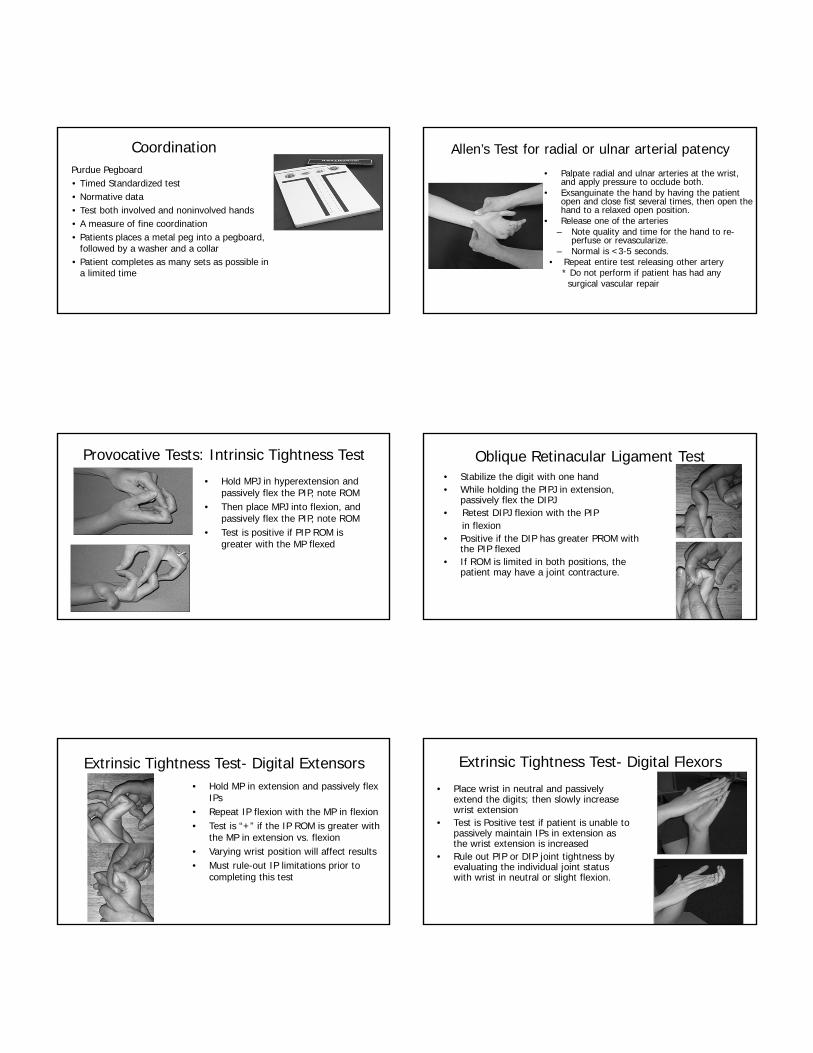
Extrinsic Tightness Test- Digital Flexors
• Place wrist in neutral and passively extend the digits; then slowly increase wrist extension
• Test is Positive test if patient is unable to passively maintain IPs in extension as the wrist extension is increased
• Rule out PIP or DIP joint tightness by evaluating the individual joint status with wrist in neutral or slight flexion.

CMC Grind Test • Test for arthritis of CMC jt. of the
thumb• Axial pressure is applied to the
shaft of the first metacarpal with rotation into the trapezium
• Positive test is pain at CMC jt.
• Sensitivity:42% • Specificity:91%
Finkelstein’s Test
• Test for tendonitis of the 1st extensor compartment (APL, EPB)• Patient flexes the thumb across the palm and bends fingers over
top of the thumb• Have patient then ulnarly deviate the wrist• Positive Test = increase of pain along the radial wrist • NOTE: this test is often uncomfortable in “normal” hands• Sensitivity 81%, Specificity 50%
Nerve Entrapment Provocative Test • Tinel’s: percussion over site
of possible entrapment• Positive test if it produces
paresthesias at the given nerve distribution.
• Can be done at shoulder, elbow, or hand
• Sensitivity: 64%• Specificity: 83%
Froment’s Sign
• Tests for weakness of the adductor pollicis and flexor pollicis brevis indicating Ulnar neuropathy.
• Ask patient to pinch paper using a lateral pinch.• Positive = Exaggerated IP flexion due to substitution with
the flexor pollicis longis (AIN)
Jeanne’s Sign • Tests specifically for weakness of
adductor pollicis
• Ask patient to pinch a piece of paper with the lateral pinch
• Positive if patient has extreme hyperextension of the MPJ
Wartenberg’s Sign
• Tests for ulnar nerve function (specifically the 3rd palmar interosseusmuscle)
• Ask patient to adduct the small finger from an abducted position toward the ring finger
• Positive if patient is unable to adduct the digit

Phalen’s Test Dr. Phalen demonstrating his famous test
CTS Provocative Tests• Phalen
• Wrist is placed in maximal flexion for 60 sec• Test is positive if it produces paresthesias in median nerve distribution
Sensitivity 68%, Specificity 71%
• Reverse Phalen• Wrist is placed in maximal extension for 60 sec• Test is positive if it reproduces parethesias in median nerve distribution
Sensitivity 65%, Specificity 85%
• Carpal Compression Test• Compression is placed over the proximal edge of CT ligament with the
examiners thumb for 30 sec• Test is positive if it produces pain or paresthesias in medial nerve
Sensitivity: 86%, Specificity 95%
Cozen’s Test for Lateral Epicondylitis• Place thumb on patient’s
lateral epicondyle• Arm is pronated, with the
elbow flexed, the patient is asked to make a fist
• Patient is then asked to extend the wrist as movement is manually resisted
• Positive if patient has severe and sudden pain in the area of the lateral epicondyle
Radial Nerve Test: Radial Tunnel
• Place elbow in extension, and manually resist supination
• Positive if patient has pain about 4-5 cm distal to the lateral epicondyle, indicating compression of the posterior interosseus nerve branch of the radial nerve
• Rule out lateral epicondylitis
Mill’s Test for Lateral Epicondylitis • Place elbow in flexion and
resist middle finger extension
• Positive if painful at the origin of the extensor muscles
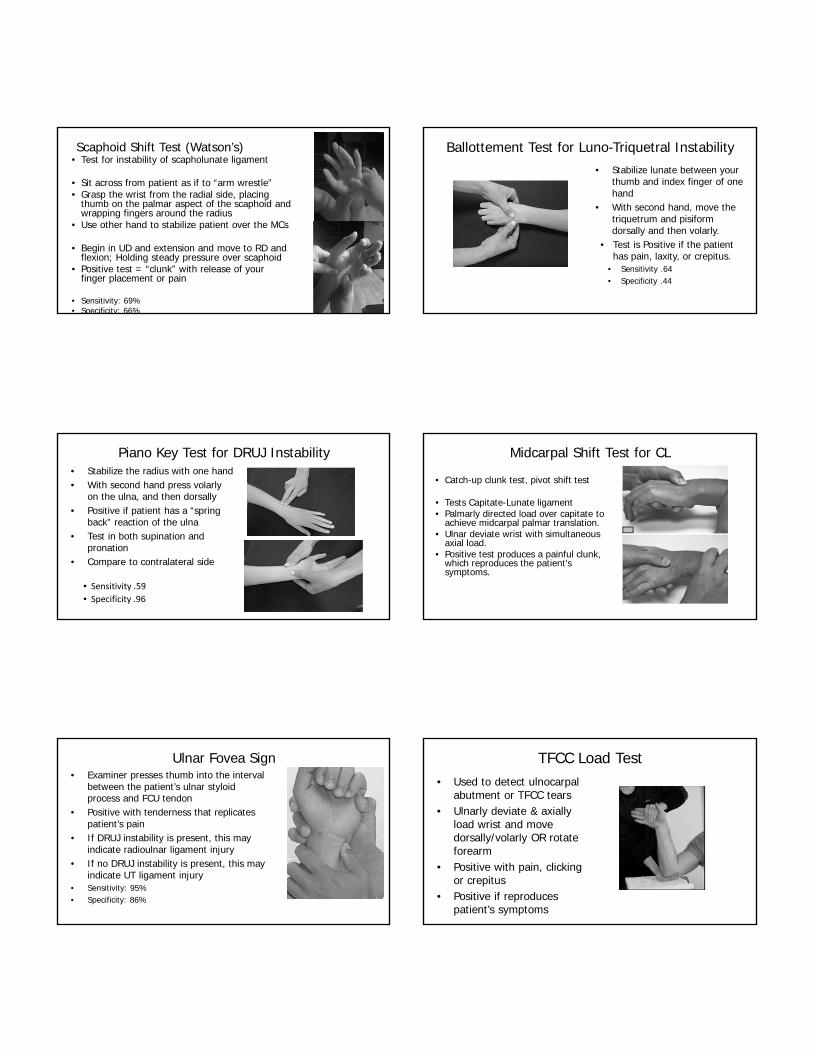
Scaphoid Shift Test (Watson’s)• Test for instability of scapholunate ligament
• Sit across from patient as if to “arm wrestle”• Grasp the wrist from the radial side, placing
thumb on the palmar aspect of the scaphoid and wrapping fingers around the radius
• Use other hand to stabilize patient over the MCs
• Begin in UD and extension and move to RD and flexion; Holding steady pressure over scaphoid
• Positive test = “clunk” with release of your finger placement or pain
• Sensitivity: 69%• Specificity: 66%
Ballottement Test for Luno-Triquetral Instability • Stabilize lunate between your
thumb and index finger of one hand
• With second hand, move the triquetrum and pisiform dorsally and then volarly.
• Test is Positive if the patient has pain, laxity, or crepitus.
• Sensitivity .64• Specificity .44
Piano Key Test for DRUJ Instability • Stabilize the radius with one hand• With second hand press volarly
on the ulna, and then dorsally• Positive if patient has a “spring
back” reaction of the ulna• Test in both supination and
pronation• Compare to contralateral side
• Sensitivity .59
• Specificity .96
Midcarpal Shift Test for CL
• Catch-up clunk test, pivot shift test
• Tests Capitate-Lunate ligament• Palmarly directed load over capitate to
achieve midcarpal palmar translation.• Ulnar deviate wrist with simultaneous
axial load.• Positive test produces a painful clunk,
which reproduces the patient's symptoms.
Ulnar Fovea Sign• Examiner presses thumb into the interval
between the patient’s ulnar styloid process and FCU tendon
• Positive with tenderness that replicates patient’s pain
• If DRUJ instability is present, this may indicate radioulnar ligament injury
• If no DRUJ instability is present, this may indicate UT ligament injury
• Sensitivity: 95%• Specificity: 86%
TFCC Load Test• Used to detect ulnocarpal
abutment or TFCC tears• Ulnarly deviate & axially
load wrist and move dorsally/volarly OR rotate forearm
• Positive with pain, clicking or crepitus
• Positive if reproduces patient’s symptoms
Summary• Evaluation with instruments that measure accurately allows physicians and therapists to correctly identify hand/upper extremity disease and dysfunction, assess the effects of treatment, and realistically apprise patients of their progress. Thank You!