standard operating procedure - n b r l . o r … · december 2005 standard operating procedure...
TRANSCRIPT

December 2005
STANDARD OPERATING PROCEDURE
PREPARATION, FREEZING, TRANSPORTATION, THAWING AND QUALITY CONTROL OF HUMAN PLATELETS ISOLATED BY
MECHANICAL CELL SEPARATING SYSTEMS AND FROZEN WITH DIMETHYLSULFOXIDE IN A 300 MILLILITER POLYVINYLCHLORIDE
PLASTIC BAG WITH REMOVAL OF THE SUPERNATANT DMSO PRIOR TO FREEZING
NAVAL BLOOD RESEARCH LABORATORY PHONE: (508) 747-4472
FAX (508) 759-2317 www.nbrl.org
e-mail: [email protected]
This work was supported by the U.S. Navy (Office of Naval Research Contract N00014-C-0118, with the funds provided by the Naval Medical Research and Development Command)
1

TABLE OF CONTENTS
PREPARATION AND FREEZING................................. 3 THAWING AND TRANSFUSION.................................. 11 SHIPPING INSTRUCTIONS.................................... 13 EQUIPMENT LIST........................................... 14 QUALITY CONTROL.......................................... 15 TABLES................................................... 18 ________________________ _______________ Reviewed and Approved Date
2

PREPARATION AND FREEZING I. INTRODUCTION The following Standard Operating Procedure describes a method to freeze single-donor human platelets. Dimethylsulfoxide (DMSO), added to the platelets to achieve a final concentration of 6%, is used as the cryoprotectant. The DMSO-treated platelets are centrifuged to reduce the total volume to approximately 10 ml and reduce the total amount of DMSO by about 95%. The concentrated, DMSO-treated platelets are frozen in a 300 milliliter polyvinylchloride plastic bag in a -80 C mechanical freezer.
This cryopreservation procedure is designed for single donor platelets. Single donor platelets containing 3.0 – 5.0 X 1011 platelets and single donor high yield platelets containing greater than 5.0 X 1011 platelets will be stored at 22 C with agitation for up to 4 days prior to freezing.
Apheresis should be done in accordance with the manufacturer's procedure manual and information referring to the specifics of the collection should be recorded in accordance with the standard operating procedures of the collection facility. Platelets can be stored prior to freezing for up to 4 hours at 22 degrees centigrade without agitation or up to 4 days at 22 degrees centigrade with agitation. The platelets can be leukoreduced by the machine during collection or by filtration either during collection, at the completion of the collection or after storage with agitation at 22 degrees centigrade for 4 days prior to the addition of the DMSO and freezing.
II. CONSUMABLES 1. Polyvinylchloride plastic bag, 300 ml (Fenwal #4R2014) 2. 27% DMSO-saline solution (Encyte Laboratories, #PN5075) each 75 ml contains 20.25 ml of DMSO and 54.75 of saline 3. Alcohol swabs (70% volume of isopropyl) 4. Waterproof tape (3M, #R202) 5. Vented spike with Drip Chamber (Encyte Laboratories, #PN5077) 6. Labels 7. 2.0 ml Cryogenic Vials (Corning 25702) 8. Filter needle, 19G (BD5200) 9. Kelly forceps (hemostats) (Fisher 08-907) 10. Sterile docking wafers (Terumo 3NCC987) 11. Corrugated cardboard box (7” X 5.25” X 2” outside dimensions)
3

III. SPECIMEN A. Method of Collection This cryopreservation procedure is designed for single donor platelets. The plateletpheresis product should contain no less than 150 ml and no more than 300 ml of plasma with a total platelet count ranging from 3.0 to 5.0x1011 as routine single-donor plateletpheresis products. In addition, platelet-rich plasma with platelet counts greater than 5.0 X 1011 as high yield platelets will be stored at 22 C for as long as 4 days prior to freezing. The two plastic bags of platelet-rich plasma will be pooled into one bag and ten (10) ml of the platelet-rich plasma will be removed to fill 4 cryogenic vials for future infectious disease testing. It is important that the label on the apheresis product and the platelet-rich plasma samples in cryogenic vials contain the date of collection, donor number, and product description. Apheresis procedures must be done in accordance with the manufacturer's procedure manual and data referring to the specifics of the collection procedure should be recorded in accordance with the standard operating procedure of the collection facility. Single donor platelets can be stored at 22 C for up to 4 hours without agitation or up to 4 days at 22 C with agitation. We recommend that platelets be kept at 22 C for the time required for completion of infectious disease testing prior to freezing for up to 4 days. The platelets can be leukoreduced by filtration during collection, at the completion of the collection and after storage with agitation at 22 C for as long as 4 days prior to the addition of the DMSO and freezing (Table 1). V. FREEZING PROCEDURE Apheresed platelets do not require agitation if frozen within 2-4 hours of storage at room temperature. Platelets that are kept for as long as 4 days before freezing must be stored at room temperature with agitation. Prior to freezing, labels with collection information on the apheresed platelets must be verified. A. Procedure for freezing provials:
4

1. Ten ml of platelet-rich plasma will be obtained from the pooled two units of platelet-rich plasma. 2. Approximately 1.5 ml of platelet-rich plasma will be added to each of the 4 labeled provials. When the provials are filled with the platelet rich plasma, secure the caps tightly. C. Procedure for freezing platelets:
1. Determine the gross weight of the pooled platelet-rich
plasma and record the weight on the platelet freeze sheet. Record collection and pre-freeze information on the platelet information worksheet (Table 1).
2. Record the volume, manufacturer, lot number and expiration date of the DMSO solution on the platelet freeze sheet.
3. Remove the solution delivery sleeve from the bottle. Peel
back the hanger strap portion of the bottle and position it for use (see Figure 1).
4. Remove the vented spike with drip chamber from the package and close the roller clamp (see Figure 2).
5. Remove the flip-off cap from the 75 ml bottle of 27% DMSO saline solution and swab the Teflon cap with an alcohol swab.
6. Insert the spike of the vented spike with drip chamber into the bottle of DMSO (see figure 2).
7. Sterilely dock the tubing of the drip chamber onto the bag containing the platelets and squeeze the weld to ensure it is open (see Figure 2).
8. Hook the bottom and top of the bag containing the platelets onto the shaker magnets of an Eberbach shaker.
9. Invert the bottle of DMSO and hang the bottle using the hang label strap on the bottle (see Figure 1).
10. The volume of 27% DMSO to be added will be either 50 ml or 75 ml depending on the volume of platelets collected (see Table 3).
11. Spread open the reusable plastic solution delivery sleeve and pass the transfer set tubing through the opening of the solution delivery sleeve. Slide the sleeve over the bottle of DMSO (see Figure 1).
12. Ensure that the vent cover of the vented drip is open.
5

Squeeze the drip chamber two to three times to prime the chamber (see Figure 2). 13. Open the roller clamp and fill the integral tubing up to the bag containing the platelets. 14. Close the roller clamp. Position the solution delivery sleeve so that the “0 ml” graduation mark of the sleeve label is parallel with the bottom of the solution meniscus in the bottle. 15. Turn on the Eberbach shaker to low speed (180 lateral oscillations per minute). 16. Open the roller clamp and allow the calculated volume to enter the bag. If 50 ml of DMSO is required based on the nomogram, close the roller clamp when the bottom of the meniscus is parallel with the 50 ml graduation mark of the solution delivery sleeve. If 75 ml of DMSO is required, empty the entire bottle. 17. After the DMSO has been added to the platelets, secure the tubing with hemostats and turn off the shaker. Heat seal the tubing connecting the 27% DMSO-saline solution to the apheresis bag, leaving 8-10 inches of plastic tubing. 18. Sterilely dock the bag containing the DMSO-treated, apheresed platelets to the tubing of the 300 milliliter plastic bag. Squeeze the weld to be sure it is open. 19. Hang the bags on the hooks provided on the pole of the Eberbach shaker and transfer all of the DMSO-treated, apheresed platelets into the 300 milliliter bag. 20. Place a hand sealer clip, not crimped, onto the tubing connecting the 300 milliliter bag to the original apheresis bag. 21. Remove the cup from the centrifuge. Lay the bag containing the platelets flat and roll up the empty apheresis bag. 22. Place both bags into the centrifuge cup and pack with gauze. 23. Weigh the centrifuge cups containing the platelets and balance with additional gauze if necessary. 24. Centrifuge the DMSO-treated platelets at 1250 X g for 10 minutes with the brake off to concentrate the platelets.
6

25. Remove the cup from the centrifuge and place the bag containing the concentrated platelets and supernatant on a plasma extractor so that the top of the bag extends over the extractor. Do not use the hooks provided. Remove the hand sealer clip and transfer all of the visible supernatant into the attached apheresis bag. Clamp off the tubing as the platelets begin to flow out with the supernatant. The final volume of the platelet unit should be 10-15 ml. In order to achieve a volume this small, some platelets will be lost with the supernatant. 26. Once the platelets have been transferred, squeeze the contents of the 300 milliliter bag until all the air has been transferred into the original apheresis collection bag. Heat-seal and discard the apheresis bag containing the supernatant solution. 27. Resuspend the concentrated platelets with gentle manual agitation for 3-5 minutes. 28. Weigh the DMSO-treated platelets and record the weight on the freeze sheet (Table 2). 29. Place the 300 milliliter bag containing the DMSO-treated platelets into a plastic overwrap bag and seal. The plastic overwrap ensures optimum freezing rates for the platelets. Place the overwrapped platelets and two of the four provials containing plasma into a cardboard freezing box and secure them with masking tape. The remaining 2 provials will be frozen separately according to the SOP of the processing facility. Close the cardboard box and secure it with masking tape to prevent it from opening during frozen storage. 30. Using masking tape, label the outside of the cardboard box with unit number, ABO, Rh, processing facility, collection date, freezing date, and expiration date. 31. Place the cardboard box on the bottom of a chest-type -80 C mechanical freezer in a horizontal position. To ensure proper freezing, never stack units to be frozen. Vertical upright type minus 80 degrees centigrade freezers are not recommended for freezing and storage of frozen platelets. Slower freezing rates may occur with upright freezers. Frozen platelets must be maintained frozen at a temperature of less than –65 C. Upright freezers are less capable of maintaining product temperature below –65 C, especially if the door is left open for prolonged periods of time or opened frequently.
7

FIGURE 1
PROPER PLACEMENT OF THE SD SLEEVE OVER THE DMSO BOTTLE
Slide SD Sleeve to align “0 mL” graduation mark with solution meniscus
-- 0 mL --50 mL
Peel and lift Hang Label Strap
SD Sleeve
Meniscus of DMSO Solution
Bottle
8

FIGURE 2
Cryosol-27™ Transfer Set for Freezing Platelets
Freezing Bag
9
Vented Drip Chamber
Vent Cover (shown in the open Position)
Spike Cover
* Note: To ensure a priming volume of < 10 mL, prime the chamber below the indicated line and ensure the overall length of tubing is <26 inches.
Roller Clamp
Tubing
Squeeze to prime chamber (not to exceed this line*)
cryosol-27™ Transfer Set for Freezing Platelets is connected to freezing bag using sterile docking device.
Tubing length <26 inches*
Freezing Bag

10

THAWING AND TRANSFUSION
I. INTRODUCTION
This Standard Operating Procedure was prepared to instruct you in the steps involved in thawing and transfusing concentrated, frozen platelets. Platelets frozen with dimethylsulfoxide in a 300 milliliter polyvinylchloride plastic bag are concentrated prior to freezing to reduce the dimethylsulfoxide by 95%. The thawed previously frozen platelets are diluted with 10 ml of 0.9% NaCl for transfusion. II. CONSUMABLES 1. 1 liter 0.9% sodium chloride (saline) solution 2. White linen towels 3. Blood component recipient set with 170-260 micron filter (Fenwal 4C2160) III. THAWING AND RESUSPENSION PROCEDURE
A. Using freezer gloves, remove the box containing the platelets from the freezer. 2. Record the time that the platelets were removed from the freezer (Table 4). Confirm that the label information on the freeze sheet matches that on the cardboard boxes.
3. Assemble the supplies you will need to thaw and transfuse the platelets. 4. If using the water bath, turn on the power switch of the water bath located at the end of the water bath. Once the water bath has reached 42 degrees centigrade, switch the pump on, and allow it to run for 1 to 2 minutes in order to circulate the water. Check the water temperature with a National Bureau of Standard verified thermometer to be sure that the water temperature is 42 degrees and stable. Alternately, the frozen platelets are thawed in a thawing bath (Thermogenesis, Rancho Cordoba, CA) maintained at 36 C in approximately 5 minutes.
5. Thaw the frozen platelets in the plastic overwrap by immersing it in the water bath or remove the plastic overwrap and place the frozen platelets into a pouch of the Thermogenesis hawing bath. t
11

6. One or more cryogenic vials containing frozen plasma stored alongside the frozen platelets can also be thawed to be used for infectious disease testing, if necessary. 7. Verify the labels on the freeze sheet, the 300 milliliter platelet freezing bag and the cryogenic vials containing the platelet-rich plasma. 8. Remove the platelets from the waterbath after they have completely thawed. Measure the surface temperature of the thawed platelets using the infrared laser scanner. The temperature should be between 32 and 34 degrees centigrade.
9. If using the plasma thawer, turn on the power to the plasma thawer and allow the system to warm to 35 degrees centigrade. Remove the plastic overwrap and place the frozen platelets into the pouches of the plasma thawer.
10. Remove the platelets from the plasma thawer after they
have completely thawed and, again, using the infrared laser scanner confirm that the product temperature is between 32 and 34 degrees centigrade. 11. Place the platelets on the clean white towel and dry all surfaces with a second towel. Check for breakage. Any sign of staining indicates breakage of the bag: these units will be contaminated and must be disposed of properly. 12. Add the approximately 10 ml of the 0.9% sodium chloride solution to the thawed previously frozen platelets. Using a scale, measure the weight of the thawed platelets resuspended in the sodium chloride solution. Record the thaw date and the weight of the 300 milliliter platelet freeing bag containing the thawed platelets diluted with 10 ml of 0.9% NaCl on the platelet recovery sheet. 13. The thawed previously frozen platelets stored in sodium chloride solution may be stored at room temperature for up to 6 hours without agitation prior to transfusion.
14. The thawed platelets in the sodium chloride solution are transfused through a 170 micron screen filter. 15. Previously frozen, thawed platelets should be studied for quality control according to the Standard Operating Procedure of the processing facility.
12

SHIPPING INSTRUCTIONS 1. Shipping Immediately prior to transportation, place twenty units of frozen platelets vertically into a polystyrene foam container with 1 inch of crushed dry ice or dry ice pellets covering the bottom of the container. Allow approximately a one-inch space in between each unit. Add 35-40 pounds of crushed dry ice or dry ice pellets between, around and on top of the units. The box should be firmly packed with dry ice to ensure minimal movement of the contents. The shipping container should have a gross weight of no less than 55 lbs to guarantee that the proper amount of dry ice has been added to the container. If fewer than 20 units of platelets are to be transported, additional dry ice should be added until the units are firmly packed. Follow established procedures for shipment of liquid blood products. 2. Receiving Immediately after opening the shipping container, place a National Bureau of Standards (NBS) verified mercury thermometer in between two of the units for approximately five minutes. Remove and record the temperature. The arrival temperature hould be -40C or lower to ensure a quality product. s
13

EQUIPMENT LIST
II. EQUIPMENT FOR PREPARATION AND FREEZING EQUIPMENT PROCEDURE -80 C mechanical freezer (chest type, 1HP Freezing compressor) Centrifuge, refrigerated. (DuPont RC-3B or Beckman J6B 4-head rotor) Freezing 37C incubator (Fisher 97-990) Freezing Eberbach shaker, (6010), modified (Fisher 14-265-10) Freezing Mettler balance, PE6000, toploading (Fisher 01-913-32) Freezing Plasma extractor (Fenwal 4R4404) Freezing Integral tube sealer (Sebra 1100) Freezing Shaker magnets (Haemonetics 9437) Freezing Tubing stripper/hand sealer (Fenwal 4R4407) Freezing Thermometer, -100C and a +50C, (Fisher 15-035) Freezing NBS Verified Mercury Thermometer Frz/Trans Sterile connection device (Haemonetics SCD312) Freezing Blue-M utility water bath (MW-1140A) (Fisher 15-453C) Thaw Pump (Circulating water) (Thomas Scientific 7887-FN) Thaw 1000 ul and 200 ul adjustable pipettes and tips (Rainin Instrument Co.) QC
Sharpie felt tip pen QC
14

QUALITY CONTROL
I. INTRODUCTION
Quality control procedures are performed to ensure that the platelet product is sterile and has acceptable in vitro parameters of pH, platelet count, R time measured using thromboelastogram, and platelet aggregates, intact platelets and platelet microparticles and surface markers measured using flow cytometer (Table 5). Quality control of frozen platelets should be performed on a pre-determined number of platelet units by the production facility. Platelet units used for quality control should not be transfused.
II. CONSUMABLES AND EQUIPMENT
A. Major Equipment
Refer to the individual SOPs for the procedures listed.
A. B. Consumables
Falcon tubes (2059 and 2063) 0.9% sodium chloride (saline) solution 1000 ul and 200 ul pipette tips AB fresh frozen plasma (FFP)
III. SPECIMEN
A. Sample Collection
Samples for quality control are removed after the addition of DMSO (pre-freeze) and after thawing (post-thaw). With a hemostat clamped on the tubing, mix the contents of the bag, cut the tubing proximal to the hemostat, release the hemostat and allow enough sample to run out of the tubing to clear it of any non-mixed platelets. Collect a 3 ml sample into a Falcon tube (2063). Heat seal the tubing four inches from the bag.
The following measurements may be made on each sample.
Pre freeze:
1. Complete blood count on performed using an automatic electronic particle counter (Coulter Counter, Beckman-Coulter) (200ul), pH at 22 C measured using a pH meter, R-time measured
15

using a thromboelastogram, and platelet aggregates, intact platelets, platelet microparticles, and GPIb, GPIIb, Annexin V binding to platelets measured using flow cytometry. R time is measured in platelets resuspended in plasma. R time is not measured in platelets diluted with 0.9% NaCl. A minimum concentration of plasma containing fibrinogen is needed to assess the R time measurement in the thromboelastogram testing. Thromboxane production by the platelets following stimulation with 50 ug AA/ml and 2 uM ADP/L.
Post-thaw: a. Concentrate alone 1. Flow cytometry (200 ul) b. Concentrate resuspended in AB fresh frozen plasma (purchased) 1. Platelet count measured using an electronic particle counter 2. Flow cytometry 3. R time measured using a thromboelastogram B. Preparation of samples for quality control
1. Complete blood count on a Coulter Counter automatic electronic analyzer or platelet count by phase microscopy.
a. Normally the platelet sample has a high concentration of platelets, it must be diluted with 0.9% NaCl in order to obtain a platelet count:
1:10: 100 ul platelets and 900 ul saline 1:20: 100 ul platelets and 1900 ul saline
b. Automated counts are done on the undiluted sample and the two dilutions.
c. If necessary, a phase platelet count is performed on both the 1:10 and the 1:20 sample.
d. Agitate the diluted platelets on a rocker at room temperature until counting. C. Platelet aggregation
16

Platelet aggregation is measured at 37 C with an aggregometer (BioData Corp., Horsham, PA). Before platelet aggregation, the platelet count is adjusted to approximately 5.0 X 106 per ml by dilution with autologous plasma or 0.9 percent NaCl. A 50 ul volume of the agonists is added to 450 ul of diluted platelets and the aggregation pattern is recorded for 5 minutes. The 5-minute aggregation pattern is analyzed by digitizing the area under the curve with the Kurta Is/ONE input system, and the data are reported in digitizer units (DU) for the 5-minute period of aggregation. The final concentrations of the agonists are AA 50 ug per ml and 2 umol ADP per L. D. Platelet thromboxane production The production of thromboxane B2 in the supernatant of the stimulated platelets is measured using the enzyme immunoassay kit Designs Correlate EIA (Catalog #900-002). Duplicate 450 ul platelet samples are stimulated with the agonists at 37 C for 5 minutes in a Bio/Data aggregometer, and 10 ul of 2 mg per ml toradol is added to each sample. The stimulated platelet sample is centrifuged at 1650 X g for 10 minutes, and the supernatant is frozen and stored at -80 C until the assay is performed. Measurements are made of the platelet count, and thromboxane levels are measured before aggregation. The thromboxane level in the supernatant of the platelet sample before aggregation is subtracted from that after aggregation, and this value is divided by the platelet count per milliliter to convert the thromboxane production per platelet. This value is reported as picograms of thromboxane X 10-6 per platelet. 2. Culture: a 2 ml sterile sample is needed for this assay. Refer to the Culture SOP. 3. pH: measured at 22 C. Refer to Standard Operating Procedure for Measurement of pH using a pH Meter. 4. Flow Cytometry: Platelet fingerprint (% microparticles, % intact platelets and % microaggregates) and surface markers (GPIb, GPIIb and annexin V binding). Refer to Standard Operating Procedure for Measurement of Platelet Surface Markers using Flow Cytometry. 5. R-time: Measure platelet R-time according to the Standard Operating Procedure for Use of the Thromboelastogram. IV. CALCULATIONS Refer to Table 6.

A. Adequate number of platelets.
1. Total platelets pre-freeze: ( A )
Plt count x Volume = Total # plts frozen.
(x 106/ml) x (ml) = (x 1011)
2. Total Platelets Post-thaw: ( B ) Plt count x Volume = Total # plts recovered post thaw. (x 106/ml) x (ml) = (x 1011)
3. Freeze-Thaw Percentage Recovery = (B)/(A) x 100
B. pH at 22 C
C. R time in thromboelastogram
D. Platelet aggregates, intact platelets and platelet microparticles; platelet GPIb, GPIIb and platelet annexin V binding in the flow cytometer
18

TABLE 1
PLATELET INFORMATION SHEET
DATE_______ SOURCE________ NBRL ACCESSION #_______ TECH INIT________ PAID DONOR_____ NON-PAID DONOR_______ TYPE AND RH__________ COLLECTION SITE___________________ UNIT DESCRIPTION: AUTOLOGOUS_______ ALLOGENEIC_____ IN VITRO______ INFECTION DISEASE TEST RESULTS
NON REACTIVE (NEG) REACTIVE SYPHILIS _________ _____ HEP B SURF ANTIGEN _________ _____ ANTIBODY TO HIV 1/2 _________ _____ ANTIBODY TO HEP B CORE ANTIGEN _________ _____ ANTIBODY TO HTLV I/II _________ _____ ANTIBODY TO HEPATITIS C _________ _____ NAT – HEPATITIS C _________ _____ NAT - HIV _________ _____ ALT:_________ ACCEPTABLE____ NOT ACCEPTABLE___ STORAGE AT 22 C:_________ HRS AGITATION_____ NO AGITATION_____ TRANSPORTATION AT 22 C: YES_____ NO_____ FILTRATION TO REMOVE WHITE BLOOD CELLS: YES_____ NO_____ IF YES, FILTER:__________________ A. IN-LINE FILTRATION_______ B. AFTER COLLECTION (0 HR)______ C. WITHIN 4 HRS OF COLLECTION_____ D. WITHIN 24 HRS OF
COLLECTION____ E. PRIOR TO FREEZING___________
19

TABLE 2
PLATELET FREEZE SHEET
WEIGHT OF PRP AT THE TIME OF DMSO ADDITION:____________GM (GROSS WEIGHT-BAG WEIGHT)/DENSITY = VOLUME OF PRP VOLUME OF DMSO ADDED TO PRP:____________ML MANUFACTURER OF DMSO: ___________________ LOT #________ MANUFACTURE DATE:_________ WEIGHT OF PRP POST DMSO ADDITION:__________GM (GROSS WEIGHT-BAG WEIGHT*)/DENSITY = VOLUME OF PRP *BAG WEIGHT = 40 gm PLATELET FREEZE BAG 300 ML PVC BAG MANUF.:_______ LOT #:______ EXP DATE:_____ BAG SEGMENT #________________ PROVIALS IN CARDBOARD CONTAINER YES______ NO_____ IN –80 C FREEZER AT NBRL YES_______ NO_____ STORAGE TEMP: -80 C: YES___ NO___
20

TABLE 3
ADDITION OF DMSO TO APHERESED PLATELETS WEIGHT OF THE PLATELETS IN PLASMA BEFORE DMSO ADDITION LESS THE VOLUME OF 27% FINAL 1000 ML PVC BAG DMSO IN SALINE CONCENTRATION (40g) DIVIDED ADDED (ML) OF DMSO (%) BY DENSITY (1.024) (ML)____________________________________________________________ 150-219 50 5.02-6.75 220-300 75 5.40-6.86
21

TABLE 4
PLATELET THAW SHEET DATE____________ UNIT #___________ TECH INIT_____ TIME THAWED:___________ THAWED FOR___________________ STUDY STORAGE: PRE FREEZE STORAGE ________HRS -80 C STORAGE ________DAYS BREAKAGE YES____ NO____ PLATELETS THAWED USING: WATERBATH_______ PLASMA THAWER_____ THAW TIME:__________MINUTES VOLUME OF THAWED PLATELETS:_________ML NUMBER OF HOURS THAWED PLATELETS STORED AT ROOM TEMPERATURE WITHOUT AGITATION PRIOR TO TRANSFUSION:__________HRS
22

TABLE 5
QUALITY CONTROL WORKSHEET DATE:___________ UNIT #___________ TECH INIT________ SAMPLE: PRE FREEZE_____ POST THAW_____ VOLUME:_________ ML ----------------------------------------------------------- PLATELET COUNT METHOD: ELECTRONIC_________ PHASE_______ DILUTION FACTOR UNDILUTED --- ____ X 103/UL OR ____106/ML DIL 1 ____ ____ X 103/UL OR ____106/ML DIL 2 ____ ____ X 103/UL OR ____106/ML AVERAGE ____ X 103/UL OR ____106/ML VOLUME OF PLATELETS X AVERAGE COUNT/ML = TOTAL # OF PLATELETS ----------------------------------------------------------------- CULTURE DONE: YES____ NO____ RESULTS: AEROBIC__________ ANAEROBIC_______ NG = NO GROWTH DATE CULTURE READ:________ TECH INIT_________ RESULTS ACCEPTED BY:____________ DATE:_____________
23

TABLE 6
QUALITY CONTROL -- RECOVERY WORKSHEET UNIT #:______________ FREEZE-THAW RECOVERY:________ (%) (TOTAL # PLATELETS POST-THAW/TOTAL # PLATELETS PRE-FREEZE) X 100 ROUTINE QUALITY CONTROL MEASUREMENTS: A. TOTAL NUMBER OF THAWED PLATELETS:__________________ B. pH AT 22 C:______________ SPECIAL (NON-ROUTINE) QUALITY CONTROL MEASUREMENTS A. PLATELET GPIb:__________________ B. PLATELET ANNEXIN V BINDING:_______________ C. PLATELET MICROPARTICLES:______________________ D. R TIME IN THE THROMBOELASTOGRAM:________________ E. THROMBOXANE PRODUCTION FOLLOWING STIMULATION WITH ARACHIDONIC ACID (AA) AND ADENOSINE DIPHOSPHATE A(ADP):_____________________

TABLE 7
Platelet count and pH for platelets resuspended in 10 ml sodium chloride solution and stored at room temperature for up to 6 hours
0 Hours
2 Hours
4 Hours 6
Hours
Unit Total Volume (mL)
Total platelets
plt ct(per mL)
pH plt ct (per mL)
pH plt ct (per mL)
pH plt ct (per mL)
pH
66887 25.90 3.51E+11 1.36E+10 6.52 1.34E+10 6.52 1.26E+10 6.5 1.23E+10 6.5 66961 28.60 4.62E+11 1.61E+10 6.59 1.58E+10 6.59 1.45E+10 6.59 1.43E+10 6.58 66970 32.40 3.63E+11 1.12E+10 6.61 1.12E+10 6.6 1.10E+10 6.61 1.10E+10 6.62 67029 29.80 6.57E+11 2.21E+10 6.44 2.15E+10 6.45 2.14E+10 6.44 2.13E+10 6.41 67043 35.70 5.51E+11 1.54E+10 6.73 1.55E+10 6.73 1.50E+10 6.71 1.51E+10 6.71
N 5 5 5 5 5 5 5 5 5.00 5 Mean 30.48 4.77E+11 1.57E+10 6.58 1.55E+10 6.58 1.49E+10 6.57 1.48E+10 6.56
SD 3.74 1.30E+11 4.05E+09 0.11 3.84E+09 0.10 3.97E+09 0.10 3.98E+09 0.11

' . i
Vox SanguinisErtitc-in-Chirtr: C P. En8alfr:rct, Amstcrdam
?'atnsuHllhcr: S. l(rrF AC, BlselPridGd h Sr'tacr|rod
Original Papers
Vox Sang 19: 245-258 (1985)
Cryopreseryation of Human Platelets Using 6% DimethylSulfoxide and Storage at -80'CEfiects of 2 Yeers of flozen Storage at -80'C and Transportetion ln Dry lcel
A.J. Melaragno, R.Carciero, H. Feingold, L.Talarico, L-Weintraub, C.R.Valeri
Naval Blood Rescarch Laboratory, Boston University School of Medicine, Boston, Mass., USA
Abstract platelet studies were done in healthy male voluntecrs and in thrombocytopcnic
patients. Some of the platelets used in the study were isolated by mcclanical apheresis using
.itn"t the Haemonetics blood processor 30, the IBM btood prooGsor 2997 or the Fenwal
C$3000 blood prooessor before freezing" Other platelets wene isolatod from individud units
of whole blood-and pooted before freezing. The platelets werc froicn with a 696 cryoprotec
tant (Dlv{SO) in a polyvinytchloride (PVC) plastic bag or a potyolefin plastic bag at -80'C in
a mechanical freezer and stored for as long as 3 years. Some of the frozen platelets were
transported in dry ie in polystyr€ne foam containers to determine'whether they would be
adversely afecteO by such treatment. Platelet recovery after freezing; thawing and washing
was about lilqf'.In the healthy male volunteers, in vivo recovery of autologous platelets l-zh
after transfirsion was about 33%, and the life span was about 8 days. In the thrombocytopenic
patients, in vivo recovery values were 50% of those from fresh platelets. The transfusion of
previously frozen washed platelets reduced clinical bleeding in the thrombocytopenic
patients with bleeding. There was no evidence of quality deterioration in platelets after
storage at -80'C for at least 2 years, as determined from in vitro recovery and in vivo
survival values, norwas there any adverse effect as a result of shipment of the frozen platelets
in dry ice in polystyrene foam containers from one facility to another.
I This work was supported by the US Narry under Offrce of Naval Research Contract N00014-79-C-0168
with funds provided by the Navat Medical Research and Development Command. The opinions or assertions
contained herein are those of the authors and are not to be construed as offrcial or reflecting the views of the
Nalry Department or Naval Sewicc at large-

''w*ii i
Iti .
246 Mclaragno/Carciero/Feingold/TalaricoAileintraubA/aleri
Introduction
Over the past 12 years the Naval BloodResearch Iaboratory has been evaluating thepreservation of human platelets frozen with
6% dimethyl sulfoxide (DMSO) and storageat -80'C 126, 271. In the studies reportedhere, platelets were isolated either from indi-
vidual units ofwholeblood or from the donor
by mechanical apheresis using the Haemone-
tics blood pro@ssor 30, the IBM blood pro-
cessor 2997 or the Fenwal CS-3000 bloodprocessor tl4l. Whichever the method of iso-lation, the platelets were pooled before theywere frozen with 60-200 ml of platelet-plas-
ma-DMSO mixture in a 800- or 1,000-mlpolryinylchloride (PVC) plastic or a 150-mlpolyolefin plastic container fl6, 24, 25, 30,
32,341.The bag of platelets was placed in an
aluminum container in a -80'C mechanicalfreezer 1291, and the platelets were frozen at
Z-3'Clmin. After thawing, the DMSO was
removed from the platelets by a dilution-centrifugation wash procedure. Washedplatelets can be resuspended in plasma and
stored at room temperature for as long as 4 hprior to transfusion [27]
This paper reports the effects of cryopre-servation and frozen storage for as long as 3years, and of shipment of the frozen platelets
in polystyrene foam containers in dry ice.
Materials and Methods
PatientsAll studies reported here were reviewed and
approved by the Institutional Review Board forHuman Research at Boston University Medical Cen-ter. Informed consent forms were signed by all thestudy subjects.
Thirty-four autologous transfusions were done in
the 28 healthy male voluntecrs; 6 healthy volunteers
were studied on two occasions. Each of 15 thrombo-
o4openic patients was trans scd with homologousplatelets collected from 15 healthy donors on 40 dif-
ferent occasions: platelcts from the same donor were
transfused as fresh and prcviously frozen washedplatclets on two separate occasions to the same throm-
bocytopenic patient In other studies, platelets werecollected from 8 patients with hematologic discascs
while they were in remission: thesc platelets were fro-
zen, thawed, washed and autotransfused-
Platelet Isolation by Manual Serial
CentrifugationWhen a manual serial ccntrifugation procedure
was used for collection, the plateles werc prcpared as
follows: 450 ml ofwholeblood was collectcd into 63 ml
of citratc-phosphatedertrosc (CD) anticoagulant in
the 80Gml primary bag of a polyvinylchloride (PVC)
quadruple-bag collcction system (Fcnwal laborato-
ries, Deerfiel4 lll., USA; No. 4R1242). The blood was
centrifugcd at 22 x. 2' Cat 1,600 g (2, 500 rpm) for 4 min
in a Sorvall RC-3 refrigerated centrifuge (DuPont
Instruments, Nefiown, C.onn., USA). The platelet-
rich plasma (PRP) was cxpressed into onc of the threc
integratly atuched transfcr packs. The primary hg
containing the red cells was scaled and scparatcd from
the integrally atUchcd bagS. The red cells were
returned to the donorby reinfusion with approximate
ty 350m1 of 0.9% NaCl solution. The collection and
separation proedure was r€pcated 4 times; the four
units of PRP wene oonentrated at22*.2'Cby oentri-
fugation at 4,5@g (4,l60rpm) for 5min in an RG3
refrigerated centrifirge. All but 20ml of the platelet-
. poor plasma (PPP) was expressed from cach of theplatelet concentrates into an integrally attached trans-
fer pack. Each platelet pellet was stored undisturbed at
room temperatune for I h, then resuspended. Thepooled platelets were added to the cryoprotectant and
frozen.
Platelet Isolation using the Haemonetics Blood
Processor 30Blood was collected in the anticoagulant acid-
citratedextrose (ACD, NIH, formula A). The PRP was
isolated by discontinuous-flow centrifugation with the
Haemonetics blood processor 30 as follows [14, 30]:
the blood was pumped into the 225-ml bowl at a flow
rate of 60-l00mVmin. As soon as the platelet band
appeared on the shoulder of the bowl, the flow rate was

Storage of Frozen Platelets at -80'C 247
rcduccd to 40mVmin. The platelet collection wasstartd whcn the platelet band had progressed to I cmalong the shoulder, and collection was continued for45 s after the red cell interfacc was reached, which waswhen the red cells appcared in the collection line. Theflow rate was maintained at 2OmUmin throughout theplatelet collection without occluding the donor's armwith a venous pressure cuff. The pRp was ccntrifugedat I 609 for t 0 min ar 22 + z'Cto remove about 90j6 ofthe contaminating red blood celts.
Platelet Isolation using the Fenwal CS-3000Blood ProcessorThe blood was collected into the ACD anticoagu-
lant at a ratio of 9 volumes of blood to I volume ofACD. The plateler were isolated by continuous-flowccntrifugation using the platelet protocol for the Fen-wal C$3000 blood proccssor. Approximately 3,500m1ofblood was proccsscd and 50 mt ofppp was collectedinto a 30Gml PVC plastic bag and stored at -g0.C inthe aluminum container with the cryoprcserved plate-lets. The PPP was uscd to resuspend the frozen-thawed-washed platelets.
. Platelet Isolation using the IBM Blood pruasor2997The blood was u,ithdrawn into the ACD antioqg-
ulant and the plarelets were isolated by continuous-flow centrifugation using the IBM blood pnocsor2997 with a dual-stage separation chamber [lq 16]-The PRP was oolletted throt,gh the.WBC collectionport at a rate of 2.0-2.5mUmin into a 60Gml pVCpack (Fenwal Laboratories, Derfield, Ill., USA;No.4R202l); the pon was attached to the.WBC ol-lection tube via an AE-2 plasma transfer set (FenwalI-aboratories, Deerfield, Ill., USA; No.4C2240). ThePPP was combined gith the red blood cells, and themixture was returned to the donor at the same rate atwhich the blood was withdrawn. About 50ml of thePPP was collected in a l5Gml pVC plastic bag (Fenwall:boratories, Deerfield, Ill., USA; No.4R200l) forstorage at -80'C wirh the cryopreserved platelets foruse as the resuspension medium for the plateletS afterthawing and washing.
Cnopreservafion o-f Platelets Isolated using theHaemonetics Blood processor 30The PRP was cenrrifuged at 4,5009 for 5 min at
22+2'C to concenrrate the platelets, and all but 30-50ml of the supernatant Ppp was expressed from the
concentrated platelets. The platelets were stored un-disturbed at room temperature for 90min and thenresuspcnded by gentle manual agitation. The volumeof platelet ooncentrate was adjusted to 50ml by addi-tion ofan appropriate volume of PPP. A 50-ml volumeof DMSO (Crown Zellerbach Corp., Camas, Wash.,USA; FDA authorization for use of DMSO: BB-IND570) and a plasma rclution containing 12 parrs ofDMSO and 88 parts of PPP was prepared by addingthe DMSO to the PPP with manual agitation over45 - 60 s. The 5G'ml volume of DMSO-plasma freezingsolution was added to the platelet concentrate over30min with mechanical agitation at about 180lateraloscillations per minute using the low speed on a mod-ified Eberbach shaker (Cryogenic Equipment Corp.,Buckeystown, Md., USA). The rate at which the cryo-protectant was added was controlled with a venosetmicrodrip infusion device (Abbott l-aboratories.North Chicago, Ill., USA). The l00ml of plarelet-plasma-DMSO mixrure then was transferred to a 150-ml polyolefin plastic bag (UCAR 2030-4, Union Car-bide C,orp., NewYork, N.Y., USA): the bagwas placedin an aluminum container for platelet freezing andstorage in a -80'C mechanical freezer.
Cryopresemation of Platelets Isolated by ManualSerial Centrifugation and u,ith the IBM BloodProcessor 2997 or the Fenx,al CS-J000 BloodProcessor -:
The CPD anticoagulant was transferred from an80Gml primary bag (Fenwal l-aboratorieq Deerfield,Il1., USA; No.4Rl242) to one of three transfer packsintegrally attached to it; the pack was sealed off anddiscarded. In some studies differential cenrrifugarionwas used to isolate the platelet concentrate from theunit of CPD blood. The 80Gml primary bag u'assecured to the modified Eberbach shaker. One of rhestylettes of the plasma transfer set (Fenual l.aborato-ries, Deerfield, Ill., USA; No.4C2243) u'as asepricalll.inserted into the special adapror porr integraltl,attached to the 800-ml primary bag. The procedurewas repeated until the four units of platelet concen-trate were pooled into the 800-ml bag.
ln other studies. 150-200mIof PRP rvas isolaredfrom the patient by apheresis using rhe IBM bloodprocessor 2997 or the Fenwal CS-3000 blood pro-cessor. The PRP u'as collecred either in a 600-mlPVC transfer pack (Fenwal Laboratories, Deerfield.Ill., USA; No.4R2023) or in a 800-ml PVC plasricbag (Fenwal laboratories, Deerfireld. Ill., USA:

248
'1;
Melaragno/C-arciero/Feingold/TalaricoAl/eintraub/Valeri
No. 4R I 242). The bag containing the PRP was secured
to a modified Eberbach shaker operating at l80lateral
oscillations pcr minute. A 50-ml volume of a sterile
solution containing l3.5ml of DMSO and 36.5m1of
0.9% NaCl (27% DMsO-saline) was added to theplatclets over 30t5min. When the platelet-plasma-
sodium chloride-DMso mixture was pnepared in the
80Gml PVC plastic bag, it was frozen in the same bag;
when it was prepared in the 60Gml PVC transfer pack,
it was transferred to a 1,000-ml PVC plastic transferpack (Fenwal Laboratories, Deerfield, Ill-, USA;
No.4R203l) which was placed in an aluminum con-
tainer and frozen as previously described [16]. The
5Gml volume of PPP that had been collected during
the apheresis procedure was transferred to a Fenwal
No.4R200l l5Gml PVC transfer pack: this was
placed in the aluminum container next to the platelets
in the freezer.
Thawing and Washing of Cryopresemed Platelets
Tothaw the platelets, the aluminum containerwas
removed from the -80'C mechanical freezer and
placed in a 42'C circulating water bath. The plastic bag
containing the partially thawed platelets was removed
from the aluminum containerand then returned to the
water bath for 3-5min longer to complete thawing.
The frozen PPP in the l5Gml bag was thawed in a
similar manner. A sample was taken from the thawedplateles for mcasuremcnts of platelet count and
DMSO conccntration.The thawed platelcts were diluted rapidly with
250m1 of a wash solution (CYtosol Laboratories,
Braintrec, Mass., USA) which contained either 0.9%
NaCl, 0.2% glucose and 40mg96 inorganic phospho-
rus, pH 5.0, or 0.9% NaCt,0.zolo glucose and 80mg%
inorganic phosphorus, pH 5.0. The diluted platelets
were @ncentrated by centrifugation at 4,5009 for5 min, and the supernatant solution was removcd. Theplateles were resuspended in 30ml ofautologous plas-
ma, and were stored at room temperature for as long as4h prior to transfusion.
In vitro Recovery of Plateles and Cultures
Platelet @unts were made using phasc microscopyas previously described [31]. The number of platelets
after the freeze-thaw-wash-resuspcnsion process was
compared to the totd numbcr of platelets frozen todetermine the in vitro numerical freeze-thaw-washrecovery value. Cultures on blood agar and peptone
broth were performed on cach platelet concentrateafter washing.
stCr Platelet Sumival and Blood Volume
MeasurementsThe survival of the autologous washed previously
frozen platelets was measured in the normal volun-
teers and in 2 patients with hcmatologic discases in
remission uging a tlCr-labcling technique [301. The
recipient's blood volumc was calculated from the plas-
ma volume, which was measurcd with l2s1-65"1"6
human albumin, and the totalbodyhematocrit" whichwas estimated from the peripheral venous hematoc-ritmultiplied by the factor 0.89 [281.
Platelet Sun'ivals in Thrombocytopenic Patients
The in vivo reooveryoffresband previously frozenplatelets transfused into patients was calculated from
the increase in the patient's platelet count, total bloodvolume, and the number of platelet transfused:
total blood v (posttransfusion (pretransfusion
volume (ml) ^
plalelet count per ml) -
platelet count per ml)
total number of platelets transfused016 in vivo r€cover! -
The recipient's blood volume was calculated from
the red cell volume measured with slCrJabeled autol-
ogous red cells and the total body hematocrit, or was
estimated from the patient's body surface area [28].
In vitro Platelet Futtction StudiesThe dense body content of fresh and previously
frozen platelets was quantitated using transmissionelectron microscopy [3]: to avoid a technical problem

I
Storage of Frozen Platelets at -80'C 249
with counting the dense bodics, the same technicianwas responsibleforall counts in this phaseofthe study.The ability of fresh and previously frozen platelets torelease laC-scrotonin after incubation with increasedconccntrations of thrombin was measured, accordingto the method of Robblee et al. [18].
EIIect of Shipment of Cryopresemed PlateleuCryoprcscrved platelets were transported in dry icc
to other US Nary medical facilities to evaluate theeffects of shipment. In these studies, the plateletsobtained from normal human volunteers were frozenand stored at -80'C at our laboratory. Some of theseplatelets were thawed and washed in our laboratory,and slCr platelet survival and platelet function wercmeasured. Other platelets collected from the samevolunteers were frozen at our laboratory and shippedindryice eitherto the National Naval Medical Center,Bethesda, Md., orthe Narral Regional Medical Center,San Diego, Calif. The platelets were stored at thesesites at -80'C fora brief period before shipment back
to ourlaboratory in dry ice. The platelets were thawedand washed at our laboratory, and slCr platelet sur-vival and platelet function in vitro were assessed.
Stabilily of 27% DMSO in 0.9% SodiumChloride after Storage at Room TemperatureT\e 27% DMSO-saline cryoprotectant solution
was prepared, and was stored at room tempemture:rs5Gml volumes in glass bottles with teflon stoppers thathad been heat-stcrilizcd in an autoclave. Bottles of thesolution stored for up to 33 months at room tempera-ture have been evaluated for stability by gas chroma-tography and l3C-nuclear magnetic resonance(NMR).
DMSO l-qelsGas chromatography (Hewlett-Packard, Model
76204) was uscd to measure the level of DMSO in thewashcd platelets. Thc cfliciency of the platelet-wash-ing proccss in removing the DMSO was calculated asfollows:
%DMSO washour - (DMSO) postthayr { ygl-u.me th?wed - (QMSO) postyash x volume washed(DMSO) postthawx volume thawed (ml)
The measurement of DMSO was made on a Hew-lett-Packard 7620A gas chromatograph, with a flameionization detector and an injection port set at 250'C[2]. Helium was used as carrier gas at a flow rate ofl5mUmin. This procedure used a Gfoot glass colum(Va in. outer diameter, 2mm inner diameter), consist-ing of 3% carbowax 20M on a chromosorb WHP80/100 mesh (Supelco Inc., Bellefonte, Penn., USA)and an oven temperature of 150'C.
The standards were prepared at a DMSO concen-tration of 0-8.25 by varying rhe amounts of DMSOdissolved in PPP. The standards and test samples werethen deproteinized by adding a l0% solution of TCA
(FisherScientific, Medford, Mass., USA). The sampleswere spun, and the clear supernatant was collected. Ofeach sample, 2pl was injected into the gas chromato-graph. The peak retention times and areas were mon-itored on a chart re@rder, where they were automati-cally integrated. The concentration of the test sampleswas compared to that of the standards. This ccmpari-son was made using a linear regression from the stan-dard curve, and the amount of DMSO was expressed in
90,6.Statistical analyses were done using nonpaired t
tests: a statistically significant difference was a p valueof less than 0.05.

250 Melaragno/Carciero/Feingold/Talarico/Weintraub/Valeri
Results
There were no statistically significant dif-ferences in the in vitro numerical recovery ofplatelets or the in vivo recovery values wheth-er platelets were frozen in an 800- or a 1000-ml PVC plastic bag, or whether the 0-90,6NaCl, 0.20/0 glucose wash solution contained40 or 80mg9o inoryanic phosphorus, pH5.0.
Platelets isolated with the IBM 2997 bloodprocessor or the Fenwal CS-3000 blood pro-
cessor, frozen with 60/0 DMSO in 200m1of platetet-plasma-sodium chloride-DMsomixture in a 1,000-ml PVC plastic bag, andwashed with a solution of 0.9016 NaCl, 0.2o/oglucose and 40mg0r6 inorganic phosphorus,pH5.0, or of 0.90,6 NaCl, 0.20/0 glucose and
80mg0/o inorganic phosphorus, pH5.0, had invitro recovery values of 78016 and in vivorecovery values of 32o/o of the platelets I -2 h
after transfusion, and a life span of about 8days. Platelets isolated with the IBM 2997blood processor, frozen with 60/o DMSO in200 ml of platelet-plasma-sodium chloride-DMSO mixture in 800-ml PVC plastic bags,and washed with 0.9% NACI, 0.20/0 glucose
and 40 mgo/o inorganic phosphorus, pH 5.0,had in vitro recovery values of 690/o and invivo recovery values of 28o/o of the platelets
I -2 h after transfusion, and life spans ofabout 8 days.
Platelets that were isolated by manualserial centrifugation, pooled, and frozenwith 60/0 DMSO in 100 ml of platelet-plasma-sodium chloride-DMso mixturein the 800-ml PVC bag had in vitro freeze-thaw-wash recovery values of 85016 and invivo recovery values of 3l% l-2h aftertransfusion, and the platelet life span was
about 8 days (fig. l).
Freczino Frceze' Volume frozen.contriner thrw'rvadr ml
recoverY, l
Number of plateletrfro:en
In vivo rccovery nr-2 hrftcr tnnsfurion. *
o IBM 4hereis
o Single unitspooled
l.000ml 78.7 t 8.3 205 t 17PVC brg
E00rnlPVC bag
84 .8 t 12 .8 107111
3.43 x 1011t 0.84(6 unitsl2.25 x 10rtr 0.48(4 unitsl
3 2 r E
3 1 t 6
t 7
{o 5 ooE+od r.g
!o
f r c(J
6q-
l nOto
& r o
1 2 3 1 5Tirne after transfusion, days
Fig.l. The in vitro and in vivo recovery of autol-
ogous platelets. Platelets that were isolated with the
IBM 2997 blood processor were frozen with 60,6
DMSO in 200m1 of platelet-plasma-sodium chloride-
DMSO mixture in 1,000-ml PVCbagsat-80'C. Plate-
lets that were isolated from individual units of bloodwere pooled and frozen with 6% DMSO in l00ml ofplatelet-plasma-sodium chloride-DMSO mixture in
800-ml PVC bags at -80'C. The platelets were washed
with a solution of either 0.90,6 NaCl,0.2o/o glucose and
40mgo/o inorganic phosphorus, pH 5.0, or of 0.90/o
NaCl. 0.20,6 glucose and 80mg% inorganic phospho-
rus, pH 5.0, resuspended with autologous plasma, and
stored at room temperature for 4h prior to reinfu-
sion.

S,oog. of Frozen platelets at _g0.C
251
Shipment of Cryopreserved platelets inDry lceIn vitro and -
not signin..ntrin ;t'Hr::ffffi:nH:the platelets were transported in dry ice fromthe Naval Blood Research Laboratory toother facilities (fie.2).The platelets that weretransported in dry ice had 6.91l.l densebodies per platelet, where", ptu,"lets thatwere not kansported had 7.2+2.6 densebodies per platelet. platelet Jease of raC_
serotonin after incubation with thrombinwas similar in the rwo groups (fig. 3). Both thenontransported and transported, previouslyfrozen platelets released signi-dcantty lessserotonin than fresh platelets (p<0.05). Thedecrease in serotonin release olurrea at thetwo highest thrombin concentrations testedfor nontransported, previously fror"r, plate_lets and at the five highest thrombin concen_trations for the transported previously frozenplatelets.
Safety and Therapeutic Effectiveness ofWashed, previously Frozin platelets fiThrombocytopenic pat ientsThe safety and therapeutic effectiveness ofpreviously frozen platelets was studied in l5thrombocytopenic patients. Thrombocyto-
penic patients were given homologous freshald previouslyfrozen platele$ obtained fromthe same healthy donor.
Ten thrombocytopenic parients were giv_en a total of 29 transfusions: l3 transfusionswere fresh platelets and 16 were previouslyfrozen platelets (tabre I). The increase inplatelet count I h aftertransfusion ofthe pre-viguslV frozen platelets was 5006 of that seenwith fresh platelets. The previously fror.nplateleh produced " pro-pi cessation ofcrin-ical bleeding when present. One occasionalminor untoward effect of transfusion of pre_viously froreo washed pf"r.f.ii-was an un-pleasant taste in the patient,s mouth due toresidual amounts of DMSO.
Frceze.thaw-rvarhrcsovcry, *
Volume frozen, ilumbcrof platrletfrozen
l1;[r rccovew
rftcr tnmfusion. iBiT
I -80 oc il 7e.0 r e.0 208 t 18 4 . 0 2 r l 0 l l 3 4 r rr 1.07
" ,t;'LH'1;oo';lo" 8r.7 r 12.3 r82 t 15 l'rl"il'ott ,, ,, 6'USRL xZ.0
Fig.2. In vitro and in vivo recove4. of platelersisolated with the IBM 2997 bloodpro..rro, "nd frozenwith 6% DMSO in 200m1 of pf"ief.t-ptasma-sodiumchloride-DMSO mixture in 1,000_mt pVC plastic bagsat -80'c- six hearthy mare vorunteers were studied ontwo separate occasions. In one study, the platelets werefrozen with 60,6 DMSO and sror; ui-_gO.C at rheNaval Blood Research Laboratory OVinfl. shipped toanother facility in dry ice, and returned ro the NavalBlood Research Iaboratory in dry ice. In both studies.the platelets were washed wittr ZiOJ "f ;,;il;;;
0.9% NaCl,O.2%oglucose and 40mgo6 inorganic phos_phorus, pH 5.0, resuspended in autologous plasma.and reinfused within 4h.
.{o'EQ)o?1
8atog
I
_C)
aFo
&oIIt(r
50
t0
30
n
'ro,
1 2 3 LTinre after transfusion, days
5

252 M el a ragno/Carci ero/Fein gold/TalaricoAMei nt ra ub/Y'aleri
ftt 60ood
i u,oI
lt)I
9 z o
lac-s-ttt uptake.96 n
I Frcsh 81.2 t2.6a Storcd rt -80 "C rt ]{BRL 77.8 t 9.3o Tr.nsported in dry icc 86.2 t 3.7
fiom rnd to il8R[
Five other patients each received 1 I plate-let transfusions: five fresh and six previouslyfrozen (table II). These patients, who hadbeen alloimmunized by previous platelettherapy, showed no increase in platelet countafter transfusions of either fresh or previouslyfrozen platelets.
Fig. 3. Thrombin-induced release of I aC-serotonin
(!4G5-HT) from plateles isolated by apheresis withthe IBM 2997 blood processor studied as fresh plate-lets and as washed, previously frozen platelets. Threehealthy male volunteers were studied on two separateoccasions. In one study, the platelets were frozen with6% DMSO in 200m1of platelet-plasma-sodium chlo-ride-DMSO mixturc in a l,00Gml PVC bag and storedat -80'C at the Naval Blood Research Laboratory(NBRL). In the other study, the platelets were frozenwith 696 DMSO in 200m1of platelet-plasma-sodiumchloride-DMSO mixture in a l,00Gml PVC bag,stored at -80'C at the Naval Blood Research I-abora-tory, then shipped to another facility in dry ice, andthen returned to the Naval Blood Research laboratoryin dry ice. In both studies, the platelets were washedwith a solution of 0.9% NaCl, 0.2% glucose and40mg% inorganic phosphorus, pH 5.0.
The in vitro function of the fresh and pre-viously frozen platelets was assessed bycounting the number of dense bodies perplatelet with a transmission electron micro-scope. The previously frozen plateletsshowed a significantly (p<0.05) lower num-berof densebodies perplatelet than the fresh
Table I. Homologous fresh and previously frozen platelets collected from the donor and transfused to throm-bocytopenic patients
Parameter Fresh platelets Frozen plateletsr
Number of patientsNumber of transfusionsMean number of platelets transfusedMean platelet increment per mmlCorrected increment per l0rr platelets transfusedl-hour posttransfusion platelet recovery, Vo
l 0r 3
3.45 +0.82 x l0rr49,060+20.25525,20919,073
62.2!23.0
l 0l 6
2.84+0.23 x l0r l21 ,019 +13,22512,94519,900
30.3X22.4
I Platelets were isolated using the IBM blood processor 2997 and frozen with 60ro DMSO in 200 ml of platelet-plasma-sodium chloride-DMSO mixture in a 1,000-ml PVC plastic bag at -80 'C tbr 1.7 * 1.3 months, with arange of 5 days-5 months. The previously frozen platelets rvere s'ashed with a solution of0.9Vo NaCl,0.2olo glu-cose and 40 mg% inorganic phosphorus, pH 5.0, resuspended in autologous plasma and stored at room tempera-ture for 4 h prior to transfusion.

Storage of Frozen Platelets at -80'C 253
Teble II. Homologous fresh and frozen platelets from the same donor transfused to five alloimmunizedthrombocytopenic patients
Parameter Fresh platelets Frozen platelets'
Number of patientsNumber of transfusionsMean number of platelets transfusedMean platclet increment per mm3C-orrected increment per lOtr platelets transfusedl -hour posttransfusion platelet recovery, 96
552.93tO.44 x l0rl
6,800t4,6M3,843 X2Ao7
9.3 ts .6
562.71+0J3 x l0 ' l
4,500+5,8002,481+3255
5.6 t7 .2
I Platelets were isolated using the IBM blood processor 2997 and frozen with 6% DMSO in 200 ml of platelet-plasma-sodium chloride-DMSO mixture in a 1,000-ml PVC plastic bag at -80'C for l.2t I months, with arange of I week-3 months. All of the previously frozen platelets werc washed with a solution of 0.9% NaCl, 0.2%glucose and 40 mg% inorganic phosphorus, pH 5.0, resuspended in plasma, and stored at room temperature for4h prior to trans sion.
platelets: fresh-platelet dense-body contentmean+sD was 8.52+0.90 (n- l9); pre-viously frozen platelet dense-body contentwas 6 .81+ 1 .68 (n : l 4 ) .
Elfect of Storage at -80'C on theViabilily of Cryopresened PlateletsSix thrombocytopenic patients were given
15 autologous transfusions of previouslyfrozen platelets that had been stored at -80'C
for I -24 months (table III). The storage at- 80'C appeared to have no adverse effects onin vitro freeze-thaw-wash recovery or on invivo survival l-2 h after transfusion. Therewere no significant differences in plateletrecovery I -2 h after transfusion whether theplatelets had been stored at -80'C for lessthan 12 months or for L2-24 months(t: 1.599, p>0.1). There \\,ere no significantdifferences in the results whether the plateletswere isolated using the Haemonetics bloodprocessor 30 or the Fenwal CS-3000 and thenfrozen for 12-24 months (table III).
Two patients with acute myelogenous leu-
kemia in remission donated platelets forcryopreservation. During a 3-year period, Ipatient received two autotransfusions, one at17 months after cryopreservation and theother after 3 years. The two autotransfusionswere done when the patient \ilas in remissionand afebrile, and had a normal platelet count.The cryopreserved platelets were isolatedusing the Haemonetics blood processor 30.frozen with 60/0 DMsO-plasma-sodium chlo-ride solution and stored in the 1,000-ml PVCtransfer pack at -80'C. The unit of plateletsstored for 17 months was thawed, labeledwith 5lCr, washed and autotransfused. The invitro freeze-thaw-wash recovery value was730/o,the in vivo platelet recovery l-2 h aftertransfusion 300/0, and the in vivo recovery ofplatelets 24 h after transfusio n 250/0. The unitstored for 3 years and processed in the samemanner had an in vitro freeze-thaw-washrecovery value of 690/0, an in r-ivo plateletrecovery | -2h after transfusion of 26010, andan in vivo recovery of platelets 24 h aftertransfusion of 320/o (fte.4).

254 Melaragno/c-arcicro/Feingold/TalaricoAve intraub/Valeri
Tirnc ol rtongcrt -80'C
Volumc frorcn.ml
Fracza-thaw'wrrhatcoGry. *
Itlumbcr of plrtclct:tnnslurcd
o 17 months
o 3 ycrr:
254.0225.3
73.168.6
1.08 x 101r
120 r 10r l
{g
f ;uo6
E , aE+( j T
b> 2 0
EJ t o
Fig.4. slCr survival, freeze-thaw-wash recovery in
vitro, the volume frozen, and the total number of
platelets transfused. The platelets from a patient with
acute myelogenous leukemia in remission were iso-
lated by the Haemonetic blood processor 30, frozen
with 6% DMSO in plasma-sodium chloride in a 1,00G
ml PVC plastic bag, stored at -80'C for up to 3 years,
andautotransfuscd when the patient was in remission,
afebrile, and had a notmd platelet count'
Table UI. Efrects of frozen storage of platelets at -80'C on autologous transfisions to afebrile thrombocyto-
pcnic patients
Stored< l2 months,Haemonetics
Stored 12-24 months
Haemonetics Fenwal
Number of PatientsNumberoftrans sions
Average length of storage at -80 'C, months
Average number of platelets transfused,
l 0 r lAverage platelet increment per mm3
Corrected increment per l0tr platelets
transfusedI -hour posttransfusion platelet recovery, 9o
Freeze-thaw-wash recovery, 016
39
3.40+ 1.4
2.63 +0.6320,026+ 5,890
l3 , l l2 !3 ,28934.6+ 10.369.3+ 12 .0
24
16.8 +4.5
4 .30 i 1 .8026,213+9,605
6 . 3 5 5 : 1 . 5 8 125.5+4.27 1 . 6 i 1 2 . 0
I2
22.5+2.1
2 .50+019,250X707
7,700128324.3+O.960.7 +2.9
platelets were isolated by apheresis using the Haemonetics blood processor 30 or the Fenrval cs-3000 blood
processor and frozen with rdq6 DMSo in prasma-sodium chloride mixture in a 150 ml polyolelin plastic bag at
-g0.c, thawed, washed with a solution oio.qg6 Nacl,0.20lo glucose and 40 mg,orb inorganic phosphorus, pH 5'0,
resuspended in autologous plasma and stored at room temperature for up to 4 h prior to transfusion'

Storage of Frozen Plateles at -80'C 255
{$ a oEt9
g o '
E.E,i. A#b>. l0g&
1 2 3 1 5 6 7Tinre after transfi.sin. days
Fig.S. The slCr survival, freeze-thaw-wash necove-
ry in vitro, and the total number of platelets trans-
fused. Autologous platelets from a patient with acute
myelogenous leukemia in remission were isolated
using the IBM blood processor 2997, frozen with 6%
DMSO in plasma-sodium chloride in a l,O0Gml PVC
plastic bag stored at -80'C fot 2.5 years, and auto'
transfused when the parient was in remission, afebrile,
and had a normal platelet count.
The second patient received one auto-transfusion 2.5 years after cryopreservation.The patient was in remission and afebrile,and had a nonnal platelet count at the time of
the autotransfusion. The platelets were iso-
lated using the IBM blood processor 2997
using the dual-stage channel, and frozen with
60/o DMSO-plasma-sodium chloride in the1,000-ml PVC bag in a -80'C mechanicalfreezer. The platelets were thawed, labeledwith 5lCr, washed. and autotransfused. The
in vitro freeze-thaw-wash recovery value was
850/0, and the in vivo platelet recovery l-zh
after transfusion \\'as 290/o (frg.5).
Stability of 27ao DMSO-Saline Solutionduring Storage at Room TemperatureEach 50-ml volume of 27o/oDMSO in 0.9V0
NaCl was prepared in a glass bottle with a
teflon stopper, autoclaved, and stored at
room temperature. Bottles stored forup to 33
months were examined by gas chromatogra-phy and were found to be free of breakdownproducts. Bottles stored for up to 18 months
were examined by trg NMR and no evidence
of DMSO breakdown products was found.
DMSO Content of the Thawed and
Washed PlateletsThe DMSO concentration in the thawed
platelets was about60/o,with a range from 5 to
7.5o/o.In 55 studies, 96+20/o of the DMSO
was removed by washing previously frozenplatelets with 250 ml of a solution of 0-9%
NaCl, O.2o/o glucose and 40 mg% inoryanicphosphorus, PH 5, or of 0.90,6 NaCl, O-2%
glucose and 80 mg0,6 inoryanic phosphorus,
pH 5.
B acteriologic CulturesAll previously frozen platelets were nega-
tive when cultured for bacterial contamina-
tion prior to transfusion.
Discussion
In our laboratory, platelets have been
frozen with 4-60/o DMSO at a rate of I to
3'Clmin: this freezing rate was achieved by
storing the platelets in a -80'C mechanical
freezer f9, 24,291. Many other investigators
have used a controlled rate of freezing plate-
lets with DMSO because they believe that this
minimizes platelet damage. Controlling the
freezing rate at l"C/min requires a specialprogrammed freezer, and this has been asso-
ciated with some problems. Satisfactory re-
sults were obtained with human platelets
frozen with 5o/o DMSO in a sPecial
grammed freezer at rates ranging from
pro-I t o
Freeze-thaw-uastr recovery 84.fLhlun$er of datetetstrarefi.red 0.42 x 0ll

256 Melaragno/Carciero/Feingold/TalaricoAlJeintraub/Valeri
_"-*G|F
II
II
,iI3'C7min, whereas when freezing rates were
increased to greater than 5'CYmin, platelet
damage was observed [17]. Major damagewas seen when platelets were frozen with 100/o
DMSO at about 8'C/min in the gas phase of
liquid nitrogen I151. On the other hand, plate-
lets frozen with 100/o DMSO at a controlled
rate of 1'C/min and stored in the gas phase of
liquid nitrogen, had postwash survival and
function values similar to those of fresh plate-
lets.Our data indicate that a 1,000-ml PVC
plastic bag was slightly better than an 800-ml
PVC plastic bag for freezing platelets in a
volume of 200 ml of platelet-plasma-DMSO
mixture. Previous studies at our laboratory
have shown that by controlling the volume
and geometry of the freezing container, it is
possible to achieve a fteezing rate of 2 to
3'C/min by storage in a -80'C mechanical
freezer f271.Results were similar whether the pool of
platelets frozen contained platelets from indi-
vidual units of blood or platelets isolated by
mechanical apheresis procedures- There was
no sign of bacterial contamination duringplatelet pooling.
Contrary to other reported studies [12]' in
none of our studies have we observed any
differences in results between platelets stored
in polyolefin plastic and those stored in PVCplastic bags [ 16, 321.
Human platelets have been frozen with
DMSO in liquid nitrogen with storage at- 150'C or at -80'C in mechanical freezers.
Platelets also have been satisfactorily frozen
with 50/o DMSO and stored in the gas phase
of liquid nitrogen at - 120"C for 3 years [4].In the study reported here, the platelets
were frozen with DMSO in a -80'C me-
chanical freezer and stored for as long as
36 months, with in vitro and in vivo results
similar to those of platelets frozen at -80'C
for only a few weeks. Only two units of aph-eresed platelets were stored at -80'C formore than 2 years, one for 2.5 years andone for 3 years. The data show that frozenplatelets can be satisfactorily stored at -80'C
for at least 2 years, but that additional data
are needed on platelets stored at -80'C for 3years.
The shipment of PreviouslY frozenplatelets in dry ice in polystyrene foam con-
tainers did not adversely affect in vitro re-
covery, in vivo survival or laC-serotonin
uptake or release: results were similar 'to
those seen in platelets not subjected to shipment.
DMSGfrozen platelets have been trans-fused without postthaw washing [4-6, 33]'
but washing reduces the risk of toxic effects
from DMSO and appears to improve in vivo
survival as well. A onedilution wash proce-
dure removed about 95% of the DMSO andleft about 300 mg in the unit. Plateletswashed with a single dilution-centrifugationprocedure were found to have better circula-
tion than unwashed platelets [9]. The results
of this study indicate that washed, previously
frozen platelets stored at room temperaturefor 4 h prior to transfusion to thrombocyto-penic patients increased platelet counts andreduced bleeding times shortly after transfu-sion. Baldini et al. [l, 10-12] have storedpreviously frozen washed platelets at room
temperature for 6-8h prior to transfusionwith acceptable results. Side-effects such as
local vasospasm and pain have been seen inpatients who were given DMSO-frozen plate-
lets that were not u'ashed[26,271.DMSO has been shown to Produce an
unpleasant odor in the recipient's mouth andmay cause nausea and vomiting, and platelet
washing may prevent these symptoms. I-arge

257Storage of Frozen Platelets at -80'C
doses of DMSO in animals have been shown
to produce lesions in the eye, particularly in
the lens, and to potentiate the hepatic toxicity
of aromatic hydrocarbons [8, l3' 19]' How-
ever, careful ophthalmologic examinations
and appropriate liver function studies made
in our healthy volunteer subjects over the
past 10 years have shown nountowardeffects
of the residual DMSO in transfused platelets'
Moreover, nny defects in platelet function
produced by residual amounts of DMSO
appear to be reversible [7].It takes about 2Vz units of cryopreserved
platelets to achieve the same number of cir-
culating platelets as one unit of fresh platelet
concentrate. ABO- and Rh-identical platelets
obtained from several donors can be either
frozen individually and pooled just prior to
transfusion, or pooled before freezing, with
comparable results 14, 20 -22, 25 -27, 341' As
many as six to eight units of platelets can be
isolated from the blood of a single donor in
z-3husing a mechanical cell separating sys-
tem, thereby reducing the risk of recipient
alloimmunization and the transmission of
disease [4, 16, 30].DMSO has been approved by the Bureau
of Biologics as a cryoprotectant for human
platelets. Data from this and previous studies
hrln. shown that platelets frozen with DMSO
have freeze-thaw-wash recovery values of
about 80% and immediate recovery values in
vivo from 40 to 800/o of those of fresh plate-
lets, normal life spans' and are hemostatically
effective immediately or shortly after transfu-
sion to thrombocytopenic patients 11,23'25'27 ,281.
Platelets frozen with 60/o DMSO and
stored at -80'C can be shipped in dry ice in
polystyrene foam containers by air without
any untoward effects on in vitro recovery or
in vivo survival.
References
1 Baldini, M.; Kim, B.: Storage of human platelets
by freezing; in Hogman, Krijnen, Valeri, Platelet
preservation and ransfusion, pp' 32-35 (Uppsala
Offset Center, UPPsala 1974)'
2 C-ontreras, T.; SheibleY, R'i Vderi, C': Accumula-
tion of di-2-cthylhexyl phthalate (DEHP) in whole
blood, platelet concentrates, and platelet-poor
plasma Transfusion 14 : 34 -46 (1974)'
3 -Costa,
J.; Detwiler, T.; Feinman, R'; Murphy' D';
Patlak, C.; Pettigrew, IC: Quantitative evaluation
of the loss of human plateletdense bodies follow-
ing stimulation by thrombin or A23187' J' Physiol'
264:297 -306 (1977).
4 Daly, P.; Schiffer, C.; Aisner, J'; Wiernik, P': Suc-
ottf"f transfusion of platelets cryopreserved for
more than 3 years. Blood 54: 1023-1027 (1979)'
5 Djerassi, I.; Roy, A-: A method for preservation of
viaUte platelets: combined cffects of sugars and
dimethylsulfoxide- Blood 22 : 703 -7 I 7 (1963)'
6 Djerassi, I.; Farber, S-; Roy, A'; Cavins, J': Prep
aration and in vivo circulation of human platelets
preserved with combined dimethylsulfoxide and
dextrose. Transfusion 6: 572-576 (1966)'
7 Fratantoni, J.; Poindextcr, B.: Dimethylsulfoxide:
effects on function of frcsh platelets and on the
viability of platelets in storage' Transfusion 23:
109- l l3 (1983) .
8 Hagemann, R.: Effect of dimethylsulfoxide on
nNe synthesis in $180 tumor cells' Experentia
25: 1298-1300 (1969)'
9 Handin, R.; Valeri, C.: Improved viability of pre-
viously frozen platelets' Blood 40:509-513
(r972).l0 Kim, B.; Baldini, M-: Preservation of viable plate-
lets by freezing. Effect of plastic containers' Proc'
Soc. exp. Biol- Med. 142:345-350 (1973)'
I I Kim, B.; Baldini, M.: Biochemistry, function
and hemostatic effectiveness of frozen human
platelets. Proc. Soc. exp. Biol' Med' I45:830-835
( I e74).12 Kim, B.; Tanoue, K.;. Baldini, M': Storage of
human platelets by freezing' Vox Sang' 30: 401-
4 1 1 ( 1 9 7 6 ) .
I 3 Kocsis, J.; HarkawaY, S.; Santoyo, M'' Sn1'der' R':
Dimethylsulfoxide: interactions with aromatic hy-
drocarbons. Science 160: 427 -428 (1968)'
14 Kurtz, S.; McMican, A-; Carciero, R'; Melaragno'
A.; Vecchione, J.; Valeri, C.: Plateletpheresis expe-

258 Melaragno/c.a rciero/Fei n gold/TalaricoAMeintraubA/aleri
rience with the Haemonetics blood processor 30,the IBM blood proc€ssor 2997, and the FenwalCS-3000 blood processor. Vox Sang. 4l:212-2lg( l e 8 l ) .
l5 I-azarus, H.; Kaniecki-Green, E.; Warm, S.; Aika-wa, M.; Herzig, R.: Therapeutic effectiveness ofcryoprescrved platelet concentnates for transfu_sion. Blood 57:243-249 (1981).
l6 Melaragno, A.; AMu, W.; Katchis, R.; Vecchione,J.; Valeri, C.: Cryopreservation of platelets iso-lated with the IBM 2992 blood cell separator. Arapid and simplified approach. Vox Sang. 4J..321_326 (1982) .
17 Murphy, S.; Sayar, S.; Abdou, N.; Gardner, F.:Platelet preservation by freezing: use of dimethyl-sulfoxide as cryoprotective agent. Transfusion /{..t39-t44 (1974\.
l8 Robblee, L.; Shepro, D.; Vecchione, J.; Valeri, C.:Increased thrombin sensitivity in human plateletsafier storage at 4t. Transfusion 19: 45-52(197e).
19 Rubin, L.; Mattis, p.: Dimethylsulfoxide: lenschanges in dogs during oral administration.Science /5J: 83-84 (1966).
20 Schiffer, C.; Buchholz, D.; Aisner, J.; Wolff, J.;Wiernik, P.: Frozen autologous platelets in thesupportive care of patients with leukemia. Trans-fusion I 6: 321 -329 (t976).
2l Schiffer, C.; Aisner, J.; Wierni\ p.: Ctinicat expe-rience with transfusion of cryopreserved platelets.Br. J. Haemat. 34:377-385 (1976).
22 Schiffer, C.; Aisner, J.; Wiernik, p.: Frozen autol-ogous platelet transfusions for patients with leu_kemia. New Engl. J. Med. 299:7 -tZ (t979).
23 Shepherd, [C; Sage, R.; Barber, S.; O'Brien, E.:Platelet preservation. l. In vitro aggregation stud-ies. Cryobiology 2t:39-43 (1984).
24 Spector, J.: Yarmala, J.; Marchionni, L.; Emerson,C.; Valeri. C.: Viability and function of plareletsfrozen al 2 to 3'C per minute with 4 or 5 per centDMSO and stored at -80'C for 8 months. Trans-fusion I7: 8-15 (t977).
25 Valeri, C.: Therapeutic effectiveness of humanplatelets freeze-preserved with dimethyl sulfoxideat -80'C: in Hogman, Krijnen, Valeri, plateletpreservalion and transfusion, pp.4l - 50 (UppsalaOffset Cenrer, Uppsala 1974\.
26 Valeri, C.: Blood banking and the use of frozenblood producrs (CRC press, Boca Raton 1976).
27 Yalei, C.: The current state of platelet and granu_locyte cryopreservation. CRC crit. Rev. ctin. I-aU.Sc i . / r ' . .2 t -74 (198t ) .
28 Valeri, C.; Cooper A.; pivacek, L.: Limitations ofmeasuring blood volume with iodinated I_ 125scrum albumin. Archs intern. Med. Ii2: i34_53g(1973).
29 Valeri, C.; Feingold, H.; Marchionni, L.: A simplemethod for freezing human platelets using 6 per_cent dimethylsulfoxide and storage at _g0.C.Blood 43: l3l-t36 (1974).
30 Vecchione, J.; Chomicz, S.; Emersor, C.i Valeri,C.: Cryopreservation of human platelets isolatedby discontinuous-flow centrifugation using theHaemonetics Model 30 blood processor. Transfu-sion 20.' 393-400 (t980).
3l Vecchione, J.; Chomica S.; Emerson, C.i Valeri,C.: Enumeration of previously frozen platelctsusing the Coulter Counter, phase microscopy, andthe Technicon optical s-vstem. Transfusion 2l:5 l l - 5 1 6 ( t 9 8 1 ) .
32 Vecchione,J.; Melaragno. A.; Hollander, A.; Defi-na, S.; Emerson, C.; Valeri, C.: Circulation andfunction of human plateler isolatcd from units ofCPDA-I, CPDA-2, and CpDA-3 anticoagulatedblood and frozen with DMSO. Transfusion 22..206-209 (1982).
33 Wybran, J.; Stacquez, C.; Govaerts, A.: Storage ofhuman platelets in liquid nitrogen _ Isotopic siud-ies. Transfusion /2.. 4t3-4t7 (t972).
34 7-aroulis, C.; Spector, J.; Emerson, C.; Valeri, C.:Therapeutic effectiveness of previousty frozenwashed human platelets. Transfusio n I9:371_ 37g(l 979).
Received: June 12, l9B4Rer.ised manuscript receir.ed: January 2g. l9g5Accepted: March 4, l98j
A.J. Melaragno.Boslon Universily School of Medicine,615 Albanl ' Slreer,Bosron. MA 021 l8 (US.{ )

596 TRANSFUSION
Volume 45, April 2005
Blackwell Science, LtdOxford, UKTRFTransfusion0041-11322005 American Association of Blood BanksApril 2005454596603Original Article
AGGREGATION AND THROMBOXANE A2 PRODUCTION IN PLTsVALERI ET AL.
ABBREVIATIONS:
AA
=
arachidonic acid; DU
=
digitizer units;
NBRL
=
Naval Blood Research Laboratory.
From the Naval Blood Research Laboratory, Boston University
School of Medicine, Boston, Massachusetts.
Address reprint requests to:
C. Robert Valeri, MD, Naval Blood
Research Laboratory, Boston University School of Medicine, 615
Albany Street, Boston, MA 02118; e-mail: [email protected].
This work was supported by the U.S. Navy (Office of Naval
Research Contracts N00014-88-C-0118, N00014-94-C-0149,
N00014-00-1-0555) and by funding provided to the U.S. Navy
Bureau of Medicine and Surgery.
The opinions or assertions contained herein are those of the
authors and are not to be construed as official or reflecting the
views of the Navy Department or Naval Service at large.
Received for publication July 14, 2004; revision received Sep-
tember 13, 2004, and accepted October 11, 2004.
TRANSFUSION
2005;45:596-603.
B L O O D C O M P O N E N T S
Correlation between in vitro aggregation and thromboxane A2 production in fresh, liquid-preserved, and cryopreserved human
platelets: effect of agonists, pH, and plasma and saline resuspension
C.R. Valeri, H. Macgregor, and G. Ragno
BACKGROUND:
Some of the tests used to assess the quality of fresh and preserved platelets (PLTs) include PLT number, PLT morphology, pH of the PLT medium, PLT response to hypotonic stress, and PLT aggregation to agonists. This study was performed to assess the function of fresh and preserved PLTs by their response to aggregation and their production of thromboxane A2 after in vitro stimulation with agonists.
STUDY DESIGN AND METHODS:
PLTs isolated by apheresis procedures were stored at 22
∞
C for as long as 5 days and then frozen with 6 percent dimethyl sulfoxide, stored at
-
80
∞
C, thawed, washed, and resuspended in medium. The effects of agonists and the pH and composition of the medium on PLT aggregation and PLT production of thromboxane A2 after stimulation were measured.
RESULTS:
The agonists and the pH and composition of the medium affected both the aggregation response and the production of thromboxane A2 by the fresh and preserved PLTs. PLT aggregation response to arachidonic acid (AA) and adenosine diphosphate (ADP) was significantly lower in the cryopreserved PLTs than in the fresh and preserved PLTs. After stimulation with AA and ADP, the cryopreserved PLTs produced more thromboxane than did the fresh and liquid-preserved PLTs.
CONCLUSIONS:
The agonists and the pH and composition of the medium affected the response to aggregate and produce thromboxane in vitro in both the fresh and the liquid-preserved PLTs. PLT thromboxane A2 production may be a better in vitro test than PLT aggregation to assess PLT function in vivo.
n vitro tests are used to assess the quality of pre-served platelets (PLTs).
1-7
PLT viability has beenassessed from pH of the PLT medium, PLT morphol-ogy, and the PLT response to hypotonic stress.
8,9
Datareported on rabbit,
10,11
mouse,
12
and baboon PLTs,
13,14
however, subjected to degranulation failed to demon-strate a correlation between morphology and the survivalof autologous PLTs. In these animals, autologous PLTs sub-jected to extensive shape changes had normal in vivo sur-vival values.
10-14
The function of fresh and preserved PLTs is assessedby PLT aggregation response to single and dual ago-nists.
15,16
PLT function can also be assessed by the produc-tion of thromboxane A2 after stimulation with agonistsduring the measurement of the aggregation response.
17
The thromboxane A2 level in shed blood collected atthe bleeding site has been correlated to bleeding time.
18-21
A correlation between bleeding time and the shed bloodthromboxane A2 level has also been observed in humansand baboons subjected to hypothermia,
22-24
in patients
I

AGGREGATION AND THROMBOXANE A2 PRODUCTION IN PLTs
Volume 45, April 2005
TRANSFUSION 597
after administration of heparin,
25
and in humans as aresult of a reduction in hematocrit (Hct).
26
A decrease inshed blood thromboxane A2 level collected at the bleedingtime site was associated with an increase in bleeding time,and an increase in shed blood thromboxane A2 level wasassociated with a decrease in the bleeding time.
22-26
In this in vitro study of human fresh, liquid-preserved, and cryopreserved PLTs, we measured theresponse to aggregation and the production of thrombox-ane A2 after stimulation. We evaluated the effects of singleand dual agonists, the concentration of agonists, the pH,and the plasma and nonplasma resuspension media onPLT aggregation and thromboxane A2 production.
MATERIALS AND METHODS
PLT collection
At the Naval Blood Research Laboratory (NBRL), PLTs werecollected by plateletpheresis from volunteer donors whomet the requirements of the AABB. The donors reportednot taking medications that affected PLT function for10 days before donation. Using a cell separator (MCS
+
,Haemonetics Corp., Braintree, MA), the PLTs were col-lected from the donor into the acid-citrate-dextrose anti-coagulant (ACD, NIH, Formula A, Baxter Healthcare Corp.,Fenwal Division, Deerfield, IL) at a ratio of 1 vol of ACD to10 vol of blood.
At the University Hospital Blood Bank at Boston Uni-versity Medical Center (Boston, MA), PLTs were collectedby plateletpheresis from volunteer donors who met therequirements of the AABB and who reported not takingmedications that affected PLT function for 10 days beforedonation. A continuous-flow blood cell separator (CobeSpectra, Cobe BCT, Lakewood, CO) was used for collectionof the blood into the ACD, NIH Formula A anticoagulantat a ratio of 1 vol of ACD to 10 vol of blood.
The study was reviewed and approved by the Institu-tional Review Board for Human Research at the BostonUniversity Medical Center. Informed consent wasobtained from each volunteer.
Liquid preservation at 22∞∞∞∞
C
The PLTs collected at the NBRL and at the Blood Bank atBoston University Medical Center were stored in a 1000-mL CLX (tri-2-ethylhexyl trimellitate) plastic bag at roomtemperature in a stationary position for 4 hours, afterwhich they were stored for as long as 5 days at 22
∞
C on anEberbach shaker operated at 70 lateral excursions perminute. Fresh PLTs refer to PLTs stored at 22
∞
C withoutagitation for 4 hours.
In some cases at the NBRL, the PLTs collected byplateletpheresis in the Haemonetics MCS
+
were filteredimmediately after collection with a white blood cell reduc-
tion filter (Pall, LRF 10, Pall Biomedical Corp., Glencove,NY). The PLTs were studied before and after filtering andafter storage at 22
∞
C for as long as 5 days.
Cryopreservation
PLTs collected in the Haemonetics MCS
+
or the CobeSpectra were stored at 22
∞
C for as long as 5 days and thentransferred to a 1000-mL polyvinylchloride PLT freezingbag system (Fenwal 4R2986). A 50- to 75-mL volumeof 27 percent dimethyl sulfoxide (DMSO) in saline wasadded to the PLTs at room temperature over a 5-minuteperiod to achieve a final concentration of 6 percentDMSO. The PLTs were placed in an aluminum container,frozen on the bottom of a
-
80
∞
C mechanical freezer for24 hours, and then stored in a
-
80
∞
C freezer for as long as1 year.
27
The PLTs were thawed in a 42
∞
C water bath anddiluted with a 250-mL volume of 0.9 percent NaCl-0.2 per-cent glucose-40 mg percent inorganic phosphorus, pH 5.0(Cytosol Laboratories, Braintree, MA) and concentrated bycentrifugation at 4500
¥
g
for 5 minutes. The supernatantwas removed, eliminating 95 percent of the DMSO, andthe PLTs were resuspended in 50 mL of autologous plasmaor 50 mL of 0.9 percent NaCl.
In some units, the previously frozen washed PLTswere divided into two equal volumes: one volume wasresuspended in saline and the other volume in autologousplasma. The effects of the pH and the resuspensionmedium on PLT aggregation and thromboxane B2 pro-duction were evaluated.
In vitro measurements
Sample preparation.
The PLT count in the PLT-richplasma was adjusted to 3.5
¥
10
8
to 5.0
¥
10
8
per mL withsaline or autologous plasma. In some studies, the pH wasaltered, decreasing it by the addition of 0.1 mol/ per L HClto decrease the pH value from 7.2 to 6.0 and increasingit by the addition of 0.1 mol per L KOH from pH 7.2 topH 7.7.
Plasma pH and hypotonic stress.
The plasma pH wasmeasured at 22
∞
C with a pH meter (Orion Model 520A,Thermo Electron Corp., Beverly, MA). The PLT response tohypotonic stress was performed as previously described.
8
Plasma thromboxane.
Thromboxane B2, a stablemetabolite of thromboxane A2, was measured with a com-mercially available radioimmunoassay kit (New EnglandNuclear, Boston, MA).
24
The level was measured in the cell-free plasma prepared by centrifugation of PLT-rich plasmaat 1650
¥
g
for 10 minutes. The PLT-poor plasma was fro-zen at
-
80
∞
C until assayed.
24
PLT aggregation.
PLT aggregation was measured at37
∞
C with an aggregometer (Bio/Data Corp., Horsham,PA).
28
Before PLT aggregation, the PLT count was adjustedto approximately 5.0
¥
10
8
per mL by dilution with autol-
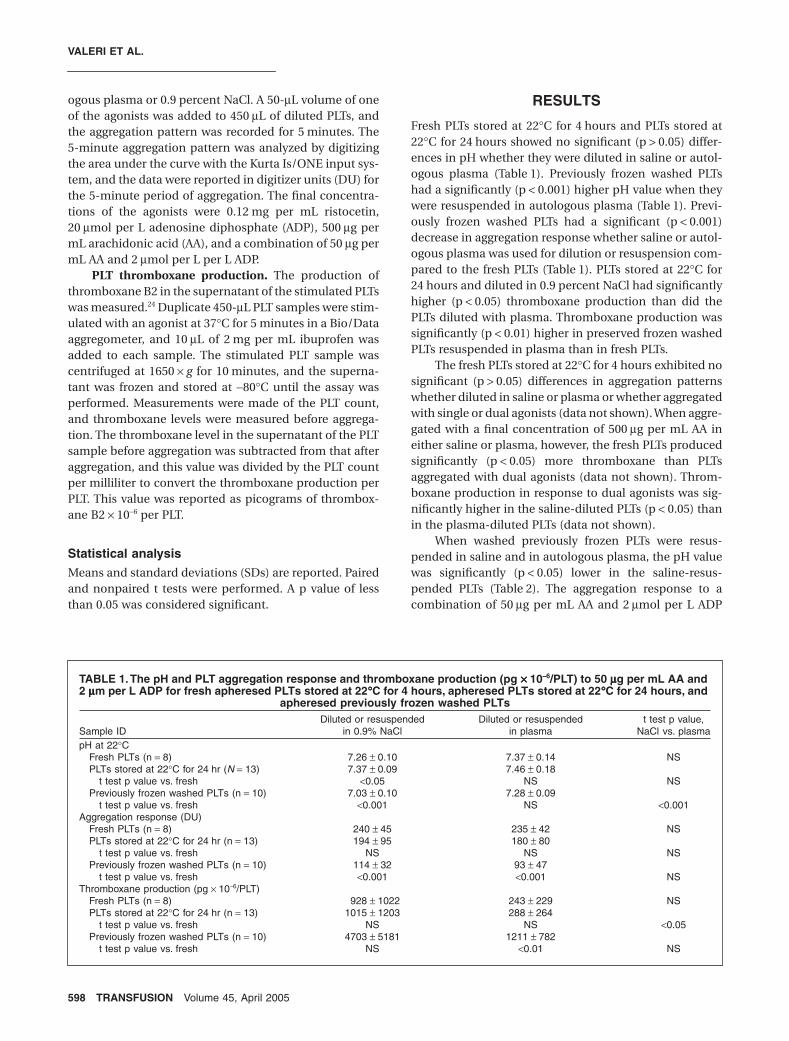
VALERI ET AL.
598 TRANSFUSION
Volume 45, April 2005
ogous plasma or 0.9 percent NaCl. A 50-
m
L volume of oneof the agonists was added to 450
m
L of diluted PLTs, andthe aggregation pattern was recorded for 5 minutes. The5-minute aggregation pattern was analyzed by digitizingthe area under the curve with the Kurta Is/ONE input sys-tem, and the data were reported in digitizer units (DU) forthe 5-minute period of aggregation. The final concentra-tions of the agonists were 0.12 mg per mL ristocetin,20
m
mol per L adenosine diphosphate (ADP), 500
m
g permL arachidonic acid (AA), and a combination of 50
m
g permL AA and 2
m
mol per L per L ADP.
PLT thromboxane production.
The production ofthromboxane B2 in the supernatant of the stimulated PLTswas measured.
24
Duplicate 450-
m
L PLT samples were stim-ulated with an agonist at 37
∞
C for 5 minutes in a Bio/Dataaggregometer, and 10
m
L of 2 mg per mL ibuprofen wasadded to each sample. The stimulated PLT sample wascentrifuged at 1650
¥
g
for 10 minutes, and the superna-tant was frozen and stored at
-
80
∞
C until the assay wasperformed. Measurements were made of the PLT count,and thromboxane levels were measured before aggrega-tion. The thromboxane level in the supernatant of the PLTsample before aggregation was subtracted from that afteraggregation, and this value was divided by the PLT countper milliliter to convert the thromboxane production perPLT. This value was reported as picograms of thrombox-ane B2
¥
10
-
6
per PLT.
Statistical analysis
Means and standard deviations (SDs) are reported. Pairedand nonpaired t tests were performed. A p value of lessthan 0.05 was considered significant.
RESULTS
Fresh PLTs stored at 22
∞
C for 4 hours and PLTs stored at22
∞
C for 24 hours showed no significant (p
>
0.05) differ-ences in pH whether they were diluted in saline or autol-ogous plasma (Table 1). Previously frozen washed PLTshad a significantly (p
<
0.001) higher pH value when theywere resuspended in autologous plasma (Table 1). Previ-ously frozen washed PLTs had a significant (p
<
0.001)decrease in aggregation response whether saline or autol-ogous plasma was used for dilution or resuspension com-pared to the fresh PLTs (Table 1). PLTs stored at 22
∞
C for24 hours and diluted in 0.9 percent NaCl had significantlyhigher (p
<
0.05) thromboxane production than did thePLTs diluted with plasma. Thromboxane production wassignificantly (p
<
0.01) higher in preserved frozen washedPLTs resuspended in plasma than in fresh PLTs.
The fresh PLTs stored at 22
∞
C for 4 hours exhibited nosignificant (p
>
0.05) differences in aggregation patternswhether diluted in saline or plasma or whether aggregatedwith single or dual agonists (data not shown). When aggre-gated with a final concentration of 500
m
g per mL AA ineither saline or plasma, however, the fresh PLTs producedsignificantly (p
<
0.05) more thromboxane than PLTsaggregated with dual agonists (data not shown). Throm-boxane production in response to dual agonists was sig-nificantly higher in the saline-diluted PLTs (p
<
0.05) thanin the plasma-diluted PLTs (data not shown).
When washed previously frozen PLTs were resus-pended in saline and in autologous plasma, the pH valuewas significantly (p
<
0.05) lower in the saline-resus-pended PLTs (Table 2). The aggregation response to acombination of 50
m
g per mL AA and 2
m
mol per L ADP
TABLE 1. The pH and PLT aggregation response and thromboxane production (pg
¥¥¥¥
10----
6
/PLT) to 50
mmmm
g per mL AA and 2
mmmm
m per L ADP for fresh apheresed PLTs stored at 22
∞∞∞∞
C for 4 hours, apheresed PLTs stored at 22
∞∞∞∞
C for 24 hours, and apheresed previously frozen washed PLTs
Sample IDDiluted or resuspended
in 0.9% NaClDiluted or resuspended
in plasmat test p value,
NaCl vs. plasmapH at 22
∞
CFresh PLTs (n
=
8) 7.26
±
0.10 7.37
±
0.14 NSPLTs stored at 22
∞
C for 24 hr (
N
=
13) 7.37
±
0.09 7.46
±
0.18t test p value vs. fresh
<
0.05 NS NSPreviously frozen washed PLTs (n
=
10) 7.03
±
0.10 7.28
±
0.09t test p value vs. fresh
<
0.001 NS
<
0.001Aggregation response (DU)
Fresh PLTs (n
=
8) 240
±
45 235
±
42 NSPLTs stored at 22
∞
C for 24 hr (n
=
13) 194
±
95 180
±
80t test p value vs. fresh NS NS NS
Previously frozen washed PLTs (n
=
10) 114
±
32 93
±
47t test p value vs. fresh
<0.001 <0.001 NSThromboxane production (pg ¥ 10-6/PLT)
Fresh PLTs (n = 8) 928 ± 1022 243 ± 229 NSPLTs stored at 22∞C for 24 hr (n = 13) 1015 ± 1203 288 ± 264
t test p value vs. fresh NS NS <0.05Previously frozen washed PLTs (n = 10) 4703 ± 5181 1211 ± 782
t test p value vs. fresh NS <0.01 NS

AGGREGATION AND THROMBOXANE A2 PRODUCTION IN PLTs
Volume 45, April 2005 TRANSFUSION 599
was significantly (p < 0.005) lower in thepreviously frozen washed PLTs resus-pended in saline than in the previouslyfrozen washed PLTs resuspended inautologous plasma (Table 2). Throm-boxane production in fresh PLTs(p < 0.05), PLTs stored at 22∞C for24 hours (p < 0.05) and in previously fro-zen, washed PLTs (p < 0.005) was sig-nificantly higher when the PLTs werediluted with or resuspended in saline(Table 2). The aggregation responseincreased significantly (p < 0.05) as thepH increased (Table 3). The thrombox-ane level decreased significantly(p < 0.05) as the pH increased (Table 3).
The fresh apheresed PLTs showed asignificantly (p < 0.05) reduced aggrega-tion response to 20 mmol per L ADP thanto the other three agonists (Table 4). Inthe fresh apheresed PLTs thromboxaneproduction was significantly greater fol-lowing stimulation with 500 mg per mLthan after stimulation with 20 mmol perL ADP, 0.12 mg per mL ristocetin, or50 mg per mL AA and 2 mmol per L ADP(Table 4).
In the apheresed PLTs stored at 22∞C for 24 hours, theaggregation response to 20 mmol per L ADP was signifi-cantly lower (p < 0.05) than the aggregation response to50 mg per mL AA and 2 mmol per L ADP, 0.12 mg per mLristocetin, or 500 mg per mL AA (Table 5). Apheresed PLTs
stored at 22∞C for 24 hours and stimulated with a finalconcentration of 500 mg per mL AA showed significantly(p < 0.01) higher thromboxane production than PLTsstimulated with 50 mg per mL AA and 2 mmol per L ADP(Table 5). Thromboxane production in response to
TABLE 2. Hypotonic stress, PLT aggregation, thromboxane production, and pH in fresh apheresed PLTs stored at 22∞∞∞∞C for 4 hours, apheresed PLTs stored at 22∞∞∞∞C for 24 hours, and apheresed previously frozen washed PLTs*
Storage
Hypotonicstress (%)
Thromboxane B2†(pg ¥ 10-6/PLT) pH
PLT aggregation†(DU)
Plasma Saline Plasma Saline Plasma Saline Plasma SalineFresh PLTs stored at 22∞C for 4 hr
Mean 82.6 80.5 310 870 7.4 7.3SD 10.4 7.2 188 865 0.2 0.1Number 13 13 20 13 13 13Paired t test p value (plasma vs. saline) NS <0.05 NS
PLTs stored at 22∞C for 24 hrMean 82.9 74.1 191 1092 7.5 7.4SD 9.7 10.9 220 1166 0.1 0.1Number 17 17 20 17 17 17Paired t test p value (plasma vs. saline) <0.001 <0.05 NS
Previously frozenMean 15.8 0.0 440 2072 7.0 6.4 82.2 40.6SD 10.2 0.0 254 473 0.1 0.1 19.5 24.1Number 5 5 25 5 5 5 5 5Paired t test p value (plasma vs. saline) <0.05 <0.005 <0.05 <0.005
* The fresh and liquid-preserved PLTs were diluted with autologous plasma or 0.9 percent NaCl. Previously frozen washed PLTs were resuspended in autologous plasma or 0.9 percent NaCl.
† PLT aggregation and thromboxane production in response to a final concentration of a combination of 50 mg per mL AA and 2 mmol per L ADP.
TABLE 3. Aggregation response and thromboxane production in response to a combination of 50 mmmmg per mL AA and 2 mmmmm per L ADP in fresh apheresis ACD-anticoagulated PLTs stored at 22∞∞∞∞C for 4 hours subjected to increases
and decreases in pH values from the initial pH value of 7.2
pH value at 22∞CAggregation
response (DU)*Thromboxane production
(pg ¥ 10-6/PLT)*6.0 (n = 4) 51.4 ± 80.1 3468 ± 20816.6 (n = 4) 92.5 ± 21.5 743 ± 2897.2 (n = 4) 167.9 ± 104.9 454 ± 355†7.7 (n = 4) 196.7 ± 19.7† 344 ± 119†
* Significantly different (p < 0.05) by analysis of variance.† Significantly different (p < 0.05) from 6.0
TABLE 4. Aggregation response and thromboxane production in response to the addition of single and dual agonists to PLTs isolated from fresh apheresed PLTs isolated from ACD-anticoagulated blood and stored at
22∞∞∞∞C for 4 hours (final concentrations)
AgonistAggregation
response (DU)*Thromboxane production
(pg ¥ 10-6/PLT)*50 mg/mL AA plus 2 mmol/L ADP 223 ± 48 (n = 7) 355 ± 241 (n = 8)0.12 mg/mL ristocetin 277 ± 45 (n = 3) 85 ± 84 (n = 3)20 mmol/L ADP 174 ± 44† (n = 5) 57 ± 43† (n = 6)500 mg/mL AA 216 ± 13 (n = 5) 9565 ± 9266† (n = 6)
* Significantly different (p < 0.05) by analysis of variance.† Significantly different (p < 0.05) from AA and/or ADP.

VALERI ET AL.
600 TRANSFUSION Volume 45, April 2005
ristocetin alone and ADP alone was sig-nificantly reduced (p < 0.05) comparedto the combination of AA and ADP(Table 5).
In previously frozen washed PLTsresuspended in ACD-anticoagulatedplasma, a negligible aggregationresponse to 20 mmol per L ADP wasobserved, but aggregation responses to0.12 mg per mL ristocetin, 500 mg permL AA, or a combination of 50 mg permL AA and 2 mmol per L ADP wereobserved (Table 6). Stimulation with500 mg per mL AA produced significantly(p < 0.05) higher thromboxane produc-tion than stimulation with 50 mg per mLAA and 2 mmol per L ADP, but negligiblethromboxane production was observedwith stimulation with 20 mmol per LADP alone or 0.12 mg per mL ristocetinalone (Table 6).
In apheresed fresh PLTs stimulatedwith a final concentration of a combina-tion of 50 mg per mL AA and 2 mmol perL ADP, the thromboxane level progres-sively increased over the 5-minute incu-bation period (Fig. 1). A similar pattern,
although to a lesser degree, was observed in the apheresedliquid-preserved PLTs stored at 22∞C for 5 days (Fig. 1). Inthe washed previously frozen apheresed PLTs resus-pended in 0.9 percent NaCl, thromboxane productionincreased progressively and to a much greater degree thanthat seen in either fresh apheresed PLTs or 5-day-old liq-uid-preserved apheresed PLTs (Fig. 1).
Stimulation with 50 mg per mL AA and 2 mmol per LADP resulted in reduced aggregation response andreduced thromboxane B2 production in apheresed PLTsstored at 22∞C for 5 days (Fig. 2). The PLT aggregationresponse after freezing, thawing, washing, and resuspen-sion in ACD-anticoagulated plasma was similar to thatobserved before freezing (Fig. 2). Thromboxane produc-tion, however, was eight times greater after freezing thanbefore (Fig. 2).
The response to hypotonic stress was not significantly(p > 0.05) different whether the fresh apheresed PLTsstored at 22∞C for 4 hour were diluted with plasma or0.9 percent NaCl (Table 2). The thromboxane production,however, was significantly higher (p < 0.05) in the PLTsdiluted with 0.9 percent NaCl than in those diluted withplasma (Table 2).
In the apheresis PLTs stored at 22∞C for 24 hours, thehypotonic stress was significantly (p < 0.001) higher in thePLTs diluted with plasma than in the PLTs diluted with0.9 percent NaCl (Table 2). Thromboxane production inthese PLTs was significantly (p < 0.05) greater in the PLTs
TABLE 5. Aggregation response and thromboxane production in response to the addition of single and dual agonists to liquid-preserved apheresed PLTs isolated from ACD-anticoagulated blood and stored at 22∞∞∞∞C for 24
hours (final concentrations)
AgonistAggregation
response (DU)*Thromboxane production
(pg ¥ 10-6/PLT)*50 mg/mL AA plus 2 mmol/L ADP 214 ± 70 (n = 17) 486 ± 525 (n = 14)0.12 mg/mL ristocetin 268 ± 46 (n = 10) 35 ± 55† (n = 10)20 mmol/L ADP 171 ± 65† (n = 10) 78 ± 118† (n = 10)500 mg/mL AA 210 ± 28 (n = 16) 5602 ± 2148† (n = 6)
* Significantly different (p < 0.05) by analysis of variance.† Significantly different (p < 0.05) from AA and/or ADP.
TABLE 6. Aggregation response and thromboxane production in response to the addition of single and dual agonists to apheresed previously frozen
washed PLTs resuspended in ACD-anticoagulated plasma (final concentrations)
AgonistAggregation
response (DU)*Thromboxane production
(pg ¥ 10-6/PLT)*50 mg/mL AA plus 2 mmol/L ADP (n = 10) 84 ± 50 (n = 12) 2032 ± 2094 (n = 12)0.12 mg/mL ristocetin (n = 10) 59 ± 92 (n = 3) 4 ± 5 (n = 3)20 mmol/L ADP (n = 10) 3 ± 3† (n = 3) 7 ± 6 (n = 3)500 mg/mL AA (n = 10) 129 ± 85 (n = 12) 4523 ± 3027† (n = 12)
* Significantly different (p < 0.05) by analysis of variance.† Significantly different (p < 0.05) from AA and/or ADP.
Fig. 1. Thromboxane production (pg ¥¥¥¥ 10----6/PLT) during the 5-
minute period after treatment with a combination of 50 mmmmg per
mL AA and 2 mmmmmol per L ADP in fresh apheresed PLTs stored at
22∞∞∞∞C for 4 hours (�); apheresed liquid-preserved PLTs stored at
22∞∞∞∞C for 5 days (�); and apheresed previously frozen washed
PLTs resuspended in 0.9 percent NaCl (�; mean).

AGGREGATION AND THROMBOXANE A2 PRODUCTION IN PLTs
Volume 45, April 2005 TRANSFUSION 601
diluted with 0.9 percent NaCl than in PLTs diluted withplasma (Table 2).
The response to hypotonic stress was significantly(p < 0.05) higher when the previously frozen PLTs wereresuspended in ACD plasma than when they were resus-pended in 0.9 percent NaCl (Table 2). Washed previouslyfrozen PLTs resuspended in 0.9 percent NaCl producedsignificantly (p < 0.005) more thromboxane than PLTsresuspended in plasma (Table 2).
A mean recovery of 75.8 ± 4.4 percent (SD) wasobserved in 5 units of previously frozen PLTs whether theywere resuspended in PLT-poor plasma or 0.9 percentNaCl. The PLTs that were resuspended in plasma exhibitedsignificantly (p < 0.05) higher pH, significantly (p < 0.05)better response to hypotonic stress, significantly(p < 0.005) better PLT aggregation response to 50 mg perAA and 2 mmol per L ADP, and significantly (p < 0.005)reduced thromboxane production than the PLTs that wereresuspended in 0.9 percent NaCl (Table 2).
DISCUSSION
An accurate method of testing PLTs in vitro to assess theirfunction has yet to be discovered. Current in vitro mea-surements use the determination of PLT aggregation toagonists alone and in combination that are present at thebleeding site, such as collagen, ADP, epinephrine, throm-bin, and calcium. Thromboxane, a potent vasoconstrictorsubstance that has been shown to accumulate at thebleeding site, also aggregates PLTs.18-21 Significant correla-tions have been observed between the bleeding time andthe shed blood thromboxane levels collected at the tem-plate bleeding time site in humans and baboon subjectedto hypothermia,22-24 in patients after administration of
heparin,25 and in humans as a result ofa reduction in Hct.26
This study was performed toassess the response of fresh and pre-served PLTs to agonists that aggregatethe PLTs and at the same time to mea-sure the PLT production of thrombox-ane. Our data show that the agonistsand the pH and composition of themedia influenced both the aggrega-tion response and the production ofthromboxane in these PLTs.
The agonists ADP and ristocetinproduced aggregation of fresh PLTsand liquid-preserved PLTs, but only anegligible amount of thromboxanewas produced. These findings aresimilar to those reported by Jin andassociates29 who found that the con-version of AA to thromboxane A2 wasnot required for PLT aggregation to
occur. AA alone or a combination of AA and ADP resultedin both PLT aggregation and thromboxane A2 productionin fresh PLTs.
We found that the liquid-preserved PLTs that werestored at 22∞C for 5 days before treatment with a combi-nation of AA and ADP had decreased PLT aggregationand decreased thromboxane A2 production. The PLTsthat were frozen after 24 hours of storage at 22∞Cthawed, washed, resuspended, and stimulated with acombination of AA and ADP had poor aggregationresponse but had increased thromboxane A2 production.PLTs that were frozen after 5 days of 22∞C storage,thawed, washed, resuspended, and stimulated with AAand ADP exhibited significantly increased thromboxaneA2 production but no significant change in aggregationresponse.
PLTs with increased pH exhibited an increased aggre-gation response, a decrease in thromboxane production,and an increase in PLT response to hypotonic stress. Whenthe pH of the medium was decreased, the PLT aggregationresponse decreased, thromboxane A2 production wasincreased, and PLT response to hypotonic stress wasdecreased.
The reduction in pH value to 6.4 in the previouslyfrozen washed PLTs resuspended in 0.9 percent NaCl wasassociated with zero PLT response to hypotonic stress, aresponse that was associated with increased permeabilityto AA and an increase in PLT production of thromboxaneA2. Five minutes after stimulation with AA and ADP,thromboxane A2 production was greater in the cryopre-served PLTs and lower in the liquid-preserved PLTs storedat 22∞C for 5 days than in the fresh PLTs. The PLTs that werestored at 22∞C for 5 days exhibited significantly greaterthromboxane production after freezing than before freez-
Fig. 2. (Left) Aggregation response (DU) and (right) thromboxane A2 production
(pg ¥¥¥¥ 10----6/PLT) in PLTs isolated by plateletpheresis with the Haemonetics MCS++++ instru-
ment, stored at 22∞∞∞∞C for 5 days, and tested before and after freezing. The previously
frozen washed PLTs were resuspended in autologous ACD-anticoagulated plasma. PLTs
were treated with 50 mmmmg per mL AA and 2 mmmmmol per L ADP (mean ±±±± SD).

VALERI ET AL.
602 TRANSFUSION Volume 45, April 2005
ing. The process of PLT freezing, thawing, washing, andresuspension in plasma stimulated thromboxane A2production.
How do these in vitro tests of PLT aggregation and PLTproduction of thromboxane relate to the in vivo functionof liquid-preserved and cryopreserved PLTs? A recentstudy published by Khuri and coworkers27 reported thatcryopreserved PLTs were more effective than liquid-pre-served PLTs in restoring hemostasis and reducing nonsur-gical blood loss in patients after cardiopulmonary bypasssurgery. These investigators found that although the sur-vival values of previously frozen washed PLTs were lowerthan liquid-preserved PLTs stored at 22∞C for a mean of3.4 days, the previously frozen and washed PLTs were sig-nificantly better in reducing nonsurgical blood loss andreducing the need for allogeneic red blood cells (RBCs)and fresh frozen plasma.27 The improved in vivo hemo-static function of cryopreserved PLTs was correlated withtheir procoagulant activity and their ability to producethromboxane at the bleeding time site.22-27 Khuri andassociates27 reported that the cryopreserved PLTs in vitroshowed a significantly lower aggregation response thanthe liquid-preserved PLTs and that after stimulation thecryopreserved PLTs produced more thromboxane thandid the fresh or liquid preserved PLTs.
A recent study was performed to assess the circula-tion and function of autologous fresh, liquid-preserved,and cryopreserved baboon PLTs transfused to correct anaspirin-induced thrombocytopathy.30 The bleeding timeand the shed blood level of thromboxane were measuredbefore and after aspirin treatment and following infusionof autologous nonaspirin treated PLTs stored at 22∞C for18 hours, 48 hours, 72 hours, or 5 days and autologouscryopreserved PLTs. Autologous PLTs stored at 22∞C for48 hours and cryopreserved PLTs reduced the bleedingtime and increased the shed blood thromboxane level atthe bleeding site. These data demonstrated that the reduc-tion in bleeding time was associated with an increase inthe shed blood thromboxane level.
It has been reported that RBCs activate PLTs.31-36 RBCsaccumulate at the bleeding site along with the tissue ago-nists to stimulate the PLTs to aggregate and to producethromboxane. In vitro studies have suggested that at Hctlevels of between 25 and 35 percent RBCs affect PLT func-tion by releasing ADP from RBCs.31 It has been reportedthat the combination of RBCs and collagen in vitro stim-ulates PLT thromboxane production better than collagenalone.34
In a study of eight men and eight women, the Hct hada significant effect on the shed blood thromboxane mea-sured at the template bleeding time site when the skintemperature ranged from 22 to 37∞C.24 At temperatures of37, 32, 28, and 22∞C, the male subjects had higher throm-boxane levels in the shed blood collected at the templatebleeding site and lower bleeding times than the female
subjects. The mean Hct value for the males was42 ± 1 vol percent (SD) and that for the female subjectswas 37 ± 2 vol percent (SD). This demonstrated that theHct affected the shed blood level of thromboxane A2 at thetemplate bleeding time site at each skin temperature thatwas studied.24 These data suggest that the presence ofRBCs in the shed blood may provide not only ADP but alsoAA for PLTs to produce thromboxane A2 at the bleedingtime site.24,34
The increased bleeding times observed in baboons,normal volunteers, and patients subjected to systemicand local hypothermia22-27 may be due to the increase inpH that occurs with hypothermia. The data reported inthis study show that when pH is increased, PLT aggrega-tion is increased and thromboxane production isdecreased, whereas when pH is reduced, PLT aggregationis reduced and thromboxane production is increased. Thedata suggest that PLT thromboxane production may bebetter than PLT aggregation as the in vitro test for predict-ing PLT function in vivo.
ACKNOWLEDGMENTS
The authors acknowledge the technical assistance of Stephanie
McCarter and Dongpo Cai and the editorial assistance of Cynthia
A. Valeri.
REFERENCES
1. Murphy S, Holme S, Nelson E, Carmen R. Paired comparison
of the in vivo and in vitro results of storage of platelet
concentrates in two containers. Transfusion 1984;24:31-4.
2. Holme S, Heaton WA, Courtright M. Improved in vivo and in
vitro viability of platelet concentrates stored for seven days
in a platelet additive solution. Br J Haematol 1987;66:233-8.
3. Murphy S, Rebulla P, Bertolini F, et al. In vitro assessment of
the quality of stored platelet concentrates. Transfus Med Rev
1994;8:29-36.
4. Holme S. Storage and quality assessment of platelets. Vox
Sang 1998;74(Suppl 2):207-16.
5. Rinder HM, Smith BR. In vitro evaluation of stored platelets:
is there hope for predicting posttransfusion platelet survival
and function. Transfusion 2003;43:2-6.
6. Murphy S. Utility of in vitro tests in predicting the in vivo
viability of stored platelets [letter to the editor]. Transfusion
2004;44:618-9.
7. International Forum. Evaluation of stored platelets. Vox
Sang 2004;86:203-23.
8. Valeri CR, Feingold H, Marchionni LD. The relation between
response to hypotonic stress and the 51Cr recovery in vivo
of preserved platelets. Transfusion 1974;14:331-7.
9. Holme S, Moroff G, Murphy S. A multi-laboratory evaluation
of in vitro platelet assays: the tests for extent of shape change
and response to hypotonic shock. Transfusion 1998;38:31-
40.

AGGREGATION AND THROMBOXANE A2 PRODUCTION IN PLTs
Volume 45, April 2005 TRANSFUSION 603
10. Reimers HJ, Packham MA, Kinlough-Rathbone RL, Mustard
JF. Effect of repeated treatment of rabbit platelets with low
concentrations of thrombin on their function, metabolism
and survival. Br J Haematol 1973;25:675-89.
11. Reimers HJ, Kinlough-Rathbone RL, Cazenave JP, et al. In
vitro and in vivo functions of thrombin-treated platelets.
Thromb Haemostat 1976;35:151-66.
12. Berger G, Hartwell D, Wagner D. P-selectin and platelet
clearance. Blood 1998;92:4446-52.
13. Michelson AD, Barnard MR, Hechtman HB, et al. In vivo
tracking of platelets: circulating degranulated platelets
rapidly lose surface P-selectin but continue to circulate and
function. Proc Natl Acad Sci U S A 1996;93:11877-82.
14. Valeri CR, Ragno G, Marks PE, et al. Effect of thrombopoietin
alone and a combination of cytochalasin B and EGTA-AM
on the survival and function of autologous baboon platelets
stored at 4∞C for as long as 5 days. Transfusion 2004;44:865-
70.
15. DiMinnio G, Silver MJ, Murphy S. Stored human platelets
retain full aggregation potential in response to pairs of
aggregating agents. Blood 1982;59:563-8.
16. Carr ME. In vitro assessment of platelet function. Transfus
Med Rev 1997;11:106-15.
17. Fitzgerald GA. Mechanisms of platelet activation:
thromboxane A2 as an amplifying signal for other agonists.
Am J Cardiol 1991;68:11B-15B.
18. Thorngren M, Shafi S, Born GV. Thromboxane synthesis in
skin-bleeding time blood and in clotted venous blood before
and after administration of acetylsalicylic acid. Lancet
1983;1:1075-8.
19. Stampfer MJ, Jakubowski JA, Deykin DA, et al. Effect of
alternate-day regular and enteric-coated aspirin on platelet
aggregation, bleeding time, and thromboxane A2 levels in
bleeding time blood. Am J Med 1986;81:400-4.
20. Gerrard JM, Taback S, Singhroy S, et al. In vivo measurement
of thromboxane B2 and 6-keto prostaglandin F1a in humans
in response to a standardized vascular injury and the
influence of aspirin. Circulation 1989;79:29-38.
21. Gerrard JM, Docherty JC, Israels SJ, et al. A reassessment of
the bleeding time: association of age, hematocrit, platelet
funciton, von Willebrand factor, and bleeding time
thromboxane B2 with the length of the bleeding time. Clin
Invest Med 1989;12:165-71.
22. Valeri CR, Feingold H, Cassidy G, et al. Hypothermia-
induced reversible platelet dysfunction. Ann Surg
1987;205:175-81.
23. Valeri CR, Khabbaz K, Khuri SF, et al. Effect of skin
temperature on platelet function in patients undergoing
extracorporeal bypass. J Thorac Cardiovasc Surg 1992;
104:108-16.
24. Valeri CR, MacGregor H, Cassidy G, Tinney R, Pompei F.
Effects of temperature on bleeding time and clotting time in
normal male and female volunteers. Crit Care Med 1995;
23:698-704.
25. Khuri SF, Valeri CR, Loscalzo J, et al. Heparin causes platelet
dysfunction and induces fibrinolysis before
cardiopulmonary bypass. Ann Thorac Surg 1995;60:1008-14.
26. Valeri CR, Cassidy G, Pivacek LE, et al. Anemia-induced
increase in the bleeding time: implications for treatment of
non-surgical blood loss. Transfusion 2001;41:977-83.
27. Khuri SF, Healey N, MacGregor H, et al. comparison of the
effects of transfusions of cryopreserved and liquid-
preserved platelets on hemostasis and blood loss after
cardiopulmonary bypass. J Thorac Cardiovasc Surg
1999;117:172-84.
28. Feingold HM, Pivacek LE, Melaragno AJ, Valeri CR.
coagulation assays and platelet aggregation patterns in
human, baboon and canine blood. Am J Vet Res 1986;47:
2197-9.
29. Jin J, Quinton TM, Zhang J, Rittenhouse SE, Kunapuli SP.
Adenosine diphosphate (ADP)-induced thromboxane A2
generation in human platelets requires coordinated
signaling through integrin aIIbB3 and ADP receptors. Blood
2002;99:193-8.
30. Valeri CR, MacGregor H, Giorgio A, Ragno G. Circulation and
hemostatic function of autologous fresh, liquid preserved
and cryopreserved baboon platelets transfused to correct an
aspirin-induced thrombocytopathy. Transfusion 2002;42:
1206-16.
31. Alkhamis TM, Beissinger RL, Chediak JR. Artificial surface
effect on red blood cells and platelets in laminar shear flow.
Blood 1990;75:1568-75.
32. Santos MT, Valles J, Marcus AJ, et al. Enhancement of
platelet reactivity and modulation of eicosanoid production
by intact erythrocytes: a new approach to platelet activation
and recruitment. J Clin Invest 1991;87:571-80.
33. Marcus AJ. Thrombosis and inflammation as multicellular
processes: pathophysiologic significance of transcellular
mechanisms. Blood 1990;76:1903-7.
34. Valles J, Santos MT, Aznar J, et al. Erythrocytes metabolically
enhance collagen-induced platelet responsiveness via
increased thromboxane production, adenosine
diphosphate release, and recruitment. Blood 1991;78:154-
62.
35. Santos MT, Valles J, Aznar J, et al. Prothrombotic effects of
erythrocytes on platelet reactivity. Circulation 1997;95:63-8.
36. Valles J, Santos MT, Aznar J, et al. Platelet–erythrocyte
interactions enhance aIIbB3 integrin receptor activation and
P-selectin expression during platelet recruitment: down-
regulation by aspirin ex vivo. Blood 2002;99:3978-84.

1890 TRANSFUSION Volume 45, December 2005
Blackwell Science, LtdOxford, UKTRFTransfusion0041-11322005 American Association of Blood BanksDecember 2005451218901898Original ArticleFREEZING PLTs WITH 6% DMSOVALERI ET AL.
From the Naval Blood Research Laboratory and the Department
of Surgery, Boston VA Healthcare System, West Roxbury Division,
Boston, Massachusetts.
Address reprint requests to: C. Robert Valeri, Naval Blood
Research Laboratory, Boston, MA 02118; e-mail: navblood@
nbrl.org.
This work was supported by the U.S. Navy (Office of Naval
Research Contract N00014-00-1-0555) and by funding provided
to the U.S. Navy Bureau of Medicine and Surgery.
The opinions or assertions contained herein are those of the
authors and are not to be construed as official or reflecting the
views of the Navy Department or Naval Service at large.
Received for publication March 10, 2005; revision received
April 22, 2005, and accepted April 28, 2005.
doi: 10.1111/j.1537-2995.2005.00647.x
TRANSFUSION 2005;45:1890-1898.
B L O O D C O M P O N E N T S
Freezing human platelets with 6 percent dimethyl sulfoxide with removal of the supernatant solution before freezing and storage at
−−−−80°°°°C without postthaw processing
C. Robert Valeri, Gina Ragno, and Shukri Khuri
BACKGROUND: Platelets (PLTs) can be frozen with 6 percent dimethyl sulfoxide (DMSO) at −80°C for up to 2 years. This method has been modified by concentrating the PLTs and removing the supernatant before freezing.STUDY DESIGN AND METHODS: High-yield leukore-duced PLTs stored at 22°C for up to 5 days were divided into three equal volumes: one was frozen with 6 percent DMSO at −80°C, thawed, washed, and resuspended in plasma (old method with DMSO); the second was treated with 6 percent DMSO, concentrated to remove the super-natant DMSO, frozen at −80°C, thawed, and diluted with 0.9 percent NaCl (new method with DMSO); and the third was treated with 0.9 percent NaCl without DMSO, con-centrated to remove the supernatant solution, frozen at −80°C, thawed, and diluted with 0.9 percent NaCl (new method without DMSO).RESULTS: Freeze-thaw-wash recovery of PLTs frozen by the old method with DMSO was 74 ± 2 percent with 5 percent PLT microparticles. Freeze-thaw recovery was 94 ± 2 percent with 7 percent PLT microparticles (new method with DMSO) and 69 ± 9 percent with 15 percent PLT microparticles (new method without DMSO). Total DMSO in washed PLTs was 400 and 600 mg in PLTs concentrated before freezing. In vivo recovery of PLTs frozen by the new method with DMSO and transfused into normal volunteers was 30 percent and the life span was 7 days.CONCLUSION: Concentrating PLTs before freezing simplified the procedure by eliminating postthaw washing. PLTs frozen by this method had more PLTs with reduced GPIb and increased annexin V binding than those frozen by the old method.
utologous human platelets (PLTs) frozen with6 percent dimethyl sulfoxide (DMSO), storedat −80°C, thawed, washed, and resuspended inautologous plasma have in vivo recovery and
life span values equivalent to autologous human liquidpreserved PLTs stored at 22°C for 5 days, but they haveimproved hemostatic function.1,2 In stable thrombocy-topenic patients, allogeneic PLTs frozen with 6 percentDMSO stored at −80°C for at least 2 years, thawed, washed,and resuspended in autologous plasma had freeze-thaw-wash recovery values of approximately 75 percent and invivo recovery values of 50 percent of the fresh allogeneicPLTs.3
Studies performed in baboons transfused with autol-ogous fresh, liquid preserved, or previously frozen washedPLTs demonstrated that previously frozen washed PLTshad slightly increased in vivo recovery and significantlybetter function than liquid-preserved autologous PLTsstored at 22°C for 5 days by their ability to reduce an aspi-rin-induced extended bleeding time and to produce shedblood thromboxane at the bleeding time site.4
In a previous study, patients undergoing cardiopul-monary bypass surgery were transfused PLTs that hadbeen frozen with 6 percent DMSO and stored at −80°C for
A

FREEZING PLTs WITH 6% DMSO
Volume 45, December 2005 TRANSFUSION 1891
as long as 2 years and after thawing and washing wereresuspended in acid citrate dextrose (ACD)-anticoagu-lated plasma for as long as 5 hours. These PLTs exhibitedgreater reduction in nonsurgical blood loss and requiredfewer transfusions of red blood cells (RBCs) and fresh-frozen plasma (FFP) than patients who received liquid-preserved PLTs that had been stored at 22°C for a mean of3.4 days.5 In that study, the previously frozen washed PLTsproduced more thromboxane A2 than did the liquid-pre-served PLTs after stimulation with arachidonic acid andadenosine diphosphate (ADP)5 and accumulated morefactor (F) V on the PLTs than did the liquid-preservedPLTs.5 The procoagulant activity and the increased throm-boxane production in the previously frozen washed PLTsproduced improved hemostasis in the patients aftertransfusion, which resulted in reduced nonsurgical bloodloss and reduced requirements for allogeneic RBCs andFFP.5
The purpose of this study was to evaluate our modi-fied method of PLT freezing in which the supernatantDMSO is removed before freezing, a modification thateliminates the need for postthaw washing and simplifiedthe cryopreservation procedure.
MATERIALS AND METHODS
At the Naval Blood Research Laboratory (Boston, MA),PLTs were collected by plateletpheresis from volunteerdonors who met the requirements of the AABB. Thedonors took no medications known to affect PLT functionfor 10 days before donation. With a PLT collection system(Haemonetics MCS+, Haemonetics Corporation, Brain-tree, MA), approximately 3.5 × 1011 to 4.0 × 1011, PLTs werecollected from the donor into ACD (NIH, Formula A, Bax-ter Healthcare Corp., Fenwal Division, Deerfield, IL) at aratio of 1 vol of ACD to 10 vol of blood. The study wasreviewed and approved by the Institutional Review Boardfor Human Research, Boston University Medical Center(Boston, MA). Informed consent was obtained from eachvolunteer.
At the American Red Cross, Northeast Region(Dedham, MA), PLTs were collected from each donor byplateletpheresis with two different instruments (COBESpectra, Gambro BCT, Lakewood, CO; and Amicus, Baxter,Deerfield, IL) at a ratio of 10 vol of blood to 1 vol of ACD(Formula A). The volunteer donors met the requirementsof the AABB and took no medication known to affect PLTfunction for 10 days before donation. The study wasreviewed and approved by the Institutional Review Boardfor Human Research, American Red Cross (Washington,DC). Informed consent was obtained from each donor.The high-yield PLTs that were leukoreduced had a totalWBC count of 5 × 106, contained more than 4.0 × 1011 PLTs,and were stored in two 200- to 300-mL volumes of plasmain 1000-mL CLX plastic bags.
Liquid preservation at 22°°°°CAt the NBRL, PLTs were collected and stored in 1000-mLCLX (tri-2-ethylhexyl trimellitate) plastic bags at roomtemperature in a stationary position for 4 hours, afterwhich they were stored for as long as 5 days at 22°C onan Eberbach shaker operated at 70 lateral excursions perminute.
The high-yield PLTs collected at the American RedCross, Northeast Region, were transported at room tem-perature to the NBRL where they were stored at 22°C foras long as 6 days on an Eberbach shaker operated at 70lateral excursions per minute.
Cryopreservation of the PLTs
The leukoreduced high-yield PLTs isolated with the COBESpectra and the Amicus instruments were stored in 2 volof 200 to 300 mL of plasma in the 1000-mL CLX plastic bagat 22°C for as long as 5 days. The 2 vol of PLT-rich plasmawere pooled and then divided into three equal volumes.
A volume of 27 percent DMSO in 0.9 percent NaClwas added to 1 vol of the PLT-rich plasma to achieve a finalconcentration of 6 percent DMSO in a 1000-mL polyvinyl-chloride (PVC) plastic bag. The plastic bag was placed inan aluminum container along with a 150-mL PVC plasticbag containing 50 mL of autologous ACD-anticoagulatedplasma and stored at the bottom of a −80°C mechanicalfreezer at −80°C for at least 2 months. The PLTs werethawed in a water bath maintained at 42°C; diluted with250 mL of 0.9 percent NaCl, 0.2 g percent glucose, and40 mg percent inorganic phosphorus, pH 5.0; and con-centrated by centrifugation at 4000 × g for 5 minutes. Thesupernatant solution was removed and the PLTs wereresuspended in 50 mL of the autologous plasma andstored at 22°C for as long as 6 hours without agitation. Thisprocedure is referred to as the old method with DMSO.
To the second volume of the PLT-rich plasma, a vol-ume of 27 percent DMSO in 0.9 percent NaCl was addedto achieve a final concentration of 6 percent DMSO forprocessing by the new method with DMSO. A volume of0.9 percent NaCl without DMSO was added to the thirdvolume of PLT-rich plasma for processing by the newmethod without DMSO. These PLTs processed by the newmethod were transferred into a 300-mL PVC plastic bagand centrifuged at 1250 × g for 10 minutes. All the super-natant solution was removed. This reduced the residualamount of DMSO in the DMSO frozen units by at least95 percent. The 300-mL PVC plastic bag containing 10 mLof the PLT concentrate was placed in a polyester plasticbag inside a rigid cardboard box, and the PLTs were frozenat the bottom of a −80°C mechanical freezer for at least2 months. The freezing rate was measured with a data log-ging system (Fluke Instruments, Everett, WA) with a ther-mocouple taped onto the PVC plastic bag. Before thawing,the polyester plastic bag was removed from the PVC bag

VALERI ET AL.
1892 TRANSFUSION Volume 45, December 2005
containing the PLTs. The PLTs were thawed in a thawingbath (Thermogenesis, Rancho Cordoba, CA) maintainedat 36°C in approximately 5 minutes. The PLTs were dilutedwith 0.9 percent NaCl and stored at room temperature foras long as 6 hours without agitation.
A special study was performed to assess the effect ofdiluting the thawed PLTs with 0.9 percent NaCl or plasmaon the pH of the PLTs after storage at 22°C for 6 hours.Ten units of PLT-rich plasma were treated with 6 percentDMSO, concentrated to remove the supernatant DMSO,and frozen by storage at the bottom of a −80°C mechanicalfreezer. After being thawed, 5 units were diluted with20 mL of 0.9 percent NaCl and the other 5 units werediluted with 20 mL of autologous plasma. These PLTs werestored at 22°C without agitation for as long as 6 hours, andthe pH at 22°C was measured.
111In-oxine labeling of autologous PLTs before freezing
Before freezing, two plateletpheresis units collected in theHaemonetics MCS+ and stored at 22°C for 4 hours withoutagitation were each labeled with 111In-oxine for the twoautologous PLT transfusions. The PLTs were diluted with100 mL of sterile 0.9 percent sodium chloride solution andconcentrated by centrifugation at 4500 × g for 5 minutesat 22°C. All the supernatant solution was removed and thePLT pellet was resuspended in 30 mL of 0.9 percentsodium chloride. Approximately 1 mCi of 111In-oxine wasadded to the PLTs with gentle agitation over a 5-minuteperiod, and the PLTs were rotated for 30 minutes at 100lateral excursions per minute in a 37°C incubator. Thelabeled PLTs were diluted with 100 mL of autologous PLTpoor plasma and 10 mL of ACD and concentrated by cen-trifugation at 4500 × g for 5 minutes, and all the superna-tant solution was removed.
Freezing of the 111In-oxine–labeled autologous PLTs isolated with the Haemonetics MCS++++The 111In-oxine labeled PLT concentrate was treated witha volume of 27 percent DMSO in 0.9 percent NaCl toachieve a final DMSO concentration of 6 percent DMSOand transferred to a 300-mL PVC plastic bag. The PLTswere concentrated by centrifugation at 1250 × g for10 minutes, all the supernatant was removed, and the PLTswere resuspended in 10 mL of the 6 percent DMSO solu-tion. The 300-mL PVC plastic bag was placed in a polyesterplastic bag inside in a cardboard box, and the PLTs werefrozen on the bottom of a −80°C freezer for only 48 hours.
The PVC plastic bag containing the frozen PLTs wasremoved from the polyester plastic bag and placed in aplasma thawer for 5 minutes to achieve a surface temper-ature of 34°C (Thermogenesis). The 10-mL volume ofthawed PLTs was diluted with 10 mL of 0.9 percent NaCl.
The freeze-thaw and freeze-thaw-wash recovery val-ues were determined from the PLT count measured withan automated blood cell counter (Coulter STKS, Beck-man-Coulter Corp., Hialeah, FL) and the volume of thePLTs before and after the freeze-thaw and freeze-thaw-wash procedures.
In vivo survival of autologous 111In-oxine–labeled PLTs
The 10-mL volume of 111In-oxine–labeled previously fro-zen PLTs was diluted with 10 mL of 0.9 percent NaCl andstored at 22°C for up to 4 h before the in vitro and in vivotesting. On the day of the autotransfusion, the 111In-oxineradioactivity was measured in the thawed PLTs and in thecell-free supernatant. PLT survival was estimated from thecell-associated radioactivity in the blood, the total bloodvolume, and the total cellular radioactivity infused.4,6 Thetotal blood volume was estimated from the plasma volumemeasured with 125I-albumin and the total body hematocrit(Hct; peripheral venous Hct multiplied by 0.89).3 PLTrecovery during the 1- to 2-hour posttransfusion periodand the life span during the 7-day posttransfusion periodwere measured. PLT survivals were measured 1, 2, 24, and48 hours and 5 and 7 days after autotransfusion. Bloodsamples were collected for measurements of hemoglobinconcentration, Hct, PLT count, and mean PLT volume inthe Coulter STKS counter. The plasma pH was measuredat 22°C with a benchtop pH meter (Orion Model 520AThermo Electron Corp., Waltham, MA). Gas chromatogra-phy (Model 7620A, Hewlett-Packard Houston, TX) wasused to measure the level of DMSO in the washed andnonwashed previously frozen PLTs.7
The thromboelastogram measurement was madein the PLT-rich plasma treated with 0.3 mol per L CaCl2
(thromboelastogram hemostasis analyzer, Model 500,Haemoscope Corp., Miles, IL).8-10 The R-time measure-ment in the thromboelastogram was determined as theperiod of time that the sample was placed in the throm-boelastogram analyzer until fibrin formation occurred.
Flow cytometry testing
Anti-CD41a-APC allophycocyanin (GPIIb, clone HIP8),anti-CD42b-PE phycoerythrin (PE; GPIb, clone HIP1),annexin V–fluorescein isothiocyanate (FITC; all threereagents purchased from BD Biosciences PharMingen,San Diego, CA) were used in the testing. PLT preparationswere labeled as previously described.11,12 A detaileddescription of PLT flow cytometry methods can be foundin Krueger and colleagues.13 Briefly, PLTs were diluted inmodified HEPES-buffered Tyrode solution and labeledwith the indicated antibodies in buffer alone or in thepresence of 3 mmol per L calcium chloride and 2.5 mmolper L Gly-Pro-Arg-Pro, which inhibited fibrinogen poly-

FREEZING PLTs WITH 6% DMSO
Volume 45, December 2005 TRANSFUSION 1893
merization. Incubations were stopped by dilution inHEPES-buffered Tyrode solution containing 1 percentultrapure formaldehyde (Polysciences, Warrington, PA).Nonspecific antibody background binding was deter-mined with the appropriately labeled isotypic controlimmunoglobulin G.
The prepared samples were analyzed in a flow cytom-eter (Coulter FC500, Beckman-Coulter) which was cali-brated daily with calibration beads (Flow-Check andFlow-Set, Beckman-Coulter). Appropriate color compen-sation was established for FITC and PE with single-labeledcontrols. PLTs were identified on the basis of their charac-teristic log forward and side light scatter and binding ofCD41a-APC (GPIIb). A minimum of 5000 PLTs were col-lected per sample, and data were saved in flow cytometrystandard listmode files.
The testing of the PLTs to measure the mean fluores-cence intensity (MFI) of GPIb and annexin V binding onPLTs and PLT microparticles on a gated FL1 versus FL2dotplot produced four quadrants in the Coulter FC500flow cytometer. Quadrant 1 detected the MFI of normalGPIb and reduced annexin V-binding PLTs. Quadrant2 detected the MFI of reduced GPIb and increasedannexin V-binding PLTs. Quadrant 3 detected MFI ofreduced GPIb and reduced annexin V binding of PLTmicroparticles, and Quadrant 4 detected MFI of reducedGPIb and increased annexin V binding of PLT microparti-cles. The total MFI of GPIb and annexin V binding to PLTsin Quadrants 1 and 2 was calculated from the total num-ber of PLTs in C1 and C2 quadrants and the MFI that wasmeasured in the C1 and C2 quadrants. Measurementswere made of the MFI of the normal GPIb and reducedannexin V binding for all the PLTs in C1 quadrant, the MFIof the reduced GPIb and increased annexin V binding forall the PLTs in C2 quadrant, and the ratio of the total GPIbMFI and total annexin V MFI in C1 and C2 quadrants. Thepercentage of PLT microparticles in the C4 quadrant wasalso measured for the PLTs frozen by the three differentfreezing procedures and for the liquid-preserved PLTsstored at 22°C with agitation for 3 to 6 days.
Statistical analyses
Statistical analyses were performed with software (SAS,SAS Institute, Inc., Cary, NC). The means and standarddeviations (SDs) are reported. Differences in means wereanalyzed with paired and nonpaired t tests. A p value ofless than 0.05 was considered significant.
RESULTS
PLTs stored at 22°C with agitation for the 3- to 6-dayperiod exhibited a decrease in the number of GPIb normaland reduced annexin V-binding PLTs and an increase inthe number of reduced GPIb and increased annexin V-
binding PLTs (Figs. 1 and 2). They also exhibited a 2 to3 percent increase in PLT microparticles (Fig. 3). The R-time of the thromboelastogram for PLTs stored at 22°C forthe 3- to 6-day period was 10 minutes and a mean pHvalue of 6.27 was observed for the PLT medium stored at22°C for 6 days.
Some of the PLTs were treated with DMSO and somewere not before concentration by centrifugation andremoval of the supernatant solution. The PVC plastic bagcontaining the PLTs was covered with a polyester plasticbag and placed in a rigid cardboard box at the bottom ofa −80°C mechanical freezer and frozen at 2 to 3°C perminute from +20 C to −60°C (Fig. 4). No breakage wasobserved for PLTs frozen with the old and new methods.
The PLTs frozen with 6 percent DMSO, washed, andresuspended in plasma (referred to as the old method withDMSO) had a mean freeze-thaw-wash recovery value of74 ± 7 percent (SD; Fig. 5). The PLTs that were treated with
Fig. 1. MFI of PLTs with normal GPIb and reduced annexin V
binding during storage of PLTs at 22°°°°C with agitation for 3 to
6 days (mean ±±±± SD).
Fig. 2. MFI of PLTs with reduced GPIb and increased annexin V
binding during storage of PLTs at 22°°°°C with agitation for 3 to
6 days (mean ±±±± SD).

VALERI ET AL.
1894 TRANSFUSION Volume 45, December 2005
6 percent DMSO and concentrated to remove the super-natant solution before freezing and after thawing werediluted with 0.9 percent NaCl (referred to as the newmethod with DMSO) had a mean freeze-thaw recoveryvalue of 94 ± 2 percent (SD). The PLTs that were treatedwith 0.9 percent NaCl without DMSO and concentrated toremove the supernatant solution before freezing and afterthawing were diluted with 0.9 percent NaCl (referred to asthe new method without DMSO) had a mean freeze-thawrecovery value of 69 ± 9 percent (SD; Fig. 5).
The PLTs that were frozen with DMSO by the oldmethod had a mean of 400 mg of DMSO in the unit. ThePLTs that were frozen with DMSO by the new method hada mean of 600 mg of DMSO in the unit. PLTs that were
frozen by the old method with DMSO contained 5 percentPLT microparticles and PLTs frozen by the new methodwith DMSO contained 7 percent PLT microparticles(Fig. 6). PLTs that were frozen by the new method without
Fig. 3. The percentage of PLT microparticles during storage of
PLTs at 22°°°°C with agitation for 3 to 6 days (mean ±±±± SD).
Fig. 4. The freezing rate of a 10-mL volume of 6 percent DMSO-
treated PLTs in the 300-mL PVC plastic bag placed in a polyester
plastic bag and stored in a cardboard box placed at the bottom
of a −−−−80°°°°C mechanical freezer. Thermocouples were placed on
the top (�) and bottom (�) of the PVC plastic bag.
Fig. 5. In vitro recovery of PLTs following the three different
freezing procedures. Mean ±±±± SD; n ==== 7. Paired t test: old versus
new, p <<<< 0.001; old versus no DMSO, NS; new versus no DMSO,
p <<<< 0.001. New method: DMSO added to 6 percent final concen-
tration, supernatant DMSO removed before freezing at −−−−80°°°°C,
and previously frozen PLTs thawed and diluted with 0.9 percent
NaCl (not washed). Old method: DMSO added to 6 percent final
concentration, frozen at −−−−80°°°°C and previously frozen PLTs
thawed, washed with 0.9 percent NaCl-0.2% glucose, and resus-
pended in plasma. No DMSO: 0.9 percent NaCl added to PLTs,
supernatant removed before freezing at −−−−80°°°°C, and previously
frozen PLTs thawed and diluted with 0.9 percent NaCl.
Fig. 6. Percentage of PLT microparticles following the three dif-
ferent freezing procedures. Mean ±±±± SD; n ==== 7. Paired t test: old
versus new, NS; old versus no DMSO, p <<<< 0.01; new versus no
DMSO, NS. New method: DMSO added to 6 percent final con-
centration, supernatant DMSO removed before freezing at
−−−−80°°°°C, and previously frozen PLTs thawed and diluted with
0.9 percent NaCl (not washed). Old method: DMSO added to
6 percent final concentration and frozen at −−−−80°°°°C and previ-
ously frozen PLTs thawed, washed with 0.9 percent NaCl-0.2%
glucose, and resuspended in plasma. No DMSO: 0.9 percent
NaCl added to PLTs, supernatant removed before freezing at
−−−−80°°°°C, and previously frozen PLTs thawed and diluted with
0.9 percent NaCl.

FREEZING PLTs WITH 6% DMSO
Volume 45, December 2005 TRANSFUSION 1895
DMSO contained 15 percent PLT microparticles (Fig. 6).The 5 units of PLTs that were frozen by the new methodwith DMSO and diluted with 20 mL of 0.9 percent NaClhad a mean pH value of 6.37 after postthaw storage at 22°Cwithout agitation for 6 hours (Table 1). The 5 units of PLTsthat were frozen by the new method with DMSO anddiluted with 20 mL of plasma had a mean pH value of 6.76after storage at room temperature without agitation for6 hours (Table 1).
After storage at room temperature for 4 hours withoutagitation, the 111In-oxine–labeled autologous PLTs thatwere frozen by the new method with DMSO exhibitedan in vivo recovery 1 to 2 hours after transfusion of30 percent, with a range of 28 to 31 percent and a life spanof 7 days for the two autotransfusions. No adverse eventswere observed in the two volunteers who received autol-ogous previously frozen PLTs.
Figure 7 illustrates that the percentage of normalGPIb and reduced annexin V binding PLTs was signifi-cantly (p < 0.05) higher by the old method with DMSOthan by the new PLT freezing method with DMSO. PLTsthat were frozen by the new method without DMSO had anegligible number of normal GPIb and reduced annexin Vbinding PLTs compared to PLTs that were frozen withDMSO by either the old or the new method.
Figure 8 illustrates that the percentage of reducedGPIb and increased annexin V binding PLTs was signifi-cantly (p < 0.01) higher by the new method with DMSOthan by the old method with DMSO. PLTs frozen by thenew method without DMSO had a significantly increasednumbers of reduced GPIb and increased annexin V-bind-ing PLTs than PLTs frozen with DMSO by either the oldmethod (p < 0.001) or the new method (p < 0.05).
DISCUSSION
Acceptable PLT preservation should ensure that both thesurvival and the function are maintained. The currentguidelines require only satisfactory PLT survival. It has
been assumed that the survival of the preserved PLTs cor-relates with PLT function. Studies on autologous pre-served baboon PLTs, however, demonstrated that thesurvival of the PLTs did not correlate with their function
TABLE 1. The pH of PLTs treated with DMSO, concentrated to remove the supernatant DMSO,
frozen, thawed, diluted with 20 mL of 0.9 percent NaCl or 20 mL of plasma, and stored at 22°°°°C for 6 hours
without agitation
SamplePLT count(×108/mL)
Time (hr) after thaw 0 2 4 6
Dilution with plasmaMean 4.06 6.85 6.83 6.81 6.76SD 0.36 0.05 0.06 0.06 0.06Number 5 5 5 5 5
Dilution with 0.9% NaClMean 3.83 6.49 6.46 6.41 6.37SD 0.19 0.07 0.09 0.10 0.11Number 5 5 5 5 5 Fig. 7. Percentage of PLTs with normal GPIb and reduced
annexin V binding following the three different freezing proce-
dures. Mean ±±±± SD; n ==== 7. Paired t test: old versus new, p <<<< 0.05;
old versus no DMSO, p <<<< 0.001; new versus no DMSO, p <<<< 0.01.
New method: DMSO added to 6 percent final concentration,
supernatant DMSO removed before freezing at −−−−80°°°°C, and pre-
viously frozen PLTs thawed and diluted with 0.9 percent NaCl
(not washed). Old method: DMSO added to 6 percent final con-
centration and frozen at −−−−80°°°°C and previously frozen PLTs
thawed, washed with 0.9 percent NaCl-0.2% glucose, and resus-
pended in plasma. No DMSO: 0.9 percent NaCl added to PLTs,
supernatant removed before freezing at −−−−80°°°°C, and previously
frozen PLTs thawed and diluted with 0.9 percent NaCl.
Fig. 8. The percentage of PLTs with reduced GPIb and increased
annexin V binding following the three different freezing proce-
dures. Mean ±±±± SD; n ==== 7. Paired t test: old versus new, p <<<< 0.01;
old versus no DMSO, p <<<< 0.001; new versus no DMSO, p <<<< 0.05.
New method: DMSO added to 6 percent final concentration,
supernatant DMSO removed before freezing at −−−−80°°°°C, and pre-
viously frozen PLTs thawed and diluted with 0.9 percent NaCl
(not washed). Old method: DMSO added to 6 percent final con-
centration and frozen at −−−−80°°°°C and previously frozen PLTs
thawed, washed with 0.9 percent NaCl-0.2% glucose, and resus-
pended in plasma. No DMSO: 0.9 percent NaCl added to PLTs,
supernatant removed before freezing at −−−−80°°°°C, and previously
frozen PLTs thawed and diluted with 0.9 percent NaCl.

VALERI ET AL.
1896 TRANSFUSION Volume 45, December 2005
to correct an aspirin-induced prolonged bleeding time,4
nor did we find any correlation between survival and func-tion of allogeneic preserved human PLTs transfused toanemic and thrombocytopenic patients after cardiopul-monary bypass surgery. The allogeneic previously frozenwashed PLTs had decreased posttransfusion survival com-pared to allogeneic liquid-preserved PLTs, but they signif-icantly reduced both nonsurgical blood loss and the needfor RBCs and FFP during the postoperative period com-pared to the liquid-preserved PLTs without any untowardeffects.5
The study reported here was performed to assess amodification of the method to freeze PLTs with 6 percentDMSO and storage at −80°C. The modification simplifiedthe freezing process by removing the supernatant solutioncontaining 95 percent of the DMSO before freezing (thenew method with DMSO). The PLTs were frozen at a rateof 2 to 3°C per minute by the storage of a 10-mL volumeof PLTs concentrated in 6 percent DMSO solution in a300 mL PVC plastic bags covered with a polyester plasticbag and stored in a rigid cardboard box placed at the bot-tom of a −80°C freezer. The amount of residual DMSO inthe previously frozen washed PLTs was 400 mg per unit,whereas that in the previously frozen nonwashed dilutedPLTs was 600 mg per unit. There is no significant differ-ence in the safety profile between 400 and 600 mg ofDMSO in the frozen PLTs processed by the old and newmethods with DMSO. The time required for thawing andwashing previously frozen PLTs resuspended in plasmawas 1 hour 15 minutes (the old method with DMSO),whereas the time required for thawing and diluting thepreviously frozen nonwashed PLTs with 0.9 percent NaClwas only 10 minutes (the new method with DMSO).
In a previous study, human and baboon PLTs thatwere frozen with 6 percent DMSO at −80°C and after thaw-ing and washing were resuspended in plasma were foundto have GPIb-normal and GPIb-reduced PLT popula-tions.11 In the baboon, there was a correlation between theautologous PLT GPIb-normal population and the 1 to 2-hour posttransfusion recovery value of 48 percent and PLTlife span of 6 days. Hoffmeister and associates14,15 havereported that the maintenance of the normal PLT GPIbcomplex was associated with normal in vivo survival ofmurine PLTs stored at 4°C. Bergmeier and associates16
have reported that the GPIb complex on in vitro aged orinjured murine PLTs was associated with their survival.Leytin and associates17 have reported that human PLTspreserved in the liquid state and transfused into rabbitstreated with ethyl palmitate had in vivo survival valuesthat correlated with the PLT GPIb complex.
In a study in baboons, the GPIb-reduced PLTs presentin PLTs frozen with 6 percent DMSO, stored at −80°C,thawed, washed, and resuspended in plasma accumu-lated the procoagulant FV and the GPIb-reduced FV-positive PLT population was rapidly removed from the
circulation within 15 minutes11 Lyophilized, reconstitutedautologous baboon PLTs were found to accumulate morePLT procoagulant FV than fresh PLTs and had in vivo sur-vival values of less than 15 minutes.18
A correlation has been observed between theimproved in vivo hemostatic function of cryopreservedPLTs processed by the old method with DMSO and theirprocoagulant activity and their ability to produce throm-boxane at the bleeding time site.5,19 The procoagulantactivity of the PLTs that were frozen by the old methodwith DMSO has been assessed from the accumulation ofFV and FX and the PLT binding of annexin V.5,11 Annexin Vbinding to cell surface–exposed phosphatidylserine canbe used to assess the procoagulant activity of PLTs and PLTmicroparticles.20-22 Phosphatidylserine on PLTs and PLT-derived microparticles support coagulation by providinga catalytic surface on which coagulation FVa and FXa bindand interact to catalyze later reactions in the coagulationcascade.20-22 Annexin V binding to phosphatidylserine alsoidentifies PLTs and PLT microparticles undergoing apop-tosis that are rapidly removed from the circulation by tis-sue macrophages.23
Analysis of PLTs that were treated with DMSO andthose not so treated, concentrated to remove the superna-tant solution, before freezing and after thawing, dilutedwith 0.9 percent NaCl showed that the PLTs that weretreated with DMSO had a freeze-thaw recovery of94 percent and 7 percent PLT microparticles compared toa freeze-thaw recovery of 69 and 15 percent PLT micropar-ticles for the PLTs without DMSO. This finding shows thatthe presence of 6 percent DMSO improved the freeze-thaw recovery value and reduced the percentage of PLTmicroparticles. The PLTs that were frozen with 6 percentDMSO at −80°C and after thawing were washed and resus-pended in plasma had a freeze-thaw-wash recovery of 74and 5 percent PLT microparticles. The washing procedureremoved 20 percent of the thawed PLTs and reduced thePLT microparticles to 5 percent.
The in vivo recovery 1 to 2 hours after the autotrans-fusion of the PLTs that were frozen by the new methodwith DMSO, diluted with 0.9 percent NaCl, and stored atroom temperature for 4 hours was approximately 30 per-cent with a life span of 7 days compared to that of 35 to40 percent and a life span of 7 days for the PLTs frozen bythe old method with DMSO and resuspended in plasma.3
PLT surface marker testing demonstrated that thePLTs that were frozen by the old method with DMSO hadsignificantly greater numbers of normal GPIb and reducedannexin V binding PLTs than the PLTs that were frozen bythe new method with DMSO which had significantlyincreased numbers of reduced GPIb and increasedannexin V-binding PLTs.
The PLTs frozen by the new method with DMSO,diluted with 0.9 percent NaCl, and stored at room temper-ature (22°C) for 6 hours without agitation had a mean pH

FREEZING PLTs WITH 6% DMSO
Volume 45, December 2005 TRANSFUSION 1897
value of 6.4. PLTs frozen by the old method with DMSO,resuspended in plasma after washing, and stored at roomtemperature for 6 hours had a mean pH value of 6.8.5 Thepreviously frozen PLTs that were resuspended in 0.9 per-cent NaCl after washing produced significantly morethromboxane A2 after stimulation with a combination ofarachidonic acid and ADP than the previously frozen PLTsthat were resuspended in plasma after washing.19 The PLTsfrozen by the new method with DMSO after thawingdiluted with 0.9 percent NaCl could not be tested in thethromboelastogram because the medium has an inade-quate concentration of plasma containing fibrinogen.
The in vivo survival of autologous DMSO-frozen PLTsprepared by the new method had an in vivo recoveryvalue 1 to 2 hours after autotransfusion that was approxi-mately 10 percent lower than the PLTs frozen by the oldmethod with DMSO (Table 2). The PLTs frozen withDMSO by the new method exhibited a significantlyincreased number of reduced GPIb and increasedannexin V-binding PLTs compared to PLTs frozen withDMSO by the old method.
Better in vivo recovery values 1 to 2 hours after trans-fusion and the PLT life span were associated with PLTswith normal GPIb and reduced annexin V binding. PLTswith reduced GPIb and increased annexin V binding wereassociated with improved hemostatic function, whichreduced nonsurgical blood loss. The reduced GPIb andincreased annexin V binding by PLTs and PLT microparti-cles, however, may be associated with thromboembolicevents in the recipients. Possible effects of PLT micropar-ticles in hemostasis include direct formation of the hemo-static plug, augmentation of PLT adhesion, support ofprothrombinase complex development, and regulation ofthrombus formation.24,25
Data have been reported by Khuri and associates5 onthe therapeutic benefit of allogeneic PLTs frozen by the oldmethod with DMSO in reducing nonsurgical blood losswithout producing adverse events in patients after car-diopulmonary bypass.5 The safety and therapeutic bene-fits of allogeneic PLTs frozen by the new method withDMSO need to be assessed to determine whether nonsur-gical blood loss can be reduced in patients after all typesof surgical procedures without producing adverse events.
The elimination of the postthaw wash-ing of the previously frozen PLTs hassimplified the procedure to provide PLTswith improved hemostatic function.
ACKNOWLEDGMENT
The editorial assistance of Cynthia A. Valeri is
acknowledged.
REFERENCES
1. Valeri CR. Hemostatic effectiveness of liquid-preserved and
previously frozen human platelets. N Engl J Med 1974;290:
353-8.
2. Valeri CR. The current state of platelet and granulocyte
cryopreservation. Crit Rev Clin Lab Sci 1981;14:21-74.
3. Melaragno AJ, Carciero R, Feingold H, et al.
Cryopreservation of human platelets using 6%
dimethylsulfoxide and storage at −80°C: effects of 2 years of
frozen storage at −80°C and transportation in dry ice. Vox
Sang 1985;49:245-58.
4. Valeri CR, MacGregor H, Giorgio A, Ragno G. Circulation and
hemostatic function of autologous fresh, liquid preserved,
and cryopreserved baboon platelets transfused to correct an
aspirin-induced thrombocytopathy. Transfusion 2002;42:
1206-16.
5. Khuri SF, Healy N, MacGregor H, et al. Comparison of
the effects of transfusions of cryopreserved and liquid-
preserved platelets on hemostasis and blood loss after
cardiopulmonary bypass. J Thorac Cardiovasc Surg
1999;117:172-84.
6. Valeri CR, Giorgio A, MacGregor H, Ragno G. Circulation
and distribution of autotransfused fresh, liquid-preserved,
and cryopreserved baboon platelets. Vox Sang 2002;83:347-
51.
7. Contreras TJ, Sheibley R, Valeri C. Accumulation of di-2-
ethylhexyl phthalate (DEHP) in whole blood, platelet
concentrates, and platelet poor plasma. Transfusion
1974;14:34-46.
8. Chandler WL. The thromboelastograph and the
thromboelastograph technique. Semin Thromb Hemost
1995;21:1-6.
9. Traverso CI, Caprini JA, Arcelus J, Arcelus M.
Thromboelastographic modifications induced by
intravenous and subcutaneous heparin administration.
Semin Thromb Hemost 1995;21:53-8.
10. Summaria L. Thromboelastographic study of fibrinolytic
agents. Semin Thromb Hemost 1995;21:63-71.
11. Barnard MR, MacGregor H, Ragno G, et al. Fresh liquid-
preserved, and cryopreserved platelets: adhesive surface
receptors and membrane procoagulant activity. Transfusion
1999;39:880-8.
12. Michelson AD, Barnard M, Hechtman HB, et al. In vivo
tracking of platelets: circulating degranulated platelets
TABLE 2. Comparison of the two methods of freezing human PLTs with 6 percent DMSO and storage at −−−−80°°°°C
Method of preservation
Cryopreserved PLTs with 6 percentDMSO and storage at −80°C
With postthawwashing
Without postthawwashing
Mean in vitro recovery (%) 70 90Bimodal population GPIb normal and GPIb reduced Yes YesPLT annexin V microparticles (%) 3-5 5-8In vivo recovery (%) 1 to 2 hr after transfusion 35-40 25-30Life span (days) 7 7Residual DMSO (mg) in the unit 400 600

VALERI ET AL.
1898 TRANSFUSION Volume 45, December 2005
rapidly lose surface P-selectin but continue to circulate and
function. Proc Natl Acad Sci U S A 1996;93:11877-82.
13. Krueger LA, Barnard MR, Frelinger AL, et al.
Immunophenotypic analysis of platelets. In: Robinson JP,
Darzynkiewicz Z, Dean PN, et al., editors. Current protocols
in cytometry. Vol. 1. New York: Wiley; 2002. p. 610.1-17.
14. Hoffmeister KM, Felbinger TW, Falet H, et al. The clearance
mechanism of chilled blood platelets. Cell 2003;112:87-97.
15. Hoffmeister KM, Josefsson EG, Isaac NA, et al. Glycosylation
restores survival of chilled blood platelets. Science 2003;
301:1531-4.
16. Bergmeier W, Burger PC, Piffath CL, et al. Metalloproteinase
inhibitors improve the recovery and hemostatic function of
in vitro-aged or -injured mouse platelets. Blood 2003;102:
4229-35.
17. Leytin V, Allen DJ, Gwozdz A, Garvey B, Freedman J. Role of
platelet surface glycoprotein Ibα and P-selectin in the
clearance of transfused platelet concentrates. Transfusion
2004;44:1487-95.
18. Valeri CR, MacGregor H, Barnard MR, et al. Survival of
biotin-X-NHS and 111In-oxine-labeled autologous fresh and
lyophilized reconstituted baboon platelets. Vox Sang
2005;88:122-9.
19. Valeri CR, MacGregor H, Ragno G. Correlation between in
vitro aggregation and thromboxane A2 production in fresh,
liquid-preserved, and cryopreserved human platelets:
effects of agonists, pH, and plasma and saline resuspension.
Transfusion 2005;45:596-603.
20. Xiao HY, Matsubayashi H, Bonderman DP, et al. Generation
of annexin V-positive platelets and shedding of micro-
particles with stimulus dependent procoagulant activity
during storage of platelets at 4°C. Transfusion 2000;40:
420-7.
21. Srivastava A, Wang J, Majumder B, et al. Localization of
phosphatidylserine binding sites to structural domains of
factorXa. J Biol Chem 2002;277:1855-63.
22. Wu JR, Zhou C, Majumder R, et al. Role of procoagulant
lipids in human prothrombin activation. 1. Prothrombin
activation by factor Xa in the absence of factor Va and in the
absence and presence of membranes. Biochemistry 2002;
43:935-49.
23. Li MO, Sarkisian MR, Mehal WZ, Rakic P, Fiavell RA.
Phosphatidylserine receptor is required for clearance of
apoptotic cells. Science 2003;302:1560-3.
24. George JN, Pickett EB, Sucerman S, et al. Platelet surface
glycoproteins: studies on resting and activated platelet and
platelet membrane microparticles in normal subjects, and
observations in patients during adult respiratory distress
syndrome and cardiac surgery. J Clin Invest 1986;78:340-8.
25. Owens MR. The role of platelet microparticles in
hemostasis. Transfus Med Rev 1994;8:37-44.

i l'-' '-1 .
'. l \ . _ l :
COMPARISON OF THE EFFECTS OF TRANSFUSIONS OF CRYOPRESERVED AND LIOUID.PRESERVEDPLATELETS ON HEMOSTASIS AND BLOOD LOSS AFTER GARDIOPULMONARY BYPASSShukri F. Khuri. MDUNancy Healey, BSaHollace MacGregor, BScMarc R. Barnard, MSbIrma O. Szymanski, MDbVladimir Birjiniuk, MDaAlan D. Michelson, MDbDavid R. Gagnon, MD, MPH, PhDdC. Robert Valeri. MDc
T h" institution of cardiopulmonary bypass (CpB)I elicits a hemostatic defect that leads to increased
blood loss after cardiac operations.l,2 Because the CpB-
From the Department of Surgery Brockton/West Roxbury VeteransAdministration Medical Center, Brigham and Women's Hospital,Harvard Medical School, Boston,a the Center for plateletFunction Studies, Department of Pediatrics, Surgery, andLaboratory Medicine, University of Massachusetts MedicalCenteq Worcester,b the Naval Blood Research Laboratory BostonUniversity School of Medicine, Boston, Boston University Schoolof Public Health," and the Massachusetts Veterans EpidemiologyResearch and Information Center,d Boston, Mass.
pported by the US Navy (Offrce of Naval Research ContractN00014-94-C-0149), with funds provided by the Naval MedicalResearch and Development Command, and the Richard WarrenSurgical Research and Educational Fund, Westwood, Mass.
objective: The aim of the study was to compare the clinical effects andhemostatic efficiency of transfusions of ptatelets preseryed in the frozenstate for as long as 2 years with transfusions of platelets preserved in theconventional manner for as long as 5 days in patients undergoing car-diopulmonary bypass. M ethods : Seventy-three patients were prospective-ly randomly assigned to receive transfusions of cryopreserved or liquid-preserved platelets. Nonsurgical blood loss was measured during andafter the operation. Bleeding time, hematologic variables, and the bleed-ing time site shed blood were assayed before cardiopulmonary bypassand at 30 minutes and 2, 4, and,24 hours after transfusion. In vitroplatelet function tests were conducted on platelets obtained fromhealthy volunteers. Results: No adverse sequelae of the transfusions wereobserved. Blood loss and the need for postoperative blood producttransfusions were lower in the group receiving cryopreserved platelets.Lower posttransfusion platelet increments and a tendency towarddecreased platelet survival were observed in patients receiving cryopre-served platelets. Hematocrit and plasma fibrinogen were significantlyhigher in this group, and the duration of intubation was shorter, Invitro, cryopreserved platelets demonstrated less aggregation, lower pH,and decreased response to hypotonic stress but generated more proco-agulant activity and thromboxane. conclusions: (l) Cryopreservedplatelet transfusions are superior to liquid-preserved platelets in reduc-ing blood loss and the need for blood product transfusions after car-diopulmonary bypass. (2) The reduction in blood loss in the patientsreceiving cryopreserved platelet transfusions after cardiopulmonarybypass probably reflects improved in vivo hemostatic function of cryo-preserved platelets. (3) Some in vitro measures of platelet quality (aggre-gation, pH, hypotonic stress) may not reflect in vivo quality of platelettransfusions after cardiopulmonary bypass, whereas other in vitro mea-sures (platelet procoagulant activity and thromboxane) do. (J ThoracCardiovasc Surg 1999 ;ll7 :17 2-84)
induced hemostatic dysfunction is related in part toplatelet dysfunction,3 platelet transfusion therapy hasbeen a major component in the management of bleed-
The opinions or assertions contained herein are those of the authorsand should not be construed as official or reflecting the views ofthe Navy Department or Naval Service at large.
Received for publication Feb 5, 1998; revisions requested March 24,1998; revisions received Aug 10, 1998; accepted for publicationAug 10, 1998.
Address for reprints: Shukri F. Khuri, MD, Surgical Service,Brockton/West Roxbury VA Medical Center, 1400 VFW park-way, West Roxbury, MA02132.
rzt1t93782
172

I
-
f4 Khuri et al
collected and frozen at University of Massachusetts MedicalCenter (Worcester, Mass) and then transported frozen,packed in dry ice, to the Naval Blood Research Laboratory(Boston), where they were stored at -80.C. As needed. thefrozen platelets from each ABO type were transported, againon dry ice, to the West Roxbury Veterans AdministrationMedical Center, where they were stored at -80.C in a mech-anical freezer until they were thawed, washed, resuspended,and stored in ACD plasma at 22C for as long as 5 hoursbefore infusion
Liquid-preserved platelets. pooled platelets were pre-pared from units of whole blood collected into citrate-phos-phate-dextrose anticoagulant that had been stored at roomtemperature for no longer than 8 hours before platelet isola-tion. The whole blood was centrifuged (20009 for 3 minutes)and the platelet-rich plasma was expressed into the attachedtransfer pack. The platelet-rich plasma was then centrifuged(50009 for 5 minutes) and all but 35 to 70 mL of the platelet_poor plasma was expressed into the second transfer pack. Theconcentrated platelets were stored undisturbed at 22c for Ihour before resuspension. The resuspended platelets werestored in CLX bags in incubators maintained at 22 + 2"Cwith rotation for as long as 5 days before pooling. No longerthan 4 hours before use, 5 to 7 units of platelets of the same
finO group were pooled in a 300-mL transfer pack or g to 10
.its were pooled in 600-mL transfer pack.Apheresed platelets were collected with a continuous-flow
centrifugation system (Fenwal CS3000 with pLT chamber).ACD (National Institutes of Health formula A) was used asthe anticoagulant at a ratio of 1 volume of ACD to l0 vol-umes of blood. The apheresed platelets were stored for aslong as 5 days in 300 mL plasma in 1000-mL CLX plasricbags- in incubators maintained at22" + 2"C with rotation.
Platelet aggregation in response to arachidonic acidand adenosine diphosphate.ls In vitro studies were donewith fresh, liquid-preserved, and previously frozen apheresisproducts. The platelet count for the in vitro testing wasadjusted to 5.0 x 108/mL with autologous platelet-poor-plas-ma and measured with an automated particle counter (coulterModel JT). A 50 pL combination of 0.5 mg/ml AA and 20pmol/L ADP was added to 450 pL diluted plarelets (finalconcentrations 50 1tg/mL AA and 2 pmolll ADp). Theplatelet aggregation pattern was recorded for 5 minutes. Thepatterns were analyzed by digitizing the area under the curvewith the Kurta Is/ONE input system (Kurta Corp, phoenix,Ariz) and the data were reported as digitizer units for the 5-minute period of aggregation.
Thromboxane B, assay.2t Thromboxane B, was measuredwith a commercially available radioimmunoassay (NewEngland Nuclear, Boston, Mass). Baseline levels of throm-
4*CLX = Tri(2)-ethylhexyl trimellitate (Cutter Laboratories, Berkeley,
F - - - r . - l : nt t r ( r l i l t I
The Journal of Thoracic andCardiovascular Surgery
January 1999
boxane were measured in the cell-free plasma, prepared bycentrifuging a 450-pL sample with 50 pL of saline solutionand 0.02 ng/mL ibuprofen at 16509 for l0 minutes. The cell-free plasma samples were frozen at -80"C until assay. In addi-tion, production of thromboxane B, per platelet was measuredin the supematant after aggregation with a combination of 50ytglmL AA and 2 Stmolfi- ADP. After 5 minures of aggrega-tion, ibuprofen (0.02 ng/ml final concentration) was added tothe cuvette to arrest thromboxane production and the samplewas placed on ice. The sample was then centrifuged (16509 at4"C for 10 minutes) and the plasma was frozen at -80"C untilassay as described previously. The thromboxane productionper platelet was calculated as follows:
Thromboxane production per platelet (pg) = (Aggregatedthromboxane B, value [pg] - Baseline thromboxane B, valuetpgl) / (Platelet count) / 0.1 mL
Platelet recovery from hypotonic stress.25 platelet countswere measured with an automated particle counter (Coultermodel JT). Response of the platelets to hypotonic stress wasdetermined with a Philips PU 8800 UVAflS spectrophotome-ter (Philips Electronic Instruments, Inc, Mahwah, NJ). Bothtest and reference positions of the spectrophotometer werezeroed at the same time with 600 pL cell-free plasma and 300pL saline solution. A 600-pL sample of the diluted apheresisproduct and a 300-pL volume of saline solution were placedin the test position and baseline optical density was recorded.A second 600-pL sample of apheresis product and a 300-pLvolume of water were placed in the test position and the opti-cal density was recorded for 10 minutes. percentage recoveryfrom hypotonic stress was calculated as follows:
Recovery from hypotonic stress (Vo) = [(Secondary decreasein transmittance for 10 minutes) / (Initial increase in trans-mittance)l x l00Vo
Plasma pFL Nondiluted platelet pheresis product sampleswere kept in sealed plastic test tubes at22C until the pH mea-surement was made. Measurements were made on an OrionSA (model 520A) pH meter (Orion Research, Inc, Boston,Mass) equipped with an Omega silver-silver chloride electroce(Omega PHB-G2; Omega Engineering, Inc, Stamford, Conn).
Procoagulant activities of fresh, liquid-preserved, and cry-opreserved platelets. This determination was performed aspreviously described elsewhere.30 Procoagulant activity wasdetermined by flow cytometric analysis of the platelet bind-ing of the coagulation factor V-specific monoclonal antibodyV237. Platelets were stimulated (10 minutes at37.C) eitherwith thrombin (2 U/mL), collagen (20 ytg/mL), and calciumchloride (3 mmol/L), with calcium chloride (3 mmol/L), orwith buffer alone. Values were expressed as the percentage ofmaximal V237 binding, as determined by the effect on freshplatelets of the calcium ionophore A23I8l (40 pmol/L) andcalcium chloride (3 mmol/L).

The Journal of Thoracic andCardiovascular SurgeryVolume 117, Number 1
quality (aggregation, pH, hypotonic stress) may not re-
flect the in vivo quality of platelet transfusions after
CPB, whereas other in vitro measures (platelet procoag-
ulant activity and thromboxane) do reflect this.
We greatly appreciate the efforts and advice of Dr MichaelCrittenden. We also acknowledge Mheir Doursounian,
Michael Zolkewitz, Gina Ragno, Maria Hansson-Wicher, andStephanie McCarter in the completion of this study.
R E F E R E N C E S
l. Khuri SF, Wolfe J, Josa M, Axford TC, Szymanski I, Assousa S,et al. Hematologic changes during and after cardiopulmonarybypass and their relationship to the bleeding time and nonsurgi-cal blood loss. J Thorac Cardiovasc Surg 1992;lO4:94-107.
2. Khuri SF, Michelson AD, Valeri CR. Effects of cardiopulmonarybypass on hemostasis. In: Loscalzo J, SchaferAI, editors. Throm-bosis and hemorrhage. Cambridge [MA]: Blackwell; 1994. p.105 I -73.
3. Kestin AS, Valeri CR, Khuri SF, Loscalzo J, Ellis PA, MacGregorH, et al. The platelet function defect of cardiopulmonary bypass.Blood 1993;82:107-17.
4. Murphy S, Rebulla P, Bertolini F, Holme S, Moroff G, Snyder E,et al. In vitro assessment of the quality of stored platelet concen-trates. Trans Med Rev 1994:8:29-36.
5. Spector JI, Skrabut EM, Valeri CR. Oxygen consumption, plateletaggregation, and release reactions in platelets freeze-preservedwith dimethysulfoxide. Transfusion | 97 7 ;17 :99 - 109.
6. Melaragno AJ, Carciero R, Feingold H, Talarico L, Weintraub L,Valeri CR. Cryopreservation of human platelets using 6Vodimethylsulfoxide and storage at -80" C: effects of 2 years offrozen storage at -80o C and transportation in dry ice. Vox Sang1985,49:245-58.
7. Dullemond-Westland AC, van Prooijen HC, Riemens MI,Akkerman JW. Cryopreservation disturbs stimulus-response cou-pling in a platelet subpopulation. Br J Haematol 1987.67:325-33.
8. Owens M, Cimino C, Donnelly J. Cryopreserved platelets havedecreased adhesive capacity. Transfusion 199 | ;3 l: I 60-3.
9. Shepherd KM, Sage RE, Barber S, O'Brien E. Platelet cryo-preservation. In vitro aggregation studies. Cryobiology 1984;21:39-43.
10. Valeri CR. Hemostatic effectiveness of liquid-preserved and pre-viously frozen human platelets. N Engl J Med 1974;290:353-8.
I l. Schiffer CA, Aisner J, Wiemik PH. Frozen autologous platelettransfusion for patients with leukemia. N Engl J Med 1978;299:7-12.
12. Blauhut B, Gross C, Necek S, Doran JE, Spath P, Lundsgaard-Hansen P. Effects of high-dose aprotinin on blood loss, plateletfunction, fibrinolysis, complement, and renal function after car-diopulmonary bypass. J Thorac Cardiovasc Surg l99l ;l0l :958-67.
13. Van Slyke DD, Phill ips RA, Dole VP, Hamilton PB, ArchibaldRM, Plazin J. Calculation of hemoglobin from blood specificgravities. J Biol Chem 1949:349-60.
14. Thompson CB, Eaton KA, Princiotta SM, Rushin CA, Valeri CR.Size dependent platelet subpopulations: relationship of plateletvolume to ultrastructure, enzymatic activity, and function. Br JHaematol I 982;50:509- I 9.
15. Feingold HM, Pivacek LE, Melaragno AJ, Valeri CR. Coagu-lation assays and platelet aggregation patterns in human, baboon,and canine blood. Am J Vet Res 1986;47:2197-9.
Khuri et al ttt\
16. Saba TM, Albert WH, Blumenstock FA, Evanega G, Staehler F,Cho F. Evaluation of a rapid immunoturbidometric assay foropsonic fibronectin in surgical and trauma patients. J Lab ClinMed l98l;98:482-91.
17. Teien AN, Lie M, Abildgaard U. Assay of heparin in plasmausing a chromogenic substrate for activated factor X. ThrombRes 1976;8:413-6.
18. Rylatt DB, Blake AS, Cottis LE, et al. An immunoassay forhuman D-dimer using monoclonal antibodies. Thromb Res 1983;3l:767-78.
19. Kingsley GR. Determination of serum total protein, albumin, andglobulin by the Buiret reactions. J Biol Chem 1939; l3 I : 197 -2O0.
20. Babson SR, Babson AL. Development and evaluation of a dis-posable device for performing simultaneous duplicate bleedingtime determinations. Am J Clin Pathol 1978:70:406-8.
21. Valeri CR, MacGregor H, Cassidy G, Tinney R, Pompei F. Effectsof temperature on bleeding time and clotting time in normal maleand female volunteers. Crit Care Med 1995;23:698-704.
22. Mannucci PM. Hemostatic drugs. N Engl J Med 1998;339:245-53 .
23. Genard JM, Taback S, Singhroy S, et al. In vivo measurement ofthromboxane B, and 6-keto-prostaglandin F,a in humans inresponse to a standard vascular injury and the influence ofaspirin. Circulation 1989 ;7 9 :29 -38.
24.Yaleri CR. Preservation of red cells and platelets: freezing, stor-age, recovery, and quality. In: Harris JR, editor.
ll"^* *qTltr_{n
and plasma fractionation. New York: Wiley-Liss; 1991. p. 127 -5
25. Valeri CR. The current state of platelet and granulocyte cryop-reservation. Crit Rev Clin Lab Sci 1981',14:21-74.
26.Yalei CR, Feingold H, Marchionni LD. The relation betweenresponse to hypotonic stress and the 5lCr recovery in vivo of pre-served platelets. Transfusion 197 4;4:331-7 .
27. Bevers EM, Comfurius P, Zwaal RF. Platelet procoagulant activ-ity: physiological significance and mechanisms of exposure.Blood Rev l99l :5:146-54.
23.Fitzgerald GA. Mechanisms of platelet activation: thromboxaneA, as an amplifying signal for other agonists. Am J Cardioll 9 9 l ; 6 8 : l l B - 5 B .
29. Johnson SA, Van Horn DL, Pederson HJ, Man J. The function ofplatef ets: a review. Transfusion | 966;6:3 - 17 .
30. Michelson AD, Barnard MR, Hechtman HB, MacGregor H,Connolly RJ, Loscalzo J, et al. In vivo tracking of platelets; cir-culating degranulated platelets rapidly lose surface P-selectin butcontinue to circulate and function. Proc Natl Acad Sci U S A1996;93:11877 -82.
Appendix
Platelet cryopreservation method. In brief, apheresedplatelets were collected with a continuous-flow centrifuga-tion system (Fenwal CS 3000, with the PLT chamber or theTNX-6 chamber; Baxter Healthcare, Deerfield, Ill). Anti-
coagulant citrate dextrose (ACD) was used as the anticoagu-lant at a ratio of I volume of ACD to between 8 and 1 I vol-umes of blood. A 50 to 15 mL volume of 277a dimethylsulfoxide in saline solution was added to the platelets cor5a\.tained in the 1000 mL polyvinyl chloride platelet-freeri,rl \
bag system (Fenwal 4R2986) to achieve a final dimethyl sul-foxide concentration of 6Vo.The platelets were placed in analuminum container, frozen at a tate of 2" to 3oC/min, andthen stored at -80'C in a mechanical freezer. Platelets were

F
I
482 Khuri et al
site was higher in the patients receiving the cryopre-served platelets than in those receiving the liquid-pre-served platelet transfusions. This difference ap-proached but did not reach statistical significancebecause of the relatively small sample size in whichthis measurement was performed. An increased abilityof platelets to generate thromboxane at the bleeding' time site has been shown to be a reliable measure of theplatelets' in vivo hemostati c effect.2r,23
This study was not designed to investigate the effectsof liquid-preserved pooled and those of liquid-pre-served apheresed platelet transfusions separatelybecause the administration of these liquid-preservedplatelet transfusions was predicated on the availabilityof either type in the blood bank. When the results forthese 2 types of liquid-preserved platelet transfusionswere analyzed separately, however, patients whoreceived the liquid-preserved pooled platelet transfu-sions were found to have required a significantly high-er volume of blood products after the operation thandid patients who received liquid-preserved apheresedplatelets (Fig 3, B). This was due in part to the higher
Flumes transfused with the pooled platelets. There,,uas also a tendency for the blood loss to be higher inthe patients who received the liquid-preserved pooledplatelet transfusions (Fig 3, A). The small sample sizeand poor statistical power, however, precluded thisstudy from making a definitive statement about themerits of liquid-preserved pooled platelets versus liq-uid-preserved apheresed platelets.
In this study decreased blood loss was demonstratedin the patients receiving cryopreserved platelets despitethe facts that smaller numbers of cryopreservedplatelets had been transfused (Table II) and the post-transfusion platelet increment was decreased in thepatients receiving cryopreserved platelet transfusions(Table IV). The decrease in platelet survival that wasobserved in the patients receiving the cryopreservedplatelets approached statistical significance and corrob-orated previous studies demonstrating inferior plateletsurvival with cryopreservation.24,2s These findings con-firmed in the setting of CPB data from a previous studyof healthy volunteers receiving aspirin that indicatedthat the in vivo hemostatic effect of transfused plateletsdid not correlate with their survival in the circulation.l0It is clear from this study that the decreased in vivo sur-vival did not interfere with the ability of the cryopre-
Jerved platelets to reduce blood loss after CpB.6rorCompared with standard liquid-preserved platelets,
''cryopreserved platelets have been reported to have
reductions in function in vitro, including adhesivecapacity,8 stimulus-response coupling,T aggregation,5,Tand granule release.5'6 They have also been found to
The Journal of Thoracic andCardiovascular Surgery
January 1999
have lower pH levels25 and more morphologic abnor-malities. This study also showed an adverse effect ofcryopreservation on in vitro quality of the platelets, asassessed by 3 commonly used tests. platelet aggregationin response to AA and ADP was lower in the cryopre-served platelets than in the liquid-preserved platelets.The pH of the milieu of the cryopreserved platelets waslower than that of the liquid-preserved platelets, and therecovery from hypotonic stress, which has been shownto correlate with in vivo platelet recovery26 was alsoless in the cryopreserved than the liquid-preservedplatelets. These in vitro tests did not correlate with thesuperior in vivo effect of the cryopreserved platelets thatwas shown by their ability to reduce blood loss afterCPB.
This study also assessed the thromboxane productionand the procoagulant activities of liquid-preserved andcryopreserved platelets, and the results of these in vitrotests did correlate with in vivo hemostatic function.Cryopreserved platelets generated more surface proco-agulant activity than did liquid-preserved platelets.Formation of a procoagulant surface for the assemblyof the coagulation system is an important function ofplatelets in the hemostatic process.2T Cryopreservedplatelets also generated more thromboxane than didliquid-preserved platelets. Thrombox ane Ar, a meta-bolic product of AA, causes vasoconstriction andplatelet aggregation.28 Through these mechanisms, theadditional generation of thromboxane by cryopre-served platelets is likely to have reduced blood lossfrom the site of injury. Additional studies are needed todetermine the mechanisms through which cryopreser-vation of platelets increases in vitro procoagulant activ-ity and thromboxane production and improves in vivohemostatic function.
In our study, patients receiving the cryopreservedplatelet transfusions had a significantly shorter dura-tion of postoperative intubation. This difference couldnot be explained by variables measured in this study.Possibly the shorter intubation reflects an improvementin pulmonary vascular permeability related to a salu-tary effect of cryopreserved platelets on endothelialintegrity. Johnson and associates2e have reported thatmaintenance of endothelial integrity is among the func-tions of platelets.
This study shows the following: (1) Cryopreservedplatelet transfusions are superior to liquid-preservedplatelets in reducing nonsurgical blood loss and the needfor blood product transfusions after CpB. (2) The reduc-tion in nonsurgical blood loss seen in the patients receiv-ing cryopreserved platelet transfusions probably reflectsimproved in vivo hemostatic function of cryopreservedplatelets after CPB. (3) Some in vitro measures of platelet
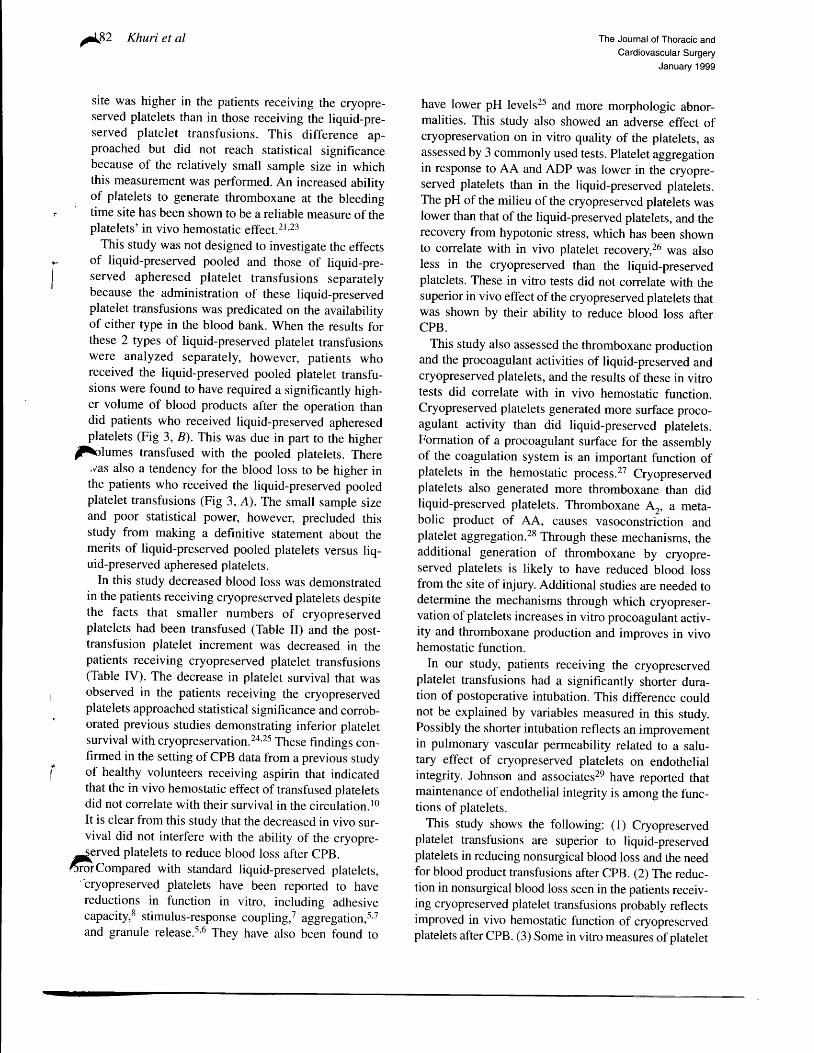
F
I
482 Khuri et al
site was higher in the patients receiving the cryopre-served platelets than in those receiving the liquid-pre-served platelet transfusions. This difference ap-proached but did not reach statistical significancebecause of the relatively small sample size in whichthis measurement was performed. An increased abilityof platelets to generate thromboxane at the bleeding' time site has been shown to be a reliable measure of theplatelets' in vivo hemostati c effect.2r,23
This study was not designed to investigate the effectsof liquid-preserved pooled and those of liquid-pre-served apheresed platelet transfusions separatelybecause the administration of these liquid-preservedplatelet transfusions was predicated on the availabilityof either type in the blood bank. When the results forthese 2 types of liquid-preserved platelet transfusionswere analyzed separately, however, patients whoreceived the liquid-preserved pooled platelet transfu-sions were found to have required a significantly high-er volume of blood products after the operation thandid patients who received liquid-preserved apheresedplatelets (Fig 3, B). This was due in part to the higher
Flumes transfused with the pooled platelets. There,,uas also a tendency for the blood loss to be higher inthe patients who received the liquid-preserved pooledplatelet transfusions (Fig 3, A). The small sample sizeand poor statistical power, however, precluded thisstudy from making a definitive statement about themerits of liquid-preserved pooled platelets versus liq-uid-preserved apheresed platelets.
In this study decreased blood loss was demonstratedin the patients receiving cryopreserved platelets despitethe facts that smaller numbers of cryopreservedplatelets had been transfused (Table II) and the post-transfusion platelet increment was decreased in thepatients receiving cryopreserved platelet transfusions(Table IV). The decrease in platelet survival that wasobserved in the patients receiving the cryopreservedplatelets approached statistical significance and corrob-orated previous studies demonstrating inferior plateletsurvival with cryopreservation.24,2s These findings con-firmed in the setting of CPB data from a previous studyof healthy volunteers receiving aspirin that indicatedthat the in vivo hemostatic effect of transfused plateletsdid not correlate with their survival in the circulation.l0It is clear from this study that the decreased in vivo sur-vival did not interfere with the ability of the cryopre-
Jerved platelets to reduce blood loss after CpB.6rorCompared with standard liquid-preserved platelets,
''cryopreserved platelets have been reported to have
reductions in function in vitro, including adhesivecapacity,8 stimulus-response coupling,T aggregation,5,Tand granule release.5'6 They have also been found to
The Journal of Thoracic andCardiovascular Surgery
January 1999
have lower pH levels25 and more morphologic abnor-malities. This study also showed an adverse effect ofcryopreservation on in vitro quality of the platelets, asassessed by 3 commonly used tests. platelet aggregationin response to AA and ADP was lower in the cryopre-served platelets than in the liquid-preserved platelets.The pH of the milieu of the cryopreserved platelets waslower than that of the liquid-preserved platelets, and therecovery from hypotonic stress, which has been shownto correlate with in vivo platelet recovery26 was alsoless in the cryopreserved than the liquid-preservedplatelets. These in vitro tests did not correlate with thesuperior in vivo effect of the cryopreserved platelets thatwas shown by their ability to reduce blood loss afterCPB.
This study also assessed the thromboxane productionand the procoagulant activities of liquid-preserved andcryopreserved platelets, and the results of these in vitrotests did correlate with in vivo hemostatic function.Cryopreserved platelets generated more surface proco-agulant activity than did liquid-preserved platelets.Formation of a procoagulant surface for the assemblyof the coagulation system is an important function ofplatelets in the hemostatic process.2T Cryopreservedplatelets also generated more thromboxane than didliquid-preserved platelets. Thrombox ane Ar, a meta-bolic product of AA, causes vasoconstriction andplatelet aggregation.28 Through these mechanisms, theadditional generation of thromboxane by cryopre-served platelets is likely to have reduced blood lossfrom the site of injury. Additional studies are needed todetermine the mechanisms through which cryopreser-vation of platelets increases in vitro procoagulant activ-ity and thromboxane production and improves in vivohemostatic function.
In our study, patients receiving the cryopreservedplatelet transfusions had a significantly shorter dura-tion of postoperative intubation. This difference couldnot be explained by variables measured in this study.Possibly the shorter intubation reflects an improvementin pulmonary vascular permeability related to a salu-tary effect of cryopreserved platelets on endothelialintegrity. Johnson and associates2e have reported thatmaintenance of endothelial integrity is among the func-tions of platelets.
This study shows the following: (1) Cryopreservedplatelet transfusions are superior to liquid-preservedplatelets in reducing nonsurgical blood loss and the needfor blood product transfusions after CpB. (2) The reduc-tion in nonsurgical blood loss seen in the patients receiv-ing cryopreserved platelet transfusions probably reflectsimproved in vivo hemostatic function of cryopreservedplatelets after CPB. (3) Some in vitro measures of platelet

The Journal of Thoracic and
Cardiovascular Surgery
Volume 117, Number 1
patients transfused with cryopreserved platelets than in
patients transfused with liquid-preserved platelets (Fig
2, B). The analysis of the blood products transfused was
also repeated after exclusion of the 6 patients undergo-
ing valve replacement in the liquid-preserved group
who had the longest duration of CPB. The mean + SD
of the total volume of blood products transfused (not
shown in Fig 2) continued to be significantly higher in
the patients who received the liquid-preserved platelet
transfusions than in those who received the cryopre-
served platelet transfusions (3426 x. 1963 mL vs 1933
+ 1042 mL, P = .0012). Fig 3, B, also shows that
patients transfused with liquid-preserved pooled
platelets received more platelets, fresh-frozen plasma,
and total blood products than did the patients who were
transfused with liquid-preserved apheresed platelets'
These statistical analyses of blood loss and transfu-
sion requirements were repeated without the exclusion
of any patient (analysis by intent to treat). statistically
significant differences continued to be observed
between the 2 types of platelet transfusion. Log trans-
formation of the data resulted in P = .04 for the differ-
ence in blood loss between the 2 groups and P = '008
for the difference in blood product transfusion between
the 2 groups.In vitro function of fresh, liquid-preserved, and
cryopreserved platelets (Table VI). The in vitro stud-
ies were performed on platelets obtained from healthy
volunteers. The pH of cryopreserved platelets was sig-
nificantly lower (P < .0001) than the pH of fresh
platelets; this in turn was significantly lower (P <
.0001) than the pH of the liquid-preserved platelets'
Likewise, the response to hypotonic stress was marked-
ly lower in the cryopreserved platelets than in either the
fresh (P = .003) or the liquid-preserved platelets (P <
.0001). Platelet aggregation after cryopreservation was
reduced with respect to that of the fresh platelets (P <
.0001); it was not significantly different from platelet
aggregation after 72 hours of liquid preservation'
In contrast, stimulation of cryopreserved platelets
with AA and ADP resulted in plasma levels of throm-
boxane B, that were significantly higher than those in
platelets stimulated after 72-hours of liquid preserva-
tion (P < .001). In addition, cryopreserved platelets had
more surface procoagulant activity than either liquid-
preserved platelets stored at 22"C for 3 to 4 days or
fresh platelets (Fig 4): 6.6Vo x' 2.77o of maximum for
cryopreserved platelets versus 0.9Vo + 0.57a of maxi-
mum for liquid-preserved platelets versus }'l%o + 0'3%o
of maximum for fresh platelets. Stimulation of the
platelets either with a combination of thrombin, colla-
gen, and calcium chloride or with calcium chloride
alone also resulted in significantly greater procoagulant
Khuri et al 181-=..{
activity on the surfaces of the cryopreserved platelets
than on the surfaces of the liquid-preserved platelets
€ie a).
Discussion
Bleeding during and after cardiac operations is relat-
ed to 2 causes: (1) the surgical incision that cuts into
blood vessels and vascularrzed tissues (surgical bleed-
ing) and (2) defects in hemostasis that prevent normal
clotting and that are amplified by the conditions of
CPB.2'3 This latter type of bleeding can be considered
nonsurgical because it does not originate from a spe-
cific anatomic incision or tear. Properly quantified,
nonsurgical blood loss has been used as a clinical tool
for the assessment of the hemostatic efficacy of phar-
macologic interventions.lz'2z In this prospective ran-
domized study, a specific effort was made to quantify
nonsurgical blood loss. In contrast to most other stud-
ies, which only measured the blood lost through the
chest tubes in the surgical intensive care unit, the mea-
surement of blood loss in this study was started in the
operating room after complete reversal with protamine
of the effects of heparin. During the ensuing period $\chest closure, all the blood oozing from the tissuel.
including the blood contained in the sponges, was col-
lected and accurately measured by a trained research
assistant. SurgiCal mishaps occurring during this period
and resulting in excessive surgical blood loss were
prospectively iclentified, and affected patients were
excluded from analysis. Patients brought back to the
operating room for control of excessive postoperative
bleeding were also excluded.The nonsurgical blood loss was significantly lower in
the patients receiving the cryopreserved platelets than
in the patients receiving the liquid-preserved platelets
(Frg 2, A), although the risk profiles of the 2 groups
were similar. This t'lifference was accompanied by a
significant, if transiont, increase in the postoperative
hematocrit in the former group (Table IV) and by a sig-
nificant reduction in the amount of blood products
transfused (Fig2, B).The reduction in the postoperative blood loss seen in
the patients receiving cryopreserved platelet transfu-
sions probably reflects botter in vivo hemostatic func-
tion of the cryopreserved platelets compared to the liq-
uid-preserved platelets. Nonsurgical blood loss after
CPB has been reco gnized as a good indicator of hemo-
static function in the comparative assessment of the refficacy of hemostatic drugs in patients undergoirf l
cardiac operations.22 Furtherrnore, although the post-
operative bleeding times wero not different in the 2
patient groups in this study, the level of thromboxane
B^ in the blood shed at the bleeding time determination

/f€0 Khuri et al The Journal of Thoracic andCardiovascular Surgery
January 1999
*- Cryopreserved --..- Liquid-preserved --+- Fresh
E A€ . == ( U( U E- = =g,E8 8 .d -
60
50
40
30
20tI
10
No Agonist Calcium ThrombinCollagenCalcium
Fig 4. In vitro procoagulant activities of fresh, liquid-preserved, and cryopreserved platelets. Liquid-pre-served platelets were stored in the blood bank for 3 to 4 days before assay. Procoagulant activity was deter-mined by flow cytometric analysis of the binding of the activated coagulation factor V-specific monoclon-al antibody V237 . Platelets were stimulated (10 minutes at 37"C) either with thrombin (2 U/mL), collagen(201tg/mL), and calcium chloride (3 mmol/L); with calcium chloride (3 mmol/L); or with buffer alone 1NoAgonist). Values were expressed as the percentage of maximal Y237 binding, as determined by the effect on-7 fresh platelets of the calcium ionophore A23I87 (40 pmol/L) and calcium chloride (3 mmol/L). Data areshown as mean + SEM. Asterisk indicates P < .05 for comparison between cryopreserved platelets and freshplatelets stimulated with the same agonist. Comparisons between liquid-preserved platelets and freshplatelets were not significantly different.
Thble Yl. Results of in vitro platelet function studies
Liquid-prese rved at 22"C
Fresh 24h 48h 72h Cryopreserved
Mean + SD n Mean + SD n Mean + SD n Mean t SD n Mean + SD n PtpH
Hypotonic stress response (7o)Platelet aggregation (DU)TXB, per plareler 1pg xlO6)
20 7.25 t0.107 79 + 18.4
20 2Ol+5720 191 x.220
20 7.33 + 0.128 7 8 + 7 . 1
20 189 + 7820 122t127
20 7.33 + 0.14 l88 7 6 t 1 3 . 1 6
l8 169 + 85 2020 115 +92 16
6.81 + 0.15 2428 + 13.3 23
140 + 31 25440+254 25
<.001 <.001<.001 <.001<.001 .083<.001 <.001
7.06 + 0.067O x.25.0
256 + 593 1 0 t 1 8 8
Liquid-preserved platelets were all apheresis units. ZXB,, Thromboxane B": DU, digitizer units.*By analysis of variance.
tDifference between 72-hour liquid-preserved and cryopreserved platelets, by / test.tI
preserved apheresed or liquid-preserved pooled plate-lets (Fig 3, A).
To ensure that the increase in blood loss observed inthe patients who received the liquid-preserved platelettransfusions was not due to the higher number of
z{atients undergoing valve replacement (with or without,' -rronary artery bypass grafting) in this group (12 vs 6
patients in the cryopreserved group), the analyses wererepeated after exclusion from the liquid-preservedgroup of the 6 patients who had the longest duration ofCPB. The average duration of CpB in the resultant 23
patients receiving liquid-preserved platelet transfusionswas 16l + 57 minutes. This was not significantly dif-ferent (P = .4) from the average CPB duration of 159 +69 minutes in the 23 patients receiving cryopreservedplatelet transfusions. The blood loss, however,remained significantly higher in the patients receivingthe liquid-preserved platelet transfusions (total medianblood loss in the latter 2329 mL, IQR 1715 mL, vs1830 mL, IQR 979 mL, in the patients receiving cry-opreserved platelet transfusions, P = .0089).
The volume of blood products used was lower in

The Journal of Thoracic andCardiovascular SurgeryVolume 117, Number 1
mination were not significantly different between thegroups. After platelet transfusion, the concentration ofthromboxane B2 in the blood shed at the site of thebleeding time determination was indeterminately high-er in the patients receiving the cryopreserved platelets(P = .068), and this also might have reached statisticalsignificance with a larger patient cohort (Table IV).
After platelet transfusion, plasma fibrinogen levelwas significantly higher in the patients receiving thecryopreserved platelets than in the patients receivingthe liquid-preserved platelets (Table IV). Serum albu-min, plasma factors V and VIII, and plasma fibronectinand D-dimer were not significantly different in the 2patient groups (Table IV).
Table V demonstrates that no differences were notedin the hematocrit, platelet count, mean platelet volume,platelet increment, platelet survival, and bleeding timeaccording to whether pooled or apheresed plateletswere transfused.
Blood loss and transfusion requirements. Theintraoperative blood loss recorded after the administra-tion of protamine accounted for 30Vo and 29Vo of the
Khuri et al t{
'' Pooled (n=10)r Apheresis (n=15)
Q r M Q 3OR
SICU
Total
2000Blood
3000Loss (ml)
Platelets
Hed cells
Fresh FrozenPlasma
Shed MediaslinalBlood
P=0'019
0 1000 2000 3000 4000 5000Volume Transfused (ml)
Fig 3. A, Blood loss measured in the operating room (OR), blood loss measured in the surgical intensive care unit(SrcU), and combined total blood loss in patients who received liquid-preserved pooled platelet transfusions andin those who received liquid-preserved apheresed platelet transfusions. Data are shown as median and IQR. M,Median; QI, 25th percentile; Q3, l5th percentile. B, Volumes of transfused blood products received by the samegroups. Data are shown as mean + SEM.
BAr
total blood loss in the patient groups receiving liquid-preserved and cryopreserved platelet transfusions,respectively (Fig 2). Blood loss after heparin reversalwith protamine was lower in patients transfused withcryopreserved platelets than in patients transfused withliquid-preserved platelets (Fig2, A). The median totalblood loss in the patients receiving the cryopreservedplatelet transfusions was ll2l mL, with an interquar-tile range (IQR) of 1l18 mL. In the patients receivingthe liquid-preserved platelet transfusions, the mediantotal blood loss was 2298 mL and the IQR was 1639mL (P = .007).Because the total surgical intensive careunit blood loss could be contaminated by serous, non-sanguineous drainage from the chest, an analysis wasperformed in which the blood loss during only the first8 hours after protamine administration was analyzed(not shown in Fig 2, A). There again was significantlyless total blood loss in the patients receiving-..y:pt.Aserved platelets (median 1093 mL, IQR 566 mL, \ \
1443 mL,IQR 1251 mL, in the patients receiving liq-uid preserved platelets, P = .05). Blood loss did not dif-fer according to whether the patient received liquid-

*18 Khuri et al
A
The Journal of Thoracic andCardiovascular Surgery
January 1999
EnP=o'144
n Liquid-preserved (n=29)tr Cryopreserved (n=24)
Q , MOR
SICU
Total
1500 2000Blood Loss (ml)
2500
Platelets
Red cells
Fresh FrozenPlasma
Shed MediastinalBlood
Total
B 0 1000 2000 3000 4000Volume Transfused (ml)
Fig 2. A, Blood loss measured in the operating room (OR), blood loss measured in the surgical intensive care unit(SICU), and combined total blood loss in patients who received liquid-preserved platelet transfusions and in thosewho received cryopreserved platelet transfusions. Data are shown as median and IQR. M, Median; el, 25th per-centile; Q3, 15th percentile. B, Volumes of transfused blood products received by the same groups. Data areshown as mean + SEM.
Thble Y. In vivo effects of transfused liquid-preserved platelets
A
Aft e r plat e I e t t ransfu s ion
Before CPB 30 min 2 h 4 h 2 4 h
Mean + SD n P* Mean + SD n Mean + SD n Mean + SD n Mean + SD n PtHematocrit (7o)
Pooled
Apheresis
Platelet count ( 106 cells/ml)
Pooled
Apheresis
Mean platelet volume (pm3)
Pooled
Apheresis
Platelet increment (108 cells)
Pooled
Apheresis
,Aatelet survival (7o)I Pooled
Apheresis
33.7 + 4.2 l033.3 t 5.3 14
191 + 66 10l9'7 + 13 13
9 . 2 + l . l 79 . 6 + l . l l l
27 .1 x .3 .3 928.8 x.3.1 14
196+62 9150 + 6 l 14
8.7 + 0.8 89 . 2 + 1 . 3 l l
3.8 + 2.3 82 .2 + 1 .8 14
34.2 x.16.3 744.5 x.21.3 12
29.6 x.4.9 630.1 + 1.4 4
180 + 62 l0142+ 6 l 15
9 .3 + 1 .0 89.5 + 1.2 l0
3 .3 x .2 .7 l 01 . 9 + 1 . 9 1 5
38.7 x.34.2 l040.5 t 36.8 14
26.2 + 3.3 6293 x.2.6 4
180 + 67 10136 + 49 15
9.3 + 0.9 89 .1 + 1 .8 l 0
3 .4 t2 .7 91 .6 + 1 .4 15
39.2 + 35.5 933.1x.29.0 14
29.6 + 2.5 528.6 + 2.1 4
161 +37 91 2 7 + 5 3 l l
9.2 x.0.9 89.4 + 1.0 6
2 .2 + 1 .8 81 . 1 + 1 . 6 1 2
33.1 x.30.6 83 3 . 0 t 3 0 . 1 l l
>,2
>,2
>.2
>.2
>,2
>.2
>.2
>.2
*Significance of / test between the 2 groups at baseline.fSignificance by analysis of variance between the 2 groups at multiple time points (30 minutes and2,4, and 24 hours).

The Journal of Thoracic andCardiovascular SurgeryVolume 117. Number 1
Table lY. In vivo effects of transfused platelets
Khuri et al tZ\
Aft e r p lat e le t tran sfu s ion
Before CPB 30 min 2 4 h
Mean + SD n P* Mean + SD n Mean x. SD n Mean x. SD n Mean x. SD n Pt
4 h2 h
Hematocrit (7o)
Liquid-preservedCryopreserved
Platelet count (106 cells/ml)Liquid-preservedCryopreserved
Mean platelet volume (pml)
Liquid-preservedCryopreserved
Platelet increment (108 cells)Liquid-preservedCryopreserved
Platelet survival (7o)
Liquid-preserved
CryopreservedBleeding time (min)
Liquid-preservedCryopreserved
Skin temp at bleeding time site (oC)
Liquid-preservedCryopreserved
Shed blood TXB, (pgl0.1 mL)Liquid-preserved
CryopreservedPlasma fibrinogen (mg/dl)
Liquid-preservedCryopreserved
Serum albumin (/dL)
Liquid-preservedCryopreserved
FactorV in plasma (7o)
Liquid-preservedCryopreserved
Factor VIII in plasma (7o)
Liquid-preservedCryopreserved
Plasma fibronectin (pddl)
Liquid-preservedCryopreserved
Plasma D-dimer (pg/dl)
Liquid-preserved
Cryopreserved
33.7 t 5.034.8 t 4.8
199 + 77179 + 53
9.5 + 1.49.2 + 0.9
27.5 x.3.9 2231.7 x.6.3 2 l
162x .62 261 2 2 + 3 3 2 1
8 .9 + l . l 2 l8.9 + 1.2 17
2.5 x.2.2 240.8 + l . l 20
36.8 t 26.0 2l16.9 x.22.1 l9
10.8 t 4.1 2510.7 + 3.2 21
30.2 + 1.8 2830.3 + 2.1 22
319 x.237 I I654 + 859 13
l 9 l t 3 5 92 6 2 + 8 6 7
2.49 x.0.46 92.58 t 0.63 9
22.4 x.6.9 l025.7 + l5.l 6
54 +23 l064+26 l
2 3 4 + 8 8 8228+ 51 8
2602x.1449 ll33ll x.1942 9
28.3 + 3.9 13
31.7 + 5.2 24
150 t 56 29124 + 42 23
9.5 + 1.4 2 l9.1 + 0.9 19
2.2 r22 21
0.9 + 1.3 24
33.5 t 31.7 26
21.8 r28.7 23
10.0 + 4.4 289.5 + 3.7 23
30.6 x.1.7 2930.5 + 2.9 22
397 + 385 13612x .464 15
187 x.46 l1290 t 105 8
2.73 + 0.59 l03.26 x.0.77 l0
28.2 + 8.5 l030.7 + 10.0 8
6 3 + 2 5 l l93+46 8
204+92 10221 + 44 10
4565 x.4155 126928x.4961 l0
>.2
>,2
>.2
281 A
27ZJ
2 lt 9
29.5 + 4.0 13
34.2 + 5.5 24
152+ 61 29127 + 41 24
9 . 3 + l . l 2 l9 .0 + 1 .0 19
2.3 x.2.3 211.3 + 1.4 24
37.2 x.35.4 26
23.6 x.27.8 22
10.9 + 4.1 2810.3 t 4.1 22
30 .1 + 1 .8 2830.1 + 2.0 23
3 3 O + 2 3 4 1 2440x.245 15
192+ 44 l l291 + ll0 8
2.79 x.053 l03.09 t 0.61 10
2 2 . 9 + 4 . 0 l l26 .1+ l2 . l 8
59 x.24 12' 7 1 + 2 8 8
223 +85 l0236+ 51 10
3333 x.1203 124320x.2225 l0
.o2l29.2 + 3.4 1228.8 t 3.8 23
>.2138 t 52 24155 +2Oi 23
>.29.3 + 0.9 179 .2 + 1 .0 18
.02r+1 .8 + 1 .6 220 ; l + L 2 2 4
.071+30.6 t 29.8 2213.4 + 19.1 24
>.27.4 + 2.6 231;7 + 3.5 22
>.2
6.8 t 2.86.9 + 3.2
29 .4 x .1 .229.3 + 1.8
825 + 840996 t7 l9
333 x.99416 x.166
3.26 x.0.433.15 t 0.30
67.5 + 19.l72.6 + 21.4
l 1 5 + 3 6128 + 12
384 x.162342 + 14
616 x.282l 0 l l t 1 2 5 8
2lZJ
2723
l l
t 4
t 38
l l8
l 07
l l1
9l0
1 28
>.2
>,2
>.2
>.2
31.7 + 2.0 2330.7 t 1.8 20 a
.06"
. l J
641 +621 121080 t l l 47 l l
.024
3 2 1 x . 8 4 ' 7
421 x.126 9>.2
2.81x.0.66 93.14 x.0.54 9
16642.3 + 15.5 1069.0 x.32.2 7
1251 1 8 + 5 6 91 6 8 + 8 7 8
>.2196+57 9221 + 44 l0
>.2+3381 x.2116 81647 x.548 1
>,2
. 1 5
>.2
>.2
temp, Tempeftture.xSignificance of t test between the 2 groups at baseline.
tSignificance between the 2 groups by repeated measures parametric analysis of variance (30 minutes and2,4, and 24 hours).
fSignificance between the groups by nonparametric analysis of variance (Friedman test).
4 hours after transfusion was significantly higher in thepatients receiving the cryopreserved platelets. Theplatelet count and the mean platelet volume were notsignificantly different between the 2 patient groups, butthe platelet increment after transfusion was significantlylower in the patients receiving the cryopreservedplatelet transfusions than in those receiving the liquid-
preserved platelet transfusions. The decrease in platelet
;::l:ffi": "*;il,n',":Tfi i"I Tl ;: :li:i::T"'ffi\platelet group (P - .071). This latter decrease mighthave achieved statistical significance with a largerpatient cohort. The postoperative bleeding times andskin temperature at the site of the bleeding time deter-

)&6 Khuri et al The Journal of Thoracic andCardiovascular Surgery
January 1999
Table Il. Comparison of characteristics of liquid-preserved pooled verst4s apheresed platelet transfusions
Pooled units Apheresis units
Age (d)
MeanMedianRange
Volume of platelets transfused per patient (mL)No. of platelets fansfused per patient ( l0r I cells)
3.27 + 0.873.02-5
669 t2929.17 + 4.3
3.43 + l . l74.02-5
346 + 1665.19 x .2 .3
>.2
.005
.01Data are expressed as mean + SD.
Table lll. Comparison of characteristics of tiquid-preserved versus cryopreserved platelet transfusions
Liqui.d-preserved Cryopreserved
Age (d)
MeanMedianRange
Volume of platelets transfused/patient (mL)No. of platelets transfused per patient (l0ll cells)
3 .4 + l . l3.82-5
487 + 2786.9 + 3.9
289 + 193250
30-720184 + 964.5 + 2.1
.0001
.0001
.008Data are expressed as mean + SD.
;A.6iu. operations during the study period was 3.8Vo..nal data analysis was therefore performed on 53
patients, 24 of whom received cryopreserved plateletsand 29 of whom received liquid-preserved platelets. Inthe group of 29 receiving the liquid-preserved platelets,10 patients received 7 to l0 random donor platelet con-centrates (pooled), l5 patients received apheresisplatelets, and 4 patients received both random donorplatelet concentrates and apheresis platelets.
Patient characteristics and outcomes. The preoper-ative patient characteristics are shown in Table I. Allpatients were men undergoing complex cardiac opera-tions with prolonged crossclamp and CpB times. Noneof the patients had received aspirin or antiplatelet agentswithin I week before the operation. Patient characteris-tics and hematocrit, platelet count, bleeding time, pro-thrombin time, and partial thromboplastin time did notdiffer significantly between the 2 groups before CpB(Thble I). Within the liquid-preserved patient groupthere were no signihcant differences in these parametersbetween those who received apheresed platelet transfu-sions and those who received pooled platelet transfu-sions. Four patients, 2 in each group, received an intra-aortic balloon pump before operation. An additional 6patients had an intra-aortic balloon pump placed either
An"q.rhe operation (2 in each group) or after the oper-
7 iofl (l ln each group).In both groups no clinical reactions were observed
after the infusion of the platelets or other blood prod-ucts. The incidences of thromboembolic complicationsand infections (wound infection, pneumonia) did not
differ statistically between the 2 groups. The duration oftracheal intubation was significantly (p = .04) longer inthe patients who received the liquid-preserved plateletsthan in the patients who received the cryopreservedplatelet transfusions (31 .7 + 25.4 and23.2 + 15.6 hours.respectively).
Characteristics and hematologic effects of trans-fused platelets. The characteristics of the platelet trans-fusions in the liquid-preserved group are shown in ThbleII. The liquid-preserved apheresed platelets were trans-fused in smaller numbers and in lesser volumes. Thecharacteristics of the transfused platelets used in the 2patient groups are shown in Table III. The storage timebefore transfusion for cryopreserved platelets was 289 +193 days, compared with 3.4 + 1.1 days for liquid-pre-served platelets (P < .0001). More than 50Vo of the liq-uid-preserved platelet transfusions were stored for 4 to5 days before administration (Fig 1). The duration ofstorage was not different between the liquid-preservedpooled platelets and the liquid-preserved apheresedplatelets. The shortest period of cryopreservation was30 days and the longest was 2 years (Fig l). A signifi-cantly higher number of platelets was administered withthe liquid-preserved transfusions than with the cryopre-served transfusions (Thble III).
Table IV lists the values of the hematologic parame-ters measured in the 2 patient groups before CpB andat designated time points after the complete adminis-tration of the platelets. There were no differencesbefore CPB between the 2 groups in any of the vari-ables listed in Table IV. The hematocrit durine the first

The Journal of Thoracic andCardiovascular SurgeryVolume 117, Number 1
Table l. Patient characteristics
Khuri et aI th
Liquid-preserved
(n = 29)
Cryopreserved
(n = 24)
Age (v)
Preoperative hematocrit (7o)
Preoperative bleeding time (min)
Preoperative ejecti on fr action (Vo)'heoperative
prothrombin time (s)
Preoperative partial thromboplastin time (s)
Platelet count (103 cells/mm3)Operation performed (no. of patients)
Primary CABG*Reoperative CABGP.i-ary valve replacement, with or without CABGReoperative valve replacement, with or without CABGP.imary valve replacement, with or without other
CPB time (min)
Lowest temperature during CPB ("C)
62.9 x.8.033.6 + 5.06.8 + 2.852+ 13
l4. l t7.036.5 t 19.1199 + 77
Il 01 2
-l
J
177 =6431 .3 t 3 .9
63.4 + 8.134.8 + 4.16.9 t3.25 5 t 1 6
13.2 + 3.433.8 + 14.2179 + 53
A-l l6IL
155 + 69
30.5 + 3.8
>.2.20
>.2>.2>.2>.2
.19
. 1 2>.2
Data are expressed as mean t SD. CABG, Coronary artery bypass grafling.*Originally scheduled for coronary artery bypass grafting and valve replacement; during the operation a decision was made not to replace the valve.
Blood samples were withdrawn at the following timepoints: (1) immediately before heparin administration, (2) 5minutes after heparin administration, (3) 40 minutes after thestart of CPB, (4) after the administration of protamine andreturn of the ACT to prebypass levels (posrCPB), (5) 30 min-utes after platelet transfusion , (6) 2 hours after platelet trans-fusion, (7) 4 hours after platelet transfusion, and (8) 24 hoursafter platelet transfusion. A standard template bleeding timewas also performed at all the study times.2O Skin temperatureat the site of the determination of the bleeding time wasrecorded with every bleeding time measurement.2l A volumeof 0.6 mL blood shed from the template bleeding time sitewas aspirated and assayed for thromboxane B, the stablemetabolite of thromboxane Ar; this is referred to henceforthas shed blood thromboxane Br. The assay employed has beendescribed previously elsewhere.2 I
Some of the hematologic measurements were made only in
a portion of the total study population. These measurements
and the numbers of randomly assigned patients in the 2 sub-groups are as follows: shed blood thromboxane Br, 21 with
cryopreserved platelets and 19 with liquid-preserved platelets;
albumin,9 with cryopreserved platelets and 11 with liquid-pre-served platelets; fibrinogen, 10 with cryopreserved platelets
and 14 with liquid-preserved platelets; fibronectin, 8 with cry-opreserved platelets and 6 with liquid-preserved platelets; fac-tor V 7 with cryopreserved platelets and 11 with liquid-pre-
served platelets; factor VIII, 5 with cryopreserved platelets and10 with liquid-preserved platelets; and D-dimer, 11 with cry-
opreserved platelets and l5 with liquid-preserved platelets.Platelet function studies. Platelet aggregation in response
to arachidonic acid (AA) and adenosine diphosphate (ADP),
thromboxane B, levels, platelet recovery from hypotonicstress, plasma pH, and procoagulant activity were measuredin the various types of platelets administered in accordancewith the methods summarized in the Appendix.
Statistical analysis. Differences between the 2 groups in the
preoperative patient characteristics, the baseline hematologicparameters, and the postoperative clinical events were assessedby the Student / test for continuous variables and the 12 test for-
dichotomous variables. The effects of platelet transftsion Athe parameters assayed at 30 minutes, and at2,4, and24 houroafter transfusion were assessed by a 2-way repeated measuresanalysis of variance. In the case of platelet increment, platelet
survival, shed blood thromboxane B, and D-dimer, a nonpara-metric repeated measures analysis of variance with treatmentand time as factors (Friedman's method) was used. A P valuewas calculated for an overall difference through time betweenthe 2 patient groups. The Wilcoxon rank test was used to assessdifferences in blood loss between the groups.
Results
Seventy-three patients were entered into the study andrandomly assigned to receive either liquid-preserved orcryopreserved platelets. Twenty patients were excludedfrom the study after random assignment. The reasonsfor exclusion were as follows: 6 patients had minimaldiffuse oozing after protamine administration and weredeemed by the surgeon not to require platelet transfu-sions, 6 patients had a documented site of surgicalbleeding after the administration of protamine (3received cryopreserved platelets and 3 received liquid-preserved platelets), and 5 patients (77o) died within 24hours after the institution of CPB for reasons not relat-ed to the platelet transfusions (3 received no platelets, Ireceived cryopreserved platelets, and 1 received liquid--preserved platelets). Three patients (2 receiving .ryoJ-'reserved platelets and 1 receiving liquid-preserveoplatelets) had e-aminocaproic acid (Amicar) inadver-tently administered during the immediate postoperativeperiod. The mortality rate for all patients undergoing

{O Khuri et at
The Journal of Thoracic andCardiovascular Surgery
January 1999
LIQU ID-PRESERVED at 22" CI Pooled unitsE Apheresis units
CRYOPRESERVED at -80"C
60
50
E nU'5
3 3 0l':
F
r * n
10
0 1 2 3 4 5
Length of Storage (Days)
Fig 1' Number of platelet transfusions administered and length of storage (days) of liquid-preserved pooledplatelets at22"C' liquid-preserved apheresed platelets at22oC,and cryopreserved platelets at -g0"c.
AA dedicated research assistant measured the brood lossstarting from the time of the neutralization of heparin. Thisincluded all the blood aspirated from the surgical fieldthrough wall suction and through a cell saver apparatus(Haemonetics corp, Braintree, Mass). It also included theblood contained in the sponges and raparotomy pads used inthe operative field. These were accuratery weighed and theirblood content was calcurated by subtracting the standardizeddry weights from the actual wet weights. The differences inthe weight of the sponges and pads were converted into mil_liliters of blood ross in accordance with the formula describedby Van Slyke and associates.l3
chest tube drainage was measured as soon as the chesttubes were placed during the operation, and this measurementwas continued until the patient was transferred out of theoperating room. The blood loss measured to this point con_stituted the intraoperative component of the blood ross.subsequent chest drainage in the surgicar intensive care unitconstituted the postoperative component of the blood loss.
Platelet products. All donors met the requirements of theAmerican Association of Blood Banks for healthy donors.
Cryopreserved platelets. The platelet cryopreservationmethod has been previously described elsewhere,6 It is sum_marized in the Appendix. The total length of storage (mean289 + 193 days) at -g0"C of the frozen platelets is shown inFig l' The mean in vitro platelet recovery after thawing, wash-ing, and resuspension of the 6g units transfused to patlnts, as
-jgtermined by phase microscopy, was 70Vo + lg.4To.tr Liquid-preserved praterets. Two types of liquid-preservedplatelets were used in this study, pooled platelets and plateretsobtained by apheresis. The methods of prepararion tf theseplatelets are described in the Appendix. patients randomlyassigned to receive liquid-preserved platelets received either
type of platelet transfusion according to the availability in theblood bank.
Recovery of transfused platelets. The total number ofplatelets transfused was determined by multiplying the vor-ume of the product transfused times ttt" p.oau"t;s prateletcount per milliliter. The patient's blood volume was estimat_ed from the body surface area, and peripheral blood plateletcount was measured with the coulter model JT automatedcell-counting system (Coulter Electronics, Hialeah, Fla). Thetotal platelet increment after transfusion at each time intervalwas determined by the increase in the absolute peripheralblood platelet count compared with the pretransfusion valuetimes the total blood volume. The percenrage recovery of thetransfused platelets was determined by the total incrementdivided by the total number of platelets transfused.
Recovery (vo) = l(Total blood volume [posttransfusion plateletcount/ml - pretransfusion platelet count/mll) / (Totalnumber of platelets transfused)l x I00Vo
Hematologic assays. Arterial blood was drawn into tri_potassium ethylenediaminetetraacetic acid-containing tubesfor measurement of hematocrit, hemoglobin, platelet-count,white blood cell count, and mean platelet volume with anelectronic particle counter (coulter moder JT)ra; and intosodium citrate-{ontaining tubes for measurement of fibrino-gen, factor Y and factor vIII with an automated coasulationsystem (Organon Teknika Co.p, Durham, NC),15 o] fib.o_nectin by an immunoturbidometric assay,l6 of heparin by achromogenic assay,lT and of D_dimer by an enzyme_linkedimmunosorbent assay.ls Serum was obtained from a tubecontaining no anticoagulant for measurement of albuminmeasured using an automated chemistry analyzer. (Cobas;Roche Diagnostic Systems, Inc, Branchburg, Ni).le

The Journal of Thoracic andCardiovascular SurgeryVolume 117, Number 1
ing after CPB. The current method of liquid storage ofplatelets at room temperature limits the duration oftheir clinical use to 5 days and results in a progressivedecline in platelet survival during this period.aCryopreservation, which allows storage of the plateletsfor as Iong2 years, represents an alternative strategy formaintaining an adequate inventory of platelets. Cryo-preserved platelets have reduced recovery and survivalin vivo and impaired response to in vitro testing com-pared with liquid-preserved platelets.5-e However,platelet recovery and survival in vivo do not correlatewith the in vivo hemostatic function of transfusedplatelets.l0 Cryopreserved platelet transfusions havedemonstrated therapeutic effectiveness6'll but have notbeen reported on in the setting of CPB. No randomizedtrials in any clinical setting have addressed the in vivohemostatic effectiveness of cryopreserved platelettransfusions compared with that of liquid-preservedplatelet transfusions.
The CPB-induced hemostatic defect offers a uniqueopportunity for the assessment of the hemostatic effec-tiveness in vivo of specific interventions because itresults in postoperative blood loss, a quantifiable vari-able that relates directly to the magnitude of the CPB-induced hemostatic dysfunction.l This paradigm hasbeen effectively employed in numerous studies thathave demonstrated the hemostatic efficacy of pharma-cologic agents, such as aprotinin, by demonstratingtheir efficacy in reducing blood loss after CPB.12 Thisstudy was designed to assess the comparative effects onhemostasis and blood loss of liquid-preserved and cry-opreserved platelet transfusions obtained from healthyvolunteers and administered to patients after complexcardiac operations. The study also provides a compari-son between the in vivo hemostatic effect and the invitro function of both liquid-preserved and cryopre-served platelet transfusions.
Methods
Study protocol. After institutional review board approvalwas obtained, this investigation was performed on73 patientsundergoing cardiac operations at the West Roxbury VeteransAdministration Medical Center. Informed consent wasobtained from patients scheduled to undergo I of a predefinedlist of complex cardiac surgical procedures. Inclusion criteriawere as follows:
1. Patient was scheduled for reoperative valve replace-ment, reoperative coronary artery bypass grafting, or both.
2. Patient was scheduled for primary valve replacementcombined with coronary artery bypass grafting.
3. Valve replacement was scheduled for a patient with aplatelet count of <150,000/1tL.
Khuri et al
4. An operation with CPB was to be performed on apatient with a preoperative intra-aortic balloon pump and aplatelet count < 100,000/pL.
These operations were chosen because they were anticipat-ed to require a prolonged period of CPB and also because areview of the institution's previous experience had revealed ahigh likelihood of their resulting in platelet transfusions. Theoperations were performed by 2 surgeons (S.F.K. and V.B.)employing a similar technique for CPB under moderate sys-temic hypothermia. A centrifugal pump and a membrane oxy-genator were used in the circuit. No prophylactic antifibri-nolytic therapy (eg, aprotinin, t-aminocaproic acid) wasadministered. Systemic anticoagulation was achieved with aninitial heparin dose of 3 mg/kg body weight and maintainedwith the activated clotting time (ACT) during CPB longerthan 480 seconds. After weaning from CPB and decannula-tion, heparin was neutralized with protamine sulfate given ina ratio of 0.5 mg of protamine to 1.0 mg of the initial heparindose and 1.0 mg of protamine to 1.0 mg of heparin for anysubsequent doses. Reversal of the heparin effect was deter-mined by the return of the ACT to baseline level. At this timemeasurement of the blood loss was started, and the platelettransfusion previously determined by the randomizationprocess was given unless the masnitude of the diffuse ooziffrom the tissues was determined by the surgeon to be mi^'
'l
mal. Throughout both the intraoperative and postoperativ-ecourses, the surgeon, the anesthesiologist, and all individualsinvolved with ordering blood products during the patient'spostoperative course were kept blinded to the type of plateletsrandomly selected for transfusion. The need for transfusionof red blood cells, fresh-frozen plasma, or further plateletswas determined by the house staff after consultation with theattending surgeon, in accordance with set protocols thatinvolved the observed blood loss and the patient's hemoglo-bin, hematocrit, and prothrombin time. A record was kept ofall blood products received after CPB including unwashedshed mediastinal blood that was collected in the chest tubePleur-evac collecting system (Deknatel, Inc, Fall River,Mass) and routinely reinfused in all patients.
Measurement of postoperative blood /oss. Measurement ofblood loss was started in the operating room when the ACTreturned to baseline after the administration of protamine. Inthe absence of specific localized surgical bleeding, the gener-alized blood loss after the neutralization of heparin wasassumed to be reflective of the patient's hemostatic state andwas termed nonsurgical blood /oss. To ensure that the bloodmeasured represented nonsurgical blood loss, patients inwhom specific surgical bleeding was encountered after theneutralization of heparin were prospectively excluded fromthe analysis. In addition, fluid irrigation was avoided duringthe closure of the chest so as not to interfere with the weightof the sponges. If inigation was necessary, the fluid, used yq\aspirated separately and sponges were not used during t[ .irrigation. In the postoperative period, patients who had toundergo reexploration for control of bleeding were alsoexcluded from the analvsis.
th\