“stabilizing mandibular complete dentures using the
TRANSCRIPT

TECHNIQUE
“STABILIZING MANDIBULAR COMPLETE DENTURESUSING THE NEUTRAL ZONE IMPRESSION TECHNIQUE”
INTRODUCTION
he major goals of providing complete dentureprosthesis to an edentulous patient include the
provision of functionally aesthetic substitutes and thereplacement of associated structures within the oral cavity.Additionally, the complete dentures should serve to redefinethe true spaces and the potentially available spaces withinthe mouth. When these are achieved, the complete dentureprosthesis occupies substantial volume in the oral cavity1.
General dental practitioners and prosthodontists alikeusually encounter problems when making complete denturesfor patients with atropic residual ridges2. This problem is
commonly encountered in mandible3 and it is difficult toachieve retention and stability in mandibular dentures ascompared to the maxillary ones. Unstability in mandibularcomplete dentures may be present due to a number ofreasons. The common ones, as described by Jagger &Harrison4 are:
a) Inappropriate extensions of buccal and lingual flangesof a denture;
b) Poorly adapting denture fitting surface;c) Severely atropic mandibular alveolar ridge;d) Poorly contoured polished surfaces of a denture;e) Abnormal denture teeth positions, inappropriate
orientation and high level of the occlusal plane and presence of occlusal errors.
The neutral zone, also known as zone of minimalconflict, exists between the buccal and lingual musculaturewithin which the polished surfaces of a denture should beideally placed5,6. It is defined as that region in the mouthwhere forces produced by the tongue directed outward arebalanced by inward forces originating from the cheeksand lips during normal neuromuscular function7. Throughoutoral function, various muscles and structures are involved.
JPDA Vol. 22 No. 02 Apr-June 2013 154
Fabrication of complete dentures using the neutral zone technique is neither recent nor original. During the pastfew decades, many articles which have incorporated or related to what we have named the ‘‘neutral zone technique’’have been published. The aim of this case report is to describe the technique to fabricate a mandibular completedenture in muscular balance, as muscular control will be the major stabilizing and retentive factor during function.The neutral zone technique is fairly easy to perform but requires an extra visit and relatively high laboratory costs.This article elaborates on a case of a 62 years old male patient with mandibular atrophic ridge treated by utilizingthe neutral zone technique.KEY WORDS: (a). Atropic residual ridges, b) Mandibular complete denture, c) Stability, d) Tissue conditionerHow to cite this article: Rashid H, Vohra FA, Haidry TZ, Karmani GD. Stabilizing mandibular complete denturesusing the neutral zone impression technique. J Pak Dent Assoc 2013;22(2):154-159.
T
Haroon Rashid1
Fahim Ahmed Vohra2
Tasneem Zoeb Haidry3
Geeta Devi Karmani4
1. Assistant Professor, Department of Prosthodontics,Ziauddin College of Dentistry, Karachi, Pakistan.
2. Assistant Professor, (SDS) Prosthetic Dental Science, King Saud University, College of Dentistry, Saudi Arabia.
3. Final Year Dental Student, Ziauddin College of Dentistry, Karachi, Pakistan.
4. Final Year Dental Student, Ziauddin College of Dentistry, Karachi, Pakistan.
Correspondence: Dr Haroon Rashid<[email protected]> Mobile : +92-323-3241889
BDS, MDScBDS, M.Clin.Dent, M.Pros, MFDS, RCPS.
The main displacing forces which add to the instability ofmandibular denture are generated by the tongue, the lowerlip and the modiolus8. Positioning teeth in the neutral zoneensures that the artificial teeth will not interfering with thenormal muscular function of the oral cavity and that thoseforces which are generated by the oral musculature aremore favourable for the stability of the denture. Thus, adenture fabricated using the neutral zone technique willhave better retention, stability and aesthetics due to goodfacial support. This technique is very effective for patientswho have had several unstable mandibular dentures overatropic residual ridges previously.
Common techniques for recording neutral zoneimpression involve the use of a modelling compound ora tissue conditioner9. The purpose of this clinical report isto describe the technique of recording the neutral zoneimpression for mandibular complete dentures using a tissueconditioner.
CASE REPORT:
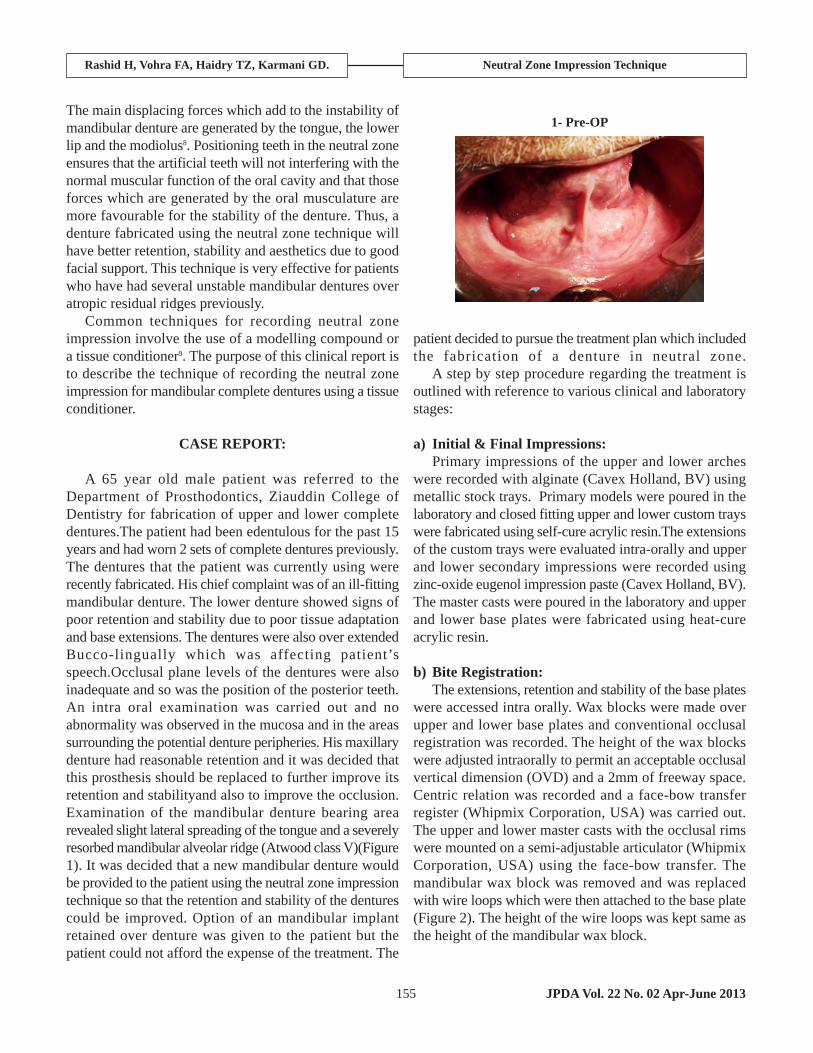
A 65 year old male patient was referred to theDepartment of Prosthodontics, Ziauddin College ofDentistry for fabrication of upper and lower completedentures.The patient had been edentulous for the past 15years and had worn 2 sets of complete dentures previously.The dentures that the patient was currently using wererecently fabricated. His chief complaint was of an ill-fittingmandibular denture. The lower denture showed signs ofpoor retention and stability due to poor tissue adaptationand base extensions. The dentures were also over extendedBucco-lingually which was affecting patient’sspeech.Occlusal plane levels of the dentures were alsoinadequate and so was the position of the posterior teeth.An intra oral examination was carried out and noabnormality was observed in the mucosa and in the areassurrounding the potential denture peripheries. His maxillarydenture had reasonable retention and it was decided thatthis prosthesis should be replaced to further improve itsretention and stabilityand also to improve the occlusion.Examination of the mandibular denture bearing arearevealed slight lateral spreading of the tongue and a severelyresorbed mandibular alveolar ridge (Atwood class V)(Figure1). It was decided that a new mandibular denture wouldbe provided to the patient using the neutral zone impressiontechnique so that the retention and stability of the denturescould be improved. Option of an mandibular implantretained over denture was given to the patient but thepatient could not afford the expense of the treatment. The
patient decided to pursue the treatment plan which includedthe fabrication of a denture in neutral zone.
A step by step procedure regarding the treatment isoutlined with reference to various clinical and laboratorystages:
a) Initial & Final Impressions:Primary impressions of the upper and lower arches
were recorded with alginate (Cavex Holland, BV) usingmetallic stock trays. Primary models were poured in thelaboratory and closed fitting upper and lower custom trayswere fabricated using self-cure acrylic resin.The extensionsof the custom trays were evaluated intra-orally and upperand lower secondary impressions were recorded usingzinc-oxide eugenol impression paste (Cavex Holland, BV).The master casts were poured in the laboratory and upperand lower base plates were fabricated using heat-cureacrylic resin.
b) Bite Registration:The extensions, retention and stability of the base plates
were accessed intra orally. Wax blocks were made overupper and lower base plates and conventional occlusalregistration was recorded. The height of the wax blockswere adjusted intraorally to permit an acceptable occlusalvertical dimension (OVD) and a 2mm of freeway space.Centric relation was recorded and a face-bow transferregister (Whipmix Corporation, USA) was carried out.The upper and lower master casts with the occlusal rimswere mounted on a semi-adjustable articulator (WhipmixCorporation, USA) using the face-bow transfer. Themandibular wax block was removed and was replacedwith wire loops which were then attached to the base plate(Figure 2). The height of the wire loops was kept same asthe height of the mandibular wax block.
JPDA Vol. 22 No. 02 Apr-June 2013155
Rashid H, Vohra FA, Haidry TZ, Karmani GD. Neutral Zone Impression Technique
1- Pre-OP

c) Recording of the Neutral Zone Impression:Bucco-lingual position of the wire loops was checked
intra-orally and the free-way space was assessed again.Tissue conditioner material (GC Tissue Conditioner, GCAmerica Inc, IL, USA) was applied over the wire loopsand was placed in the patient’s mouth. The patient wasthen told to perform various oral movements of his lips,tongue and the cheek.These movements included sucking,swallowing, pursing lips, pronouncing E and O soundsand protruding the tongue to simulate physiologicalmovements. While the patient was performing thesemovements, the occlusal rims were kept in occlusal contactwhere possible. The shaping / moulding of the tissueconditioner material facilitated the recording of the neutralzone when patient performed various oral movements.During function of the lips, cheeks, and the tongue, theforces exerted on the tissue conditioner molded it into the
shape of the neutral zone.(Figure 3). These movements(as explained earlier)were performed for a period of 20minutes after which the base-plate was removed alongwith the finished neutral zone impression which was sent
to the laboratory following disinfection.Maxillary teeth were set-up in the laboratory and silicone
putty (Alphasil, Müller Omicron, GmbH, Germany) indicesof mandibular base-plate and the tissue conditioner materialwas made (Figure 4, Figure 5). The wire-loops along withthe tissue conditioner material were removed and werereplaced with modelling wax using the putty indices andmandibular teeth set-up was carried out. These were thenreturned chair-side so that trial could be carried outconventionally.
d) Trial:Trial of the maxillary and mandibular was performed.
Occlusion was checked and retention and stability of theboth maxillary and mandibular dentures were assessedand found satisfactory both for the upper and the lowerarches. The trial dentures were then returned to thelaboratory for processing and finishing as usual(Figure 6,
JPDA Vol. 22 No. 02 Apr-June 2013 156
2- Tray with wire loops
3- Completed impression
4- Putty index lingual
5- Putty index complete
Rashid H, Vohra FA, Haidry TZ, Karmani GD. Neutral Zone Impression Technique

Figure 7).
e) Insertion and Follow-up:
The dentures were fitted into the patient’s mouth (Figure8, Figure 9) and the patient was reviewed on a couple ofoccasions. The patient was pleased and reported satisfactionwith his existing prosthesis.
DISCUSSION:
When mandibular ridge is severely resorbed, gainingretention and stability in a denture becomes a challenge.Positioning of the artificial teeth and connection of thepolished surfaces with the surrounding tissues are twomajor factors that determine success in complete denturetherapy. When artificial teeth are arranged within theneutral zone, the prosthetic teeth do not interfere with thenormal oral function. This technique typically helps tolocate posterior denture teeth in a slight facial positionrather than their arrangement over the crest of alveolarridge10.
Provision of a mandibular complete denture is oftendifficult than a maxillary complete denture and it becomeseven more difficult when powerful activity of oralmusculature exists. Dental implants are a good alternativetreatment option in such scenarios however; they may becontraindicated in patients due to a variety of reasons.There are economic, clinical, and medical contraindicationswhen providing dental implants to a patient. Provision ofa denture using neutral zone technique may help inovercoming these difficulties. Firstly, it will be ensuredthat the oral musculature aids in the retention andstabilization of the denture rather than dislodging thedenture during function. The dentures made using the NZtechnique will have other advantages such as reduced foodentrapment, good esthetics due to facial support and properpositioning of the posterior teeth which will allow forsufficient tongue space. Since the current dentures provided
157 JPDA Vol. 22 No. 02 Apr-June 2013
6- Articulation - Front View
7- Articulation - Side View
8- Post-OP-Buccal
9- Post-OP
Rashid H, Vohra FA, Haidry TZ, Karmani GD. Neutral Zone Impression Technique

JPDA Vol. 22 No. 02 Apr-June 2013 158
to the patient were constructed in harmony with theirsurroundings,remarkable improvement in facial appearance,stability and retention during function was noticed ascompared to the patient’s previous dentures.
Fish5 introduced the principal of the neutral zone inprosthetic dentistryand directed the profession’s attentionto the importance of designing the dentures in muscularbalance.He recommended that the dentures should bedesigned in such a way that they are concave from thebuccal side to accommodate the check muscle.Theadvantage of recording the neutral zone impression tostabilize mandibular complete dentures isoutlined in variousclinical studies2,3,8,9,11,12,13,14. These studies suggested that thistechnique helps in functional contouring of all the externalsurfaces of a finished denture and thus improved retentionand stability in a denture can be achieved. Fahmy andKharat11 conducted a study that included two groups ofpatients, one with conventionally fabricated dentures andthe other with dentures that were constructed with theneutral zone technique. Mastication, comfort and speechwere compared in both the groups. Most of the patientswere satisfied with the dentures made using the neutralzone technique. Ohkubo et.al.,12 suggested that a suitabledenture can be made if arrangement of teeth using neutralzone approach is carried out. They mentioned that thistechnique is not only helpful in edentulous patients butalso for patients with oral deformities. Gupta & Agarawal13
stated that the neutral zone concept implies acquired musclecontrol especially by tongue, lips and cheeks towardsstability of a mandibular complete denture and by applyingthe neutral zone concept, the dislodging muscle force canbecome a retentive and a stabilization force. Rehmann et.al.,14 have used an alternative technique for recording ofneutral zone impression in which acrylic resin base platewith posterior occlusal rims were used. The base plateswere worn by patients for a period of two days and theimpressions were recorded. Majority of the patients reportedimproved denture stability and satisfaction with theirdentures. However their technique cannot be used in routineclinical conditions.Watt et. al.,15 described an entirelydifferent approach of tooth placement for dentures. Theystudied the pattern of post-extraction resorption in 100edentulous subjects and found that the vestige of the lingualgingival margin could be identified on the casts and canbe utilized as a reliable guide to the placement of theartificial teeth.
Neill & Glaysher16 conducted a study in which theyevaluated different placement criteria of denture teeth.They used miniature foil strain guages which were installed
with the dentures surfaces which were connected to therecording equipment extra-orally through wires. Movementsof the jaws were monitored by kinesiograph. The pressuremeasurements and alterations in position of the jaws wererecorded on a six channel Grass recorder. The stated thatFish’s concepts of teeth positioning results in dentureinstability and that the technique of piezography is helpfulin determining the teeth position which may require furtherinvestigation. They also stated that biometric guides totooth placement are valuable in determining the lowertooth placement.
The technique for recording neutral zone in the currentcase report is simple. Tissue conditioner material waspreferred to obtain the impression on the wire loops becauseit has various advantages. It is a mucostatic material andthus does not apply pressure over the soft tissues. It istasteless and has no odor. The material also has long settingtime and all the functional movements of the oralmusculature can be recorded during the muscular activities.Another reason why tissue conditioner was used is becauseit is easily available for most of the clinicians. Thedisadvantages of the neutral zone technique, in view ofauthors are high cost of the material, increased laboratorycosts and the requirement of an extra visit to record theneutral zone impression.
CONCLUSION:
The neutral zone technique for denture fabricationhasan advantage that it stabilizes the denture with thesurroundingsoft tissues, instead of being dislodged bythem. Retentionand stability of dentures are greatlyimproved, especially inthe severely atrophic ridges. Whenpatients cannot undergoan implant overdenture therapydue to medical and dental contraindications, the neutralzone technique providesan alternative, time-saving, andrelatively simpleway to obtain a favorable result. Adisadvantage of thistechnique involves the laboratoryaspect. Increased laboratorytime and cost are necessary,and the laboratorytechnician must be trained to supportthis clinicalprocedure.Considering the benefits of thistechnique, it is recommended that clinicians shouldincorporate it in their routine prosthodontic managementof edentulous patients.
REFERENCES:
1. Cagna DR, Massad JJ, Schiesser FJ. The neutral zonerevisited: From historical concepts to modern
Rashid H, Vohra FA, Haidry TZ, Karmani GD. Neutral Zone Impression Technique

JPDA Vol. 22 No. 02 Apr-June 2013159
application. J Prosthet. Dent. 2009; 101: 405-412.2. Pinar K, Nilgun A, Calikkocaoglu S. Using Tissue
Conditioner Material IN NEUTRAL ZONE TECHNIQUE. NY State Dent J. 2007; 73: 40-42.
3. Lynch CD, Allen PF. Overcoming the mandibular unstable denture: The neutral zone impression technique.Dent Update. 2006; 33: 21-26.
4. Jagger D, Harrison A. Complete Dentures- problem solving. London; BDJ Books. 1999.
5. Fish EW. Principles of full denture prosthesis. 1st ed.London; Staples press.1933.
6. Basker RM, Davenport JC. Prosthetic treatment of edentulous patient. 4th ed. Oxford; Blackwell Munksgaard, 2002.
7. Beresin V E, Schiesser F J. The neutral zone in completeand partial dentures C.V. Mosby Co., 1978. p 15.
8. Gahan MJ, Walmsley AD. The neutral zone impressionrevisited. Br. Dent. J 2005; 198: 269-272.
9. Makzoume´ JE. Morphologic comparison of two neutralzone impression techniques: A pilot study. J Prosthet Dent 2004; 92: 563-568.
10.Boucher CO. Complete denture prosthodontics – Thestate of the art. J Prosthet Dent 1975;34:372-383.
11.Fahmy FM, Kharat DU. A study of the importance ofthe neutral zone in completedentures. J Prosthet Dent.1990;64:459-462.
12.Ohkubo C, Hanatani S, Hosoi T, Mizuno Y. Neutralzoneapproach for denture fabrication for a partial glossectomy patient: a clinical report.J Prosthet Dent.2000; 84:390-393.
13.Gupta KL, Agarwal S.Salvation of a severely resorbedmandibular ridge with a neutral zone technique.IndianJ Dent Res.2011; 22 :883.
14.Rehmann P, Zenginel M, Wostmann B. Alternative procedure to improve the stability of mandibular complete dentures: a modified neutral zone technique.IntJ Prosthodont.2012; 25: 506-508.
15.Watt DM, Durren CM, Adenubi JO. Biometric guidesto the design of complete maxillary denture. Dent MagOral Topics. 1873; 84: 109.
16.Neill DJ, Glaysher JK. Identifying the denture space.J Oral Rehabil. 1982 ;9:259-277.
Rashid H, Vohra FA, Haidry TZ, Karmani GD. Neutral Zone Impression Technique