st3 introduction programme directors: dr christine marshall dr richard de ferrars dr andrew cochrane...
TRANSCRIPT
ST3 Introduction
Programme Directors:Dr Christine MarshallDr Richard de FerrarsDr Andrew Cochrane
Introduces self
Clarifies roles

Name the Musical and Song…
Greets patient
Demonstrates interest & respect

Daft Diversion...
Greets patient
Demonstrates interest & respect
Watch the
bottom right...
Meaning and
relevance to
follow

What Would YOU Like To Know About?
We have several
areas to run through
but what is on your
mind?
Opening question
Identifies the reason for the consultation
Agenda setting

ST3 Introduction
• Enhanced ST3• MRCGP Exam Overview• Year Planning• KSS Policies• Overview of the VTS• E-Portfolio & Learning Log• OOH Training• Local Training Agreement.
Provides structure to the consultation
Sequencing

ST3 Representative
• Dr Hannah Pedley expressed interest
• Deputy please?
• VTS Rep at KSS Trainee’s Committee– Vicky Goodall.
Encourages the patient to contribute

Enhanced ST3
• First real step towards ST4
• Additional 3 months as ST3
• Details TBC…
• Last year - AKT score over 70%
CSA early (Dec/ Jan)
• Develop further skills– CCG work– Stage 1 Educators Pathway.
Sequencing
Timing
MRCGP Overview
Provides Rationale

AKT
Hurrah - Majority have negotiated this challenge If not: 2-3 attempts left? = please take it in October
final attempt? = take it May 2016
(focus on CSA first)
AKT Failed Twice?If you had problems with written exams at medical school,
consider a dyslexia assessment
Costs about £300
Gain additional time in exam (30 or 45min).
Sharing of thought

CSA – Lots of Choice!
Now held monthly from October to May
KSS and VTS set a pace aimed at Jan / Feb / Mar
- November: Cumberland Lodge
- December: KSS day at the RCGP exam centre
- January: Thursday pm sessions
Enhanced ST3 – need to work ahead of the pace.
Provides rationale
Examination

CSA – Lots of Choice!
Nov/ Dec - risk wasting £1700 (and one of your 4 attempts)- needed by some (maternity, enhanced ST3)- results come out mid December
Jan/ Mar - Makes sense for most- Allows Apr/ May re-sit without extension- But result is not out until early March…
May - Will need extension to re-sit
VTS teaching is aimed at January - March date
Take your trainer’s advice!.
Offers choice

WPBA AssessmentsPortfolio close will be end of May
– Get ES review 1 done by mid JanuaryHalf the assessments before review 1
– Get ES review 2 done by mid MayHalf the assessments before review 2
Full year = CBD x12
COT x12 (some kept on video please)
MSF x2 (Need 10 back: 5 clinical, 5 non-clinical)
PSQ x1 (Feb/ March/ April)
DOPS replaced by CEPS.Clarification

CEPS
Clinical Examination & Procedural Skills
•Now 13th DoC replacing skills log
•Evidence tagging includes COT, CSR, log, MSF
•CEPS form more flexible than DOPS
•Should still have a “form” for intimate exams

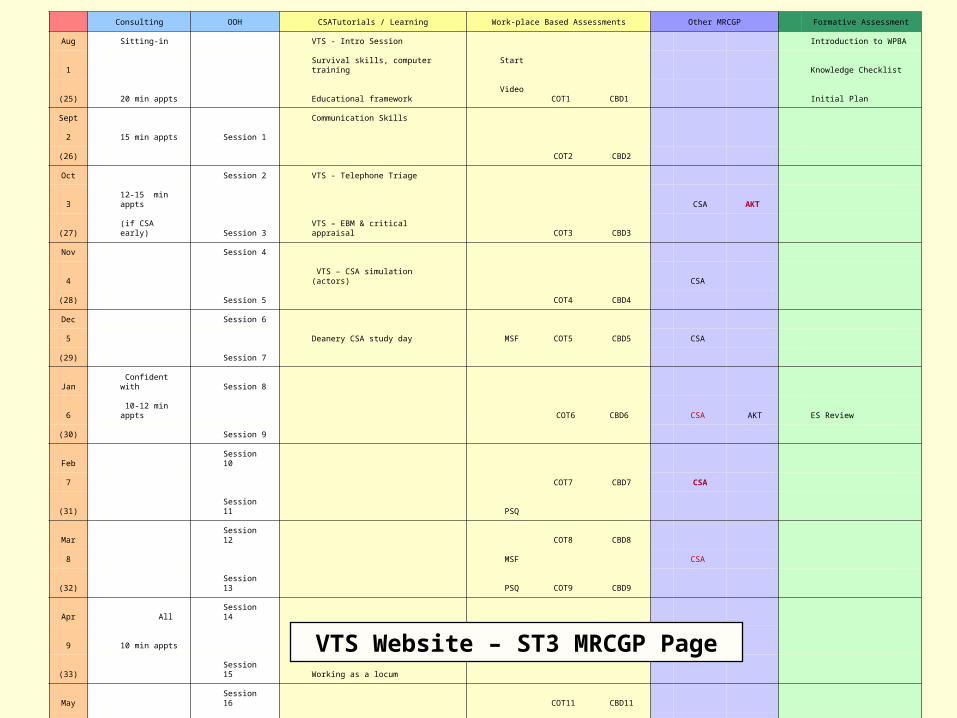
Planning the Year
The tube map - looks complex at first glance but is very useful…..
Uses visual methods of conveying information
Consulting OOH CSATutorials / Learning Work-place Based Assessments Other MRCGP Formative Assessment
Aug Sitting-in VTS - Intro Session Introduction to WPBA
1 Survival skills, computer training Start Knowledge Checklist
(25) 20 min appts Educational framework Video COT1 CBD1 Initial Plan
Sept Communication Skills
2 15 min appts Session 1
(26) COT2 CBD2
Oct Session 2 VTS - Telephone Triage
3 12-15 min appts CSA AKT
(27) (if CSA early) Session 3 VTS – EBM & critical appraisal COT3 CBD3
Nov Session 4
4 VTS – CSA simulation (actors) CSA
(28) Session 5 COT4 CBD4
Dec Session 6
5 Deanery CSA study day MSF COT5 CBD5 CSA
(29) Session 7
Jan Confident with Session 8
6 10-12 min appts COT6 CBD6 CSA AKT ES Review
(30) Session 9
Feb Session 10
7 COT7 CBD7 CSA
(31) Session 11 PSQ
Mar Session 12 COT8 CBD8
8 MSF CSA
(32) Session 13 PSQ COT9 CBD9
Apr All Session 14
9 10 min appts Finding a practice PSQ COT10 CBD10 CSA AKT
(33) Session 15 Working as a locum
May Session 16 COT11 CBD11
10 Practice finance & admin CSA ES Final Review
(34) Session 17 COT12 CBD12
Jun Session 18 NHS Appraisal
11
(35) Session …
Jul
12
VTS Website – ST3 MRCGP Page

MRCGP Summary
AKT - well done if passed in ST2
- others, please take in October
- delay any final attempt until May
CSA - Nov & Dec for some
- Jan Feb Mar for most
WPBA - use the planner and keep to speed.Chunks & checks
Uses repitition & summary
Offers choices

KSS Policies & Plans
• Chaperone policy
• Dress code
• Car allowance
Contracting

Chaperone Policy
Sensitivity
Assesses patient’s starting point
Encourages patient to contribute
Dress Code
Sensitivity
Assesses patient’s starting point
Encourages patient to contribute
“Conventionally in the UK, formal professional practice between doctors and patients is appropriately marked by a certain formality of dress. It is, therefore, legitimate to require trainees to dress in this fashion.”

KSS Policies & Plans
• Chaperone policy
• Dress code
• Car allowance– Mileage for home visits, travel to teaching– Up to 20 miles to & from home when NEED car…– NEED car if you do a visit or travel to teaching…– Must keep daily record to complete a claim
Contracting
VTS Overview
Much mystery surrounds the activities of the GP trainees on Thursday afternoons…..
Elicits patient’s health beliefs
VTS Overview
How can we all get the most out of the VTS?• Time-keeping• Participation• Cumberland Lodge
Cumberland Lodge dates:
November
March
June
PASS THESE DATES TO PMs
Ideas & concerns

The Learning Log/ PDP
Shares own thoughts
Picks up verbal & non-verbal cues

Categories of Log EntriesHow should Trainees use the learning log?
1) Simple list of useful information from teaching:CURB scoringCauses of amenorrhoea
2) Recording of a “required event”Audit project Child protection Statement of LeaveOOH session Leadership CPR/ AED
3) Genuine educational activityTutorials, VTS sessionsInteresting cases, followed by reading up
4) “Domains of competence” eventReflection from a competency, not a clinical, perspective
Organises explanation

Categories of Log EntriesHow should Trainees use the learning log?
1) Simple list of useful information from teaching:OK to record but don’t bother sharing(unless you want to see how sarcastic your ES can be)
2) Recording of a “required event”As and when appropriateDo count towards 2-per-week target
3) Genuine educational activityTutorials, VTS sessions, interesting cases & readingNo more than 1-per-week about a teaching session
4) “Domains of competence” eventReflection from a competency, not a clinical, perspectiveSuperb for ES Reviews – try and write 2-3 per month

Required/ Mandatory EventsLevel 3 Child Protection
VTS session, e-modules if on leave
ST3 GP AuditOne 8-stage audit cycle – see website
Leadership event See VTS website for optionsForm to complete is on KSS website
CPR/ AED certificateUsually done in term 3
Two Significant Events[Complaints], near misses, cancer diagnoses
All of these MUST be shared. Uses explicit categorisation

Audit & Leadership
• Move away from 8-point audit
• Move towards CCG project work (QIP)
• Mandatory move if doing enhanced ST3
Offers choices

E-Portfolio
Non-verbal behaviour

Practice Swaps
• We encourage ST3s to try another practice for 1 week
• W/C June 2nd 2016
• Avoid A/L that week please.
Offers choices

Out-of-Hours• You all hate it• Hard work for supervisors• Look at the VTS website
25% pay supplement
£50 supervision fee
72 hours is mandatory (may increase)
Good preparation for CSA so NO GAPS PLEASE
Log-entry at end of each shift
OOH sheet from supervisor IF NOT YOUR TRAINER
Ask your supervisor to work through the FPCS Induction Forms with you – on the VTS website
PROFESSIONALISMBooked shift = be there (unless you have died) Empathy & support

Out-of-HoursTraffic Light – PLEASE DISCUSS WITH YOUR ES
• Red = ST1/2 (observe only)• Amber = first few ST3 months.
Avoid phone triage until after training
Can see patients at base from the start
Supervisor can go on a visit with you
If left at base, must have phone or alternative• Green = last 5 shifts
You take a slot on the rota
Do everything including solo visits
Supervisor could be by phone.Empathy & support

Admin Required for OOH
• Medical Indemnity Insurance
• GMC Number
• BLS certificate
• Safeguarding Level 3 Certificate
• Information Governance Certificate
• DBS certificate
• Hep B status

OOH – Key Points
• New shift e-booking system to try out
• Must compete admin checklist
• Must complete clinical induction checklist with supervisor
• Must discuss RAG with trainer/ ES
• Must keep back FIVE green shifts for last 3 months of training

Local Trainers Agreement
Use of notes

Local Trainers Agreement
• The Working Week
• Annual Leave
• VTS & Educational Activities
• Study Leave
• Private Study (Flexible Education Session)
• Out-of-Hours Training
• Read through NOW. Any questions?
Checks patient’s understanding of information

Daft Diversion...
Greets patient
Demonstrates interest & respect
Any answers?

Daft Diversion...
Calgary-Cambridge consultation model
Doctor-patient relationship and patient-centred consulting
Does NOT mean doing what the patient wants
Facilitating them to reach agreement on what is best for them
Trainer-trainee relationship and adult learning
Does NOT mean doing what the trainee wants
Facilitating them to reach agreement on what is best for them.

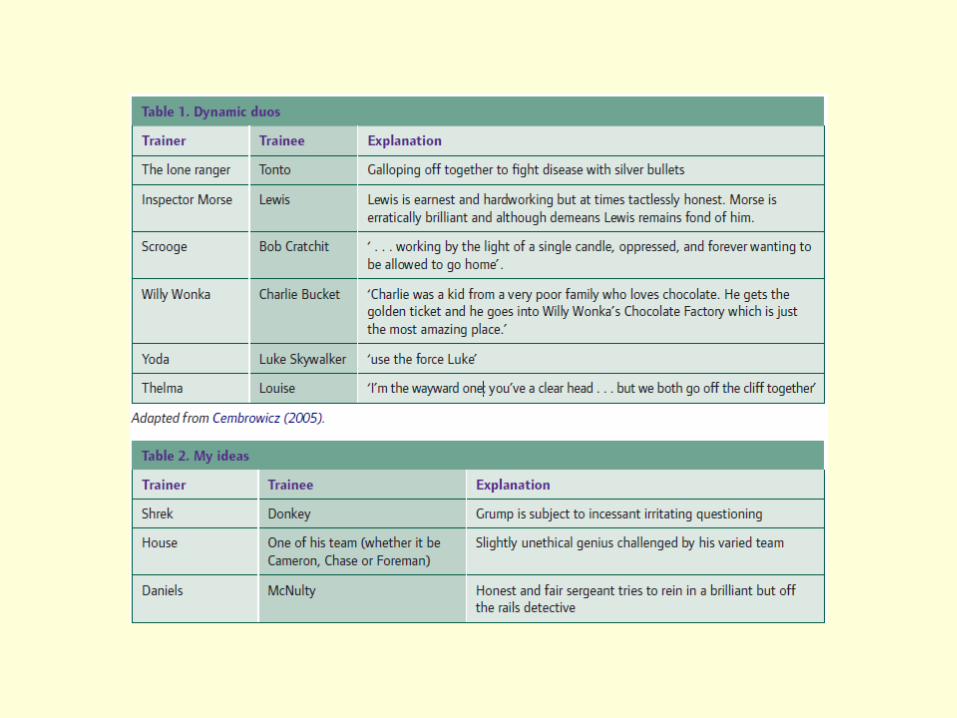
Trainer-Trainee Relationship
Consider the analogy to the doctor-patient relationship?
Develop relationship & rapport – chat time!
What can go wrong at the start?
What happens over time?
What happens when Dr & patients disagree?
GPs can have a bad day and take it out on patients
Trainers can have bad days…

ST3 Introduction
• Enhanced ST3• MRCGP Exam Overview• Year Planning• Chaperones• Overview of the VTS• E-Portfolio& Learning Log• OOH Training• Local Training Agreement
Checks with patient
End summary

The EndSafety netting
Final checking