st. louis integrated health network (ihn) · pdf filethe hssn agreed on several charges and...
TRANSCRIPT
St. Louis Integrated Health Network (IHN)Re-Entry Community Linkages (RE-LINK)
Evidence-based CHW systems navigation in St. Louis to link recently incarcerated young adults to community resources: Addressing improved provider care continuity, reduction in health disparities, and
reduction in recidivism post-Ferguson
Mikel Whittier, MHA – Program ManagerAtara Estes – Certified Community Health Worker
Phillip Brooks – Certified Community Health Worker
The St. Louis Integrated Health Network, through collaboration and partnership, will strive for quality, accessible and affordable
healthcare services for all residents of Metropolitan St. Louis, with an emphasis on the medically underserved.

St. Louis Integrated Health Network
ABOUT IHN
A non-profit membership health intermediary organization that collaborates with community health centers, public health departments, hospital systems, academic medical institutions and other safety net organizations to advance its mission.
The IHN acts as a convener and facilitates partnerships across the safety-net system toward the common goal of advancing health equity by increasing healthcare access and quality for the medically under-served.
2

IHN Board Network
Community Health Centers
HospitalSystems
Public Health Departments
Academic Institutions
Other Safety-Net Orgs
3

A Regional Crisis
Ferguson Commission (2015) noted:
“for thousands of St. Louisans, the status quo is killing them. The status quo means living in a food desert, with no grocery stores for miles around. The status quo means sending your children to underperforming schools that get fewer resources but dole out more punishments. The status quo means driving in fear of a court system that will put you in jail for failure to pay a traffic ticket” (p. 21).
4
Photograph by J. B. Forbes AP Photo/St. Louis Post-Dispatch.

Regional PrioritiesAccording to Ferguson Commission (2015), regional priorities should include:
• Justice for All
• Youth
• Economic Opportunity
• Safe Space for Conversation for Process Improvement
These priorities should be considered in regards to racial equity, tangible change, and health equity supported by research to be transformational, urgent, and unflinching.
Ferguson Commission. Forward through Ferguson: a path toward racial equality. 2015. Available at: http:// forwardthroughferguson.org
5

A divided region
Many social issues including race and access to resources can be illustrated with the Delmar Divide
Purnell J, Camberos G, Fields R. For the sake of all: a report on the health and well-being of African Americans in St. Louis and why it matters for everyone. 2014. p. 29. Available at: https://forthesakeofall. files.wordpress.com/2014/05/for-thesake-of-all-report.pdf
FULL FOR SAKE OF ALL REPORT: https://forthesakeofall.org/wp-content/uploads/2016/06/FSOA_report_2.pdf6

Ferguson Commission. Forward through Ferguson: a path toward racial equality. 2015. Available at: http:// forwardthroughferguson.org
FULL FERGUSION COMMISSION REPORT: http://3680or2khmk3bzkp33juiea1.wpengine.netdna-cdn.com/wp-content/uploads/2015/09/101415_FergusonCommissionReport.pdf
7

Purnell J, Camberos G, Fields R. For the sake of all: a report on the health and well-being of African Americans in St. Louis and why it matters for everyone. 2014. p. 30. Available at: https://forthesakeofall. files.wordpress.com/2014/05/for-thesake-of-all-report.pdf
Addressing Health Disparities
8

Purnell J, Camberos G, Fields R. For the sake of all: a report on the health and well-being of African Americans in St. Louis and why it matters for everyone. 2014. p. 30. Available at: https://forthesakeofall. files.wordpress.com/2014/05/for-thesake-of-all-report.pdf
Addressing Health Disparities
9

Health Access Best Practice➢ Healthy People 2020 has featured the IHN’s Community Referral
Coordinator (CRC) Program in their sharing library of "Who's Leading the Leading Health Indicators?“ as a national best practice.
➢ The CRC program is working towards Healthy People's goal of improving access to comprehensive, quality health care services.
➢ The CRC (1) meets non-emergent and/or admitted Hospital patients to provide education regarding availability of primary, specialty, behavioral health and urgent care services; (2) offer patients a choice of primary care homes; and (3) assist with scheduling follow-up appointments and arranging transportation/support services as needed.
➢ This same approach has been utilized in addressing crime prevention in the Re-Entry Community Linkages (RE-LINK) and Community Health Worker (CHW) model
10

CRIME IS A HEALTH AND WELLNESS CRISIS
11
Criminogenic Risk Factors = Social Determinants of Health

Crime Density in St. Louis
12

13
CRIME IN ST. LOUIS
CURRENTLY • Over the past 6 months, St.
Louis has experienced
roughly 4900 violent crimes
within the city limits City of St. Louis Metropolitan Police Department. (n.d.). Crime Mapping.
Retrieved July 7, 2017, from http://www.slmpd.org/crime_mapping.shtml

HOW CRIME COSTS HEALTHCARE. . . .
14
ASSAULT-RELATED GUNSHOT INJURIES LEVEL OF CARE AND COST
Number of Injuries Cost
2012
Emergency Department 188 $1,440,783
Inpatient Hospitalization 139 $9,844,379
2013
Emergency Department 175 $1,489,877
Inpatient Hospitalization 132 $12,127,613
2014
Emergency Department 190 $1,799,329
Inpatient Hospitalization 165 $14,639,410
Total 989 $41,341,382
MODHSS (Missouri Department of Health and Senior Services). MICA. In Injury MICA. Retrieved January, 2017, from
http://health.mo.gov/data/mica/InjuryMICA/

15

Purnell J, Camberos G, Fields R. For the sake of all: a report on the health and well-being of African Americans in St. Louis and why it matters for everyone. 2014. p. 19. Available at: https://forthesakeofall. files.wordpress.com/2014/05/for-thesake-of-all-report.pdf
Metropolitan St. Louis population. . .
16
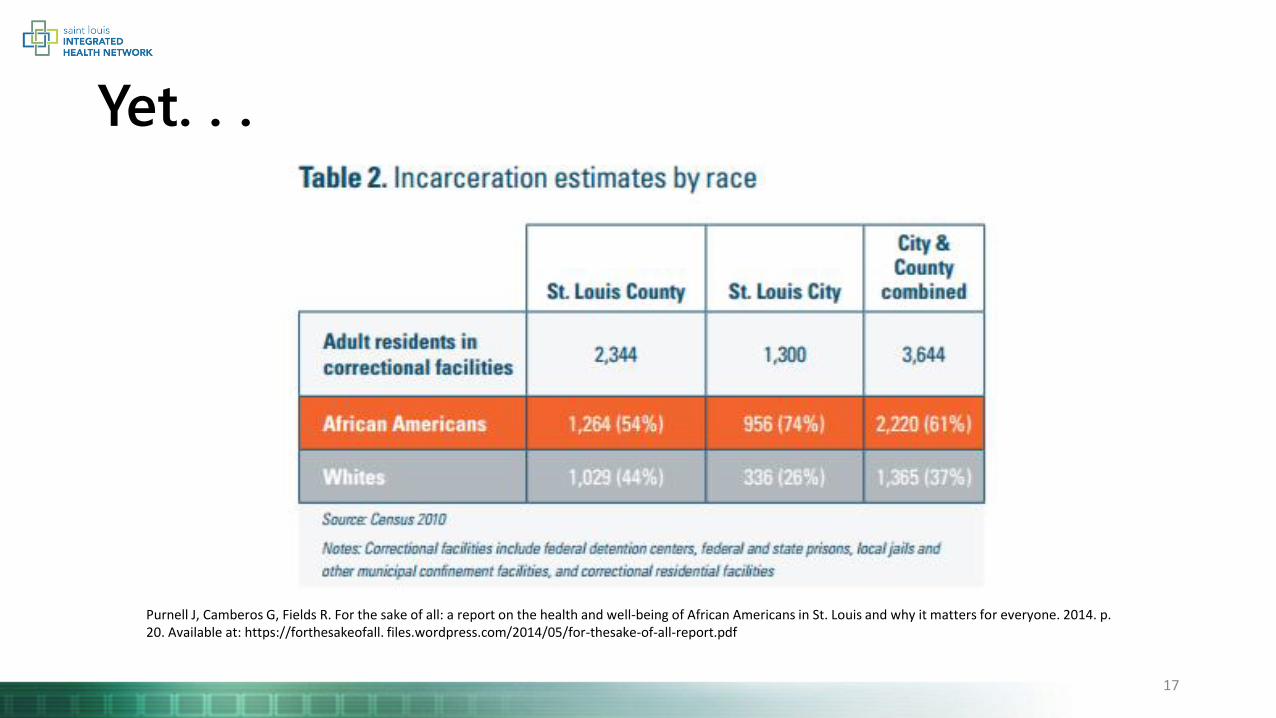
Yet. . .
Purnell J, Camberos G, Fields R. For the sake of all: a report on the health and well-being of African Americans in St. Louis and why it matters for everyone. 2014. p. 20. Available at: https://forthesakeofall. files.wordpress.com/2014/05/for-thesake-of-all-report.pdf
17

RE-LINK Objectives
AIM
• To demonstrate the effectiveness of multiple stakeholders
• Specifically, public health system and community support system working
• Implement a model transition process from jail
• minority and/or economically or environmentally disadvantaged re-entrants ages 18-
26
• “Link” community reentrants to community-based organizations and
resources
• healthcare providers, health care coverage, behavioral health, and social service
supports.
18

RE-LINK Strategic Planning
IHN’s goals were to align regional priorities including health and racial equity for:
• Improved transitions of care
• Improved access
• Improved health and social service network interoperability
• Improved sharing of data for translation into informational and evidence
Photograph by J. B. Forbes AP Photo/St. Louis Post-Dispatch.
19
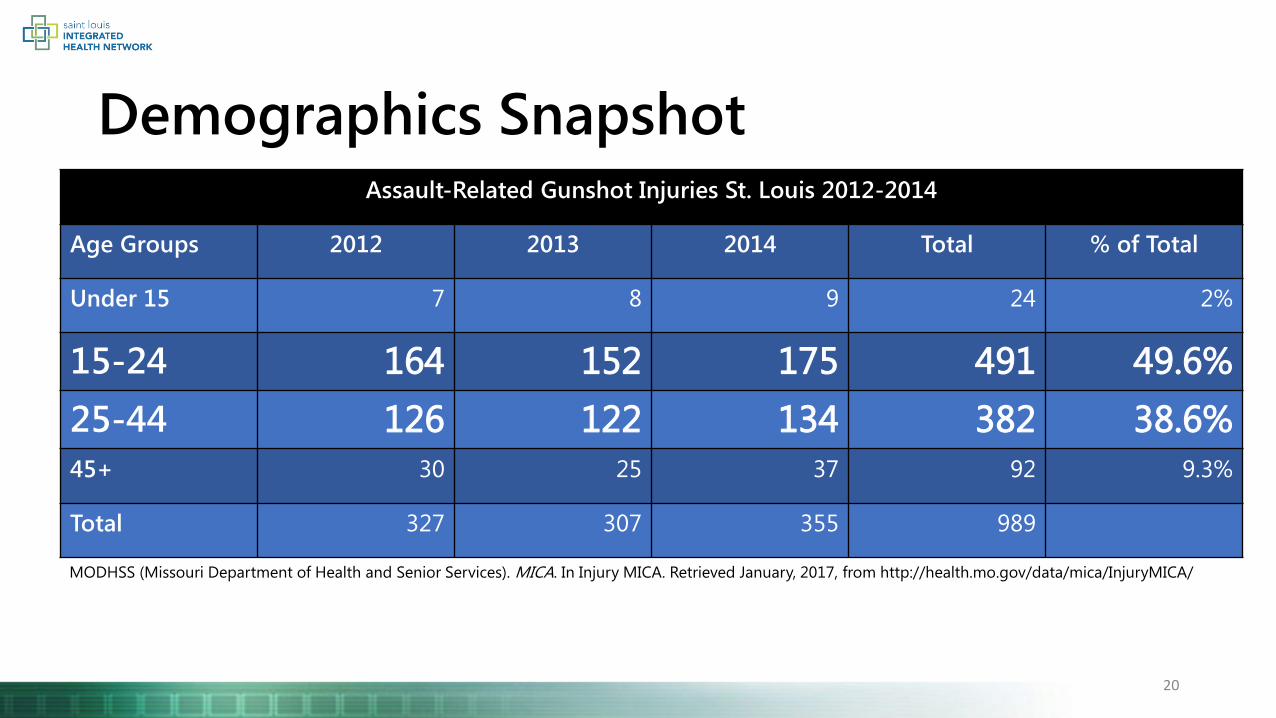
Demographics SnapshotAssault-Related Gunshot Injuries St. Louis 2012-2014
Age Groups 2012 2013 2014 Total % of Total
Under 15 7 8 9 24 2%
15-24 164 152 175 491 49.6%
25-44 126 122 134 382 38.6%
45+ 30 25 37 92 9.3%
Total 327 307 355 989
20
MODHSS (Missouri Department of Health and Senior Services). MICA. In Injury MICA. Retrieved January, 2017, from http://health.mo.gov/data/mica/InjuryMICA/

21
Health Centers, Health Providers, &
Health Intermediaries
Government Agencies
Housing
Employment Services
Multi-dimensional Social Service
Providers
Academic Partners
Community Health Worker
St. Louis City Jails
The RE-LINK model
Health & Social Services Network

Utilization of a Health & Social Services Network (HSSN) for Reentry
22
GOALS/CHARGES
• Improve collaboration and communication
• Promote the sustainability of resources
• Enhance the RE-LINK CHW model
• If program is effective at reducing recidivism
• pursue sustainability and expansion of the model
• Identify and address policy gaps and systemic barriers to successful reentry to the community

Health and Social Services Network (HSSN)The HSSN agreed on several charges and deliverables to ensure the network is working efficiently and effectively yet also to ensure reproducibility and sustainability
2017 Deliverables
Policy and Systems Change
• Develop a shared policy platform across the network
• Offer training and open houses to HSSN member organizations (e.g. policy engagement, tour of the jails, health equity, CLAS, trauma-informed care, etc.)
Communication and Coordination among Providers
• Identify common language to use across the network
• Documented processes and protocol for referral network communication and coordination between the jails, probation and parole, community reentrants, social service providers, and healthcare providers
Access and Care Continuity for Reentrants
• Quarterly review of program data to identify trends, barriers, and areas to improve access
• Identify and prioritize target populations to be impacted by efforts and measurable outcomes that will indicate progress
• Strategic plan for communication of HSSN efforts to providers, government, public health, and broader community
23

Defining policy for sustainable change
Building… • A shared vision of perpetual improvements that builds consensus and informs all
stakeholders
In order to Develop… • A course of action or guiding principles to achieve enduring community wellbeing
That is Implemented through…
• A law, regulation, procedure, administrative action, incentive, or voluntary practice being adopted by individuals, organizations, systems, and/or government.
Policy is. . .
24

RELINK Health and Social Service Network (HSSN)Backward Plan for Implementation of Policy Reform
Today
Sep Nov 2017 Mar May Jul Sep Nov 2018
First Health and Social Service Network Convening
9/1/2016
Develop HSSN Charge and Deliverables -Charge to build a Policy Platform
10/18/2016
Key Stakeholder Interviews to inform Policy Reform Ideas
11/1/2016
Policy Mapping Sessions
12/9/2016
HSSN Partners identify Policy Recommendations
1/12/2017
Identify HSSN Policy Prioritizations
3/9/2017
Finalize Policy Actions
3/31/2017
Implementation (update on ongoing progress)
5/11/2017
Complete Actions for 2017
11/9/2017 Revisit Plan and Prioritize for 20181/11/2018
BUILD DEVELOP IMPLEMENT BUILD
25

26
67%
31%
2%
Male Female Transgender
20
24
4
1
Age 18-21
Age 22-25
Age 26 Age 27*
84%
10%
4% 2%
Black/African American
White/Caucasian
Mixed/Multi-Racial
Unknown94% are Single
31% are Parents *One participant turned 27 shortly before Intake
Top 5 Most Common Charges
Unlawful Use of Weapon
Burglary
Probation Violation
Possession of Controlled Substance
Assault
Pending Charges
Other
Probation Violation
Revocation/Technical Violation
Pre-Trial
Parole Violation
Already Sentences
Reason for Confinement
DEMOGRAPHICS
78% have at least one prior arrest
Preliminary Data – Not for Distribution

27
39%indicated that for 15
or more of the last
30 days their mental
health* was not good
41%have at least 1
chronic health
condition
88%have a history of
substance use
30
17
2
No Insurance Public Insurance Insurance throughfamily member
Insurance Coverage Before Jail
1
2
3
5
16
Don't Know
Urgent Care
Doctor's Office
Hospital Emergency Room
Clinic or Health Center
Usual Source of Care
51% indicated they had a regular source
of care prior to jail
Most Common Chronic Conditions
Mental Health
Asthma
Substance Use
Hepatitis C
Chronic Pain
Seizures
Diabetes
*Including stress, depression, and problems with emotions
64%
21%
12%
2%
Frequency of Substance Use
Daily2-3/weekLess than once/month
35% of substance users indicated
stress was their main trigger
MEDICAL
Preliminary Data – Not for Distribution

Preliminary Data – Not for Distribution 28
SOCIAL DETERMINANTS OF HEALTH
Mode of Transportation
6
25
97
2
8th GradeCompleted
Up to 12thGrade, Nodiploma
GED High SchoolGraduate
Some College, Nodegree
Educational Attainment
33
10
41 1
Staying withFriends/Family
Own/rent houseor Apt
Homeless - OnStreet or in Car
Staying inShelter
Hotel
Housing Before Jail
20
17
8
13
Working for payat a job
Not working andlooking for work
Not working andnot looking for
work
Working but notfor pay at family-owned business
Unknown
Employment Status Before Jail

29
49 participants completed the intake process
25in pre-release
status
13released &
active in
program
9released &
currently
missing
2unenrolled*
from
program
*Reasons for disenrollment: 1) Death due to overdose 2) Moving out of state
22 referrals issued
10 unique individuals
Applications Completed
Gateway to Better Health (11)
Medicaid (7)
SNAP (3)
SSI/SSDI (3)
Types of Referrals
Substance Use (6)
Mental Health/Behavioral Health (4)
Job Training (4)
Housing Services (3)
Education (3)
Medical (2)
Others (5)
58%appointment
kept rate
REFERRALS
Averages 2.7
referrals per
person
5 RELINK
participants were
previously served by
CRC Program
LOCATION OF REFERRALS
Employment Connections
Places for People
Myrtle Hilliard Davis
Mission St. Louis
People Ready
Community Action Agency
Preliminary Data – Not for Distribution

30

Calls to action for preventing crime1. Like community health, crime prevention requires taking a holistic
approach addressing various aspects of one’s life that influences criminal behavior
2. Promote system accountability for sustained community wellbeing
3. Do not assume community members understand how to create and sustain health and wellness
a. Health literacy entails an individual’s ability to:
i. (1) read, (2) understand, and (3) communicate important health needs and the information necessary for addressing these needs
4. Sustainability. . . .
31

QUESTIONS
The St. Louis Integrated Health Network, through collaboration and partnership, will strive for quality, accessible and affordable
healthcare services for all residents of Metropolitan St. Louis, with an emphasis on the medically underserved.

APPENDIX
33
Health and Social Services Network (HSSN)
Government Agencies
• City of St. Louis
• City of St. Louis Mayor’s Office
• Senator Claire McCaskill’s Office
• Missouri Board of Probation and Parole
• City of St. Louis Department of Health
• Department of Corrections/St. Louis City Justice Center including Corizon and SLU OT program
Health Centers and Health Service Providers
• Myrtle Hilliard Davis Comprehensive Health Centers
• Family Care Health Centers
• Betty Jean Kerr People’s Health Centers
• Affinia Healthcare
• Preferred Family Healthcare/Bridgeway Behavioral Health
• People’s Community Action Corporation
• Places for People 34

Health and Social Services Network (HSSN)
Health Intermediaries
• Behavioral Health Network of Greater St. Louis
• Saint Louis Mental Health Board
Housing
• Criminal Justice Ministry
Employment Services
• Connections to Success
• Employment Connection
Multi-dimensional Social Service Providers
• Fathers’ Support Center
• The SPOT
• Mission St. Louis
• Center for Women in Transition
Academic Partners
• Washington University Evaluation Center
• SMART Decarceration Initiative
• St. Louis Alliance for Reentry
35

What does the referral process look like?
36

Pick 3 Policy Reform Recommendations
Coordinate and standardize the intake and discharge process within the jails. This could include:• Develop a formal method in the jails to track all inmates in need of services apart from those on the sentencing list
• Develop a standardized discharge planning process
• Develop a process to triage patients, but especially behavioral health patientsSuspend Medicaid upon incarceration rather than terminate coverage so that Medicaid can be immediately reinstated upon release from jails
Develop a digital regional platform for referral network resources for the public defenders (to help coordinate the overloaded public defender program)
Develop a centralized record system for the reentry population at the provider organizations
Create a system to get IDs without having to use community provider voucher programs
Enhance programming within the jails. This could include:• Develop more reentry related programming within the jails
• Design programs within the jails that are fun and engaging (e.g. art opportunities, t-shirt or game design, etc.)
• Reentry programming needs to start as soon as an individual comes into the jails
• Continue to expand the work of Agency Forward, to bring external programs into the jails to inform others of their servicesCreate a mental health court that for pre-charge diversion programming
Require formal accreditation standards for health services provided in the jails
Coordination of care after release. This could include:
• For provider capacity, work with service providers to track and coordinate when there are open spots for care
• Pilot a standardized process for communication between service providers (e.g. between health and social service providers coordinating shared
clients, etc.)
• Identify a strategy for a reentrant to keep a CM/assigned support to stay with you despite the services you receive or where you move to (e.g. Atara
Estes, RELINK CHW)
Provide support for training and workforce development/culture change. This could include:• Provide training to provider HSSN partners on topics such as cognitive thinking, equity and racial bias, strengths-based approaches, correctional
workforce training, and others as identified
• Create a trauma-informed culture at the jails and with all supporting partnersCreate opportunities for people who have been through the system to share their story and inform policy
Build a singular database like HMIS/Systems of Care to track participant success/engagement
Reform for charges and misdemeanors. This can include:• Issue misdemeanors as a citation only – no threat of incarceration for misdemeanors
• Remove incarceration as a sanction for probation and parole violations
• Advocate for policy to ban the box – focus on skills and abilities instead of convictions
• Work with judges to reconsider how to open up more pro bono legal services for misdemeanor cases
Develop a system to coordinate court dates. This can include:• Easy access to potential pending court dates
• Develop a system to attach the inmate roster
• Clarify the process for release datesRedesign/modify the building environment within the jails to support better health and decrease deprivation (e.g. color on the walls, lighting, sound)
Align funding for reentry to support identified priorities. This could include:• Funding strategy that supports organizational capacity of providers to adequately serve reentrants referred to programming
• Funding is coordinated to align with priorities set by the HSSN (e.g. need substance abuse treatment, behavioral health, housing, etc.)
37
Template Action PlanPolicy Reform Priority Action(s)
List actions your organization can take to support the
identified policy reform – include key steps needed to
take action
By When?
Day/Month/Year
By Whom?
Name key authorizing
leadership and
stakeholders within
your organization
How will success be
measured?
Identify key metrics,
outcomes, infrastructure,
and processes that will be
built as a result of the
action
1.
2.
3.
38

RE-LINK’s Comprehensive Staff
Bethany Johnson-Javois, CEO
Jessica Holmes, Principal Strategist –Alignment, Innovation, Growth
Amanda Stoermer, Outcomes and Information Manager
Casey Peetz, HR & Office Manager
Sagar Mehta, Health Equity Fellow
Mikel Whittier, RE-LINK Program Manager
Atara Estes, Community Health Worker
Phillip Brooks, Community Health Worker
Nancy Mueller, Network Evaluation Lead
Carrie Pettus-Davis, Co-Lead
Bobbi Carothers, Senior Data Analyst
Sarah Bobmeyer, Evaluator
Mackenzie Staub, Project Coordinator
Annie Grier, Content Consultant
Washington University in St. Louis
(Evaluation Team)
St. Louis Integrated Health Network
39

RE-LINK’s Jail Partners
Robin Edwards, Program Director
Jennifer Davis, Reentry Case Manager
Markeisha Franklin, Reentry Case Manager
Michelle Wayman, Corizon Discharge Planner
Brittany Conners, SLU Occupational Therapist
40