spp e eecchh y&& rll aanngguuaagge tthheerrappy ... · test of nonverbal intelligence – 2...
TRANSCRIPT

SSppeeeecchh && LLaanngguuaaggee TThheerraappyy SSeerrvviiccee
MMooddeell && EEffffeeccttiivveenneessss RReevviieeww::
SSttaaggee II ((00--55 yyeeaarr oollddss))
Department of Children’s Services & Department of Health, South
Australia
Leah Jeffries
Centre for Allied Health Evidence
University of South Australia
North Terrace
Adelaide SA 5000
Email: [email protected]
Telephone : (08) 83021403

The Centre for Allied Health Evidence (CAHE)
2
Contents Page
Glossary Outcome Measures 3
1. Introduction 4
2. Aim 7
3. Research Questions 7
4. Method 9
4.1. PECOT (Population, Exposure, Comparator,
Outcomes, Time) 9
4.2. Search strategy 10
4.2.1. Search terms 10
4.2.2. Databases 11
4.2.3. Search limits 11
4.2.4. Search validation 11
4.2.5. Data extraction 11
5. Results 13
5.1. Country of origin 13
5.2. Level of evidence/Quality of research 13
5.3 Summary of results 14
5.4 Key points 23
6. Discussion 28
7. Core Learnings 34
8. Conclusions 35
9. References 36
Acknowledgments 42
Appendix 1: Summaries of included papers 43
Tables
Table 1. Frequency of publication by country 13
Table 2. Frequency of publication by level of evidence 13
Table 3. Summary of results 15

The Centre for Allied Health Evidence (CAHE)
3
Glossary of Outcome Measures
Outcome measure: Measures: Assessment of Phonological Processes – revised (APP-R)
Phonology
Clinical evaluation of language fundamentals –3 (CELF-3): sentence structure subtest
Language comprehension
Clinical evaluation of language fundamentals –3 (CELF-3): word structure and word association subtests
Language production
Clinical evaluation of language fundamentals –3 (CELF – 3): recalling sentences subtest
Verbal memory
Communicative development inventories (CDI)
Vocabulary size
Developmental sentence scores (DSS)
Expressive language ability
Goldman-Fristoe Test of Articulation –Revised (GFTA-R)
Articulation
Index of Productive Syntax (IPSyn) Language production skills
Mean length of utterances (MLU) Syntax Metaphonological abilities battery (MAB)
Represents increasing levels of difficulty in the development of metaphonological abilities. Consists of rhyme matching, word initial matching, blending phonemes, word initial segmentation/matching and consonant deletion.
Parent responses to child utterances (PARESP)
Parent language modeling techniques.
Peabody individual achievement test – revised (PIAT): reading recognition and reading comprehension subtests
Reading
Peabody individual achievement test – revised (PIAT):spelling subtest
Spelling
Peabody individual achievement test – revised (PIAT): arithmetic subtest
Arithmetic
Peabody Picture Vocabulary Test – revised (PPVT-R)
Language comprehension
Percentage consonants correct metric (PCC) Phonology Pre-school language scales (PLS-3) Language ability: expression, comprehension and total
language Proportional number of utterances of parent and child (PROPUTT)
Is based on a count of all utterances including those that are unintelligible or incomplete occurring in the 10-minute transcript and then the child to parent ratio is calculated.
Receptive Expressive Emergent Language Scales (REEL)
Receptive and expressive language development.
Speech and Language Assessment Scale (SLAS)
Articulation, language and pragmatics
Test of language development – 2 Primary (TOLD-P 2)
Word discrimination
Test of nonverbal intelligence – 2 (TONI-2): geometric categories, sequences, and analogies subtest
Non-verbal skills
Total number of words (TNW) Linguistic complexity
The Centre for Allied Health Evidence (CAHE)
4
1 Introduction
The State Government of South Australia recognises the importance of optimal
speech and language outcomes, as measured by literacy and numeracy rates, for all
children in South Australia and this has been demonstrated in “South Australia‟s
Strategic Plan 2007”. Children with speech and language difficulties may have
poorer achievement and educational outcomes unless these difficulties are
addressed in a timely and effective manner (Stothard et al 1998).
Speech and language difficulties are common in childhood (Tomblin et al 1997).
They may be secondary to disabilities such as autism, hearing impairment, general
developmental difficulties, behavioural or emotional difficulties or neurological
impairment, or may be a primary condition (Law et al 2003). The prevalence of
speech and language difficulties varies from 1 to 15%, but 6-7% is the average
(Blum-Harasty & Rosenthal 1992, Law et al 2003, Tomblin et al 1997). These
difficulties may be transient or persistent, and may manifest in speech or language
impairment in receptive, expressive or metalinguistic domains, severally or together.
Risk factors include chronic otitis media, male gender, genetic factors, socio-
economic status, maternal level of education, positive family history of speech and
language impairment, difficulties in pregnancy and oral-motor difficulties (Campbell
et al 2003, Fox & Dodd 2002, Law et al 2003).
Speech and language therapy interventions are important in these children in order
to reduce the potential for significant short and long term implications for the child,
family and society since language delay can have a significant effect on school
achievement, social, emotional and behavioural development and adult literacy
(Felsenfeld et al 1992, 1994, Law et al 2003, Lewis and Freebairn 1992, Snowling et
al 2000, Stothard et al 1998). Intervention approaches for speech and language
delay disorders include didactic (direct training of linguistic behaviours), naturalistic
(teaching the child to respond effectively to the linguistic demands of the
environment) and hybrid (a combination of the two other forms) (Fey 1986). Direct
intervention can be provided either individually or within a group of children.

The Centre for Allied Health Evidence (CAHE)
5
Once a speech pathologist has identified impairment in speech and/or language,
specific interventions may be recommended. Therapy can take place in various
settings including but not limited to speech and language specialty clinics, home, and
schools or classrooms. Direct therapy or group therapy provided by a clinician,
caretaker, or teacher can be child-centered and/or include peer and family
components. Intervention duration often varies, depending on individual needs.
Intervention strategies usually focus on more than one domain depending on
individual needs such as phonology and syntax. Therapy strategies include
facilitative play, naming objects, modeling and prompting, imitation, drill, recasts,
discrimination tasks, reading, and conversation
Children whose speech and language impairment has have not remitted by the time
they start school are at increased risk for learning and acquiring literacy skills
(Bishop and Adams 1990). However, for many children, their speech and language
impairment is not detected until they reach school age (Gillon & Dodd 1993). It is
clear that early identification of problems can facilitate early introduction of
appropriate interventions, thus preventing further delay upon school entry. Delay at
school entry may lead to overall academic underachievement and, in some cases,
lower IQ scores that may persist into young adulthood (Lewis & Freebairn 1992).
Given the increasing recognition of early intervention in children with speech and
language delay, it is important to evaluate service delivery models aimed at children
in the pre-school age (i.e. <5 years) in order to ensure access to optimal services in
a timely manner, thus preventing further delay once they attend school. It is also
anticipated that both innovative and varying means of identification and intervention
in this young age group need to be considered because of the possibility that these
children may slip through the system undetected.
Although a previous systematic review (Law et al 2003) concluded that speech and
language therapy interventions for children with expressive phonological and
expressive vocabulary difficulties had a positive effect, the review only considered
randomised controlled trials, and did not examine the constructs underpinning
service delivery models. It also did not present results according to the children‘s
age. Additionally there is growing concern within the speech pathology discipline

The Centre for Allied Health Evidence (CAHE)
6
about reliance on randomised controlled trials (RCTs) because of the limitations
associated with applying standardized therapy across the wide heterogeneity of
participants (Bernstein Ratner 2006, Gillam & Gillam 2006).
Thus, children aged 0-5 years with a primary speech and/or language delay/disorder
form the population focus of this review. Since it is widely recognised that in addition
to knowing ―what‖ works best, it is also important to know ―how‖ to go about
performing what is considered to be best practice, we aim to investigate not only the
effectiveness of speech and language therapy for this population, but also the
constructs underpinning service delivery models.

The Centre for Allied Health Evidence (CAHE)
7
2 Aim
The overall aim is to provide an overview of the literature on the effectiveness and
models of service delivery of speech and language therapies for children with
speech and/or language difficulties/delay. This project has been divided into four
phases based on population characteristics (see Figure 1). This report relates to
Phase I.
3 Research Questions
Phase 1: What is the evidence underpinning speech and language therapy services
for children aged less than 5 years with primary speech and/or language
impairment/delay/disorder for improved speech and communication outcomes?
Phase 2: What is the evidence underpinning speech and language therapy services
for children aged 5-8 years with primary speech and/or language
impairment/delay/disorder for improved speech and communication outcomes?
Phase 3: What is the evidence underpinning speech and language therapy services
for children aged 9-18 years with primary speech and/or language
impairment/delay/disorder for improved speech and communication outcomes?
Phase 4: What is the evidence underpinning speech and language therapy services
for children with speech and/or language impairment/delay/disorder secondary to
associated co-morbidities for improved speech and communication outcomes?

The Centre for Allied Health Evidence (CAHE)
8
Review of literature on the effectiveness and models of service delivery of speech and language therapies for
children with speech and language difficulties
PHASE I Investigate research evidence for speech and language therapy for children with primary speech language impairment/delay/ disorder aged less than 5 years
PHASE II Investigate research evidence for speech and language therapy for children with primary speech language impairment/ delay/disorder aged 5 - 8 years
PHASE III Investigate research evidence for speech and language therapy for children with primary speech language impairment/ delay/disorder aged 9-18 years
PHASE IV Investigate research evidence for speech and language therapy for children aged less than 18 years with speech language impairment/ delay/disorder secondary to associated co-morbidities
Development of evidence based best practice statements which will assist in safe and quality health and educational service delivery for children with speech and language difficulties and achieve outcomes relevant for all
stakeholders concerned

The Centre for Allied Health Evidence (CAHE)
9
4 Method
4.1 PECOT (Population, Exposure, Comparator, Outcomes, Time)
P Phase I-III: Children (aged < 5 years; 5-8 years or 9-18 years respectively)
with primary speech and language problems (e.g. non-verbal, unintelligible,
dyspraxic/apraxic) that are not secondary to a diagnosed co-morbid condition
For Phase IV: Children (aged up to 18 years) whose speech and
language deficits have been diagnosed as being secondary to a co-morbid
condition (such as Downs Syndrome)
E Speech and language therapy including: parent training/education/Hanen,
consultative therapy, teacher training, group therapy, communication partner,
school-based therapy
C Either usual/standard care, placebo or no treatment, or no comparator
O Primary: speech, language, communication skills (including verbal and non-
verbal), articulation, intelligibility, fluency, functional
Secondary: parents behaviour/responsiveness
T Short term (immediate post intervention) and long term outcomes will be
considered if possible. Since speech and language difficulties can have a
lasting impact it is vitally important to consider long term impact of
interventions for children, their families and other stakeholders involved in
health and educational service delivery.

The Centre for Allied Health Evidence (CAHE)
10
4.2 Search strategy
A literature search of peer-reviewed databases was conducted in order to identify all
levels of evidence-based research. Included were any studies that reported speech
or communication outcome data (or secondary parental outcome data) in relation to
speech and language therapy services for children (aged < 5 years; 5-8 years or 9-
18 years) with speech and language delay/disorder/impairment. Specifically
included in phase I were any research papers that related to children aged less than
5 years at the commencement of therapy. Study participants must have had a
primary speech and/or language delay/disorder/impairment or at least be at risk of
such problems, with no diagnosis of any co-morbid conditions that impacted on their
speech or communication abilities.
4.2.1 Search terms Phase I
Term 1 Term 2 Term 3 Term 4
Global delay Child* Speech therapy Speech
Communication impairment Pre-school Language therapy Language skills
Severe communication
impairment
Kindergarten Therapy Communication skills
Developmental disability or
delay
Child care Parent training Articulation
(Speech or language)
impairment or delay or
disorder
0-5 year* Parent education Intelligibility
Non-verbal Consultative Function*
Unintelligible Hanen Parent*
Phonological disorder or
delay
Parenting skills Behaviour
Dyspraxia Teacher training Responsiveness
Apraxia Group therapy Communicative
interactions
Pre-verbal Communication partner Fluency
pre-linguistic
Pre-intentional
Cognitive delay

The Centre for Allied Health Evidence (CAHE)
11
Terms in each column will be linked with OR, and between columns linked with AND.
4.2.2 Databases
CINAHL
AMED
Medline
Psychlit
Psychinfo
A+ Education
Education (SAGE)
ERIC
Psycharticles
Psychology (SAGE)
Linguistics and language behaviour abstracts
4.2.3 Search limits
Publication type: outcome based research paper
Year of publication: 1990 onwards
Language: English
Age: <5 year olds (Phase I), 5-8 year olds (Phase II); 9-18 year olds (Phase
III), 0-18 years (Phase IV)
4.2.4 Search validation
The reference list was reviewed by a content expert with thorough knowledge of the
literature in this area, and additional references were identified in this manner.
4.2.5 Data extraction
The Centre for Allied Health Evidence (CAHE)
12
Once the relevant publications were identified and retrieved, they were summarised
using a standardised data extraction form that included the reference details, country
of publication, level of evidence (NHMRC classification, 1999), population, service
setting, service delivery model, frequency/length/duration/total number of
intervention sessions, study outcomes, author‘s conclusion and reviewer‘s
conclusion. The extracted information was then synthesised in order to provide a
summary of the current evidence for the effectiveness and service delivery models of
speech and language therapy for children aged less than 5 years.

The Centre for Allied Health Evidence (CAHE)
13
5 Results
A total of 39 papers were identified as meeting the inclusion criteria for phase I of the
review.
5.1 Country of Origin
All of the research papers were published in the western world, as can be seen in
table 1.
Table 1. Frequency of publication by country
5.2 Level of evidence/Quality of research
The majority of research papers were level III-2, or comparative studies as can be
seen in table 2.
NHMRC level of evidence No. of publications
II Randomised controlled trial 5
III-1 Pseudo-randomised controlled trial 2
III-2 Comparative study with control group 20
III-3 Comparative study with historical control 1
IV Case series 10
Conference proceeding 1
Table 2. Frequency of publication by level of evidence (NHMRC 1999)
Country No. of publications
UK 10
USA 10
Canada 8
Australia 6
Netherlands 2
UK/Australia 2
New Zealand 1

The Centre for Allied Health Evidence (CAHE)
14
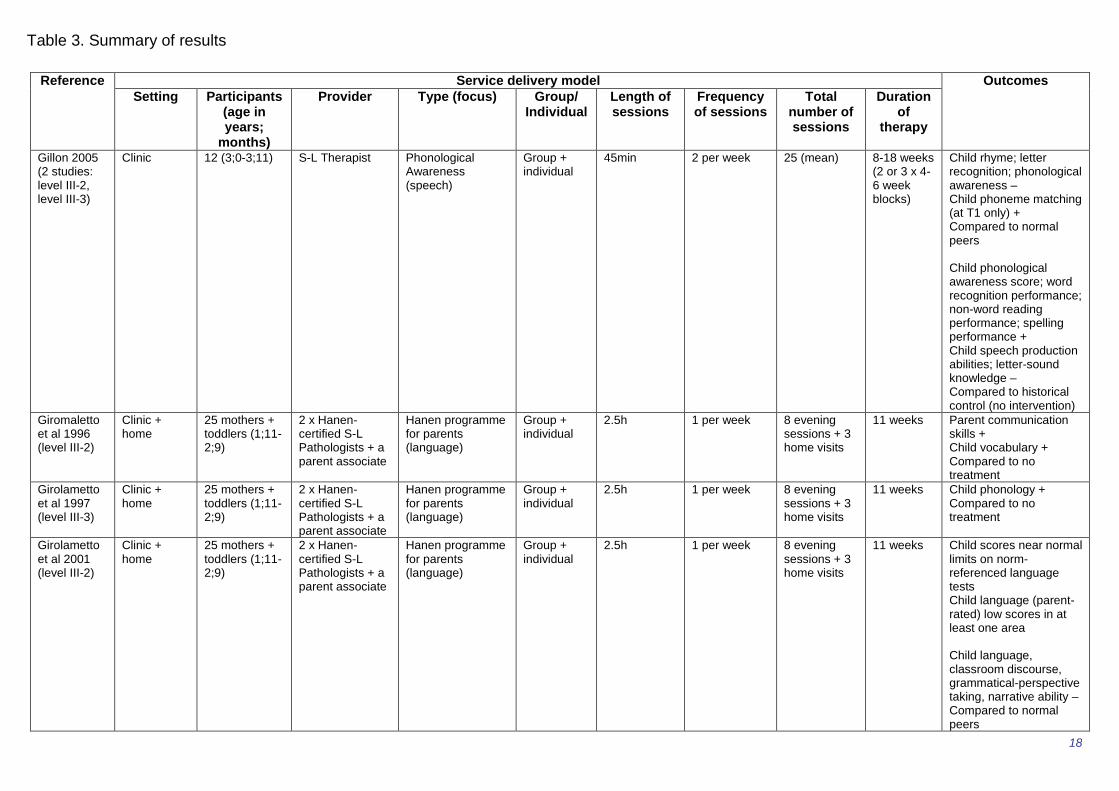
5.3 Summary of results
Please refer to table 3. for a summary table of the service delivery model descriptors
and effectiveness/outcome data for the included studies. Appendix 1 contains a full
summary of all the included studies.

Reference Service delivery model Outcomes
Setting Participants (age in years;
months)
Provider Type (focus) Group/ Individual
Length of sessions
Frequency of sessions
Total number of sessions
Duration of
therapy
Almost & Rosenbaum 1998 (level II)
Community hospital
30 (<6) S-L Pathologist Direct phonological (speech)
Individual 30min 2 per week 4 months Child phonology + Compared to no treatment
Baxendale & Hesketh 2003 (level III-2)
Clinic 37 (2;6–3;6) S & L therapist Hanen Parent training (language)
Group 2h15 1 per week 8 group + 3 home visits
11 weeks Parent language modelling + Child receptive and expressive language; length of utterance + Parent-child utterance ratio + = to individual clinic-based therapy
Bernhardt & Major 2005 (level IV)
Community clinic
12 (3;3-4;11) S-L Pathologist Direct Phonological (speech)
Individual 45min 3 per week 48 16 weeks Child speech; language; literacy + At 3 year follow-up
Best et al 1993 (level III-2)
Day nurseries
32 (2;1-4;0) Nursery-Officer + either S & L Therapist or Psychologist
Communication (language)
Small group 40min 2 per week 18-22 3-4 months Child knowledge relational concepts; initiations/interactions; engagement + Compared to no intervention
Bowen & Cupples 1998 (level IV)
Clinic 1 (4;4) ‗therapist‘ Direct Phonological (speech)
Individual 50min 1? per week 22 treatment + 5 assessment
17 months Child severity rating normal by 5;9; reading skills age appropriate by 6;7
Bowen & Cupples 1999a (level III-2)
Clinic 14 (2;11-4;9) ‗therapist‘ Direct Phonological (PACT) (speech)
Individual 50min 1? per week 21 10 months Child phonology + Compared to no treatment
Bowen & Cupples 1999b (level IV)
Clinic 1 (4;4) ‗therapist‘ Direct Phonological (PACT) (speech)
Individual ?50min 1? per week 18 treatment + 5 assessment
10 months Child phonology +
Bowen & Cupples 2004 (level IV)
Clinic 13 families ‗therapist‘ Direct Phonological (PACT) (speech)
Individual 50min ? 10-42 ? Not clearly reported
Table 3. Summary of results

The Centre for Allied Health Evidence (CAHE)
16
Reference Service delivery model Outcomes
Setting Participants (age in years;
months)
Provider Type (focus) Group/ Individual
Length of sessions
Frequency of sessions
Total number of sessions
Duration of
therapy
Crosbie et al 2005 (level III-1)
Clinic 18 (4;8-6;5) S-L Pathologist Core vocabulary vs. Phonological contrast (speech)
Individual 30min 2 per week 16 8-9weeks Child consonant accuracy; consistency + Core vocabulary more effective for inconsistent speech disorder Phonological contrast more effective for consistent speech disorder
Coulter & Gallagher 2001 (level III-2)
Nurseries 23 nursery staff + 52 children (3;4-4;2)
Teachers & learning support assistants
Early childhood educator training (Hanen) (language)
Group 15 h Child receptive & expressive language – Child social interaction skills + Provider confidence & skills + Compared to no intervention
Dodd & Bradford 2000 (level IV)
Clinic 3 (3;5-4;3) Speech therapist Phonological contrast vs. core vocabulary vs. PROMPT (speech)
Individual 30min 2 per week 12 6 weeks Child vocabulary; consistency + Core vocabulary more effective for inconsistent speech disorder Phonological contrast more effective for consistent speech disorder
Dowd et al 2007 (Level IV)
Community clinic
11 mothers + infants (0;6-2;6)
Speech pathologist + community worker
Parent-child interaction training (YMTD) (language)
Group 1 per week 8 8 weeks Parent communication; interaction +
Feldman et al 1993 (level III-2)
Home 28 mentally-retarded mothers + infants (0;5-2;4)
Psychologist or early childhood educator
Parent-child interaction training (communication)
Individual 60min 1 per week 21 Child verbalisations; vocalisations + Parent interactions; physical affection; praise; communication skills + Compared to attention control training at long term follow up (13-82 weeks)
Table 3. Summary of results

The Centre for Allied Health Evidence (CAHE)
17
Reference Service delivery model Outcomes
Setting Participants (age in years;
months)
Provider Type (focus) Group/ Individual
Length of sessions
Frequency of sessions
Total number of sessions
Duration of
therapy
Fey et al 1993 (level II)
Home + clinic
30 (3;8-5;10) S-L Pathologist vs. parents trained by S-LP
Parent-administered (following training) vs. clinician-administered grammar facilitation (language)
Individual + group
Parent training: 2hr Clinic visits: 1h Clinician administered: 1h individual 1h group
Parent meetings: 1 per week (first 12 weeks) then 1 per month Clinic visits: 1 per month Clinician administered: 1 per week individual 2 per week group
Parent training: 15 training/ meeting + 4 clinic visits Clinician administered: ~20 individual + ~40 group
4.5 months Child grammatical expression + Child use of pronouns - Compared to no intervention Parent-administered = clinician-administered
Gibbard 1994 (level III-2)
Community health centre
36 + 25 (2 studies) (2;3-3;3)
S & L Therapist? Parent speech and language therapy training (language)
Group 1h 1 per fortnight 11 6 months Child expressive language skills + Compared to no intervention and control intervention = to individual direct therapy
Table 3. Summary of results
The Centre for Allied Health Evidence (CAHE)
18
Reference Service delivery model Outcomes
Setting Participants (age in years;
months)
Provider Type (focus) Group/ Individual
Length of sessions
Frequency of sessions
Total number of sessions
Duration of
therapy
Gillon 2005 (2 studies: level III-2, level III-3)
Clinic 12 (3;0-3;11) S-L Therapist Phonological Awareness (speech)
Group + individual
45min 2 per week 25 (mean) 8-18 weeks (2 or 3 x 4-6 week blocks)
Child rhyme; letter recognition; phonological awareness – Child phoneme matching (at T1 only) + Compared to normal peers Child phonological awareness score; word recognition performance; non-word reading performance; spelling performance + Child speech production abilities; letter-sound knowledge – Compared to historical control (no intervention)
Giromaletto et al 1996 (level III-2)
Clinic + home
25 mothers + toddlers (1;11-2;9)
2 x Hanen-certified S-L Pathologists + a parent associate
Hanen programme for parents (language)
Group + individual
2.5h 1 per week 8 evening sessions + 3 home visits
11 weeks Parent communication skills + Child vocabulary + Compared to no treatment
Girolametto et al 1997 (level III-3)
Clinic + home
25 mothers + toddlers (1;11-2;9)
2 x Hanen-certified S-L Pathologists + a parent associate
Hanen programme for parents (language)
Group + individual
2.5h 1 per week 8 evening sessions + 3 home visits
11 weeks Child phonology + Compared to no treatment
Girolametto et al 2001 (level III-2)
Clinic + home
25 mothers + toddlers (1;11-2;9)
2 x Hanen-certified S-L Pathologists + a parent associate
Hanen programme for parents (language)
Group + individual
2.5h 1 per week 8 evening sessions + 3 home visits
11 weeks Child scores near normal limits on norm-referenced language tests Child language (parent-rated) low scores in at least one area Child language, classroom discourse, grammatical-perspective taking, narrative ability – Compared to normal peers
Table 3. Summary of results

The Centre for Allied Health Evidence (CAHE)
19
Reference Service delivery model Outcomes
Setting Participants (age in years;
months)
Provider Type (focus) Group/ Individual
Length of sessions
Frequency of sessions
Total number of sessions
Duration of
therapy
Glogowska et al 2000 (level II)
Community 159 (<3;6) Therapist Speech & language therapy (unclear)
Individual 50min 1 per month 8 8 months Child auditory comprehension + Child expressive language; phonology; language development; improvement to criterion level - Compared to watchful waiting
Goorhuis-Brouwer & Knijff 2002 (level III-3)
? 31 (1;5-5;4) Speech therapist Speech therapy (unclear)
? ? ? ? ? Child receptive & expressive language + Although some benefited from a watchful waiting approach alone
Harbers et al 1999 (level IV)
Clinic 4 (3;5-4;2) S-L pathologist? Phonological awareness & production (speech)
Individual 45min 2 per week 6-9 months Child production + Child feature awareness -
Hesketh et al 2000 (level III-2)
Clinic 61 (3;6–5;0) S & L Therapist Phonological awareness vs. articulatory therapy (speech)
Individual ? 1 per week 10 10 weeks Child meta-phonological ability; + Compared to progress in normal speakers Phonological = articulation
Hesketh et al 2007 (level II)
42 (4;0-4;6) Home or school (parent preference)
S & L Therapist? Phonological awareness (speech)
Individual 30min 2-3 per week 20 10 weeks Child phoneme isolation; phoneme segmentation; phoneme manipulation + Child alliteration awareness – Compared to control treatment
Jones 1995 (conference proceeding)
Home Not specified (2-5)
Early childhood specialist educator
Early language programme (Laurel House) (language)
Individual 45min 1 per week 12 12 weeks then monthly for 3 months + check up once per term if required
Not clearly reported
Table 3. Summary of results

The Centre for Allied Health Evidence (CAHE)
20
Reference Service delivery model Outcomes
Setting Participants (age in years;
months)
Provider Type (focus) Group/ Individual
Length of sessions
Frequency of sessions
Total number of sessions
Duration of
therapy
Leonard et al 2004 (level III-2)
University 31 (3;0-4;4) S-L pathologist and/or S-L Pathology student
Third-person singular –s vs. Auxiliary is/are/was training (language)
Individual ? 4 per week 48 12 weeks Child use of grammatical morpheme type that was target of the intervention + Third-person = auxiliary
Leonard et al 2006 (level III-2)
University 25 (3;0-4;4) S-L pathologist and/or S-L Pathology student
Third-person singular –s vs. Auxiliary is/are/was training (language)
Individual ? 4 per week 96 24 weeks Child use of grammatical morpheme type that was target of the intervention; use of morpheme serving as target for other group (mid-pt to end-pt only) + Third-person = auxiliary
Littleton 2004 (level III-2)
Home 8 parents + toddlers
S & L Pathologist + non-SLP early interventionist
Modified focussed stimulation parent training (language)
Individual ? ? ? ? Child vocabulary; talkativeness; language complexity + Parent communication + Compared to control intervention
Major & Bernhardt 1998 (level IV)
Clinic 19 (3;0-4;11) S & L Pathologist Phonological +/- metaphonological training (speech)
individual 3 per week 48 5-10 months
Child phonological development; metaphonological task performance +
McDade & McCartan 1998 (level III-2)
Community clinic + home
11 families (approx 2;0)
? ‗Partnership with parents‘ parent training (Hanen) (language)
Group + individual
? 1 per week 9 evening sessions + 3 home visits
12 weeks Child expressive & total language + Parent engagement + Compared to no treatment
Robertson & Weismer 1997 (2 studies: level III-2, level IV)
Classroom Study 1: 20 (3;8-5;1) Study 2: 6 (4;0-4;10)
Peers used as models
Structured interaction with peer models (language)
Group 15min 4 3 weeks Child vocabulary; lexical diversity; play theme related acts; use of linguistic markers + Compared to control intervention
Robertson & Weismer 1999 (level III-2)
‗Birth to 3‘ centre
21 (1;9-2;6) S-L Pathologists Interactive early language programme (language)
Small group 75min 2 per week 24 12 weeks Child utterances; vocabulary; intelligibility; socialisation skills + Parent stress + Compared to no treatment
Rvachew et al 2004
Hospital 34 (3;5-4;11) S-L Pathologist + student research
Phonemic perception training
Individual
Initial S & L therapy: 12
5 months Child phonemic perception; accuracy of
Table 3. Summary of results

The Centre for Allied Health Evidence (CAHE)
21
Reference Service delivery model Outcomes
Setting Participants (age in years;
months)
Provider Type (focus) Group/ Individual
Length of sessions
Frequency of sessions
Total number of sessions
Duration of
therapy
(level II) assistant and/or parent
(speech) Perception training: 15min
Perception training: 1 per week
Perception training: 16
articulation + Child phonological awareness - Compared to control intervention
Schuele et al 1995 (level IV)
Language acquisition pre-school
4 (3;10-5;3) S-L Pathologist + assistant teacher + 1-2 SP students
Redirect strategy (language)
Group 40min 4 per week 36 9 weeks Teacher use of redirects & prompted initiations + Child peer initiations unclear
Segers & Verhoeven 2004 (level III-2)
Special schools
24 (4;10-6;11) Experimenter Computer supported phonological awareness (speech)
Small group (although worked individually)
15min 2-3 per week 10-15 5 weeks Child phonological awareness + Speech manipulation did not produce any additional effect Compared to control intervention
Smith & Fluck 2000 (level III-2)
Diagnostic nursery & mainstream school (support centre)
20 (3-5) Teacher (+2 nursery nurses in nursery) + speech therapist ½ time
Structured game formats (language)
Small group ? ? ? ? Child participation in games; language + Compared to no intervention
van Kleeck et al 2006 (level III-1)
Pre-school Head Start programme
30 (3;10-5;0) Trained graduate and undergraduate research assistants from programmes in communication sciences and disorders
Book sharing sessions (language)
Individual 15min 2 per week 16 8 weeks Child literal language (receptive vocabulary); inferential language + Compared to no intervention
Ward 1999 (level III-2)
Home 122 (0;8-1;9) 2 x S & L Therapists
Speech and language therapy (language)
Individual ~30min Parent-administered sessions: 1 per day
4 home visits 4 months Child receptive & expressive language + at 2 year follow-up Compared to no intervention
Table 3. Summary of results

The Centre for Allied Health Evidence (CAHE)
22
Reference Service delivery model Outcomes
Setting Participants (age in years;
months)
Provider Type (focus) Group/ Individual
Length of sessions
Frequency of sessions
Total number of sessions
Duration of
therapy
Watson & Leahy 1995 (level IV)
University clinic
1 (3;1) Graduate and undergraduate students of communication disorders + Supervisor
Pre-school programme (speech)
Individual + group
2h + summer programme: 2.5h
2 per week 5 per week
12 week blocks over 2 years + 6 weeks over 2 summers
Child communication +
+ indicates positive outcome in experimental group; - indicates lack of positive outcome in experimental group; = indicates equivocal outcome between comparison groups Indicates Randomised controlled trial (RCT)
Table 3. Summary of results

5.4. Key points
Service delivery:
Intervention agents: In 29 studies, the agent was a speech pathologist
providing direct individual or group therapy to young children, or parent
training models. In some cases this was assumed but not necessarily clearly
specified (i.e. author provided the intervention but did not provide further
details on their qualifications). Other agents included teachers (in nursery or
pre-school settings) either alone or combination with a speech pathologist,
psychologists and, in some cases, research assistants with unspecified
qualifications.
Therapy approaches Direct therapy occurred in 26 studies where the agent
worked with individual children or groups of children. Indirect therapy was
assessed in 13 studies whereby the agent worked with parents or teachers to
teach them language facilitation techniques to use with children in their care.
Of these, the use of the Hanen program was the most frequent.
Therapy goals included phonological perception training, peer interaction
(including the redirect strategy whereby the agent redirected child initiations to
adults towards their peers), parent-child interaction, and vocabulary
development. A total of 20 studies examined a language therapy intervention,
16 studied speech therapy interventions (including speech, phonology and
phonological awareness), one paper examined a communication intervention
(parent-child interaction) and the remaining two studies did not clearly outline
the intervention type.
Intervention context The majority of therapy was administered on a 1:1
basis (21/32 studies). Group therapy was also commonly used in pre-school
or nursery settings where the whole class participated, or small groups of 3-6
children (occasionally with normally developing peers) (10/32 studies). Some
studies examined a combination of individual and group therapy (7/32 studies)
and the remaining study did not clearly report on the intervention context.
Dosage
o Session duration The length of sessions varied. Individual and group
sessions varied from 15 to 50 minutes duration (19 studies). Overall
the sessions varied from 15 minutes to 2.5 hours, although the longer

The Centre for Allied Health Evidence (CAHE)
24
sessions tended to be aimed at parents rather than the children. Parent
training sessions varied from 1 to 2.5 hours and usually occurred
weekly over a number of weeks with accompanying home visits to
check on their progress.
o Frequency This varied from daily to weekly to monthly and non-
intensive (1 session per month over a few months). One to two
sessions per week appeared to be the most common intervention
frequency. Whilst a comparison of frequency of service delivery was
not performed in any study, a frequency of once a month or less
seemed to be no more effective than ‗watchful waiting‘ in one study
(Glogowska et al 2000).
o Quantum of therapy The duration of therapy was commonly around 6-
12 weeks (12 studies), however some of the parent-training
programmes were hold over longer periods, and on some occasions
treatment was provided for up to 2 years (although this tended to occur
in smaller studies).
Effectiveness:
Overall, speech therapy appears effective in improving various outcomes for
children aged 0-5 years with speech and/or language delay, with all studies
finding at least one positive outcome following intervention.
Five randomised controlled trials were identified (Almost & Rosenbaum 1998,
Fey et al 1993, Glogowska et al 2000, Hesketh et al 2007 and Rvachew et al
2004), and the majority of remaining studies (n=19) were NHMRC level III-2
evidence (non-randomised controlled/comparative studies).
o Given that all five RCTs made different treatment comparisons, and
measured different outcomes it is not possible to synthesise results in
order to draw firm conclusions on the high-level evidence of
effectiveness of speech and language therapy for children aged 0-5
years.
o Almost & Rosenbaum (1998) found that four months of direct
phonological therapy improved children‘s phonological skills
significantly more than no therapy.

The Centre for Allied Health Evidence (CAHE)
25
o Hesketh et al (2007) also examined the effectiveness of phonological
therapy over 10 weeks, and compared it to a control treatment
(language stimulation): phonological therapy was more effective in
improving phonological skills but not alliteration awareness.
o Rvachew et al (2004) found that individual computer-based phonemic
perception training over 5 months led to a significant improvement in
children‘s phonemic perception and articulation accuracy, but not in
their phonological awareness when compared to a control intervention
(computer based stories)
o Fey et al (1993) compared parent-administered speech therapy
(following parent training) to clinician-administered therapy, and found
no significant difference between the two, with both improving the
children‘s grammatical expression but not use of pronouns over a
delayed-treatment control group.
o Glogowska et al (2000) compared individual speech and language
therapy to watchful waiting and although auditory comprehension was
significantly improved in the speech therapy group, there were no
significant improvements over watchful waiting in children‘s expressive
language, phonology, language development, or improvement to
criterion level. This study however provided a very small and non-
intensive therapy programme that varied between participants. Given
that the participant diagnoses and the interventions were not defined
adequately, this precluded clear conclusions on the effect of the
therapy.
o Thus the higher level evidence relating to the effectiveness of speech
therapy in this population remains unclear, although it appears that
speech therapy (phonological therapy in particular) may be more
effective in terms of selected outcomes over no therapy or control
therapy
The trends from the lower levels of evidence (single case descriptive studies
through to non-randomised comparative or controlled studies) indicated that
therapy was effective, resulting in improved outcomes in at least one aspect
of communication

The Centre for Allied Health Evidence (CAHE)
26
All of the studies of parent-administered intervention that measured parental
outcomes (n=7) demonstrated positive outcomes for parent‘s in terms of:
increased interaction skills; communication skills with their children and/or
reduced stress
11 studies included very young children (less than 3 years), and all of these
studies used a parent-training approach, with five studies examining the
Hanen approach
All of the studies involving the very young age group found that parent training
approaches led to a significant improvement in children‘s communication
when compared to either no treatment or control treatment
Parent training was equally effective to individual clinician-administered
therapy in the three studies (Baxendale & Hesketh 2003, Fey et al 1993,
Gibbard 1994) that made this comparison
Only one study used a parent training approach in the older (3-5 years) age
group (Fey et al 1993) and found that it was equally effective to individual
therapy, with both improving children‘s grammatical expression to a similar
degree
All 14 studies comparing a speech and/or language intervention to a no
treatment group found positive outcomes for children and/or parents in the
intervention group (except for one study that examined early childhood
educator training – Coulter & Gallagher 2001 – which is examined separately
below)
All seven of the studies comparing a speech and/or language intervention to a
control (either a non-speech and language focus, or ‗traditional therapy‘)
intervention found a significantly positive effect for the majority of children‘s
outcomes in the experimental group over the control group
Two studies compared speech therapy to ‗watchful waiting‘, with only one
finding that therapy was superior (and even then some children in the watchful
waiting group improved), perhaps suggesting that watchful waiting may in fact
have a positive effect on parent‘s behaviour
Group therapy was not compared to individual therapy in any of the included
studies. Studies reporting on both group and individual based therapy
provision reported at least one positive outcome for children and/or parents.

The Centre for Allied Health Evidence (CAHE)
27
Early childhood educator training (based on Hanen principles) was examined
in one study (Coulter & Gallagher 2001) and involved 15 hours training for
teachers and learning support assistants, although positive outcomes were
only demonstrated for teachers, but not for children‘s communication skills
Only three studies measured long term outcomes (up to 3 years following
intervention), with all three finding that positive outcomes immediately
following the intervention were maintained at follow-up

The Centre for Allied Health Evidence (CAHE)
28
6 Discussion
Effectiveness
Overall therapy was found to be effective for young children aged less than five
years with speech and/or language delay/disorder. Both the higher and lower levels
of evidence supported the effectiveness of speech and/or language therapy in this
population.
Of the higher level evidence (Almost & Rosenbaum 1998, Fey et al 1993, Glogowska
et al 2000, Hesketh et al 2007 and Rvachew et al 2004) there are indications that
speech therapy is effective in improving communication outcomes in young children
with speech and/or language problems. Whilst differences in intervention
approaches and outcome measures prevented pooling of results, the higher level
evidence suggests that from 10 weeks up to 4-5 months of phonological therapy is
more effective than either no treatment, or a control treatment in improving young
children‘s phonological perception skills. The results of one RCT lend support to the
equal effectiveness of parent administered language therapy to clinician
administered language therapy (Fey et al 1993). This finding was supported by a
recent systematic review by Law et al (2003) in which there was no significant
difference between the use of trained parents and clinicians to provide speech
therapy (for both phonology and expressive interventions).
Of the lower level evidence (non-randomised controlled studies through to case
series involving one or more subjects) there were indications that speech therapy
was associated with improvements in children‘s outcomes ranging from: receptive
and expressive language; length of utterance; speech; literacy; knowledge of
relational concepts; word recognition; spelling; peer
initiations/interactions/engagement; phonological skills; consonant accuracy;
consistency; vocabulary; social interaction skills; verbalizations; vocalizations;
talkativeness; and lexical diversity. Improvements were also noted in several parent
outcomes (that may in turn further influence children‘s outcomes) including:
language modeling; parent-child interactions/engagement; physical affection; use of

The Centre for Allied Health Evidence (CAHE)
29
praise; stress; and communication skills. Given the methodological limitations
inherent in these types of evidence it is not possible to infer that the interventions
used directly led to these positive outcomes, but taken with the higher level
evidence, it lends further support to the effectiveness of speech therapy for young
children with speech and/or language delay.
Given the recent advances in newborn screening and early detection of speech and
language problems, or even potential problems, children are being identified at a
much younger age and there is the potential to intervene at this early age, and thus
potentially prevent further delay as the children approach school age. Although it
cannot be strongly concluded on the basis of one randomized controlled trial (Fey et
al 1993) and two non-randomised studies (Baxendale & Hesketh 2003, Gibbard
1994) that parent training approaches are equal to, or more effective than, individual
clinician-administered language therapy, parent training may be an appropriate and
feasible initial intervention for young children with speech and/or language delay.
There is currently no evidence to suggest that parents are an inferior provider of
‗therapy‘ for their children, provided they are appropriately trained by a speech and
language therapist. Law et al (2003) in their systematic review provide further
evidence (across a wider participant age range and for both phonological and
expressive interventions) that there is no significant difference between therapy
administered by trained parents and clinicians. Since there were no studies included
in this review that compared clinician-administered to parent- administered therapy
for phonological disorders, any conclusions made on the basis of the language
studies cannot be automatically transferred.
Parent training approaches, although potentially effective for language disorders,
have the potential for a more varied outcomes for children, perhaps suggesting that
some parents may be more suited to parent treatment than others (Law et al 2003).
Further research is required to determine which parent characteristics are associated
with better outcomes for children. The success of any parent-training approach may
be dependent on the quality of the training programme used, and its ability to bring
about changes in the knowledge, skills and behaviour of trainees.
The Centre for Allied Health Evidence (CAHE)
30
Whilst parent training approaches on the whole appeared to be effective, the
evidence underpinning teacher training was less clearly established. The
effectiveness of early educator training was examined in one study (Coulter &
Gallagher 2001). The Hanen Early Childhood Educators (EEC) programme was
provided to teachers and learning support assistants with positive outcomes for
teachers undertaking the programme in terms of increased confidence, skills and
awareness. There was however no significant difference in receptive or expressive
language skills between children being taught by the trained teachers and those in a
non-trained group, however the sample population included children regardless of
whether they had an established diagnosis of speech and language delay/disorder or
additional impairments.
It would appear however that direct therapy provided by a speech pathologist (either
on an individual or group basis) was a more commonly utilised approach with the
pre-school (3-5 years) age group and was associated with positive outcomes in
these children. Since there were no studies that made a direct comparison between
individual and group therapy for the same intervention, it was not possible to draw
any conclusions about the comparative effectiveness of individual and group
therapy. Law et al (2003) examined this comparison and concluded on the basis of
one phonological and one expressive intervention study that there was no significant
difference between group and individual therapy. Considering the lack of clear
evidence to guide clinical decision making, both clinician judgement and patient
preferences can be utilized to determine the most appropriate approach for individual
children.
Therefore, if an initial parent-based approach has failed to demonstrate an
improvement by the age of three or four, or the child is only identified as having a
delay at this age, either direct individual or group therapy may be more appropriate
given the shorter time frame available to achieve age-appropriate levels of
communication prior to commencement of primary school. Using clinical experience
this decision may be dependent on a number of factors such as: the setting that the
child was identified as having a problem in; child care, nursery or pre-school
attendance; financial constraints; clinician time, family capacity, geographical issues
and availability.

The Centre for Allied Health Evidence (CAHE)
31
Service delivery models
Overall, there was a wide range of service delivery models incorporated into a
variety of different research methodologies, most of which represented low levels of
evidence.
There were two main types of service delivery across the 39 identified studies: direct
and indirect therapy. Direct therapy involved speech pathologists conducting
therapy directly with children, either individually or in groups. Parents may or may not
be present during the intervention sessions. The speech pathologist often
determined therapy goals, intervention context, therapy procedures, and the dosage.
The overall aim of these studies is first order change in terms of reducing impairment
(i.e. the linguistic deficit). In indirect therapy speech pathologists trained and
educated other people in techniques known to facilitate communication. Speech
pathologists may train parents, teachers, or learning support assistants to provide
therapy in the home or other settings. Indirect therapy achieves second order
change in children‘s outcomes via aiming to changing the children‘s communicative
environment. Thus indirect therapy influences activity and participation constructs.
Whilst there is no clear evidence on which type of service delivery model is more
effective than others, or what components are required to ensure the success of an
intervention, there are common components across the studies that suggest they
may play an important role.
Firstly, an intervention is most likely to be effective if it is provided by a qualified
speech and language therapist. The therapist may be directly involved in one-on-
one therapy or facilitating group sessions, or they may train parents or other people
involved in the care of these children to interact and communicate with the children
in ways that are likely to enhance their language development. By involving parents
in the therapy, it is likely that parents will also benefit, not only in ways that will
further benefit their children (i.e. improved interaction and communication skills) but
also in terms of reduced stress.

The Centre for Allied Health Evidence (CAHE)
32
Secondly, the choice of the type of therapy provided is most likely to be effective if it
is targeted at individual children‘s needs. Evidence of this is provided by studies by
Leonard et al (2004, 2006) which compared two types of therapy, third-person
singular –s and auxiliary is/are/was and found that each group showed significantly
greater use of the grammatical morpheme type that served as their respective target
than they showed on the past –ed and the control form. It was a common finding in
many studies that the outcome that demonstrated the most improvement was the
one that was most directly linked to the aim of the intervention, as in Rvachew et al
(2004) who found that five months phonemic perception training led to improved
phonemic perception but not phonological awareness in comparison to a control
intervention.
Thirdly, although not directly compared in any of the research, the dosage of therapy
is likely to have an impact on its effectiveness. Across the studies, therapy was
commonly provided at least weekly, and in some cases more frequently. Given that
all studies found at least one significant outcome, it appears that an average
frequency of once weekly therapy has the potential to bring about positive outcomes.
There may be also be a minimum amount of therapy required in that Glogowska et al
(2000) in their RCT found therapy to be no more effective than watchful waiting,
possibly due to the very low amount of therapy offered to the children. Although
Glogowska et al (2000) failed to find an effect after only 8 sessions over 8 months, a
more recent RCT (Hesketh et al 2007) found significant improvements following 20
sessions of phonological therapy after only 10 weeks when compared to a control
treatment. The remaining two RCTs (Almost & Rosenbaum 1998, Rvachew et al
2004) that found positive effects following phonological therapy offered one to two
sessions per week over a four or five month period. Thus it is possible that children
may demonstrate improvements in as little as 10 weeks, provided a sufficient
amount of therapy is provided.

The Centre for Allied Health Evidence (CAHE)
33
Common session durations for young children ranged from 15 minutes up to 50
minutes. Although there is no indication of the optimum session duration, there are
several factors that should be taken into consideration when planning a therapy
model. Younger children will obviously benefit from shorter periods in order to
maintain their concentration and attention, however there needs to be sufficient time
to allow feedback, learning and development.

The Centre for Allied Health Evidence (CAHE)
34
7 Core learnings
1. Speech and/or language therapy is effective for young children (aged
less than 5 years) with speech and/or language delay.
2. Parents, who have been trained by a speech pathologist, can provide
therapy with similar language outcomes to speech pathologists,
however more research is required to determine parental factors that
influence compliance and treatment success.
3. More research is required to address the paucity of literature on the
comparative effectiveness of parents versus clinicians in terms of
speech outcomes.
4. Since the literature did not indicate the superiority of either group or
individual direct therapy, clinical decision making can take into account
clinician judgement and experience, and client preference.
5. Direct therapy and parent training should ideally be administered by a
qualified speech pathologist.
6. The type of therapy should be influenced by, and tailored to, individual
children‘s needs.
7. The length of therapy sessions should be limited to 50 minutes or less
when focused on young children aged less than 5 years
8. A frequency of at least once weekly therapy is commonly associated
with positive treatment outcomes.
9. Improvements in children‘s communication outcomes may occur within
as little as 6-10 weeks of commencing therapy.

The Centre for Allied Health Evidence (CAHE)
35
8 Conclusion
On the basis of this systematic review of the literature pertaining to models of speech
pathology service delivery for children aged less than five years with speech and/or
language delay/disorder, speech therapy appears to be an effective intervention for
improving communication outcomes in this population.
Given the recent advances in early screening and detection of such disorders,
efficient and effective strategies are required to ensure that the potentially increasing
numbers of children diagnosed with these disorders achieve the best possible
outcomes and thus avoid the potential academic and vocational issues that they
would otherwise face. Addressing these problems, or preventing potential problems
at this early age will help to ensure that children may be able to reach their full
potential in terms of speech and language skills, in line with “South Australia‟s
Strategic Plan 2007”.

The Centre for Allied Health Evidence (CAHE)
36
9 References
Baxendale, J, and Hesketh, A 2003, ‗Comparison of the effectiveness of the Hanen
Parent Programme and traditional clinic therapy‘, International Journal of Language
& Communication Disorders, vol. 38, no. 4, pp. 397-415.
Bernhardt, B and Major, E 2005, ‗Speech, language and literacy skills 3 years later:
a follow-up study of early phonological and metaphonological intervention‘,
International Journal of Language & Communication Disorders, vol. 40, no. 1, pp. 1-
27.
Bernstein Ratner, N. 2006, ‗Evidence-based practice: An examination of its
ramifications for the practice of speech-language pathology‘. Language, Speech &
Hearing Services in Schools, vol. 37, no. 4, pp. 257-267.
Best, W, Melvin, D and Williams, S 1993, ‗The effectiveness of communication
groups in day nurseries‘, European Journal of Disorders of Communication, vol. 28,
no. 2, pp. 187-212.
Bishop, DVM, & Adams, C 1990, ‗A prospective study of the relationship between
specific language impairment, phonological disorders and reading retardation‘. The
Journal of Child Psychology and Psychiatry, vol. 31, no. 7, pp.1027-1050.
Blum-Harasty, JA, & Rosenthal, JBM 1992, ‗The prevalence of communication
disorders in children: A summary and critical review‘. Australian Journal of Human
Communication Disorders, vol. 20, pp. 63-80.
Bowen, C and Cupples, L 1998, ‗A tested phonological therapy in practice‘, Child
Language Teaching and Therapy, vol. 14, pp. 29-50.
Bowen, C and Cupples, L 1999a, ‗Parents and children together (PACT): a
collaborative approach to phonological therapy‘, International Journal of Language
and Communication Disorders, vol. 34, pp. 35-55.

The Centre for Allied Health Evidence (CAHE)
37
Bowen, C and Cupples, L 1999b, ‗A phonological therapy in depth: a reply to
commentaries‘, International Journal of Language and Communication Disorders,
vol. 34, pp. 65-38.
Bowen, C and Cupples, L 2004, ‗The role of families in optimizing phonological
therapy outcomes‘, Child Language Teaching & Therapy, vol. 20, no. 3, pp. 245-60.
Campbell, TF, Dollaghan, CA, Rockette, HE, Paradise, JL, Feldman HM, Shriberg,
LD, Sabo, DL, & Kurs-Lasky, M 2003, ‗Risk factors for speech delay of unknown
origin in 3-year-old children‘. Child Development, vol. 74, no.2, pp. 346-357.
Crosbie, S, Holm, A and Dodd, B 2005, ‗Intervention for children with severe speech
disorder: A comparison of two approaches‘, International Journal of Language &
Communication Disorder, vol. 40, no. 4, pp. 467-92.
Coulter, L and Gallagher, C 2001, ‗Evaluation of the Hanen Early Childhood
Educators Programme‘, International Journal of Language and Communication
Disorders, vol. 36 (Suppl), pp. 264-9.
Dodd, B and Bradford, A 2000, ‗A comparison of three therapy methods for children
with different types of developmental phonological disorder‘, International Journal of
Language & Communication Disorders, vol. 35, no. 2, pp. 189-209.
Dowd, T, Withers, E, Hackwood, J and Shuter, P 2007, ‗An Australian pilot study of a
parent-child interaction program - You make the difference‘, Neonatal, Paediatric &
Child Health Nursing, vol. 10, no. 1, pp. 13-9.
Feldman, M, Sparks B and Case, L 1993, ‗Effectiveness of home-based early
intervention on the language development of children of mothers with mental
retardation‘, Research on Developmental Disabilities, vol. 14, no. 5, pp. 387-408.

The Centre for Allied Health Evidence (CAHE)
38
Felsenfeld, S, Broen, PA, & McGue, M 1992, ‗A 28-year follow-up of adults with a
history of moderate phonological disorder: Linguistic and personality results‘. Journal
of Speech and Hearing Research, vol. 35, pp. 1114-1125.
Felsenfeld, S, Broen, PA, & McGue, M 1994, ‗A 28-year follow-up of adults with a
history of moderate phonological disorder: Educational and occupational results‘.
Journal of Speech and Hearing Research, vol. 37, pp. 1341-1353.
Fey, ME 1986 ‗Language intervention with young children‘. London: Taylor &
Francis.
Fey, M, Cleave, P, Long, S and Hughes, D 1993, ‗Two approaches to the facilitation
of grammar in children with language impairment: an experimental evaluation‘,
Journal of Speech & Hearing Research, vol. 36, no. 1, pp. 141-57.
Fox, AV, Dodd, B, & Howard, D 2002, ‗Risk factors for speech disorders in children‘.
International Journal of Language and Communication Disorders, vol. 37, pp. 117-
132.
Gibbard, D 1994, ‗Parental-based intervention with pre-school language-delayed
children‘, European Journal of Disorders Communication, vol. 29, no. 2, pp. 131-50.
Gillam, SL, & Gillam, RB 2006, ‗Making evidence-based decisions about child
language intervention in schools‘. Language, Speech & Hearing Services in Schools,
vol. 37, no. 4, pp. 304-315.
Gillon, GT 2005, ‗Facilitating phoneme awareness development in 3- and 4-year-old
children with speech impairment‘. Language Speech and Hearing Services in
Schools, vol. 36, pp. 308–324.
Gillon, G & Dodd, B 1993, ‗The phonological, syntactic and semantic skills of
children with specific reading disability‘. Australian Journal of Human Communication
Disorders, vol. 21, no.1, pp. 86-102.

The Centre for Allied Health Evidence (CAHE)
39
Girolametto, L, Pearce, P and Weitzman, E 1996, ‗Interactive focused stimulation for
toddlers with expressive vocabulary delays‘, Journal of Speech and Hearing
Research, vol. 39, no. 6, pp. 1274-83.
Glogowska, M, Roulstone, S, Enderby, P and Peters, T 2000, ‗Randomised
controlled trial of community based speech and language therapy in preschool
children‘, British Medical Journal, vol. 321, no. 7266, pp. 923-6.
Goorhuis-Brouwer, S and Knijff, W 2002, ‗Efficacy of speech therapy in children with
language disorders: specific language impairment compared with language
impairment in comorbidity with cognitive delay‘, International Journal of Pediatric
Otorhinolaryngology, vol. 63, no. 2, pp. 129-36.
Government of South Australia 2007, ‗South Australia‘s Strategic Plan‘.
http://www.stateplan.sa.gov.au/, accessed 24/9/07.
Hesketh, A, Adams, C, Nightingale, C and Hall, R 2000, ‗Phonological awareness
therapy and articulatory training approaches for children with phonological disorders:
a comparative outcome study‘, International Journal of Language & Communication
Disorders, vol. 35, no. 3, pp. 337-54.
Jones, J 1995, ‗The Laurel House Early Language Program‘, in 'Communicating
'now we're really talking': 12th State Conference of the Australian Early Intervention
Association (NSW Chapter) Inc, Vineyard Resort; Pokolbin NSW'.
Law J, Garrett Z and Nye C 2003, ‗Speech and language therapy interventions for
children with primary speech and language delay or disorder‘. The Cochrane
Database of Systematic Reviews, Issue 3.
Leonard, LB, Camarata, SM, Pawlowska, M, Brown, B and Camarata, MN 2006,
‗Tense and agreement morphemes in the speech of children with specific language
impairment during intervention: phase 2‘, Journal of Speech, Language and Hearing
Research, vol. 49, no. 4, pp. 749-70.
The Centre for Allied Health Evidence (CAHE)
40
Leonard, L, Camarata, S, Brown, B and Camarata, M 2004, ‗Tense and agreement
in the speech of children with specific language impairment: patterns of
generalization through intervention‘, Journal of Speech, Language and Hearing
Research, vol. 47, pp. 1363-1379.
Lewis, BA & Freebairn, L 1992, ‗Residual effects of preschool phonology disorders in
grade school, adolescence and adulthood‘. Journal of Speech and Hearing
Research, vol. 35, pp. 819-831.
Littleton, R 2004, ‗The Modifiability of Language Input with Toddlers with Expressive
Language Delay: A Study of a Team Approach to Parent Training‘, Dissertation
Abstracts International, A: The Humanities and Social Sciences, vol. 65, no. 1, pp.
115-A.
McDade, A and McCartan, P 1998, ‗'Partnership with parents' a pilot project‘,
International Journal of Language & Communication Disorders, vol. 33 Suppl, pp.
556-61.
Robertson, S and Weismer, S 1997, ‗The influence of peer models on the play
scripts of children with specific language impairment‘, Journal of Speech Language &
Hearing Research, vol. 40, no. 1, pp. 49-61.
Robertson, S and Weismer S 1999, ‗Effects of treatment on linguistic and social
skills in toddlers with delayed language development‘, Journal of Speech, Language
and Hearing Research, vol. 45, no. 5, pp. 1234-48.
Rvachew, S, Nowak, M, and Cloutier, G 2004, ‗Effect of phonemic perception
training on the speech production and phonological awareness skills of children with
expressive phonological delay‘, American Journal of Speech-Language Pathology,
vol. 13, no. 3, pp. 250-63.
Schuele, C, Rice, M and Wilcox, K 1995, ‗Redirects: a strategy to increase peer
initiations‘, Journal of Speech & Hearing Research, vol. 38, no. 6, pp. 1319-33.
The Centre for Allied Health Evidence (CAHE)
41
Segers, E, and Verhoeven, L 2004, ‗Computer-supported phonological awareness
intervention for kindergarten children with specific language impairment‘, Language,
Speech & Hearing Services in the Schools, vol. 35, no. 3, pp. 229-39.
Smith, C and Fluck, M 2000, ‗(Re-) constructing pre-linguistic interpersonal
processes to promote language development in young children with deviant or
delayed communication skills‘, British Journal of Educational Psychology, vol. 70(Pt
3), pp. 369-89.
Snowling, MJ, Bishop, DVM, & Stothard, SE 2000, ‗Is preschool language
impairment a risk factor for dyslexia in adolescence?‘ Journal of Child Psychology
and Psychiatry, vol. 41, pp. 587-600.
Stothard, SE, Snowling MJ, Bishop, DVM, Chipchase, BB, & Kaplan, CA 1998,
‗Language impaired preschoolers: A follow-up into adolescence‘. Journal of Speech,
Language and Hearing Research, vol. 41, pp. 407-418.
Tomblin, JB, Records, NL, Buckwater, P, Zhang, X, Smith, E, & O'Brien, M 1997,
‗Prevalence of specific language impairment in kindergarten children‘. Journal of
Speech, Language and Hearing Research, vol. 40, pp. 1245-1260.
van Kleeck, A, Vander Woude, J and Hammett, L 2006, ‗Fostering literal and
inferential language skills in Head Start preschoolers with language impairment
using scripted book-sharing discussions‘, American Journal of Speech-Language
Pathology, vol. 15, no. 1, pp. 85-95.
Ward, S 1999, ‗An investigation into the effectiveness of an early intervention
method for delayed language development in young children‘, International Journal
of Language & Communication Disorders, vol. 34, no. 3, pp. 243-64.
Watson, M and Leahy, J 1995, ‗Multimodal Therapy for a Child with Development
Apraxia of Speech: A Case Study‘, Child Language Teaching and Therapy, vol. 11,
no. 3, pp. 264-272.

The Centre for Allied Health Evidence (CAHE)
42
Acknowledgements
DECS and Department of Health, SA for funding this project.
Deb James for her valuable expert knowledge and input into the final report.
Cathy Olsson, Jenny Moody, Ellie Chronis, Linda Nimmo & other members of the
Statewide Interagency Speech Pathology Reference Group, SA for their guidance.

The Centre for Allied Health Evidence (CAHE)
43
Appendix 1 Summaries of included papers

The Centre for Allied Health Evidence (CAHE)
44
Summary of intervention program: Phonological Therapy
Reference:
Almost D & Rosenbaum P, 1998, ‗Effectiveness of speech intervention for phonological disorders: a randomized controlled trial‘, Developmental Medicine & Child Neurology, vol. 40, pp. 319-325
Country of
publication:
Canada
Publication type
(include level of
evidence):
Randomised controlled trial (level II)
Population:
30 children aged less than 6 years (mean 42 months) with severe phonological disorder but normal hearing skills, normal oral structures and function. The children functioned normally in receptive language, hearing, behaviour and social skills. Children were randomly assigned to one of two treatment groups: 4 months treatment followed by 4 months without treatment or the same treatments in reverse order.
Service setting:
Community: Hospital Speech-Language Pathology Department (individual therapy)
Service delivery
model:
Remediation for phonological disorders
Provided by speech-language pathologist with master‘s degree in Communicative Disorders
4-6 targets chosen for remediation for each child at the beginning
Typically one phonological process was targeted per session and focus changed to a new process approximately every four sessions
Each target repeated 2-3 times or until correct in conversation (modified-cycles approach)
Initially minimal pairs were used to teach the child the phonological contrasts
Emphasis then placed on production of the patterns in a traditional articulation therapy hierarchy (word, phrase, sentence, conversational levels)
Frequency/
intensity/
duration of service
provision:
30 min sessions twice weekly over 4 months
Outcomes evaluation
(by disorder subtype
if possible):
After treatment the groups were significantly different in all 3 phonology measures (APP-R (p=0.003), GFTA (p=0.001), PCC (0.001)) at the 4-month assessment and for PCC only (p=0.042) at the 8-month assessment
Group x time interaction for the 3 phonology measures indicated that the groups reacted differently over the different time intervals
Group x time interaction not significant for syntax (MLU)
Author’s conclusion: Pre-school children who received active speech intervention for

The Centre for Allied Health Evidence (CAHE)
45
remediation of a severe phonological disorder made greater gains over the 4-month treatment period than the improvements that occurred naturally in matched children who did not receive treatment during the same period. This suggests that conventional speech therapy for phonological disorders as currently practiced in a community setting is efficacious and effective for this population.
Reviewer’s
conclusion:
Community-based individual therapy appeared to be more effective for remediation of severe phonological disorders than no treatment.

The Centre for Allied Health Evidence (CAHE)
46
Summary of intervention program: Hanen vs. Conventional clinic-based
Reference:
Baxendale, J, and Hesketh, A 2003, ‗Comparison of the effectiveness of the Hanen Parent Programme and traditional clinic therapy‘, International Journal of Language & Communication Disorders, vol. 38, no. 4, pp. 397-415.
Country of
publication:
UK
Publication type
(include level of
evidence):
Comparative study (level III-2)
Population:
Thirty-seven children aged 2;6–3;6 years with a diagnosis of language impairment and their parents. Inclusion criteria:
Between the ages of 30 and 42 months at initial assessment.
To have received no previous therapy.
No profound sensorineural hearing loss.
Normal non-verbal development. Language impairment was classified according to the following criteria:
Expressive language impairment: o Standard score of 80 or less on the expressive section of the
PLS3-UK. o Standard score of 81 or more on the receptive section of the
PLS3-UK (Comprehension was therefore within normal limits).
Receptive/expressive language impairment: o A standard score of 80 or less on both the receptive and
expressive sections of the PLS3-UK. English was first language and all children were Caucasian.
Service setting:
Hanen Parent Programme (HPP) parent group training vs. conventional clinic-based individual therapy.
Service delivery
model:
HPP:
group sessions carried out by two trained speech & language therapists
focus on parents‘ language and interaction style
typical session included reviewing the previous week, the presentation of new information, videotapes and role-play to illustrate key techniques and for discussion
carryover tasks assigned
3 home visits where parent and child were briefly recorded during free play and the tape was reviewed by the parent and therapist to provide immediate feedback
Clinic-based intervention:
one-to-one conventional therapy with a speech & language therapist with no experience with HPP
Therapy should focus on a child‘s expressive and receptive language abilities (not phonology).
parent or carer present for all sessions
therapist interacts directly with the child to elicit a response and to demonstrate to the parent various techniques that promote language

The Centre for Allied Health Evidence (CAHE)
47
such as modelling, imitation, expansion and focusing attention through play
Frequency/
intensity/
duration of
service provision:
HPP:
11-week programme included eight weekly group sessions and three home visits
2 hours 15 minutes sessions
Time allocated to any one family was about 30–45 minutes. Clinic-based intervention:
a minimum of eight and up to a maximum of 12 weekly 45-minute sessions (to match HPP)
Outcomes
evaluation (by
disorder subtype
if possible):
The majority of children improved in their language standard scores
No significant difference between programmes for PLS-3 (UK) scores, MLU scores, turn taking (PROPUTT scores), and parent responses to child utterances (PARESP)
The Hanen therapy produced better results than clinic therapy for those children with receptive language difficulties on the PLS-3
The children with expressive language difficulties appeared to improve more quickly in the clinic group than the Hanen group
Both types of therapy were associated with an increase in expansion and imitation strategies by parents and a relative reduction of utterances compared with the number their child produced.
HPP was more costly than clinic-based therapy when measured in therapist time however it depended on how many families were included in the group.
Author’s
conclusion:
The majority of children involved in the project (71%) improved in language skills over the 12 months. However, given the severity of the children‘s language difficulties, the fact that there was no comparative control group means that we cannot attribute change in language scores to therapy alone, but improvements may have occurred as a result of maturation. There were no differences in outcomes between HPP and clinic-based therapy, however different families benefit from different types of therapy and they should be selected accordingly.
Reviewer’s
conclusion:
It appears that both HPP and clinic-based therapy can lead to improved outcomes for children with language impairment. There was some suggestion that children with receptive language difficulties may benefit more from HPP whereas children with expressive language difficulties might benefit earlier from clinic-based one-on-one therapy.

The Centre for Allied Health Evidence (CAHE)
48
Summary of intervention program: Phonological therapy
Reference:
Bernhardt, B and Major, E 2005, ‗Speech, language and literacy skills 3 years later: a follow-up study of early phonological and metaphonological intervention‘, International Journal of Language & Communication Disorders, vol. 40, no. 1, pp. 1-27.
Country of
publication:
Canada
Publication type
(include level of
evidence):
Case series (level IV)
Population:
12 children with moderate to severe phonological impairments aged between 3;3 and 4;11 years of age at the commencement of the programme, followed up 3 years later at mean age 7;2 years. The children had normal hearing and oral-motor function at the time of testing.
Service setting:
Community, clinic-based individual therapy
Service delivery
model:
Conducted by community speech-language pathologist
Based on non-linear phonological analyses and treatment approaches that emphasized the componential structure of speech sounds, syllables and words
Children participated with ‗significant others‘
One-on-one sessions
First 12 weeks addressed phonological goals, divided equally between syllable structure and segments (phonemes) and features
Final 4 weeks also addressed metaphonological goals in rhyming, alliteration and/or segmentation
Goals for each child were based on individual needs as determined by the analyses, in accordance with three basic principles (strengths, address phonological categories and target non-default structure and features).
SLPs received 2 days of training to learn the analysis and treatment procedures
Frequency/
intensity/
duration of
service provision:
45 min individual treatment sessions three times a week over 16 weeks
Outcomes
evaluation (by
disorder subtype
if possible):
Significant gains on all measures (PCC, word shape match, metaphonology & IPSyn) immediately after intervention
At 3 year follow up:
All children were intelligible in conversation
7/12 had average or above average GFTA-R scores
All participants scored within normal limits on the Word Discrimination subtest of the TOLD-2P, although 6/12 children scored in the low average range.
Total metaphonology scores ranged from 18 to a ceiling score of 60

The Centre for Allied Health Evidence (CAHE)
49
All children scored within normal limits or above on the Sentence Structure subtest of the CELF-3 and the PPVT-R
Language production scores on the CELF-3 Word Structure and Word Association subtests also showed average or above average performance
11/12 children had average or above average scores on the WISC-III (Wechsler 1989) digit span subtest.
8/12 had average or above average scores on the Recalling Sentences subtest of the CELF-3
All children scored within or above normal limits on the three subtests of the TONI-2
On the PIAT-R Reading Recognition (RR) and Reading Comprehension (RC) tasks, 10/12 children had average or above average scores; on the arithmetic subtest, 9/12 children had average or above average performance; and on the spelling subtest, 7/12 children had average or above performance.
Only one preschool study variable was significantly correlated with later reading and spelling skills: post-intervention metaphonology
Author’s
conclusion:
Most children performed within normal limits on a number of speech, language and literacy tasks, in spite of their early history of severe phonological impairments and delays in language production and metaphonology. Early phonological and metaphonological intervention can promote normalization of speech development, and normal acquisition of literacy skills for children with severe phonological impairments. Not all children will demonstrate short-term normalization, but the level and prevalence of risk can be reduced.
Reviewer’s
conclusion:
The phonological intervention appeared to lead to improved outcomes for children with phonological impairments, both in the short term, and at 3 years follow-up. Although only a small case series, it may give some indication that ongoing intensive therapy may not be required for this population.

The Centre for Allied Health Evidence (CAHE)
50
Summary of intervention program: Day Nursery small group therapy
Reference:
Best, W, Melvin, D and Williams, S 1993, ‗The effectiveness of communication groups in day nurseries‘, European Journal of Disorders of Communication, vol. 28, no. 2, pp. 187-212.
Country of
publication:
UK
Publication type
(include level of
evidence):
Comparative study (level III-2)
Population:
32 children aged 25-48 months who either: represented a concern to parents or staff of a day nursery regarding their coping, and especially their communication; or had a language delay in expression or understanding or inappropriate social communication; or a high score on a behaviour checklist. 29% failed a hearing test, and for a further 46% there were queries over their hearing. Children did not have a severe language delay, a specific or severe disorder of communication or emotional development, severe specific phonological or articulatory problems, little or no English, or involvement in other regular intervention.
Service setting:
Three inner London Day Nurseries (two were run by Social Services, the other was a community day nursery) providing small-group therapy.
Service delivery
model:
The nurseries operated using a key-worker system where one nursery-officer was responsible for the daily care of a small group of children
Baseline and follow-up assessment for both communication and control groups were administered by a research assistant
Communication group:
Small-group approach with high adult:child ratio
5-6 children, 1 of 2 nursery staff, either the speech and language therapist or psychologist were involved in the sessions
Parents were informed of the aims and times of the sessions and were invited to attend
Themes were decided on by project and nursery staff and were repeated at regular intervals
Toys and equipment reflected the multicultural nature of the group
General guidelines on ‗attention getting‘, language development, concentration and involvement of children in the group were discussed
Aims were developed for individual children based on initial assessment and observation and these incorporated smaller steps which could be reviewed
Control group:

The Centre for Allied Health Evidence (CAHE)
51
Not strictly classified as ‗no intervention‘
Several key workers and parents had attended or received feedback from assessments
Children remained in the day nursery room whilst the communication group received the intervention
Frequency/
intensity/
duration of service
provision:
40-minute sessions, twice per week
Average total of 18-22 (?slightly unclear) sessions over 3-4 months
15 minutes of free play, 15 minutes of attention, listening and language games, 5-10 minutes of action songs
Outcomes evaluation
(by disorder subtype
if possible):
At initial baseline assessment children were more than 9 months behind on verbal assessments and at or above age appropriate level on non-verbal assessments
Post-treatment, children in the communication group performed significantly better than baseline on the test of concept development; raw score for drawing of figures and shapes; rating for figure drawing whereas the control group did not
Both intervention and control groups improved on: two verbal measures (100 words expressive vocabulary and raw score of Boehm test of concept development)
Intervention group made significantly more initiations and interactions than baseline but the control group did not
Length of interactions and level of engagement improved significantly for the intervention group but not for the control group
Change scores were significantly greater for the intervention group for Boehm test of concept development
Author’s conclusion:
This small group intervention was shown to improve children‘s communication more than a matched control group from the same day nursery who did not receive the intervention.
Reviewer’s
conclusion:
Although the intervention group made significant improvements in communication and the control group did not, the improvement from baseline was only significantly different between the groups for: Boehm test of concept development; number of initiations/interactions and level of engagement.

The Centre for Allied Health Evidence (CAHE)
52
Summary of intervention program: PACT (Phonological Therapy)
Reference:
Bowen, C and Cupples, L 1998, ‗A tested phonological therapy in practice‘, Child Language Teaching and Therapy, vol. 14, pp. 29-50.
Country of
publication:
Australia (NSW)
Publication type
(include level of
evidence):
Case study (level IV)
Population:
A girl aged 4;4 years at the study outset, with a moderate phonological disability. She was a monolingual speaker of Australian English with normal hearing, and her language skills, other than phonology, were within the average range.
Service setting:
Clinic-based individual therapy
Service delivery
model:
Individual sessions with child and mother
Additionally, the speech homework book went to preschool once a week on the same day during therapy blocks.
Involved multiple exemplar techniques, including auditory bombardment and minimal meaningful contrasts activities and metalinguistic tasks, for example, homophony confrontation, lexical and grammatical innovations using new words, and plural and past tense morphemes to facilitate the emergence of new phonological contrasts and phoneme–grapheme correspondence awareness to facilitate awareness of systematic sound patterning.
Integral to the model are: parent education, phonetic production training, the blocks-and-breaks scheduling of consultations, parent participation and homework.
Frequency/
intensity/
duration of
service provision:
50 minute sessions
Block one: nine consultations. Break: 10 weeks.
Block two: eight consultations. Break two: 10 weeks.
Block three: eight consultations. Break three: 14 weeks
Block four: three consultations.
During therapy blocks 18 x 5-min homework sessions per week at home one-to-one with her mother, and one 5-min session per week at pre-school one-to-one with her teacher.
Total 27 consultations (5 assessments and 22 treatment sessions) over 17 months
Outcomes
evaluation (by
disorder subtype
if possible):
Between the ages of 4;4 and 5;9 years descriptive severity rating progressed from moderate to normal with no phonological deviations, or phonemic replacements, apparent in her phonology
At follow up at age 6;5 years difficulties with the first stages of reading acquisition were quite quickly overcome with appropriate help (she received nine weeks, twice-weekly individual reading remediation with a specialist teacher).

The Centre for Allied Health Evidence (CAHE)
53
When re-tested at 6;7, on the Woodcock test her reading skills were age appropriate and approximated the grade average
Author’s
conclusion:
The strengths of the model are the particular combination of techniques used, the way in which information is disseminated to parents and teachers, the planned blocks and breaks scheduling of appointments, the methods used for measuring severity and for recording progress, and the degree of family participation in therapy programmes.
Reviewer’s
conclusion:
This paper provides an overview of a broad-based phonological therapy methodology for developmental phonological disorders, with reference to one child‘s progress. It does not indicate treatment efficacy, but does suggest important constructs underpinning the service delivery model:
combination of techniques
parent education
phonetic production training
the blocks-and-breaks scheduling of consultations
parent participation
homework

The Centre for Allied Health Evidence (CAHE)
54
Summary of intervention program: PACT (Phonological Therapy)
Reference:
Bowen, C and Cupples, L 1999a, ‗Parents and children together (PACT): a collaborative approach to phonological therapy‘, International Journal of Language and Communication Disorders, vol. 34, pp. 35-55. Based on doctoral dissertation: Bowen (1996), Evaluation of a phonological therapy with treated and untreated groups of young children. Ph.D. dissertation, Macquarie University.
Country of
publication:
Australia (NSW)
Publication type
(include level of
evidence):
Research underpinning paper: comparative efficacy study (level III-2).
Population:
14 preschoolers, aged 2;11 to 4;9 at the outset, with phonological development significantly below age expectations and a matched control group of eight children. The children had normal hearing and English as their first language (monolingual households).
Service setting:
Clinic-based individual therapy
Service delivery
model:
Guiding principles:
The therapy model is based on phonological analysis and assessment, which includes basic, intermediate and specific goals.
Therapy planning is predicated on the principle that there are predictable patterns or regularities in the child‘s productive phonology.
Therapy is based on the principle that the main function of phonological patterning is its communicative function in signalling meaning.
Therapy emphasizes the importance of fostering in the child awareness that the purpose of phonological development is effective communication and hence, aims to nurture metaphonetic and metaphonological awareness.
Therapy aims to change the child‘s phonological patterns so as to facilitate the development of a more functional system of sound structures and contrasts.
Therapy is structured to take advantage of the organization of phonological patterning by eliciting and establishing changes in the child‘s productive patterns, through the use of natural sound classes and structures.
Therapy involves enlisting family participation in a range of formal and informal homework activities, for reasons inextricably bound up with the connections between communicative context, communicative intent, and communicative effectiveness.
Therapy targets are selected using linguistic criteria taking into account motivational factors.
Family education and training occur through a combination of observing and participating during assessment and therapy sessions, general and specific written information, direct instruction,

The Centre for Allied Health Evidence (CAHE)
55
role play, and discussion.
The metalinguistic tasks constituent provides the parents and child opportunities to talk, think and learn about language, with an emphasis on the phonological levels.
Metalinguistic tasks training may include: Metaphonetic activities, Phoneme–grapheme correspondences, Activities involving phoneme segmentation for onset matching, Activities to increase word and rhyme awareness, Conceptualizing ‗sound ‘ and ‗word ‘ (or ‗name‘), Activities to increase awareness of sound patterns between words, Judgement of phonological correctness, Awareness of revisions and repairs, Lexical and grammatical innovations.
Phonetic production training is not counted as a phonological component per se, but it is considered theoretically coherent to include it in the model.
A balance of around 50:50 between listening and conceptual and speaking tasks is suggested to the parents.
Multiple exemplar training (minimal contrasts therapy and auditory bombardment) are performed within therapy sessions and for homework.
Some examples of multiple exemplar training include: „Point to the one I say‟, „Put the rhyming words with these words‟, „Say the word that rhymes with the one I say‟, „Give me the word that rhymes with the one I say ‟, „Tell me the one to give you‟, „You be the teacher, and tell me if I say these words the right way or the wrong way‟, „Silly sentences‟, „Shake-ups and match-ups‟, „Walk when you hear the two-steps‟
Homework is a crucial component
Breaks are planned as a necessary component of the therapy, accommodating to the gradual nature of phonological acquisition.
The first therapy appointment after a break includes a review assessment, and further therapy appointments are scheduled, as required.
Frequency/
intensity/
duration of service
provision:
Children attend with their parent(s) weekly for approximately 10 weeks, and then have about 10 weeks break from therapy attendance.
If children miss therapy appointments (due to illness, for example), additional appointments are arranged at the end of the series of 10 weeks, if necessary.
Overall, the 13 children averaged 10.6 months of therapy and 21 consultations.
Outcomes evaluation
(by disorder subtype
if possible):
At the probe (post-treatment) assessment, the 14 treated children showed accelerated improvement in their phonological patterns (Bowen‘s Severity Index) compared with the untreated eight, who did not.
A commensurate improvement in receptive vocabulary and Mean Length of Utterance in morphemes (MLUm) was not observed in either group, pointing to the specificity of the treatment.
The phonological patterns of seven of the 13 children available for follow-up to treatment completion were normal within 3–10 months of initial assessment (mean=7.4 months).
The other five children had normal phonology within 12–19 months (mean=15.8 months).

The Centre for Allied Health Evidence (CAHE)
56
In the ‗faster‘ group, the number of 50 minute consultations the children had ranged from 10 to 23 consultations (mean=16 consultations).
In the ‗slower‘ group, the children had 22 to 36 consultations before their phonology was age-appropriate (mean= 33 consultations).
Author’s conclusion:
A phonological therapy approach aims to facilitate age-appropriate phonological patterns through activities that encourage and nurture the development of the appropriate cognitive organization of the child‘s underlying phonological system. The rationale for this intervention model involves two aspects:
A theoretically based view of phonological acquisition as a complex developmental interaction between motoric, perceptual, conceptual, and cognitive-linguistic capacities and capabilities at the intrapersonal level
The development of such capacities and capabilities is facilitated by interpersonal communication experiences in the child‘s particular and immediate linguistic surroundings.
Reviewer’s
conclusion:
Although not an effectiveness study as such, this paper gives a good description of the PACT phonological therapy model.

The Centre for Allied Health Evidence (CAHE)
57
Summary of intervention program: PACT (Phonological Therapy)
Reference:
Bowen, C and Cupples, L 1999b, ‗A phonological therapy in depth: a reply to commentaries‘, International Journal of Language and Communication Disorders, vol. 34, pp. 65-38.
Country of
publication:
Australia (NSW)
Publication type
(include level of
evidence):
Case study (level IV)
Population:
One 4;5 year old child with moderately severe phonological disorder
Service setting:
Clinic-based individual therapy
Service delivery
model:
mother attended all clinic visits with child
homework 100% with mother
Speech book to preschool once per week, where teacher gave general encouragement and modelling
Frequency/
intensity/
duration of service
provision:
23 consultations (18 treatments, 5 assessments) over 10 months
Block 1: 11 consultations
Break 1: 8 weeks
Block 2: 11 consultations
Break 2: 10 weeks
Block 3: 1 consultation
Outcomes evaluation
(by disorder subtype
if possible):
Ceri was initially unintelligible to the clinician beyond the single word level and had velar fronting 100%, palatoalveolar fronting SFWF 100%, gliding of fricatives SIWI 87% and cluster reduction SIWI 100%, and a score of 4 in incidence category 5 (80-100%) at her initial assessment (age 4;5)
By age 5;3 no phonological deviations were present and she was discharged from therapy
In her first year at school, her reading was well advanced
Author’s conclusion:
This is no cookbook approach, but a model individually geared to individual children‘s specific needs, based on detailed and ongoing phonological analysis.
Reviewer’s
conclusion:
The main aim of this paper was to address and respond to ‗critics‘ comments regarding the PACT therapy model. In order to address these issues a successful case example was presented.
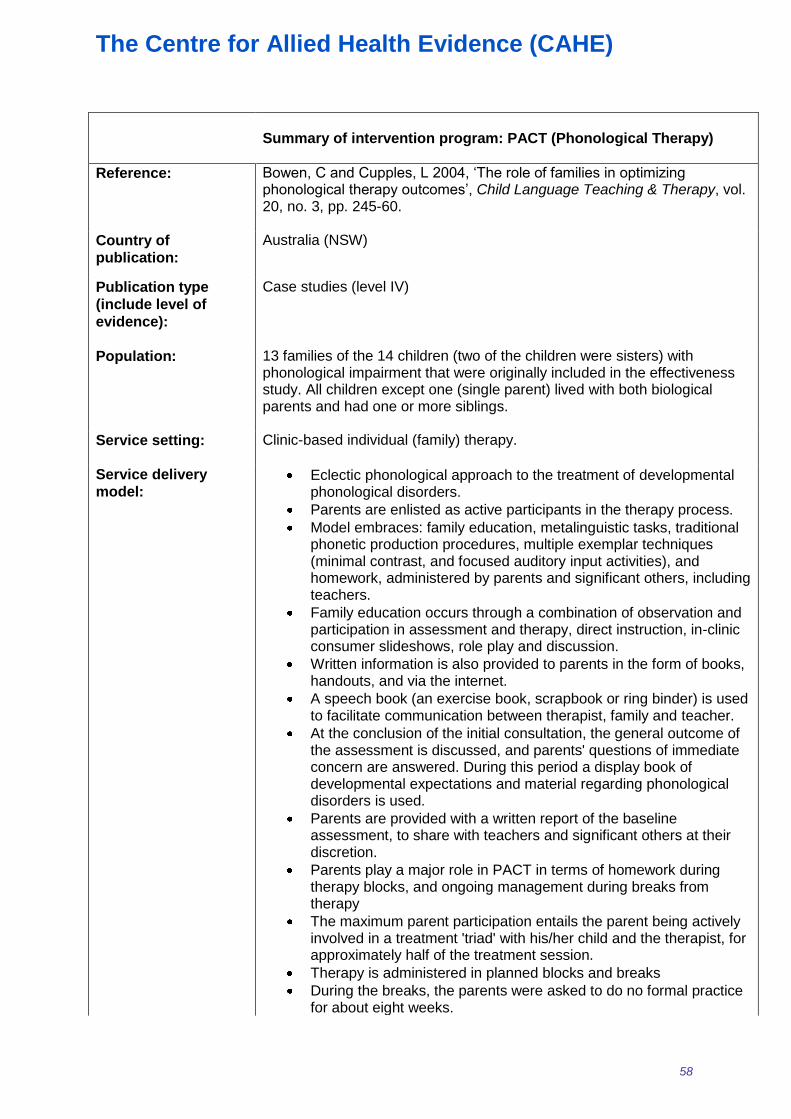
The Centre for Allied Health Evidence (CAHE)
58
Summary of intervention program: PACT (Phonological Therapy)
Reference:
Bowen, C and Cupples, L 2004, ‗The role of families in optimizing phonological therapy outcomes‘, Child Language Teaching & Therapy, vol. 20, no. 3, pp. 245-60.
Country of
publication:
Australia (NSW)
Publication type
(include level of
evidence):
Case studies (level IV)
Population:
13 families of the 14 children (two of the children were sisters) with phonological impairment that were originally included in the effectiveness study. All children except one (single parent) lived with both biological parents and had one or more siblings.
Service setting:
Clinic-based individual (family) therapy.
Service delivery
model:
Eclectic phonological approach to the treatment of developmental phonological disorders.
Parents are enlisted as active participants in the therapy process.
Model embraces: family education, metalinguistic tasks, traditional phonetic production procedures, multiple exemplar techniques (minimal contrast, and focused auditory input activities), and homework, administered by parents and significant others, including teachers.
Family education occurs through a combination of observation and participation in assessment and therapy, direct instruction, in-clinic consumer slideshows, role play and discussion.
Written information is also provided to parents in the form of books, handouts, and via the internet.
A speech book (an exercise book, scrapbook or ring binder) is used to facilitate communication between therapist, family and teacher.
At the conclusion of the initial consultation, the general outcome of the assessment is discussed, and parents' questions of immediate concern are answered. During this period a display book of developmental expectations and material regarding phonological disorders is used.
Parents are provided with a written report of the baseline assessment, to share with teachers and significant others at their discretion.
Parents play a major role in PACT in terms of homework during therapy blocks, and ongoing management during breaks from therapy
The maximum parent participation entails the parent being actively involved in a treatment 'triad' with his/her child and the therapist, for approximately half of the treatment session.
Therapy is administered in planned blocks and breaks
During the breaks, the parents were asked to do no formal practice for about eight weeks.

The Centre for Allied Health Evidence (CAHE)
59
Two weeks prior to the next treatment block, they were asked to read the speech book with the child a few times and to do any activities the child was interested in doing.
Throughout the breaks, they were to focus on providing modelling corrections, reinforcement of revisions and repairs, and metalinguistic activities, incidentally, as opportunities arose.
A three-page summary for therapists, teachers and consumers, of the components of PACT, and how to administer them is currently available at: http://members.tripod.com/CarolineBowen/pactsummary.pdf
Frequency/
intensity/
duration of service
provision:
Treatment sessions are usually of 50 minutes duration.
The child usually spends 30 to 40 minutes alone with the therapist.
The minimum amount of parent participation at the clinic involves the parent joining the therapist and child for 10 to 20 minutes at the end of a session, or 10 minutes at the beginning and 10 minutes at the end.
The first block and the first break are usually of approximately 10 weeks duration each, after which the number of therapy sessions per block tends to diminish, with the period between blocks remaining about the same.
All the children attended their appointments in the morning or early Afternoon (finishing no later than 3pm).
Parents administer homework in five to seven minute periods, once, twice or three times daily, five or six days a week.
Practice periods may be as little as 10 minutes apart, always in good listening conditions.
Outcomes evaluation
(by disorder subtype
if possible):
Therapy attendance and punctuality figures for all the children in the study were good.
Mothers reported that homework was done around 15 times per week on average, with a range from 8 times per week to 24 times per week.
According to self-report, the majority of homework (around 68.2%) was administered by mothers, but fathers also played a significant role, administering homework on the remaining 31.8% of occasions.
All the families reported that they did the homework as recommended and were compliant and consistent.
Author’s conclusion:
The PACT approach is a broad-based family-centred phonological therapy model that has already been shown to be effective in treatment of phonological disorder. We believe that the ways in which parents and significant others, including teachers, are involved in the therapy process make a key contribution to the efficacy and effectiveness of PACT.
Reviewer’s
conclusion:
Although difficult to determine directly from this paper, it appears that certainly part of the success of PACT may be related to the family focus of the intervention.

The Centre for Allied Health Evidence (CAHE)
60
Summary of intervention program: Core vocabulary vs. phonological contrast
Reference:
Crosbie, S, Holm, A and Dodd, B 2005, ‗Intervention for children with severe speech disorder: A comparison of two approaches‘, International Journal of Language & Communication Disorder, vol. 40, no. 4, pp. 467-92.
Country of
publication:
UK (research conducted in Qld, Australia)
Publication type
(include level of
evidence):
Multiple baseline cross-over comparative study (level III-1)
Population: 18 children aged between 4;8 and 6;5 years with moderate to severe phonological disorder. Children had an inconsistent speech disorder or a consistent speech disorder and normal oro-motor structure and skills, receptive language, non-verbal skills, hearing and were monolingual speakers of English.
Service setting: Clinic-based individual therapy.
Service delivery
model: An experienced paediatric speech–language pathologist assessed
each child in a quiet room at their school or preschool prior to treatment.
Two experienced paediatric speech language pathologists administered the intervention.
Each child received both intervention blocks from the same SLP.
In most cases one intervention session each week was provided at home and one session at school to allow the SLP to liaise with both parents and teachers.
Parents were asked to complete daily practice activities at home during the treatment blocks.
There was no revision during the withdrawal periods.
The Phonology and Inconsistency assessments from the DEAP were elicited at the end of each treatment block and again 8 weeks after the final assessment.
Phonological contrast therapy:
Error patterns were identified from analysis of the phonological assessment data.
An error pattern was selected for intervention according to the following criteria: targeting non-developmental patterns before developmental; consistency and frequency of the use of the error pattern; effect on intelligibility of successful remediation; and stimulability of the speech sounds required.
Each error pattern was targeted in four stages: auditory discrimination; production in single words; production in phrases (set and then spontaneous); and production in sentences within conversation.
A minimal pair approach (sometimes with multiple oppositions) was used to reorganize the child‘s phonological system.

The Centre for Allied Health Evidence (CAHE)
61
The first stage of the treatment was auditory discrimination.
The child was then required to start producing the minimal pairs, initially in imitation, and then spontaneously.
Feedback provided.
Core vocabulary therapy (targeting consistency of word production):
The child, parents and teacher selected a list of 50 words that were functionally ‗powerful‘ for the child.
Each week, ten words were randomly selected from the set of 50 target words.
The clinician established the child‘s best production of each target word.
The child‘s best production was achieved by teaching the word sound-by-sound, using cues such as syllable segmentation, imitation and cued articulation.
After the best production was established, the child was required to produce those ten words in the same way throughout the week.
The parents and teacher practiced the words daily with the child, and reinforced productions of those words in everyday communication situations.
The ten target words were revised in games and activities during the second weekly session with the SLP.
At the end of the second weekly session, the child was asked to produce the ten words three times.
Any words they produced consistently were removed from the list of 50 words.
Frequency/
intensity/
duration of
service provision:
Each child participated in 16 (30-minute) individual therapy sessions in two 8–9-week treatment blocks (either core vocabulary followed by phonological contrast or phonological contrast followed by core vocabulary) with a 4 week break in between.
Outcomes
evaluation (by
disorder subtype
if possible):
Insignificant difference between pre- and post-therapy scores for:
PCC following core vocabulary therapy
PCC following phonological contrast therapy
inconsistency score following core vocabulary therapy,
inconsistency score following phonological contrast therapy
Consistency of word production:
significant effect of therapy and subgroup (inconsistent speech disorder improved more than consistent speech disorder)
significant interaction between type of therapy and subgroup (core vocabulary resulted in greater change to consistency than phonological contrast therapy)
increased most for children with inconsistent speech through core vocabulary therapy.
changed more for children with consistent speech disorder when they received phonological contrast therapy.
Speech accuracy:
Significant effect of therapy (phonological contrast therapy was more effective in changing the PCC than core vocabulary

The Centre for Allied Health Evidence (CAHE)
62
therapy).
The effect of group was not significant
Significant interaction between the type of therapy and subgroup of speech disorder
Phonological contrast therapy was most effective in changing the PCC of children with a consistent speech disorder.
PCC of children with inconsistent speech disorder increased when they received core vocabulary therapy.
At 8 weeks post intervention:
no effect of assessment time (immediately following therapy versus
follow-up) or interaction between time of assessment and group
All children maintained the accuracy gains made during therapy.
no significant differences at follow-up between the subgroups of children
there were no order effects of treatment, with no significant differences between subgroups after phonological contrast therapy
Author’s
conclusion:
All the children increased their consonant accuracy during intervention. However, core vocabulary therapy resulted in greater change in children with inconsistent speech disorder and phonological contrast therapy resulted in greater change in children with consistent speech disorder. The results provide evidence that treatment targeting the speech processing deficit underlying the child‘s speech disorder will result in generalization. Core vocabulary therapy provided to children diagnosed with an inconsistent disorder resulted in consistent phonological output of both treated and untreated words. Similarly, phonological contrast therapy resulted in suppression of error patterns, not just remediation of targeted lexical items.
Reviewer’s
conclusion:
Children with inconsistent speech disorder may benefit more from core vocabulary training and children with consistent speech disorder may benefit more from phonological contrast therapy.

The Centre for Allied Health Evidence (CAHE)
63
Summary of intervention program: Early Childhood Educators (EEC) programme
Reference:
Coulter, L and Gallagher, C 2001, ‗Evaluation of the Hanen Early Childhood Educators Programme‘, International Journal of Language and Communication Disorders, vol. 36 (Suppl), pp. 264-9.
Country of
publication:
UK
Publication type
(include level of
evidence):
Comparative study (level III-2)
Population:
23 female staff employed in an Education and Library Board nursery and enrolled in an EEC programme. They had between 1-10 years experience in pre-school education. 30% had a professional teaching qualification, remainder were classroom assistants or NVQ students. 52 children aged 40-50 months who attended one of two randomly selected Education and Library Board nurseries that followed a common curriculum. Children were included regardless of whether they had an established diagnosis of speech and language delay/disorder or additional impairments.
Service setting:
Two Education and Library Board nurseries
Service delivery
model:
Hanen Early Childhood Educators (EEC) programme:
Provides teachers and learning support assistants with the knowledge and support they need to help children learn to communicate
Parent-focussed programme
Provide enriched interactive learning environment
Adults encouraged to adapt their language and interactive style to meed the needs of individual children
Frequency/
intensity/
duration of
service provision:
15 hours of group learning and individual video feedback sessions
Outcomes
evaluation (by
disorder subtype
if possible):
No statistically significant differences in children‘s receptive and expressive language ratings between the training and no training group at any time point
Statistically significantly higher subjective rating of children‘s social interaction skills in the training group over the no training group
No statistically significant difference between groups on all of the teacher checklists
Marked changes in staff confidence and skills following the programme
High satisfaction rating for the content of the programme
Increased staff awareness of their interaction styles
Less controlling questions, more modelling and commenting

The Centre for Allied Health Evidence (CAHE)
64
Author’s
conclusion:
There was no significant change in children‘s speech and language skills as a result of staff participating in an Early Childhood Educators Programme. There was a subjective improvement in children‘s social interaction skills however. There were positive changes in staff skill and knowledge levels following the programme.
Reviewer’s
conclusion:
A 15 hour education programme aimed at early childhood teachers and support workers appeared to improve awareness of interaction styles in the staff, however there was no improvement in children‘s speech or language skills following the programme.

The Centre for Allied Health Evidence (CAHE)
65
Summary of intervention program: Phonological Contrast vs. Core Vocabulary vs. PROMPT
Reference:
Dodd, B and Bradford, A 2000, ‗A comparison of three therapy methods for children with different types of developmental phonological disorder‘, International Journal of Language & Communication Disorders, vol. 35, no. 2, pp. 189-209.
Country of
publication:
UK/Australia
Publication type
(include level of
evidence):
Case series (level IV) with multiple baseline design (alternating treatments)
Population:
Three boys with moderate to severe phonological impairment aged between 3;5 and 4;3 years. All children had normal hearing, as tested within 6 months of participation in the intervention programme and mothers reported no current concerns. The subjects came from single income, two parent families of middle socioeconomic status. The mother was the primary care giver in all cases.
Service setting:
Clinic-based individual therapy.
Service delivery
model:
The children‘s baseline speech, language and oro-motor skills were assessed by an experienced speech–language therapist in a quiet clinic room.
Treatment 1 was implemented after the initial assessment, followed by a 3-week withdrawal period, Treatment 2, withdrawal, then Treatment 3 (the order of treatments was random).
For home follow-up, parents repeated the activities observed in the most recent therapy sessions using the same target words or contrasts focused on in therapy.
There was no revision during the breaks.
A final assessment occurred three weeks after the final treatment session.
Phonological contrast therapy (targeting phonological processes):
A single phonological rule was chosen based on phonological analysis of the connected and elicited speech samples.
Criteria for phonological process target selection included: stimulability of speech sounds required; the relative effect on intelligibility of successful remediation of different processes; normal developmental sequence maintained; targeting deviant before developmental processes and consistency of use of the rule.
Rules that were not frequently used were considered poor candidates for this approach because remediation would be likely to have a limited effect on overall accuracy.
Target minimal pairs/triplets were used in a standard Metaphon programme.
Core vocabulary therapy (targeting consistency of word production):
Parents selected words that were powerful or useful for the subject
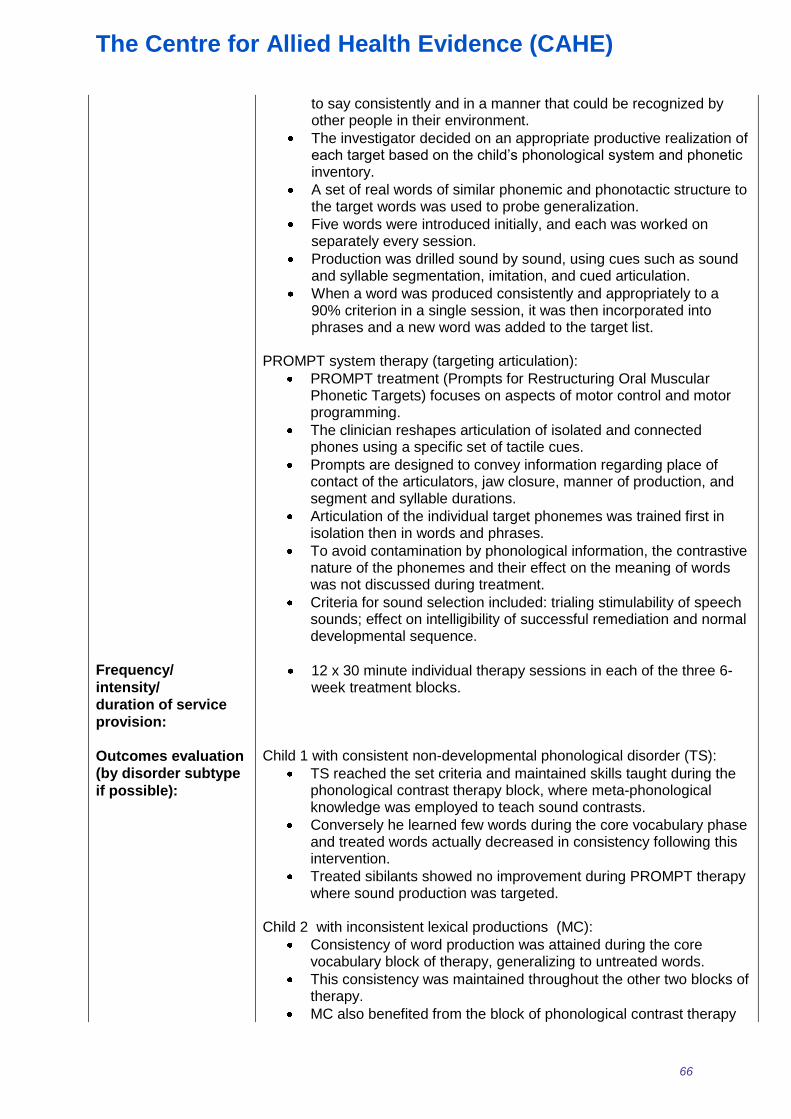
The Centre for Allied Health Evidence (CAHE)
66
to say consistently and in a manner that could be recognized by other people in their environment.
The investigator decided on an appropriate productive realization of each target based on the child‘s phonological system and phonetic inventory.
A set of real words of similar phonemic and phonotactic structure to the target words was used to probe generalization.
Five words were introduced initially, and each was worked on separately every session.
Production was drilled sound by sound, using cues such as sound and syllable segmentation, imitation, and cued articulation.
When a word was produced consistently and appropriately to a 90% criterion in a single session, it was then incorporated into phrases and a new word was added to the target list.
PROMPT system therapy (targeting articulation):
PROMPT treatment (Prompts for Restructuring Oral Muscular Phonetic Targets) focuses on aspects of motor control and motor programming.
The clinician reshapes articulation of isolated and connected phones using a specific set of tactile cues.
Prompts are designed to convey information regarding place of contact of the articulators, jaw closure, manner of production, and segment and syllable durations.
Articulation of the individual target phonemes was trained first in isolation then in words and phrases.
To avoid contamination by phonological information, the contrastive nature of the phonemes and their effect on the meaning of words was not discussed during treatment.
Criteria for sound selection included: trialing stimulability of speech sounds; effect on intelligibility of successful remediation and normal developmental sequence.
Frequency/
intensity/
duration of service
provision:
12 x 30 minute individual therapy sessions in each of the three 6-week treatment blocks.
Outcomes evaluation
(by disorder subtype
if possible):
Child 1 with consistent non-developmental phonological disorder (TS):
TS reached the set criteria and maintained skills taught during the phonological contrast therapy block, where meta-phonological knowledge was employed to teach sound contrasts.
Conversely he learned few words during the core vocabulary phase and treated words actually decreased in consistency following this intervention.
Treated sibilants showed no improvement during PROMPT therapy where sound production was targeted.
Child 2 with inconsistent lexical productions (MC):
Consistency of word production was attained during the core vocabulary block of therapy, generalizing to untreated words.
This consistency was maintained throughout the other two blocks of therapy.
MC also benefited from the block of phonological contrast therapy

The Centre for Allied Health Evidence (CAHE)
67
where gliding was eliminated for treated words, although generalization to untreated words was more limited.
MC did not benefit from the PROMPT therapy approach. Child 3 with inconsistent lexical productions (TN):
TN benefited from the core vocabulary block of therapy.
Consistency of production of both treated and untreated items was increased and that gain was maintained.
In contrast, neither of the other two therapy blocks led to improvement.
Author’s conclusion:
The child with deviant consistent phonological disorder benefited most from the phonologically based intervention whereas the core vocabulary approach resulted in increased consistency of production for the two children with inconsistent speech disorder. The two children with inconsistent speech disorder responded differently to the three treatments however, and this may be a result of child specific factors (e.g. other abilities, family situation); disorder characteristics (more detailed examination of speech error patterns might reveal differences between children); target of therapy choice; length of block; and sequencing of therapeutic approaches. Clinically there is a need for thorough assessment of all children who present with developmental speech disorders. The results of this investigation indicate that different parts of the speech processing chain may respond to various types of treatment that target different links in the chain: articulation of phones, contrastive use of phonemes, and consistent production of words. Just as no single treatment approach is appropriate for all children with disordered phonology, management of some children with speech disorder may not simply involve choosing one appropriate intervention approach, but selecting and sequencing a range of approaches to address different underlying deficits.
Reviewer’s
conclusion:
Appropriate treatment requires thorough assessment of children‘s speech disorder, and several approaches may be required to address the varying deficits. Children with consistent phonological disorder may benefit from initial phonologically based intervention whereas children with inconsistent speech disorder may benefit initially from a core vocabulary approach. Careful assessment and monitoring should ensure that each child is receiving the optimal treatment.

The Centre for Allied Health Evidence (CAHE)
68
Summary of intervention program: “You make the difference”
Reference:
Dowd, T, Withers, E, Hackwood, J and Shuter, P 2007, ‗An Australian pilot study of a parent-child interaction program - You make the difference‘, Neonatal, Paediatric & Child Health Nursing, vol. 10, no. 1, pp. 13-9.
Country of
publication:
Australia
Publication type
(include level of
evidence):
Case study (level IV)
Population:
11 mothers and their infants aged 6 months-2.5 years from local community groups. All were ―Anglo-Saxon‖ or ―Celtic‖ except for one who was of Torres Strait Islander descent. Nine were first time mothers.
Service setting:
Community-based group parent-child therapy.
Service delivery
model:
―You make the difference‖ (YMTD) Parent-child interaction programme:
A Hanen strategy
Part of a larger community-based Play and Talk health promotion strategy
Run by speech pathologist who was an accredited YMTD facilitator and a community worker
Aims to lessen the demand on speech pathology services by supporting the re-orientation of such services towards early intervention and prevention of early childhood communication problems
Parents are key facilitators in enhancing child language development
Experiential training processes are the most effective way to promote communication development
Optimal language competency will develop as a consequence of language interactions in the child‘s everyday activities
The skills of parents in facilitating language development can be easily integrated into a wide range of routine daily activities
Targets children without an identified communication problem, but who may be at risk of a communication problem
Instructional and experiential education programme designed to enrich parent-child interaction as part of an overall prevention strategy
Help parents engage in mutually satisfying interactions with their child to help children learn in naturalistic settings
Designed for parents of children up to 4 years of age
Step-by-step guidelines based on the 3A‘s: allowing the child to lead; adapting to share the moment; adding information and ideas
Short video clips of parent-child interactions are played at the beginning of each session
Time is allowed at the end of each session to discuss and practice the application of the 3A‘s to everyday situations
A different toy is used during the videotaping practice and taken home each week

The Centre for Allied Health Evidence (CAHE)
69
Frequency/
intensity/
duration of service
provision:
Minimum of 8 weekly interactive group sessions for up to 10 parents with individual videotaping of parents interacting with their children and coaching from a facilitator
Outcomes evaluation
(by disorder subtype
if possible):
All mothers agreed their communication and interaction with their children improved beyond their expectations
Mothers allowed their child to lead and tuned into their child‘s level of communication and interaction
All advocated that the programme should be widely promoted and recommended follow up groups to provide ongoing support
Journal notes of the speech pathologist and community development worker supported these findings
Author’s conclusion:
The overall positive outcome of the ―You make the difference‖ programme highlights the need to provide accessible, community-based programmes to support the critical role of parents as facilitators of communication development in very young children. YMTD is now being implemented across the state.
Reviewer’s
conclusion:
There were positive signs of improved parent-child interaction as a result of this Hanen based ―You mean the difference‖ parent-training however further evaluation is required to determine whether it leads to improved communication outcomes for the children.

The Centre for Allied Health Evidence (CAHE)
70
Summary of intervention program: Parent interaction training
Reference:
Feldman, M, Sparks B and Case, L 1993, ‗Effectiveness of home-based early intervention on the language development of children of mothers with mental retardation‘, Research on Developmental Disabilities, vol. 14, no. 5, pp. 387-408.
Country of
publication:
Canada
Publication type
(include level of
evidence):
Randomised controlled trial within a case-control study (level III-2)
Population:
28 mothers independently diagnosed as mentally retarded and all were primary care providers for their children. The children of the mothers were aged 5 to 28 months and none had any known physical contraindications for normal growth and development. Upon entering the program, 16 children were already showing delays (i.e., scoring < 1 SD below the mean on the Bayley Scales of Infant Development, Mental Development Index; BSID-MDI). Before their involvement in this study, seven of nine mothers who had a previous child had that child taken into custody because of documented neglect (n = 2), physical abuse (n = I), or workers‘ concerns about parenting competency (n = 4). Moreover, nine mothers were currently under the court-ordered supervision of a child-protection agency.
A mixed comparison group of 38 mothers of low to high socioeconomic status without mental retardation, whose parenting skills were not of concern, was included for social comparison of pre- and post-intervention mother-child interaction and child language scores and to establish realistic training goals. The comparison children ranged in age from 4 to 46 months and based upon the reports of the observers and the mothers, all these children were developing normally.
Service setting:
Home-based individual treatment.
Service delivery
model:
For pre-, post- and follow-up observations, the mother-child dyad was observed in its home; the play sessions were not formally structured, and the mothers were simply asked to ―play with your child the way you usually do.‖
No further instructions or training were provided during these probes, which lasted approximately 10 min; a 10-s observe, 10-s record, partial interval time sampling procedure was employed.
Interaction Training:
Provided by 5 women with undergraduate degrees in psychology or early childhood education and 3 to 8 years experience.
Each family had a consistent trainer for the duration of the study.
Before their involvement in this study, the parent trainers had received instruction (readings, discussions, modelling, and feedback) over 1 month in the clinical and research skills needed to work with at-risk families, young children, and parents with cognitive limitations.

The Centre for Allied Health Evidence (CAHE)
71
Sessions were scheduled weekly in the family home in the play context and consisted of verbal instruction and discussion, modelling, feedback, and reinforcement.
Interaction training was considered the focus of the session.
The sequence of training was imitation, then praise, followed by physical affection.
The therapists also gave mothers recommendations on play activities that matched the child‘s developmental level and provided toys on loan if the parents did not own appropriate toys.
The actual training session consisted of the trainer first describing the interactional skill to be taught and why it is important for the mother to learn (e.g., ―just like us, children like to be praised when they do something well‖).
The trainer would model the skill several times with the mother‘s own child and then asked the mother to try it.
Immediately following the completion of a training session, the therapist gave the general prompt to the mother ―play with your child the way you usually do‖ and observed for the occurrence of the trained skills.
Following completion of the training session, the therapist would also give intermittent verbal feedback to the mother on the skills trained that day if observed to occur spontaneously during the remainder of the visit.
Once mothers performed at least 30% correct on each skill they received tokens that could be exchanged for small gifts and a new skill was added to the training session.
Attention control:
Home visits with the attention-control group members were designed to duplicate in as many ways as possible the experiences of the interactional training group, except that the control group received training in home safety and emergency skills.
Training in safety and emergency skills was the priority.
Used the same instructional strategies as interaction training described above (i.e., discussion, modelling, feedback, coupon reinforcement).
The mothers in the attention-control group were also: (a) asked to play with their children, (b) given advice on play activities to match the developmental level of their child, and (c) loaned child age-appropriate toys.
No training was provided on any of the interaction skills to the control group during the training phase.
The mothers were observed playing with their children following being asked to ―play with your child the way you usually do.‖
After the posttests, interaction training was offered to the mothers in the attention-control group; eight mothers accepted.

The Centre for Allied Health Evidence (CAHE)
72
Frequency/
intensity/
duration of service
provision:
Weekly 60-minute sessions in the home (the amount of time actually spent on training was about 10 min).
Mean 21 home visits for the interaction training and 24 visits for the attention control training.
Outcomes evaluation
(by disorder subtype
if possible):
Both the mothers and the children in the training group scored significantly higher than the attention-control group on all the post-tests (total maternal interactions, imitation of child vocalizations, praise, physical affection, talking to child, child vocalizations, and child verbalizations).
The children of the training group mothers began to verbalize at an earlier age than the age matched children of the attention-control group mothers.
The training group mothers had significantly more total interactions, praise, imitation of vocalizations, physical affection, and talking to their children than the attention-control group mothers.
The training group mothers showed significantly more total interactions, imitation, praise, and physical affection with their children than the normative comparison group mothers, but talking was not significantly different.
The attention-control group mothers had significantly less imitation, praise, and talking to their children than the normative comparison group mothers, but physical affection and total interactions were not significantly different.
The children of the training group mothers vocalized and verbalized significantly more than the children of the attention-control group mothers.
There were no significant differences between the children of the training group mothers and the children of the normative group mothers on the occurrence of vocalizations and verbalizations.
The children of the attention-control group mothers verbalized significantly less than the children of the normative comparison group mothers, but there were no significant differences in occurrence of vocalizations.
8 of the 14 mothers in the training group were followed up for 13-82 weeks following training:
The remaining members of the interaction training group generally maintained their skills.
The difference between the pretest and follow-up scores of the training group was significant on all measures except physical affection and talking to the child.
The training group posttest and follow-up scores were significantly different on only child vocalizations, which continued to increase from the posttest score.
Upon receiving interaction training, the eight remaining members of the attention-control group replicated the results of the first training group.
Author’s conclusion:
Home-based parent-child interaction training significantly increased the responsive and reinforcing interactions of mothers with mental retardation, which resulted in significant increases in the emergent language performance of their infants and toddlers. The improvements in child language appeared to be a function of increased quality rather than just

The Centre for Allied Health Evidence (CAHE)
73
quantity of mother-child verbal interactions.
Reviewer’s
conclusion:
Although not specifically a speech and language therapy programme, this parent-child interaction training programme appeared to lead to improved communication outcomes for the children of mentally-retarded mothers.

The Centre for Allied Health Evidence (CAHE)
74
Summary of intervention program: Grammar facilitation (therapist-administered vs. parent-administered)
Reference:
Fey, M, Cleave, P, Long, S and Hughes, D 1993, ‗Two approaches to the facilitation of grammar in children with language impairment: an experimental evaluation‘, Journal of Speech & Hearing Research, vol. 36, no. 1, pp. 141-57.
Country of
publication:
USA
Publication type
(include level of
evidence):
Randomised clinical (three-tier) trial (level II)
Population:
30 children aged 3;8-5;10 years who had marked delays in grammatical development.
Service setting:
Home based parent administered individual therapy and combination of clinician administered clinic-based therapy and home visits.
Service delivery
model:
A speech-language pathologist with master‘s degree and 2 years post-masters experience conducted all clinician and parent training
Five general principles: intensive; reasonable clinician time costs; programmes based on similar goal setting principles, goal-attack strategies, and procedures; procedures had to be useable in the context of play settings, activities of daily living, and typical pre-school activities; parent treatment reflected a smaller clinician time commitment than if the clinician were to provide the treatment
Each child had a set of 4 specific goals
New specific goals were introduced gradually, one at a time
Parent-administered
4-6 parents and their children participated
Parent training sessions and regular parent meetings
Project speech-language pathologist made 3 home visits during the 12-week training phase to observe, provide feedback, and demonstrate where necessary
Monthly clinic visits for parent and child
No interventionist-oriented activity such as prompts for imitation as in the clinician group
Clinician-administered:
4-6 children in a group
Individual and group therapy
Each individual session began with a highly structured activity that involved imitation of the target for the week as well as of a language form that was contrastive to the target (approx 10 minutes of session)
Delayed treatment (control) group:
Received treatment at the end of the study

The Centre for Allied Health Evidence (CAHE)
75
Frequency/
intensity/
duration of service
provision:
Intervention programme lasted 4 ½ months Parent-administered:
2 hour parent training session
Parent meetings once weekly for the first 12 weeks of the programme and once monthly for the remaining 2 months
Monthly one-hour clinic visit Clinician-administered:
One-hour individual session per week
Two x one-hour group sessions per week
Outcomes evaluation
(by disorder subtype
if possible):
DSS:
Both clinician- (p=0.0005, effect size=0.81) and parent-administered treatment groups (p=0.0001, effect size=0.96) scored significantly higher than the delayed-treatment group
Small non-significant difference between the 2 treatment groups
Delayed treatment group made no gains over the waiting period Main Verb score per sentence:
Both treatment groups again performed significantly better than the delayed-treatment group (clinician vs. delayed p=0.004; parent vs. delayed p=0.04), however there was no difference between the two treatment groups
Personal pronouns:
Lack of treatment effect (p=0.64)
Percentage of sentences receiving a sentence point:
Both treatment groups again performed significantly better than the delayed-treatment group (clinician vs. delayed p=0.0005; parent vs. delayed p=0.03), however there was no difference between the two treatment groups
Overall:
More consistent DSS; Main Verb score per sentence; and Percentage of sentences receiving a sentence point gains in the clinician group, whereas the gains in the parent group were distributed bi-modally, with some showing small gains, and others showing large gains
Author’s conclusion:
Two treatment packages using focussed stimulation procedures, but differing in that one was administered by trained parents, and the other was administered by a clinician both resulted in significant gains in grammatical expression after 4 ½ months treatment, when compared to a waiting list control group receiving no treatment.
Reviewer’s
conclusion:
Both parent and clinician provided focussed stimulation appeared to be more effective than no treatment in improving grammatical expression in children with marked delays in grammatical development.

The Centre for Allied Health Evidence (CAHE)
76
Summary of intervention program: Parental-based speech and language therapy
Reference:
Gibbard, D 1994, ‗Parental-based intervention with pre-school language-delayed children‘, European Journal of Disorders Communication, vol. 29, no. 2, pp. 131-50.
Country of
publication:
UK
Publication type
(include level of
evidence):
Study 1 Comparative study (level III-2) Study 2 Comparative study (level III-2)
Population:
Study 1 36 children aged 2;3-3;3 years that had been referred to a speech and language therapy department at a local health centre. All had a vocabulary of fewer than 30 words, did not have general developmental delay, or any other medical condition indicative of language delay/disorder and had not previously received speech and language therapy. 18 mothers participated in the parent training. Study 2 25 children aged 2;3-3;3 years that had been referred to a speech and language therapy department at a local health centre. All had a vocabulary of fewer than 30 words, did not have general developmental delay, or any other medical condition indicative of language delay/disorder and had not previously received speech and language therapy. 17 mothers participated in the parent training.
Service setting:
Community health centre (group therapy).
Service delivery
model:
Pre-test conducted including full history and formal/informal assessments
Post-test included repetition of all formal and informal tests Study 1
Experimental group:
Mothers (primary carers) attended group speech and language therapy training sessions at a health centre
Fortnightly objectives were set for the parents to work on, with methods and games suggested
Emphasis on transferring linguistic skills achieved during these games to daily life situations
Many sessions included small group activity, with mothers working in groups of three to devise a new game or activity for achieving a particular objective
A structured teaching method was demonstrated
Main treatment objective was to increase the child‘s linguistic complexity from a single word level to three- to four-word utterances

The Centre for Allied Health Evidence (CAHE)
77
Control group:
No intervention Study 2 Parental Language group:
Indirect parental-based group treatment using specific language objective and activities
Identical to experimental group in study 1 Parental Control group:
Indirect parental-based group treatment using non-specific cognitive tasks unrelated directly to speech and language therapy
Fortnightly objectives were set during the group sessions for the mothers to work on with their children at home
Games and methods to work on these skills were suggested and explained
All objectives were chosen to teach cognitive skills other than language development and were based on skills taught as part of the ‗Portage Scheme‘
Individual group:
Direct speech and language therapy on a one-to-one basis
Children formed a part of the clinician‘s caseload
Parents received general advice on the aims of the sessions and strategies used to achieve them
Frequency/
intensity/
duration of service
provision:
All parental-based group treatments:
11 x 1 hour sessions once a fortnight over 6 months Individual one-on-one therapy (comparison group study 2):
Weekly 30 minute sessions over 6 months
Outcomes evaluation
(by disorder subtype
if possible):
Study 1:
Taking into account non-significant differences between the experimental and control groups pre-therapy, the experimental group demonstrated significantly greater gains in children‘s expressive language skills
Study 2:
Post-therapy, the parental language group generally obtained the highest mean scores for all outcomes, followed by the individual group and then the parental control group
Statistical analysis revealed that differences in post-therapy scores were significant for some measures but not others
Parental language therapy was at least as effective and direct, individual speech and language therapy, and gains tended to be higher in the parental language group, although these were only significant for one outcome (mean length of utterance)
The parental language therapy group made consistently significantly greater language gains than the parental control group
The individual therapy group made greater language gains than the parental control group, however these were only significant for

The Centre for Allied Health Evidence (CAHE)
78
mean length of utterance and Derbyshire total scores
Author’s conclusion:
Substantial language gains can be achieved in young children with expressive language delay by working through their parents. The language gains produced from parental group therapy are comparable with direct individual treatment from a speech and language therapist. Group therapy may be cheaper to provide with no loss of effectiveness, and because an increased number of children may receive intervention as soon as it is required, waiting times could be reduced.
Reviewer’s
conclusion:
Parental group training was found to be at least as effective as individual one-on-one therapy provided directly by a speech and language therapist.

The Centre for Allied Health Evidence (CAHE)
79
Summary of intervention program: Phonological Awareness Training
Reference:
Gillon, GT 2005, ‗Facilitating phoneme awareness development in 3- and 4-year-old children with speech impairment‘. Language Speech and Hearing Services in Schools, vol. 36, pp. 308–324.
Country of
publication:
New Zealand
Publication type
(include level of
evidence):
Study 1 Case-control study (level III-2) Study 2 Comparative study with historical control (level III-3)
Population:
Study 1 12 children with speech impairment aged 3;0-3;11 years. The children appeared to have specific speech difficulties that required further assessment. The children had speech difficulties in the absence of diagnosed sensory, neurological, physical, or intellectual disabilities and a moderate or severe speech delay but receptive vocabulary knowledge within or above the normal range. 19 children with typically developing speech and language skills participated in the control group (mean age = 41.89 months). Study 2 10 children in the experimental group from study 1 remained in the study (now aged on average 6 years) and were compared to a matched historical control group of children with speech impairment on phonological awareness, word recognition, spelling, and non-word reading measures. Children in the control group had not received phonological awareness intervention during their preschool and school program.
Service setting:
Clinic-based (individual and group) therapy
Service delivery
model:
All of the children were administered the rhyme and phoneme tasks on three assessment periods (at approximately a 7–8-month interval) between the ages of 3–5 years (T1, T2, and T3) in study 1
Children were assessed at 6 years of age in study 2 Experimental group:
Two or three blocks of therapy between the ages of 3 and 5 years, with their first block of therapy being implemented following their initial assessment at 3 years of age
Number of blocks received depended on the children‘s speech production needs
Individual and group sessions with 2 or 3 other children participating in the study
Children‘s primary caregiver usually attended the sessions but acted in a support role only (i.e., they were not specifically trained to implement the therapy procedures at home)
All of the therapy sessions were administered at the university‘s speech

The Centre for Allied Health Evidence (CAHE)
80
and language therapy clinic
The researcher, or a qualified SLP trained by the researcher, administered all of the group sessions.
These sessions were conducted in a clinic room that was fitted with a soundfield system to provide optimal listening conditions
A senior speech-language therapy student administered the individual sessions under the supervision of a qualified SLP who was trained on program content
Children continued to receive their regular early childhood education program at their kindergarten or preschool
Each treatment session targeted three areas: o improvement of the child‘s speech intelligibility (Cycles
Phonological Remediation Approach) o facilitation of phonological awareness at the phoneme level o letter-name and letter-sound knowledge
Control group:
Exposed to the same types of early education program at their kindergarten or preschools as the children in the experimental group and received no other type of educational intervention during the study
Frequency/
intensity/
duration of service
provision:
Each block of therapy (which typically lasted between 4–6 weeks depending on the availability of children and therapists) followed the same model: two 45-min therapy sessions per week consisting of one group and one individual session each week.
The average number of therapy sessions received by the children before school entry was 25.5 sessions
Outcomes evaluation
(by disorder subtype
if possible):
Study 1:
A significant time effect for rhyme oddity; phoneme matching; and letter recognition (group‘s average performances improved at each assessment time
No significant interaction between time and group for rhyme and letter recognition (both experimental and control group of normally developing peers improved similarly over time)
The interaction between assessment time and group for the phoneme matching task was significant (there was a significant group difference at T1 but not T2 or T3 with experimental group making significantly more gains than control group at T1 only)
Significantly more children in the experimental group than the control group demonstrated competency at 70% correct or better in phoneme matching
Performance on the Phonological awareness standardized test close to school entry at 5 years of age and up to one year after starting school was no different between the experimental or control groups
Descriptive statistics showed rapid growth in speech production during the first 8–12 months of the study for the children with speech impairment
The speech performance of the children with speech impairment at 5 years of age was significantly inferior to the control group of children‘s speech performance at study entry when they were only aged 3;5
Study 2:
The performance of children in the experimental group was superior to

The Centre for Allied Health Evidence (CAHE)
81
that of the children in the historical control group on the following measures: phonological awareness score, word recognition performance; non-word reading performance; and spelling performance
No significant group differences in current-age, speech production abilities, or letter-sound knowledge
The majority of children (n = 7) in the control group were identified as being at risk, with only 2 children performing within the average range on all subtests
Whereas the majority of children (n = 6) in the experimental group performed within or above the average range on all subtests, with 2 children identified as being at risk.
All of the children with speech impairment who received phonological awareness intervention in their preschool years were reading at or above the expected level for their age.
In contrast, the majority of children in the control group showed delayed development in word recognition
Author’s conclusion:
The findings from this study suggest that strong phonological awareness skills at the phoneme level are indeed a critical factor in determining successful early reading and spelling experiences for children with speech impairment. Despite a history of moderate or severe speech impairment and a known risk factor of commencing literacy instruction with persistent speech impairment, the children in the experimental group demonstrated average or well above average reading performance in their first or second year at school. They also demonstrated strong early spelling knowledge. Early intervention that is aimed specifically at facilitating phoneme awareness and letter knowledge in addition to improving speech intelligibility contributed to these children‘s strong phoneme awareness development and subsequent success at decoding and encoding the printed word. The study results provide valuable evidence to support the clinical practice of integrating phoneme awareness and letter knowledge activities into therapy sessions for 3- and 4-year-old children who have speech impairment.
Reviewer’s
conclusion:
Although children with moderate to severe speech impairment made gains in the first 8 months, they remained well below their normally developing peers at age 5. The children also made more gains than a historical control group up to age 6, however given the nature of the study it is not possible to determine whether this was due solely to the intervention.

The Centre for Allied Health Evidence (CAHE)
82
Summary of intervention program: Interactive focussed stimulation (Hanen therapy)
Reference:
Girolametto, L, Pearce, P and Weitzman, E 1996, ‗Interactive focused stimulation for toddlers with expressive vocabulary delays‘, Journal of Speech and Hearing Research, vol. 39, no. 6, pp. 1274-83.
Country of
publication:
Canada
Publication type
(include level of
evidence):
Comparative study (level III-2)
Population:
25 toddlers aged 23-33 months with expressive vocabulary delays and their mothers. All children were at the single word stage of language development and spoke English at home. None had major sensory impairments, oral motor problems, frank neurological impairments, PDD or autism.
Service setting:
Clinic-based group parent training and individual home visits
Service delivery
model:
Pre-testing on 2 sessions x 1.5 hours each
Post-testing 3 weeks after end of intervention on 2 occasions x 1.5 hours each
Experimental group:
Indirect therapy (via parents)
Hanen Programme for Parents was administered by 2 experienced and Hanen-certified speech-language pathologists
A parent associate who had a child with language delay and had completed a programme assisted with administration
Evening sessions were to teach programme strategies using videotapes, participative lectures, role plays and focussed discussions
Home practice was assigned and reviewed at the beginning of the subsequent session
Home visits provided individual feedback to parents regarding their own and their child‘s progress
Interactions were videotaped and played back to provide feedback and on-the-spot coaching was provided as appropriate
The content of the Hanen programme was adapted to include 3 modifications consistent with a focussed stimulation approach: 10 target words introduced during the 2nd evening session; parents trained to select lexical targets once child had used it spontaneously; during final evening session parents were taught to model two-word combinations
Control group:
No intervention offered over the 4 months
Delayed treatment offered after this period
Frequency/ 8 x 2.5 hour evening sessions and three home visits over 11 weeks

The Centre for Allied Health Evidence (CAHE)
83
intensity/
duration of service
provision:
Outcomes evaluation
(by disorder subtype
if possible):
Mother‘s outcome:
Significant multivariate group x treatment interaction associated with total number of utterances and words per minute by mothers however only one significant finding on univariate analysis: mothers in experimental group used fewer words per minute than the control group
A significant multivariate group x treatment interaction for mother‘s mean length of utterance in morphemes (MLU) and type-token ratio (TTR) however only MLU was significant in univariate analysis
After treatment mothers in experimental group used significantly shorter utterances than mothers in the control group
A significant multivariate group x treatment interaction for mother‘s use of labels
Univariate analysis revealed mothers in the experimental group used a greater number of target words in their play interactions and used more focussed stimulation of target words than mothers in control group
Children‘s outcome:
Significant group x treatment multivariate analysis for 4 vocabulary measures (parent report of vocabulary size on the CDI; total number of different words used in interaction; number of different words used in interaction; number of different control words used in interaction)
Univariate analysis revealed: children who received intervention had larger vocabularies; used a greater number of different words (and target words) in interactions and learnt more of the untreated (control) words than children in the control group
Semi-structured probes confirmed the results listed above
No multivariate interaction of group x treatment for children‘s talkativeness
A significant multivariate interaction of group x treatment for Structural Complexity subscale of CDI and number of multiword combinations used in 30 minutes, with univariate analysis revealing that children receiving intervention using more structurally complete utterances and more multi-word utterances than children in the control group
Author’s conclusion:
This study demonstrated that mothers adopted the language-modelling techniques recommended by the focussed stimulation intervention. The results for children overwhelmingly support the short-term efficacy of early intervention for children with expressive vocabulary delays. Children in the experimental group made developmental gains in vocabulary, the use of multi-word phrases, and grammatical complexity over and above maturational changes in the control group that received no treatment. The focussed stimulation version of the interactive model appears to be a viable method for late talkers who are active conversationalists with delays in expressive vocabulary and language development.
Reviewer’s Indirect therapy provided by parents who are trained by speech-language

The Centre for Allied Health Evidence (CAHE)
84
conclusion:
pathologists may be an effective method of intervention for young children with expressive language delay.
The Centre for Allied Health Evidence (CAHE)
85
Summary of intervention program: Interactive focussed stimulation (Hanen therapy)
Reference:
Girolametto, L, Pearce, PS, & Weitzman, 1997, ‗Effects of lexical intervention on the phonology of later talkers‘. Journal of Speech, Language, and Hearing Research, vol. 40, no.2, pp. 338-348.
Country of
publication:
Canada
Publication type
(include level of
evidence):
Comparative study (level III-2)
Population:
25 toddlers aged 23-33 months with expressive vocabulary delays and their mothers. The children were at single word level stage of language development and all spoke English at home. None had major sensory impairments, oral motor problems, frank neurological problems or pervasive developmental disorder.
Service setting:
Clinic-based group parent training and individual home visits
Service delivery
model:
Pre-test over 2 sessions of 1.5 hours each
Post-test conducted 3 weeks following experimental programme, also 2 x 1.5 hour sessions
Experimental group:
Hanen programme for Parents
Administered by two experienced speech-language pathologists (both certified by the Hanen Centre) and a parent associated who had a child with language delay and had completed a programme
Evening sessions to teach programme strategies
Parents observed videotapes illustrating programme techniques and engaged in participative lectures, role plays and focussed discussions
Home practice assigned and reviewed at the beginning of subsequent sessions
Home visits to provide parents with individual feedback
Mothers videotaped interacting with their child, and these were reviewed to provide feedback
The content of the Hanen programme was adapted to include 3 modifications consistent with a focussed stimulation approach: 10 target words introduced during the 2nd evening session; parents trained to select lexical targets once child had used it spontaneously; during final evening session parents were taught to model two-word combinations
Control group:
No intervention
Received intervention after the study was completed

The Centre for Allied Health Evidence (CAHE)
86
Frequency/
intensity/
duration of service
provision:
8 x 2.5 hour evening sessions and 3 home visits over 11 weeks
Outcomes evaluation
(by disorder subtype
if possible):
No significant group x treatment interaction for number of vocalisations
Significant multivariate group x treatment interaction for children‘s syllable levels (when analysed together), however only significant univariate group x treatment interaction for level 3 vocalisations
Therefore the children in the experimental group made greater gains in their use of level 3 vocalisations than children in the control group
Significant multivariate group x treatment interaction for the three consonant inventories
Follow up univariate analysis revealed children in experimental group used a greater inventory of consonants in all three classes, and greater number of different consonants in both syllable-initial and syllable-final positions
No significant difference attributable to treatment between the two groups for percent consonants correct
Author’s conclusion:
This study suggests that targeting vocabulary in a group of late talkers can have an indirect effect on their emerging phonological skills. Toddlers who received 4 months intervention focussing on lexical targets made treatment gains in syllable structure and consonant inventory. They used a greater variety of complex word and non word syllable shapes and expanded their speech sound inventories to include more consonant sounds. Children‘s speech intelligibility or production accuracy did not improve however. Therapy may not therefore need to target phonology concurrently with vocabulary until intelligibility of speech is identified as a separate intervention goal.
Reviewer’s
conclusion:
Four months of therapy targeting vocabulary in a group of late talkers appeared to indirectly improve their emerging phonological skills significantly more that no treatment over a 4 month treatment period.

The Centre for Allied Health Evidence (CAHE)
87
Summary of intervention program: Interactive focussed stimulation (Hanen therapy)
Reference:
Girolametto L, Wiigs M, Smyth R, Weitzman E, & Pearce PS, 2001, ‗Children with a history of expressive vocabulary delay: Outcomes at 5 years of age‘. American Journal of Speech-Language Pathology, vol. 10, no.4, pp. 358-369.
Country of
publication:
Canada
Publication type
(include level of
evidence):
Case-control study (level III-2)
Population:
21 children previously identified as late talkers at 2 years of age and who had participated in an intervention study (Girolametto et al 1996, 1997) were seen for follow up assessments between 64 and 76 months of age. Children aged between 23-33 months at time of intake and were at the single word stage of language development. 21 children with histories of typical language development as a normal comparison group.
Service setting:
Clinic-based group parent training and individual home visits
Service delivery
model:
Same as Girolametto et al 1996, 1997 above
Frequency/
intensity/
duration of service
provision:
Same as Girolametto et al 1996, 1997 above
Outcomes evaluation
(by disorder subtype
if possible):
13 of the 21 families received subsequent speech and language services following completion of the parent programme
Only 4 of the 11 children who received direct intervention were still receiving treatment at follow up assessment
14 children received low scores in at least one area of the parent-rated SLAS (phonology, language or pragmatics)
The majority of the 21 late talking children scored within normal limits on all three norm-referenced tests (TOLD-2, PLAI, Bus Story Test)
Children in the late talking group received lower scores on the TOLD-2, PLAI, perspective taking tasks than children in the age-matched control group
Late talkers used shorter MLU and fewer complete cohesive ties, scored lower on the narrative stage assignment and required more prompting to complete their stories than the age-matched control group
Author’s conclusion:
The majority of late talkers performed within normal limits on norm-referenced tests of language development by 5 years of age. Aside from this apparent catch-up, parents still reported multiple language

The Centre for Allied Health Evidence (CAHE)
88
weaknesses and the late talkers had poorer general language skills and more complex measures of classroom discourse, grammatical-perspective taking, and narrative ability than a group of normally developing peers.
Reviewer’s
conclusion:
Although the majority of children who participated in a parent-child interactive therapy had achieved normal levels of language development according to norm-referenced tests when followed up at five years of age (three years after therapy), parents still reported language weaknesses and the children performed more poorly than a group of normally developing peers on a number of measures.

The Centre for Allied Health Evidence (CAHE)
89
Summary of intervention program: Speech & Language therapy
Reference:
Glogowska, M, Roulstone, S, Enderby, P and Peters, T 2000, ‗Randomised controlled trial of community based speech and language therapy in preschool children‘, British Medical Journal, vol. 321, no. 7266, pp. 923-6.
Country of
publication:
UK
Publication type
(include level of
evidence):
Pragmatic randomised controlled trial (level II)
Population:
159 preschool children (aged under 3½ years at initial attendance for speech and language therapy assessment) with appreciable speech or language difficulties who fulfilled criteria for admission to speech and language therapy. Children did not have a diagnosis of severe learning difficulties or autism, oromotor deficits or primary diagnosis of dysfluency stammering) or dysphonia (voice disorders).
Service setting:
16 community clinics providing individual therapy
Service delivery
model:
Speech & language therapy:
Onetoone therapy routinely offered by the therapist that was tailored to individual needs.
Therapy tended to focus on several areas of language simultaneously.
Techniques included Derbyshire language scheme tasks, as well as everyday play and games used as contexts for modelling language for the child.
Goals covered a wide range of language stages, e.g. understanding and building single words, using narratives, and identifying consonants in words.
No further description provided. Watchful waiting:
Parents of children could request therapy at any time if they were concerned about their child's progress.
If children still experiencing difficulties at 12 months follow-up, two research therapists provided up to 12 therapy sessions.
Frequency/
intensity/
duration of service
provision:
Mean length of sessions 47 minutes
Mean 6 hours of therapy
Mean 8 contacts with therapist
Mean frequency once monthly
Mean duration of therapy 8.4 months
Outcomes evaluation
(by disorder subtype
if possible):
Although all of the observed comparisons for the primary outcome measures were in favour of the therapy group, only one was statistically significant - auditory comprehension.
Of the secondary outcome measures, only two were significantly

The Centre for Allied Health Evidence (CAHE)
90
different between the therapy and control group with a greater proportion of children in the therapy group improving their phonology and no longer satisfying the original eligibility criteria for the trial.
There were non-significant differences between the therapy and control group for the other primary outcome measures (expressive language scores, phonology error rate, the score for the Bristol language development scales, and a binary variable indicating whether the child, by 12 months, had improved sufficiently on the single clinical measure on which he or she had entered the study to no longer satisfy that particular criterion) and remaining secondary outcome measures (four therapy outcome measures; attention and play ratings; the Vineland socialisation domain; and separate binary variables indicating improvement or no deterioration over 12 months in auditory comprehension and expressive language).
Author’s conclusion:
Most children in this study still had important clinical difficulties at 12 months, regardless of trial allocation; indeed, many remained eligible for the trial, with little evidence of ―spontaneous resolution.‖ This study provides little evidence for the effectiveness of speech and language therapy when compared with ―watchful waiting‖ over 12 months. In clinical terms, these findings suggest that speech and language therapy for preschool children should be reconsidered in terms of appropriateness, timing, nature, and intensity.
Reviewer’s
conclusion:
In this pragmatic trial, therapy was provided based on individual need and structured how it would typically be provided in the community. There did not appear to be much benefit over no treatment (―watchful waiting‖). Since the therapy varied somewhat between children it is not possible to deconstruct the service model.

The Centre for Allied Health Evidence (CAHE)
91
Summary of intervention program: Speech therapy
Reference:
Goorhuis-Brouwer, S and Knijff, W 2002, ‗Efficacy of speech therapy in children with language disorders: specific language impairment compared with language impairment in comorbidity with cognitive delay‘, International Journal of Pediatric Otorhinolaryngology, vol. 63, no. 2, pp. 129-36.
Country of
publication:
Netherlands
Publication type
(include level of
evidence):
Retrospective cohort study (level III-3)
Population:
Thirty-one healthy children with normal hearing but with language problems aged between 1;5 and 5;4 years.
Service setting:
Not specified
Service delivery
model:
Speech therapy provided as the main therapy for children with specific language impairment (SLI) and in conjunction with special education for children with language impairment in co-morbidity with cognitive delay (non-SLI).
Speech therapy can be given by private speech therapists or can be integrated in the education in schools for hearing and/or language impaired children (SH/ESM-education).
No further description provided.
Frequency/
intensity/
duration of service
provision:
Not specified
Outcomes evaluation
(by disorder subtype
if possible):
Most parents followed the given advice regarding therapy (87% in the SLI group and 73% in the non-SLI group)
For language comprehension (SLI group): two children both improved significantly (100%) after a wait and see attitude was followed and six of the nine children receiving speech therapy (66%) and two of the five children following SH/ESM education (40%) also improved significantly
For language production (SLI group): improvement was seen in both children for which a wait and see attitude was followed (100%), in seven of the nine children (78%) receiving speech therapy and in one of the five children (20%) following SH/ESM education
For non-verbal intelligence (SLI group): four of the nine children (44%) receiving speech therapy improved and one of the five children (20%) following SH/ESM education; the children for which a wait and see attitude was followed did not improve
No difference in improvement in language comprehension or non-verbal intelligence between children with SLI and those with non-SLI
A significant difference in improvement in language production between the two groups in favour of the SLI group

The Centre for Allied Health Evidence (CAHE)
92
Author’s conclusion:
Speech therapy seems to be effective for children with SLI. Some children also benefit from a wait and see attitude. We hypothesise that a diagnostic procedure can reassure parents, which can result in a positive effect on child-rearing practice.
Reviewer’s
conclusion:
Although this paper did not provide information on the type of speech therapy the children received, therapy appeared successful in improving receptive and expressive language skills in children with specific language impairment. Also useful was a wait and see approach (although a small number of children contributed to this conclusion).

The Centre for Allied Health Evidence (CAHE)
93
Summary of intervention program: Phonological therapy
Reference:
Harbers HM, Paden EP, & Halle JW, 1999, ‗Phonological awareness and production: Changes during intervention‘. Language, Speech & Hearing Services in Schools, vol. 30, no. 1, pp. 50-60.
Country of
publication:
USA
Publication type
(include level of
evidence):
Case series (level IV)
Population:
4 children aged 3;5-4;2 with severe phonological deviancy. All had normal control of articulators, normal intelligence, normal hearing, normal middle ear function, age-appropriate auditory comprehension and expressive language skills.
Service setting:
Clinic (university)-based individual therapy
Service delivery
model:
Three patterns with at least 40% deficiency were chosen for intervention for each child
Overall 5 different patterns were targeted: initial strident clusters, velars, singleton stridents, final consonants, and liquids
The initial strident cluster received intervention first and thereafter the order was determined by the patterns that were deficient in each child
Performance on feature/syllable shape awareness and production were assessed after every two sessions
Continuation of the intervention phase was determined by performance on the production and awareness tasks
No more than 5 probes per treatment phase (for a total of 10 sessions)
Emphasis on conceptual awareness and production
Components from the Metaphon approach were combined with an approach of Hodson and Paden (1991)
Variations in the basic framework were made on an individual basis and were determined by each child‘s level of awareness and ease in producing the target pattern
The following programme was used for each session: exposure to rhyme/alliteration; auditory bombardment with slight amplification; conceptualising the features of the target pattern; experiential play/production practice; awareness feedback
Treatment provided by the first author (speech-language pathologist?)
Family members observed sessions and was given specific instruction in verbal and written form on how to respond to their child‘s communication efforts
Frequency/
intensity/
duration of service
provision:
45 minute sessions x twice per week
6-9 months treatment

The Centre for Allied Health Evidence (CAHE)
94
Outcomes evaluation
(by disorder subtype
if possible):
When intervention focussed on initial strident clusters, production performances of all children improved substantially
A comparison of pre-and post-assessment percentages on the APP-R revealed increases in 9/11 instances where patterns received intervention
Levels of feature awareness during intervention were similar to those during baseline; there was no evidence that intervention alone accounted for increases
Author’s conclusion:
There was an improvement in production for four out of five patterns and modest improvement in feature awareness for all four participants following a conceptual awareness and production intervention in 4 children with severe phonological deviancy. Improvement in production or feature awareness did not always accompany one another. Improvement in feature awareness was not as clear cut as improvement in production. Findings from this study suggest the importance of examining both awareness and production to better understand children‘s phonological systems.
Reviewer’s
conclusion:
A conceptual awareness and production intervention over 6-9 months appeared to lead to an improvement in production, however given that this was a case series of only 4 participants it is not possible to directly attribute any improvements to the intervention alone.

The Centre for Allied Health Evidence (CAHE)
95
Summary of intervention program: Articulation-based therapy vs. Metaphonologically-based therapy
Reference:
Hesketh, A, Adams, C, Nightingale, C and Hall, R 2000, ‗Phonological awareness therapy and articulatory training approaches for children with phonological disorders: a comparative outcome study‘, International Journal of Language & Communication Disorders, vol. 35, no. 3, pp. 337-54.
Country of
publication:
UK
Publication type
(include level of
evidence):
Comparative study within a case-control study (level III-2)
Population:
61 children aged 3;6–5;0 years and known to have a phonological disorder (PD) for which they had not yet received any therapy referred by Speech and Language Therapy (SLT) services. The children had normal hearing as shown by their last hearing test, no structural or motor speech problems apparent on oral examination and English as a first language. 33 children aged 3;6–5;0 years and considered of normal academic and linguistic ability by their teachers were recruited from three schools in socio-economically contrasting local areas to establish norms for the acquisition of phonological awareness. 59 normally speaking control children aged between 3;6 and 5;0 years were recruited to control for amount of improvement in speech and phonological awareness which might be expected through normal development during a period of intervention.
Service setting:
Clinic-based individual therapy
Service delivery
model:
Target processes or phonemes for intervention were selected according to individual phonemic inventories in priority order: o stimulable but not used spontaneously; o developmentally the next appropriate; o having the greatest effect on intelligibility
Provided by a registered speech and language therapist Articulation (ART)-based therapy:
Involved tasks which practised the production of phonemes or phoneme classes which assessment had shown to be problematic, but the therapy did not directly target underlying phonological knowledge.
Practice tasks worked through the target sounds or groups of sounds in isolation, in simple CV or VC structures (if appropriate), in words containing the target in initial or final word position and, finally, in sentences containing such words.
If the child became consistent within the therapy period at producing all his/her target sounds or eliminating the process at a sentence level, then a new target sound or process would be

The Centre for Allied Health Evidence (CAHE)
96
introduced.
The emphasis was on lots of physical practice at producing the correct form of a sound or sounds.
Metaphonologically (MET)-based therapy:
Included both general phonological awareness tasks and on more specific awareness tasks involving their target phonemes or processes.
The first four sessions involved work on rhyming, syllable clapping, alliteration, blending and segmenting games.
In sessions 5–8 the phonological awareness tasks focused on the therapy targets.
If the child had a particular phonological process occurring in his/her speech output, the features of that process were discussed.
Only in the last 2 weeks of therapy was production work involved, using contrasting sounds and minimally paired words.
In the last 2 weeks children were not directly corrected on their speech attempt but were given feedback commenting on phonological features of their production.
Frequency/
intensity/
duration of service
provision:
10 weekly sessions of individual phonological therapy.
Outcomes evaluation
(by disorder subtype
if possible):
The PD group made significantly more change than the normally speaking controls in metaphonological ability (MAB) from pre- to post-test, and the differences in means after the therapy were not significant
There was no post-therapy difference in MAB between the ART and MET groups
For speech output: there were significant differences between the ART/control and MET/control groups, however there was no significant difference between ART and MET groups; the ART group made significantly more change than MET group on the probe measure; of the children that received no further therapy both ART and MET groups showed slight deterioration in probe measure between post-therapy and 3-month follow-up
When children were stratified as poor or good on their baseline MAB scores, there was no difference in probe change or PCC
Author’s conclusion:
A clear effect has emerged of the benefits of even modest amounts of speech and language therapy for children with phonological disorders. Both the ART and MET therapy groups made more progress during 10 sessions of therapy than the normal speakers in that time. Children that received no further therapy then demonstrated an overall deterioration suggesting a specific training effect that diminished at the end of a short period of therapy and which may be more marked in the ART group. There was no effect of therapy type, although this may be an artefact of small group size.
Reviewer’s
conclusion:
Although there did not appear to be a significant difference between ART-and MET-based therapy, both types of therapy appeared to be equally effective in improving children‘s metaphonological ability and speech output.

The Centre for Allied Health Evidence (CAHE)
97
Summary of intervention program: Phonological Awareness
Reference:
Hesketh A, Dima E & Nelson V, 2007, ‗Teaching phoneme awareness to pre-literate children with speech disorder: a randomized controlled trial‘. International Journal of Language and Communication Disorders, vol. 42, no. 3, pp. 251-271
Country of
publication:
UK
Publication type
(include level of
evidence):
Randomised controlled trial (level II)
Population:
42 children aged 4;0-4;6 with speech problems. All children spoke English as their first language, had no hearing impairment, no apparent structural or neurological problem affecting speech production and had normal range language and cognitive abilities.
Service setting:
Home or school-based individual therapy (depended on parental preference)
Service delivery
model:
Programmes did not constitute speech and language therapy and activities were not tailored to child‘s individual communication profile
Provided by one of two researchers (speech and language therapists?) Phonological Awareness (PA) (intervention) programme:
Tasks progressing from syllable to phoneme awareness
First four sessions targeted syllable and rhyme awareness; thereafter the focus was on individual phonemes beginning with word onsets and building up to the manipulation of individual phonemes at the beginning or end of words, including addition and deletion within clusters
Language Stimulation (LS) (control) programme:
Linked to nursery and reception curricula, aiming to develop children‘s language abilities
Sessions focussed on listening comprehension, print awareness, expression of feelings, developing vocabulary and general knowledge of concepts like animals, means of transportation, seasons, days of the week
Frequency/
intensity/
duration of service
provision:
20 x 30-min sessions given 2-3 times weekly over 10 weeks
Outcomes evaluation
(by disorder subtype
if possible):
Few (n=4) participants improved overall in Alliteration Awareness and there was no significant difference between the groups
More participants (n=20) improved in Phoneme Isolation, particularly in the PA group and the difference between the groups was significant (p<0.01)

The Centre for Allied Health Evidence (CAHE)
98
Few (n=7) participants improved in Phoneme Segmentation but all who did received the PA intervention and there was a significant inter-group difference (p<0.01)
The few (n=6) children improved to above-chance performance on Phoneme Manipulation were all in the PA group and the inter-group difference was significant (p=0.02)
Author’s conclusion:
The results show that for three out of four measures significantly more children improved in the Phonological Awareness group than the Language Stimulation group. It is possible therefore to teach phoneme awareness to pre-literate children with speech disorder by means of targeted activities. However the low number of children who did improve and the large variability in performance within the PA group indicates a need for caution in accepting this conclusion.
Reviewer’s
conclusion:
Phonological awareness improved significantly more following a Phonological awareness programme than a control treatment involving language stimulation, however only small numbers of children improved in the intervention group.

The Centre for Allied Health Evidence (CAHE)
99
Summary of intervention program: Laurel House Early Language Programme
Reference:
Jones, J 1995, ‗The Laurel House Early Language Program‘, in 'Communicating 'now we're really talking': 12th State Conference of the Australian Early Intervention Association (NSW Chapter) Inc, Vineyard Resort; Pokolbin NSW'.
Country of
publication:
Australia
Publication type
(include level of
evidence):
Conference proceeding
Population:
Children aged 2-5 years with, or at risk of, language delay.
Service setting:
Home-based individual therapy
Service delivery
model:
Based initially on the ‗Ready, Set, Go Talk to Me‘ programme of Horstmeier & MacDonald (1978)
Run by an early childhood specialist educator
Child‘s language development status is determined on entry to the programme using formal and informal assessment of receptive and expressive language, pragmatic development and play skills
Starting off point is identified and targets for therapy are suggested
Targets discussed with parents and agreed upon before suggested activities are modelled with the parents and child
No formal goals are set, rather aims are set
Written information on stages of early language development, suggestions for appropriate adult language and ways to encourage play are given to the parents
Each session involves reporting on the previous week‘s progress, revision of activities previously suggested and introduction and practice of new activities
Typical session may include: o Role play and role exchange in a turn taking setting o Modifying adult language model for initiation commensurate with
child‘s language o Use of expansion, extension, commenting, binary choice, home
rules o Discussing implantation of new activities and strategies at home
No formal sequence
Emphasis on situations and activities that are compatible with child‘s interests and abilities, parent‘s available time, progress at a comfortable rate for child and parents
Play is principal medium for encouraging and teaching communication
Attention is given to turn taking and joint attention
Strategies include modelling, prompting, commenting, visual and verbal cueing, extension and expansion, and following the child‘s interests and leads

The Centre for Allied Health Evidence (CAHE)
100
Praise and success are important
Extensive use of natural gesture and signs
Parents encouraged to share the programme and activities with other members of the family
Contact with preschool, day care centres or early intervention programmes is recommended
Progress routinely assessed after 6 months in the programme
Frequency/
intensity/
duration of service
provision:
Stage 1: 12 x 45 minute weekly visits
Stage 2: visit at 3-4 weekly intervals for 3 months
Stage 3: check up visits once a term if required
Outcomes evaluation
(by disorder subtype
if possible):
Consistent gains in both receptive and expressive language, although progress depends on the degree of delay, nature of the disability, and the parent‘s ability to follow through on activities and suggestions
‗Typical gains‘ over the period as measured by the Proportional Change Index were presented but there is no indication of how representative these children are of the population, and no statistical analysis is presented
There was no data available beyond the 6-month assessments
Author’s conclusion:
The individualised nature of the Laurel House Early Language Program, along with the sensitivity to different family structures, needs and management styles ensures that the parents develop their skills in such a way that they are able to take a more active, informed role in encouraging their children‘s language development.
Reviewer’s
conclusion:
Although a detailed description of the programme was provided there was insufficient outcome data reported to make a determination of the effectiveness of the programme.

The Centre for Allied Health Evidence (CAHE)
101
Summary of intervention program: Third-person singular –s vs. Auxiliary is/are/was training
Reference:
Leonard, L, Camarata, S, Brown, B and Camarata, M 2004, ‗Tense and agreement in the speech of children with specific language impairment: patterns of generalization through intervention‘, Journal of Speech, Language and Hearing Research, vol. 47, pp. 1363-1379.
Country of
publication:
USA
Publication type
(include level of
evidence):
Comparative study (level III-2)
Population:
31 children aged 3;0-4;4 years meeting the diagnostic criteria for Specific Language Impairment (SLI). Each child was from a monolingual English-speaking home, and had normal hearing.
Service setting:
Two universities (individual therapy)
Service delivery
model:
Therapy provided by speech-language pathologists and/or speech-language pathology students
Two different treatments followed identical procedures except for the details dictated by the choice of targets
Each session involved two types of activities
First activity represented use of focused stimulation through a story read by the clinician
Second activity involved the clinician‘s use of conversational recasting during play with the child
Where 2 sessions were held in the same day, a play period or language stimulation activity occurred in between the sessions
48 stories were used (one per session)
In each story the target form was presented 12 times in total
Contrasts between the third-person singular and plural (is-are), between present and past (is-was), and between finite and non-finite (is fixing-fixing)
Assumed that the presentation of multiple instances of the target form along with grammatically contrastive forms would be beneficial to the children‘s learning
Each story included an error by the clinician that was then immediately and overtly corrected
Child encouraged to play with the toy characters and props used in the story
Clinician provided additional material for the child to talk about
Clinician provided 12 recasts that contained either the third-person singular –s forms or the three overt auxiliaries is, are and was depending on training group
Recasts were conversationally appropriate replies to utterances produced by the child
Clinicians were responsive to the children‘s requests and questions and were free to initiate conversation about the materials
Total number of target exposures during the intervention period was

The Centre for Allied Health Evidence (CAHE)
102
1152
Targets differed according to treatment program below Third-person singular –s (―3S treatment‖)
Target form = third-person singular –s appeared 12 times in each story, and there were no instances of auxiliary or copula be forms and no instances of past –ed.
Auxiliary is/are/was (AUX treatment)
Target = three overt auxiliaries is, are and was appeared a total of 12 times in each story (4 each)
The stories did not include any instances of third-person singular –s or past –ed
Frequency/
intensity/
duration of service
provision:
48 treatment sessions, 4 per week (in most cases 2 sessions per day, on 2 days of the week) over 12 weeks
Outcomes evaluation
(by disorder subtype
if possible):
No main effect of participant group, with overall gains in the 3S and AUX treatment groups being comparable
Significant main effect for grammatical morpheme type
Statistically significant interaction between participant group and grammatical morpheme type
Each group showed significantly greater use of the grammatical morpheme type that served as their respective target than they showed on the past –ed and the control form
In addition each group showed use of one non-target tense/agreement morpheme type
No child achieved mastery level on the target form after the 48 interventions
All children‘s DSS scores remained below the 10th percentile for their age after the treatment
Author’s conclusion:
This study demonstrated that modest gains in the use of target and related forms can be seen in children with SLI following an intervention program composed of (a) focused stimulation with grammatical contrasts, (b) conversational recasts, and (c) errors with self-correction.
Reviewer’s
conclusion:
Both third-person singular –s and Auxiliary is/are/was training appeared to produce moderate gains in the use of the forms that were the target of the programme in children with SLI. However, this was not a randomised controlled trial and as such any improvements cannot be directly attributed to the intervention. Also, most children in the study were attending their own additional therapy so it unclear whether the benefits can be solely attributed to the interventions in this study.

The Centre for Allied Health Evidence (CAHE)
103
Summary of intervention program: Third-person singular –s vs. Auxiliary is/are/was training
Reference:
Leonard, LB, Camarata, SM, Pawlowska, M, Brown, B and Camarata, MN 2006, ‗Tense and agreement morphemes in the speech of children with specific language impairment during intervention: phase 2‘, Journal of Speech, Language and Hearing Research, vol. 49, no. 4, pp. 749-70.
Country of
publication:
USA
Publication type
(include level of
evidence):
Comparative study (level III-2)
Population:
25 children aged 3;0-4;4 years who met the customary selection criteria for specific language impairment (SLI). Each child was from a monolingual English-speaking home, and had normal hearing.
Service setting:
Two universities (individual therapy)
Service delivery
model:
Therapy provided by speech-language pathologists and/or speech-language pathology students
Two different treatments followed identical procedures except for the details dictated by the choice of targets
Each session involved two types of activities
First activity represented use of focused stimulation through a story read by the clinician
Second activity involved the clinician‘s use of conversational recasting during play with the child
Where 2 sessions were held in the same day, a play period or language stimulation activity occurred in between the sessions
48 stories were used for the first 48 sessions, and then re-used in a random order for the following 48 sessions
In each story the target form was presented 12 times in total
Contrasts between the third-person singular and plural (is-are), between present and past (is-was), and between finite and non-finite (is fixing-fixing)
Assumed that the presentation of multiple instances of the target form along with grammatically contrastive forms would be beneficial to the children‘s learning
Each story included an error by the clinician that was then immediately and overtly corrected
Child encouraged to play with the toy characters and props used in the story
Clinician provided additional material for the child to talk about
Clinician provided 12 recasts that contained either the third-person singular –s forms or the three overt auxiliaries is, are and was depending on training group
Recasts were conversationally appropriate replies to utterances produced by the child
Clinicians were responsive to the children‘s requests and questions

The Centre for Allied Health Evidence (CAHE)
104
and were free to initiate conversation about the materials
Total number of target exposures during the intervention period was 2304
Targets differed according to treatment program below Third-person singular –s (―3S treatment‖)
Target form = third-person singular –s appeared 12 times in each story, and there were no instances of auxiliary or copula be forms and no instances of past –ed.
Auxiliary is/are/was (AUX treatment)
Target = three overt auxiliaries is, are and was appeared a total of 12 times in each story (4 each)
The stories did not include any instances of third-person singular –s or past –ed
Frequency/
intensity/
duration of service
provision:
96 treatment sessions, 4 per week (in most cases 2 sessions per day, on 2 days of the week) over 24 weeks
Outcomes evaluation
(by disorder subtype
if possible):
No main effect of participant group, with overall gains in the 3S and AUX treatment groups being comparable
Significant main effect for morpheme type and time
Both groups made similar progress from the start to mid-point and end of the 96 treatment sessions
Participant group x morpheme type interaction was significant
Morpheme type x time interaction was significant
Three-way interaction between group, morpheme type and group also proved significant
For both groups there was no significant difference between the target and any of the other morpheme types at baseline
For both groups at the mid-point (after 48 treatments) and post-treatment (after 96 treatments) the target was significantly greater than both the past tense and the target serving as the morpheme for the other group
For both groups the morpheme serving as the target for the other group did not significantly change from baseline to mid-point, however a significant increase occurred from mid-point to post-treatment
Great deal of individual variation in the gains children made on the different morphemes
Both groups contained children that made no progress at all by the end of treatment
At the end of the intervention, 11 of the 15 children in the 3S group and 9 of the 10 children in the AUX group continued to score below the 10th percentile on the DSS for their age group
Author’s conclusion:
It appears that both interventions facilitated children‘s use of the target form, although only a few children‘s gains were suggestive of mastery levels. Gains in certain morphemes seemed to promote gains in others, but some of this might not be related to treatment. The greatest gains were seen for the target form and the smallest gains seen for the past tense –ed.
The Centre for Allied Health Evidence (CAHE)
105
Reviewer’s
conclusion:
Although both third-person singular –s and Auxiliary is/are/was training appeared to produce moderate gains in the use of the forms that were the target of the programme in children with SLI it is not possible to directly attribute these gains to the intervention on the basis of this non-randomised comparative study. Also, most children in the study were attending their own additional therapy so it unclear whether the benefits can be solely attributed to the interventions in this study.
The Centre for Allied Health Evidence (CAHE)
106
Summary of intervention program: Prescriptive activity-based treatment
Reference:
Littleton, R 2004, ‗The Modifiability of Language Input with Toddlers with Expressive Language Delay: A Study of a Team Approach to Parent Training‘, Dissertation Abstracts International, A: The Humanities and Social Sciences, vol. 65, no. 1, pp. 115-A. Note: abstract only available
Country of
publication:
USA
Publication type
(include level of
evidence):
Comparative study (level III-2)
Population:
Eight parents and their toddlers with expressive language delay were randomly assigned to receive either prescriptive activity-based treatment (Treatment/PAT group) or traditional early intervention (Delayed-treatment Control/TEI group).
Service setting:
Not specifically reported in abstract but assumed similar to Girolametto et
al (1996).
Service delivery
model:
Experimental group:
Modified version of the focussed stimulation intervention used by Girolametto et al (1996)
Modified in a manner that increased reliance on a broader array of elements of responsive adult input (RAI), while eliminating reliance on a stipulated frequency of repetition
Prescriptive activity-based parent teaching was provided in the home by a team comprised of a speech and language pathologist (SLP) and a non-SLP early interventionist who was delegated responsibility for the majority of treatment
Protocols for assignment of vocabulary targets and collection of outcome data were intended to replicate those of Girolametto et al. (1996)
Control group:
Received traditional early intervention services during the experimental period
Frequency/
intensity/
duration of service
provision:
Not specifically reported in abstract but assumed similar to Girolametto et al (1996)
Outcomes evaluation
(by disorder subtype
if possible):
With one exception (Type Token Ratio), results indicate changes in the predicted direction for treatment group (PAT) parents and children receiving prescriptive activity-based treatment
Inferential statistics indicated a significant interaction for the

The Centre for Allied Health Evidence (CAHE)
107
Symbolic Play Test
Results for measures that did not achieve statistical significance are attributed to the fact that the control group (TEI) received traditional early interventionist services during which non-SLP early interventionists modelled RAI elements
Following treatment, the language of parents receiving prescriptive activity-based treatment was slower, less complex, and more focused than those in the control group.
Author’s conclusion:
Treatment group children used more target words during naturalistic observations, used more words during free-play, and made substantial gains in vocabulary. Substantial gains were also identified in talkativeness and structural complexity of child language. This study compares favourably with Girolametto et al (1996) on numeric scores and magnitudes of effect.
Reviewer’s
conclusion:
The results of this study appear to replicate those of Girolametto et al (1996), thus supporting the use of early indirect intervention by trained parents.
The Centre for Allied Health Evidence (CAHE)
108
Summary of intervention program: Phonological +/- Metaphonological Intervention
Reference:
Major EM & Bernhardt BH 1998, ‗Metaphonological skills of children with phonological disorders before and after phonological and metaphonological intervention‘. International Journal of Language and Communication Disorders, vol. 33, no. 4, pp. 413-444.
Country of
publication:
Canada
Publication type
(include level of
evidence):
Case series (level IV)
Population:
19 pre-school children aged 3;0-4;11 with moderate to severe phonological disorders. All children has restricted phonetic inventories, reduced word and syllable shapes and had substitutions that are not common. The hearing, oral-motor structure and function, and language comprehension of all children were within normal limits.
Service setting:
Clinic- (health centre) based individual therapy
Service delivery
model:
Speech and language pathologists conducted the interventions
University research team provided training and set up individual intervention programmes and provided ongoing consultation to the clinicians
Children assessed before intervention (T1), following phonological intervention only (T2) and then following phonological plus metaphonological intervention (T3)
Phonological intervention:
Assessment and follow-up probes were administered at the end of each treatment block and were done in addition to the 48 therapy sessions
Children semi-randomly assigned to conditions in counterbalanced orders in terms of phonological goals and intervention methods
Block 3 considered ‗ethical‘ phonological intervention block
Phonological goals and methods were designed to address specific needs of children
Therapy techniques included awareness activities, perceptual contrast training and production activities
All sessions began with a short awareness activity with no required verbal response
Each of the first two treatment blocks had four main goals (two segmental and two word and syllable structure) and four main treatment techniques with four sessions each
In each of the first two blocks there were four sessions of awareness and perceptual contrast activities for a particular speech sound or feature and four sessions utilised oral-motor facilitation techniques with imitation training

The Centre for Allied Health Evidence (CAHE)
109
Production activities for the eight sessions of word and syllable structure goals per block involved imitation and spontaneous productions
In four sessions subsyllabic sequences were presented as onsets and rhyme units
In the remaining four sessions sequences were presented as CV units with separate additional consonants
Rhythmic accentuation highlighted stress-bearing units
In the final block the most facilitative phonological intervention techniques for a specific child were used
Metaphonological intervention:
Block 3 (12 sessions) included metaphonological training in the context of phonological intervention
Primary focus remained on phonology
Phonological awareness training was incorporated through activities that drew children‘s attention specifically to onsets, rhymes and individual sounds
Rhyming and alliteration were introduced in stimuli sets for awareness, perceptual contrast training and imitation
Frequency/
intensity/
duration of service
provision:
48 therapy sessions (3 per week) over three treatment blocks
Blocks 1 and 2 consisted of 18 sessions and block 3 comprised 12 sessions
Programme length ranged from 5-10 months
Outcomes evaluation
(by disorder subtype
if possible):
Children‘s phonological development was significant (p<0.05) for all measures between T1 and T2 and between T2 and T3
A significant difference in children‘s metaphonological task performance between T1-T2 and T2-T3 (p<0.05)
Correlations were not significant between changes in phonological outcome measures and changes in total metaphonology scores
Author’s conclusion:
The metaphonological skills of children with moderately severe to severe phonological disorders were related to their morphosyntactic production and phonological abilities. Children with phonological disorders can improve their phonological awareness skills and some children may improve their skills with only limited training. Other children may require more explicit metaphonological training to increase their skills on such tasks. Because of individual differences it is important to monitor each child‘s abilities and to focus treatment more specifically on metaphonology for children who require this level of intervention.
Reviewer’s
conclusion:
Examines the relationship between children‘s phonological and syntactic production skills, and makes recommendation that intervention needs to be individually tailored to children‘s needs.

The Centre for Allied Health Evidence (CAHE)
110
Summary of intervention program: “Partnership with Parents” (parent programme)
Reference:
McDade, A and McCartan, P 1998, ‗'Partnership with parents' a pilot project‘, International Journal of Language & Communication Disorders, vol. 33 Suppl, pp. 556-61.
Country of
publication:
UK (Scotland)
Publication type
(include level of
evidence):
Comparative study (level III-2)
Population:
11 families of children referred by health visitors to a paediatric speech and language therapy community clinic. Control group (who received no treatment) of 9 families of children referred to clinics matched for sex, chronological age, mother‘s educational level and maternal age. All children had fewer than 50 words, no word combinations at two years, and normal receptive language. Although the age of the children was not directly specified, children were „usually referred‟ to speech and language therapy at 24 months.
Service setting:
Community clinic and home-based
Service delivery
model:
Parents attended an orientation session
Home visit to videotape (15 mins) a pre-treatment mother-child interaction (instructed to play as normally would)
Hanen programme used (no further description provided)
Frequency/
intensity/
duration of service
provision:
9 evening sessions at local health centres and 3 home visits over 12 weeks
Outcomes evaluation
(by disorder subtype
if possible):
Parent training group showed a significant treatment effect for actual time and percentage of total time in interactive engagement whereas the control group remained virtually unchanged
Actual time and percentage of total time in unengagement decreased significantly for the parent training group
PLS-3 scores increased significantly for the parent training group for expressive language and total language scores, whereas they did not for the control group
Author’s conclusion:
The results indicate the potential effectiveness of this type of parent training intervention for children identified as being ‗at risk‘ of language delay.
Reviewer’s
conclusion:
This parent training programme, based on the Hanen programme appeared to be beneficial in terms of parent behaviour and children‘s language.

The Centre for Allied Health Evidence (CAHE)
111
Summary of intervention program: Structured interaction using peer modelling
Reference:
Robertson, S and Weismer, S 1997, ‗The influence of peer models on the play scripts of children with specific language impairment‘, Journal of Speech Language & Hearing Research, vol. 40, no. 1, pp. 49-61.
Country of
publication:
USA
Publication type
(include level of
evidence):
Study 1: comparative study (level III-2) Study 2: case series (level V)
Population:
Study 1 20 children aged 3;8-5;1 years with Specific Language Impairment (SLI) and 10 age-matched peer models with normal language abilities. All children with SLI were enrolled in a language-based early childhood classroom. Children did not have concomitant motor, emotional, or physical handicaps or hearing/visual problems. All children were monolingual speakers of American English. Study 2 6 children aged 48-58 months with SLI from the control group (SLI-C) and 2 peer models (both selected from study 1 sample).
Service setting:
Classroom based group therapy
Service delivery
model:
Study 1
All children with SLI were encouraged to ―play house‖ with 1-3 other classmates and then verbal scripts were elicited from all 30 children prior to intervention
Following experimental or control treatment, scripts for playing house were again elicited from all 30 children
A follow up play script was elicited from SLI children 3 weeks after the final session
Experimental group (SLI-E):
Play sessions with peer models in a specially designed play environment using props to support the play themes previously identified in peer model script reports
Children with SLI were paired with a different peer model during each session
Each session videotaped
No adult directives given Control group (SLI-C):
Continued to participate in their self-contained classroom with opportunities for play in a house area containing the same props given to the SLI-E group
Study 2
Baseline measurements taken

The Centre for Allied Health Evidence (CAHE)
112
4 randomly assignment dyads were formed: 2 x 2 SLI children; 2 x 1 SLI + 1 peer model
New partners were not assigned for each session, dyads remained the same for the intervention period
Same specialised environment as described in study 1
Frequency/
intensity/
duration of service
provision:
Study 1:
―play house‖ for at least 4 periods of 15-20 minutes prior to intervention
Children in SLI-E group participated in four dyadic 15 minute play sessions with peer models over 3 weeks
Study 2:
Four dyadic 15 minute play sessions with a peer model over 3 weeks
Outcomes evaluation
(by disorder subtype
if possible):
Study 1:
SLI-E group produced significantly more words in their script reports than the SLI-C group both immediately after treatment and at 3 weeks follow up
SLI-E group employed more lexical diversity in their script reports than the SLI-C group both immediately and 3 weeks after intervention
SLI-E group had significantly greater number of play-theme related acts present in their script reports than the SLI-C group both immediately and 3 weeks after intervention
SLI-E group demonstrated significantly greater gains in use of linguistic markers than the SLI-C group both immediately and 3 weeks after treatment
Study 2:
Data representing individual subject performance across the same 4 variables measured in study 1 revealed that play with typically developing peer models produces positive increases in the play scripts of children with SLI
None of the children in the control dyads (2 children with SLI) improved on more than one variable whereas the children with SLI that were paired with peer models showed improvement on all variables
Author’s conclusion:
The combined results for both phases of this study provide support for the use of structured interaction with typically developing peers acting as play models to develop the play scripts of children with SLI.
Reviewer’s
conclusion:
Peer modelling during structured play interaction may be a relatively simple and early approach for improving the language of young children with language impairment.

The Centre for Allied Health Evidence (CAHE)
113
Summary of intervention program: Early language intervention
Reference:
Robertson, S and Weismer S 1999, ‗Effects of treatment on linguistic and social skills in toddlers with delayed language development‘, Journal of Speech, Language and Hearing Research, vol. 45, no. 5, pp. 1234-48.
Country of
publication:
USA
Publication type
(include level of
evidence):
Comparative study (level III-2)
Population:
21 late talking toddlers aged 21-30 months. All had significant delays in the acquisition of language (both expressive and receptive but majority expressive) but normal development in other areas. All had normal hearing, oral and speech motor abilities, and no frank neurological deficits. All came from monolingual, English-speaking homes.
Service setting:
Centre-based birth to 3 programme (small group therapy)
Service delivery
model:
Treatment group:
Direct, clinician implemented treatment
Interactive, child-centred approach that provided general stimulation emphasising vocabulary development and use of early 2- or 3-word combinations within a social context
Provided by 3 ASHA-certified speech-language pathologists (each had at least 2 years experience in assessment and treatment of children with language delay)
No more than 4 children enrolled in each group
Clinician paired with the same group of children throughout
Intervention based on a familiar routine or script
Once established, specific components of the script were manipulated
A unit or theme was designated on a weekly or biweekly basis
Linguistic input naturally paired with hands on activities and visual cues that encouraged mapping of new information through cross-modal referencing
Clinicians systematically employed reduction in the rate of input, manipulation of stress to emphasise particular linguistic targets, and positioning of targeted vocabulary at the beginning or end of an utterance
Key component was to encourage communicative attempts and to facilitate improvement in children‘s linguistic skills through particular techniques (scaffolding/mediation)
Specific techniques chosen for individual children based on their current level of functioning
Organisation of the intervention environment to provide multiple opportunities for the child to share information, participate in naturally occurring interactions, regulate the behaviour of others, and receive appropriate feedback and reinforcement
Parents not directly involved but permitted to observe

The Centre for Allied Health Evidence (CAHE)
114
Delayed-treatment (control) group:
Given the opportunity to participate in the same treatment given to the experimental group at the end of the study
Frequency/
intensity/
duration of service
provision:
2 x 75 minute therapy session per week over 12 weeks
Outcomes evaluation
(by disorder subtype
if possible):
Children in the treatment group exhibited significantly greater increases in MLU than the control group (all children in the treatment group had begun to use multiword utterances)
Children in the treatment group produced significantly more words (on TNW) with a mean increase of 21 words, than the control group
Children in the treatment group exhibited significantly greater lexical diversity than children in the control group, with an average increase of 10 words
Children in the treatment group demonstrated significantly greater gains in their reported vocabulary size than the control group, with an average increase of 38 words
Children in the treatment group produced significantly more intelligible spontaneous utterances than the control group
A significant increase in socialisation skills in the treatment group over the control group
A significant reduction in parental stress in the treatment group over the control group
Author’s conclusion:
Children receiving an early language intervention based on small group therapy exhibited improvements in vocabulary and multiword combinations, and other areas that were not specifically targeted by the intervention: social skills, speech intelligibility and parental stress. This suggested that clinician led language intervention can produce significant short term improvements over a relatively short treatment interval.
Reviewer’s
conclusion:
A small group centre-based language therapy intervention produced a significantly greater improvement in vocabulary and socialisation skills when compared to no treatment for a group of young children with language delays.

The Centre for Allied Health Evidence (CAHE)
115
Summary of intervention program: Phonemic perception training
Reference:
Rvachew, S, Nowak, M, and Cloutier, G 2004, ‗Effect of phonemic perception training on the speech production and phonological awareness skills of children with expressive phonological delay‘, American Journal of Speech-Language Pathology, vol. 13, no. 3, pp. 250-63.
Country of
publication:
Canada
Publication type
(include level of
evidence):
Randomised controlled trial (level II)
Population:
34 children aged 41-59 months scheduled to receive speech therapy from the hospital in their pre-kindergarten year. All children had moderate to severe delays in expressive phonological skills and average or above average receptive vocabulary skills. They had normal hearing and oro-motor structure and functioning. 17 children participated in speech therapy, and 17 formed the control group.
Service setting:
Children‘s hospital
Service delivery
model:
Pre-treatment assessment
All children received speech therapy directed at the remediation of their sound production errors
Treatment sessions under either experimental or control conditions as per below
Where possible experimental/control treatments were scheduled to occur directly after the regular speech therapy session
Post-treatment assessment administered 6 months after the pre-treatment assessment
Initial speech therapy:
Provided by speech-language pathologist to all 34 children
Approaches varied and included cycles, sensorimotor, or traditional approaches to phonological intervention
Experimental treatment programme:
Child played computer game with assistance of student research assistant and/or parent
Research assistant provided written report about each session
Computer game based on the SAILS platform
Corrective feedback provided
First 8 lessons focussed on one of the following sounds, in order as written, in the word-initial position: /t, p, m, k, l, r, f, s/
Last 8 lessons targeted these consonants in the same order, but in the word-final position
Each lesson comprised the same four tasks: phonemic perception, letter recognition, letter-sound association, and onset (or rime) association
Sequence of tasks repeated three times in each session providing a minimum of 30 trials for each task

The Centre for Allied Health Evidence (CAHE)
116
Control treatment programme:
Provided by a student research assistant and parents
Research assistant provided written report about each session
Each lesson based on commercially available computer-presented stories
One quarter of each book was completed during each lesson
Parent asked child about the illustrations and story covered
Parent provided correct responses if necessary
Questions became increasingly complex and abstract
Progress from matching perception to selective analysis of perception, re-ordering perception, and reasoning about perception
Lessons did not include any active teaching of phonemic perception, phonological awareness, phonics or reading
Frequency/
intensity/
duration of service
provision:
Treating speech-language pathologist determined the duration, frequency and number of sessions of the initial remediation of sound production errors (mean 624 minutes of therapy in 12 sessions over 5 month period)
Additional 16 x 15 minute training sessions (experimental or control) on a weekly basis
Outcomes evaluation
(by disorder subtype
if possible):
Neither group made significant gains in expressive syntax ability
Children in experimental group made greater gains in phonemic perception and articulatory accuracy than children in the control group (after controlling for their pre-treatment performance), but there was no difference between groups for phonological awareness
Significant differences in post-treatment articulation accuracy as a function of treatment group and pre-treatment phonemic perception ability
Although both groups improved their phonological awareness skills, there was not a significant difference between the groups
Author’s conclusion:
Phonemic perception intervention significantly improves the effectiveness of speech therapy that is directed at the remediation of children‘s articulation errors. However the phonemic perception intervention did not improve children‘s phonological awareness skills over that of a control group receiving vocabulary and verbal reasoning skills.
Reviewer’s
conclusion:
The addition of phonemic perception to ‗usual‘ speech therapy may be effective in improving phonemic perception and accuracy of articulation, however it was no more effective than a control treatment in improving phonological awareness.

The Centre for Allied Health Evidence (CAHE)
117
Summary of intervention program: Redirect strategy
Reference:
Schuele, C, Rice, M and Wilcox, K 1995, ‗Redirects: a strategy to increase peer initiations‘, Journal of Speech & Hearing Research, vol. 38, no. 6, pp. 1319-33.
Country of
publication:
USA
Publication type
(include level of
evidence):
Case series (level IV)
Population:
4 boys with SLI aged 3;10-5;3 years who were enrolled in a Language Acquisition Pre-school (LAP). All children had intellectual abilities within normal limits and none had a physical or visual disorder or hearing loss.
Service setting:
Language Acquisition Pre-School at a university for children with language impairments (SLI), children learning English as a second language (ESL) and children developing language normally (ND).
Service delivery
model:
Children free to play in any of the activity areas: art, dramatic play, quiet area (books and puzzles), block area (blocks and trucks)
Children were free to move about the room and interact with whomever they liked, whenever they liked
Adults present included: classroom teacher (either a certified speech-language pathologist or a graduate speech-language pathology student completing an internship), an assistant teacher (with Bachelor‘s degree in early childhood education) and 1-2 speech-language pathology student clinicians
Assistant teacher implemented the redirect strategy from weeks 3-11 after a training session in week 2 of the semester
A redirect occurs in an initiation made by a child
A prompted initiation occurs when an adult initiates the interaction with a child and prompts the child to initiate to a peer
Teacher instructed to redirect all children at the beginning of the study (targeted participants were not identified)
3 weeks after the intervention began the teacher was informed of the targets and asked to increase redirects to them
Frequency/
intensity/
duration of service
provision:
40-minute classes x 4 days per week over 9 weeks
Assistant teacher participated in a 2 hour training session
Outcomes evaluation
(by disorder subtype
if possible):
Prior to training, the teacher rarely used the redirect strategy
Following training, the teacher substantially increased her rate of redirecting children‘s initiations as well as prompted initiations
Approximately one third of the 4 target children‘s initiations were redirected
Children responded to 57% of redirects, 27% were overridden, 16% were not responded to
In general, peer‘s response to redirects were positive

The Centre for Allied Health Evidence (CAHE)
118
In the non-intervention semester there was little change in the subjects‘ mean proportion of peer initiations
In the intervention semester there was considerable individual variation in mean proportion of peer initiations, with 2 subjects improving, one remaining unchanged and the fourth child made similar improvements in both semesters (thus effect of intervention was unclear)
Author’s conclusion:
The redirect strategy appears promising for facilitating peer interactions in pre-school classrooms.
Reviewer’s
conclusion:
It is difficult to determine whether the redirect strategy used in this study is likely to improve children‘s language skills given the study methodology, and the fact that language outcomes were not measured.

The Centre for Allied Health Evidence (CAHE)
119
Summary of intervention program: Computer-supported phonological awareness intervention
Reference:
Segers, E, and Verhoeven, L 2004, ‗Computer-supported phonological awareness intervention for kindergarten children with specific language impairment‘, Language, Speech & Hearing Services in the Schools, vol. 35, no. 3, pp. 229-39.
Country of
publication:
The Netherlands
Publication type
(include level of
evidence):
Comparative study (level III-2)
Population:
24 children with Specific Language Impairment (SLI) aged 4;10-6;11 years who were enrolled in a kindergarten programme in special schools. SLI was diagnosed by an independent team (clinical linguists and school psychologists) as significant deficit in production and/or comprehension of language that cannot be explained by general cognitive impairments, sensorimotor deficits, neurological disorders, psychiatric diagnosis, or a general lack of exposure to language. Children had no significant hearing loss and normal intelligence.
Service setting:
Five different classrooms in two special schools (small group intervention although children worked independently from each other).
Service delivery
model:
Experimental intervention:
―Rhyming and synthesis‖ game from an educational software programme developed for the study
Alternates between rhyming and synthesis
Focussed on emergent and beginning literacy skills
Phonological awareness
10 different games used
Child received a more difficult game once achieved less than 20% error in the previous game
Each game has three sets of five exercises, increasing in difficulty
Programme provides feedback on performance
Help is offered when child provides incorrect answer so they do not get stuck in the programme
Intervention involved groups of 3 children (one from each experimental group)
Experimental group 1 received the computer phonological awareness intervention as above
Experimental group 2 received the computer programme, however the speech was slowed down by 150% and the fast transitional elements in the speech were enhanced up to 20dB, with the amount of speech manipulation decreasing as the intervention proceeded
Control group intervention:
Children listed to a story on the computer and answered questions by pointing to the screen

The Centre for Allied Health Evidence (CAHE)
120
Child could choose one of 4 story settings to play vocabulary games
Each story setting contained 10 sets of 5 questions each
Audio and visual feedback
Frequency/
intensity/
duration of service
provision:
2-3 x 15-minute computer sessions per week for 5 weeks
Experimental group 2: 4 sessions with maximum speech manipulation, 4 sessions with no delay but enhancement to 20dB, 3 sessions with enhancement up 10dB, and 3 sessions with normal speech
Outcomes evaluation
(by disorder subtype
if possible):
Significant main effects for time and test
Significant interaction between time and test
No significant interactions between test and group; time and group suggesting that group differences were not dependent on a particular test or time of testing
No significant difference between groups on the different phonological awareness tasks
Non-significant three way interaction between group, time and test
Child syllabic awareness; rhyme awareness; phoneme analysis & synthesis demonstrated significant improvement in general
Using group as the between-subjects factor, there was a significant main effect of group directly after the intervention
Experimental group 1 made significantly more overall progress than the control group
Experimental group 2 did not differ from group 1 or the control group
18 weeks after the intervention the phonological awareness tasks were administered again and there was no longer a significant effect of group
Author’s conclusion:
Kindergarten children with SLI benefited from a short, intensive computer assisted phonological awareness intervention. Speech manipulation did not produce any additional effect.
Reviewer’s
conclusion:
A short computer assisted phonological awareness programme appeared to be beneficial for children with SLI, however the addition of speech manipulation may have actually decreased its effectiveness as these children were no different to the control group. It is also possible that the control treatment may have improved children‘s phonological skills.
The Centre for Allied Health Evidence (CAHE)
121
Summary of intervention program: Structured game formats
Reference:
Smith, C and Fluck, M 2000, ‗(Re-) constructing pre-linguistic interpersonal processes to promote language development in young children with deviant or delayed communication skills‘, British Journal of Educational Psychology, vol. 70(Pt 3), pp. 369-89.
Country of
publication:
UK
Publication type
(include level of
evidence):
Comparative study (level III-2)
Population:
20 children aged 3-5 years with limited communication skills (12 x 3-year olds attending a diagnostic nursery and 8 x 5-year old children attending a support centre for children with specific speech and language disorder attached to a mainstream school). No child had utterances longer than one word.
Service setting:
Diagnostic nursery and a support centre within a mainstream school (small group intervention).
Service delivery
model:
All children monitored for 6-month baseline prior to intervention during which they received ongoing speech and language therapy and regular small group experience
Group A received the structured intervention after this baseline period whilst group B began their baseline period, thus serving as a control group (group B later received the intervention)
Diagnostic nursery:
Inclusion model of experience in a small group setting
12 children in session (half with difficulties and half developing normally)
Staffed by teacher and 2 nursery nurses
Speech therapist attends on a half-time basis
Psychologist visits weekly
Intervention conducted according to a pre-arranged programme Speech and language support centre:
Also follows inclusion model within a regular small group structured play setting
Attached to reception class in a mainstream school
Curriculum delivered predominantly through supporting children in the mainstream class
Parents:
Given workshops and the opportunity to participate if wished Intervention:
Aimed at fostering more complex role-taking in game formats as a means of promoting social non-verbal and verbal communication
Follows specific game formats based on individual assessment of

The Centre for Allied Health Evidence (CAHE)
122
child‘s cognitive development
Phase 1 – establishing social attention (adult acts out a sequence then imitates the child‘s actions), ongoing teaching of new skills
Phase 2 – development of triadic attention and role exchange, fostering communication
Phase 3 – development of more complex role exchanges, i.e. initiator in a range of games in dyads and triads to then negotiator with small group of peers and adults in a creative game setting
Frequency/
intensity/
duration of service
provision:
Not specified
Outcomes evaluation
(by disorder subtype
if possible):
Between-participants comparison (Group A vs. Group B):
Significant effects of role, game and role x game
Highly significant main effect of phase confirmed that the intervention was associated with an improvement in the overall level of children‘s participation in social game formats
Highly significant phase x role interaction but no phase x game interaction
A significant phase x game x role interaction indicates the efficacy of the intervention was confined to particular combinations of game level and role
Significantly greater improvement in all language measures for the intervention group over the control group
Within-participants comparison (all participants as their own control):
None of the effects involving group was significant, thus they did not differ in terms of the effect of the intervention
Effects of role, game and role x game were significant
Main effect of phase was highly significant confirming that the intervention was associated with a greater overall increase in children‘s participation in social game formats
Phase x role and phase x role x game interactions were highly significant, however phase x game was not, confirming that the intervention was associated with greater improvements in the amount of game participation except at the very simplest or the most complex combinations of game level and role
Significantly more improvement in the intervention phase than the baseline phase
Summary:
The intervention significantly influenced children‘s level of participation in social game formats
The effectiveness of the intervention depended on the combination of role complexity and the cognitive game level
Game and role levels are developmentally ordered
Highly significant positive correlation between children‘s level of participation in social game formats and their improvement on language measures
Author’s conclusion:
Improvement in the level of game participation and language development was significantly greater than in the baseline or control periods. Therefore

The Centre for Allied Health Evidence (CAHE)
123
language development can be promoted in language-delayed preschool children by systematically improving their participation in socially constructed game formats.
Reviewer’s
conclusion:
It appears that language development is related to participation in socially constructed games, however the direction of causality between the two variables remains unclear.

The Centre for Allied Health Evidence (CAHE)
124
Summary of intervention program: Book sharing-sessions
Reference:
van Kleeck, A, Vander Woude, J and Hammett, L 2006, ‗Fostering literal and inferential language skills in Head Start preschoolers with language impairment using scripted book-sharing discussions‘, American Journal of Speech-Language Pathology, vol. 15, no. 1, pp. 85-95.
Country of
publication:
USA
Publication type
(include level of
evidence):
Pseudo-randomised controlled trial (level III-1)
Population:
30 children aged 3;10-5;0 years enrolled in Head Start pre-school programmes. Children had multiple risk factors that might impede their development of inferential language skills. All had language impairments and were from low socioeconomic backgrounds.
Service setting:
One northern and one southern state pre-school Head Start programmes (individual therapy).
Service delivery
model:
Both treatment and control groups continued to receive speech and language intervention services through their Head Start Programmes
Treatment group participated in book sharing sessions whereas the control group did not
Book sharing-sessions:
Provided by trained graduate and undergraduate research assistants from programmes in communication sciences and disorders
Two books by Frank Asch were used: ‗Mooncake‘ (1987) and ‗Skyfire‘ (1990)
There were 3 sets of 25 scripted questions for each book (70% were literal levels, 30% were inferential levels)
Some questions had scripted prompts
Answers to all questions were scripted
Natural confirmation provided for correct answers
Frequency/
intensity/
duration of service
provision:
15-minute sessions, twice per week, over 8 weeks
Outcomes evaluation
(by disorder subtype
if possible):
A significant group x time interaction for literal language (medium to large effect) even after controlling for group differences at baseline
Statistically significant positive change for the treatment group literal language scores, but not for the control group indicating that book sharing had a positive effect on literal language development as measured by receptive vocabulary growth
A significant group interaction for inferential language (medium to large effect)

The Centre for Allied Health Evidence (CAHE)
125
Statistically significant positive change for the treatment group inferential language scores, but not for the control group
Author’s conclusion:
Children in the book-sharing group had greater gains in literal and inferential language skills than children in a control group not receiving the intervention. Effect sizes for treatment gain on inferential language however were substantially smaller than those for literal language.
Reviewer’s
conclusion:
A book-sharing intervention in addition to standard speech and language therapy appeared to be more effective than standard speech and language therapy alone for improving inferential and especially literal language in children with language impairments and at risk of delay.

The Centre for Allied Health Evidence (CAHE)
126
Summary of intervention program: Home-based speech and language therapy
Reference:
Ward, S 1999, ‗An investigation into the effectiveness of an early intervention method for delayed language development in young children‘, International Journal of Language & Communication Disorders, vol. 34, no. 3, pp. 243-64.
Country of
publication:
UK
Publication type
(include level of
evidence):
Comparative study (level III-2)
Population:
122 very young language delayed children aged 8-21 months (divided into matched experimental and control (no treatment) groups). Infants were classified into three groups:
Group 1—where receptive and expressive delay is associated with generalized listening difficulties.
Group 2—where infants respond normally to environmental sound but fail to develop verbal comprehension. Expressive language development is in line with receptive.
Group 3—where the infants present with normal receptive language development and a delay in expressive development.
Service setting:
Home-based individual therapy
Service delivery
model:
Two speech and language therapists conducted all assessments and carried out the intervention together
Aim to facilitate normal linguistic development rather than label infants with a disability
Appropriate initial intervention was explained and demonstrated in the infant‘s home
Based on providing the infants with sufficient input of the appropriate quality in an environment in which they were able to benefit from this
Subsequent programmes were given when the items on the previous one were part of daily living, and intervention was concluded when language levels were in line with general developmental level.
REEL was re-administered when the infant had had the third programme for 4 weeks and at subsequent 4-weekly intervals if intervention was not concluded at that stage
Has similarities with some aspects of ‗milieu teaching‘, in that language is embedded in ongoing interaction between carer and infant, and multiple naturally occurring examples are used to input language forms
It differs, however, in that there is never any explicit prompting of expressive speech
Intervention is based solely on input
A specific play session of a few minutes daily, in which two or three specific activities were to be carried out

The Centre for Allied Health Evidence (CAHE)
127
Each programme also contained two or three suggestions for activities to be carried out in naturally occurring situations
Each carer received the minimum number of programme items, which was considered important in terms of acceptability of the intervention
The programme items for the three groups are cumulative Group 3:
The aim of all the programme items for this group was to change the carers‘ input to enable the infants to make the necessary auditory discriminations
Child-led shared attention
The carer imitatively models the infant ‘s sounds
Imitating environmental sounds for the purpose of increasing the infant ‘s enjoyment and interest in sounds
Repetition so that the infant hears words sufficiently frequently to enable eventual accurate recall
Group 2:
Aim to change both quantity and quality of carers‘ input to enable verbal comprehension to develop.
Promote the infant ‘s interest and enjoyment in listening to voice, by providing increased stimulus of an appropriate nature
Carer uses rhymes and ritualized vocalizations
Carer is also encouraged imitatively to model the infant‘s sounds
Concept of following the infant ‘s focus of attention is introduced to facilitate the mapping of meaning onto words
Increase the quantity both of input and interaction, and to give the infant opportunities to perceive the prosodic aspects of speech
Running commentary and modifications of adult–child speech to facilitate the child‘s comprehension
Group 1:
Objective of the first programme for this group is to enable the infant to structure the auditory field
The reduction or, if possible, elimination of background sound for part of each day is essential for these infants
Carer encourages play with noisemakers and sings or tells rhymes and action rhymes to foster the enjoyment of foreground sound in an interactive setting
The carer is encouraged to help the infant to link sounds with their sources
Increase the quantity of vocal/verbal input to the infant (the suggestion is given directly, followed by that of developing infant-led joint attention, vital in facilitating auditory attention)
Beginnings of adult–child speech modification are introduced with examples of appropriate short utterances, as is the concept of the ‗running commentary‘
Suggestion that the carer always responds to the infant ‘s communicative attempts
Suggestion that the carer not to use speech to reprimand the infant whenever possible, to remove from his environment anything that would tend to make him reluctant to listen to speech

The Centre for Allied Health Evidence (CAHE)
128
Additional items for this programme address the quality of the carer‘s input
Frequency/
intensity/
duration of service
provision:
Typically children received 4 months of intervention involving an average of four home visits by the two workers
Mean treatment time was 140 minutes from each of the 2 therapists
Infant re-visited 2 weeks after receiving the first programme, with further visits made at 4-weekly intervals
The great majority of carers reported that they spent on average ~20 minutes daily on the specific play sessions, and 5–10 minutes on the other suggested activities
2-year follow-up
Outcomes evaluation
(by disorder subtype
if possible):
At post-intervention mean receptive language quotient for the group 1 infants had risen from 65.8 to 99.8, and for group 2 from 66 to 101, with similar changes in group 3 expressive language quotients
At 1 year after initial assessment, expressive language quotients were all in line with receptive for all 3 groups
The differences in mean language quotients in experimental and control groups were significant for group 1 at both one- and two-year follow-ups
Statistical analysis was not attempted for groups 2 and 3 as the sample sizes were small
The effects of intervention had been maintained: all the infants who had received intervention were linguistically within normal limits as measured by REEL
The improvement in the experimental groups had been maintained at 2 years in all but two children in group 1 and one in group 2.
30% of the controls had been referred for speech and language therapy by the 2nd-year follow-up, while none of the experimental group had been
A considerable difference in the numbers who had been given places in local authority day nurseries: 5% of the experimental group and 24% of the controls
Author’s conclusion:
The intervention appeared effective in preventing problems at the age at which children are usually referred for speech and language therapy. All but three of the children who completed the intervention were within normal limits linguistically at 3 years of age, and a number showed language development above their chronological age. There appeared to be a sensitive period in which relatively small amounts of finely tuned appropriate intervention had a large effect.
Reviewer’s
conclusion:
The programme described above appeared to be effective in improving children‘s receptive and/or expressive language at an early age, thus perhaps preventing language delay upon school entry.
The Centre for Allied Health Evidence (CAHE)
129
Summary of intervention program: Pre-school programme
Reference:
Watson, M and Leahy, J 1995, ‗Multimodal Therapy for a Child with Development Apraxia of Speech: A Case Study‘, Child Language Teaching and Therapy, vol. 11, no. 3, pp. 264-272.
Country of
publication:
USA
Publication type
(include level of
evidence):
Case study (level IV)
Population:
One child with Developmental Apraxia of Speech (DAS) who was followed up between the ages 3;1-4;10 years. Specific oral-motor function was not documented other than that he had excessive drooling.
Service setting:
University clinic (combination of individual and group therapy)
Service delivery
model:
Pre-school programme for child with speech- and language- impaired children
One hour devoted to individual therapy
Other hour involved developing communication abilities in larger group setting
Provided by graduate and undergraduate students of communication disorders, supervised by a certified clinical supervisor
Additional summer programme (combination of individual and group therapy)
Child‘s mother was a qualified speech-language pathologist (undergraduate level)
Sign language and finger spelling were used as an immediate form of communication
Modelling and requesting imitation of signs was used to facilitate manual communication
Modelling, visual and tactile cues were used to facilitate oral motor movement for speech
Manual signing decreased as emphasis placed on oral communication
Therapy structured around reading books and telling stories
From age 5 child received private individual therapy
Frequency/
intensity/
duration of service
provision:
2 x 2 hour sessions per week
12 week blocks over approximately 2 years
Summer programme 2.5 hours per day x 5 mornings per week for 6 weeks over 2 summers
Outcomes evaluation
(by disorder subtype
if possible):
Entered school at age 5;8 years and did not qualify to receive speech and language services
Documentation of continued speech improvement through periodic language samples
Near perfect consonant articulation and ability to produce a variety of syllabic shapes however occasional vowel errors were still

The Centre for Allied Health Evidence (CAHE)
130
demonstrated and unusual prosodic patterns were often noted
Author’s conclusion:
This case study demonstrated communication growth by a child diagnosed with Developmental Apraxia of Speech. The child appeared to benefit from therapy implemented from an early age, on a fairly intensive basis. The success was felt to be due to an interaction of many variables: his desire to communicate and to use alternate communication modes; clinical intervention principles that were sensitive to the child‘s needs; and a supportive home environment.
Reviewer’s
conclusion:
This case study demonstrates how therapy can be tailored to a child‘s needs, and makes assumptions on the effective components on the service delivery.