spotlight case february 2004 delay in antibiotics— a fatal mistake
TRANSCRIPT
Spotlight Case February 2004
Delay in Antibiotics—
A Fatal Mistake

2
Source and Credits
• This presentation is based on the Feb. 2004 AHRQ WebM&M Spotlight Case in Medicine
• See the full article at http://webmm.ahrq.gov • CME credit is available through the Web site
– Commentary by: Lisa Bellini, MD, University of Pennsylvania School of Medicine
– Editor, AHRQ WebM&M: Robert Wachter, MD– Spotlight Editor: Tracy Minichiello, MD– Managing Editor: Erin Hartman, MS

3
Learning ObjectivesAt the conclusion of this educational activity, participants should be able to:
• Understand the importance of ongoing patient re-evaluation to confirm initial clinical impression
• Define the role of the attending with respect to “remote supervision”
• Outline the program director’s role in processing medical errors
• List different forums for processing medical errors

4
Case: Delay in Antibiotics
A 21-year-old woman with SLE, on long-term prednisone, presented to the ED with a few hours of fever, chills, myalgias, and vomiting. She was hypotensive, but responded to IV fluid resuscitation. A blood test revealed an elevated white count. Medical housestaff evaluated her, contacted the admitting attending by phone, and admitted her to a medical ward with a presumed diagnosis of viral syndrome vs. food poisoning.

5
Case: Delay in Antibiotics (cont.)
On the floor, the patient continued to require fluid resuscitation for blood pressure support. No antibiotics were given. In the morning, 10 hours after admission, her condition began to deteriorate. Her hypotension no longer responded to fluid boluses, and a subtle petechial rash was noted.

6
Examples of Petechial Rash
Petechiae Purpura
7
Case: Delay in Antibiotics (cont.)
At that time, the patient was examined by the attending physician. The attending suspected meningococcemia, started antibiotic therapy, and transferred the patient to the ICU. Despite initiation of antibiotics and full supportive treatment, the patient had a cardiac arrest and died.

8
What Went Wrong?
• Issues related to resident education
• Issues related to resident supervision

9
• Fund of knowledge deficit– Chronic prednisone use results in
immunocompromised state
• Error in clinical judgment– Differential diagnosis of hypotension should
have included sepsis and adrenal insufficiency
– Failure to re-consider diagnosis when hypotension persisted despite fluid challenges
Issues Related to Resident Education

10
Medical Errors Among Residents
• 254 residents surveyed regarding medical errors– 45% reported a mistake (114/254)– 22% declined to answer questions – 33% did not respond
Wu AW, et al. JAMA. 1991;265:2089-94.

11
Errors in Diagnosis33%
Prescribing29%
Evaluation21%
Communication5%
Procedural Complications
11%
Types of Medical Errors Reported Among Residents
Wu AW, et al. JAMA. 1991;265:2089-94.

12
Issues Related to Resident Supervision
• “Remote supervision”: attending physician not physically present to evaluate the patient– Contact via phone
– Dependent on housestaff clinical skills to be surrogate
– “Only as good as the information you receive”

13
Rethinking “Remote Supervision”
• Driving forces– Cost containment– Demands for improved quality of care– Work hours regulations

14
Rethinking “Remote Supervision”
• Hospitalists: individuals who practice at least 25% time in the inpatient setting– Inpatient ward is the practice venue – Available more often throughout the day
and even the night– Supervision of housestaff no longer remote
Wachter RM. Ann Intern Med. 1999;130:338-42.
15
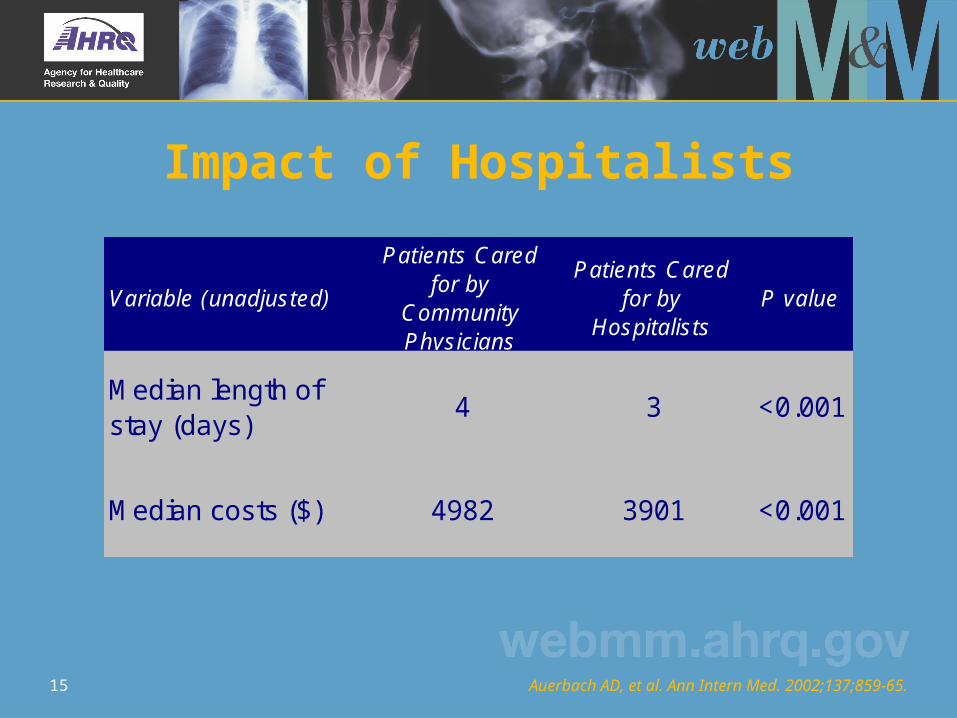
Impact of Hospitalists
Variable (unadjusted)
Patients Cared for by
Community Physicians
Patients Cared for by
HospitalistsP value
Median length of stay (days)
4 3 <0.001
Median costs ($) 4982 3901 <0.001
Auerbach AD, et al. Ann Intern Med. 2002;137;859-65.

16
Impact of Hospitalists on Mortality
Auerbach AD, et al. Ann Intern Med. 2002;137;859-65.
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
In-hospital death Death at 30 days Death at 60 days
Patients Cared for by Community Physicians Patients Cared for by Hospitalists

17
Impact of Hospitalists
• Impact of hospitalists on errors not known• One recent study revealed no impact on
presence of in-house attending trauma surgeons on mortality or length of stay
• The Leapfrog Group requires on-site intensivists as a marker of quality care in ICU; ? whether hospitalists might improve safety more generally in hospital
Arbabi S, et al. Arch Surg. 2003;138:47-51. The Leapfrog Group. October 2003.

18
Effect of Increased Supervision on Housestaff Autonomy
• Survey of residents comparing experience on traditional service vs. hospitalist service
• No significant differences were found in residents’ satisfaction with: – Relations with attending (p = 0.16)– Autonomy in management decisions (p = 0.84)– Weight given to own decisions (p = 0.8)
Chung P, et al. Am J Med. 2002;112:597-601.

19
Percentage of Residents ‘Very Satisfied’
Chung P, et al. Am J Med. 2002;112:597-601.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Relations with attending Autonomy in managementdecisions
Weight given to owndecisions
Traditional Service Hospitalist Service

20
Duty Hours Regulations
• July 2003 ACGME mandate• Resident work hours must be limited to 80
hours per week averaged over 4 weeks• No shift to exceed 24 continuous hours with
an additional 6 hours for education and transfer of care
• A minimum of 1 day off in 7
Resident duty hours: ACGME Web site.

21
Impact of Duty Hours Regulations on Attending Involvement
• Increased number of “handoffs”
• Increased dependency on attending to provide continuity of care
• Increase in implementation of non-teaching services covered by hospitalists
Morelock JA, Stern DT. Am J Med. 2003;115163-9.

22
Role of Program Director in Processing Errors
• Individual Level– Address issue with resident: is it a pattern?– Determine cause: fund of knowledge, clinical
skills, depression, substance abuse, etc.• Program Level
– Examine curriculum: create educational initiative to prevent future errors if appropriate (i.e., M&M)
• Health Care System Level– Serve as liaison between the program and the
hospital administration

23
Strategies to Address Medical Errors
• Ensure adequate supervision for housestaff• Monthly patient safety discussions at
residents’ report– Moderated by VP for quality and patient safety
• Implementation of anonymous web-based medical errors reporting system– All personnel encouraged to report errors– Information collated centrally – Systems changes implemented

24
• Residents should have multiple venues available to discuss, report, and process medical errors
• Increased supervision and less reliance on “remote supervision” may result in improved patient care
• The Program Director should play a key role in identifying and processing medical errors
Take-Home Points