spontaneous rupture of the esophagus joint hospital surgical grand round 21 april 2012 dr lee wang...
TRANSCRIPT

Spontaneous Rupture of the Esophagus
Joint Hospital Surgical Grand Round21 April 2012
Dr Lee Wang Fai FrankPrincess Margaret Hospital
Originally described in 1724 by Dutch physician Hermann Boerhaave
Classical symptoms: Forceful vomiting followed by pain, dyspnoea, shock
Spontaneous rupture of the esophagus Rare condition with high mortality rate

Barogenic rupture caused by rapid rise in intraluminal pressure in the distal esophagus
90% at the left lateral position of lower third of esophagus due to anatomic weakness at that point
Esophageal and gastric contents sucked out through the perforation into mediastinum by negative intrathoracic pressure
Chemical burn by gastric juice Super-imposed necrotizing infection due
to digestive enzymes and oral bacteria Rapid tissue destruction and severe
sepsis

Mackler's triad (<14% of patients)• Vomiting (~80%)• Lower chest pain• Subcutaneous emphysema (~25%)
Common misdiagnosis• PPU• Myocardial infarction• Pneumonia• Pulmonary embolism• Aortic dissection• Pancreatitis
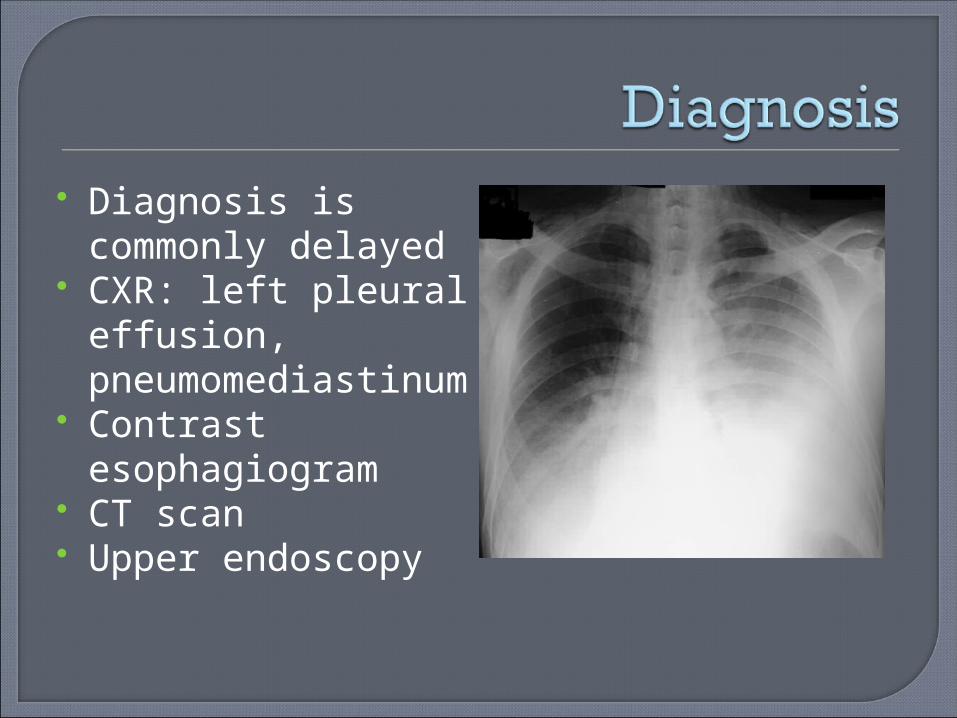
Diagnosis is commonly delayed
CXR: left pleural effusion, pneumomediastinum
Contrast esophagiogram
CT scan Upper endoscopy
Resuscitation and stabilization Elimination of infection
• Prevent further spoilage from the perforation
• Control of extraluminal contamination• Appropriate broad-spectrum antibiotics
coverage Enteric access for nutritional support Restoration of gastrointestinal
continuity

Conservative treatment Surgical treatment ("Gold standard")
• Primary closure +/- reinforcement• Drainage• Exclusion and diversion• Esophagectomy
Endoscopic treatment• Esophageal stenting• Endoclip application

Location of perforation Degree of tissue destruction Degree of contamination and sepsis Time interval from injury Presence of underlying esophageal
disorder Patient’s general condition and
comorbidities
In patients present late, with contained perforation
Patient selection• Criteria by Cameron (1970)
Minimal clinical sepsis Disruption contained in mediastinum Drainage of the cavity back into esophagus

Principles:• Restriction of oral intake• Parenteral antibiotics• Gastric acid suppresion• Fluid resuscitation• +/- Percutaneous drainage of abscess• +/- Nasogastric tube insertion
Transthoracic primary repair• “Gold standard”• Best result for patients present within 24
hours• Tension-free apposition of healthy mucosal
and submucosal tissue• +/- Reinforcement with autologous tissue,
e.g. intercostal muscle, pleural or omental flap
• Thoracotomy vs VATS

Drainage• When direct repair is thought to have high
chance of leakage• Drainage alone• +/- T-tube• Convert into controlled fistula
Exclusion and diversion• Repair may be impossible in some patients, who
present late with sepsis, heavy mediastinal contamination and devitalized esophageal tissue
• Exclusion of the esophagus Ligation of the cardia Prevent reflux of gastric content
• Diversion of oral secretions Cervical esophagostomy
• Require a second operation for restoration of gastrointestinal continuity
• Esophagus is preserved for later reconstruction
Esophagectomy• When there is heavy mediastinal
contamination and necrotized esophageal tissue beyond salvage, or when underlying esophageal pathology is suspected
• Transthoracic / transhiatal esophagectomy• Closure of cardia• Formation of cervical esophagostomy• Delayed reconstruction
Additional procedures to consider• Decompressing gastrostomy
Drainage of gastric content• Feeding jejunostomy
Facilitate early enteric feeding• Fundoplication
Prevention of reflux
Endoscopic stenting• Self-expanding metallic stent (SEMS)
Fully covered vs Partially covered• Self-expanding plastic stent (SEPS)
Effective seal of perforation
• High reported success rate (~85%)• Mean time of stent placement: 6-8 weeks• Time delay between rupture and treatment
remains most critical prognostic factor• Require concurrent adequate drainage of
fluid collection in mediastinum / pleural cavity
• Patient selection remains a topic of continued study; no guideline available currently
Complications• Stent migration (25%)
More common in fully covered stent• Tissue in-growth and over-growth
Increased difficulty in removal of stent More common in partially covered stent
No significant differences in efficacy between different types of stents
Endoscopic clipping• Limited to small clean perforations
(<1.5cm) and minimal symptoms of infection
• Early diagnosis and treatment• Reports of successful clipping of late,
mature perforation

Reported mortality varies in the literature (8-60%)
Mortality remains high and seemingly unchanged in recent 20 years
Delayed treatment is associated with higher mortality and complication rate
Multiple treatment options and operative strategies
Limited evidence in the literature on best treatment• Rare disease• Retrospective case series, case reports, expert
opinions• Reporting bias
Treatment should be individualized Early recognition and prompt treatment
are needed to maximize survival