spinal cord injuries
TRANSCRIPT

Spinal Cord InjuriesAlex Fergie – 16/4/2015

Overview
• Anatomy
• Facts/Definitions
• Mechanisms and Spinal Cord Syndromes
• How to examine pts with spinal cord injuries
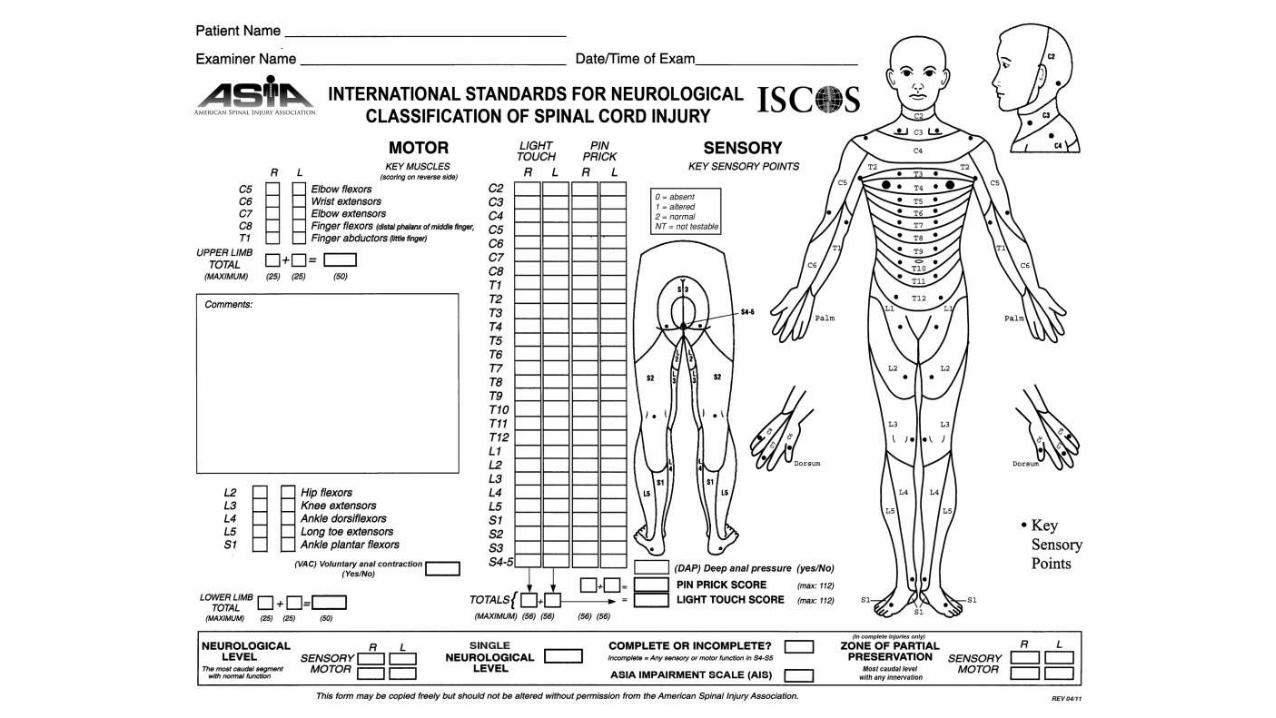
• ASIA chart
• Management in the ED
• Steroids
• Vertebral #s quiz
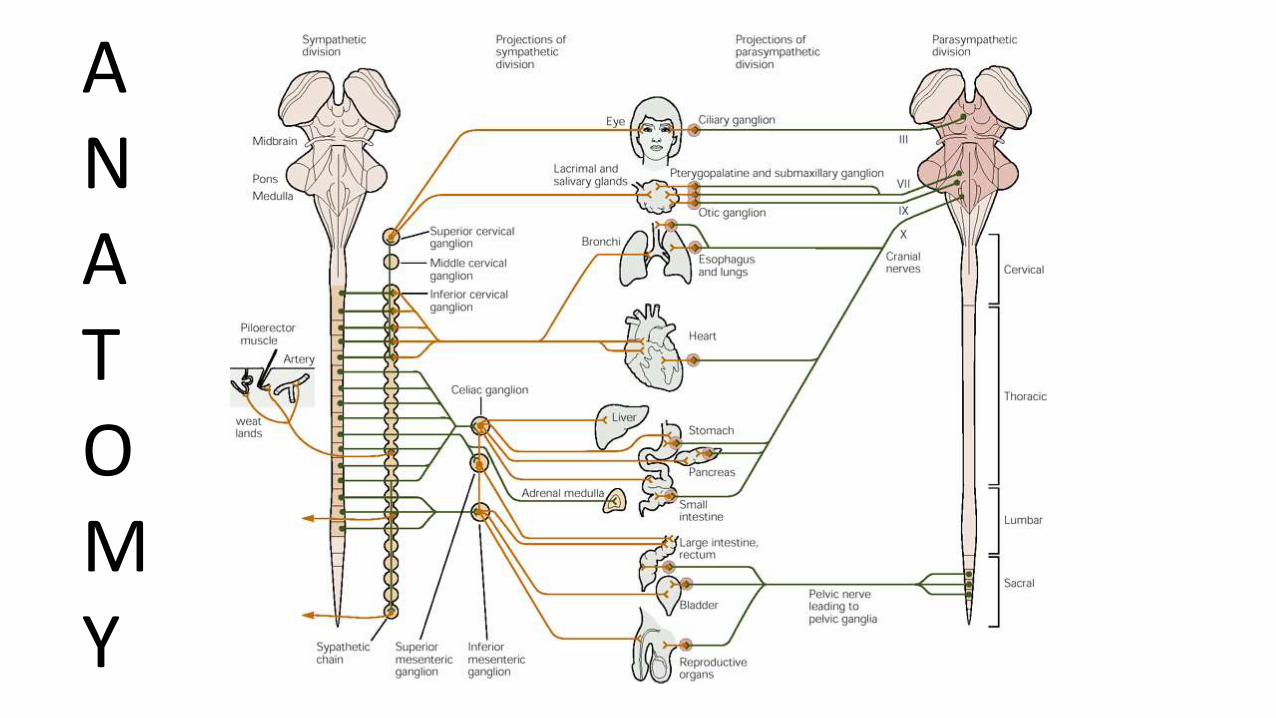
ANATOMY


FACTS• Men 85% > women 15%
• Ages 16-30
• TRAUMA (US)= MVA (40%), Violence (22%), Falls (22%), Sports –diving, horse-riding (8%),
• In Australia >50% due to MVAs – the rest on Australia day (pool/beach)
• Non-trauma = malignancy, infection (TB, epidural abscess), vascular (x-clamping aorta)
• Cord Injuries: Cervical = 60%, Thoracic = 30%, lumbar = 4%, and Sacral = 2%
• Most common at C5,6,7 due to greatest mobility at these levels
• 10% of vertebral # will have another (sometimes distal) #. “when thinking the spine, think the whole spine”
• The pt with a spinal cord injury will usually have other devastating injuries –therefore cord injuries are to be found on the secondary survey

Definitions• Primary vs Secondary (hypoxia, hypotension, movement and inflammation).
• Complete vs Incomplete (preservation of any sensory or motor function –esp. sacral sparing = big toe flexion, perianal sensation and bulbocavernosusreflex)
• “Spinal shock” = transient loss of function below the level of injury
• “Neurogenic Shock” = functional sympathomectomy, ↓BP & ↓HR (not responsive to IVH)
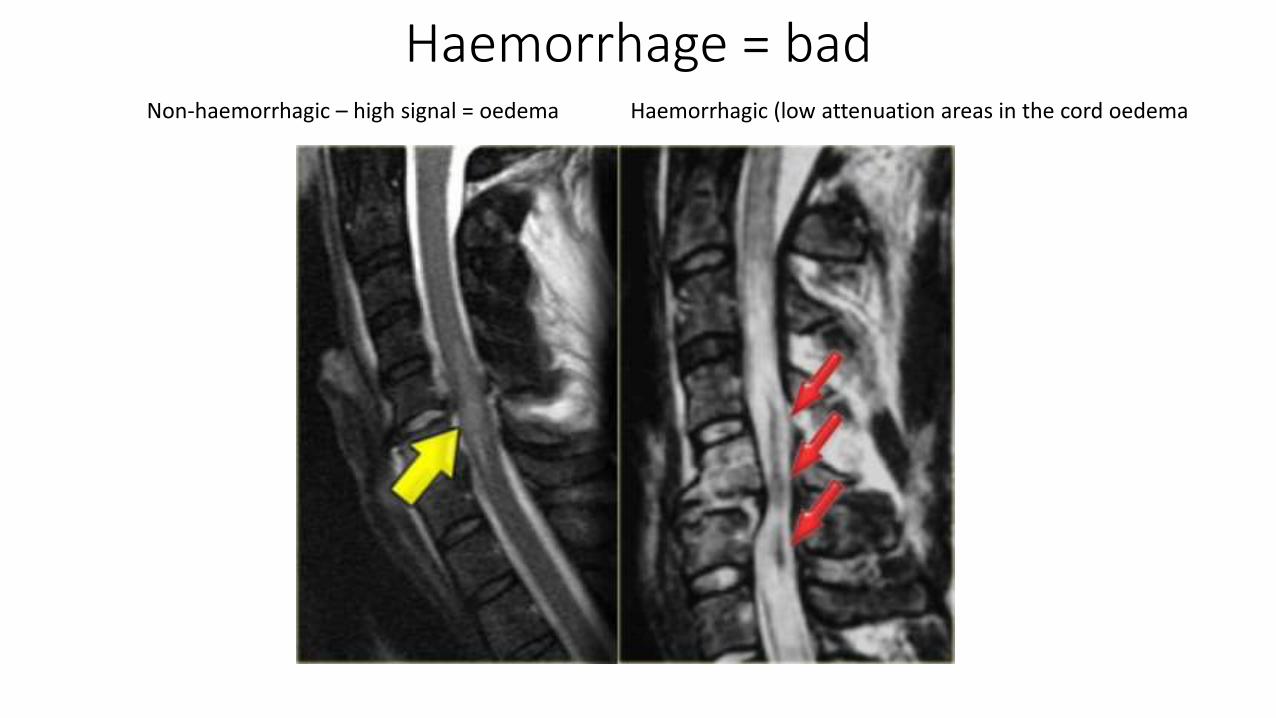
Haemorrhage = badNon-haemorrhagic – high signal = oedema Haemorrhagic (low attenuation areas in the cord oedema

Haemorrhage = bad
The chart on the left is showing the motor recovery rate for patients with oedema alone (in blue) vs oedema plus cord haemorrhage (in red). The motor recovery rate is for the legs only

Length of cord injury
Long = badNot so long = not so bad

Cord Syndromes – incomplete (some sensory/motor function retained)
• Central Cord Syndrome - hyperextension
• Anterior Cord Syndrome – flexion/rotation
• Brown-Séquard Syndrome – knife in the back
• Posterior Cord Syndrome – rare. Hyperextension/knife
• Cord Concussion = full resolution within 48hrs

Hyperextension


Central cord Syndrome
• Hyperextension
• Old people
• Osteophytes
• Motor: Arm > Leg weakness
• Sensory: Arms>Legs
• Reflexes: may vary
• Usually sacral sensory sparing

Hyperflexion Injuries
Retropulsed C5-6 disc. Oedema posteriorly. Ruptured ligamentum flavum and interspinous ligament.

Anterior Cord Syndrome
• anterior spinal artery compressed by bone fragments
• Primarily affects motor – paralysis• Can involve corticospinal tracts• Rarely involves dorsal columns• Can occur with AAA and x-clamping
of the aorta

Brown-Séquard
Stab wound with a screwdriver
• Rare• Knife in back or rotational or
fracture/dislocation• Ipsilateral motor loss
(corticospinal)• Contralateral sensory
(pain/temp) loss (spinothalamic)
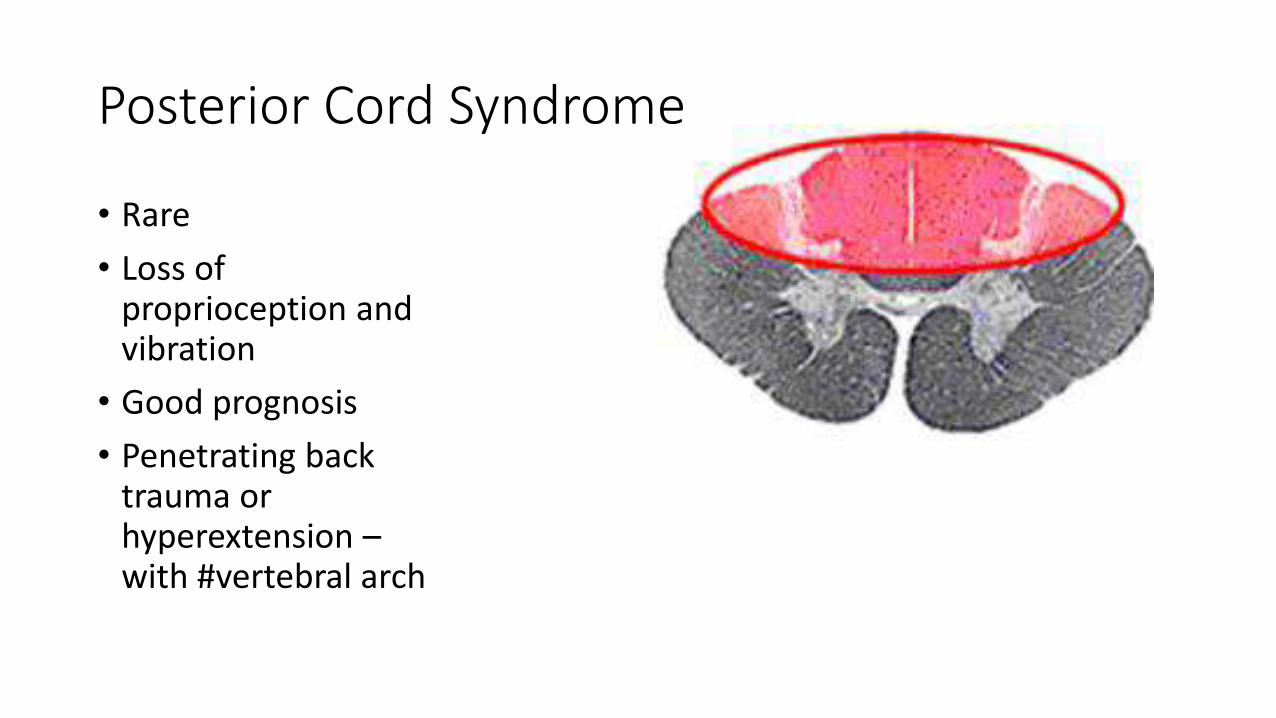
Posterior Cord Syndrome
• Rare
• Loss of proprioception and vibration
• Good prognosis
• Penetrating back trauma or hyperextension –with #vertebral arch

Cauda Equina Syndrome
• Not a cord syndrome. Technically a LMN lesion.
• LMN lesion = loss of knee reflexes. Leg weakness
• Bladder/bowel dysfunction
• Saddle anaesthesia
• Loss of anal tone
• Sexual dysfunction
• CES mainly affects middle-aged individuals, particularly those in their forties and fifties, and presents more often in men
SCIWORA (spinal cord injury without radiological abnormality)
• Dx = no bony or ligamentous injury on x-ray or CT
• With MRI real “SCIWORA” is rare.
• There is usually cord/ligament injury on MRI
• More common in children – spine more flexible and less likely to #
• Typically in the cervical region

How to examine a trauma pt. in ED• Primary survey first
• Cord and vertebral injuries will be picked up on 2° survey
• Tell everybody there is a risk of this patient having a spinal injury
• Remove from trauma board
• Head – toe approach
• Look – head, neck, mouth (prevertebral haematoma), paradoxical breathing, lap seatbelt sign, gross deformity, priapism usually reflects a complete cord injury, bilateral horner’s syndrome (>T1 and sometimes >T4)
• Feel – feel along the midline of the neck – feeling for deformity and areas of maximal tenderness. Log Roll - ?90° ?20°
• Examine each modality separately. Head – neck – upper limbs – torso – lower limbs
• Motor – grading /5
• Sensory – soft touch (dorsal columns) and pain (spinothalamic). ?just pain?
• Reflexes – especially anal tone
• Documentation….

Print out the ASIA chart


Management in the ED• ABC approach.
• A - Intubation will be affected by a hard collar – take it off - inline immobilization. Use a video laryngoscope (proven to cause less movement)
• B – watch for paradoxical breathing (paralysed chest wall unassisted diaphragm)- Passive regurgitation and aspiration – early NG tube.- Intubate early to protect fatigue or ascending paralysis due to oedema
• C – Hypotension/brady - If no response to 2L NS (blood if bleeding) start inotropes. MAP ≥60.
• D – associate with signification head injury – CT
• E – Poikilothermic (monitor temperature).
• Other – Analgesia, Urinary retention, Ileus, antiemetics, pressure area (c-collar),

Imaging
• X-rays are crap. If you think they’ve got an injury – CT/MRI
• CT everything first – whilst arranging the MRI
• This is an emergency – like code STEMI – “Code MRI” and active the MRI team (call the duty consultant if there’s any issues)
Methylprednisolone
• Cochrane 2012 found that methylprednisolone within 8 hrs gave a significant recovery of motor function
• Contraindications: heavily contaminated wounds, bowel perforation , sepsis
• Considerations: T2DM, effects on BSL, peptic ulcer risk
• In Australia, spinal cord injury is not listed as an indication for high-dose methyl pred.
• Decision to use steroids should be made in consultation with the spinal specialist.
• Please give it to me if I come in with a cord injury


Other stuff to know about
• Cruciate Paralysis of Bell = odontoid rams into the cord = paralysis of one arm and the opposite leg
• Conus Medullaris Syndrome: may have some UMN signs (increased tone and hyperreflexia). Differentiating between cauda equinasyndrome and CMS doesn’t matter - Still an emergency – needs MRI and neurosurgery.
Fun Fellowship Exam Facts• SCIWORA more common in children
• Can use Sux in first 12-24hrs but use Roc (1.2mg/kg).
• 10% of unconscious trauma pts have a significant vertebral injury
• Teardrops #s: stable in flexion but highly unstable in extension
• A patient can be ambulant with an unstable injury
• C-collars raise ICP and don’t provide any clinical benefit in the conscious patient (except to alert medical staff to the possibility of an injury). Exchange them for softer collars (Philli etc..)
• Pre-vertebral soft tissue swelling rules = in adults this should be <7 mm at C2 or <22 mm at C6/7. Children this is said to be <14 mm at C6.
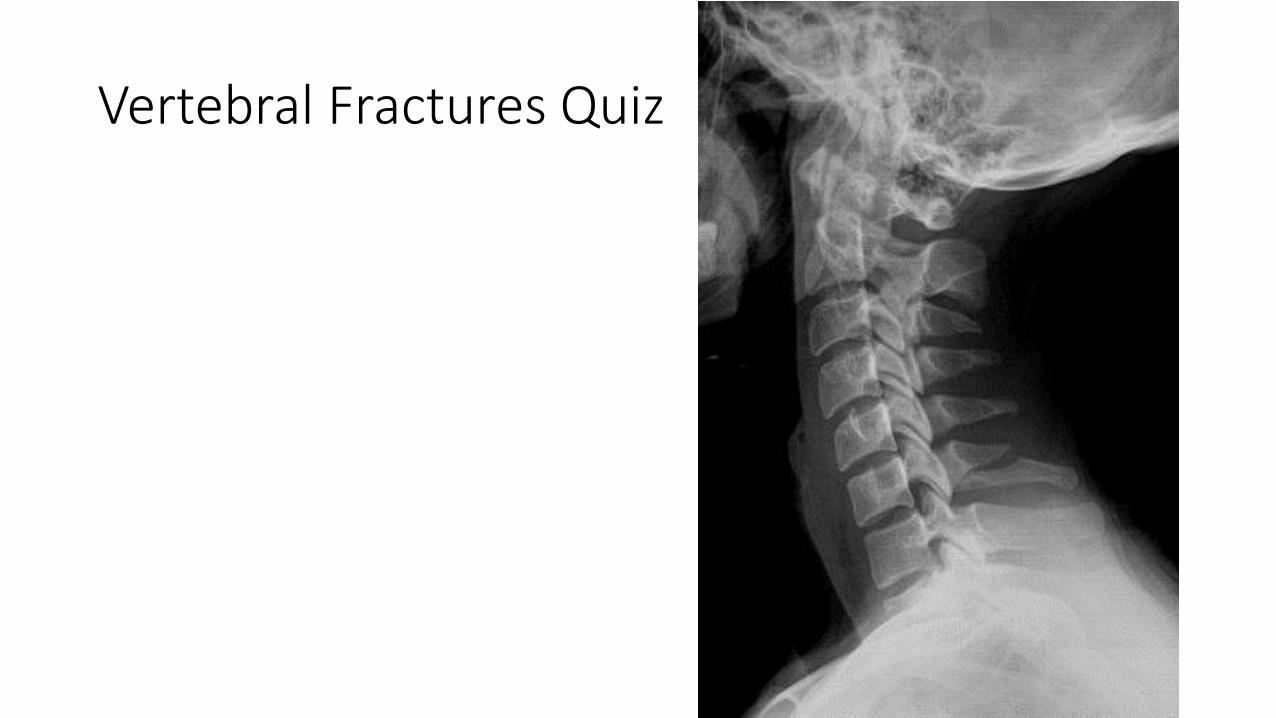
Vertebral Fractures Quiz






