spigelian hernia- a rare abdominal hernia: a case reporttheantiseptic.in/uploads/medicine/spigelian...
TRANSCRIPT

November 201638 THE ANTISEPTIC
Spigelian Hernia- A Rare Abdominal Hernia: A Case ReportJAGADANANDA MISHRA, ASISO KUMAR PRADHAN, HIMANSU SHEKHAR MISHRA
Jagadananda Mishra, Associate professor,Asiso Kumar Pradhan, Assistant professor,Himansu Shekhar Mishra, PG student, Department of General Surgery, VSS Institute of Medical Sc. and Research, Burla, Odisha, India
Specially Contributed to "The Antiseptic" Vol. 113 No. 11 & P : 38 - 40
ABSTRACT
Spigelian hernias arise through a defective spigelian fascia which is the aponeurosis of transverse abdominis muscle that lies between the semi lunar line and the lateral rectus muscle. The absence of typical hernial symptoms, elusive abdominal complaint and lack of consistent physical findings categorise the disease as an under-diagnosed and rare entity. Over here, the case of a 60 year old female patient was presented with a lower abdominal non tender swelling associated with colicky lower abdominal pain. Spigelian hernia was diagnosed and confirmed through exploration. She underwent a surgical schedule with reduction of hernia and onlay prolene mesh repair followed by an uneventful recovery.Keywords: Spigelian hernia, Abdominal wall, Mesh repair.
Introduction
Spigelian hernia, also known as spontaneous lateral ventral hernia, is a protrusion of preperitoneal fat or a sac of peritoneum or an organ through a defect or weakness in spigelian fascia1. It was named after the Belgian anatomist van den Spieghel, who was the first to describe the semilunar line in 16452 and Klinkosh, in1764, first recognized it3. It comprises of 0.12–2.4% of all abdominal wall hernias that have been reported in the world literature2. These hernias advance through the internal oblique, but spread out deep to external oblique aponeurosis, hence also called as interparietal, interstitial, intermuscular, intramuscular or intra-mural hernia. The majority of spigelian hernias are found in a transverse band lying within 6 cms cranial to a line running between both anterior superior iliac spines referred to as the spigelian hernia belt where the spigelian fascia is the widest4. Spigelian hernia can be congenital or acquired5. The etiology of Spigelian hernias is thought to be the result of
fascial weakness associated with perforating vessels. It also may be due to previous abdominal operations that cause weakening of the semilunar line. Increased pressure on the abdominal wall aponeurosis due to conditions like prostate enlargement, previous surgery, obesity, chronic bronchopathy, multiparity and constipation, are predisposing factors for development of Spigelian hernia6.
After clinical examination, ultrasonography and computerized tomography (CT) scan of the abdomen confirms the diagnosis. Once diagnosed, Spigelian hernias require operative repair.Case report
A 60 yr old obese female patient from Sambalpur presented with a painful swelling in left lower abdomen for 7 months. Swelling was gradually progressive to attain present size. The swelling was prominent on standing and after exercise, disappearing on lying down position. Bladder & bowel habit were normal.
On examination, previous hysterectomy scar was found. There was a swelling of size 5cm x 6cm in left iliac fossa which was nontender, smooth; impulse on coughing was present, decreased on lying down position.
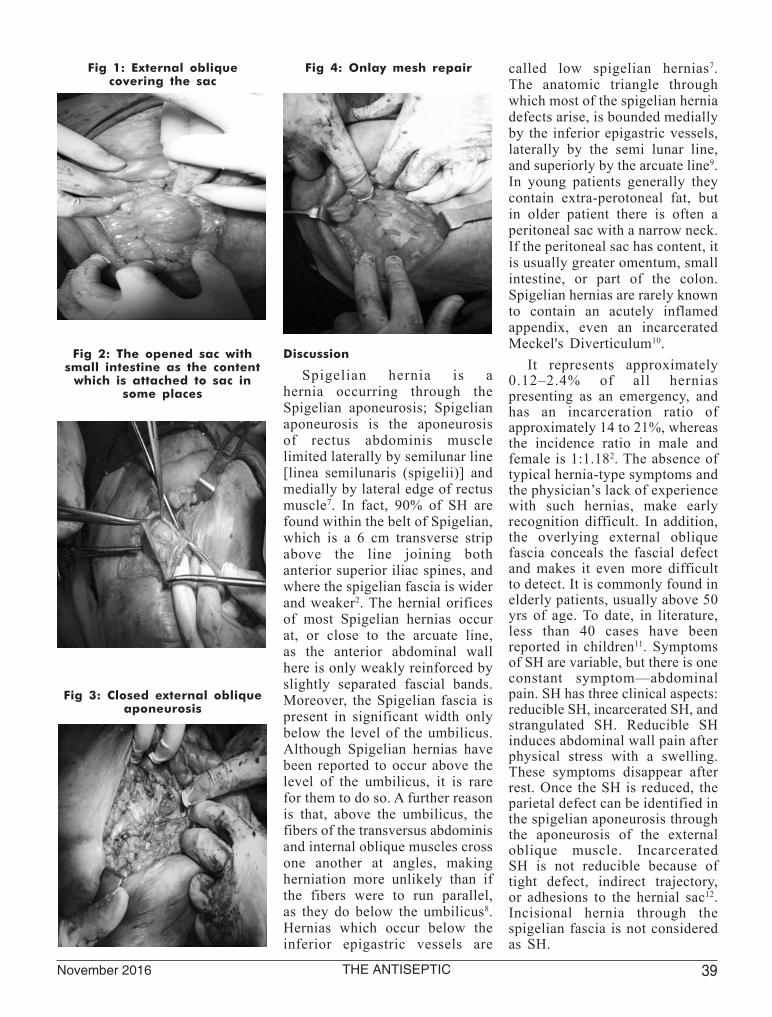
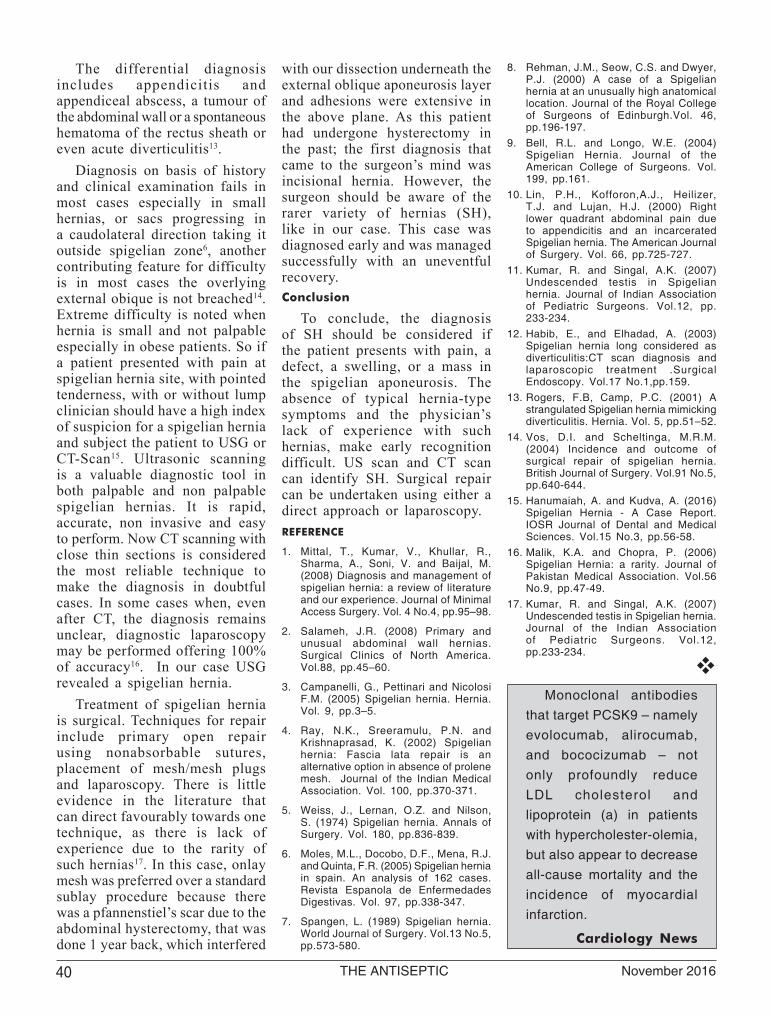
Straight X-ray abdomen shows no air fluid level to suggest intestinal obstruction. USG report revealed a defect of size 4 cm in left iliac fossa with bowel and omental contents. After adequate preparation she was taken for surgery. Transverse incision was given above the swelling under spinal anaesthesia. A defect was found along the lateral border of rectus sheath with a thin layer of external oblique intact over it (Fig-1). Incision was given over the external oblique, sac was identified. The defect was found to be of 3cm X 3cm in the musculoaponeuritic sheath of internal oblique & transverse abdominis muscle. The sac was opened after mobilization (Fig-2). There was herniation of omentum & small intestine which were adherent to wall of the sac in some places. Small intestine was viable. Adhesiolysis was done. The redundant sac was excised & closed with vicryl (2-0). External oblique aponeurosis was closed with prolene (1-0), (Fig-3). Onlay mesh repair was done with a prolene mesh of size (7.5cmx7cm) which was fixed over the external oblique (Fig-4). Bilateral closed drain was given, which was removed after 48 hours. Stitches ware removed after 10 days. Postoperatively patient’s recovery was uneventful.
39 THE ANTISEPTIC November 2016
Discussion
Spigelian hernia is a hernia occurring through the Spigelian aponeurosis; Spigelian aponeurosis is the aponeurosis of rectus abdominis muscle limited laterally by semilunar line [linea semilunaris (spigelii)] and medially by lateral edge of rectus muscle7. In fact, 90% of SH are found within the belt of Spigelian, which is a 6 cm transverse strip above the line joining both anterior superior iliac spines, and where the spigelian fascia is wider and weaker2. The hernial orifices of most Spigelian hernias occur at, or close to the arcuate line, as the anterior abdominal wall here is only weakly reinforced by slightly separated fascial bands. Moreover, the Spigelian fascia is present in significant width only below the level of the umbilicus. Although Spigelian hernias have been reported to occur above the level of the umbilicus, it is rare for them to do so. A further reason is that, above the umbilicus, the fibers of the transversus abdominis and internal oblique muscles cross one another at angles, making herniation more unlikely than if the fibers were to run parallel, as they do below the umbilicus8. Hernias which occur below the inferior epigastric vessels are
called low spigelian hernias7. The anatomic triangle through which most of the spigelian hernia defects arise, is bounded medially by the inferior epigastric vessels, laterally by the semi lunar line, and superiorly by the arcuate line9. In young patients generally they contain extra-perotoneal fat, but in older patient there is often a peritoneal sac with a narrow neck. If the peritoneal sac has content, it is usually greater omentum, small intestine, or part of the colon. Spigelian hernias are rarely known to contain an acutely inflamed appendix, even an incarcerated Meckel's Diverticulum10.
It represents approximately 0.12–2.4% of all hernias presenting as an emergency, and has an incarceration ratio of approximately 14 to 21%, whereas the incidence ratio in male and female is 1:1.182. The absence of typical hernia-type symptoms and the physician’s lack of experience with such hernias, make early recognition difficult. In addition, the overlying external oblique fascia conceals the fascial defect and makes it even more difficult to detect. It is commonly found in elderly patients, usually above 50 yrs of age. To date, in literature, less than 40 cases have been reported in children11. Symptoms of SH are variable, but there is one constant symptom—abdominal pain. SH has three clinical aspects: reducible SH, incarcerated SH, and strangulated SH. Reducible SH induces abdominal wall pain after physical stress with a swelling. These symptoms disappear after rest. Once the SH is reduced, the parietal defect can be identified in the spigelian aponeurosis through the aponeurosis of the external oblique muscle. Incarcerated SH is not reducible because of tight defect, indirect trajectory, or adhesions to the hernial sac12. Incisional hernia through the spigelian fascia is not considered as SH.
Fig 1: External oblique covering the sac
Fig 2: The opened sac with small intestine as the content
which is attached to sac in some places
Fig 3: Closed external oblique aponeurosis
Fig 4: Onlay mesh repair
November 201640 THE ANTISEPTIC
The differential diagnosis includes appendicitis and appendiceal abscess, a tumour of the abdominal wall or a spontaneous hematoma of the rectus sheath or even acute diverticulitis13.
Diagnosis on basis of history and clinical examination fails in most cases especially in small hernias, or sacs progressing in a caudolateral direction taking it outside spigelian zone6, another contributing feature for difficulty is in most cases the overlying external obique is not breached14. Extreme difficulty is noted when hernia is small and not palpable especially in obese patients. So if a patient presented with pain at spigelian hernia site, with pointed tenderness, with or without lump clinician should have a high index of suspicion for a spigelian hernia and subject the patient to USG or CT-Scan15. Ultrasonic scanning is a valuable diagnostic tool in both palpable and non palpable spigelian hernias. It is rapid, accurate, non invasive and easy to perform. Now CT scanning with close thin sections is considered the most reliable technique to make the diagnosis in doubtful cases. In some cases when, even after CT, the diagnosis remains unclear, diagnostic laparoscopy may be performed offering 100% of accuracy16. In our case USG revealed a spigelian hernia.
Treatment of spigelian hernia is surgical. Techniques for repair include primary open repair using nonabsorbable sutures, placement of mesh/mesh plugs and laparoscopy. There is little evidence in the literature that can direct favourably towards one technique, as there is lack of experience due to the rarity of such hernias17. In this case, onlay mesh was preferred over a standard sublay procedure because there was a pfannenstiel’s scar due to the abdominal hysterectomy, that was done 1 year back, which interfered
with our dissection underneath the external oblique aponeurosis layer and adhesions were extensive in the above plane. As this patient had undergone hysterectomy in the past; the first diagnosis that came to the surgeon’s mind was incisional hernia. However, the surgeon should be aware of the rarer variety of hernias (SH), like in our case. This case was diagnosed early and was managed successfully with an uneventful recovery. Conclusion
To conclude, the diagnosis of SH should be considered if the patient presents with pain, a defect, a swelling, or a mass in the spigelian aponeurosis. The absence of typical hernia-type symptoms and the physician’s lack of experience with such hernias, make early recognition difficult. US scan and CT scan can identify SH. Surgical repair can be undertaken using either a direct approach or laparoscopy.REFERENCE
1. Mittal, T., Kumar, V., Khullar, R., Sharma, A., Soni, V. and Baijal, M. (2008) Diagnosis and management of spigelian hernia: a review of literature and our experience. Journal of Minimal Access Surgery. Vol. 4 No.4, pp.95–98.
2. Salameh, J.R. (2008) Primary and unusual abdominal wall hernias. Surgical Clinics of North America. Vol.88, pp.45–60.
3. Campanelli, G., Pettinari and Nicolosi F.M. (2005) Spigelian hernia. Hernia. Vol. 9, pp.3–5.
4. Ray, N.K., Sreeramulu, P.N. and Krishnaprasad, K. (2002) Spigelian hernia: Fascia lata repair is an alternative option in absence of prolene mesh. Journal of the Indian Medical Association. Vol. 100, pp.370-371.
5. Weiss, J., Lernan, O.Z. and Nilson, S. (1974) Spigelian hernia. Annals of Surgery. Vol. 180, pp.836-839.
6. Moles, M.L., Docobo, D.F., Mena, R.J. and Quinta, F.R. (2005) Spigelian hernia in spain. An analysis of 162 cases. Revista Espanola de Enfermedades Digestivas. Vol. 97, pp.338-347.
7. Spangen, L. (1989) Spigelian hernia. World Journal of Surgery. Vol.13 No.5, pp.573-580.
8. Rehman, J.M., Seow, C.S. and Dwyer, P.J. (2000) A case of a Spigelian hernia at an unusually high anatomical location. Journal of the Royal College of Surgeons of Edinburgh.Vol. 46, pp.196-197.
9. Bell, R.L. and Longo, W.E. (2004) Spigelian Hernia. Journal of the American College of Surgeons. Vol. 199, pp.161.
10. Lin, P.H., Kofforon,A.J., Heilizer, T.J. and Lujan, H.J. (2000) Right lower quadrant abdominal pain due to appendicitis and an incarcerated Spigelian hernia. The American Journal of Surgery. Vol. 66, pp.725-727.
11. Kumar, R. and Singal, A.K. (2007) Undescended testis in Spigelian hernia. Journal of Indian Association of Pediatric Surgeons. Vol.12, pp. 233-234.
12. Habib, E., and Elhadad, A. (2003) Spigelian hernia long considered as diverticulitis:CT scan diagnosis and laparoscopic treatment .Surgical Endoscopy. Vol.17 No.1,pp.159.
13. Rogers, F.B, Camp, P.C. (2001) A strangulated Spigelian hernia mimicking diverticulitis. Hernia. Vol. 5, pp.51–52.
14. Vos, D.I. and Scheltinga, M.R.M. (2004) Incidence and outcome of surgical repair of spigelian hernia. British Journal of Surgery. Vol.91 No.5, pp.640-644.
15. Hanumaiah, A. and Kudva, A. (2016) Spigelian Hernia - A Case Report. IOSR Journal of Dental and Medical Sciences. Vol.15 No.3, pp.56-58.
16. Malik, K.A. and Chopra, P. (2006) Spigelian Hernia: a rarity. Journal of Pakistan Medical Association. Vol.56 No.9, pp.47-49.
17. Kumar, R. and Singal, A.K. (2007) Undescended testis in Spigelian hernia. Journal of the Indian Association of Pediatric Surgeons. Vol.12, pp.233-234.
Monoclonal antibodies
that target PCSK9 – namely evolocumab, alirocumab, and bococizumab – not only profoundly reduce LDL cholesterol and lipoprotein (a) in patients with hypercholester-olemia, but also appear to decrease all-cause mortality and the incidence of myocardial infarction.
Cardiology News