southern med review - medical and health sciences€¦ · pj ballantyne associate ... babar zu....
TRANSCRIPT

Southern MedReview
Volume 4 Issue 1 April 2011
ISSN 1174-2704
An International Journal to Promote Pharmaceutical Policy Research
Social pharmacy: borrowing tools and theories the world over
Medicines use and access research: diverse methodologies show a complex picture requiring our attention
A history of medicines use in rural Nepal
Pharmaceutical situation in Afghanistan
A critical review of pharmacists’ impacts in primary health care
Medicines use in Cameroon
Selection of essential medicines in China
An International Journal to Promote Pharmaceutical Policy Research
Southern MedReview
Editor-in-Chief
Z. Babar
Guest Editor
PJ Ballantyne
Associate Editors
S. Scahill
A. Tahira
Editorial SupportE.C.L. Cazedey
H. Håkonsen
S. Jamshed
A. Hussain
Graphic Designer
J. Allen
Technical Support
S. Chen
International advisory boardAgnes Vitry
Senior Research Fellow, School of Pharmacy, University of South Australia, Australia
Albert Wertheimer
Professor, School of Pharmacy, Temple University, Philadelphia, USA
Andy Gray
Senior Lecturer, Nelson R Mandela School of Medicine, University of KwaZulu-Natal,
South Africa
Anwar Gilani
Professor of Pharmacology, The Aga Khan University, Karachi, Pakistan
Bruce Scoggins
Former Chief Executive, Health Research Council (HRC), New Zealand
Dzulkifli Abdul Razak
Vice Chancellor, Universiti Sains Malaysia, Penang, Malaysia
Herida Regina Nunes Salgado
Universidade Estadual Paulista Rodovia Araraquara, Araraquara, Brazil
Janie Sheridan
Associate Professor, School of Pharmacy, The University of Auckland, Auckland,
New Zealand
K Balasubramaniam
Coordinator, Health Action International Asia Pacific (HAIAP),Colombo, Sri Lanka
Kirsten Myhr
Head, RELIS Drug Info and Pharmacovigilance Centre, Oslo, Norway
Margaret Ewen
Coordinator, Global Projects (Pricing) Health Action International Global, Amsterdam,
Netherlands
Mohamed Izham Mohamed Ibrahim
Professor, College of Pharmacy, Al Qassim University, Al Qassim, Saudi Arabia
Nadeem Irfan Bukhari
Assistant Professor, College of Pharmacy, University of the Punjab, Lahore, Pakistan
Peri Ballantyne
Professor of Sociology, Trent University, Ontario, Canada
Sanjay Garg
Associate Professor, School of Pharmacy, The University of Auckland, Auckland,
New Zealand

An International Journal to Promote Pharmaceutical Policy Research
Southern MedReview
Context: In developing countries where health systems and health policy
are constantly evolving, there is a great need to publish informative research.
However, there are few avenues to do so. Also, some of the other challenges
are inexperienced or untrained researchers, topics out of the scope of current
mainstream journals and limited funding.
Aims and Objectives: Southern Med Review provides a platform for researchers
to disseminate commentary and empirical research findings, with a view to
improve the rational use of and access to essential medicines.
About the Journal: The Southern Med Review is an independent, open access,
not for profit, peer reviewed journal which is published 2 times a year from
Auckland, New Zealand. If you have interesting work to share, please contact the
editor: [email protected] or [email protected].
The Editor and Publisher of Southern Med Review is Zaheer Babar PhD, School of
Pharmacy, University of Auckland. Auckland, New Zealand. The journal’s financial
transactions are managed by Auckland UniServiced Ltd, Auckland, New Zealand.
The “Southern Med Review” can be distributed freely; however no part can be
copied without the permission of the Editor. The opinions and interpretations
expressed herein by the authors are their own and do not necessarily reflect those
of the publisher, editors, or organizations with which they are affiliated. Southern
Med Review (ISSN: 1174-2704) – All rights reserved, Copyright @2011.
Southern Med Review welcomes feature articles, research papers, learning in
practice, pharmacy in our part of the world, policy briefs, letters to the editor and
other forms of scholarship. All forms of articles should be within the range of
6000 words. Articles must be submitted in Vancouver Style, which is a numerical
style that follows the rules established by the International Committee of Medical
Journal Editors (http://www.icmje.org/).
Indexing and Abstracting: The journal is indexed in Scopus, CrossRef, EMBASE,
Directory of Open Access Journals (DOAJ), EBSCO Host, Open J Link, Gale, Global
Health, CAB Abstract Databases, Ulrich’s Periodical Directory and in New Zealand’s
National Library. Articles are also deposited in the WHO’s Essential Medicines
Documentation Database. The journal is also freely available from the Journal’s
website www.southernmedreview.org or from the University of Auckland’s
website www.fmhs.auckland.ac.nz/sop/smr

An International Journal to Promote Pharmaceutical Policy Research
Southern MedReview
Contents
Social Pharmacy: borrowing tools and theories the world over 1Shane Lindsay Scahill, Zaheer-Ud-Din Babar
Medicines use and access research: diverse methodologies show a complex picture requiring our attention 2Peri Joanne Ballantyne
Mountains and medicines: history and medicines use in rural Nepal 4Susan Heydon
Sociocultural, economic and regulatory influences on medicine use by consumers in a rural township in Cameroon 9Robert Chapchet Chana, Hazel Bradley
Assessing pharmacists’ impacts in primary health care: are we asking the right questions? 17Peri Joanne Ballantyne
The selection of essential medicines in China: progress and the way forward 22Difei Wang, Xinping Zhang
Afghanistan pharmaceutical sector development: problems and prospects 29Jonathan Harper, Gunnar Strote
Performance based reward for immunization: experiences from GAVI 40Rete Trap, Birna Trap, Torsten Wind Hansen, Ebba Holme Hansen

1 Southern Med Review Vol 4 Issue 1 April 2011
Editorial
Social Pharmacy: borrowing tools and theories the world over Citation: Scahill SL, Babar ZU. Social Pharmacy: borrowing tools and theories the world over. Southern Med Review (2011) 4;1:1doi:10.5655/smr.v4i1.78
questions. Second, it provides an impetus for countries in the
Global South to view “medicines” in their totality, as part of
the wider health system, rather than just “isolated chemical
entities”. Increasingly pharmacy schools in low income countries
are teaching social pharmacy concepts7 and there is a greater
call for the strengthening of Social Pharmacy before establishing
clinical pharmacy practice8.
We are cognizant that there are three main mechanisms by
which the Social Pharmacy discipline can “spread the word”and
“show the value” in the broadest sense. Teaching, research
and partnering with or gaining support from significant non-
government organisations (NGO’s) such as the World Health
Organisation (WHO) are the main mechanisms cited in the
literature1. Apart from teaching and learning of Social Pharmacy,
more work needs to be undertaken to improve the other two
mechanisms of internationalization of our discipline; research
dissemination and development of partnerships.
Shane Lindsay Scahill, BPharm, MMgt
Zaheer-Ud-Din Babar, PhD
School of Pharmacy, University of Auckland, Auckland,
New Zealand
References1. Norris PT. Challenges facing social pharmacy. Research in Social
and Administrative Pharmacy. 2009;5(3):195-196.
2. Bissell P, Morgall Traulsen J. Sociology and Pharmacy Practice. 1st ed. London: Pharmaceutical Press; 2005.
3. About Social Pharmacy, Faculty of Pharmacy, Universitetet I Oslo, Norway. Available at, http://www.farmasi.uio.no/seksjoner/farmasoytisk/english.html. Accessed 23rd March 2011.
4. Department of Social Pharmacy, Faculty of Pharmacy, University of Kuopio, Finland. Available at, http://www.uku.fi/farmasia/sofa/english/. Accessed 23rd March 2011.
5. Section for Social Pharmacy, Faculty of Pharmaceutical Sciences, University of Copenhagen, Denmark. Available at, http://www.farma.ku.dk/index.php?id=181. Accessed 23 March 2011.
6. Babar Z, Beswick T. Southern Med Review: A New Forum to Publish “Local Pharmaceutical Policy in a Global Context”. Pharmacy World & Science. 2009;31(2):143.
7. Clinical and Social Pharmacy, Faculty of Pharmaceutical Sciences, Kwame Nkrumah University of Science and Technology, Ghana.Available at, http://www.knust.edu.gh/pages/sections.php?siteid=pharmacy&mid=607&sid=1827. Accessed 23rd March 2011.
8. Babar Z, Jamshed S. Social pharmacy strengthening clinical pharmacy: why pharmaceutical policy research is needed in Pakistan? Pharmacy World & Science. 2008;30(5):617.
There is no denying that challenges lay ahead for the discipline
of Social Pharmacy. These challenges are both considerable
and global; requiring the involvement of fraternities from both
academia and practice. To date, high income countries adopting
the western research paradigm have informed these challenges.
They centre on improving practice, teaching and research
through the application of knowledge and theories from other
disciplines1.
Beginning to think like those who trained outside of conventional
pharmacy, and applying accepted theoretical frameworks
requires a shift in thought, along with considerable time and
energy. Sustainable research streams within our emerging
discipline of Social Pharmacy need to be structured upon what
we need to know, but equally upon approaches that have gone
before us by other disciplines. Since the mid 1960’s the umbrella
of academic pharmacy has developed from a predominantly
science based paradigm to include a much broader view of the
world2. This has been achieved through the study of medicines
in society and the term “Social Pharmacy” was coined.
Social Pharmacy researchers based in the western world have
borrowed tools and theories from the social sciences including:
anthropology, sociology, history, economics and organizational
science in order to answer complex questions relating to society
and medicines2. Historically this occurred in the Nordic Countries
because Europe, in particular faced up to the challenges of their
ageing population3-5. Pharmacists were keen to study both
medicines seeking and medicines use behavior and it all began
from there. Elsewhere in high income countries, it has taken a
while however now it is happening and this demonstrates the
coming of maturity within the profession; at least in academic
terms.
In the same fashion we argue for the increased utility of Social
Pharmacy in the context of low and middle income nations. This
focus needs to be driven by academics resident in developing
countries, but also those academics within the high income
nations whom have a passion for, and are qualified to, explore
broader “medicines use issues” through a different lens. A
“North-South Collaboration” is increasingly happening, as
evidenced by the publications in this as well as previous issues
of this journal. The Southern Med Review provides a sound
platform for propagating this collaboration6.
We argue that the benefits of Social Pharmacy research in the
Global South are two-fold. First, techniques borrowed from
the social sciences could be applied to address fundamental

2 Southern Med Review Vol 4 Issue 1 April 2011
Guest Editorial
Medicines use and access research: diverse methodologies show a complex picture requiring our attentionCitation: Ballantyne PJ. Medicines use and access research: diverse methodologies show a complex picture requiring our attention. Southern Med Review (2011) 4;1:2-3 doi:10.5655/smr.v4i1.79
of access to and use of medicines by rural Nepalese. Heydon
describes how the unique historical context of (western) health
care development in the region - in particular, the introduction
of western medicine by the expedition culture from the 1960s,
and the ongoing influence of recreational visitors to the region
on medicines availability and use – has resulted in Sherpas’
familiarity with accessing and using ‘western’ medicines.
However, serious gaps in access to and the quality of western
health care (providers and medicines), has meant that a place
for traditional healers and medicines has never been usurped,
and a setting of medical pluralism prevails in the region.
Jonathan Harper and Gunnar Strote provide a broad, sweeping
look at the Afghanistan pharmaceutical sector, relying on a mix
of methods to examine current problems and prospects. They
report that despite assistance from the international donor
community in Afghanistan, its pharmaceutical sector “suffers
from major deficiencies in terms of policy implementation,
regulation, and management… with governance, structural
and capacity weaknesses at both the central and provincial
level”. They emphasize in particular the presence of a market
for counterfeit and substandard medicines as an urgent public
health problem.
My own article considers the pharmacist-professional role in
assuring the appropriate use of medicines by the public. The
article is intended to be a reminder that availability, access and
affordability aside, medicines-use outcomes may be harmful
if not carefully supervised. Demonstration of the positive and
negative impacts of medication supervision – or lack of it – from
pharmacists or other health care professionals (or from non-
professionals) on the public’s health is important, but must be
creatively planned and executed.
Robert Chapchet Chana and Hazel Bradley provide an interesting
view of medicine use by consumers in Tiko, Cameroon. Using
focus groups and key informant interviews, these authors
describe important social-cultural factors influencing medicine-
seeking and use – key among these is socio-economic status of
consumers, and the costs of medicines. Medicines-access and
use occur in a context of poor medicines regulation and control;
costs vary widely by provider (roadside kiosks, itinerant vendors,
In a guest editorial in the September 2009 special issue of SMR
(on access to medicines, pricing and generics), Professor Albert
Wertheimer describes the complex array of pre-conditions for
and consequences of an individual getting and using a medicine.
He states that “the patient gets the appropriate medication
only when there is a concordance of several endeavors. To
achieve success, we need to have availability, affordability and
access…”1.
Articles included in the current issue of SMR reinforce
Wertheimer’s assertion, as I describe here. However, I would
add that an additional endeavor ought to be added to his list.
Acknowledging the gap between expert/scientific knowledge
about medicines and lay perspectives and knowledge – I would
suggest that an additional factor influencing success in medicine
use outcomes is professional [pharmaceutical] care. Thus, in
reading the articles in the current issue, I would ask you to
consider [in addition to availability, affordability and access],
the importance of professional surveillance and supervision of
lay medicine use for optimal medicine use outcomes – and the
consequences of its absence. Additionally, the current issue
illustrates an impressive array of research approaches and
methodologies for assessing medicines availability, affordability,
access and care. We encourage readers to consider the utility of
these for their future research endeavors.
First, addressing access to essential medicines at a population
level, Trap Rete and colleagues describe the results of an
evaluation of the Global Alliance for Vaccine and Immunization
service support (GAVI-ISS) undertaken to assess the coverage
(as well as the quality, efficiency, security and usefulness of the
evaluation system) of childhood diphtheria-tetanus-pertussis
immunization (DTP3) in 9 developing nations. The GAVI-
ISS combines an evaluation of the quality of the country’s
immunization reporting system with performance based
financial rewards, country-specific recommendations and
implementation support. The authors detail the methods used,
and impressive outcomes – findings of improved reporting
quality for all nine countries included in the study.
Susan Heydon illustrates the use of historical case study
methodology to provide a perspective and understanding

3 Southern Med Review Vol 4 Issue 1 April 2011
Medicines use and access research
community medicines stores, private hospital pharmacy, public
hospital pharmacy and community pharmacies) in a setting
of “unbridled illicit trade in pharmaceuticals”. Medicines are
valued and sought after, funded out-of-pocket by people with
limited means, and commonly used without supervision.
Difei Wang’s article is focused on the important topic of the
evolving ‘essential medicine’ list that determines a population’s
access to medicines. Wang describes the history of World Health
Organization list of essential medicines (EM) and the Chinese
National Essential Medicines List (NEML), and compares their
convergences and differences over time. Wang reports significant
improvement in China’s NEML, but calls for improvements in the
transparency and accountability of medicines selected for the
list.
Peri Joanne Ballantyne, PhD
Department of Sociology
Trent University, Canada
References1. Wertheimer AI. Access to medicines: Complex entities and
behaviours seem unavoidable. Southern Med Review (2009)2; 2:1-1
4 Southern Med Review Vol 4 Issue 1 April 2011
Commentary
Mountains and medicines: history and medicines use in rural NepalSusan Heydon
School of Pharmacy, University of Otago, New Zealand
Address for Correspondence: Susan Heydon, School of Pharmacy, University of Otago, PO Box 56, Dunedin 9054, New Zealand. E-mail: [email protected]
Citation: Heydon S. Mountains and medicines: history and medicines use in rural Nepal. Southern Med Review (2011) 4;1:4-8doi:10.5655/smr.v4i1.77
AbstractThe aim of this article is to highlight the value of an historical approach for current health research into access and use of medicines. It
also suggests that historical research complements the perspectives of other social science disciplines. This study focuses on the rugged
Mt Everest region of Nepal and the mainly Sherpa inhabitants from the 1960s through to the present. It draws on an in-depth historical
case study of Khunde Hospital, which is the main provider of health services in the area, and an exploratory study of people’s use of
medicines over time. This historical perspective deepens our understanding of both the consumer and provider of medicines in the
Everest area. The research employs a variety of qualitative methods and uses a wide range of written and oral, primary and secondary,
published and unpublished sources as well as participant observation and further fieldwork. Multiple separate and interconnected
factors have influenced medicines use over time. The study identifies the importance of medicines in the introduction and spread of
‘modern’ medicine in the area, but like elsewhere in the Himalayan region modern health care and its medicines are used within a plural
medical environment. The Mt Everest region has become a major tourist destination which has led both to considerable economic
development in the area but has also influenced the supply and use of medicines. While medicines use unsurprisingly is different today,
this development overall has occurred within a framework of both continuity and change that underpins Sherpa life more broadly.
Keywords: medicines, mountains, Nepal, medicines use, medicines access, history
While there is a growing historical literature about the discovery
and role of medicines in tackling disease, there is little relating
to current medicines issues and pharmacy practice. The aim
of this paper is to bring an historical approach to considering
current access and use of medicines in rural Nepal. In particular
it will focus on the Mt Everest region. Although the number
of pharmacists and pharmacy assistants in Nepal has increased
considerably in recent years, in 2007 less than 8% of registered
pharmacists and 37% pharmacy assistants worked in hospital
and community pharmacies13. As is to be found elsewhere in
the wider region, most people in Nepal obtain their medicines
through various retail outlets where often the staff has little
training in medicines14. Also, as noted recently in Pakistan, most
pharmacies sell medicines without prescriptions15-16. In 2007
the Nepalese government declared that many basic medicines
could be obtained for free at government health institutions,
but in early 2010 local media, referring to a Ministry of Health
and Population source, claimed that 85% of government
health institutions in Nepal were without stocks of essential
medicines17. While a person was able to consult a health worker
for free, people had to go elsewhere and buy some or all of
the medicines they required from the private sector instead of
IntroductionIn the past ten years a number of articles have appeared in
a range of journals that discuss the value and ways of using
an historical approach in current health research, policy and
practice1-8. While an interest in history has long been present
in the study of health, these articles cumulatively suggest
that historians through their different interests, conceptual
approaches and particular methods can provide valuable insights
into today’s concerns9-10. These perspectives complement those
provided by researchers from other social science disciplines and,
in terms of the patient or consumer of services, further deepen
our understanding, whether at an individual or population
level. For the most part, this debate about history has been
conducted in and about developed countries and has focused
on public health. Nevertheless an increasing interest is being
shown in developing countries where these other social science
disciplines, and especially anthropology, already have a major
involvement in health research11. In late 2004 the World Health
Organization (WHO) established the Global Health Histories
(GHH) project which ‘promotes the concept that learning from
history is vital to help shape a healthier future for everyone,
especially those most in need’12.

5 Southern Med Review Vol 4 Issue 1 April 2011
Mountains and medicines: history and medicines use in rural Nepal
being supplied from the government clinic or hospital. Nepal
is one of the poorest countries in the world, but a 1998 study
showed that funds for almost three-quarters (74%) of the
country’s health care came from the out-of-pocket expenditures
of households18.
This paper draws on two historical studies undertaken in the
Mt Everest region: a case study of the area’s main provider of
health services and an exploratory study into changing patterns
of medicines use19-20. The research began as history of health,
but as its relevance to current practice became more striking its
focus shifted towards history in health1. Both studies draw on a
range of primary and secondary, written and oral sources, as well
as participant observation through being a volunteer at Khunde*
Hospital for over two years and subsequent visits. Documentary
sources include hospital records, reports, correspondence and
diaries, while oral history interviews were carried out with present
and former hospital staff and members of the local community.
The first part of the paper examines current access and use of
medicines in the Mt Everest area while the second section adopts
an historical approach to understanding these patterns.
Medicines in the Mt Everest area of Nepal The Mt Everest region is situated on Nepal’s northern border with
the Tibet Autonomous Region of China and is a spectacular and
challenging high-altitude mountain environment. There are no
roads. A national park, it is home to the Sherpas who during the
first half of the twentieth century became internationally famous
through their role as high-altitude support personnel on climbing
expeditions. In 1953 New Zealander Edmund Hillary and Tenzing
Norgay made the first successful ascent of Mt Everest. Today this
region, which has a population of approximately 3500, is one of
Nepal’s major tourist destinations19(p.321). The rise of tourism has
fuelled the area’s economic development and has encouraged
people from other ethnic groups to move into these high valleys
for employment.
Unlike most of rural Nepal the Everest region has had a permanent
and functioning health infrastructure since the 1960s. Currently,
while the main provider of services and medicines is Khunde
Hospital, which was built by Sir Edmund Hillary in 1966 as part
of his ongoing aid programme, people can also obtain medicines
from various other sources. These include the hospital’s village
clinics, government clinics, tourists (whether or not they are
health professionals), the dental clinic, various temporary or
permanent aid projects and non-government organisations
(NGOs), local initiatives, a licensed pharmacy and general
shops. Visitors to the area also donate medicines to local health
organisations. In general, people obtain most of their medicines
from facilities run by health personnel with varying levels of
training, but none have registered pharmacists or pharmacist
assistants on their staff.
Sherpas today are familiar with accessing and using medicines.
Despite the poverty of most Nepalese, many Sherpas are
affluent, travel and obtain medicines while away, whether
within Nepal, such as in the capital Kathmandu, or overseas on
a trip sponsored by a visitor. People are aware that medicines
exist for different health concerns, such as to relieve pain or
help one sleep, but mostly see them in terms of what they do
rather than by name21. For example, they know antibiotics can
be medicines that dry lesions. Communicable diseases remain
important health issues in Nepal, but chronic non-communicable
conditions are an increasing burden for health services. Among
Sherpas, a changing and often more sedentary lifestyle has led
to a growing number of people now needing to take medicines
on a long-term basis. Khunde Hospital’s annual report for
2008/09 notes that hypertension is common with more than
sixty people under regular medication22. The report also
mentions an increasing prevalence of type two diabetes mellitus
and gout. Currently, the hospital is able to obtain sufficient and
appropriate medicines for patients with chronic conditions, and
currently staff regard adherence as good21. Supplies are bought
in Kathmandu, but the hospital is also happy to accept medicines
donations from visitors. Internationally, the issue is of concern
regarding quality, appropriateness, expiry and proper disposal.
International guidelines exist, but mostly remain guidelines23.
Particularly useful donations for Khunde Hospital are analgesics
and antibiotics, but this is not the case with all medicines
received. Only some visitors ask the hospital what is needed.
Good relationships with organisations operational during the
trekking season may also see left over medicines coming to
Khunde. Currently this happens with the IPPG (International
Porter Protection Group)22.
In 2006/07 there were 8013 outpatient attendances at Khunde
Hospital(19p.320). Although many people now go to Khunde
Hospital as their first choice and use its medicines, especially
antibiotics and analgesics, modern medicine – as this type of
health care is often referred to in Nepal – also operates in a
fluid plural medical environment. Sherpas believe in a variety
of gods and supernatural spirits and these beliefs inform their
ideas about sickness, disease causation and the internal body.
For example, a pem (a type of ‘witch’ spirit) is usually held
responsible for prolonged diarrhoea and vomiting. People will
take medicines from the hospital to relieve the symptoms, but
the hospital is not the appropriate place for dealing with the pem
that has caused the illness. Sherpas, who originally came from
Tibet, are Buddhist and in the Everest area can obtain medicines
from some religious lama (a senior monk) and amchi (a Tibetan
medical practitioner). Recently an NGO project established
medical herb gardens and began to make medicines, but while a
Himalayan Trust nursery at Phurte grows some plants for Tibetan
medicines, a large tourist lodge now stands on what was the
Sacred Land project nursery site24. Nevertheless, the hospital and
community are used to each other in a relationship that is in
practice a coexistence of difference19. Each acknowledges and
incorporates aspects of the other’s beliefs and practices when
dealing with a person’s sickness, but remains separate. It is a
relationship that has built up over time.
* An alternative spelling is Kunde.

6 Southern Med Review Vol 4 Issue 1 April 2011
Mountains and medicines: history and medicines use in rural Nepal
Historical perspectives on access and use of medicines in the Mt Everest regionA great strength of historical research is its interest in and ability
to investigate the wider context. While an examination of the
current situation identifies multiple aspects to medicines use in
the Everest area, historical perspectives explore these over time.
This research highlights the importance of medicines in the
introduction and spread of modern medicine in the area; that
multiple separate and interconnected factors have influenced
medicines use; and that while medicines use unsurprisingly
is different today from fifty years ago, this development has
occurred within a framework of both continuity as well as
change that underpins Sherpa life more broadly25.
Before the mid-1960s, people in the Everest region had very little
access to and so little use of modern medicines. Instead, Sherpas
used various rituals and a few herbal medicines. While Nepal had
few biomedical services, Sherpas employed on mountaineering
expeditions came into contact with their medical services. These
expeditions often carried extensive supplies of medicines26. A
few Sherpas were also trained to assist. New Zealand climber
Norman Hardie wrote about his five-month stay in 1954/55 in
the village of Khumjung and provides an explicit reference to
the important role of medicines in promoting the introduction
and spread of modern medicine: ‘This assistant could be taught
the uses of the appropriate pills for the treatment of the
major fevers, dysentery and high altitude headaches. Besides
assisting the party home, it would slowly diminish the deep-
rooted superstitions that exist in the home villages’27. Expedition
medical care, nevertheless, was a short-term option.
Although slowly expanding, government health services
throughout Nepal remained limited in the 1960s and especially
in rural areas where most of the population lived28. In the Everest
area the situation changed, particularly after the opening of the
small hospital at Khunde in 1966. The government also opened
a small clinic in the area’s administrative centre of Namche
Bazar. Khunde Hospital, run by Hillary’s aid organisation the
Himalayan Trust, soon became the main provider of both the
medical services and the medicines. Nevertheless people’s use
of the hospital was pragmatic and selective based on their
perceptions as to the hospital being the appropriate place
to go for their particular health concern19. Most people had
expectations that modern medicines should work in a very short
space of time29(p.268). If they did not, they tried other systems.
The overseas volunteer medical staff had to adapt their practice
to the conditions and to how people used the hospital and
its medicines – for example, how to devise a dosage regimen
when people did not have clocks30? Initially people thought
that the hospital’s medicines were no good because they were
free and it was only when people travelled to Kathmandu that
they found the same medicines could be expensive to buy31.
Then they began to increase their use of the hospital. Sherpas
considered that the new medicines could treat the symptoms
but were not the real cure32. In the 1950s and 1960s many
new medicines became available, especially antibiotics for the
treatment of infectious disease, impressing both local people
and the hospital staff. Overseas volunteer Lesley Evans wrote in
her diary in 1968 during the walk in to Khunde: ‘We saw awful
impetigo on two children in tonight’s surgery. … But gosh, how
speedily infections get better. They’re so sensitive to antibiotics
…’33.
At Khunde Hospital staff assumed they would have the necessary
medicines to treat a wide range of health problems presented by
the increasing number of patients. They thought of medicines
mainly in terms of supply issues. Between 1967 and 2006/07
patient numbers quadrupled, from 1924 to 801319(p.319-20).
Initially most medicines were brought in from New Zealand and
many of these were donated, but gradually as more medicines
became available in Nepal the hospital bought its supplies
internally. Contact with government health services was very
limited, except in the areas of medicines for government
preventive health programmes with which the hospital became
increasingly involved. These were vaccines, tuberculosis and
leprosy medicines, family planning supplies and iodised oil
injections. Most of these medicines came from international aid
sources, but while hospital staff initially obtained some directly
from the respective donor, increasingly staff found they were
instructed to obtain these through the particular government
programme as these developed34.
As with general use of the hospital’s services, therapeutic
success increased the hospital’s acceptance in the community,
although not everyone is happy with modern medicines. The
younger wife of an elderly man, who has forgotten the English
he learned while on expeditions in the 1960s, blames his loss of
‘memories’ on all the medicines he has taken during his life35.
While he still takes his medicines, treatment failure could have a
negative effect on people’s perceptions and use of the hospital.
Over time this has affected the hospital’s efforts to develop
services. In 1980 a one-year old child died in a village following
an injection of penicillin. Although unrelated, this hindered
uptake of the hospital’s vaccination programme in the villages
in the upper valley. Hospital staff made periodic attempts to
immunise, but not till 1997 was this successful36. While the issue
was more complex, the effect of the belief that ‘vaccinations kill
babies’ was powerful and long lasting37. Medicine and mode of
delivery were synonymous.
Like elsewhere in the Himalayan region, modern health services
functioned within a changing but plural medical environment,
with people deciding which system to use based on their
perceptions of the cause of their problem38. Religious and amchi
medicines also circulated in the community and ritual remained
important. Medicines were made by lamas from instructions in
the religious books, but some medicines were more preventive
and ‘not really medicine’21. Small red or brown/black pills,
which remain popular, were regarded as good for everything
and helped a person keep healthy. Their ingredients included
holy water and their preparation involved prayer. They were

7 Southern Med Review Vol 4 Issue 1 April 2011
Mountains and medicines: history and medicines use in rural Nepal
also given for non-specific illness and people about to die. The
use of lhawa (a spirit medium/shaman) has decreased, but their
declining numbers were due more to the lure of employment in
the trekking industry than competition from modern medicine.
Amchi medicine had a more limited influence in the area29(p.261).
Sherpas used to supplement their subsistence lifestyle with trade
and while away bought medicines. Trade with Tibet declined
after the intensification of the Chinese presence in the 1950s,
but some amchi moved permanently into the Everest region.
The last aspect to be considered is the ongoing influence of
recreational visitors on medicines availability and use. When few
their impact was limited, but increasing numbers became integral
to the economic development of the area. Tourist numbers have
risen from 20 in 1964 to 28,999 in 2008/09, with totals peaking
in the spring and autumn trekking seasons19(p.322),22. Most visitors
experience some form of sickness, ranging from the relatively
minor inconvenience of the common cold to conditions resulting
in death. When sick, tourists self-treat, are treated by their group
or another visitor, or seek help from a health facility. At Khunde
Hospital, visitors consume medicines from the hospital’s supply
but pay for their cost.
Visitors have influenced medicines use in a number of ways that
may also conflict with one another. Individually and as groups,
they have provided much of the region’s health infrastructure
through a desire to help and have also been an important
source of medicines donations. These supplemented the
hospital’s supplies and therefore helped to contain costs and
to increase the quantity and variety of medicines available at
the hospital. On the other hand, despite the presence of health
facilities, climbing expeditions and trekkers have continued to
give out medicines and provide treatment to local people. In the
1970s and early 1980s Khunde Hospital staff were particularly
concerned about fragmentation of care for people with chronic
conditions such as tuberculosis which was common at the
time and had a longer treatment time than today19(p.209). Such
medical help was carried out in good faith on both sides, but
while a focus on the provision of basic health services may be
appropriate policy for the area, it is also not surprising that
local people wanted what they thought to be a better option.
They did not consider receiving treatment from various sources
to be a problem. They knew visitors carried medicines for
their own use and over the years this has created some issues
for staff at Khunde Hospital such as the use of antibiotics in
cases of diarrhoea, which is very common among both local
people and visitors. While the use of oral fluids for rehydration
is recommended in cases of uncomplicated diarrhoea, visitors
often have potent antibiotics, which can considerably speed up
recovery from an unpleasant condition. Not surprisingly local
people wanted similar treatment39.
ConclusionThis historical research has highlighted the central role that
medicines have had in the introduction and spread of modern
health care in the Mt Everest region of Nepal and has identified
the wide range of complex, separate and interconnected
issues and how these have changed over time. When Western
medicine encountered Sherpa beliefs and practices the response
was neither a one-way diffusion of Western medical practice,
nor a collision between the spirit-suffused system of the
Sherpas and scientific biomedicine. People used the hospital
and its medicines for some things but not others, based on their
perception as to whether the hospital was the effective and
appropriate option to take.
Nevertheless, as with the health services more broadly, multiple
factors have influenced access and use of medicines. Increasing
availability and use, together with changing patterns, has
occurred within a framework of both continuity and change
that underpinned Sherpa life more broadly and which we need
to better understand if we want to know more about what
people do when they incorporate dealing with sickness into
their and their family’s daily life. An understanding of these
complexities over time is important for developing strategies
to improve medicines policies and practices, whether, as in the
Everest area, other health professionals (such as a doctor, nurse
or medical assistant at Khunde Hospital) are involved rather
than pharmacists or pharmacy assistants. It is also important for
efforts to contain costs, an issue that is of concern not just to
Khunde Hospital or Nepalese government health services. The
increasing burden of chronic, non-communicable illness and the
need in many cases for long-term medication is an issue facing
all countries.
AcknowledgementI would like to thank the many people in Nepal and New Zealand
who have helped me with my research. I would also like to thank
the School of Pharmacy for a Start-up grant that enabled me to
return to Nepal in early 2010 to undertake fieldwork.
References1. Perdiguero E. History of health, a valuable tool in public health.
J Epidemiol Community Health 2001; 55: 667-73.
2. Berridge V. Public or policy understanding of history? Social History of Medicine 2003; 16(3): 511-23.
3. Scally G, Womack J. The importance of the past in public health. J Epidemiol Community Health 2004; 58: 751-5.
4. Bashford A, Strange C. Thinking historically about public health. Med Humanities 2007; 33: 87-92.
5. Sheard S. History in health and health services: exploring the possibilities. J Epidemiol Community Health 2008; 62: 740-4.
6. Berridge V. History matters? History’s role in health policy making. Medical History 2008; 52: 311-26.
7. Szreter S. History, policy and the social history of medicine. Social History of Medicine 2009; 22(2): 235-44.
8. Dolan B. History, medical humanities and medical education. Social History of Medicine 2010; 23(2): 393-405.
9. Berridge V. Introduction to history in health. In: Green J, Browne J, eds. Principles of social research. Maidenhead: Open University Press, 2009. p. 145-55.

8 Southern Med Review Vol 4 Issue 1 April 2011
Mountains and medicines: history and medicines use in rural Nepal
10. Green J, Browne J. Introduction to social research. In: Green J, Browne J, eds. Principles of social research. Maidenhead: Open University Press, 2009. p. 7-14.
11. Bhattacharya S, Dasgupta R. A tale of two global health programs: smallpox eradication’s lessons for the antipolio campaign in India. Am J Public Health 2009; 99(7): 1176-84.
12. WHO. Global health histories. http://www.who.int/global_health_histories/en/ (14 Oct. 2010).
13. Nepal Pharmacy Council. NPC newsletter. In: Nepal Pharmacy Council. 2007; 2(1):1-8. http://www.nepalpharmacycouncil.org.np/index.php?link=download (7 December 2010).
14. Kafle KK et al. Drug retailer training: experiences from Nepal. Soc. Sci. Med. 1992; 35(8): 1015-25.
15. Hussain S et al. Exploring health seeking behavior, medicine use and self medication in urban and rural Pakistan. Southern Med Review 2010; 3(2): 32–4.
16. Wachter DA et al. Antibiotic dispensing by drug retailers in Kathmandu, Nepal. Tropical Medicine and International Health 1999; 4(11): 782-8.
17. Health facilities sans drugs. Kathmandu Post 27 Jan. 2010: 1.
18. Hotchkiss DR et al. Household health expenditures in Nepal: implications for health care financing reform. Health Policy and Planning 1998; 13(4): 371-83.
19. Heydon S. Modern medicine and international aid: Khunde Hospital, Nepal, 1966 – 1998. New Delhi: Orient BlackSwan, 2009.
20. Heydon SJ. Changing patterns in medicines use in the Mount Everest region of Nepal. Pharmacy Practice 2010; 8(Suppl 1): 107.
21. Sherpa KT; doctor in charge of Khunde Hospital. Interview. 15 February 2010.
22. Kunde Hospital Annual Report 2008/2009.
23. WHO. Guidelines for drug donations. Geneva: World Health Organization, 1999. http://apps.who.int/medicinedocs/en/d/Jwhozip52e/5.1.html (5 August 2010).
24. Rangit Gurung; forestry supervisor, Himalayan Trust. Personal communication. 2 February 2010.
25. Fisher JF. Sherpas: reflections on change in Himalayan Nepal.Delhi: Oxford University Press, 1997 [1990].
26. Hingston RWG. Medical Notes. In: Norton EF. The fight for Everest 1924. Varanasi and Kathmandu: Pilgrims, 2002 [1925]. p. 350 –3.
27. Hardie N. In highest Nepal: our life among the Sherpas. London: George Allen & Unwin, 1957. p. 121.
28. Dixit H. Nepal’s quest for health, 3rd ed. Kathmandu: Educational Publishing, 2005. p. 130.
29. Draper J. Beyond medicine: sickness, healing, and order in Sherpa society. Sydney: University of Sydney, [1995] (PhD).
30. Evans L; overseas volunteer, Khunde Hospital. Letter from the Himalayas No. 2. Khunde Hospital papers; undated [1968/9].
31. Nima Yangen Sherpa; first nurse-assistant, Khunde Hospital, 1966-8. Interview. 1 July 2003.
32. Adams V. Healing Buddhas and mountain guides: the production of self within society through medication. Berkeley: University of California, 1989 (PhD). p. 146.
33. Evans L; overseas volunteer, Khunde Hospital. 17 August 1968. Letters from Nepal from Dr Richard and Lesley Evans to their family, 1968–69. Christchurch, 2004.
34. Mathema KB; Programme Officer, UNICEF. 13 August 1976. Letter to Dr R Riley, Khunde Hospital, copied to Dr HD Pradhan, Senior Public Health Administrator, Department of Health Services. Khunde Hospital papers.
35. Mingma Temba Sherpa; hospital manager, Khunde Hospital. Interview. 11 February 2010.
36. Kunde Hospital and Village Clinics Annual Report 1997.
37. Kunde Hospital Annual Report September 1st 1983 – August 31st 1984.
38. Lambert H. Plural traditions? Folk therapeutics and ‘English’ medicine in Rajasthan. In: Cunningham A, Andrews B, eds. Western medicine as contested knowledge. Manchester: Manchester University Press, 1997. p. 191-211.
39. Heydon SJ; overseas volunteer, Khunde Hospital, 1996-8. Personal communication. June 2004.
9 Southern Med Review Vol 4 Issue 1 April 2011
Research Article
Sociocultural, economic and regulatory influences on medicine use by consumers in a rural township in CameroonRobert Chapchet Chana1, Hazel Bradley2
1Core Pharmacy, P.O.Box 332 Tiko, Cameroon 2School of Public Health, University of the Western Cape, South Africa
Address for Correspondence: Robert Chapchet Chana, Core Pharmacy Likomba, Tiko, South West Region, Cameroon. E-mail: [email protected]
Citation: Chana RC, Bradley H. Sociocultural, economic and regulatory influences on medicine use by consumers in a rural township in Cameroon. Southern Med Review (2011) 4;1:9-16 doi:10.5655/smr.v4i1.73
AbstractObjectives: The objective of the study was to analyze the sociocultural, economic and regulatory factors influencing access to and the
use of medicines by consumers in Tiko, Cameroon.
Method: Using focus group discussions information was obtained from members of Plantain Traders Association, Township Taxi
Drivers Association and Teachers of Government Bilingual High School (GBHS) Tiko. This information was triangulated with those
obtained from key informant interviews with sellers of medicines in community pharmacies.
Results: Key influences on medicines use were reported to have emanated from the sociocultural and economic background of the
people and also from inappropriate regulation on medicine distribution and sales and included the perceived need for medicines,
the cost of medicines, the purchasing habits, the medicine use culture, medicine supply channels and poor medicines regulation and
control.
Conclusion: Consumers’ perceived need for medicines generated a pattern of use that included medicines sharing attitudes and
polypharmacy. Their medicine purchasing attitudes were greatly influenced by their financial constraints. The lack of proper regulation
also contributed towards the irrational use of medicines.
Keywords: Medicines, medicines use, consumers, patients, community pharmacies, self medication, Cameroon.
The inappropriate use of medicines results in increased morbidity
and mortality, especially in disease conditions like hypertension,
diabetes and epilepsy where it is critical that medicines are taken
regularly and appropriately3. It also wastes resources and results
in poor patient outcomes and adverse drug reactions3. Antibiotic
resistance is on the increase due to overuse of antibiotics, and
inappropriate use of injections, especially non-sterile injections,
has resulted in increased transmission of HIV/AIDS and hepatitis4.
The rational use of medicines is one of the core components
of the pharmaceutical policy of Cameroon5. The strategic
document for the implementation of a National Pharmaceutical
Policy in Cameroon recognizes that, despite the creation of a
Central Pharmaceutical Store for the nation, health units still
IntroductionEssential medicines, or drugs, are those which satisfy the priority
health care needs of the population1. They should be of good
quality, available at all times and affordable. When used properly,
these medicines provide simple cost-effective solutions to our
health care needs1. “The rational use of medicines requires that
patients receive medications appropriate to their clinical needs,
in doses that meet their own individual requirements, for an
adequate period of time, and at the lowest cost to them and
their community.”2 Unfortunately, studies indicate that on a
global level, more than 50% of all medicines are prescribed,
dispensed, or sold inappropriately and 50% of patients fail to
take them correctly3.

10 Southern Med Review Vol 4 Issue 1 April 2011
Medicines use in Cameroon
run out of stock of essential medicines5. In addition, the illicit
trade in pharmaceuticals, most especially counterfeit medicines
is increasing and no public health programs exist to educate
actors involved in medicine use on the appropriate use of
pharmaceuticals, a problem which is further exacerbated by
the lack of sufficient number of health professionals. In 2000,
it was estimated that the pharmacist to population ratio was
1:26930 persons while for doctors (general practitioner) it
was 1:12,500 persons and for nurses 1:2083 persons5. This is
a particular cause for concern because modern medicines are
found everywhere and can be sold by anyone6. Previous studies
conducted in Cameroon to promote rational use of medicines
have focused on health worker prescribing and dispensing.
Enhancing optimal practices by heath care workers can only
partly improve the use of medicines, because Cameroonians,
instead of going to the formal health sector when sick regularly
self-medicate or visit a street vendor, traditional or faith healer7.
It was noted that when consumers self-medicate, they obtain
their medicines from informal drug distribution channels and
from pharmacies. It was estimated in 2006 that 44% of sick
patients in Cameroon relied on self treatment, 26% and 17%
respectively went to state-own health facilities and private health
facilities while 8% of patients went to an informal health facility,
mainly illicit drug retailers, traditional healers and religious
healers8. In addition, the use of medicines is not rationalized
and constitutes 81% of the total health expenditure8.
Frequently consumers request capsules or tablets of medications
ranging from anti-infectious agents such as antibiotics and
antimalarials to analgesics and, for various reasons, not all of
these patients buy the full course of therapy and even when
they do, they may not take all the medicines as prescribed.
In 2008 and 2009, it was estimated that households were
paying 77% to 90% of the annual total health expenditures
of Cameroon and that 94.8% of this contribution came
as out-of-pockets spending during illness episodes8 in the
formal and informal health sectors. Successful strategies to
improve the use of medicines by consumers must be based
on a clear understanding of consumers’ beliefs, expectations
and approaches to medicines, so that specific issues can be
targeted. This study therefore investigates the ways consumers’
in Tiko Sub division, Cameroon, use medicines and the factors
influencing them to do so.
The study took place in Tiko Sub-division, a rural sub-division in
the South-West Region, one of the two English speaking regions
of the Republic of Cameroon. Tiko Sub-division is a coastal plain
and has a hot climate. The population size is approximately
55,914 inhabitants9, made up of approximately 47.8 % males
and 52.2% females. The principal sources of income of the Tiko
population are trading, farming and plantation wage earnings.
Plantation wage earners and farmers make up 81% of the poor
population in Cameroon10. As in other parts of the country,
malaria, pneumonia and diarrheal diseases are the leading
causes of death especially of under-5 mortality11 while HIV/AIDS
and tuberculosis are also common. Tiko is an easy access point
to neighbouring countries like Nigeria and Equatorial Guinea.
English and French languages are the two official languages in
Cameroon. However, there are about 250 ethnic groups, each
with its own language. Pidgin is a frequently spoken language
and is used in various settings across Cameroon by all age
groups but more frequently nowadays, by the uneducated.
Pharmaceutical Situation in CameroonIn Cameroon, only pharmacists registered with the
Pharmaceutical Society of Cameroon are legally authorized to
import, stock, distribute and dispense medications. However,
in reality all doctors in private practice and some in the public
sector stock and dispense medicines to patients.
Cameroon runs a district health care system. Tiko health district
is governed by a district management committee and services
are provided in both the formal and informal sectors. The formal
sector consists of all accredited hospitals, health centers and
community pharmacies. The state owned health care services
in the formal sector consists of one district hospital, three
maternity units with facilities for out-patient consultations and
seven health centres. Private institutions in the formal sector
include two faith-based hospitals, two private surgeries and
five community pharmacies. There also exists a health service
complex owned by Cameroon Development Corporation (CDC)
which is intended to take care of employees of CDC. Apart
from CDC health staff, there are ten medical doctors working in
both the public and private sectors. The informal sector is made
up of medicine sellers in stalls, kiosks, hawkers and medicine
peddlers. Throughout Tiko Sub-division, it is estimated that
there are approximately 100 people involved in this informal
trade in medicines. Trading informally in medicines is against
the law; however, this practice thrives. Those involved in the
informal trade in medicine are not under the jurisdiction of any
professional body and do not need any formal qualification
to participate in the trade. The medicines they sell range from
simple over the counter medicines, like paracetamol, to the
most costly antibiotics like the third generation cephalosporins.
In this context, the present study was conducted. The objective
of the study was to analyze the sociocultural, economic and
regulatory factors influencing access to and the use of medicines
by consumers in Tiko, Cameroon.
MethodologyThis study was exploratory. The sample was selected from men
and women, aged 18 years and above, living in one of three
zones (Tiko town, Likomba and Mutengene) in Tiko Sub division.
The three zones of Tiko Sub-division were chosen because they
have more than 70% of the population, and about 80% of the
hospitals, community pharmacies and informal private medicine
stores and it was easy to commute within them.
11 Southern Med Review Vol 4 Issue 1 April 2011
Medicines use in Cameroon
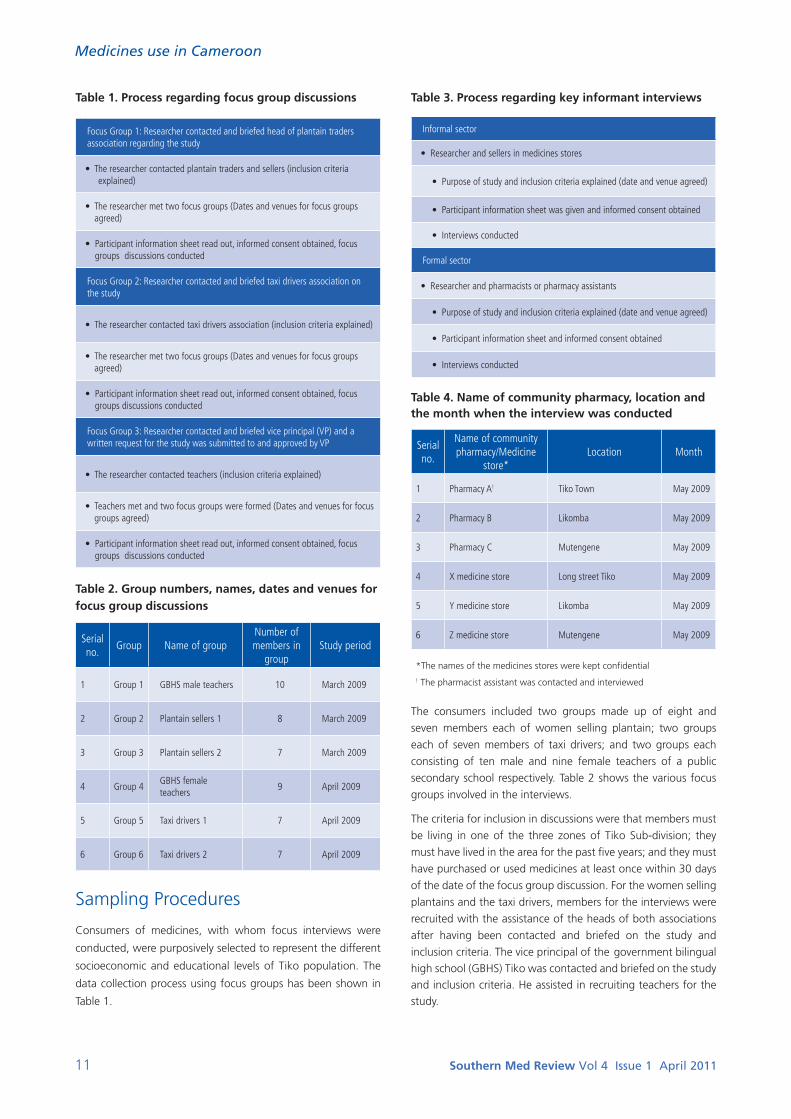
Table 1. Process regarding focus group discussions
Focus Group 1: Researcher contacted and briefed head of plantain traders associa tion regarding the study
• T he researcher contacted plantain traders and sellers (inclusion criteria explained)
• The researcher met two focus groups (Dates and venues for focus groups agreed)
• Participant information sheet read out, informed consent obtained, focus groups discussions conducted
Focus Group 2: Researcher contacted and briefed taxi drivers association on the study
• The researcher contacted taxi drivers association (inclusion criteria explained)
• The researcher met two focus groups (Dates and venues for focus groups agreed)
• Participant information sheet read out, informed consent obtained, focus groups discussions conducted
Focus Group 3: Researcher contacted and briefed vice principal (VP) and a written request for the study was submitted to and approved by VP
• The researcher contacted teachers (inclusion criteria explained)
• Teachers met and two focus groups were formed (Dates and venues for focus groups agreed)
• Participant information sheet read out, informed consent obtained, focus groups discussions conducted
Table 2. Group numbers, names, dates and venues for focus group discussions
Serial no.
Group Name of groupNumber of members in
groupStudy period
1 Group 1 GBHS male teachers 10 March 2009
2 Group 2 Plantain sellers 1 8 March 2009
3 Group 3 Plantain sellers 2 7 March 2009
4 Group 4GBHS female teachers
9 April 2009
5 Group 5 Taxi drivers 1 7 April 2009
6 Group 6 Taxi drivers 2 7 April 2009
Sampling Procedures
Consumers of medicines, with whom focus interviews were
conducted, were purposively selected to represent the different
socioeconomic and educational levels of Tiko population. The
data collection process using focus groups has been shown in
Table 1.
Table 3. Process regarding key informant interviews
Informal sector
• Researcher and sellers in medicines stores
• Purpose of study and inclusion criteria explained (date and venue agreed)
• Participant information sheet was given and informed consent obtained
• Interviews conducted
Formal sector
• Researcher and pharmacists or pharmacy assistants
• Purpose of study and inclusion criteria explained (date and venue agreed)
• Participant information sheet and informed consent obtained
• Interviews conducted
Table 4. Name of community pharmacy, location and the month when the interview was conducted
Serial no.
Name of community pharmacy/Medicine
store*Location Month
1 Pharmacy A! Tiko Town May 2009
2 Pharmacy B Likomba May 2009
3 Pharmacy C Mutengene May 2009
4 X medicine store Long street Tiko May 2009
5 Y medicine store Likomba May 2009
6 Z medicine store Mutengene May 2009
*The names of the medicines stores were kept confidential
! The pharmacist assistant was contacted and interviewed
The consumers included two groups made up of eight and
seven members each of women selling plantain; two groups
each of seven members of taxi drivers; and two groups each
consisting of ten male and nine female teachers of a public
secondary school respectively. Table 2 shows the various focus
groups involved in the interviews.
The criteria for inclusion in discussions were that members must
be living in one of the three zones of Tiko Sub-division; they
must have lived in the area for the past five years; and they must
have purchased or used medicines at least once within 30 days
of the date of the focus group discussion. For the women selling
plantains and the taxi drivers, members for the interviews were
recruited with the assistance of the heads of both associations
after having been contacted and briefed on the study and
inclusion criteria. The vice principal of the government bilingual high school (GBHS) Tiko was contacted and briefed on the study and inclusion criteria. He assisted in recruiting teachers for the study.
12 Southern Med Review Vol 4 Issue 1 April 2011
Medicines use in Cameroon
Six key informant interviews were conducted, three each with
medicine sellers and pharmacy assistants. Table 3 shows the
sampling process for the key informant interviews.
The inclusion criteria for the key informants were that the
registered community pharmacy and the informal store must
have traded in that locality for at least three years and that
the person interviewed must have worked in that facility for
at least one year. Because pharmacy assistants often interact
with patients in this setting more than pharmacists, they were
interviewed. The interviewer personally contacted the key
informants. However, those in the informal sector preferred to
stay anonymous. Table 4 shows the community pharmacies and
the dates of interviews.
Data collectionThe focus group discussions were conducted in both English
and Pidgin. English language was used during the group
discussion with the male and female teachers while Pidgin was
used in the discussion with plantain sellers and taxi drivers. The
key informant interviews were conducted in English. Interviews
were conducted in the community pharmacies and in the
medicine stores.
For all the focus group discussions and key interviews, an
observer, a social science university student, took notes and
recorded non-verbal cues. The interviews were also audio-taped
and the recordings transcribed. The focus group discussions
and key informant interviews were conducted by the principal
researcher. The group discussions for taxi drivers and plantain
sellers were conducted in Pidgin and in English for the teachers.
The researcher and observer were Cameroonians fluent in both
English and Pidgin and they both translated the pidgin version
to English.
An interview guide was used for both interviews. The questions
focused on the effects of consumers’ health seeking behaviour,
access to medicines, the use of medicines and the type and
sources of information consumers have for the use of medicines.
Ethical approval for the study was accorded by the University
of the Western Cape Ethics Committee and supported by the
district medical officer of Tiko Health district.
Results
Sociocultural factors
Perceived need for medicines
Consumers’ reported their perceived need for medicines were
guided by feeling of ill-health, the feeling of wellness and the
desire to stay healthy.
When consumers felt sick “they rushed immediately to get some medicines”. Taxi drivers reported that when they “felt like having fever”, they visited road side kiosks and medicine stores
for a prescription and to purchase medicines. They called the
medicine they took “first aid” and said that if they did not get
better, they would then go to the hospital.
“Me a no di waste time. When ma skin wan just worry me I di
go find medicine. A di tell dat boy them wey them di sell say
make them mix me some merecin for fever. If a take am den
a well then fine. If no bi so then a go go hospital. Da merecin
them for corner road e just dey like na first aid”
The English version is:
“I do not delay. As soon as I feel sick, I look for some medicines. I
tell the sellers in the medicine store to mix for me some tablets. I
will go to the hospital only if the medicine I drank did not relieve
me of my sickness. Those medicines sold in medicine stores and
kiosks are for first aid purposes.”
Plantain sellers said that they often took pain killers when they
felt they were going to suffer from generalized body pains. They
said that they did so because they did not want to fall sick and
“lose market days”.
Pharmacy assistants and medicine sellers reported that
consumers often requested medicines because they felt sick or
were about to get sick and that they sometimes asked for “a
dose of red and yellow capsules to treat a running stomach” and
at other times the sellers prescribed and dispensed medicines to
consumers.
Taxi drivers and male and female teachers also reported that
they stopped taking medicines when they felt better while some
teachers deliberately did not use up all the medicines because
they thought that it was useful to have some medicines left over
to use if the sickness returned.
The desire to stay healthy was expressed by participants in
all the focus group discussions. They reported that they took
medicines “to stay healthy, for cleansing of the system and to
have energy”.
Medicine use culture
The consumers reported sharing medicines with one another,
taking various kinds of medicines mixed together, and taking
medicines kept from a previously uncompleted treatment.
Consumers reported various instances of sharing medicines with
their friends and neighbours.
A female teacher reported the way in which she participated in
medicine sharing.
“I used ranitidine for my gastric. I wanted to know if it was a
good medicine for gastric ulcer before I bought it. A friend of
mine gave me some tablets from her house. They were almost
expired but I drank some and they helped. However, kindly
let me know if it’s a good medicine before I buy because I do
not want to continue drinking the medicine which is about to
expire.”
Sellers in medicine stores and pharmacy assistants reported that
consumers requested for a mixture of various kinds of medicines
including, metronidazole for running stomach (diarrhea), or a

13 Southern Med Review Vol 4 Issue 1 April 2011
Medicines use in Cameroon
single or multiple dose of mix medication (chloramphenicol,
ibuprofen, iron tablet) for fever. They also reported that men
drank alcohol while taking their medications (some feeling that
there is a therapeutic benefit in doing so) and also that some
female students bought menstrogen during holiday periods
to terminate unwanted pregnancy. In addition, they reported
that females preferred doxycyline while men took tetracycline
capsules, which they referred to as “red and yellow capsule”
for cleansing of the system and against running stomach (for
this they take with a bottle of Guinness, an alcohol). These
medications are supposed to be dispensed strictly against a
prescription and some of the combinations requested contain
medicines belonging to the same therapeutic class. These
medicines were usually kept in their homes or purchased
regularly from the sellers. Pain medicines were used regularly
by all the groups. Male and female teachers and women selling
plantains kept medicines at home to treat fever, stomach
ache and worms. They reported that they kept paracetamol,
metronidazole, amodiaquine, quinine and mebendazole. They
did not know the strengths of the medicines. These medicines
were used to prevent malaria (reportedly administered every
six months) in their children, to treat “running stomach” in
addition to taking them as a “first aid measure” before a formal
consultation if necessary, with a health worker.
A male teacher said,
“I do keep medicines at home. I buy them from the pro pharmacy
in the hospital. I give malaria medicines to my children every six
months to prevent them from getting malaria fever. I also give
them worm medicines”.
Pharmacy assistants and medicine sellers reported that
consumers gave a variety of reasons when they came to
purchase medicines. Sellers in the medicine stores said that
some consumers bought medicines regularly because their
doctor told them to take the medicine for a long time while
others requested medicines for specific purposes. For instance:
antibiotics were reportedly requested because consumers are
using them to clean their system.
Pharmacy assistants also reported that consumers requested
refills of anti-diabetic and anti hypertensive without prescription
and that consumers requested multivitamin tablets for their
children for appetite. It was common for pharmacy assistants,
medicine sellers or consumers to make diagnoses and prescribe
to anyone in need of medication. A pharmacy assistant reported
as follows:
“…a pastor and another lady came here (pharmacy) to buy
medicine. After she (pastor) had narrated the problem of her
child, I concluded that the child had malaria and I told her.
When I was about to give her the anti-malarial medicine, the
woman who came with her said that it was “aspergic”( aspergic
is lysine acetylsalicylate) that was good for fever. I insisted and
told them that aspergic was only to bring down the body’s
temperature. She told me to give as her friend had suggested
saying that her friend has children at home so she knew it. I
gave as they requested. After about 24hours, the pastror came
back complaining that she wanted fever medicine and not
medicine to cool body temperature. Unfortunately for her, I was
the one on duty, and I told her it was her fault. Her friend looked
at the counter of medicines again and saw another medicine,
pregnatal (a ferrous product for pregnant women). She advised
the pastor to get it for the sick child because “pregnatal”it was
the best medicine to replenish iron during pregnancy but that
when her daughter went to the antenatal clinic they did not
prescribed it for her so she took her daughter to the pharmacy
and bought it for her”.
This narrative illustrates the complex interaction between
medicine sellers, consumers and the sick. Pharmacy assistants
and medicine sellers reported that consumers gave a variety of
reasons when they came to purchase medicines including advice
from their doctor to take the medicine “for a long time”.
Economic factors
Cost of medicines
All consumers said that medicines were expensive. The cost
of medicines influenced the way consumers’ access and used
medicines. Community pharmacies were reportedly the most
expensive source, followed by medicine stores and then the
public hospital pharmacies. Even though consumers believed
that community pharmacies had better quality medicines, they
still resorted to other medicine supply channels which had lower
cost medicines.
Because of cost, some male teachers said that when they went
for prescription from a doctor, they had to know why each
medicine was prescribed. While some male teachers reported
that they bought medicines from public hospital pharmacies
where some bought in bulk to “make sure” they had medicines
available when they needed them, others venture to avoid
paying high costs for medicines by purchasing them through
friends.
“My friend is a nurse in Yaounde. Whenever I need medicine as
I needed Oflocet recently I called my friend who gave whom I
sent 5000frs CFA to get me a packet. It is the same Oflocet that
is sold in the pharmacies for 11,000frs CFA. You know, in the
pharmacies they have various taxes they pay. They also have the
salaries of the workers to pay. These all put together make the
medicine expensive”.
Consumers said that community pharmacies did not split
packets of medicines. This made it difficult for them to buy from
there unlike medicine stores which retailed from packets and
offer a mixture of medicines. Plantain sellers said that before
they could go to the hospital they had to be sure that they
had sufficient money to buy the medicines to be prescribed.
When the prescribed medicines were not available at the public
hospital pharmacy, they bought the medicines from community
medicine stores except when the doctor insisted that they buy
them from the community pharmacies. However, even when the

14 Southern Med Review Vol 4 Issue 1 April 2011
Medicines use in Cameroon
doctor insisted, they did not at all times buy all the medicines
at once from the community pharmacies. They bought their
medicines one after the other as they had the money to pay
for it, a process that might undermine therapeutic efficacy of
prescribed medicines.
Consumers reported that because of cost of medicines, they
sought care where they could get services on credit and also
sought alternative sources of healing which some combined
with biomedicine. This was reported by female teachers and taxi
drivers. Taxi drivers further reported that they often contributed
money for a sick colleague who could not afford to go to the
hospital or buy his drugs. A female teacher said,
“I do not have sufficient money. I am a single mother and I have
to take care of the children. I have a friend who is a pharmacist.
She burrows me medicines when I do not have money. At times
I ask her to select those medicines which are very important so
I can buy them. I sometimes ask from her pharmacy that they
should give me the same medicine as that of the packet I have”.
Regulatory factors
All consumers interviewed reported that medicines were freely
available from a wide variety of sources and that there were no
restrictions to purchase. Medicine sellers said that they supplied
consumers with whatever medicines they requested, whereas
pharmacy assistants reported that they sold medicines according
to what they felt was professionally appropriate. All consumers
interviewed made out-of-pocket payments for their medicines.
Sellers in medicine stores and community pharmacies said that
they sold in cash based on the amount of money the patient
had.
The male teachers reported that the cost of medicines resulted
in everybody taking advantage of the high cost of medicines
in pharmacies by getting involved in selling medicines. In
the hospital pharmacies for instance, they reported that
the medicines which were not supposed to be sold without
prescription were sold even in bulk to those whom the sellers
knew and to some community medicine store owners. Even
nurses in the hospital sold medicines to patients.
DiscussionIt was found that the way members of the community obtained
and used their medicines appeared to be influenced by the way
they perceived their need for medicine. Also it was influenced by
their ideas about efficacy, costs and the availability of medicines.
The need for medicines was mentioned in a variety of contexts:
to treat illness, prevent an illness and to maintain wellness. It
was common for both male and female teachers, taxi drivers
and plantain sellers to obtain medicines to treat a variety of
symptoms, such as pains and fever. It was also common for them
to reserve their medicines without seeking medical advice, when
they felt well. Teachers, taxi drivers and plantain sellers also took
medicines because they wanted to stay strong and healthy.
This finding was similar on one hand to that of Rasmussen et
al., 12, who reported that consumers believed that “medicine
is needed for every illness. If medicine is not used, the illness
will become serious”. On the other hand, it could be said that
consumers’ perceived severity of disease seemed to influence
their continuation on therapy13.
Consumers’ perception of the ‘power’ of medicines seems to
influence their desire to acquire medicines. On the one hand,
consumers believed that medicines were powerful and could
“cure” certain conditions. For instance, medicine sellers from
both the formal and informal sectors reported that consumers
used antibiotics to “cleanse their systems”, especially after sexual
intercourse; and they also took multivitamin products to prevent
the skin of their palms from peeling off. Plantain sellers took
paracetamol to cure fever and body pains. Some of these uses
are inappropriate and it is uncertain how this misinformation
got into the community. It does however illustrate a lack of
reliable information about medicines which was found in similar
research in Ghana14 and in a Filipino village15,16.
Polypharmacy was also found to be rife with consumers
requesting mixtures of medication to treat their illnesses. This
seemed to indicate that they did not have sufficient trust in
one medicine to treat their illness and so they would “make
sure” by taking two or three medicines together - hoping that
at least one will work. For example, sellers of medicines from
the informal sector reported that a mixture of medicines that
included “buta” (an analgesic), indocid® (another analgesic and
anti-inflammatory), some quinine (for malaria), multivitamins
and chloramphenicol were put together in a medicine sachet
given for the treatment of typhoid and malaria. It was a common
practice for consumers to take antibiotics with Guinness when
they have “running stomach” (diarrhea). Guinness (an alcoholic
drink) was attributed by consumers in this community to “cause
a tight stomach” (constipation) -a counter to the running
stomach. In other settings polytherapy has been reported to be
the outcome of the uncertainty people have on the cause of
their illness and choice of therapy17. As has been observed in this
study and in addition to the above, it could be suggested that
polytherapy was practiced because people wanted to get well
fast in order to be relieved of the discomfort associated with
their illness and also, for economic reasons - so that they didn’t
have to be absent from their daily activities. This was particularly
true of the poorer groups - the plantain sellers and taxi drivers
who depended on their daily income. Some of the taxi drivers
reported using pain killers and traditional treatment when they
had sprains. Using such combination might lead to therapeutic
interaction or people may abandon one and move on to the
other. This may have an implication in chronic diseases condition
where the medicine has to be taken for a long time.
Sharing of medicines with neighbours and friends was a common
practice. Consumers did this by supplying medicines from those
stored at home from previous or current treatments. Whilst
sharing possessions and helping your neighbour was expected

15 Southern Med Review Vol 4 Issue 1 April 2011
Medicines use in Cameroon
by community members, it is not appropriate behaviour with
regard to medicines use. It may mean that individuals do not
get a full course of treatment, say for malaria or a sexually
transmitted infection, or they may receive below the therapeutic
dose for conditions like hypertension or epilepsy. This illustrates
lack of understanding of treatment regimens and may lead to
treatment failure and bacteria resistance in the case of the use
of antibacterials18; 4.
Consumers and sellers of medicines in the informal sector
believed that medicines have power to treat diseases and heal
the sick. However, because of the monetary value attached to
medicines, they treated medicines as objects of trade 19. Even
though medicines are treated in this manner all over the world,
it is not appropriate in the current setting because of poverty
and consumers make more than 80% out of pocket payment
for treatment. It was common in this study for consumers to
request for a “few tablets of….” and for sellers to offer a “few
tablets of antibiotics” for treatment of diseases. Trading in
medicines seemed to be seen as a means of making a living by
some medicine sellers. The study found that consumers wanted
to stay healthy - medicine was thought to be a tool to achieving
this and thus many people were trading in pharmaceuticals. 20; 19
In Tiko Sub-division, financial considerations seemed to have
played a key role in consumers’ access and use of medicines.
In Cameroon, consumers pay all costs including the costs
of medicines when they visit health facilities. The system of
user fees was introduced to decrease unnecessary demand
for health care services, raise additional funds for the health
system and improve efficiency, especially the availability of
essential medicines 21. Prior to the implementation of user fees
government pro-pharmacies always ran out of stock of essential
medicines22;23.
In public hospitals, essential medicines are sold in pro-
pharmacies and they are substantially cheaper when purchased
here than from other sources. However, consumers said that
they did not obtain medicines from the pro-pharmacies for
various reasons which included the fact that sometimes doctors
prescribed medicines that were not on the essential list and
therefore not stocked at the pro-pharmacy. So, this left them
with the option of having to obtain medicines either from a
range of informal traders or registered community pharmacies.
Both of these options posed problematic issues for the rational
use of medicines in this community.
Consumers reported that the medicines from the community
pharmacies were good quality but expensive. Van der Geest24
compared prices of medicines sold at the community pharmacies
with those sold at the government pro-pharmacies and found
that those sold through community pharmacies were about 400
times higher. This resulted in consumers asking pharmacists about
which medicines to buy from a list of prescribed medications. This
would result in patients not following the prescribed regimen.
This could have been different if pharmacists were stocking
generic medicines at affordable prices or consumers educated
to insist on generic medicines from community pharmacies. Pharmacies are challenged to provide cheaper generics where they can make generic substitution. Even though consumers should get quality medicines and advice from a community pharmacy this source is not accessible to many due to cost.
Many consumers said they visited medicine stores or hawkers as their first port of call because medicines from these places were cheaper than in community pharmacies. In addition they said medicine sellers were ‘more flexible’ and amenable to selling part of packets. The medicine store owners opened up packet of medicine and sold part of its content to the patient. Splitting a patient-ready pack of medicines is forbidden by law in Cameroon. The system is highly problematic, accounting for the problematic nature of medicine consumption by individual. More so, this practice of selling by the pill does not promote rational medicines use because most patients do not come back to complete their course of medicines. It was also reported that roadside sellers and kiosk owners put expired medicines into packets which had a valid date and sold them to unsuspecting consumers. Whilst selling of medicines by the pill could help alleviate immediate symptoms, it may not treat the underlying cause of the disease and in case of infectious disease; this might result in resistance to the microorganism 4.
Regulatory decisions about medicines are supposed to restrict the handling and use of medicines as a means of contributing to the safe and appropriate use of medicines but regulations are not enforced 25. More so, a comprehensive pharmaceutical policy for Cameroon detailing who does what and how is yet to be developed. This study found that consumers in Tiko Sub-division bought their medicines, in ascending order, from hawkers, street corners, medicine stores, pro-pharmacies and community pharmacies. Community pharmacies are the only officially licensed outlets to sell drugs to the public. Pro- pharmacies are to issue drugs to the sick who visit public hospitals. However, the illicit trade in pharmaceuticals is unbridled. The illicit trade in pharmaceuticals in the Cameroon and other African countries, Ghana and Nigeria, has been reported in other studies 20; 26; 14. The uncontrolled sale of medicines causes the circulation of poor quality medicines, compromising patient safety and rational use.
Consumers reported that medicines found in the various
medicine sales outlets were not of same quality. Poor quality
medicines were reported in the community medicine stores
and with hawkers. In community pharmacies, although the
medicines were of good quality, consumers reported, they were
expensive. In pro-pharmacies, the medicines were invariably out
of stock. It has been reported elsewhere that when medicines
were out of stock dispensers dispensed what they have in
stock 27. Sometimes they dispensed branded products when
international non-proprietary names (generic names) were
prescribed 28. Consequently, it is frequent in these settings that
dispensers and patients do not adhere to prescription regimens.
It was reported by male teachers that in Tiko Sub-division doctors
were few compared to population size and that some doctors
did not understand English or pidgin, which are the common

16 Southern Med Review Vol 4 Issue 1 April 2011
Medicines use in Cameroon
languages of community members. Holloway 25 suggested
that setting educational standards for health professionals and
developing and enforcing codes of conduct would improve
medicines use. Medicine use by community members is unlikely
to be appropriate if prescribers do not communicate adequately
with patients.
ConclusionSociocultural factors that affected consumers’ use of medicines
were found to relate to the perception that they needed
medicines to stay healthy and when they felt sick. The consumers
would also abandon their medicines when they felt they were
well again. As a result and because of their financial constraints
and the cost of medicines they adopted coping mechanisms
which included purchase of medicines in small quantities,
practiced polypharmacy/polytherapy, shared their medicines
with one another and also to self medicate with prescription
medicines. In conclusion consumers’ medicine purchasing were
greatly influenced by their financial constraints.
References1. Brundtland, H. G. (2002). Essential Medicines: 25 Years of Better
Health. Journal of the American Medical Association .288:3102
2. Quick, J. D., Rankin, J. R., Laing, R. O., O’Connor, R. W., Hogerzeil,H.V., Dukes M.N.G., and Garnett, A.(eds)(1997). Managing Drug Supply. West Hartford, Connecticut, USA: Kumarian Press.
3. Holloway, K. (2006). Understanding Rational Use of Medicines. Contact no: 183 Autumn/Winter 2006 p 2-4. [Online] Available: http://www.oikoumene.org/fileadmin/files-main/documents/p4/contact/con-183-epdf
4. Khor, M (2005). Medicines Becoming Useless Due To Overuse, Global Trends. Third World Network, 6 June2005 [Online] Available: http://www.twn.side.org.sg/title2/gtrends57.htm
5. (MOH) Ministry of Health (2000). National Strategic Document for the Implementation of a Pharmaceutical Policy in Cameroon. Yaounde: Ministry of Public Health Cameroon
6. Jamea, J (2008) Cameroon: Stopping the Sales, Dispensing of Medicines By Unqualified Persons. allafrica.com, 16 March 2008
7. World Bank (1995) Cameroon: diversity, growth and poverty reduction. Report no. 13167-CM. Population and Human Resources Division, Central and Indian Ocean Department, African Regional Office.
8. Nkoa, C. F. and Ongolo-Zogo (2009) Scaling up enrolment in community based health insurance in Cameroon. Policy Brief. Centre for the Development of Best Practices in Health, Yaounde Central Hospital
9. Tiko (2011), In Encyclopedia Britannica. [online] Available : http://www.britannica.com/EBchecked/topic/597511/TIKO Downloaded 2011/02/11
10. World Bank (2008) Cameroon Poverty Reduction Strategy, the Heavily Indebted Poor Countries Initiative and the Millenium Development Goals. [Online] Available: http://go.worldbank.org/G1AZYHQVV0/ Downloaded 2008/11/01
11. World Health Organization (2010) Cameroon: Health profile. World Health Organisation, World Health Statistics. World Health Organisation. Last update 13 August 2010
12. Rasmussen, Z. R., Rahim, M., Streefland, P. S., Hardon, A.,
and Juroonisa (1996) Enhancing appropriate medicine use in the Karakoram Mountains. Community drug use studies. Amsterdam: Het Spinhuis; 1996
13. Hardon, A., and van der Geest, S (1987) Hazards of Self Medication. World Health Forum Vol. 8. p 469-471
14. Senah, K. A. (1994). ‘Blofa tshofa: Local perception of medicines in a Ghanaian coastal community.’ In: N. L Etkin and M. L Tan (eds), Medicines: Meanings and contexts. Quenzon City: HAIN: 83-101.
15. Hardon, A. P. (1987) The use of modern pharmaceuticals in a Filipino village: Doctors’ perception and self medication.’ Social Science and Medicine 25(3): 277-292.
16. Haafkens, J. (1997) Rituals of Silence: Long term tranquilizer use by women in The Netherlands. A social case study. Amsterdam: Het Spinhuis publishers 1997.
17. Hardon, A.P., Hodgkin, C. and Fresle, D. (2004). How to investigate the use of medicines by consumers. World Health Organisation and University of Amsterdam, 2004
18. Van der Geest, S., and Hardon, A. (1990) Self Medication in Developing Countries Journal of Social and Administrative Pharmacy. 7(4): 199-205
19. Van der Geest, S., and Whyte, S. R. (1991) ‘The charm of medicines: metaphors and metonyms.’ Medical Anthropology Quarterly 3(4): 345-367.
20. Van der Geest, S. (1982) Part 1: The efficiency of Inefficiency: Medicine Distribution in SouthCameroon. Social Science and Medicine 16(24) 2145- 2153.
21. Shaw, R. P., and Griffin, C. (1995). Financing health care in sub-Saharan Africa through user fees and insurance. Washington DC: World Bank.
22. Van der Geest, S. (1991) Marketplace Conversation in Cameroon: How and Why Popular Medical Knowledge Comes into Being. Culture, Medicine and Psychiatry 15: 69-90, 1991
23. Hours, B. (1985). L’etat sorcier: Sante publique et societe au Cameroon. Paris: L’Harmattan .International conference on national medicinal policies – the way forward. Australian Pr escriber 1997; 20 (Suppl 1).
24. Van der Geest, S. (1987) Self-care and The Informal Sale of Drugs in South Cameroon. Social Science and Medicine 25(3) 293-305
25. Holloway, K. (August 2005). Impact of Health Care Systems on Drug Use Institut Pasteur Euroconferences, Paris, October 20-25, 2005 [ABSTRACT] [Online] Available: http://www.pasteur.fr/application/euroconf/antiinfectionstherapies/4_Holloway_abstract.pdf
26. Alubo, S.O. (1985) Drugging the Nigerian People: The Public Hazards of Private Profits In The Impact of Development and Modern Technologies in Third World Health. Barbara E. Jackson and Antonio Ugalde, eds. Pp. 89-113. Williamsburg, VA: Studies in Third World Science, No. 34.
27. Groom, A., and Hedlund, K. (1998). Promoting Appropriate Drug Use in Missionary Health Facilities in Cameroon. Action Programme on Essential Drugs, World Health Organisation WHO/DAP/98.14.
28. Commeyras, C., Ndo, J. R., Merabet, O., Kone, H., and Rakotondrabe, F. P. (2006) Caractéristiques de la consommation de soins et de médicaments au Cameroun. Cahiers d’études et de recherches francophones / Santé. Volume 16, Numéro 1, 13-9, Janvier-Février-Mars 2006, Étude originale [Online] Available : http://www.john-libbey-eurotext.fr/fr/revues/sante_pub/san/sommaire.phtml?cle_parution=1276

17 Southern Med Review Vol 4 Issue 1 April 2011
Review Article
Assessing pharmacists’ impacts in primary health care: are we asking the right questions?Peri Joanne Ballantyne
Department of Sociology, Trent University, Peterborough, Ontario, Canada.
Address for Correspondence: Peri Joanne Ballantyne, Department of Sociology, Trent University, Peterborough, Ontario, Canada. E-mail: [email protected]
Citation: Ballantyne PJ. Assessing pharmacists’ impacts in primary health care: are we asking the right questions? Southern Med Review (2011) 4;1:17-21 doi:10.5655/smr.v4i1.76
AbstractIn some settings, steps are being taken to more fully integrate pharmacists in primary health care as a means of improving the public’s health and reducing drug-related iatrogenesis. Yet, evidence of improvement in health outcomes from pharmacists’ inputs is mixed; the diversity of research approaches and methodologies makes it difficult to reach an overall conclusion about it. A detailed review and analysis of two published articles using different methodological approaches to assess the role of community pharmacists in primary health care, but similarly reporting unfavourable findings regarding pharmacists’ impacts, is conducted. The Randomized Controlled Trials (RCT) design did not account for possible within-group differences in the delivery of the pharmacist intervention, and could not ascertain there were differences in pharmaceutical care received by intervention and control group heart failure patients. The RCT did not include an evaluation of pharmacists’ recommendations to physicians. The qualitative discourse analysis did not distinguish between patients’ response to pharmacists’ recommendations and the appropriateness of those recommendations. Researchers face two key challenges in demonstrating pharmacist impacts in primary care. The first is methodological – and relates to the need to identify, measure and evaluate the range and complexity of pharmacists’ work in conducting medication review and pharmaceutical care. The second relates to the differing levels of status and power of two key players in the field of medicines-related health care – the physician and pharmacist –a relationship whose contribution to ‘negative impact’ studies needs consideration. An appeal for ‘methodological creativity’ in pharmacist impact studies is made.
Keywords: pharmacist-impacts; pharmaceutical public health; methodology review; pharmacist-physician relationship
There are hundreds of individual pharmacist-impact studies
examining specific populations (i.e. elderly), specific disease
categories (i.e. asthma, hypertension) and various outcomes
(humanistic and quality of life, economic, clinical), and it is not
my intent to review these here. Published reviews of this literature
indicate that, given the variability in patient populations, disease
states, and pharmacists’ interventions included – and the varied
positive, neutral, and negative findings of individual studies, it
is difficult to reach an overall conclusion about the impact of
pharmacists’ health care provision on patient outcomes10-13.
Holland and colleagues11 provide a most strenuous argument for
the need to clarify what is known about pharmacists’ impacts
on the public’s health. In their review, Holland et al. examine
eight large studies of medication review in older populations.
They conclude that “the most successful interventions have
been delivered by small numbers of pharmacists working in
close liaison with primary care physicians, but that services…
set up at a distance from physicians, have either failed to
BackgroundGovernments in Canada, Britain and elsewhere are increasingly
recognizing the potential of a fuller integration of pharmacists
in primary health care as a means of improving the public’s
health and reducing drug-related iatrogenesis. For example,
the UK “Choosing Health through Pharmacy”1,2 initiative was
rolled out to enhance pharmaceutical-related public health
and the pharmacist’s role in it. In Ontario, Canada, in 2007
the Medscheck’3,4 program was piloted, initially providing cost-
free (government funded) pharmacist counselling to Ontarians
taking 3 or more medications for a chronic condition, and
expanded in 2010 to all residents of licensed long-term care
homes, all Ontarians living with diabetes, and to home-bound
persons not able to attend their community pharmacy for the
service. The growing recognition of pharmacy’s responsibility for
the publics’ uses of medicines is also reflected in pharmacists’
evolving role as prescribers – worldwide5; in Canada6,7 the UK8
and the US9.

18 Southern Med Review Vol 4 Issue 1 April 2011
Assessing pharmacists’ impacts in primary health care: are we asking the right questions?
deliver clear positive outcomes, or have potentially worsened
health outcomes” (p. 92). These authors question the logic of
the UK government investment of £40 million for community
pharmacist led services1, asserting:
…medication review, like drugs themselves, has the potential to
yield benefits, but may also cause harm. The [medication review]
intervention delivered by professionals not primarily responsible
for prescribing decisions should be considered in the same way
as other health technologies and be expected to adequately
demonstrate not just effectiveness, but also cost effectiveness
before being introduced more widely. At the moment, the jury is
still out on this newly promoted form of public health pharmacy
(pp. 92-93)11”.
I argue here that two key challenges confront researchers
seeking to clarify the impacts of pharmacist efforts in primary
care. The first is methodological – and relates to the requirement
that research studies identify, measure and evaluate the range
and complexity of pharmacists’ work in conducting medication
review and pharmaceutical care. The second relates to the
differing levels of status and power of the two key players in
the field of medicines-related health care – the physician and
pharmacist – a relationship whose contribution to ‘negative’ or
‘positive impact’ studies needs to be carefully examined.
In this article, I conduct a detailed critical analysis of two empirical
studies taking different methodological approaches to assessing
the role of community pharmacists in primary health care, but
similarly reporting ‘unfavourable findings’ regarding the role
of pharmacists in improving patient outcomes. I summarize
how pharmacists’ impacts were evaluated in each study; and
re-direct attention to the array of pharmacist activities – and
to pharmacist-physician relations that – had they been more
closely scrutinized in each study - might have led the authors to
different, potentially more positive, conclusionsi.
Reviewing how we analyze pharmacist-impacts: two illustrative casesThe two studies examined here include a randomized controlled
trial of the effectiveness of visits from community pharmacists
for patients with heart failure15; and a qualitative discourse
analysis of the advice giving role of the pharmacist during
consultations for medication review with patients aged 80 or
more16. In the following paragraphs, the key design features and
results of each study are examination and discussed in detail.
The Holland et al. randomized controlled trial (RCT)15, included
149 heart failure patients in a pharmacist-intervention group,
and 144 heart failure patient-controls who received ‘usual care’.
The authors’ recognition of the need for specialist personnel to
deliver education and self-management intervention to heart
failure patients; a shortage of specialist staff, and an abundance
and wide availability of community pharmacists motivated the
study.
The intervention involved two home visits by one of 17
community pharmacists within 2 and 8 weeks of patients’
discharge from hospital, and included numerous inputs:
intervention pharmacists educated patients about heart failure
and their medications; they gave basic exercise, dietary and
smoking cessation advice; they encouraged completion of
simple sign and symptom monitoring diary cards; they removed
discontinued medication. Intervention pharmacists were also
required to provide recommendations to the general practitioner
and the local pharmacist – regarding the need for medication
adherence aids15.
Intervention pharmacists had post-graduate qualifications
in pharmacy practice or recent professional development in
therapeutics. All intervention pharmacists had 7 contact training
hours including a lecture on heart failure, heart failure drugs,
exercise, diet and smoking cessation; more than half attended
two evening training events on communication skills (4 contact
hours); 14/17 intervention pharmacists received training in
medication review as part of previous trial (14 contact hours),
the other 3 received additional medication review training (1
day)15.
The primary outcome was total emergency admissions to hospital
at 6 months. The secondary outcomes included mortality;
quality of life, medication adherence; a heart failure self care
behaviour scale; and primary care activity. The authors reported
finding no significant differences in hospital admissions at six
months, quality of life, or mortality between the intervention-
group patients and heart failure patients who received ‘usual
care’15.
In this study, the authors’ aims to understand the impact
of pharmacists’ care on an extremely vulnerable patient
population is laudable. However, a vision of pharmacists’ care as
‘standardized’ and thus as suitable for a RCT is concerning, and
leads to a number of questions pertaining to the design of the
study and its findings. Here, I consider the following: a) was the
intervention different from ‘usual care’ provided to heart failure
patients?; b) in what ways are the study outcomes problematic?;
and c) what might an analysis of intervention pharmacists’
recommendations to patients and physicians have taught us
about the appropriateness of (requirement for) pharmacists care
of heart failure patients?
Question a) suggests a need to examine the standards of
practice in pharmacy, specifically, professional autonomy around
the delivery of ‘pharmaceutical care’. As with other professional
occupations, pharmacy practice involves the provision of
standardized and non-standardized services to members of
the public17. In this study, patients in the control-group may
have encountered pharmacists with similar qualifications to
the intervention group pharmacists; and ‘usual care’ for the
control group heart failure patients may have been very similar
to the care provided to intervention group patients. That is,
if good pharmacists deliver pharmaceutical care – a hallmark
of the claim to professional status, involving the pharmacist’s
i This analysis is an elaboration of an editorial addressing the same issue, published in the British Medical Journal in 200714

19 Southern Med Review Vol 4 Issue 1 April 2011
Assessing pharmacists’ impacts in primary health care: are we asking the right questions?
cooperation with the patient and other professionals in
implementing a therapeutic plan that addresses the individual
needs of the (heart failure) patient18 – then the ‘intervention’ in
the study may have been redundant.
Further, like other health professionals, pharmacists
have tremendous autonomy in their everyday delivery of
pharmaceutical care. This means that of the 17 pharmacists
who participated in the ‘intervention’, the quality and nature
of pharmaceutical care delivered to heart failure patients was
likely quite variableii. In this study, the impact of variation in the
‘intervention’ was not examined in a systematic way (it is not
a feature of the RCT), but it might have been. For example, it
was reported that 91% of patients received one or two visits
from [intervention] pharmacists15, but differences in outcomes
for intervention-group patients who received 1 rather than 2
visits were not assessed.
Thus, the potential lack of differentiation in pharmacy-related
services received by intervention- and control-group patients,
within-group variation [among intervention– but also among
control-group pharmacists], as well as the range and complexity
of intervention-pharmacists’ activities suggest the RCT may not
be the best methodology to assess the impacts of pharmacist-
delivered primary health care.
Question b) is related to the outcomes of the RCT which included
no statistically significant differences in hospital readmissions at
six months, quality of life, or mortality between intervention-
group patients and heart failure patients who received ‘usual
care’; and a 17% overall increase in primary care activity in the
intervention- as compared to the control-group15.
The reporting of global outcomes in this way (i.e. reporting
of differences between intervention and control groups, as is
standard in RCT studies) obscures an analysis of the processes
that led to the particular outcomes assessed. For example, it
could be interpreted that intervention pharmacists’ activities led
to necessary primary care – visits to doctors, medication reviews
– and sometimes to hospital admissions – and that these actions
may have reduced illness and possibly saved lives. Instead, the
global outcomes were interpreted as negative, based on an
assumption that a successful intervention would reduce heart
failure patients’ use of any health care resources.
An additional outcome measured in the study was medication
adherence, which was reported to be unusually high in both
intervention and control groupsiii. This finding, too, makes
plausible an interpretation that all heart failure patients received
similar pharmaceutical care from all pharmacists (intervention,
community or hospital pharmacists), or from other health care
professionals (physicians, nurses) encountered since their first
heart failure incident.
Question c) pertains to the limitation of the RCT methodology
to capture and evaluate details such as whether pharmacists’
recommendations to physicians were relevant, whether/to
what extent physicians responded to them; and the effects
of action/non-action on individual patient outcomes. In this
study, it is reported that pharmacists’ home visits to patients
with heart failure resulted in 384 recommendations to general
practitioners15. These recommendations were made despite the
very high levels of adherence mentioned previously - in other
words, the recommendations to doctors appear not to have
been motivated by patient medication non-adherence. Further,
the authors reported that only 51% of recommendations
were fully or partly enacted by general practitioners after the
pharmacists’ first patient home-visits, while no data were
provided as to whether second home-visit recommendations
were enacted by GPs15.
This aspect of the study highlights the differing levels of status
and power of the two key players in the field of medicines-
related health care – the physician and pharmacist – and the
uneven playing field in which pharmacists interact with patients.
The failure of physicians to follow up on a large proportion of
(potentially life saving) recommendations made by pharmacists
regarding seriously ill heart failure patients highlights both
the discretionary power of the physician as well as the lack
of respect shown to pharmacists by physicians (at least in this
particular study). Without a clear analysis of the consequences
of pharmacists’ recommendations – whether they were
appropriate, whether the physician heeded them, and what
particular effect was produced as a result of the pharmacist’s
recommendation - it seems premature to judge the impact of a
pharmacist-led intervention with heart failure patients.
In the second study, Salter et al., examined elderly patients’
responses to advice given by a pharmacist during medication
reviews. This is an important study that highlights the value of
using qualitative methods to examine the practice of medication
review, and to understand it from a patient-perspective. In
the article, the authors report that despite finding many
opportunities to offer advice, information and instruction,
the didactic, pharmacist-initiated and controlled encounter
was frequently resisted or rejected by elderly patients and
‘interactional difficulties’ with the pharmacist ensued16. Through
analysis of the discourse between pharmacist and patient, the
authors rightfully problematize the practice of medication
review, and raise questions related to the potential negative
impact of certain forms of interaction.
Salter et al. are emphatic about the negative impact of
pharmacists’ advice-giving – the major finding and the emphasis
of discussion in this article. The authors emphasize the potential
harm of (unsolicited) advice-giving on patients’ sense of
competence and self-governance, observing that pharmacists
ii The study authors also were interested in the delivery of the intervention by pharmacists. They recorded a selection of pharmacists’ visits to investigate the intervention’s delivery and the pharmacists’ communication skills (p. 2 of 7), reporting that each component of the intervention was delivered, and that pharmacists used good consultation styles (p. 6 of 7)15.iii In a recent review, it is estimated that general non-adherence is about 20-50%19; whereas Holland et al. report adherence levels at ~ 95% for both groups (using mean adherence scores), at baseline, at 3 months and 6 months15.

20 Southern Med Review Vol 4 Issue 1 April 2011
Assessing pharmacists’ impacts in primary health care: are we asking the right questions?
“provided advice, information or instruction on a constant
basis” (p.3 0f 6); and that almost no patient-initiated requests
for advice or information were observed16. They reported that
in resisting or rejecting pharmacists’ advice, “patients adopted
a variety of conversational strategies, including direct or indirect
challenges to the pharmacists’ authority and knowledge
boundaries” (p. 3 of 6)16. The authors reported that “one of
the strongest rebuttals to the pharmacists’ attempts to counsel
and give advice was patients’ use of the higher authority of the
doctor” (p. 4 of 6)16.
However, in this study there was a failure to recognize the
important distinction between patients’ unwillingness to
accept pharmacists’ advice from the appropriateness of that
advice itself. Its design did not include the identification and
classification of the specific drug-related problems identified
which would have enabled an assessment of the potential harm-
averted by the pharmacist’s advice. Further, the pharmacist’s
drug review and advice may have led patients to seek necessary
care that resulted in necessary attention …even if, in interaction
with the pharmacist, the advice remained unacknowledged or
was resisted or rejected.
At the least, the findings from this study, as with the previous
one, indicate that pharmacists uncovered numerous problems
regarding patients’ medicine regimes. That the patients were
uncomfortable with the (unsolicited) input from the pharmacist
doesn’t detract from that important conclusion.
ConclusionI have argued that two key challenges need to be addressed in
research designed to assess the effectiveness of the pharmacists’
provision of primary care. First is the limitations imposed
by a standardization method like the RCT used in a context
where professional services are not readily standardized. The
assessment of the ‘pharmacist-consultation-as-intervention’
does not provide any means of discerning the diverse ‘inputs’
of an individual pharmacist in consultation with an individual
patient. Hence, study findings of differences between patients
assigned to intervention and control groups in the trial run
the risk of internal invalidity…a failure to discern that within
an ‘intervention’, specific aspects of pharmacists’ work may
improve patient outcomes, while other aspects may alienate the
patient, or otherwise fail to impact his or her outcomes.
A second key challenge relates to the differing levels of status
and power of two key players in field of medicines-related health
care – the physician and the pharmacist – whose contribution
to outcome studies needs consideration. The importance
of this relationship was alluded to by Holland et al. in their
review of pharmacist-impact research, where it was observed
that successful interventions involved pharmacists working
closely with primary care physicians11. In my review here, I
have suggested how in future research, if study designs are
to distinguish the relevance of pharmacists’ recommendations
from patients’ and physicians’ responses to them, very different
conclusions about the impact of pharmacists’ involvement in
primary health care may be reached.
AcknowledgementsThis paper elaborates on an editorial by the author published in
the BMJ in 200714, and a presentation at the 15th International
Social Pharmacy Workshop, Queenstown, New Zealand, July,
2008.
References1. Reports. Choosing health through pharmacy implementation.
The Pharmacueutical Journal 278(7442). March 10 2007. p. 285.
2. Choosing health through pharmacy – a programme for pharmaceutical public health 2005 – 2015. UK Department of Health, 2005. www.dh.gov.uk/publications.
3. About MedsCheck, Ministry of Health and Long Term Care, Government of Ontario, Canada, Queen’s Printer for Ontario. http://www.health.gov.on.ca/en/public/programs/drugs/medscheck/medscheck_original.aspx; Accessed February 24, 2011.
4. Ministry of Health and Long Term Care, Government of Ontario, Canada. (2007). McGuinty Government Unveils New Health Care Service for Ontarians. Medscheck Offers Free, One-on-One Pharmacist Review of Clients’ Medication. http://www.hlth.gov.on.ca/medscheck_nr_05_20070416.pdf Accessed February 24, 2011.
5. Emmerton L, Marriott J, Bessell T, Nissen L, Dean L. Pharmacists and prescribing rights: review of international developments. J Pharm Pharmaceut Sci 2005; 8(2): 217-225.
6. Puxley C. (2008). Ontario Pharmacists Could Become the Latest in Canada to Prescribe Drugs. Canadian Press. http://redorbit.com/modules/news/tools.php?tool=print&id=1411450
7. Pearson GJ. (2007). Evolution in the practice of pharmacy – not a revolution! CMAJ 176(9): 1295-96. April 24, 2007.
8. Weiss MC & Sutton J. The changing nature of prescribing: pharmacists as prescribers and challenges to medical dominance. Soc Hlth Illness 2009, 31(3): 406-421.
9. Status of collaborative drug therapy management in the United States, March 2004. Am J Health Syst Pharm 2004;61:1609-10.
10. Pickard AS, Hung S-Y. An update on evidence of clinical pharmacy services’ impact on health-related quality of life. Ann Pharmacother 2006;40:1623-34.
11. Holland R, Smith R, Harvey I. Where now for pharmacist led medication review? J Epidemiol Community Health 2006; 60:92-93.
12. Van Wijk BLG. Effectiveness of interventions by community pharmacists to improve patient adherence to chronic medication: a systematic review. Ann Pharmacother 2005;39(2): 319-28.
13. Anderson C, Blenkinsopp A, Armstrong M. Feedback from community pharmacy users on the contribution of community pharmacy to improving the public’s health: a systematic review of the peer reviewed and non-peer reviewed literature 1990 – 2002. Health Expectations 2004; 7: 191-202.
14. Ballantyne P. (2007). The role of pharmacists in primary care. British Medical Journal (May 26) 334: 1066-1067. (Editorial).
15. Holland R, Brooksby I, Lenaghan E, Ashton K, Hay L, Smith R, et al. Effectiveness of visits from community pharmacists for

21 Southern Med Review Vol 4 Issue 1 April 2011
Assessing pharmacists’ impacts in primary health care: are we asking the right questions?
patients with heart failure: HeartMed randomised controlled trial. BMJ 2007; 334/ BMJ, doi:10.1136/bmj.39164.568183.AE (published 23 April 2007).
16. Salter C, Holland R, Harvey I, Henwood K. “I haven’t even phoned my doctor yet.” The advice giving role of the pharmacist during consultations for medication review with patients aged 80 or more: qualitative discourse analysis. BMJ 2007;334; 1098; BMJ, doi:10.1136/bmj.39164.568183.AE (published 23 April 2007).
17. Buerki RA and LD Vottero. The purposes of professions in society. In Pharmaceutical Care, CH Knowlton and RP Penna (eds). Pp. 3-17. Chapman and Hall, 1996.
18. Hepler, D.D., Strand, L.M. Opportunities and responsibilities in pharmaceutical care, Am J Pharm Ed, 1989, 53, 7S – 15S.
19. Kripalani, S., Yao, X., & Haynes, B. Interventions to enhance medication adherence in chronic medical conditions. Archives of Internal Medicine, 2007,167, 540-550.
22 Southern Med Review Vol 4 Issue 1 April 2011
Analysis
The selection of essential medicines in China: progress and the way forwardDifei Wang, Xinping Zhang
School of Health and Medical Management, Tongji Medical College of Huazhong University of Science and Technology, Wuhan, China.
Address for Correspondence: Xinping Zhang. School of Medical and Health Management, Tongji Medical College of Huazhong University of Science and Technology, Wuhan City, Hubei Province. Peoples Republic of China. E-mail: [email protected]
Citation: Wang Wang D, Zhang X. The selection of essential medicines in China: progress and the way forward. Southern Med Review (2011) 4;1:22-28 doi:10.5655/smr.v4i1.71
AbstractObjective: The objective of this paper is to analyze the development of China’s national essential medicines list (NEML) from 1979 to 2010. These findings were then used as a basis to provide suggestions on how to improve essential medicines selection in China.
Methods: The literature search was conducted on the issues related to “essential medicines”, “China” and “national essential medicines lists”. The information on essential medicines principles, criteria and procedures was also reviewed. Literature review and key informants interview were also conducted. Key informants were interviewed mainly on how medicines are selected at central and provincial level and how medicine selection could be improved in China.
Results: In the past, China’s national essential medicines list has not been successful in promoting access to essential medicines. Reasons for this failure included biased selection and non evidence-based selection. Analysis of China’s essential medicines list and WHO’s generic essential medicines show that two lists varied substantially in disease coverage. The NEML failed to cover some diseases of public health significance in China such as cancers. The way medicines are classified and defined is also different between the two lists, e.g., medicines in the NEML are listed without defining the dose. There are differing levels in transparency, involvement, collaboration and accountability in the way the medicines are selected. Lastly, most of the provinces selected additional medicines to complement NEML. However, in 2009 version of Chinese essential medicines list, some improvements have been noted.
Conclusions: There has been significant improvement in China’s NEML. The latest NEML made progress by setting achievable targets, adopting balanced guidelines and updating principles and criteria. However, there is still need to increase evidence-based selection, reassess which diseases are in need to be covered and define medicines with dosage forms and doses. In selecting medicines, efforts should be made towards higher transparency, involvement, collaboration and accountability. Provincial selection should be improved by establishing relevant measures and receiving technical support from the national government.
Keywords: essential medicines, medicines list, selection, China
total income in public health facilities in 2009 was generated
by using and selling medicines5. The high medicine expenditure
was indeed attributable to irrational use of medicines and
prescriber’s preference of high price medicines over low price
genenics6. The use and access of medicines could be improved
by proper selection and implementation of a national essential
medicines list (NEML). In the latest health reform initiated in
2008, the government made a commitment to provide basic
health care, including essential medicines, to all by 20207.
This paper describes and identifies the progress and challenges
in the essential medicines selection from 1979 to 2010. We
compare the latest NEML to the WHO model list in terms of
IntroductionEssential medicines (EMs) are medicines that address the
priority health care needs of the population. They are selected
with regards to public health relevance, evidence on efficacy
and safety and comparative cost-effectiveness1. Establishing
a national essential medicines list (NEML) is a core element to
national pharmaceutical policy2,3.
As the largest developing country with the population of more
than 1.34 billion and medicines accounting for over 40% of
total health expenditure, promoting essential medicines use
in China is extremely important. China’s public health facilities
sell medicines for profit with a mark up of 15%4. Over 45% of
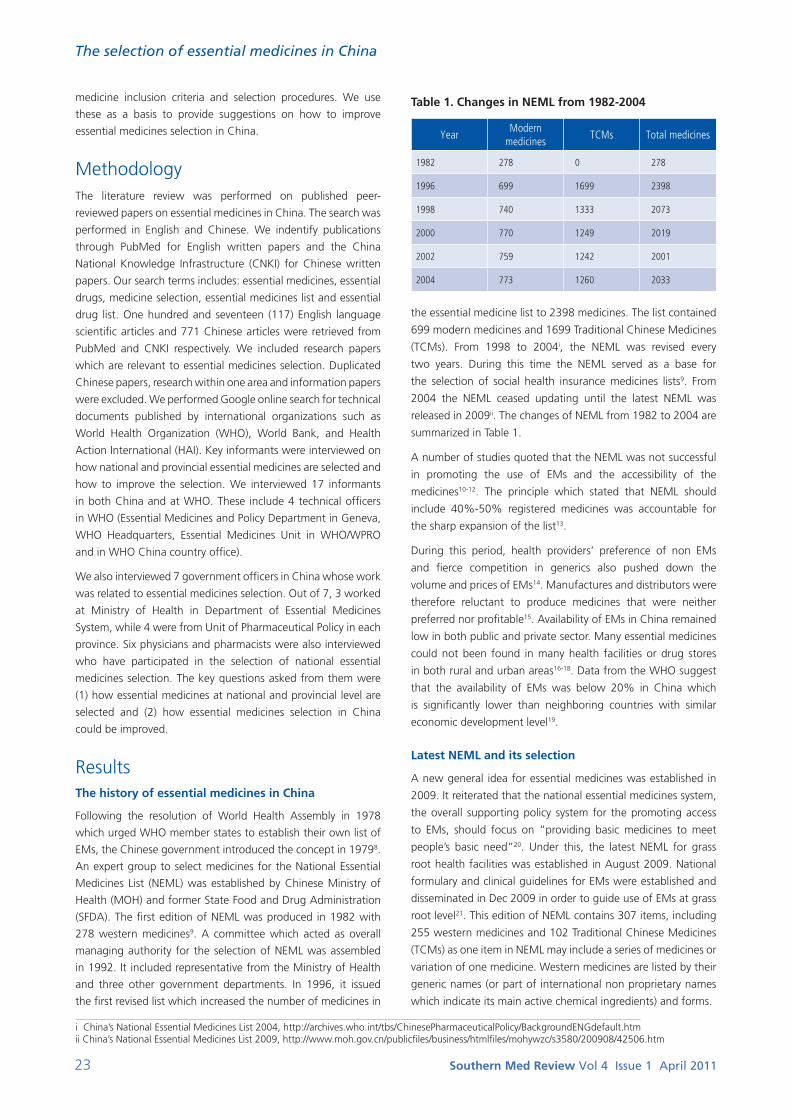
23 Southern Med Review Vol 4 Issue 1 April 2011
The selection of essential medicines in China
medicine inclusion criteria and selection procedures. We use
these as a basis to provide suggestions on how to improve
essential medicines selection in China.
MethodologyThe literature review was performed on published peer-
reviewed papers on essential medicines in China. The search was
performed in English and Chinese. We indentify publications
through PubMed for English written papers and the China
National Knowledge Infrastructure (CNKI) for Chinese written
papers. Our search terms includes: essential medicines, essential
drugs, medicine selection, essential medicines list and essential
drug list. One hundred and seventeen (117) English language
scientific articles and 771 Chinese articles were retrieved from
PubMed and CNKI respectively. We included research papers
which are relevant to essential medicines selection. Duplicated
Chinese papers, research within one area and information papers
were excluded. We performed Google online search for technical
documents published by international organizations such as
World Health Organization (WHO), World Bank, and Health
Action International (HAI). Key informants were interviewed on
how national and provincial essential medicines are selected and
how to improve the selection. We interviewed 17 informants
in both China and at WHO. These include 4 technical officers
in WHO (Essential Medicines and Policy Department in Geneva,
WHO Headquarters, Essential Medicines Unit in WHO/WPRO
and in WHO China country office).
We also interviewed 7 government officers in China whose work
was related to essential medicines selection. Out of 7, 3 worked
at Ministry of Health in Department of Essential Medicines
System, while 4 were from Unit of Pharmaceutical Policy in each
province. Six physicians and pharmacists were also interviewed
who have participated in the selection of national essential
medicines selection. The key questions asked from them were
(1) how essential medicines at national and provincial level are
selected and (2) how essential medicines selection in China
could be improved.
ResultsThe history of essential medicines in China
Following the resolution of World Health Assembly in 1978
which urged WHO member states to establish their own list of
EMs, the Chinese government introduced the concept in 19798.
An expert group to select medicines for the National Essential
Medicines List (NEML) was established by Chinese Ministry of
Health (MOH) and former State Food and Drug Administration
(SFDA). The first edition of NEML was produced in 1982 with
278 western medicines9. A committee which acted as overall
managing authority for the selection of NEML was assembled
in 1992. It included representative from the Ministry of Health
and three other government departments. In 1996, it issued
the first revised list which increased the number of medicines in
Table 1. Changes in NEML from 1982-2004
YearModern
medicinesTCMs Total medicines
1982 278 0 278
1996 699 1699 2398
1998 740 1333 2073
2000 770 1249 2019
2002 759 1242 2001
2004 773 1260 2033
the essential medicine list to 2398 medicines. The list contained
699 modern medicines and 1699 Traditional Chinese Medicines
(TCMs). From 1998 to 2004i, the NEML was revised every
two years. During this time the NEML served as a base for
the selection of social health insurance medicines lists9. From
2004 the NEML ceased updating until the latest NEML was
released in 2009ii. The changes of NEML from 1982 to 2004 are
summarized in Table 1.
A number of studies quoted that the NEML was not successful
in promoting the use of EMs and the accessibility of the
medicines10-12. The principle which stated that NEML should
include 40%-50% registered medicines was accountable for
the sharp expansion of the list13.
During this period, health providers’ preference of non EMs
and fierce competition in generics also pushed down the
volume and prices of EMs14. Manufactures and distributors were
therefore reluctant to produce medicines that were neither
preferred nor profitable15. Availability of EMs in China remained
low in both public and private sector. Many essential medicines
could not been found in many health facilities or drug stores
in both rural and urban areas16-18. Data from the WHO suggest
that the availability of EMs was below 20% in China which
is significantly lower than neighboring countries with similar
economic development level19.
Latest NEML and its selection
A new general idea for essential medicines was established in
2009. It reiterated that the national essential medicines system,
the overall supporting policy system for the promoting access
to EMs, should focus on “providing basic medicines to meet
people’s basic need”20. Under this, the latest NEML for grass
root health facilities was established in August 2009. National
formulary and clinical guidelines for EMs were established and
disseminated in Dec 2009 in order to guide use of EMs at grass
root level21. This edition of NEML contains 307 items, including
255 western medicines and 102 Traditional Chinese Medicines
(TCMs) as one item in NEML may include a series of medicines or
variation of one medicine. Western medicines are listed by their
generic names (or part of international non proprietary names
which indicate its main active chemical ingredients) and forms.
i China’s National Essential Medicines List 2004, http://archives.who.int/tbs/ChinesePharmaceuticalPolicy/BackgroundENGdefault.htmii China’s National Essential Medicines List 2009, http://www.moh.gov.cn/publicfiles/business/htmlfiles/mohywzc/s3580/200908/42506.htm

24 Southern Med Review Vol 4 Issue 1 April 2011
The selection of essential medicines in China
Table 2. Discrepancies between the WHO list and the NEML
ItemsThe WHO model list
16th editionNEML for grass root
level
Medicines 358 357
Western medicines 358 255
TCMs 0 102
Complementary medicines
Complementary list Provincial selection
Revising interval 2 years 3 years
Classification methodology
Anatomical Therapeutic Chemical Classification
Clinical Pharmacology Classification
Defined forms for western medicines
Yes Yes
Supporting documentsSTGs, formulary for essential medicines
National formulary and guidelines for EMs
Essential medicine list for children
Yes No
The overall managing authority called National Essential
Medicines Working Group decides the new principles and
criteria22. Medicines are listed on the basis that they should be
necessary for clinical use and disease prevention and should
be of high efficacy, safety and assured quality. They should be
convenient to use and rationally priced. The managing authority
reiterates that TCMs should be considered with same importance
as western medicines. Selecting principles and criteria apply
to both western medicines and TCMs. It also states that the
selection should “learn from international experience”22.
The Ministry of Health (MOH) is responsible for selection of
EMs for the latest NEML. The MOH has formed a committee
which consists of a pool of experts in the field of medicine,
pharmaceutical economics, pharmacy, health insurance, health
management and pricing. Experts are divided into a review group
and a consult group whose members are mutually exclusive. The
consult group evaluates medicines and proposes their opinions
on the medicines before forming candidate lists. The reviewing
group votes for the candidate lists and determines the draft list.
The draft list receives comments from government departments
before handing to managing authority for final approval23.
The WHO model list and the NEML
By comparing the WHO EM list and the NEML of China, we can
see some important differences. First, the quantity of included
western medicines varied substantially. As a result, the diseases
covered by the two lists are different. The WHO list has 358
western medicines which is 103 more than NEML. The WHO
list covers some important diseases such as cancers that the
NEML does not cover. The WHO list also covers more medicines
within some disease, e.g. there are more medicines for diabetes
in the WHO list than the NEML24. In the WHO list, medicines
are defined using doses and dosage forms. In the NEML
list medicines are only defined using dosage forms for both
western and TCMs. This influences the EMs manufacturing,
procurement and use. Second, medicine classification and
the definition of medicines varies between the two lists. The
Anatomical Therapeutic Chemical Classification (ATC-C) is used
in the WHO list to classify medicines while Clinical Pharmacology
Classification is used for western medicines in the NEML. This is
because the NEML may need to conform to other medicines
lists for social health insurance schemes. Third the WHO has
selected a complementary list which presents EMs for priority
diseases that need specialized diagnostic or monitoring facilities
and may have lower cost-effectiveness in some circumstances25.
The WHO has also selected two editions of essential medicines
for children. Even though a group of national representatives in
China urged the government to select essential medicines for
children26, no official response has been found for this appeal.
The NEML does not have complementary medicines; however,
provincial selection is allowed to add medicines to complement
NEML but must include every medicine in the NEML27. We
summarize discrepancies between the two lists in Table 2.
Discrepancies in selection
The different selection procedures of the WHO list and the
NEML could have an effect on end users. The WHO’s selection
criteria, used as a model for countries, emphasizes evidence
of medicines’ safety and efficacy, cost-effectiveness and total
cost of treatment, availability and stability of medicines and
high priority of single-compound medicines1. The NEML,
which is aimed at the needs of China, emphasizes similar
criteria of WHO’s selection with additional consideration given
to the medicines needed in grass root level, local availability,
affordability, priority diseases22.
Although it is important that China establishes its own list, the
list should be made in a way that is transparent, involves all
stakeholders and accountable to the population. The WHO
makes its list using a presenter from the expert committee who
is appointed to summarize data on comparative efficacy, safety
and cost-effectiveness. The recommendation is written by the
presenter and is sent to experts inside the WHO for review
and is posted on the WHO website for public comments. The
expert committee reviews all the information and makes final
selection recommendations28. In China, medicines are chosen
and the candidate list is made by a group of consultants. The
candidate list is sent to a review group whose members vote
for medicines in the candidate list. The draft list is built on the
result of voting29. Detailed information of selection procedures
is not revealed and information on the methods of selection is
not disclosed.
There are also differences in the number of experts and the
size of the selection committee. The expert advisory panels
and committees contain 781 experts of various areas (January
2006)30. When selecting the WHO list, 8-12 members are
chosen from expert committees for the selection of EMs, who
then make the selection decision for the WHO list28. The expert
pool for the NEML is substantially larger, containing over 3000
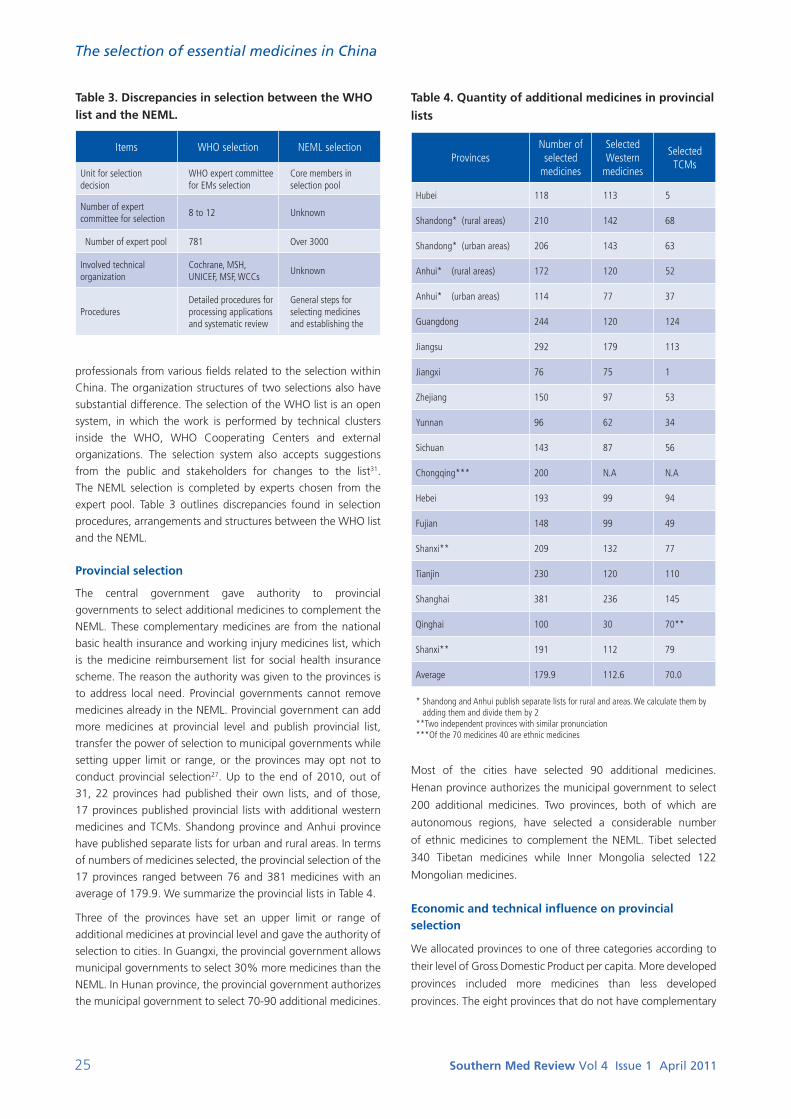
25 Southern Med Review Vol 4 Issue 1 April 2011
The selection of essential medicines in China
Table 3. Discrepancies in selection between the WHO list and the NEML.
Items WHO selection NEML selection
Unit for selection decision
WHO expert committee for EMs selection
Core members in selection pool
Number of expert committee for selection
8 to 12 Unknown
Number of expert pool 781 Over 3000
Involved technical organization
Cochrane, MSH, UNICEF, MSF, WCCs
Unknown
ProceduresDetailed procedures for processing applications and systematic review
General steps for selecting medicines and establishing the
professionals from various fields related to the selection within
China. The organization structures of two selections also have
substantial difference. The selection of the WHO list is an open
system, in which the work is performed by technical clusters
inside the WHO, WHO Cooperating Centers and external
organizations. The selection system also accepts suggestions
from the public and stakeholders for changes to the list31.
The NEML selection is completed by experts chosen from the
expert pool. Table 3 outlines discrepancies found in selection
procedures, arrangements and structures between the WHO list
and the NEML.
Provincial selection
The central government gave authority to provincial
governments to select additional medicines to complement the
NEML. These complementary medicines are from the national
basic health insurance and working injury medicines list, which
is the medicine reimbursement list for social health insurance
scheme. The reason the authority was given to the provinces is
to address local need. Provincial governments cannot remove
medicines already in the NEML. Provincial government can add
more medicines at provincial level and publish provincial list,
transfer the power of selection to municipal governments while
setting upper limit or range, or the provinces may opt not to
conduct provincial selection27. Up to the end of 2010, out of
31, 22 provinces had published their own lists, and of those,
17 provinces published provincial lists with additional western
medicines and TCMs. Shandong province and Anhui province
have published separate lists for urban and rural areas. In terms
of numbers of medicines selected, the provincial selection of the
17 provinces ranged between 76 and 381 medicines with an
average of 179.9. We summarize the provincial lists in Table 4.
Three of the provinces have set an upper limit or range of
additional medicines at provincial level and gave the authority of
selection to cities. In Guangxi, the provincial government allows
municipal governments to select 30% more medicines than the
NEML. In Hunan province, the provincial government authorizes
the municipal government to select 70-90 additional medicines.
Table 4. Quantity of additional medicines in provincial
lists
ProvincesNumber of selected
medicines
Selected Western
medicines
Selected TCMs
Hubei 118 113 5
Shandong* (rural areas) 210 142 68
Shandong* (urban areas) 206 143 63
Anhui* (rural areas) 172 120 52
Anhui* (urban areas) 114 77 37
Guangdong 244 120 124
Jiangsu 292 179 113
Jiangxi 76 75 1
Zhejiang 150 97 53
Yunnan 96 62 34
Sichuan 143 87 56
Chongqing*** 200 N.A N.A
Hebei 193 99 94
Fujian 148 99 49
Shanxi** 209 132 77
Tianjin 230 120 110
Shanghai 381 236 145
Qinghai 100 30 70**
Shanxi** 191 112 79
Average 179.9 112.6 70.0
* Shandong and Anhui publish separate lists for rural and areas. We calculate them by adding them and divide them by 2
**Two independent provinces with similar pronunciation ***Of the 70 medicines 40 are ethnic medicines
Most of the cities have selected 90 additional medicines.
Henan province authorizes the municipal government to select
200 additional medicines. Two provinces, both of which are
autonomous regions, have selected a considerable number
of ethnic medicines to complement the NEML. Tibet selected
340 Tibetan medicines while Inner Mongolia selected 122
Mongolian medicines.
Economic and technical influence on provincial selection
We allocated provinces to one of three categories according to
their level of Gross Domestic Product per capita. More developed
provinces included more medicines than less developed
provinces. The eight provinces that do not have complementary
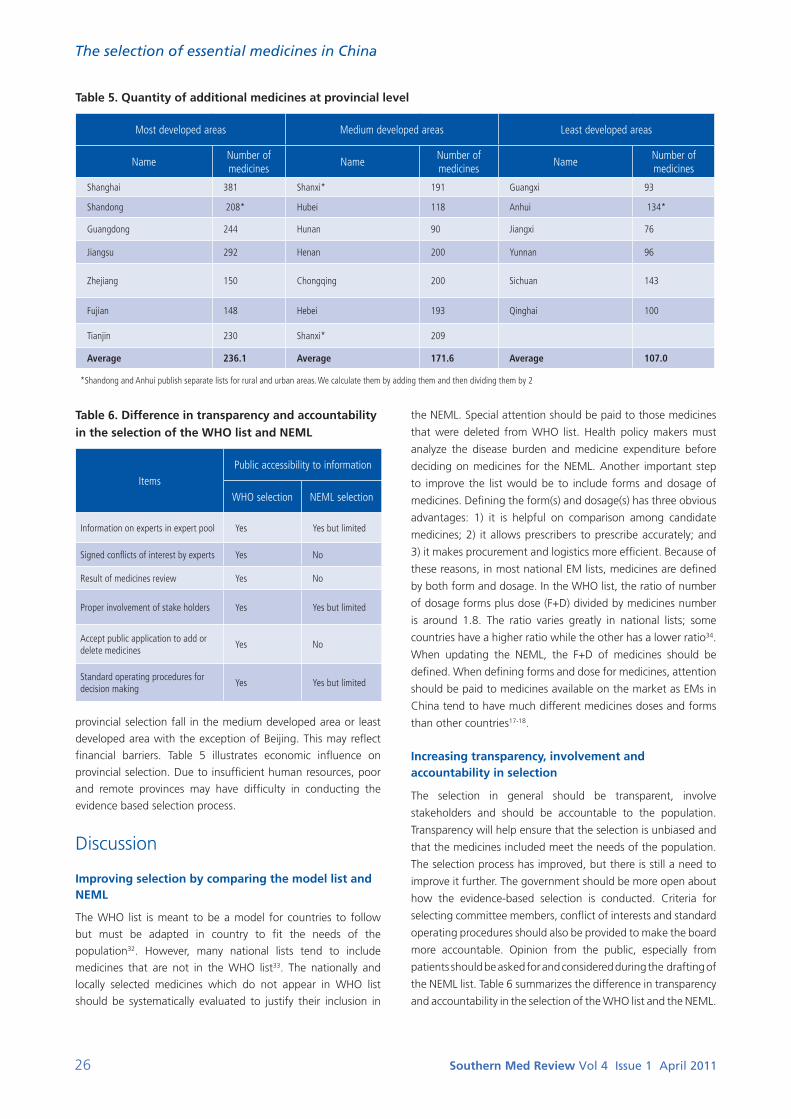
26 Southern Med Review Vol 4 Issue 1 April 2011
The selection of essential medicines in China
Table 6. Difference in transparency and accountability in the selection of the WHO list and NEML
ItemsPublic accessibility to information
WHO selection NEML selection
Information on experts in expert pool Yes Yes but limited
Signed conflicts of interest by experts Yes No
Result of medicines review Yes No
Proper involvement of stake holders Yes Yes but limited
Accept public application to add or delete medicines
Yes No
Standard operating procedures for decision making
Yes Yes but limited
provincial selection fall in the medium developed area or least
developed area with the exception of Beijing. This may reflect
financial barriers. Table 5 illustrates economic influence on
provincial selection. Due to insufficient human resources, poor
and remote provinces may have difficulty in conducting the
evidence based selection process.
Discussion
Improving selection by comparing the model list and NEML
The WHO list is meant to be a model for countries to follow
but must be adapted in country to fit the needs of the
population32. However, many national lists tend to include
medicines that are not in the WHO list33. The nationally and
locally selected medicines which do not appear in WHO list
should be systematically evaluated to justify their inclusion in
the NEML. Special attention should be paid to those medicines
that were deleted from WHO list. Health policy makers must
analyze the disease burden and medicine expenditure before
deciding on medicines for the NEML. Another important step
to improve the list would be to include forms and dosage of
medicines. Defining the form(s) and dosage(s) has three obvious
advantages: 1) it is helpful on comparison among candidate
medicines; 2) it allows prescribers to prescribe accurately; and
3) it makes procurement and logistics more efficient. Because of
these reasons, in most national EM lists, medicines are defined
by both form and dosage. In the WHO list, the ratio of number
of dosage forms plus dose (F+D) divided by medicines number
is around 1.8. The ratio varies greatly in national lists; some
countries have a higher ratio while the other has a lower ratio34.
When updating the NEML, the F+D of medicines should be
defined. When defining forms and dose for medicines, attention
should be paid to medicines available on the market as EMs in
China tend to have much different medicines doses and forms
than other countries17-18.
Increasing transparency, involvement and accountability in selection
The selection in general should be transparent, involve
stakeholders and should be accountable to the population.
Transparency will help ensure that the selection is unbiased and
that the medicines included meet the needs of the population.
The selection process has improved, but there is still a need to
improve it further. The government should be more open about
how the evidence-based selection is conducted. Criteria for
selecting committee members, conflict of interests and standard
operating procedures should also be provided to make the board
more accountable. Opinion from the public, especially from
patients should be asked for and considered during the drafting of
the NEML list. Table 6 summarizes the difference in transparency
and accountability in the selection of the WHO list and the NEML.
Table 5. Quantity of additional medicines at provincial level
Most developed areas Medium developed areas Least developed areas
NameNumber of medicines
NameNumber of medicines
NameNumber of medicines
Shanghai 381 Shanxi* 191 Guangxi 93
Shandong 208* Hubei 118 Anhui 134*
Guangdong 244 Hunan 90 Jiangxi 76
Jiangsu 292 Henan 200 Yunnan 96
Zhejiang 150 Chongqing 200 Sichuan 143
Fujian 148 Hebei 193 Qinghai 100
Tianjin 230 Shanxi* 209
Average 236.1 Average 171.6 Average 107.0
*Shandong and Anhui publish separate lists for rural and urban areas. We calculate them by adding them and then dividing them by 2
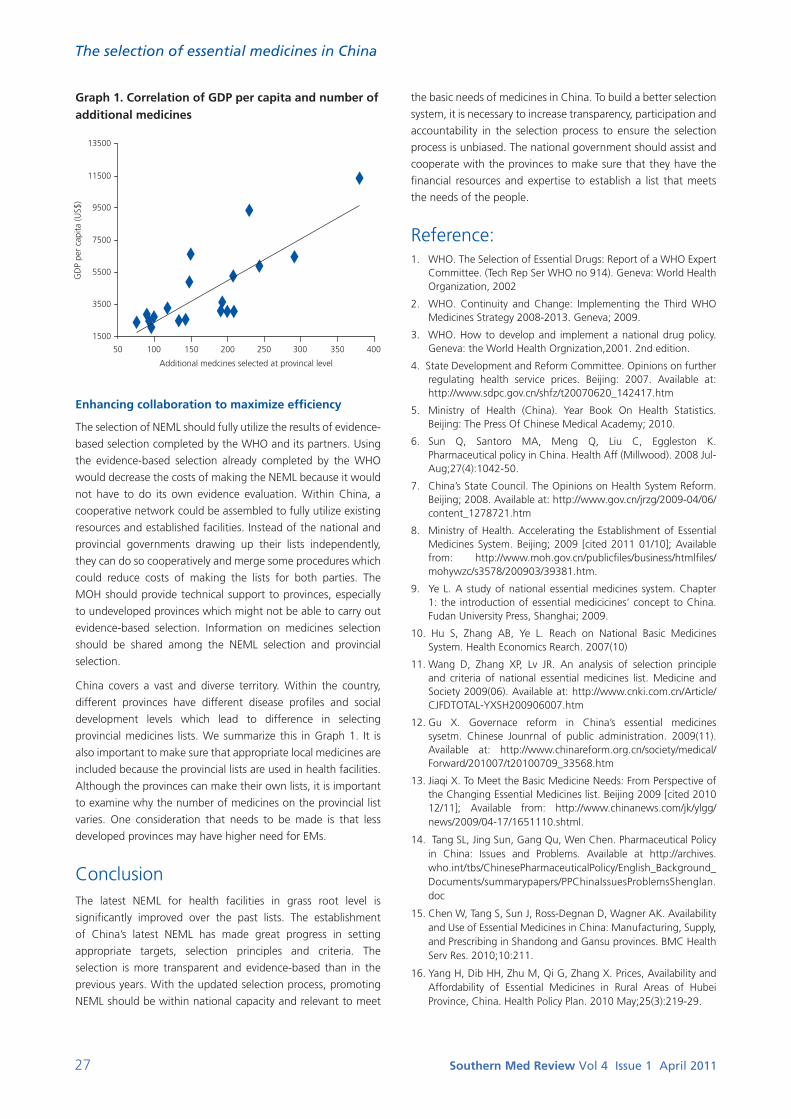
27 Southern Med Review Vol 4 Issue 1 April 2011
The selection of essential medicines in China
Graph 1. Correlation of GDP per capita and number of additional medicines
the basic needs of medicines in China. To build a better selection
system, it is necessary to increase transparency, participation and
accountability in the selection process to ensure the selection
process is unbiased. The national government should assist and
cooperate with the provinces to make sure that they have the
financial resources and expertise to establish a list that meets
the needs of the people.
Reference:1. WHO. The Selection of Essential Drugs: Report of a WHO Expert
Committee. (Tech Rep Ser WHO no 914). Geneva: World Health Organization, 2002
2. WHO. Continuity and Change: Implementing the Third WHO Medicines Strategy 2008-2013. Geneva; 2009.
3. WHO. How to develop and implement a national drug policy. Geneva: the World Health Orgnization,2001. 2nd edition.
4. State Development and Reform Committee. Opinions on further regulating health service prices. Beijing: 2007. Available at: http://www.sdpc.gov.cn/shfz/t20070620_142417.htm
5. Ministry of Health (China). Year Book On Health Statistics. Beijing: The Press Of Chinese Medical Academy; 2010.
6. Sun Q, Santoro MA, Meng Q, Liu C, Eggleston K. Pharmaceutical policy in China. Health Aff (Millwood). 2008 Jul-Aug;27(4):1042-50.
7. China’s State Council. The Opinions on Health System Reform. Beijing; 2008. Available at: http://www.gov.cn/jrzg/2009-04/06/content_1278721.htm
8. Ministry of Health. Accelerating the Establishment of Essential Medicines System. Beijing; 2009 [cited 2011 01/10]; Available from: http://www.moh.gov.cn/publicfiles/business/htmlfiles/mohywzc/s3578/200903/39381.htm.
9. Ye L. A study of national essential medicines system. Chapter 1: the introduction of essential medicicines’ concept to China. Fudan University Press, Shanghai; 2009.
10. Hu S, Zhang AB, Ye L. Reach on National Basic Medicines System. Health Economics Rearch. 2007(10)
11. Wang D, Zhang XP, Lv JR. An analysis of selection principle and criteria of national essential medicines list. Medicine and Society 2009(06). Available at: http://www.cnki.com.cn/Article/CJFDTOTAL-YXSH200906007.htm
12. Gu X. Governace reform in China’s essential medicines sysetm. Chinese Jounrnal of public administration. 2009(11). Available at: http://www.chinareform.org.cn/society/medical/Forward/201007/t20100709_33568.htm
13. Jiaqi X. To Meet the Basic Medicine Needs: From Perspective of the Changing Essential Medicines list. Beijing 2009 [cited 2010 12/11]; Available from: http://www.chinanews.com/jk/ylgg/news/2009/04-17/1651110.shtml.
14. Tang SL, Jing Sun, Gang Qu, Wen Chen. Pharmaceutical Policy in China: Issues and Problems. Available at http://archives.who.int/tbs/ChinesePharmaceuticalPolicy/English_Background_Documents/summarypapers/PPChinaIssuesProblemsShenglan.doc
15. Chen W, Tang S, Sun J, Ross-Degnan D, Wagner AK. Availability and Use of Essential Medicines in China: Manufacturing, Supply, and Prescribing in Shandong and Gansu provinces. BMC Health Serv Res. 2010;10:211.
16. Yang H, Dib HH, Zhu M, Qi G, Zhang X. Prices, Availability and Affordability of Essential Medicines in Rural Areas of Hubei Province, China. Health Policy Plan. 2010 May;25(3):219-29.
1500
13500
11500
9500
7500
5500
3500
GD
P pe
r ca
pita
(US$
)
Additional medcines selected at provincal level
50 100 150 200 250 300 350 400
Enhancing collaboration to maximize efficiency
The selection of NEML should fully utilize the results of evidence-
based selection completed by the WHO and its partners. Using
the evidence-based selection already completed by the WHO
would decrease the costs of making the NEML because it would
not have to do its own evidence evaluation. Within China, a
cooperative network could be assembled to fully utilize existing
resources and established facilities. Instead of the national and
provincial governments drawing up their lists independently,
they can do so cooperatively and merge some procedures which
could reduce costs of making the lists for both parties. The
MOH should provide technical support to provinces, especially
to undeveloped provinces which might not be able to carry out
evidence-based selection. Information on medicines selection
should be shared among the NEML selection and provincial
selection.
China covers a vast and diverse territory. Within the country,
different provinces have different disease profiles and social
development levels which lead to difference in selecting
provincial medicines lists. We summarize this in Graph 1. It is
also important to make sure that appropriate local medicines are
included because the provincial lists are used in health facilities.
Although the provinces can make their own lists, it is important
to examine why the number of medicines on the provincial list
varies. One consideration that needs to be made is that less
developed provinces may have higher need for EMs.
ConclusionThe latest NEML for health facilities in grass root level is
significantly improved over the past lists. The establishment
of China’s latest NEML has made great progress in setting
appropriate targets, selection principles and criteria. The
selection is more transparent and evidence-based than in the
previous years. With the updated selection process, promoting
NEML should be within national capacity and relevant to meet
28 Southern Med Review Vol 4 Issue 1 April 2011
The selection of essential medicines in China
17. Lu Y. A Survey of Medicine Prices, Availability and Affordability in Shanghai, China using the WHO/HAI Methodology: WHO/HAI2006. Available at: http://www.haiweb.org/medicineprices/surveys/200609CNS/survey_report.pdf
18. Qiang S. A Survey of Medicine Prices, Availability, Affordability and Price Components in Shandong Province, China: HAI2005. Available at http://www.haiweb.org/medicineprices/surveys/200411CN/survey_report.pdf
19. WHO. MDG Target 8.E: In Cooperation with Pharmaceutical Companies, Provide Access to Affordable Essential Drugs in Developing Countries. 2010 [cited 2010 11/10]; Available from: http://www.who.int/gho/mdg/medicines/situation_trends_availability/en/index.html.
20. China’s State’s council. CPC and state’s council’s opinions on health sector reform. Beijing;2009.
21. Ministy of Health, et al. National clinical guidelines and formulary for essential medicines list. Beijing: 2009.
22. Minstry of Health, et al. Notice on publishing managing measures(temporary) for national essential medicines list. Beijing: 2009.
23 Zheng H. Press conference of Ministry of Health on establishing nationl essential medicines system: how national essential medicines list is selected. Beijing: 2009. Available at: http://www.china.com.cn/zhibo/2009-08/20/content_18365751.htm
24. Wang L, Zhang C, Yuan Q, Zhang LL, Li YP. A comparsion between WHO essential medicines list and China’s national essential medicines list. China’s Journal of evidence-based medicine. 2009, 9(11): 1173 1184. Available at: http://www.healthpolicy.cn/rdfx/jbywzd/gjjy2/who/yjwx/201002/P020100311037204598531.pdf
25. World Health Organization. The selection and use of essential medicines : report of the WHO Expert Committee, 2003 (including the 13th Model list of essential medicines. Geneva: World Health Organization; 2004.
26. Li Z. Experts urge to add essential medicines for children. Nanfang Daily. Guagnzhou; 7/15/2010.
27. Minstry of Health, et al. Opinions on establishing essential medicines system. Beijing: 2009. Available at: http://www.moh.gov.cn/publicfiles/business/htmlfiles/mohywzc/s3581/200908/42498.htm
28. World Health Orgnization. Revised procedure for updating WHO’s Model List of Essential Drugs. EB109/8;2001.
29. Zheng H. The participation of thousands experts ensure appropriate selection for essential medicines. Interview on director of national pharamceutical policy and essential medicines, Ministry of Health. Beijing: 2009. Available at: http://news.xinhuanet.com/video/2009-08/21/content_11923014.htm
30. WHO. The expert advisory panel and committees. Geneva: World Health orgnization, 2006.
31. Kishore SP, Herbstman, BJ. Adding a medicine to the WHO model list of essential medicines. Clin Pharmacol Ther. 2009 Feb85(23):237-9.
32. Azizkhon Jafarov. Selection of Essential Medicines in Central Asian Republics. Comparsion and discrepancies. 2002 May. Available at http://dcc2.bumc.bu.edu/richard l/RPM+_project/aziz.htm
33. Jean Claude Mugiraneza. Is the World Health Organization Model List of Essential Drugs Relevant to Member States? National Essential Drugs Lists of Selected African Countries in Comparative Perspective. Buffalo, NY: 2009. Available at: http://apps.who.int/medicinedocs/en/m/abstract/Js16786e/
34. Laing R, Waning B, Gray A, Ford N, t Hoen E. 25 years of the WHO essential medicines lists: progress and challenges. Lancet. 2003 May 17;361(9370):1723-9.

29 Southern Med Review Vol 4 Issue 1 April 2011
Research Article
Afghanistan pharmaceutical sector development: problems and prospectsJonathan Harper1, Gunnar Strote2
1 Independent International Pharmaceutical Policy & Regulation Consultant, Budapest Hungary2 GFA Consulting Group, Hamburg Germany
Address for Correspondence: Jonathan Harper, Dunasétány 7, Budakalász 2011 Hungary. E-mail: [email protected]
Citation: Harper J, Strote J. Afghanistan pharmaceutical sector development: problems and prospects. Southern Med Review (2011) 4;1:29-39doi:10.5655/smr.v4i1.75
AbstractObjective: To provide an up to date comprehensive overview of the Afghanistan pharmaceutical sector situation and its future
development needs and priorities.
Methods: The methods employed for researching and writing this paper were based on (i) structured interviews and workshop with
Afghanistan pharmaceutical sector stakeholders, (ii) site visits, (iii) sector data review of relevant reports and documents, and (iv) use of
sector assessment tool methodology. A full review of sector policy, regulation and management was conducted covering the complete
pharmaceutical supply chain.
Results: The International Donor Community (IDC) in recent years has provided major assistance for the development of the
Afghanistan health sector with some tangible successes. However, for several reasons the Afghanistan pharmaceutical sub sector
suffers from major deficiencies in terms of implementation of policy, regulation and management. There are significant governance,
structural and capacity weaknesses at both the central and provincial level. The consequence of this has been a pharmaceutical market
and supply system contaminated with substandard, falsified, counterfeit and diverted medicines. The accessibility, affordability and
availability of medicines are highly variable across the country.
Conclusions: Reports on the Afghanistan pharmaceutical sector have hitherto been scarce in the international literature and the
quality and availability of sector data is generally low. The sector for several reasons is one of the least developed in the world, operates
in a chaotic faction and suffers from many weaknesses that cover the entire spectrum of sector activities. The market presence of
substandard and counterfeit medicines is likely to be significant and should be considered a public health menace demanding urgent
attention. A number of sector development interventions are required to address both institutional and market weaknesses.
Keywords: Medicines policy, medicines regulation, medicines pricing, counterfeit medicines, pharmaceutical situation; Afghanistan.
Health Organization (WHO) in 2002, and highlighted severe
infrastructural damage, lack and low quality of essential
medicines, widespread irrational medicines usage and reliance
on medicines donations by the international community9.
The WHO classifies Afghanistan as belonging to a group of
countries (including Iraq, Palestine, Sudan, and Somalia) that
have ongoing emergency situations and that require emergency
supply of medicines with as much quality control as possible.
These countries require major assistance for pharmaceutical
sector strengthening and provision of adequate pharmaceutical
public health.
The Afghanistan pharmaceutical sector is currently, and for
the foreseeable future, managed and publicly financed via
a dual administrative system: (i) the General Directorate for
IntroductionGeneral background
The Islamic Republic of Afghanistan is a landlocked central
Asian country consisting of 34 provinces and with a population
of approximately 28 million. It is classified by the UN as a Least
Developed Country (LDC), is in a state of ongoing conflict and
can be described as both a fragile1 and failed state2. The poor
health, socioeconomic and governance status of Afghanistan
is summarised by a number of indicators presented in Table 1.
Pharmaceutical sector background
The first Afghanistan pharmaceutical sector assessment after
the fall of the Taliban regime was conducted by the World

30 Southern Med Review Vol 4 Issue 1 April 2011
Afghanistan pharmaceutical sector development: problems and prospects
Table 1. Afghanistan Governance, Socioeconomic and Health Indicators
Indicator Value Year
Failed State Index (rank out of 177)2 6 2010
Corruption perceptions index (rank out of 178)3 176 = 2010
Human Development Index rank4 (rank out of 169) 155 2010
Gross national income (PPP $US per capita)5 1,100 2008
% population living on < 1 $US / day (national poverty line)6 42 2009
Crude birth rate (per 1,000)5 47 2008
Crude death rate (per 1,000)5 20 2008
Life expectancy at birth (total years)7 42 2008
Under-5 mortality rate (per 1,000 live births)7 257 2008
Maternal mortality rate (per 1,000 live births) 7 14 2008
Adult mortality rate (per 1,000)7 479 2008
Health system performance rank8 168 2004
Total health expenditure (as % of GDP)7 7.3 2008
Public health expenditure per capita ($US)7 10 2008
Total health expenditure per capita ($US) 7 48 2008
Health expenditure, public (% of total public expenditure)5 3.7 2008
Health expenditure, public (% of total health expenditure)7 21.2 2008
Total pharmaceutical expenditure (as % of total health expenditure)8 15 2004
Note: PPP = Purchasing Power Parity
Pharmaceutical Affairs (GDPA), a directorate of the Ministry
of Public Health (MoPH), which also oversees sector provincial
management via a system of Provincial Pharmacy Officers (PPOs)
located in Provincial Public Health Departments (PPHDs); and
(ii) the International Donor Community (IDC), principally the
World Bank, US Agency for International Development (USAID)
and European Commission (EC), which finances and oversees
the provision of medicines supplied via the Basic Package of
Health Services (BPHS) by International Donor Community (IDC)
contracted Non-Governmental Organisations (NGOs).
The corner stone of Afghanistan health and pharmaceutical
sector development since 2003 has been the implementation
of a BPHS10 which includes a defined set of cost-effective
interventions aimed at addressing the principal health problems
of the population, with an emphasis on the most vulnerable
groups, women and children, but with provisions made for
the eventual incorporation of interventions targeting other
vulnerable groups. More recently in 2005, the Essential Package
of Hospital Services (EPHS) has been created in an attempt to
develop a functional referral system for more severe cases of
disease11.
Since 2002 there has been a significant increase in the quantity
of both donated and privately imported medicines entering
Afghanistan following the involvement of the international
community in this country’s health sector. The profile of the
Afghanistan pharmaceutical market can only be described in
general terms as there is a lack of accurate collected data12;
and where such data has been collected it is largely done on
an ad hoc and non-repeated basis. For example, only one
comprehensive baseline pharmaceutical sector indicator
study, designed in accordance with WHO recommended
Afghanistan Stakeholders International Donor Community (IDC) Stakeholders
1 Deputy Minister, Ministry of Public Health (MoPH) 1 Task Manager Health and Disability Sector, Delegation of the European Commission (EC)
2 Director, General Directorate for Pharmaceutical Affairs (GDPA) 2 Project Manager, EC Afghanistan Provincial Public Health Project
3 Senior Officer, Essential Drug Department GDPA 3 Team Leader, EC Support for Institutional Development of the Afghanistan MoPH Project
4 Director, National Medicines Quality Control Laboratory Kabul 4 Health, Population and Nutrition Officer, US Agency for International Development (USAID)
5 Director, MoPH Central Medical Stores Kabul 5Project Manager, USAID Techserve / Strengthening Pharmaceutical Systems Afghanistan program
6 Dean, Kabul University Pharmacy Faculty 6 Afghanistan Public Health Specialist, World Bank
7 MoPH Technical Advisory Board for Pharmaceutical Affairs (TAB) 7 HIV/AIDS Adviser, World Bank Afghanistan HIV/AIDS Control Program
8 General Director, Avicenna Pharmaceutical Industry Kabul 8 Project Manager, Johns Hopkins University Afghanistan MoPH Support Project
9 Local Pharmacies (N = 10) 9 Health Cooperation Planning Officer, Japan International Cooperation Agency (JICA)
10 Local Health Facilities (N = 3) 10 Medical Officer, WHO Representative Office Kabul
11 Afghan BPHS NGOs (N = 3) 11Team Leader, Afghanistan Blood Transfusion and Diagnostic Facility Project, French Development Agency
12 International BPHS NGOs (N = 2)
Table 2. Afghanistan Pharmaceutical Sector Key Stakeholders Interviewed

31 Southern Med Review Vol 4 Issue 1 April 2011
Afghanistan pharmaceutical sector development: problems and prospects
Title Theme
1 Baghdadi G, Chomilier C, Graaff P. Pharmaceutical Situation in Afghanistan. WHO Preliminary Assessment (14-23 January 2002) Sector Assessment
2Mansoor, B, Najib, Mohd. Baseline Drug Indicator Study, A comparative Cross-Sectional Study in SCA Health Facilities in Afghanistan, Part II Results and Next Steps. Swedish Committee for Afghanistan (2003)
Sector Assessment
3 Afghanistan Private Pharmacies Survey. Management Sciences for Health (August 2004) Sector Assessment
4 Understanding markets in Afghanistan: A study of the market for pharmaceuticals. Afghanistan Research and Evaluation Unit (December 2005) Sector Assessment
5 2006 Afghanistan Health Survey. Ministry of Public Health, Islamic Republic of Afghanistan (2006) Sector Assessment
6 2007 Afghanistan National Health Services Performance Assessment. Johns Hopkins University (2007) Sector Assessment
7 Afghanistan National Medicines Policy (2003) Policy
8 Drug donation guidelines. HealthCare and Promotion Department, Ministry of Public Health, Islamic Republic of Afghanistan (2003) Policy
9 International Donor Community Afghanistan Health Sector Strategic Planning Retreat Report (October 2007) Policy
10Afghanistan Donor health sector review: ‘Building on early gains: the role and structure of government in further strengthening Afghanistan’s health sector’ (October 2007)
Policy
11 Draft Terms of Reference for General Directorate of Pharmaceutical Affairs (2007) Policy
12 Afghanistan National Essential Drug List (December 2007) Policy
13Provincial Pharmacy Officer Job Description. General Directorate for Pharmaceutical Affairs Ministry of Public Health, Islamic Republic of Afghanistan (2007)
Policy
14Afghanistan Health and Nutrition Sector Strategy (HNSS) 2008-2013. Ministry of Public Health; Ministry of Agriculture, Irrigation & Livestock Ministry of Public Health, Islamic Republic of Afghanistan (2008)
Policy
15 Workshop Report for Pooled Procurement of Essential Drugs. Management Sciences for Health (July 2003) Medicines Supply
16 Inventory of drugs available in Kabul. Ministry of Public Health, Islamic Republic of Afghanistan (2004) Medicines Supply
17Procurement Procedure of Goods, Services, Medicine-Medical Items for the Procurement Department of Ministry of Public Health. Oxford Policy Management (February 2005)
Medicines Supply
18Concept Paper for the General Directorate of Planning & Procurement, Ministry of Public Health; Procurement Reform in the Ministry of Public Health, Afghanistan, JICA (February 2006)
Medicines Supply
19Assessment of the Pharmaceutical Logistics Management Capacity of REACH Grantee NGOs - Rural Expansion of Afghanistan’s Community-based Healthcare Program (MSH / REACH, USAID), (July 2006)
Medicines Supply
20MIAR (Monthly Integrated Activity Report) – Facilities with at least 1 stock out by province. Ministry of Public Health, Islamic Republic of Afghanistan (March 2006-March 2007)
Medicines Supply
21 Strengthening Logistics System in Urban Kabul Project. JICA (August 2007) Medicines Supply
22 Terms of Reference for EC NGO BPHS Contractors concerning drug provision (2007) Medicines Supply
23Coordinated Procurement and Distribution System (CPDS) Governance Framework. General Directorate of Pharmaceutical Affairs Ministry of Public Health, Islamic Republic of Afghanistan (March 2010)
Medicines Supply
24 Drug Quality Assessment Study Afghanistan 2007. Ministry of Public Health Islamic Republic of Afghanistan (2007) Regulation
25National Licensed Drugs List. General Directorate of Pharmaceutical Affairs, Ministry of Public Health, Islamic Republic of Afghanistan; Essential Drug Department, Avicenna Pharmaceutical Institute (December 2007)
Regulation
26Procedure for application for inclusion of medicines on the essential drugs list of the Ministry of Public Health of Afghanistan. General Directorate of Pharmaceutical Affairs, Ministry of Public Health, Islamic Republic of Afghanistan; Essential Drug Department, Avicenna Pharmaceutical Institute (2007)
Regulation
27Procedure for application for inclusion of medicines on the essential drugs list of the Ministry of Public Health of Afghanistan. . General Directorate of Pharmaceutical Affairs, Ministry of Public Health, Islamic Republic of Afghanistan; Essential Drug Department, Avicenna Pharmaceutical Institute (2007)
Regulation
28Procedure for application for inclusion of medicines on the licensed drugs list of the Ministry of Public Health of Afghanistan. . General Directorate of Pharmaceutical Affairs, Ministry of Public Health, Islamic Republic of Afghanistan; Essential Drug Department, Avicenna Pharmaceutical Institute (2007)
Regulation
29 Afghanistan National Medicines Law (2006) Legislation
30 Regulation on ‘import and production of medicines and medical devices’ (2005) Legislation
31 Regulation on ‘pharmacies’ (2006) Legislation
Table 3. Principal Documents and Reports Reviewed
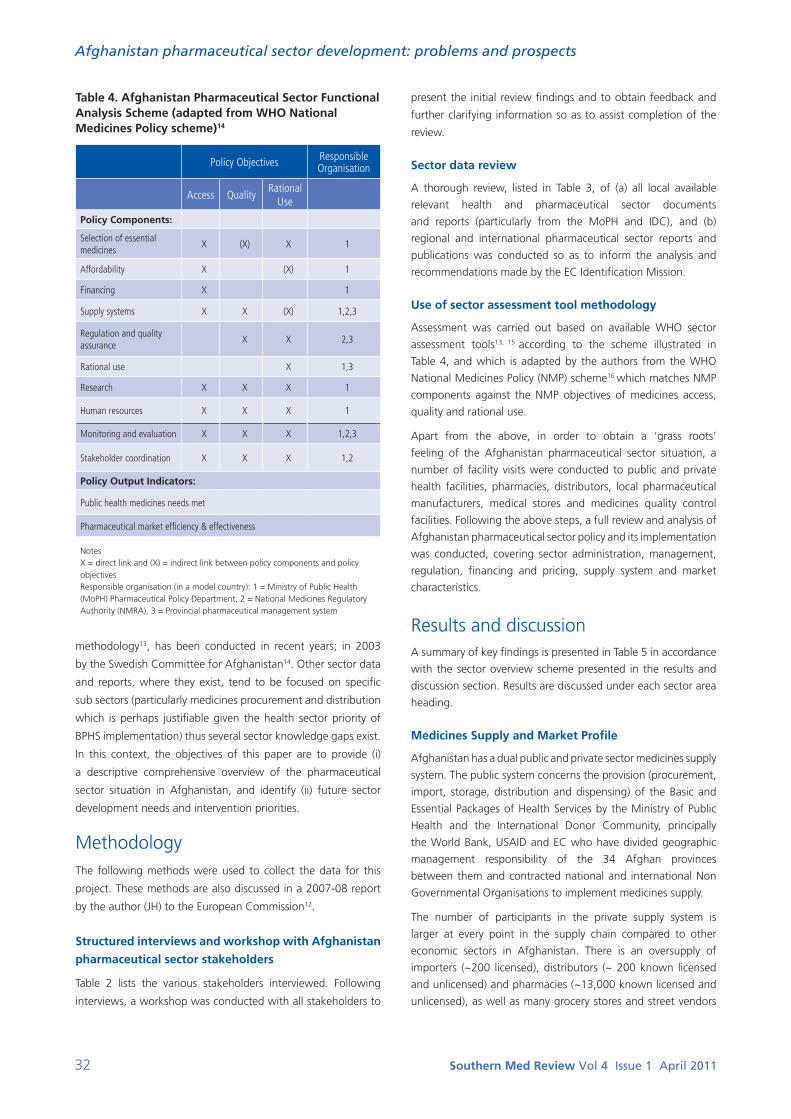
32 Southern Med Review Vol 4 Issue 1 April 2011
Afghanistan pharmaceutical sector development: problems and prospects
Table 4. Afghanistan Pharmaceutical Sector Functional Analysis Scheme (adapted from WHO National Medicines Policy scheme)14
Policy Objectives Responsible Organisation
Access QualityRational
Use
Policy Components:
Selection of essential medicines
X (X) X 1
Affordability X (X) 1
Financing X 1
Supply systems X X (X) 1,2,3
Regulation and quality assurance
X X 2,3
Rational use X 1,3
Research X X X 1
Human resources X X X 1
Monitoring and evaluation X X X 1,2,3
Stakeholder coordination X X X 1,2
Policy Output Indicators:
Public health medicines needs met
Pharmaceutical market efficiency & effectiveness
Notes X = direct link and (X) = indirect link between policy components and policy objectivesResponsible organisation (in a model country): 1 = Ministry of Public Health (MoPH) Pharmaceutical Policy Department, 2 = National Medicines Regulatory Authority (NMRA), 3 = Provincial pharmaceutical management system
methodology13, has been conducted in recent years; in 2003
by the Swedish Committee for Afghanistan14. Other sector data
and reports, where they exist, tend to be focused on specific
sub sectors (particularly medicines procurement and distribution
which is perhaps justifiable given the health sector priority of
BPHS implementation) thus several sector knowledge gaps exist.
In this context, the objectives of this paper are to provide (i)
a descriptive comprehensive overview of the pharmaceutical
sector situation in Afghanistan, and identify (ii) future sector
development needs and intervention priorities.
MethodologyThe following methods were used to collect the data for this
project. These methods are also discussed in a 2007-08 report
by the author (JH) to the European Commission12.
Structured interviews and workshop with Afghanistan
pharmaceutical sector stakeholders
Table 2 lists the various stakeholders interviewed. Following
interviews, a workshop was conducted with all stakeholders to
present the initial review findings and to obtain feedback and
further clarifying information so as to assist completion of the
review.
Sector data review
A thorough review, listed in Table 3, of (a) all local available
relevant health and pharmaceutical sector documents
and reports (particularly from the MoPH and IDC), and (b)
regional and international pharmaceutical sector reports and
publications was conducted so as to inform the analysis and
recommendations made by the EC Identification Mission.
Use of sector assessment tool methodology
Assessment was carried out based on available WHO sector
assessment tools13, 15 according to the scheme illustrated in
Table 4, and which is adapted by the authors from the WHO
National Medicines Policy (NMP) scheme16 which matches NMP
components against the NMP objectives of medicines access,
quality and rational use.
Apart from the above, in order to obtain a ‘grass roots’
feeling of the Afghanistan pharmaceutical sector situation, a
number of facility visits were conducted to public and private
health facilities, pharmacies, distributors, local pharmaceutical
manufacturers, medical stores and medicines quality control
facilities. Following the above steps, a full review and analysis of
Afghanistan pharmaceutical sector policy and its implementation
was conducted, covering sector administration, management,
regulation, financing and pricing, supply system and market
characteristics.
Results and discussionA summary of key findings is presented in Table 5 in accordance
with the sector overview scheme presented in the results and
discussion section. Results are discussed under each sector area
heading.
Medicines Supply and Market Profile
Afghanistan has a dual public and private sector medicines supply
system. The public system concerns the provision (procurement,
import, storage, distribution and dispensing) of the Basic and
Essential Packages of Health Services by the Ministry of Public
Health and the International Donor Community, principally
the World Bank, USAID and EC who have divided geographic
management responsibility of the 34 Afghan provinces
between them and contracted national and international Non
Governmental Organisations to implement medicines supply.
The number of participants in the private supply system is
larger at every point in the supply chain compared to other
economic sectors in Afghanistan. There is an oversupply of
importers (~200 licensed), distributors (~ 200 known licensed
and unlicensed) and pharmacies (~13,000 known licensed and
unlicensed), as well as many grocery stores and street vendors
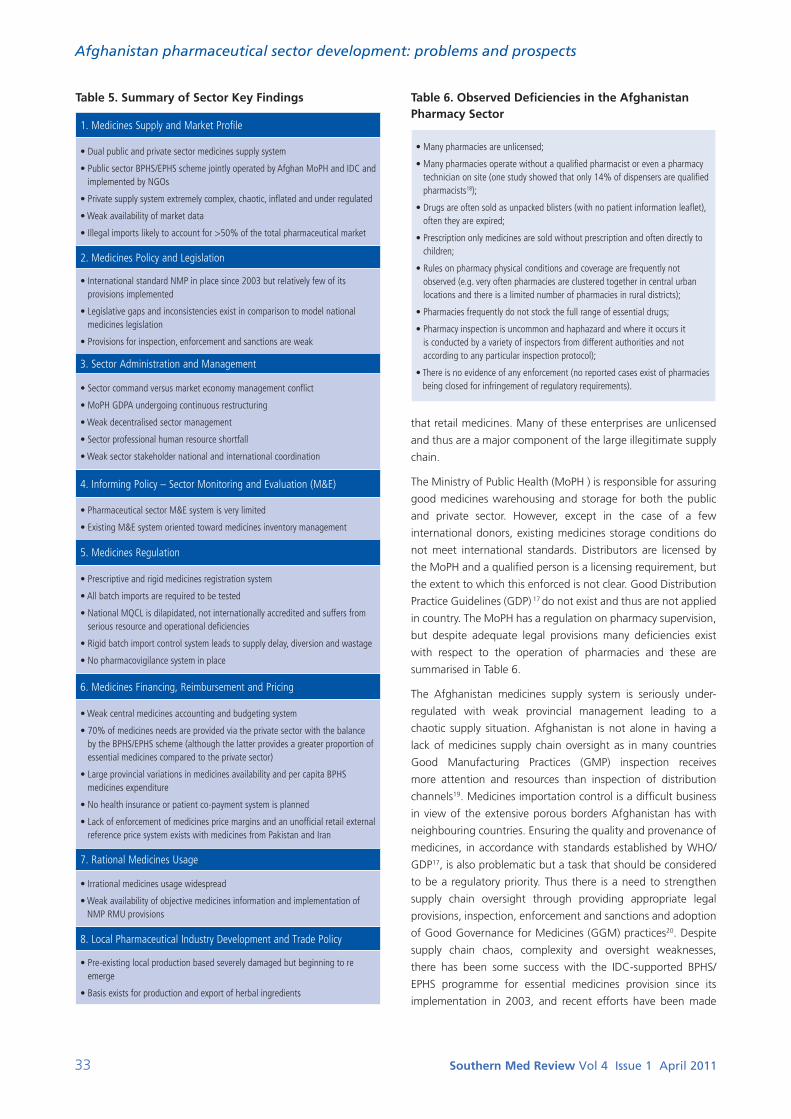
33 Southern Med Review Vol 4 Issue 1 April 2011
Afghanistan pharmaceutical sector development: problems and prospects
Table 5. Summary of Sector Key Findings
1. Medicines Supply and Market Profile
• Dual public and private sector medicines supply system
• Public sector BPHS/EPHS scheme jointly operated by Afghan MoPH and IDC and implemented by NGOs
• Private supply system extremely complex, chaotic, inflated and under regulated
• Weak availability of market data
• Illegal imports likely to account for >50% of the total pharmaceutical market
2. Medicines Policy and Legislation
• International standard NMP in place since 2003 but relatively few of its provisions implemented
• Legislative gaps and inconsistencies exist in comparison to model national medicines legislation
• Provisions for inspection, enforcement and sanctions are weak
3. Sector Administration and Management
• Sector command versus market economy management conflict
• MoPH GDPA undergoing continuous restructuring
• Weak decentralised sector management
• Sector professional human resource shortfall
• Weak sector stakeholder national and international coordination
4. Informing Policy – Sector Monitoring and Evaluation (M&E)
• Pharmaceutical sector M&E system is very limited
• Existing M&E system oriented toward medicines inventory management
5. Medicines Regulation
• Prescriptive and rigid medicines registration system
• All batch imports are required to be tested
• National MQCL is dilapidated, not internationally accredited and suffers from serious resource and operational deficiencies
• Rigid batch import control system leads to supply delay, diversion and wastage
• No pharmacovigilance system in place
6. Medicines Financing, Reimbursement and Pricing
• Weak central medicines accounting and budgeting system
• 70% of medicines needs are provided via the private sector with the balance by the BPHS/EPHS scheme (although the latter provides a greater proportion of essential medicines compared to the private sector)
• Large provincial variations in medicines availability and per capita BPHS medicines expenditure
• No health insurance or patient co-payment system is planned
• Lack of enforcement of medicines price margins and an unofficial retail external reference price system exists with medicines from Pakistan and Iran
7. Rational Medicines Usage
• Irrational medicines usage widespread
• Weak availability of objective medicines information and implementation of NMP RMU provisions
8. Local Pharmaceutical Industry Development and Trade Policy
• Pre-existing local production based severely damaged but beginning to re emerge
• Basis exists for production and export of herbal ingredients
Table 6. Observed Deficiencies in the Afghanistan Pharmacy Sector
• Many pharmacies are unlicensed;
• Many pharmacies operate without a qualified pharmacist or even a pharmacy technician on site (one study showed that only 14% of dispensers are qualified pharmacists18);
• Drugs are often sold as unpacked blisters (with no patient information leaflet), often they are expired;
• Prescription only medicines are sold without prescription and often directly to children;
• Rules on pharmacy physical conditions and coverage are frequently not observed (e.g. very often pharmacies are clustered together in central urban locations and there is a limited number of pharmacies in rural districts);
• Pharmacies frequently do not stock the full range of essential drugs;
• Pharmacy inspection is uncommon and haphazard and where it occurs it is conducted by a variety of inspectors from different authorities and not according to any particular inspection protocol);
• There is no evidence of any enforcement (no reported cases exist of pharmacies being closed for infringement of regulatory requirements).
that retail medicines. Many of these enterprises are unlicensed
and thus are a major component of the large illegitimate supply
chain.
The Ministry of Public Health (MoPH ) is responsible for assuring
good medicines warehousing and storage for both the public
and private sector. However, except in the case of a few
international donors, existing medicines storage conditions do
not meet international standards. Distributors are licensed by
the MoPH and a qualified person is a licensing requirement, but
the extent to which this enforced is not clear. Good Distribution
Practice Guidelines (GDP) 17 do not exist and thus are not applied
in country. The MoPH has a regulation on pharmacy supervision,
but despite adequate legal provisions many deficiencies exist
with respect to the operation of pharmacies and these are
summarised in Table 6.
The Afghanistan medicines supply system is seriously under-
regulated with weak provincial management leading to a
chaotic supply situation. Afghanistan is not alone in having a
lack of medicines supply chain oversight as in many countries
Good Manufacturing Practices (GMP) inspection receives
more attention and resources than inspection of distribution
channels19. Medicines importation control is a difficult business
in view of the extensive porous borders Afghanistan has with
neighbouring countries. Ensuring the quality and provenance of
medicines, in accordance with standards established by WHO/
GDP17, is also problematic but a task that should be considered
to be a regulatory priority. Thus there is a need to strengthen
supply chain oversight through providing appropriate legal
provisions, inspection, enforcement and sanctions and adoption
of Good Governance for Medicines (GGM) practices20. Despite
supply chain chaos, complexity and oversight weaknesses,
there has been some success with the IDC-supported BPHS/
EPHS programme for essential medicines provision since its
implementation in 2003, and recent efforts have been made

34 Southern Med Review Vol 4 Issue 1 April 2011
Afghanistan pharmaceutical sector development: problems and prospects
to establish a BPHS/EPHS coordination mechanism via the
Governance Framework on Coordinated Procurement and
Distribution System (CPDS)21.
In the absence of accurate data, it estimated that (i) the private
sector accounts for 70% of the total pharmaceutical market (of
which 95% consists of imported medicines from many sources in
the region), and (ii) 30% of the market consists of international
drug donations which are provided largely through the BPHS/
EPHS essential medicines scheme, the balance provided through
international humanitarian pharmaceutical assistance12, 22. Illegal
imports, which can also contaminate the legitimate supply
chain, probably account for greater than 50% of the total
pharmaceutical market12, 22; a major contributory factor that
Afghanistan has lengthy porous borders, particularly the borders
with Pakistan and Iran. The MoPH estimates that the number of
unregistered far exceeds registered medicines on the market12.
Although identification of substandard and counterfeit
medicines in the Afghanistan market is a straight forward task
and cases can readily be identified12, for a number of reasons
the estimation of the prevalence of substandard, counterfeit
(falsified), adulterated and diverted medicines in Afghanistan is
extremely difficult. Difficulties in estimating prevalence are due
to weak Post Market Surveillance (PMS), a chaotic and complex
supply chain and an absence of clear and internationally
harmonised definitions of counterfeit and substandard
medicines.
One recent study23 was conducted in Afghanistan to examine
medicines quality and which concluded that medicines provided
publicly by the IDC through the BPHS were generally of an
acceptable standard; however the sample size from the private
sector was too small to draw any conclusions concerning
private sector substandard medicine prevalence. Given the
estimated high proportion of illegal imports a high prevalence
of substandard (and counterfeit) medicines cannot be ruled
out and PMS efforts need to be enhanced. The Afghan conflict
situation is likely to provide fertile ground for pharmaceutical
crime activity, particularly given the close association between
organised crime and medicines counterfeiting24. Counterfeiting
is also perhaps a disincentive for research-based and branded
medicines manufacturers to register their products in
Afghanistan.
In 2010, the WHO conducted a questionnaire-based survey of
several EMROi and SADCii countries25, including Afghanistan,
with the objective of reviewing the counterfeit medicine
situation so as to provide a more informed basis for developing
and implementing counterfeit medicine policy and action.
Conclusions applicable to most countries surveyed, including
Afghanistan, were a need for (i) specific legislation that
empowers National Medicines Regulatory Authorities (NMRAs)
and criminalises medicines counterfeiting, (ii) strengthened
cooperation and information-sharing among the various
key players at national, regional and global levels, and (iii)
strengthened weak market control systems. Thus, in order
to tackle the problem in Afghanistan a number of actions
are required, several of which will require IDC assistance for
implementation.
Medicines Policy and Legislation
Afghanistan is in possession of a National Medicines Policy (NMP) dating from 2003 and which has been designed in accordance with the WHO national medicines policy model scheme and guidelines16. Aside from the creation of an Essential Medicines List (EML), last updated in 2007, and the supply of essential medicines via the BPHS/EPHS, other NMP provisions (e.g. rational medicines usage policies) are underrepresented in the MoPH pharmaceutical sector management programme, the latter effectively being the NMP implementation plan26. While medicines supply management is an important policy area and which hitherto has been seen as a priority area in view of the emphasis on BPHS implementation, other areas of NMP equally deserve and require attention for implementation.
The sector legislative and regulatory framework is provided by a framework Medicines Law (2006) and Regulations covering local manufacturing, import, procurement, distribution and retail. The Afghanistan Medicines Law omits several regulatory areas that would normally be included in a model national medicines law and includes a number of areas that normally would not be included12. For example, the law makes no provision for medicines intellectual property issues (IPR) issues, i.e. patent and brand name protection, data exclusivity and issues relating to Trade Related Intellectual Property Rights (TRIPS) flexibilities. Provisions for implementation and enforcement of the law and sanctions for violations are weak. There is scope to align the existing medicines legislation in accordance with regional and international standards and practices and to introduce stronger provisions concerning implementation, enforcement and sanctions.
Sector Administration and Management
Health sector stewardship is defined by the WHO as being one
of the four essential functions of the health system in addition
to service provision, resource generation and financing27, 28. The
Ministry of Public Health General Directorate for Pharmaceutical
Affairs is responsible for pharmaceutical sector stewardship
(sector policy and regulation) but also, as a legacy of the
Soviet occupation period, continues to perform a command
style of sector management and consequently conducts a
range of commercial activities outside of its stewardship role
and not related to medicines policy and regulation such as
manufacturing, operating a pharmacy retail chain, wholesaling,
warehousing and importing. This situation is in conflict with
market economy based systems being introduced by the IDC
and has a detrimental impact on activities that are within its
terms of reference.
The MoPH, and particularly its GDPA, is continuing to undergo
a long period of restructuring with regular organisational
changes often driven by political reasons and consequently
remains unsettled and not modelled in conformance with the
i East Mediterranean Regional Office of the WHOii SADC – Southern African Development Community. Inter-governmental organisation of 15 southern African states

35 Southern Med Review Vol 4 Issue 1 April 2011
Afghanistan pharmaceutical sector development: problems and prospects
Table 7. Afghanistan Pharmaceutical Sector Performance Indicators
a. MoPH HMIS (Health Management Information System) - MIAR (Monthly Integrated Activity Report) – healthcare facilities with at least 1 drug stock out (assessed by province);
b. Balanced Score Card (BSC) performance assessment of BPHS delivery (indicator relevant to the pharmaceutical sector is ‘Indicator 7: Drug availability index’*;
c. USAID assessment of the pharmaceutical logistics management capacity of NGO grantees (utilising an Inventory Management Assessment Tool).
* measures the continuous availability of a set of essential drugs in health facilities. This indicator is included in the BSC system adopted by the Afghanistan MoPH as a tool to measure and manage BPHS performance delivery30. The median score for this indicator in 2004 was 69% and which had risen to 85% by 2006, thus indicating an increase in public sector essential drug availability.
tasks necessary to conduct its sector stewardship function. In
comparison to other MoPH directorates, the GDPA has lacked
IDC support which has contributed to both its unsettled
organisational situation and lack of development. Afghanistan
is a highly decentralised country and effective management of
its pharmaceutical sector is reliant on the Provincial Pharmacy
Officer system which is principally tasked with ensuring public
sector medicines supply via the BPHS/EPHS programme in the
provinces. An examination of the PPO task description and
PPO-GDPA reporting system was conducted and revealed
several inadequacies, particularly an absence of any provincial
regulatory function as well as coordination activity with the IDC
system that provides the BPHS/EPHS.
In 2004, the WHO estimated that a third of countries have
no medicines regulation or a regulatory capacity that hardly
functions8; it is certain that Afghanistan belongs in this category,
particularly given the findings from the EC sector survey12 which
highlight major regulatory gaps and weaknesses as evidenced
by the chaotic nature of its pharmaceutical market. Concerning
sector human resources, Afghanistan has one pharmacy faculty
training 120 pharmacists annually and which recommenced
operations in 2001 following a long hiatus due to many years of
conflict. Afghanistan health sector human resource development
strategy is skewed towards recruitment of doctors and thus
there is a major shortfall in qualified pharmacists and pharmacy
technicians against the background of a rapidly expanding
private pharmaceutical sector12 which hinders effective sector
functioning.
A necessary measure for effective and efficient sector
management is sufficient coordination with sector stakeholders
at both the national and international (particularly the Asia
region) levels. An examination of national sector coordination
between the various stakeholders revealed that this was very
weak (even between the different IDC parties), and also at the
international level, although Afghanistan is a member of the
regional Economic Cooperation Organisation (ECO)iii (which
offers a framework for pharmaceutical regulatory cooperation)
and the South Asian Association for Regional Cooperation
(SAARC)iv. The Afghanistan pharmaceutical sector largely
operates in an international void against the background of a
global pharmaceutical market, a situation which is not conducive
for its development.
Afghanistan is judged to be the second most corrupt country in
the world3 and evidence suggests that the Afghanistan health
and pharmaceutical sector is particularly adversely affected by
corruption12, 22, 29. Transparency International claims that in some
countries up to two thirds of hospital medicines supplies are
lost to corruption and fraud and it is estimated that 10–25%
of global spending on public medicines procurement is lost to
corruption3. This leads one to conclude that there is a pressing
need to introduce medicines good governance measures in
Afghanistan which can potentially be achieved via adopting the
WHO Good Governance for Medicines (GGM) programme20 in
this country.
The Afghanistan pharmaceutical sector possesses a satisfactory
enabling policy (and to a lesser extent legislative) framework
and thus sector development now needs to focus on a number
of areas which all require long term IDC support:
(i).capacity building (e.g. human resource development);
(ii). institution building. It is necessary to build an international
standard medicines regulatory structure and function as a
priority and which operates in accordance with the principles
of good regulatory practices. Medicines policy and regulation
functions require significant rationalisation and development to
meet international norms and standards. This can be facilitated
by benchmarking pharmaceutical regulatory structure and
activities against those of other countries in the region and
elsewhere. Further GDPA institution building efforts will require
a functional separation of sector administration from service
delivery;
(iii). sector coordination (with corresponding authorities)
strengthening at both the national and international levels; and
(iv). introduction of medicines good governance.
Informing Policy – Sector Monitoring and Evaluation (M&E)
Sector Monitoring and Evaluation (M&E) is a vital stewardship
function (i.e. generation of intelligence) which permits
evidence-based policy making. However, pharmaceutical Sector
M&E (and supporting sector management information systems),
within the framework of overall health sector M&E and national
health accounts is extremely limited in Afghanistan. Existing
sector performance indicators tend to be directed towards
medicines inventory management and are summarised in Table
7. In addition to the national level drug inventory Monitoring &
Evaluation system, one international donor (USAID) employs a
detailed Basic Package of Health Services inventory management
assessment tool, while other donors employ no assessment tool
at all.
iii Afghanistan, Azerbaijan, Iran , Kazakhstan, Kyrgyzstan , Pakistan, Turkey, Turkmenistan, Tajikistan and Uzbekistaniv Afghanistan, Bangladesh, Bhutan, India, the Maldives, Nepal, Pakistan and Sri Lanka

36 Southern Med Review Vol 4 Issue 1 April 2011
Afghanistan pharmaceutical sector development: problems and prospects
Other sector data, where it is available, tends to be collected
on an ad hoc basis by the IDC and contracted NGOs, however
many sector areas outside of medicines inventory management
are not monitored or evaluated (e.g. medicines quality, safety,
usage and pricing). The failure of sector data coordination occurs
due to the fact that the sector is currently managed jointly by
the Afghan authorities and several international donors. The
actual assimilation and utilisation of available sector data by the
MoPH GDPA is hard to determine. Thus, as is often the case in
developing countries, local data is sparse and the majority of
policy decisions tend to be based on data which is gathered,
modelled and published by international agencies31.
There is much scope to adopt a unified, standardised and
comprehensive pharmaceutical sector M&E system (which
should be incorporated into the overall health sector M&E
system) to serve the purposes of both the MoPH and the IDC.
The introduction of regular pharmaceutical sector baseline
studies can complement and feed into this system.
Medicines Regulation, Registration and Quality Control
The Afghanistan Licensed Drug List (LDL)32 is determined jointly
by the MoPH and IDC, is based on the WHO Model List of
Essential Medicines (MLEM) and prescribes which medicines
can be registered in Afghanistan as well as included in the
Afghanistan Essential Medicines List (EML). A full medicines
registration dossier, that should include both clinical efficacy and
safety evidence and pharmacoeconomic data33, is required to be
submitted for all LDL applications. Thus there are no provisions
for abbreviated medicines registration in the case of an existing
reference product on the Afghanistan market. Limited provisions
exist concerning intellectual property issues (i.e. data exclusivity,
patent protection, registration of brand and trademark names).
The Ministry of Public Health Medicines Quality Control
Laboratory (MQCL) is responsible for medicines Quality Control
(QC) and carries out testing for registration, batch import QC,
and ostensibly for Post Market Surveillance (PMS) purposes. As
there is no capacity to conduct Good Manufacturing Practice
(GMP) inspections and a lack of recognition of international
manufacturing authorisations and GMP certificates, the MoPH
relies on a system of testing every imported batch (except for
batches imported by some international donors who have
obtained a MoPH testing waiver), although the capacity and
capability of the national Medicines QC laboratory to do such is
far from adequate. The MQCL is not internationally accredited,
is operating in a dilapidated condition, suffers from serious
resource (staff and equipment) and operational deficiencies,
and is inadequate in all respects to be able conduct medicines
testing according to international standards12. The ultimate
organisational position of the MQCL is yet to be determined.
Medicines import and export is regulated according to a batch
import licensing system; however customs control procedures
are reported by several stakeholders as being detrimental,
inefficient and non transparent12. The rigid import license
process and requirement for all batches to be QC tested by
the central MQCL often results in delays of approximately
three months for medicines to be imported into Afghanistan;
often large amounts of import batch stock are damaged or
misappropriated (diversion, ‘system leakage’) while in customs
clearance; no customs risk analysis procedure is applied to
imported medicines and there is no central customs bonded
warehouse22. There is no system of medicines export and transit
licensing. Importers are licensed by the MoPH and licenses can
be obtained by general traders (i.e. not just specialist medicine
distribution companies that employ a qualified person).
The Afghanistan medicines regulation system is underdeveloped,
weakly implemented and not internationally harmonised. There
are a number of weaknesses and gaps and principally there is a
need to harmonise the medicines law and its regulations with
existing international models, adopt internationally harmonised
medicines registration procedures, invest in an adequate
medicines QC infrastructure and implement a pharmacovigilance
system.
Medicines Financing, Reimbursement and Pricing
It is difficult to make an accurate assessment of the public
medicines financing situation in Afghanistan for a number of
reasons: (i) no national health account system exists, (ii) there
is no central compilation of medicines financing statistics or
national medicines budget formula in operation, (iii) public
health financing is derived and applied by a number of
funders, i.e. Ministry of Public Health and International Donor
Community, and (iv) medicines financing data is not routinely
collected and where it exists it is of a limited nature. Thus there
is a need for the IDC to assist and involve the MoPH in assessing
medicines needs and monitoring sector financial flows.
The public Basic and Essential Packages of Health Services
medicines budget is ~ 4 USD per capita per year12. The best
available statistics suggest that 70% of the country’s medicines
needs are provided via the private sector with the remainder
being supplied by the 100% publicly funded essential
medicine BPHS/EPHS scheme (90% funded by IDC with the
Afghanistan Ministry of Finance contributing the balance);
however the proportion of essential medicines provided by
the public BPHS/EPHS scheme which is estimated to have 80%
population coverage (as a % of total essential drugs supplied) is
proportionately higher. It is estimated that an average of 20% of
the BPHS/EPHS budget across all donors is spent on medicines12,
although there is a wide variation in per capita medicines
expenditure between provinces and between donors (as a result
of variations in medicines financing policies between the donors
and which are not centrally coordinated).
Large variations occur in medicines availability and per capita
BPHS medicines expenditure between the provinces for reasons
that are not entirely clear and may be partly related to donor and
MoPH incoordination in terms of estimating medicines needs. In
spite of the public BPHS/EPHS system ‘out of pocket’ payments

37 Southern Med Review Vol 4 Issue 1 April 2011
Afghanistan pharmaceutical sector development: problems and prospects
for medicines constitute a significant part of private household
expenditure34. Anecdotal evidence suggests that patients meet
a substantial part of their medicines needs from the private
sector for a number of reasons; e.g. perception of product
quality source, lack of availability in public health facilities, long
waiting times, ability to obtain medicines without the need for
a prescription. Thus fundamental medicines availability issues in
Afghanistan require major attention.
Afghanistan Medicines legislation makes provision for
controlling medicines prices via defining import, wholesale and
retail margins, for both publicly and privately supplied medicines.
Despite the existence of legislation governing medicines price
margins, observance of regulated margins is not followed
in practice and are hardly inspected or enforced. Very often
pharmacies set retail prices by referring to the retail price of
medicines in either Pakistan or Iran. The BPHS/EPHS medicines list
is based on the MoPH EDL and inclusion of a medicine on the list
requires the submission of pharmacoeconomic data35, however
the appropriateness and capacity of the Afghanistan authorities
to employ pharmacoeconomic analysis in medicines assessment
has to be seriously questioned. Strong arguments exist against
blindly applying developed country pharmacoeconomic
models and techniques in LDCs as they can in the first instance
effectively manage scarce resources by applying effective pricing
policies, differential pricing and by improving transparency and
accountability within the medicines system36.
It is unrealistic in the long term to expect the IDC to continue to
fund Afghanistan’s essential medicines needs so a system needs
to be put in place whereby all regulatory-approved essential
medicines, irrespective of source, come under the provisions of
a national medicines financing and reimbursement system and
with the introduction of international reference prices.
Rational Medicines Usage (RMU)
Irrational medicines prescribing, dispensing and consumption
have been reported as being widespread in Afghanistan and
include overuse of antimicrobials and injections and the
dispensation of half treatment courses9, 14. Medicines are widely
available without prescription and a serious problem exists with
diagnosis and prescription by unqualified persons posing as
doctors in private clinics and working in private pharmacies as
well as by street vendors22. It has been noted that consumers
cannot always afford complete courses of therapy and that
generic medicines are perceived to be of low quality leading
to the prescription of high doses and multiple products in the
same therapeutic category9. The usage of traditional and herbal
medicines in Afghanistan medical practice continues to be a
major part of health care delivery although utilised traditional
remedies may or may not be clinically appropriate22.
The availability of objective medicines information is particularly
weak although a few public education campaigns on medicines
usage are in existence22. The Afghanistan National Medicines
Policy makes provision for implementing several RMU policy
measures, e.g. creation of impartial medicines information
resources (such as a national medicines information centre and
a national medicines formulary) and national clinical protocols,
but aside from the creation of the EML so far none have been
implemented due to capacity and resource constraints.There
is a real need for the implementation of a range of RMU
policy measures including professional curricula development,
medicines utilisation review and household consumption studies,
health facility Drugs and Therapeutics Committees (DTCs),
objective medicines information (for prescribers, dispensers and
consumers), clinical protocols, and Good Pharmacy Practice
guidelines.
Local Pharmaceutical Industry Development and Trade Policy
Only a decade ago Afghanistan was producing the majority of
its medicine needs inside the country and was even developing
an export market. As a result of the many recent conflicts in is
history, Afghanistan’s pharmaceutical industry, which was strong
in the period between the 1970s to the early 1990s, has been
severely damaged. There are currently two credible foreign-
owned manufacturers and a pre-existing major state-owned
manufacturer (the latter existing in a dilapidated condition
but attempting to revitalise its production base in accordance
with international manufacturing standards). In addition there
are a large number of small scale 100 percent Afghan-owned
pharmaceutical manufacturers, the number of which is growing.
Afghanistan also produces many herbal ingredients that are
exported for use in herbal medicines; 28.6 million US$ of
‘medical plants’ were exported in 2010 accounting for 7%
of total exports37. Thus the development of herbal medicine
local production appears rational as the country is a reservoir
of potentially valuable herbal active substances with cultivation
experience.
The MoPH considers the development of local production
and import substitution to be a major pharmaceutical sector
strategic objective, but no state incentive schemes exist for
supporting local essential medicines production. Due to its land-
locked location the costs of importing bulky essential drugs
can be prohibitive and above international reference prices and
its porous borders make it difficult to control imports. Thus
there is real justification for developing a local pharmaceutical
industry that can contribute to supplying the country’s essential
medicines needs and which will require introducing effective
import substitution policy measures.
Conclusions The Afghanistan pharmaceutical sector for several reasons is
one of the least developed in the world, operates in a chaotic
faction and suffers from many weaknesses that cover the
entire spectrum of sector activities. The market presence of
substandard and counterfeit medicines is likely to be significant
and should be considered a public health menace demanding

38 Southern Med Review Vol 4 Issue 1 April 2011
Afghanistan pharmaceutical sector development: problems and prospects
urgent attention. As a result of International Donor Community
assistance, there are signs of improvement in Afghanistan
healthcare delivery (particularly the contribution of the Basic
Package of Health Services / Essential Package of Hospital
Services programme), although the country still remains at the
bottom of the world health league. However, the IDC focus
on providing its health sector development support to the
BPHS/EPHS programme has meant that pharmaceutical sector
development has been relatively neglected.
Afghanistan pharmaceutical sector development needs and
intervention priorities can be described under the separate
headings of institutional and market. Institutional needs and
priorities cover strengthening (i) sector stewardship, good
governance and full National Medicines Policy implementation,
(ii) organisational capacity and resources, (iii) sector Monitoring
& Evaluation, and (iv) national and international sector
coordination. Market needs and priorities cover strengthening
(i) medicines regulation - ensuring medicines quality, safety and
efficacy, (ii) supply chain regulation, (iii) the drug financing,
reimbursement and pricing system, (iv) rational medicines
usage, and (v) local pharmaceutical industry.
The sector is currently being financed and managed jointly by
the Afghanistan government and the IDC; a situation that is
likely to continue for the foreseeable future and which should
coexist with an ongoing IDC-supported Afghan MoPH and
GDPA capacity building programme and sector infrastructural
investment that will address the numerous challenges that the
sector faces.
Acknowledgements and fundingThis work was supported by a GFA Consulting Group Hamburg
research grant. The authors would like to acknowledge the
funding provided by the European Commission (and the mission
support provided by AEDES Brussels) for the Afghanistan
Pharmaceutical Sector Identification Mission carried out in
2007-8 that greatly informed the writing of this paper.
References1 Stewart F, Brown G. Fragile States. CRISE Working Paper No.
51 January 2009. Available from URL: http://www.crise.ox.ac.uk/pubs/workingpaper51.pdf [Accessed 2010 Nov 14]
2 Failed States Index. The Fund For Peace. Available from URL: http://www.fundforpeace.org/web/index.php?option=com_content&task=view&id=99&Itemid=140 [Accessed 2010 Nov 14]
3 Corruption Perceptions Index 2010. Transparency International. Available from URL: http://www.transparency.org/policy_research/surveys_indices/cpi/2010/results [Accessed 2010 Nov 10]
4 Human Development Report. UNDP, New York 2010. Available from URL: http://hdr.undp.org/en/media/HDR_2010_EN_Table1_reprint.pdf [Accessed 2011 Feb 17]
5 Indicators [Online]. The World Bank. Available from URL: http://data.worldbank.org/indicator [Accessed 2010 Nov 9]
6 Human and income poverty: developing countries / Population
living below national poverty line), Human Development Indices: A statistical update 2008, UNDP, New York 2008. Available from URL: http://hdr.undp.org/en/media/HDI_2008_EN_Tables.pdf [Accessed 2010 Nov 8]
7 WHO Global Health Observatory (GHO) 2010. Available from URL: http://www.who.int/gho/en [Accessed 2010 Nov 10]
8 WHO. The world medicines situation [WHO/EDM/PAR/2004.5]. Geneva: WHO, 2004 [online]. Available from URL: http://www.searo.who.int/LinkFiles/Reports_World_Medicines_Situation.pdf [Accessed 2010 Nov 9]
9 Baghdadi G, Chomilier C, Graaff P. Pharmaceutical Situation in Afghanistan. Preliminary Assessment. WHO, 14-23 January 2002. Available from URL: http://whqlibdoc.who.int/HQ/2002/WHO_EDM_DAP_2002.1.pdf [Accessed 2010 Nov 10]
10 Sabri B, Siddiqi S, Ahmed AM, Kakar FK, Perrot J. Towards sustainable delivery of health services in Afghanistan: options for the future. Bull World Health Organ. 2007 Sep; 85(9):712-8.
11 The Essential Package of Hospital Services for Afghanistan. Islamic Republic of Afghanistan Ministry of Public Health July 2005. Available from URL: http://www.msh.org/afghanistan/pdf/Afghanistan_EPHS.pdf [Accessed 2011 Feb 14]
12 Harper JR, Shahab A. Afghanistan Pharmaceutical Sector EC Identification Mission Report (FWC contract 144147). European Commission; 2008.
13 WHO Operational Package for assessing, monitoring and evaluating country pharmaceutical situations”. Guide for coordinators and data collectors. WHO Geneva 2007. Available from URL: http://apps.who.int/medicinedocs/documents/s14877e/s14877e.pdf [Accessed 2010 Oct 22]
14 Mansoor, B, Najib, Mohd. Baseline Drug Indicator Study, A comparative Cross-Sectional Study in SCA Health Facilities in Afghanistan, Part II Results and Next Steps. Swedish Committee for Afghanistan, 2003.
15 WHO Data Collection Tool for the Review of Drug Regulatory Systems. WHO Geneva, 2007. Available from URL: http://www.who.int/medicines/areas/quality_safety/regulation_legislation/ENdatacollectiontool.pdf
16 How to Develop and Implement a National Drug Policy - WHO Policy Perspectives on Medicines, No. 006, 2003. Available from URL: http://infocooperation.org/hss/en/d/Js4869e/5.html [Accessed 2010 Oct 22]
17 Annex 5 WHO good distribution practices for pharmaceutical products. WHO Technical Report Series 957. WHO Expert Committee on Specifications for Pharmaceutical Preparations. Forty-fourth report. WHO Geneva, 2010. Available from URL: http://whqlibdoc.who.int/trs/WHO_TRS_957_eng.pdf (Accessed Nov 9 2010)
18 Afghanistan Private Pharmacies Survey. Management Sciences for Health (August 2004) Hard copy only, referenced in other reports
19 WHO Medicines Strategy 2004-2007: countries at the core. WHO Geneva, 2004 Available from URL: http://whqlibdoc.who.int/hq/2004/WHO_EDM_2004.5.pdf [Accessed 2010 Nov 10]
20 Good Governance for Medicines. Curbing Corruption in Medicines Regulation and Supply. WHO Geneva, 2007. Available from URL: http://www.who.int/medicines/areas/policy/goodgovernance/GGM.pdf [Accessed 2010 Nov 10]
21 Coordinated Procurement and Distribution System (CPDS) Governance Framework. General Directorate of Pharmaceutical Affairs Ministry of Public Health, Islamic Republic of Afghanistan, March 2010. PDF sent by EC

39 Southern Med Review Vol 4 Issue 1 April 2011
Afghanistan pharmaceutical sector development: problems and prospects
22 Paterson A, Karimi A. Understanding markets in Afghanistan: A study of the market for pharmaceuticals. Afghanistan Research and Evaluation Unit. Kabul Afghanistan, December 2005. Available from URL: http://www.a-acc.org/files/Understanding%20Markets%20Pharmaceuticals%20CS%5B1%5D.pdf [accessed 2010 Nov 9]
23 Drug Quality Assessment Study Afghanistan 2007. Ministry of Public Health Islamic Republic of Afghanistan. Available from URL: http://www.moph.gov.af/en/reports/Afghanistan-National-Drug-Quality-Assessment-2007-English.pdf [Accessed 2010 Nov 10]
24 Coincidence or Crisis? Prescription Medicine Counterfeiting. Pitts PJ Editor, Stockholm Network London 2006. Available from URL: www.stockholm-network.org/.../d41d8cd9-Coincidence%20or%20Crisis.pdf [Accessed 2010 Nov 4]
25 Report of the situation of counterfeit medicines based on data collection tool WHO Regions for Africa and Eastern Mediterranean. WHO Geneva 2010. Available from URL: http://www.who.int/medicines/services/expertcommittees/pharmprep/WHO-ACM-3IMPACTSurveyDataCollectionToolReport.pdf [Accessed 2010 Nov 4]
26 Afghanistan Health and Nutrition Sector Strategy (HNSS) 2008-2013. Ministry of Public Health, Ministry of Agriculture, Irrigation & Livestock Islamic Republic of Afghanistan, 2008. Available from URL: http://www.moph.gov.af/en/downloads/Strategy_2007_2008_2012_2013.pdf [Accessed 2010 Nov 4]
27 The World Health Report 2000. Health Systems: Improving Performance. WHO Geneva, 2000 Available from URL: http://www.who.int/whr/2000/en/whr00_en.pdf [Accessed 2010 Nov 10]
28 Travis P, Egger D, Davies P, Mechbal A. Towards better stewardship: concepts and critical issues. Global Programme on Evidence for Health Policy Discussion Papers, No. 48. WHO Geneva, 2002. Available from URL: http://www.who.int/healthinfo/paper48.pdf [Accessed 2010 Nov 10]
29 Corruption widespread in Afghanistan, UNODC survey says. United Nations Office on Drugs and Crime. 19 Jan 2010. Available from URL: http://www.unodc.org/unodc/en/frontpage/2010/January/corruption-widespread-in-afghanistan-unodc-survey-says.html [Accessed 2010 Nov 10]
30 Hansen PM, Peters DH, Niayesh H, Singh LP, Dwivedi V, Burnham G. Measuring and managing progress in the establishment of basic health services: the Afghanistan health sector balanced scorecard. Int J Health Plann Manage. 2008 Apr-Jun; 23(2):107-17.
31 Babar ZU, Scahill SL. Evidence based pharmaceutical policy research: Is it all talk or does it contribute to improving health in developing countries? Southern Med Review (2010) 3; 1:1-1.
32 National Licensed Drugs List (December 2007). General Directorate of Pharmaceutical Affairs, Ministry of Public Health, Islamic Republic of Afghanistan; Essential Drug Department, Avicenna Pharmaceutical Institute. Available from URL: http://www.moph.gov.af/en/downloads/Afghanistan-National-Licensed-Drug-List-December-2007.pdf [accessed 2010 Nov 9]
33 Procedure for application for inclusion of medicines on the licensed drugs list of the Ministry of Public Health of Afghanistan (2007). General Directorate of Pharmaceutical Affairs, Ministry of Public Health, Islamic Republic of Afghanistan; Essential Drug Department, Avicenna Pharmaceutical Institute. Available from URL: http://www.moph.gov.af/en/downloads/Procedure-for-inclusion-of-medicine-in-LDL.pdf [accessed 2010 Nov 9]
34 2006 Afghanistan Health Survey (AHS). Ministry of Public Health, Islamic Republic of Afghanistan. 2006. Available from URL: http://www.humanitarianreform.org/humanitarianreform/Portals/1/cluster%20approach%20page/ Afghanistan/Afghanistan%20Health%20Survey%20Report%202006.pdf [Accessed 2010 Nov 10]
35 Procedure for application for inclusion of medicines on the essential drugs list of the Ministry of Public Health of Afghanistan (2007). General Directorate of Pharmaceutical Affairs, Ministry of Public Health, Islamic Republic of Afghanistan; Essential Drug Department, Avicenna Pharmaceutical Institute. Available from URL: http://www.moph.gov.af/en/downloads/Procedure-for-inclusion-medicine-in-EDL.pdf [accessed 2010 Nov 9]
36 Babar ZU, Scahill SL. Is There a Role for Pharmacoeconomics in Developing Countries? Pharmacoeconomics. 2010: 1-6
37 Afghanistan Statistical Yearbook 2009/2010. Central Statistics Organization (CSO), Islamic Republic of Afghanistan Available from URL: http://www.cso.gov.af/yearbook.zip [accessed 2011 Feb 17]
40 Southern Med Review Vol 4 Issue 1 April 2011
Research Article
Performance based reward for immunization: experiences from GAVIRete Trap1,2, Birna Trap2,3, Torsten Wind Hansen2, Ebba Holme Hansen4
1Department of Surgery, Aabenraa, University Hospital, Denmark2Euro Health Group, Denmark3Management Sciences for Health, SURE Program, Kampala, Uganda4Faculty of Pharmaceutical Sciences, Department of Pharmacology and Pharmacotherapy, University of Copenhagen
Address for Correspondence: Rete Trap, Aabenraa University Hospital, Egelund 10, 6200 Aabenraa, Denmark. E-mail: [email protected]
Citation: Trap R, Trap B, Hansen TW, Hansen EH. Performance based reward for immunization: experiences from GAVI. Southern Med Review (2011) 4;1:40-47 doi:10.5655/smr.v4i1.69
Abstract Objective: To assess whether linking the Global Alliance for Vaccine and Immunization (GAVI) service support with performance-based interventions has influenced the quality of reporting and of immunization systems. GAVI Service Support (ISS) combines performance assessment, recommendations and implementation support with financial reward.
Methods: A retrospective study based on data from Data Quality Audit (DQA), a validated standardized indicator-based performance assessment tool which evaluates reporting consistency, accuracy and the quality of the immunization system. Participants are nine developing countries, sampling 421 health units, 72 districts, which have had two consecutive DQAs in the period 2002 to 2005.
Results: Both the quality of reporting and the immunization system improved following GAVI ISS intervention. Reporting quality was associated with the enhanced overall quality of the immunization system and with immunization coverage. Immunisation coverage improved in eight of the nine countries.
Conclusions: The study indicates that the combined GAVI ISS intervention strategy is effective, resulting in increased immunization coverage, enhanced reporting quality and improved quality of the immunization system set-up at all levels of healthcare. High quality reporting is instrumental in focusing immunization management on setting targets for increased coverage, demonstrated by the correlation between increased reporting quality and immunization coverage. Repeated assessments are recommended to ensure sustainable immunization system improvements.
Keywords: Immunization system; immunization reporting; quality improvements; performance-based financial reward strategy; Global Alliance for Vaccines and Immunization
Based Financial Rewarding (PBFR), a scheme that pays a fixed
fee for children immunised with DTP3 as reported by the
country1,6-7. Immunization service support funding is calculated
based on the prospective performance indicator multiplied
by US$20 in the first investment phase and by US$20 in the
reward phase. Reliable and accurate reporting of the number
of children immunised is a prerequisite for being allowed to
participate in the reward scheme. The Global Alliance for
Vaccines and Immunization uses a data quality audit (DQA) with
a pass and fail limit to verify the consistency and accuracy of
the EPI (expanded programme on immunization) administrative
reporting system6,8.
An independent DQA is conducted at national (Nat), district (Dis)
and health unit (HU) levels. After a DQA has been completed,
IntroductionGlobal coverage of childhood Diptheria-Tetanus-Pertussis
(DTP3) immunization increased to 80% in 1990, after
which immunization rates declined considerably in many
countries1,2. Several initiatives have been introduced to
strengthen immunization3-5. The Global Alliance for Vaccines
and Immunization (GAVI) initiative, the most costly, has been
introduced in over 75 countries. However, the effectiveness of
this initiative needs to be further investigated.
The Global Alliance for Vaccines and Immunization (GAVI), a
public-private global health partnership, was established in
1999 for strengthening immunization service support (ISS).
Immunization service support (ISS) is linked to Performance-

41 Southern Med Review Vol 4 Issue 1 April 2011
Performance based reward for immunization: experiences from GAVI
immunization system quality findings and recommendations are shared with national authorities. A country that fails the DQA is given a second chance two to three years later2,6,9.
Ronveaux et al. conducted a validation of the DQA by reviewing the results from 27 DQAs undertaken8. The DQA was found to be a tool that provides a sound basis for assessing the quality of the national immunization system: a) the consistency and accuracy of the EPI administrative reporting system, and b) the overall quality of the national immunization set-up8. Accurate immunization reports are essential for depicting the actual situation, for decision making and achieving increased immunization coverage10. Much effort has been put into strengthening reporting and data quality and management, e.g. by developing guidelines, training initiatives and standard practices8-10. However, as demonstrated by the findings from GAVI, these initiatives have not led to the desired reporting quality as almost half of the 41 assessed countries did not pass DQA due to poor reporting quality11.
The new GAVI initiative links the reporting quality assessed by DQA with performance-based financial rewarding, providing country-specific recommendations and implementation-support in order to improve reporting quality and thus immunization.
The objective of this study is to assess the effectiveness of the
combined GAVI immunization service support strategy, utilizing
countries that have had two consecutive DQAs in a pre-DQA
and post-DQA study design. This study assesses whether
the GAVI ISS strategy linking reward-based interventions to
immunization system assessment (DQA) and recommendations
for improvements and implementation support have improved
the quality of the national immunization systems in terms of:
a. the consistency and accuracy of the expanded programme on
immunization administrative reporting system and
b. the overall quality of the national immunization set-up.
MethodologyData Quality Audit
Data quality audit, a WHO validated and standardised survey
method based on sentinel indicators measuring consistency of
national reports and quality, efficiency, security and usefulness
of the immunization set-up at each reporting level (national,
district and health unit), was conducted pre and post in all nine
countries8.
Box 1
Verification factor (VF), a key performance measure at national (Nat), district (Dis) and health unit (HU) levels, measuring reporting consistency.
VF (HU): Calculated in each districti (based on the previous year’s reported activity) as the sum from all 6 selected HUs(j=1-6) of the quotient: the numbers of DTP3 vaccinations that are recounted from records in the selected health units, divided by the number of DTP3 vaccinations entered in the district files as reported from the very same health units.
(Xij = the number of recounted DTP3 vaccinations found in the records of the HUj in the Disj;
Yij = the number of reported DTP3 vaccinations found in district file records as reported by the HUj in the Disi)
VF (Dis): Calculated as VF (HU) Disi multiplied by the ratio of all DTP3 vaccinations reported to national level from all HUs in the districti found at district level, divided by number of all reported DTP3 vaccinations found at national level from districti.
(Rdi = At district level, the number of all DTP3 vaccinations reported from all HUs from the district to the national level; Rni = At national level, the number of DTP3 vaccinations reported by the district)
VF (Nat): Calculated as the weighted average of the VF (Dis), from all four selected districts.
A score of 1 is a complete match between recounted/reported. No more then 20 % deviation is accepted for a passing DQA score, so scores between 0.8 and 1.2 in the VF (Nat) are the threshold for release of funds8.
VF (HU) Disi =
=
=
6
1
6
1
jij
jij
y
x
VF (Dis)i =i
i
jij
jij
RnRd
i
i
RnRd
y
x
=
=
6
1
6
1 [ ]iDisHUVF )(=
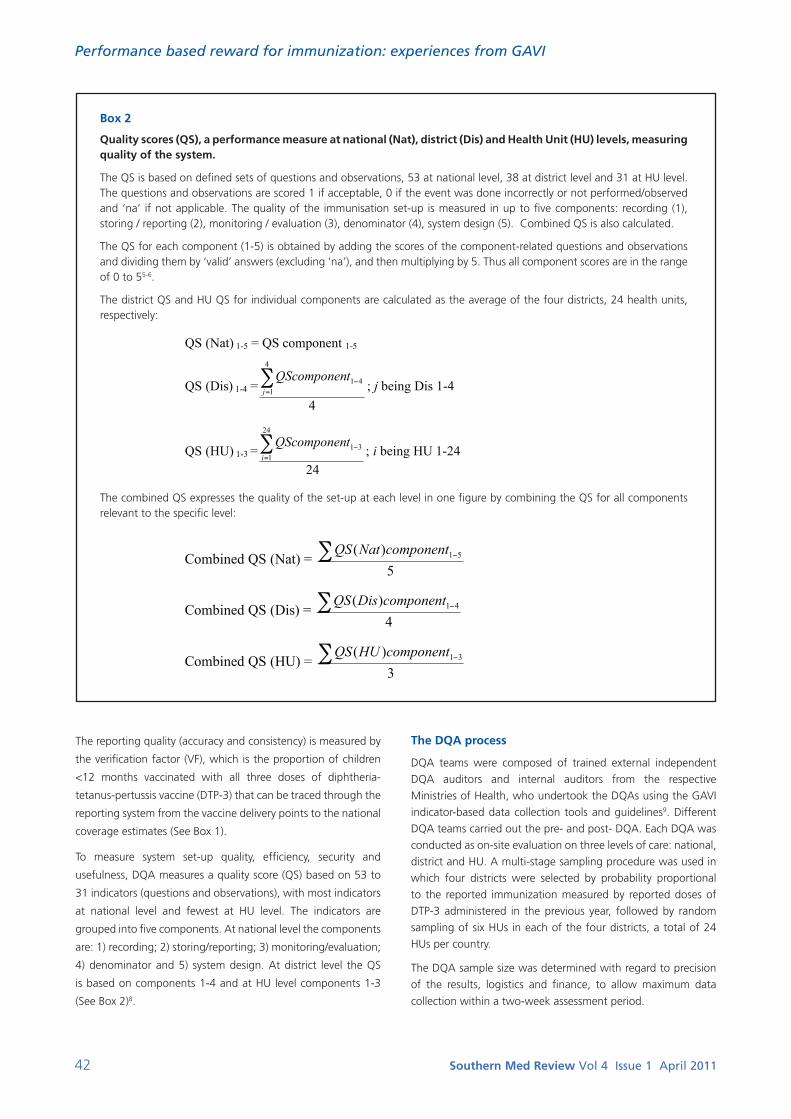
42 Southern Med Review Vol 4 Issue 1 April 2011
Performance based reward for immunization: experiences from GAVI
Box 2
Quality scores (QS), a performance measure at national (Nat), district (Dis) and Health Unit (HU) levels, measuring quality of the system.
The QS is based on defined sets of questions and observations, 53 at national level, 38 at district level and 31 at HU level. The questions and observations are scored 1 if acceptable, 0 if the event was done incorrectly or not performed/observed and ‘na’ if not applicable. The quality of the immunisation set-up is measured in up to five components: recording (1), storing / reporting (2), monitoring / evaluation (3), denominator (4), system design (5). Combined QS is also calculated.
The QS for each component (1-5) is obtained by adding the scores of the component-related questions and observations and dividing them by ‘valid’ answers (excluding ‘na’), and then multiplying by 5. Thus all component scores are in the range of 0 to 55-6.
The district QS and HU QS for individual components are calculated as the average of the four districts, 24 health units, respectively:
The combined QS expresses the quality of the set-up at each level in one figure by combining the QS for all components relevant to the specific level:
QS (Nat) 1-5 = QS component 1-5
QS (Dis) 1-4 =4
4
141
=j
tQScomponen; j being Dis 1-4
QS (HU) 1-3 =24
24
131
=i
tQScomponen; i being HU 1-24
Combined QS (Nat) = 5
)( 51componentNatQS
Combined QS (Dis) = 4
)( 41componentDisQS
Combined QS (HU) = 3
)( 31componentHUQS
The reporting quality (accuracy and consistency) is measured by
the verification factor (VF), which is the proportion of children
<12 months vaccinated with all three doses of diphtheria-
tetanus-pertussis vaccine (DTP-3) that can be traced through the
reporting system from the vaccine delivery points to the national
coverage estimates (See Box 1).
To measure system set-up quality, efficiency, security and
usefulness, DQA measures a quality score (QS) based on 53 to
31 indicators (questions and observations), with most indicators
at national level and fewest at HU level. The indicators are
grouped into five components. At national level the components
are: 1) recording; 2) storing/reporting; 3) monitoring/evaluation;
4) denominator and 5) system design. At district level the QS
is based on components 1-4 and at HU level components 1-3
(See Box 2)8.
The DQA process
DQA teams were composed of trained external independent
DQA auditors and internal auditors from the respective
Ministries of Health, who undertook the DQAs using the GAVI
indicator-based data collection tools and guidelines9. Different
DQA teams carried out the pre- and post- DQA. Each DQA was
conducted as on-site evaluation on three levels of care: national,
district and HU. A multi-stage sampling procedure was used in
which four districts were selected by probability proportional
to the reported immunization measured by reported doses of
DTP-3 administered in the previous year, followed by random
sampling of six HUs in each of the four districts, a total of 24
HUs per country.
The DQA sample size was determined with regard to precision
of the results, logistics and finance, to allow maximum data
collection within a two-week assessment period.
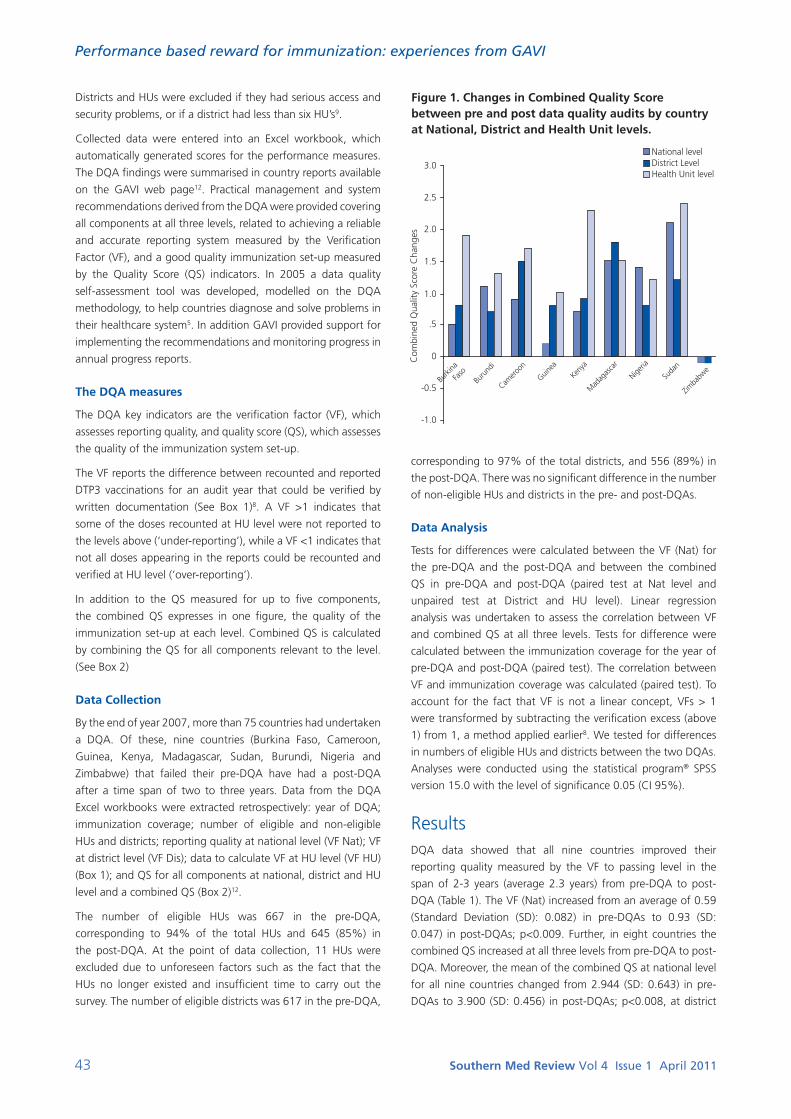
43 Southern Med Review Vol 4 Issue 1 April 2011
Performance based reward for immunization: experiences from GAVI
Districts and HUs were excluded if they had serious access and
security problems, or if a district had less than six HU’s9.
Collected data were entered into an Excel workbook, which
automatically generated scores for the performance measures.
The DQA findings were summarised in country reports available
on the GAVI web page12. Practical management and system
recommendations derived from the DQA were provided covering
all components at all three levels, related to achieving a reliable
and accurate reporting system measured by the Verification
Factor (VF), and a good quality immunization set-up measured
by the Quality Score (QS) indicators. In 2005 a data quality
self-assessment tool was developed, modelled on the DQA
methodology, to help countries diagnose and solve problems in
their healthcare system5. In addition GAVI provided support for
implementing the recommendations and monitoring progress in
annual progress reports.
The DQA measures
The DQA key indicators are the verification factor (VF), which
assesses reporting quality, and quality score (QS), which assesses
the quality of the immunization system set-up.
The VF reports the difference between recounted and reported
DTP3 vaccinations for an audit year that could be verified by
written documentation (See Box 1)8. A VF >1 indicates that
some of the doses recounted at HU level were not reported to
the levels above (‘under-reporting’), while a VF <1 indicates that
not all doses appearing in the reports could be recounted and
verified at HU level (‘over-reporting’).
In addition to the QS measured for up to five components,
the combined QS expresses in one figure, the quality of the
immunization set-up at each level. Combined QS is calculated
by combining the QS for all components relevant to the level.
(See Box 2)
Data Collection
By the end of year 2007, more than 75 countries had undertaken
a DQA. Of these, nine countries (Burkina Faso, Cameroon,
Guinea, Kenya, Madagascar, Sudan, Burundi, Nigeria and
Zimbabwe) that failed their pre-DQA have had a post-DQA
after a time span of two to three years. Data from the DQA
Excel workbooks were extracted retrospectively: year of DQA;
immunization coverage; number of eligible and non-eligible
HUs and districts; reporting quality at national level (VF Nat); VF
at district level (VF Dis); data to calculate VF at HU level (VF HU)
(Box 1); and QS for all components at national, district and HU
level and a combined QS (Box 2)12.
The number of eligible HUs was 667 in the pre-DQA,
corresponding to 94% of the total HUs and 645 (85%) in
the post-DQA. At the point of data collection, 11 HUs were
excluded due to unforeseen factors such as the fact that the
HUs no longer existed and insufficient time to carry out the
survey. The number of eligible districts was 617 in the pre-DQA,
corresponding to 97% of the total districts, and 556 (89%) in
the post-DQA. There was no significant difference in the number
of non-eligible HUs and districts in the pre- and post-DQAs.
Data Analysis
Tests for differences were calculated between the VF (Nat) for
the pre-DQA and the post-DQA and between the combined
QS in pre-DQA and post-DQA (paired test at Nat level and
unpaired test at District and HU level). Linear regression
analysis was undertaken to assess the correlation between VF
and combined QS at all three levels. Tests for difference were
calculated between the immunization coverage for the year of
pre-DQA and post-DQA (paired test). The correlation between
VF and immunization coverage was calculated (paired test). To
account for the fact that VF is not a linear concept, VFs > 1
were transformed by subtracting the verification excess (above
1) from 1, a method applied earlier8. We tested for differences
in numbers of eligible HUs and districts between the two DQAs.
Analyses were conducted using the statistical program® SPSS
version 15.0 with the level of significance 0.05 (CI 95%).
ResultsDQA data showed that all nine countries improved their
reporting quality measured by the VF to passing level in the
span of 2-3 years (average 2.3 years) from pre-DQA to post-
DQA (Table 1). The VF (Nat) increased from an average of 0.59
(Standard Deviation (SD): 0.082) in pre-DQAs to 0.93 (SD:
0.047) in post-DQAs; p<0.009. Further, in eight countries the
combined QS increased at all three levels from pre-DQA to post-
DQA. Moreover, the mean of the combined QS at national level
for all nine countries changed from 2.944 (SD: 0.643) in pre-
DQAs to 3.900 (SD: 0.456) in post-DQAs; p<0.008, at district
Figure 1. Changes in Combined Quality Score between pre and post data quality audits by country at National, District and Health Unit levels.
0
.5
-0.5
-1.0
1.0
1.5
2.0
2.5
3.0
National levelDistrict LevelHealth Unit level
Com
bine
d Q
ualit
y Sc
ore
Cha
nges
Burki
na
Faso
Buru
ndi
Camero
on
Guinea
Kenya
Mad
agas
car
Nigeria
Suda
n
Zimba
bwe

44 Southern Med Review Vol 4 Issue 1 April 2011
Performance based reward for immunization: experiences from GAVI
level from 3.069 (SD: 0.4391) to 4.005 (SD: 0.384); p<0.002
and at HU level from 2.747 (SD: 0.736) to 4.223 (SD: 0.259);
p<0.002. The changes in the combined QS were highest at HU
level and lowest at national level (Figure 1).
The one country with a decrease in the combined QS was
Zimbabwe. However, the score remained at a high level and
decreased by only 0.1. In addition, reporting consistency in
Zimbabwe improved at district level with the range of the VF
(Dis) narrowing from pre-DQA to post-DQA by 0.46 - 1.11 and
0.90 - 1.12 respectively.
Figure 2* displays the combined QS found in the two
consecutive DQAs for all nine countries at the three levels. The
figure shows that there was a general increase at all three levels
and a reduction in the SD.
Table 1 shows that there was no unified direction for the
changes in the five QS components at the various levels in the
nine countries. Immunization coverage was seen to increase
significantly in all but one country, from an average of 59.9%
(SD: 21.2) in pre-DQAs to 66.4% (SD: 19.6) in post-DQAs;
p<0.02.
Table 2 shows the correlation between the VF and the combined
QS and the components QS. A correlation was found between
the VF (Nat) and the combined QS (Nat), the VF (Dis) and
the combined QS (Dis), and between the VF (HU) and the
combined QS (HU), showing that an improvement in the quality
of the overall immunization set-up was associated with an
improvement in the quality of reporting.
A correlation was found between reporting quality (VF) and all
five QS components except the denominator component, but
not at all levels. At national level we found a correlation between
the VF (Nat) and the QS component, system design (Table 2). At
district level a correlation was found between the VF (Dis) and
the QS components, recording and monitoring/evaluation. At HU
level, a correlation was found between the VF (HU) and the three
QS components, recording, storing/reporting and monitoring/
evaluation (Table 2). Hence, all QS components with the exception
of the denominator were related to reporting quality.
We found a significant correlation between the VF (Nat)
and immunization coverage, with a positive and moderate
correlation of 0.43; p<0.009 (Figure 3).
DiscussionFinding improved reporting quality from pre-DQA to post-DQA
in all nine countries is really quite astounding, especially when
taking into consideration the short average time span of 2.3
years that it took to implement the changes and make the
improvements even down at rural health facility level. National
interventions such as the revision or introduction of standardised
operational procedures, report formats and use of carbon
paper reports as recommended following the DQA are believed
to have led to the improved reporting quality. Moreover, the
recommendations provided in the pre-DQAs regarding system
quality have led to documented improvements at all levels in the
quality of the immunization set-up. In spite of the acknowledged
difficulties in ensuring appropriate reporting management,
this study suggests the effectiveness of the GAVI ISS strategy,
a strategy which combines auditing, recommendations and
reward, in identifying and improving reporting quality as well as
in strengthening the quality, efficiency, security and usefulness
of the system at all levels.
In Zimbabwe, only the verification factor improved. It is likely
that the minimal decrease in the quality of the set-up observed
Figure 3. Verification Factor and Immunization Coverage (DTP3) in the nine countries with pre and post data quality audits.
0 0
20
40
60
80
100
0.2
0.4
0.6
0.8
1
VFImm Cov
Verif
catio
n Fa
ctor
– V
F
Imm
unis
atio
n C
over
age
(%) –
Imm
Cov
1 3 5 7 9 11Pre- and Post-Date Quality Audit date of the nine countries
13 15 17
* DQA1 Nat CQS (0.56; 2.5) Nigeria and DQA2 Nat CQS (0.95; 3.9) Burundi are not depicted in the figure, as they are “behind” identical figures for DQA1 District CQS and respective DQA2 Health Unit CQS.
Figure 2. National Verification Factor versus the Combined Quality Score at National, District and Health Unit levels in nine countries with pre and post data quality audits.
1.5
2.5
2.0
3.0
3.5
4.0
4.5
5.0
0.4 0.5 0.6 0.7 0.8 0.9 1.0
Com
bine
d Q
ualit
y Sc
ores
National Verification Factor
DQA1 National CQSDQA1 District CQSDQA1 Health Unit CQSDQA2 National CQSDQA2 District CQSDQA2 Health Unit CQS
Pre data quality audit (DQA1): symbolised byPost data quality audit (DQA2): symbolised by
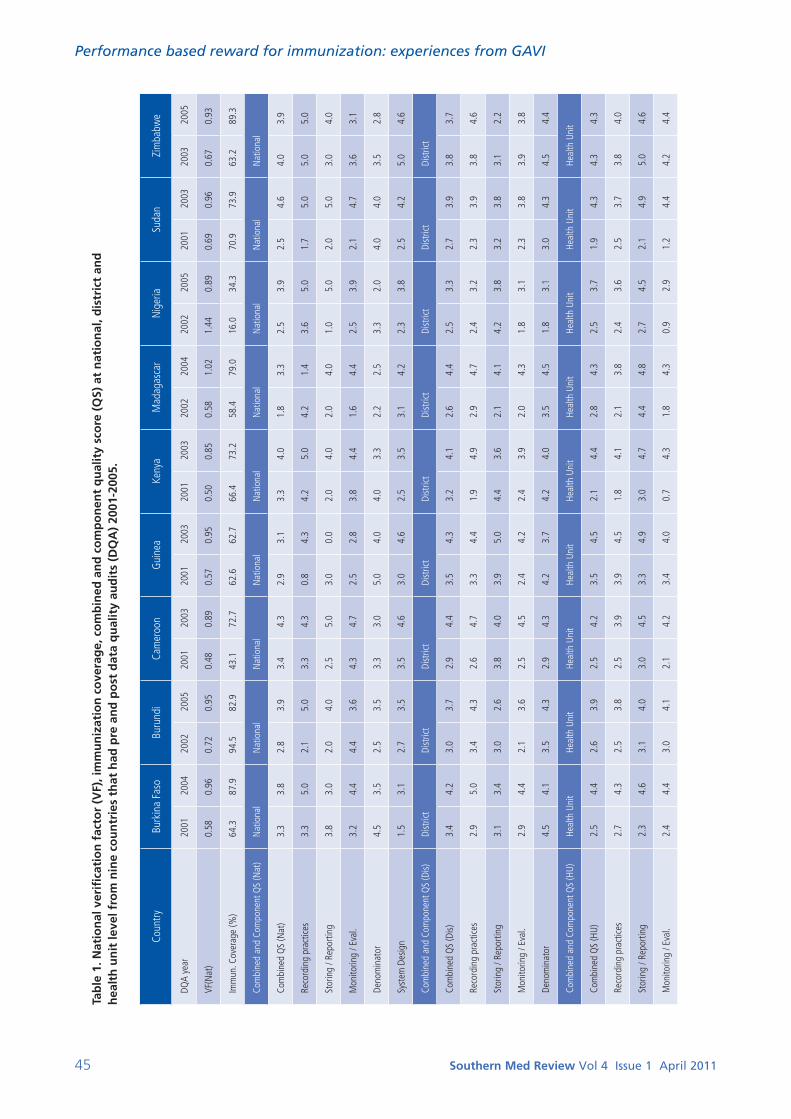
45 Southern Med Review Vol 4 Issue 1 April 2011
Performance based reward for immunization: experiences from GAVI
Tab
le 1
. Nat
ion
al v
erifi
cati
on
fac
tor
(VF)
, im
mu
niz
atio
n c
ove
rag
e, c
om
bin
ed a
nd
co
mp
on
ent
qu
alit
y sc
ore
(Q
S) a
t n
atio
nal
, dis
tric
t an
d
hea
lth
un
it le
vel f
rom
nin
e co
un
trie
s th
at h
ad p
re a
nd
po
st d
ata
qu
alit
y au
dit
s (D
QA
) 20
01-2
005.
Coun
tryBu
rkin
a Fa
soBu
rund
iCa
mer
oon
Gui
nea
Keny
aM
adag
asca
rN
iger
iaSu
dan
Zim
babw
e
DQA
year
2001
2004
2002
2005
2001
2003
2001
2003
2001
2003
2002
2004
2002
2005
2001
2003
2003
2005
VF(N
at)
0.58
0.96
0.72
0.95
0.48
0.89
0.57
0.95
0.50
0.85
0.58
1.02
1.44
0.89
0.69
0.96
0.67
0.93
Imm
un. C
over
age
(%)
64.3
87.9
94.5
82.9
43.1
72.7
62.6
62.7
66.4
73.2
58.4
79.0
16.0
34.3
70.9
73.9
63.2
89.3
Com
bine
d an
d Co
mpo
nent
QS
(Nat
)N
atio
nal
Nat
iona
lN
atio
nal
Nat
iona
lN
atio
nal
Nat
iona
lN
atio
nal
Nat
iona
lN
atio
nal
Com
bine
d Q
S (N
at)
3.3
3.8
2.8
3.9
3.4
4.3
2.9
3.1
3.3
4.0
1.8
3.3
2.5
3.9
2.5
4.6
4.0
3.9
Reco
rdin
g pr
actic
es
3.3
5.0
2.1
5.0
3.3
4.3
0.8
4.3
4.2
5.0
4.2
1.4
3.6
5.0
1.7
5.0
5.0
5.0
Stor
ing
/ Rep
ortin
g 3.
83.
02.
04.
02.
55.
03.
00.
02.
04.
02.
04.
01.
05.
02.
05.
03.
04.
0
Mon
itorin
g / E
val.
3.2
4.4
4.4
3.6
4.3
4.7
2.5
2.8
3.8
4.4
1.6
4.4
2.5
3.9
2.1
4.7
3.6
3.1
Deno
min
ator
4.5
3.5
2.5
3.5
3.3
3.0
5.0
4.0
4.0
3.3
2.2
2.5
3.3
2.0
4.0
4.0
3.5
2.8
Syst
em D
esig
n1.
53.
12.
73.
53.
54.
63.
04.
62.
53.
53.
14.
22.
33.
82.
54.
25.
04.
6
Com
bine
d an
d Co
mpo
nent
QS
(Dis)
Dist
rict
Dist
rict
Dist
rict
Dist
rict
Dist
rict
Dist
rict
Dist
rict
Dist
rict
Dist
rict
Com
bine
d Q
S (D
is)3.
44.
23.
03.
72.
94.
43.
54.
33.
24.
12.
64.
42.
53.
32.
73.
93.
83.
7
Reco
rdin
g pr
actic
es2.
95.
03.
44.
32.
64.
73.
34.
41.
94.
92.
94.
72.
43.
22.
33.
93.
84.
6
Stor
ing
/ Rep
ortin
g 3.
13.
43.
02.
63.
84.
03.
95.
04.
43.
62.
14.
14.
23.
83.
23.
83.
12.
2
Mon
itorin
g / E
val.
2.9
4.4
2.1
3.6
2.5
4.5
2.4
4.2
2.4
3.9
2.0
4.3
1.8
3.1
2.3
3.8
3.9
3.8
Deno
min
ator
4.5
4.1
3.5
4.3
2.9
4.3
4.2
3.7
4.2
4.0
3.5
4.5
1.8
3.1
3.0
4.3
4.5
4.4
Com
bine
d an
d Co
mpo
nent
QS
(HU)
Heal
th U
nit
Heal
th U
nit
Heal
th U
nit
Heal
th U
nit
Heal
th U
nit
Heal
th U
nit
Heal
th U
nit
Heal
th U
nit
Heal
th U
nit
Com
bine
d Q
S (H
U)2.
54.
42.
63.
92.
54.
23.
54.
52.
14.
42.
84.
32.
53.
71.
94.
34.
34.
3
Reco
rdin
g pr
actic
es2.
74.
32.
53.
82.
53.
93.
94.
51.
84.
12.
13.
82.
43.
62.
53.
73.
84.
0
Stor
ing
/ Rep
ortin
g2.
34.
63.
14.
03.
04.
53.
34.
93.
04.
74.
44.
82.
74.
52.
14.
95.
04.
6
Mon
itorin
g / E
val.
2.4
4.4
3.0
4.1
2.1
4.2
3.4
4.0
0.7
4.3
1.8
4.3
0.9
2.9
1.2
4.4
4.2
4.4

46 Southern Med Review Vol 4 Issue 1 April 2011
Performance based reward for immunization: experiences from GAVI
is related to the initially high and above-average level of quality
coupled with the limited availability of resources as a result of
the prevailing political and socio-economic situation.
The GAVI ISS strategy provides an assessment of the
national immunization system (DQA) recommendations for
improvements and reward funding. Many factors influence
the impact of an intervention. To adequately assess the impact
of the GAVI intervention it ought to be controlled for existing
trends or other influencing factors. A rigorous controlled trial
study design would therefore have been preferable rather
than this pre-post study. In studies related to rational drug use,
combining managerial and financial strategies has proven to be
the most effective and sustainable strategy13-14. Moreover, there
are longstanding concerns that performance-oriented initiatives
such as GAVI ISS might encourage over-reporting2,15. However,
this study documents that combining financial, managerial
and educational strategies not only increased reporting quality
(VF>80%), but decreased over-reporting from 40% to 7%,
and improved overall system quality. An earlier study found
that over-reporting tended to increase with time and was most
pronounced after three years15. Although the present study
indicates that the GAVI ISS strategy ensures high reporting
quality, the sustainability is not known. Therefore repeated
follow-up DQA is recommended.
Our findings showing improvements at all levels indicate that corrective measures, as outlined in the DQA recommendations, have been implemented at all levels within a very short span of time, less than three years. As the reward system is directly linked to a passing verification factor score, improvements in the VF alone would have been sufficient. However, the documented improvement in set-up quality indicates that the nationally applied strategies focused not only on increasing the VF but on the overall immunization system as well. The correlation between the VF at the three levels and all the QS components apart from the denominator indicates that an immunization system providing a reliable and accurate reporting system is associated with high quality immunization procedures and managerial set-ups at all levels. In line with our findings, a previous GAVI study found that there was a correlation between the QSs at the various levels (Nat, Dis and HU)11.
The explanation of non-significance with the denominator component might be the low sample number (nine), as the denominator is only measured at national level. The importance of the comprehensive ISS strategy, e.g. country-specific recommendations and implementation support in achieving such nationwide improvements, is not clear. However, there is good reason to believe that such specific and practical recommendations combined with implementation support and progress reporting have been crucial to the demonstrated improved overall quality of the national immunization system.
We found a positive correlation at all three levels between VF and combined QS, while earlier studies only found a correlation between VF and combined QS at district and HU level8,11. Our findings indicate that a well functioning, high quality immunization set-up, including all the QS components and at all levels, with correctly implemented operational procedures, leads to accurate and reliable reporting.
A correlation was only found between the VF and system design at national level, whereas more components were correlated to the VF at lower levels, i.e. recording and monitoring / evaluation at district level and all three (recording, monitoring / evaluation and storing / reporting) at HU level indicating that the QS at district and HU levels have the highest impact on the VF. Therefore interventions to support a country in passing the DQA must ensure system improvements at all levels, particularly at HU and district levels. An analysis of the correlation between the QS components and the VF has not been included in the prior analysis8,11. Based on the significant correlation between QS and VF shown in this study it is justified and rational to introduce and implement interventions to strengthen the system and thereby improving the VF.
Despite the fact that passing the DQA is only linked to the VF score, the fact that improvements were found in all the QS components except the denominator QS component indicates that there is no need to establish minimum or ‘pass’ scores for
the QS as the QS is indirectly linked to passing.
Moreover, the finding of a significant increase in immunization
coverage in eight of the nine countries points to the
Table 2. Correlation between the combined and component quality scores (QS) and the verification factor (VF) at national, district and health unit levels.
VF Level Quality Score (QS) p- values ß-values
VF(National)
VF(District)
VF(Health Unit)
Combined QS (National)
Combined QS (District)
Combined QS (Health Unit)
* 0.01
* 0.00
* 0.00
0.608
0.431
0.592
VF(National) QS (National), Recording
QS (National), Storing / Reporting
QS (National), Monitoring / Evaluation
QS (National), Denominator
QS (National), System Design
0.37
0.06
0.08
0.26
* 0.01
1.430
1.300
0.883
0.789
0.790
VF(District) QS(District), Recording
QS(District), Storing /Reporting
QS(District), Monitoring / Evaluation
QS(District), Denominator
* 0.00
0.97
* 0.00
0.06
0.585
0.780
0.567
0.677
VF(Health Unit) QS(Health Unit), Recording
QS(Health Unit), Storing /Reporting
QS(Health Unit), Monitoring / Evaluation
* 0.00
* 0.00
* 0.00
0.518
0.770
0.952
Test method: Linear regression analysis, ß = mean change in VF per unit in QS * indicates significant correlation (p<0.05)
47 Southern Med Review Vol 4 Issue 1 April 2011
Performance based reward for immunization: experiences from GAVI
appropriateness of the combined GAVI ISS strategy. Based
on the improved reporting quality and the decrease in over-
reporting between the pre- and post- DQAs, which provided
more reliable data, it is reasonable to assume that the measured
increase in DPT3 is a real increase. This assumption is further
substantiated by the fact that even with constant coverage the
decrease in over-reported vaccinations would have resulted in a
decrease in coverage.
The finding of a positive and moderate correlation between
reporting quality and immunization coverage indicates that
improved reporting quality enables better target setting,
which leads to strengthened immunization management and
thereby improved coverage. However, in line with our findings,
earlier studies indicate that having a system with a high
quality of reporting ensures evidence-based decision making
and management which aims at increasing immunization
coverage7,10,16.
ConclusionAs demonstrated by the fact that all the countries in the study
passed their second assessment, there is good reason to believe
that the combined GAVI ISS strategy linking reward-based
interventions to immunization system assessment (DQA) and
recommendations for improvements and implementation
support have been instrumental in improving the quality of
reporting. Moreover, quality reporting which provides accurate
and consistent data is instrumental in focusing immunization
management on setting targets for increased coverage,
demonstrated by the correlation between increased reporting
quality (VF) and increased immunization coverage. Finally, the
study showed that improvements in the immunization set-up
at all levels were fundamental to improving reporting quality
as demonstrated by the correlation between VF and combined
QS. However, it is not clear if the achieved improvements in
the national immunization system (VF, QS) are sustainable.
Therefore, we recommend that system assessment be repeated
regularly, either by self-assessment or DQA.
AcknowledgmentWe would like to thank Bjørn Melgaard (Euro Health Group),
Olivier Ronveaux and Abdallah Bchir (GAVI Alliance, Geneva,
Switzerland) for their suggestions on the manuscript at several
stages. We also thank the staff in all the countries concerned
with GAVI and DQA for their support and collaboration.
References1. Wittet S. Introducing GAVI and the Global Fund for Children’s
Vaccines. Vaccine 2001; 91: 385-386.
2. Brugha R, Starling M, Walt G. GAVI, The first steps: lessons for the Global Fund. The Lancet 2002; 359: 435-438.
3. Murray CJL, Shengelia B, Neeru G, Moussavi S, Ajay T, Thieren M. Validity of reported vaccination coverage in 45 countries. The Lancet 2003; 362, 1022-1027.
4. Onta SR, Sabroe S, Hansen EH. The quality of immunization data from routine primary health care reports: a case from Nepal. Health Policy and Planning 1998; 13, 131-139.
5. World Health Organization. Immunization in Practice. A Practical Resource Guide for Health Workers. 2004 Update. WHO, Geneva. http://aim.path.org/en/vaccines/welcome/index.html Accessed [2008].
6. Global Alliance for Vaccines and Immunization. How to Prepare for a Data Quality Audit – Briefing Paper: http://www.gavialliance.org/resources/DQABriefPaper02.pdf. Accessed [2008]
7. Martin JF, Marshall J. New tendencies and strategies in international immunization: GAVI and The Vaccine Fund. Vaccine 2003; 21, 587-592.
8. Ronveaux O, Rickert D, Hadler S, et al. The immunization data quality audit: verifying the quality and consistency of immunization monitoring systems. Bull World Health Organ. 2005; 7: 503-510.
9. World Health Organization. The immunization data quality audit (DQA) procedure. Geneva: WHO; 2003. WHO document WHO/V&B/03.19.: http://www.who.int/vaccines-documents/DoxGen/H5-Surv.htm Accessed [2008].
10. Papania M, Rodewald L. For better immunization coverage, measure coverage better. The Lancet 2006; 367, 965-966.
11. Bosch-Capblanch X, Ronveaux O, Doyle V, Remedios V, Bchir A. Accuracy and quality of immunization information systems in forty-one low income countries. Tropical Medicine and International Health 2009; 14:1-10.
12. GAVI Alliance, Country data: http://www.gavialliance.org/performance/country_results/dqas/index.php, Accessed [2008]
13. World Health Organization. Interventions and strategies to improve The use of antimicrobials in developing countries: a review. Drug Management Program. WHO/CDS/CSR/DRS/2001.9: http://whqlibdoc.who.int/hq/2001/WHO_CDS_CSR_DRS_2001.9.pdf , Accessed [2008]
14. Holloway K. Understanding Rational Use of medicines. A publication of the World Council of Churches. Contact 2006; 183: 2-4.
15. Lim SS, Stein DB, Charrow A, Murray CJL. Tracking progress towards universal childhood immunization and the impact of global initiatives: a systematic analysis of three-dose diphtheria, tetanus, and pertussis immunization coverage. The Lancet 2008; 372: 2031-2046.
16. GAVI alliance: Achieving our Immunization Goals. Final report.McKinsey-GAVI.2003: http://www.gaviallaince.org/resources/achieving_immunization_goals_april03.pdf. Accessed [2008]