sorveglianza attiva e trattamenti ablativi vincenzo ficarra direttore clinica di urologia azienda...
TRANSCRIPT

Sorveglianza attiva e trattamenti ablativi
Vincenzo Ficarra
Direttore Clinica di Urologia Azienda Ospedaliera Universitaria di Udine
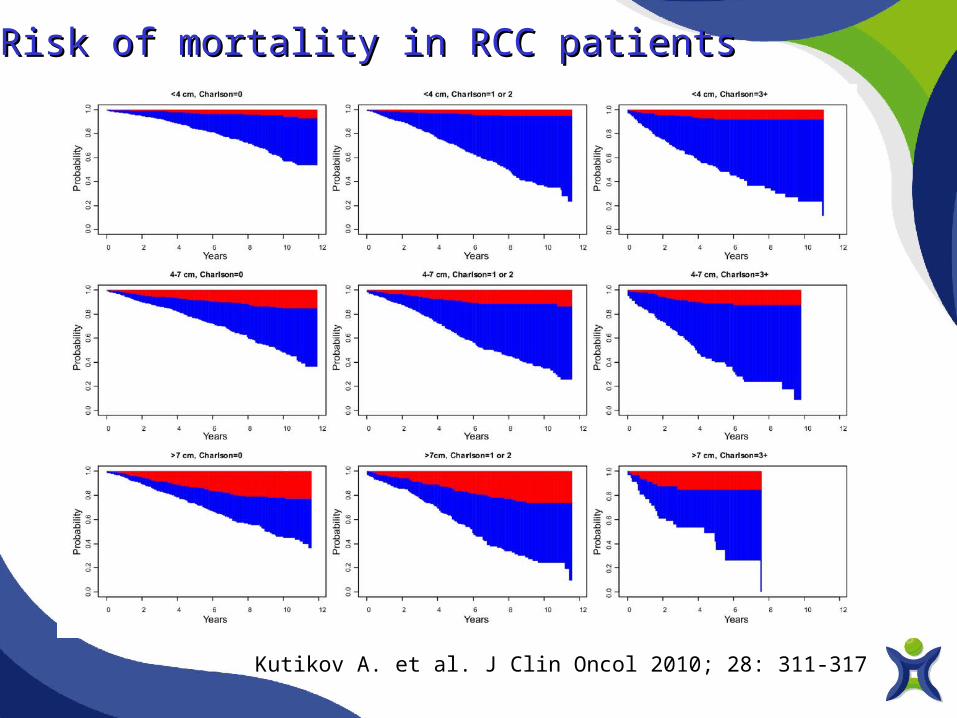
Risk of mortality in RCC patientsRisk of mortality in RCC patients
Kutikov A. et al. J Clin Oncol 2010; 28: 311-317
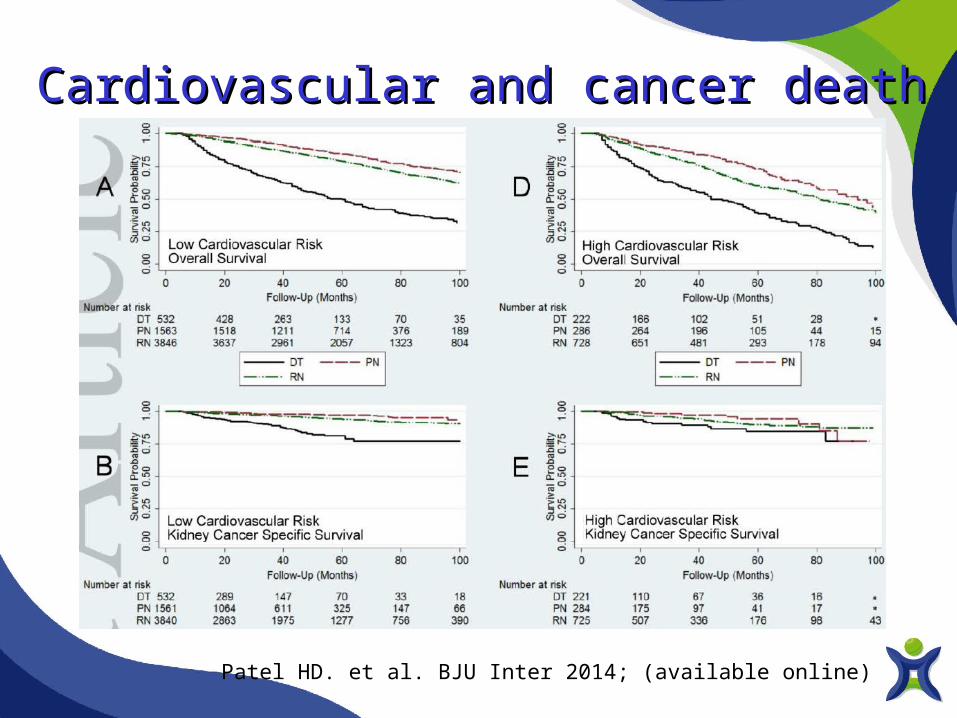
Cardiovascular and cancer death Cardiovascular and cancer death
Patel HD. et al. BJU Inter 2014; (available online)
Active SurveillanceActive Surveillance• Active surveillance is defined as the initial
monitoring of tumour size by serial abdominal imaging (ultrasound, CT, or MRI) with delayed intervention reserved for those tumours that show clinical progression during follow-up
• Active surveillance is a reasonable option for elderly and/or comorbid patients with small renal masses and limited life expectancy
Ljungberg B. et al. EAU Guidelines, 2014
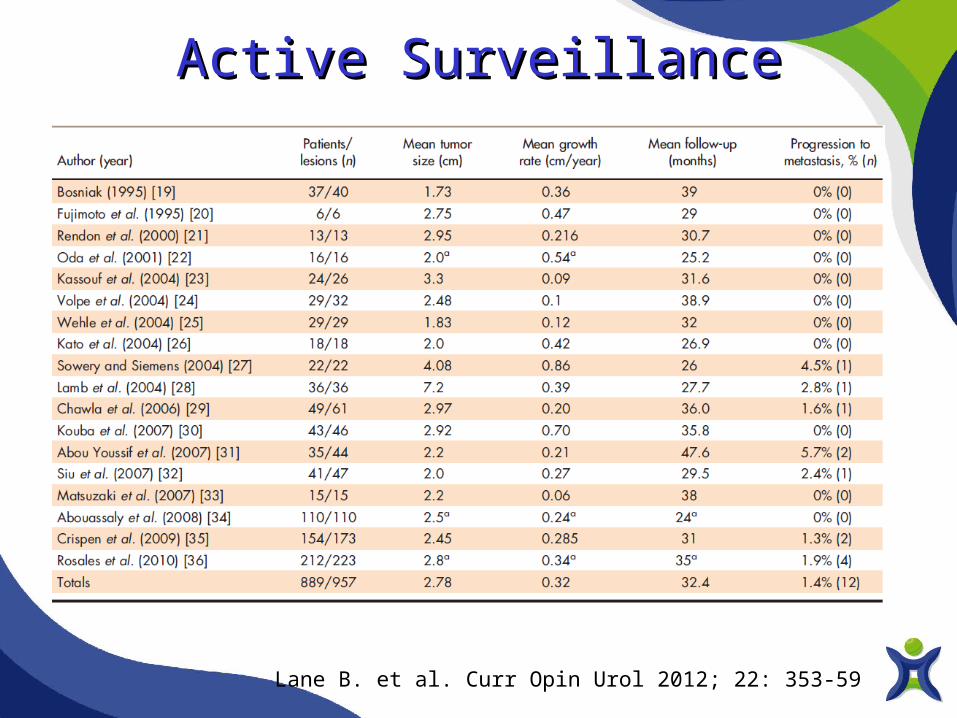
Active SurveillanceActive Surveillance
Lane B. et al. Curr Opin Urol 2012; 22: 353-59
Active SurveillanceActive Surveillance
Lane B. et al. Curr Opin Urol 2012; 22: 353-59
• SRMs less than 3 cm are very unlikely to metastasize and deferring treatment has not been associated with increased failure to cure.
• Active surveillance is a reasonable initial strategy in most patients with SRMs, particularly those with limited life-expectancy and increased perioperative risk.
• Intervention should be considered for growth to greater than 3–4 cm or by greater than 0.4–0.5 cm/year while on active surveillance.
Surveillance protocols Surveillance protocols • A definite protocol for ‘active’ surveillance of SRMs has yet to be defined
• A suggested approach consists to alternate between US and cross-sectional (CT or magnetic resonance) imaging (some would argue that the inconsistency in size estimates using multiple modalities is a weakness of this approach)
• Imaging interval: every 3 months for 1 year, every 6 months for the second year, and annually thereafter
Lane B. et al. Curr Opin Urol 2012; 22: 353-59

AUA, 2009 ESMO, 2010 EAU, 2014 NCCN, 2014
• Recommended
in cT1a cases with major comorbidities and increased surgical risk
• Optional
in healthy patients with cT1a tumor
• Investigational
In all cases
• Grade A
Patients with small tumours and/or significant comorbidity who are unfit for surgery should be considered for an ablative approach
• Category 2A
AT can be considered for patients with cT1a renal lesions and who are not surgical candidates
Indications for Ablative Therapies

Oncological aim of ablative Oncological aim of ablative technologytechnology
• Ablative technology must be able to completly destroy all viable tissue, with no area of viable tissue left
• The surgeon must be able to monitor and precisely target the area to be ablated to assure complete tumour destrucion
• Low morbidity

Autorino R et al. Urol Oncol 2012; 30: 20-27Autorino R et al. Urol Oncol 2012; 30: 20-27

Mechanisms of CryoablationMechanisms of Cryoablation
Normal renal tissue(- 19.4 °C)
Renal tumour(- 40 °C)
Cryoablation approaches
• Laparoscopic Cryoablation Laparoscopic Cryoablation (LCA)(LCA)
- general anaesthesia mandatory- general anaesthesia mandatory
• Percutaneous Cryoablation Percutaneous Cryoablation (PCA)(PCA)
- MRI guided (reported under GA)- MRI guided (reported under GA) - CT guided (reported under sedation)- CT guided (reported under sedation)
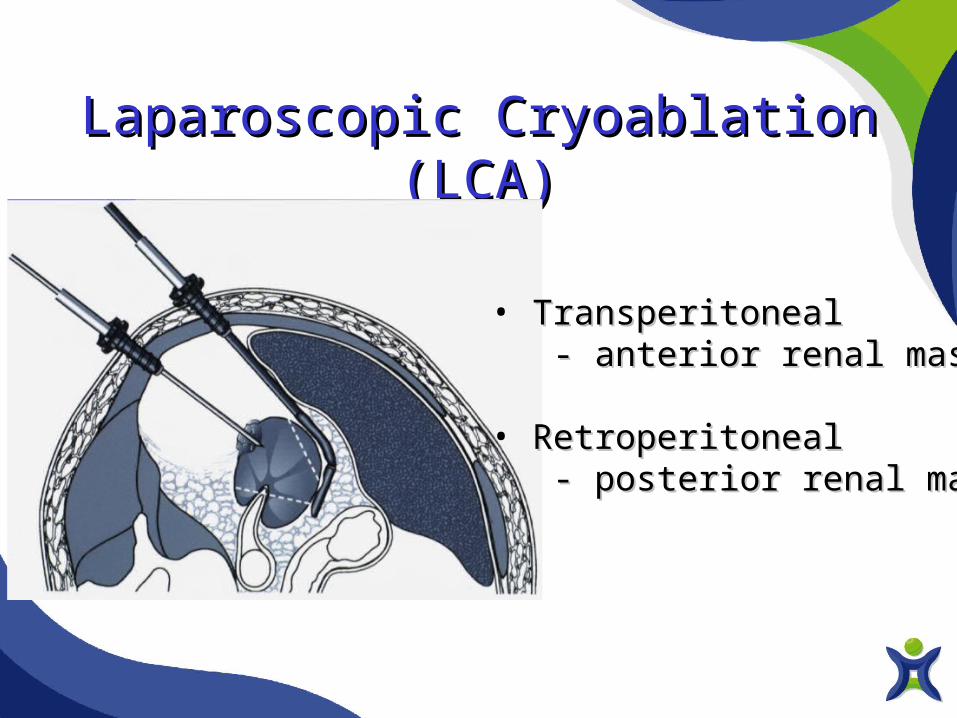
Laparoscopic Cryoablation (LCA)Laparoscopic Cryoablation (LCA)
• TransperitonealTransperitoneal - anterior renal mass- anterior renal mass
• RetroperitonealRetroperitoneal - posterior renal mass- posterior renal mass

Percutaneous Cryoablation (PCA)Percutaneous Cryoablation (PCA)
MRI guided CT guided

Cryoablation approaches
Mechanisms of Mechanisms of Radiofrequency Ablation (RFA)
• Heat based ablative techniqueHeat based ablative technique
• High-frequency alternating current High-frequency alternating current emitted through electrode placed within emitted through electrode placed within targeted tissuetargeted tissue
• T° > 60° C with denaturation of T° > 60° C with denaturation of proteins; melting of cell membranes, proteins; melting of cell membranes, loss of enzymatic function, destruction loss of enzymatic function, destruction of cytoplasmof cytoplasm

Radiofrequency Ablation (RFA): Approaches
• Laparoscopic Radiofrency Laparoscopic Radiofrency Ablation (LRFA)Ablation (LRFA)
- general anaesthesia mandatory- general anaesthesia mandatory
• Percutaneous Radiofrequency Percutaneous Radiofrequency Ablation (PRFA)Ablation (PRFA)
- MRI guided (reported under GA)- MRI guided (reported under GA) - CT guided (reported under sedation)- CT guided (reported under sedation)

RFA: Image guidance and ablation monitoring
• US: limited useUS: limited use
• CT: usedCT: used - limitation in the detection of residual - limitation in the detection of residual
tumour in the same sessiontumour in the same session
• MRI: currently the bestMRI: currently the best - allows re-treatment of residual - allows re-treatment of residual
tumour in the same sessiontumour in the same session
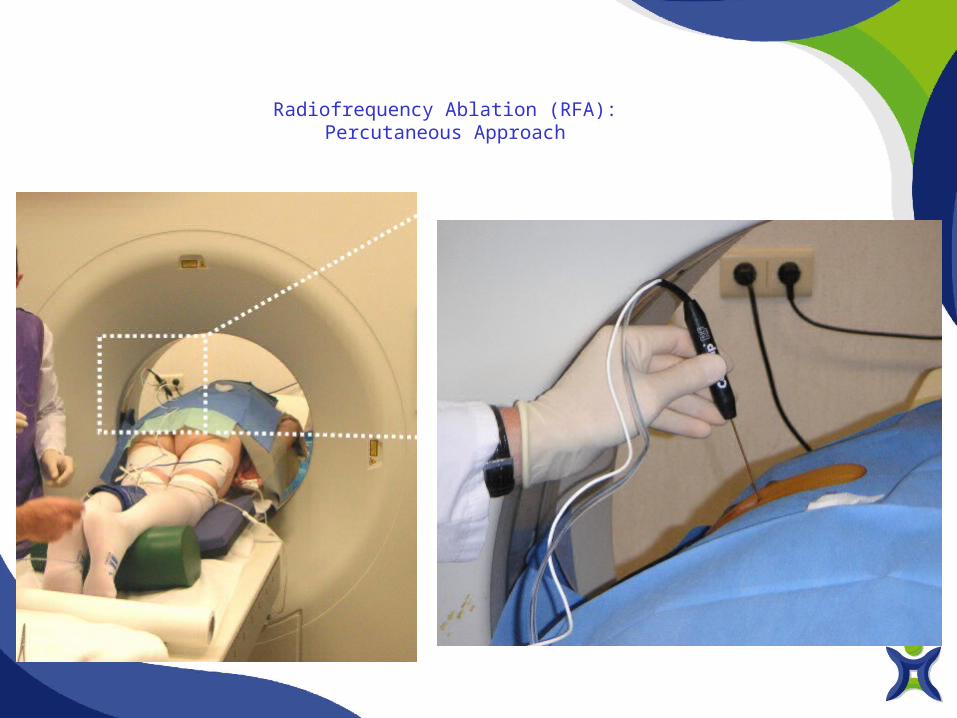
Radiofrequency Ablation (RFA): Percutaneous Approach
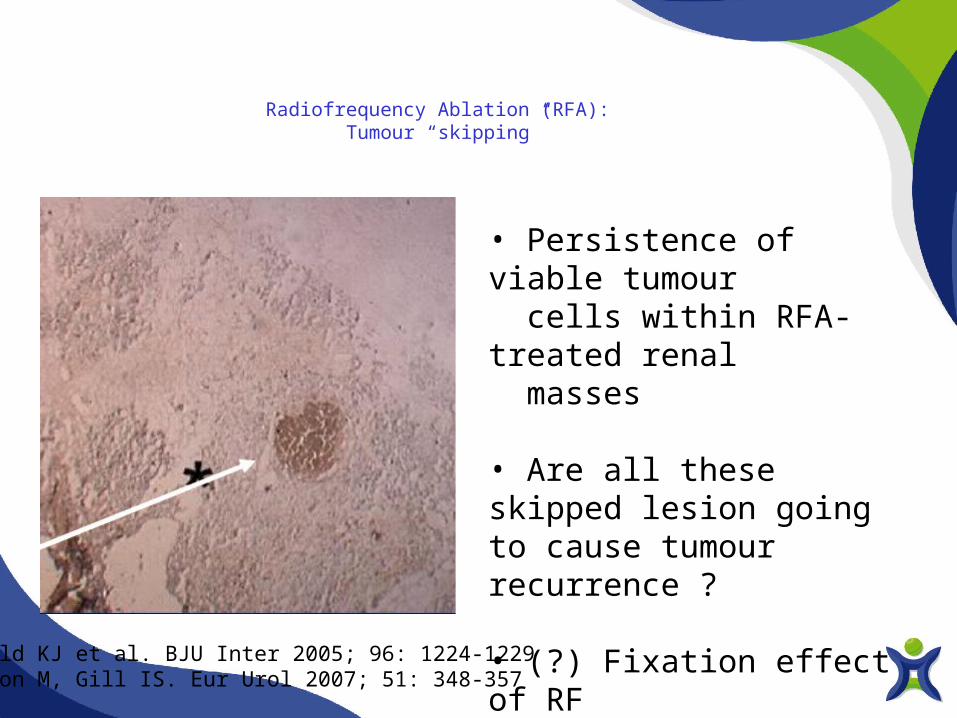
Radiofrequency Ablation (RFA): Tumour “skipping”
• Persistence of viable tumour cells within RFA-treated renal masses
• Are all these skipped lesion going to cause tumour recurrence ?
• (?) Fixation effect of RF energy
Weld KJ et al. BJU Inter 2005; 96: 1224-1229Aron M, Gill IS. Eur Urol 2007; 51: 348-357

Alternative Treatments: Follow-up and outcomes
Kunkle DA et al J Urol 2008; 179: 1227-1234
• Radiographic follow-up (CT scan or MRI) - enhancement on post-contrast imaging is considered evidence of incompletely treated disease - Grossly viable disease
• Percutaneous biopsies - viable tumour may be present despite a lack of radiographic enhancement - microscopic disease

Cryoablation: meta-analysis of case series studies (efficacy 89%)
El Dib C. et al. BJU Inter 2012; 110: 510-516El Dib C. et al. BJU Inter 2012; 110: 510-516
Successfully treated tumour was defined as no growth or no evidence of recurrence on CT scan or MRI
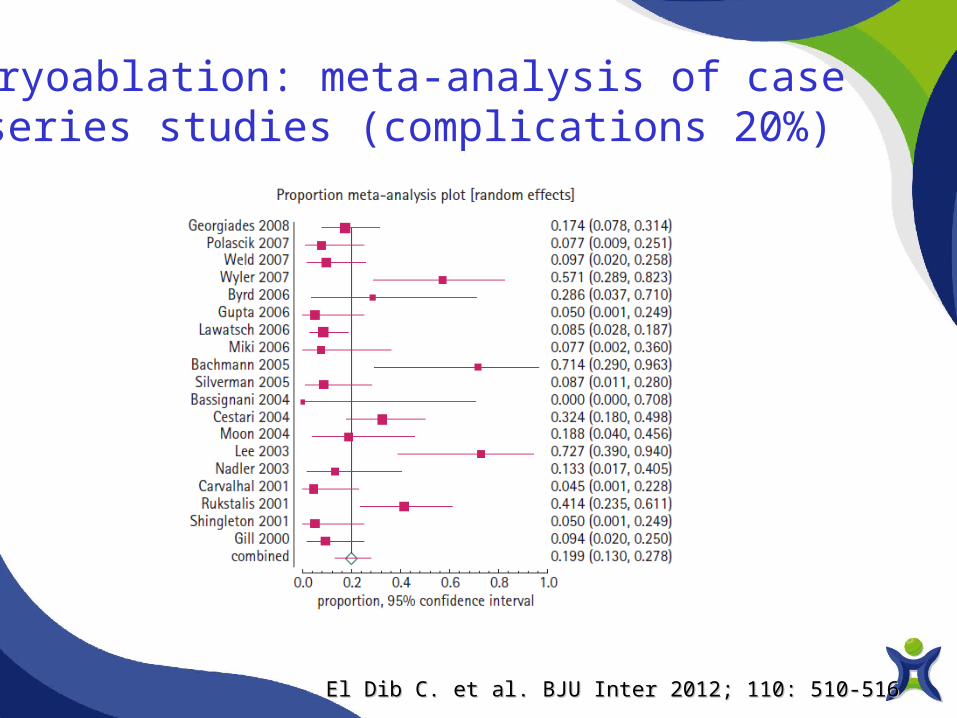
Cryoablation: meta-analysis of case series studies (complications 20%)
El Dib C. et al. BJU Inter 2012; 110: 510-516El Dib C. et al. BJU Inter 2012; 110: 510-516

Cryoablation: functional outcomes
Autorino R et al. Urol Oncol 2012; 30: 20-27Autorino R et al. Urol Oncol 2012; 30: 20-27
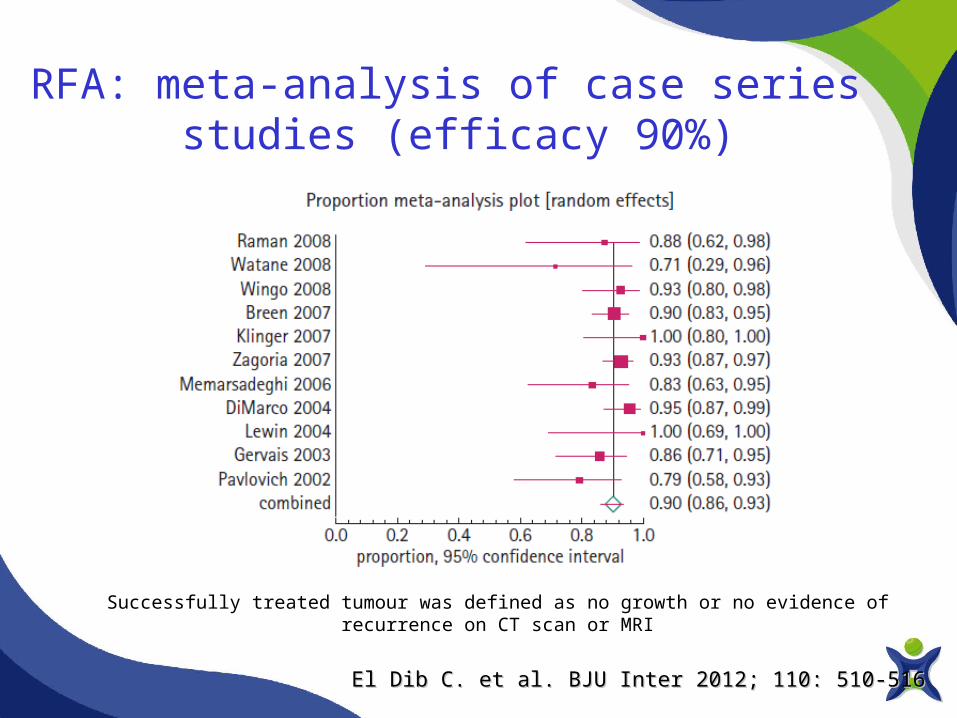
RFA: meta-analysis of case series studies (efficacy 90%)
El Dib C. et al. BJU Inter 2012; 110: 510-516El Dib C. et al. BJU Inter 2012; 110: 510-516
Successfully treated tumour was defined as no growth or no evidence of recurrence on CT scan or MRI
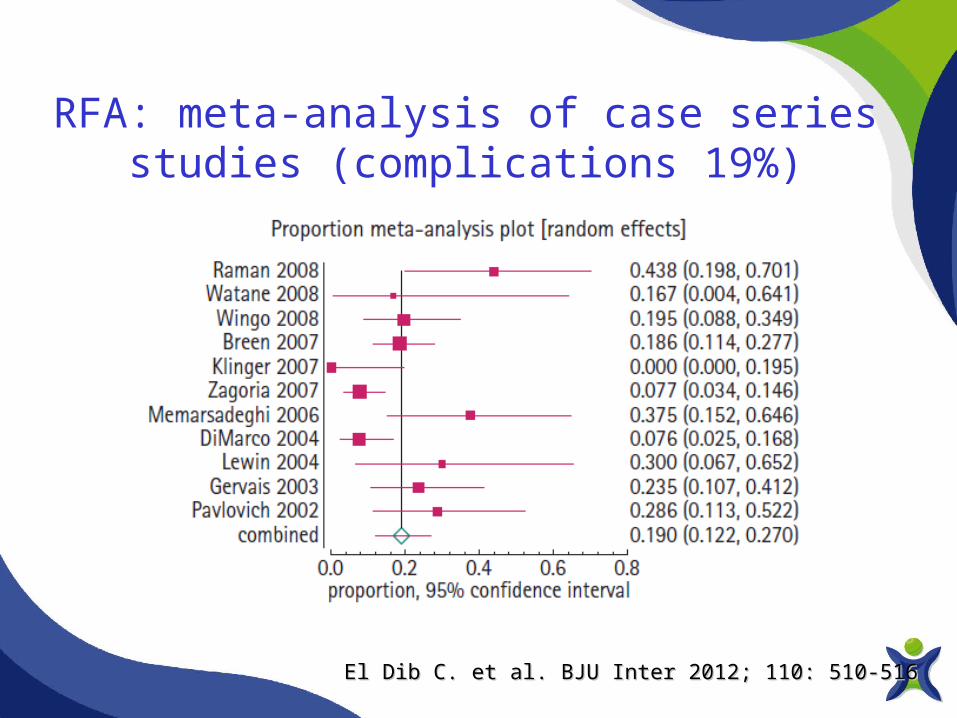
RFA: meta-analysis of case series studies (complications 19%)
El Dib C. et al. BJU Inter 2012; 110: 510-516El Dib C. et al. BJU Inter 2012; 110: 510-516
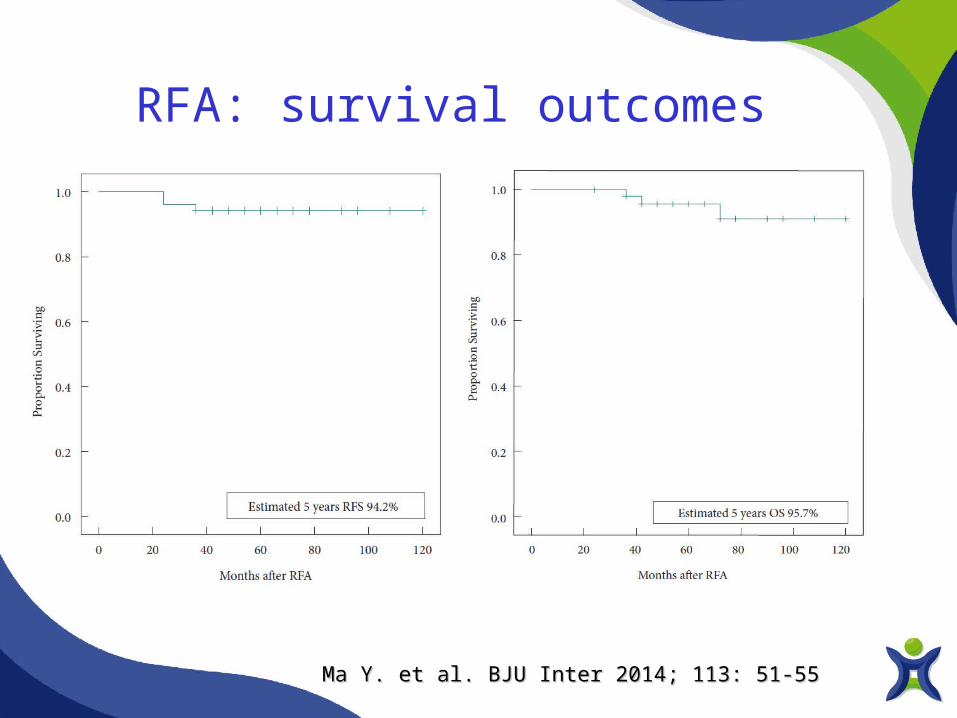
RFA: survival outcomes
Ma Y. et al. BJU Inter 2014; 113: 51-55Ma Y. et al. BJU Inter 2014; 113: 51-55

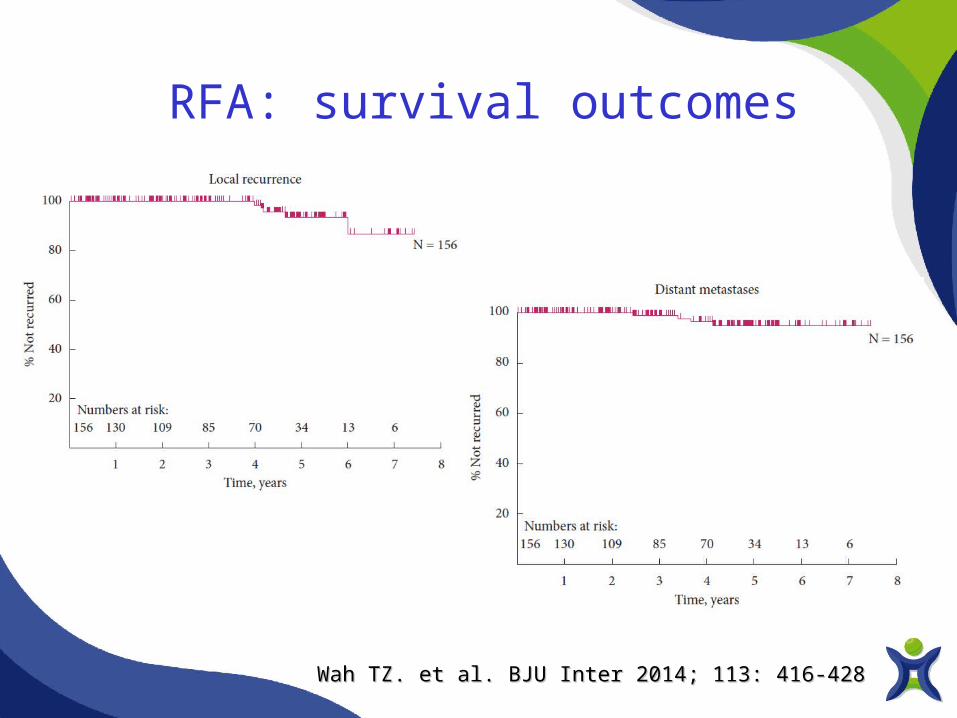
RFA: survival outcomes
Wah TZ. et al. BJU Inter 2014; 113: 416-428Wah TZ. et al. BJU Inter 2014; 113: 416-428
RFA: survival outcomes
Wah TZ. et al. BJU Inter 2014; 113: 416-428Wah TZ. et al. BJU Inter 2014; 113: 416-428

Alternative Treatments: Radiofrequency or Cryoablation
Kunkle DA et al J Urol 2008; 179: 1227-1234
Meta-Analysis of studies published between 1980 to 2006

Alternative Treatments: Radiofrequency or Cryoablation
Kunkle DA et al J Urol 2008; 179: 1227-1234
Meta-Analysis of studies published between 1980 to 2006

Alternative Treatments: Differences in clinical application
Kunkle DA et al J Urol 2008; 179: 1227-1234
60
66
67
68
56
58
60
62
64
66
68
70
NSS Cryoabl RFA AS
**
*p < 0.05
Patient’s age(Yrs) *

Alternative Treatments: Differences in clinical application
Kunkle DA et al J Urol 2008; 179: 1227-1234
3,4
2,5 2,6
3
0
0,5
1
1,5
2
2,5
3
3,5
4
NSS Cryoabl RFA AS
* *
*p < 0.05
Tumour size (cm)

Alternative Treatments: Differences in clinical application
Kunkle DA et al J Urol 2008; 179: 1227-1234
54
1816
33
0
10
20
30
40
50
60
NSS Cryoabl RFA AS
* *
*p < 0.05
Follow-up (months)
*
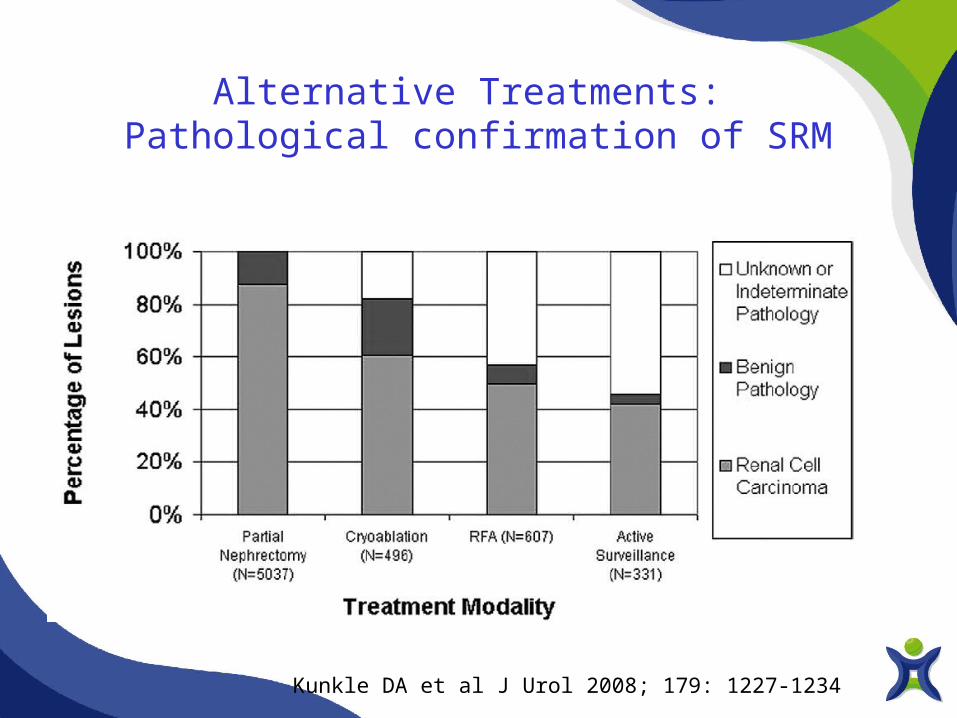
Alternative Treatments: Pathological confirmation of SRM
Kunkle DA et al J Urol 2008; 179: 1227-1234

Local recurrence-free survival
Campbell S et al J Urol 2009; 182: 1271-79
Statistically significant differences (p < 0.05): LPN, OPN, LRN, and ORN rates are statistically indistinguishable and are all significantly higher than Cryo and RFA rates; Cryo and RFA rates are statistically indistinguishable

AUA, 2009 ESMO, 2010 EAU, 2014 NCCN, 2014
• Recommended
in cT1a cases with major comorbidities and increased surgical risk
• Optional
in healthy patients with cT1a tumor
• Investigational
In all cases
• Grade A
Patients with small tumours and/or significant comorbidity who are unfit for surgery should be considered for an ablative approach
• Category 2A
AT can be considered for patients with cT1a renal lesions and who are not surgical candidates
Indications for Ablative Therapies