soluble flt-1 as a diagnostic mrker of preeclampsia 2008
TRANSCRIPT

7/26/2019 Soluble Flt-1 as a Diagnostic Mrker of Preeclampsia 2008
http://slidepdf.com/reader/full/soluble-flt-1-as-a-diagnostic-mrker-of-preeclampsia-2008 1/7
Australian and New Zealand Journal of Obstetrics and Gynaecology 2008; 48: 64–70 DOI: 10.1111/j.1479-828X.2007.00804.x
64 © 2008 The Authors
Journal compilation © 2008 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists
BlackwellPublishing Asia
Original Article
Soluble Flt-1 as a diagnostic marker of pre-eclampsia
Jane WOOLCOCK,1 Annemarie HENNESSY,2 Bei XU,3 Charlene THORNTON,2 Jane TOOHER,1
Angela MAKRIS4 and Robert OGLE1
1Department of Obstetrics and Gynecology, Royal Prince Alfred Hospital, Camperdown, New South Wales, 2School of Medicine, University
of Western Sydney, Penrith, New South Wales, 3Vascular Immunology Research Group, Heart Research Institute, Camperdown, New South
Wales, 4Department of Renal Medicine, Liverpool Hospital, Sydney, New South Wales, Australia
Backgound: Serum levels of soluble fms-like tyrosine kinase (sFlt-1) increase in pre-eclampsia (PE).
Aims: To determine whether concentrations of serum sFlt-1 can differentiate PE or superimposed PE (SPE)
from gestational hypertension (GH) or chronic hypertension (CH).
Methods: Blood was collected from pregnant women being investigated for hypertension (blood pressure of
> 140 and/or 90 mmHg). Normotensive (NP) and pre-eclamptic (PE-C) control ranges were measured.
Results: Patients with evolving hypertension in pregnancy eventually fell into four groups: GH (n = 14), PE
(n = 7), CH (n = 9) and SPE (n = 9). Patients who later developed pre-eclampsia had a higher sFlt-1 (PE:
2.61 ng/mL and SPE: 2.77 ng/mL, respectively) than GH (P < 0.001) or CH (1.05 ng/mL, P = 0.11). Women
with established PE at recruitment (PE-C; (n = 18) (3.13 ng/mL; interquartile range (IQR): 2.14–4.17 ng/mL)
had a median sFlt-1 higher than NP (n = 18) (0.47 ng/mL; IQR: 0.11–0.89) (P < 0.0008). Patients with GH
compared to NP had a slight increase (1.33 ng/mL, P < 0.003). Using a sFlt-1 cut-off of ≥ 1.9 ng/mL yielded
a sensitivity of 94% (95% confidence interval (CI) 73–100%) and specificity of 78% (95% CI 64–82%).
Conclusions: sFlt-1 was elevated in women with PE compared to NP. The sFlt-1 also differentiated women
destined to develop PE among those who presented with a diagnostic rise in maternal blood pressure. The
sFlt-1 test is a useful diagnostic test for PE.
Key words: diagnostic, hypertension, pre-eclampsia, pregnancy, sflt-1.
Background
Pre-eclampsia affects around 5% of pregnancies
causing substantial maternal and fetal morbidity and
mortality,1 although the aetiology and pathogenesis of
pre-eclampsia remain largely unknown. It has been
hypothesised that the initial cause is abnormal
implantation of the placenta resulting in impaired
placental blood flow.1 The hypoxic placenta releases
soluble factors into the maternal circulation, which
induces systemic endothelial dysfunction. This gives
rise to the clinical features of hypertension, proteinuria,
oedema and coagulation abnormalities.1
The circulating factor or factors secreted by the
placenta that are responsible for the widespread
endothelial dysfunction in pre-eclampsia have been
difficult to elucidate despite extensive efforts. Maynard
et al . and others discovered the placenta of pregnant
women with pre-eclampsia produced increased levels
of soluble fms-like tyrosine kinase 1 receptor (sFlt-1).2,3
They also demonstrated that exogenous sFlt-1
administered to pregnant rats produces hypertension,
proteinuria and histological glomeruloendotheliosis,
which are all features of human pre-eclampsia.
Makris et al . have recently proved that elevated sFlt-1
is caused by placental ischaemia.4
sFlt-1 acts by binding to the receptor binding
domains of vascular endothelial growth factor (VEGF)
and placental growth factor (PlGF), another member
Correspondence: Professor Annemarie Hennessy,
University of Western Sydney, Locked Bag 1797,
Penrith South DC, NSW 1797, USA.
Email: [email protected]
This research was undertaken under the auspices of a
grant provided by the ANZCOG.
Received 01 June 2007; accepted 07 November 2007.

7/26/2019 Soluble Flt-1 as a Diagnostic Mrker of Preeclampsia 2008
http://slidepdf.com/reader/full/soluble-flt-1-as-a-diagnostic-mrker-of-preeclampsia-2008 2/7
sFlt-1 as a diagnostic marker of pre-eclampsia
© 2008 The Authors 65
Journal compilation © 2008 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists; 48: 64–70
of the VEGF family that is made predominantly by
the placanta.2 VEGF is known to have potent
angiogenic properties and also promotes vasodilation.5
VEGF exerts its biological effects through Flt-1, a
membrane-bound receptor tyrosine kinase. sFlt-1 is
the soluble secreted variant of this receptor which
lacks the transmembrane and cytoplasmic domains
and antagonises VEGF and PlGF.6 Increased levels of
sFlt-1 in the maternal circulation will therefore result
in reduced levels of free VEGF and free PlGF, creating
an antiangiogenic state that may be responsible for
the hypertension and proteinuria of pre-eclampsia.2
Levine et al . demonstrated that increased levels
of sFlt-1 and reduced levels of PlGF predict the
development of pre-eclampsia up to five weeks
before the onset of clinical symptoms in stored
blood samples.7
This study aimed to determine if sFlt-1 levels at
the time of first elevation in blood pressure could be
used to differentiate pre-eclampsia from gestational
hypertension (GH) and escalating chronichypertension (CH). Women who have CH develop
pre-eclampsia with increased frequency and severity
and it is often difficult to diagnose pre-eclampsia
due to the similarity of signs.8 An accurate diagnostic
test for pre-eclampsia would be especially useful
for this group of patients. We hypothesised that sFlt-1
would be elevated in patients who were subsequently
proven on clinical grounds to have progressed to
pre-eclampsia.
Methods
Patients were selected prospectively from ward or
delivery suite admissions, day stay assessment or
antenatal clinic at Royal Prince Alfred Women and
Babies, a large teaching hospital in Sydney, Australia.
Subjects were recruited consecutively by a single
clinician. Patients were being investigated for a new
rise in blood pressure (systolic blood pressure of
≥ 140 mmHg or diastolic blood pressure of ≥ 90 mmHg
on at least two occasions > 4 h apart). They were
assessed in four groups according to their final
diagnosis: GH (n = 14), pre-eclampsia (n = 7), CH
(n = 9), and superimposed pre-eclampsia (SPE,
n = 9). Data were established for normotensive
controls (NP, n = 18) and women with pre-eclampsia
at presentation (pre-eclampsia controls: PE-C,
n = 18). Results for CH and gestational hypertension
were also compared to NP.
Pre-eclampsia was defined as hypertension with
at least one other feature of pre-eclampsia. These
included proteinuria (one dipstick measurement
≥ 2+ or ≥ 300 mg in a 24-h urine collection), reduced
platelet count < 150 × 109/L, elevated liver function
tests (alanine aminotransferase > 35 iu/L) or birthweight
below the third centile, according to the classification
system of the Australasian Society for the Study of
Hypertension in Pregnancy (ASSHP).8 Chronic
hypertension was defined as blood pressure requiring
treatment with antihypertensive medication outside
pregnancy or an antenatal blood pressure at less than
20 weeks gestation of ≥ 140/90 mmHg on more than
two occasions at least four hours apart which was
treated and controlled to below 140/90 prior to
inclusion in the study. A final diagnosis was made
post-partum as to whether patients had developed
additional defining features of pre-eclampsia.
Normotensive controls were matched by age
(within two years) and gestation (within one week) to
control patients with pre-eclampsia, that is, patients
with pre-eclampsia at the time of recruitment. Normal
pregnancies were not complicated by medical or
obstetric complications and delivered an infant of greater than 2500 g at term. Pre-eclampsia controls
had diagnostic features of pre-eclampsia, as described
above at the time of presentation.
All women provided written informed consent
prior to collection of serum samples, which were
collected between March 2005 and January 2006.
This study was approved by the Ethics Committee of
Royal Prince Alfred Hospital in accordance with
National Health and Medical Research Council
Guidelines for Human Research.
Venepuncture, using an 18-gauge needle and
vacutainer system at the cubital fossa, was performedat the time of recruitment and blood collected into
tubes containing EDTA. The samples were centrifuged
within four hours of collection and the serum stored
at –70°C. The concentrations of sFlt-1 were measured
with the use of enzyme-linked immunosorbent assay
(ELISA) from BD (San Jose, CA, USA) by a single
operator. The person who performed the assay was
blinded to the clinical diagnoses of the patients. All
measurements were made in duplicate on 1:2 dilution
of the sera. The microtitre plates were read with a
programmable spectrophotometer.
Data were analysed using Minitab 10, utilising
Kruskal–Wallis and Mann–Whitney tests for non-
parametric data. Data are presented as medians and
interquartile ranges. Significance was assumed for a
P -value of < 0.05. Sensitivity, specificity, positive
predictive value, negative predictive value, positive
likelihood ratio and negative likelihood ratio were
calculated using an arbitrary cut-off of serum sFlt-1
at 1.9 ng/mL.
7/26/2019 Soluble Flt-1 as a Diagnostic Mrker of Preeclampsia 2008
http://slidepdf.com/reader/full/soluble-flt-1-as-a-diagnostic-mrker-of-preeclampsia-2008 3/7
J. Woolcock et al .
66 © 2008 The Authors
Journal compilation © 2008 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists; 48: 64–70
Results
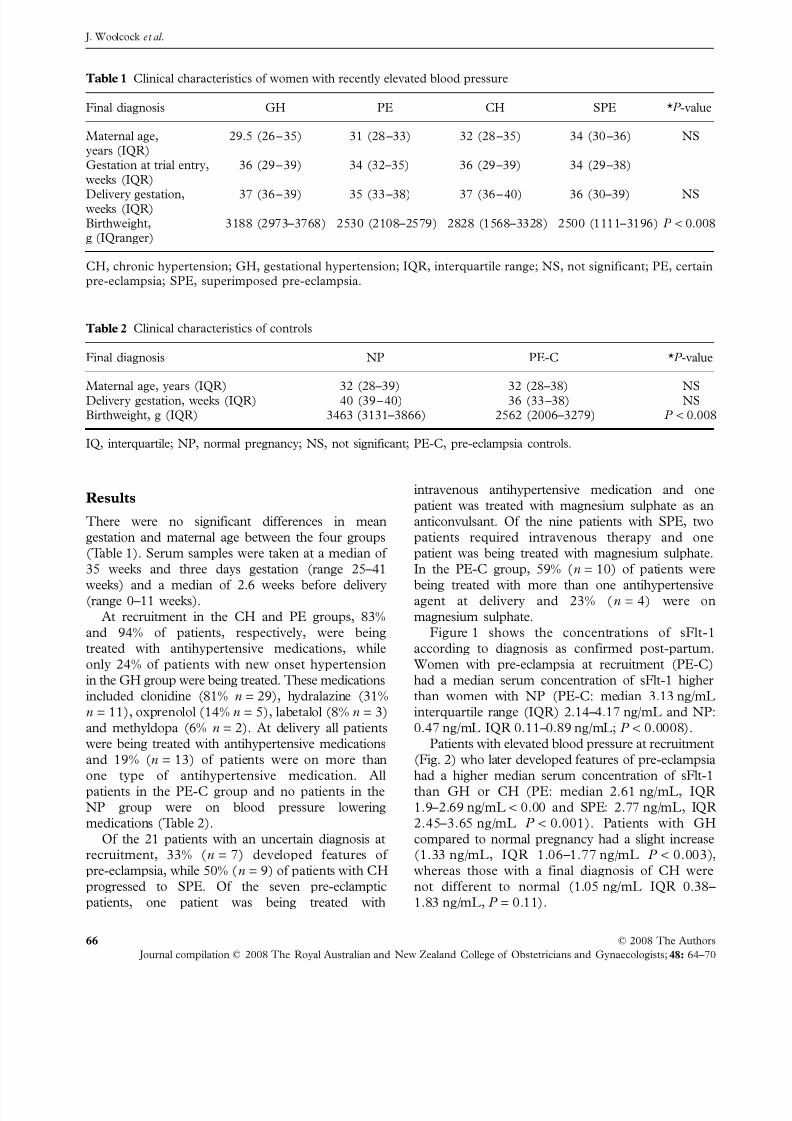
There were no significant differences in mean
gestation and maternal age between the four groups
(Table 1). Serum samples were taken at a median of
35 weeks and three days gestation (range 25–41
weeks) and a median of 2.6 weeks before delivery(range 0–11 weeks).
At recruitment in the CH and PE groups, 83%
and 94% of patients, respectively, were being
treated with antihypertensive medications, while
only 24% of patients with new onset hypertension
in the GH group were being treated. These medications
included clonidine (81% n = 29), hydralazine (31%
n = 11), oxprenolol (14% n = 5), labetalol (8% n = 3)
and methyldopa (6% n = 2). At delivery all patients
were being treated with antihypertensive medications
and 19% (n = 13) of patients were on more than
one type of antihypertensive medication. All
patients in the PE-C group and no patients in the
NP group were on blood pressure lowering
medications (Table 2).
Of the 21 patients with an uncertain diagnosis at
recruitment, 33% (n = 7) developed features of
pre-eclampsia, while 50% (n = 9) of patients with CH
progressed to SPE. Of the seven pre-eclamptic
patients, one patient was being treated with
intravenous antihypertensive medication and one
patient was treated with magnesium sulphate as an
anticonvulsant. Of the nine patients with SPE, two
patients required intravenous therapy and one
patient was being treated with magnesium sulphate.
In the PE-C group, 59% (n = 10) of patients were
being treated with more than one antihypertensiveagent at delivery and 23% (n = 4) were on
magnesium sulphate.
Figure 1 shows the concentrations of sFlt-1
according to diagnosis as confirmed post-partum.
Women with pre-eclampsia at recruitment (PE-C)
had a median serum concentration of sFlt-1 higher
than women with NP (PE-C: median 3.13 ng/mL
interquartile range (IQR) 2.14–4.17 ng/mL and NP:
0.47 ng/mL IQR 0.11–0.89 ng/mL; P < 0.0008).
Patients with elevated blood pressure at recruitment
(Fig. 2) who later developed features of pre-eclampsia
had a higher median serum concentration of sFlt-1
than GH or CH (PE: median 2.61 ng/mL, IQR
1.9–2.69 ng/mL < 0.00 and SPE: 2.77 ng/mL, IQR
2.45–3.65 ng/mL P < 0.001). Patients with GH
compared to normal pregnancy had a slight increase
(1.33 ng/mL, IQR 1.06–1.77 ng/mL P < 0.003),
whereas those with a final diagnosis of CH were
not different to normal (1.05 ng/mL IQR 0.38–
1.83 ng/mL, P = 0.11).
Table 1 Clinical characteristics of women with recently elevated blood pressure
Final diagnosis GH PE CH SPE *P -value
Maternal age,
years (IQR)
29.5 (26–35) 31 (28–33) 32 (28–35) 34 (30–36) NS
Gestation at trial entry,
weeks (IQR)
36 (29–39) 34 (32–35) 36 (29–39) 34 (29–38)
Delivery gestation,weeks (IQR)
37 (36–39) 35 (33–38) 37 (36–40) 36 (30–39) NS
Birthweight,
g (IQranger)
3188 (2973–3768) 2530 (2108–2579) 2828 (1568–3328) 2500 (1111–3196) P < 0.008
CH, chronic hypertension; GH, gestational hypertension; IQR, interquartile range; NS, not significant; PE, certain
pre-eclampsia; SPE, superimposed pre-eclampsia.
Table 2 Clinical characteristics of controls
Final diagnosis NP PE-C *P -value
Maternal age, years (IQR) 32 (28–39) 32 (28–38) NS
Delivery gestation, weeks (IQR) 40 (39–40) 36 (33–38) NS
Birthweight, g (IQR) 3463 (3131–3866) 2562 (2006–3279) P < 0.008
IQ, interquartile; NP, normal pregnancy; NS, not significant; PE-C, pre-eclampsia controls.

7/26/2019 Soluble Flt-1 as a Diagnostic Mrker of Preeclampsia 2008
http://slidepdf.com/reader/full/soluble-flt-1-as-a-diagnostic-mrker-of-preeclampsia-2008 4/7
sFlt-1 as a diagnostic marker of pre-eclampsia
© 2008 The Authors 67
Journal compilation © 2008 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists; 48: 64–70
Using a sFlt-1 cut-off of ≥ 1.9 ng/mL this test yielded
a sensitivity of 94% (95% confidence interval (CI)
73–100%) and specificity of 78% (95% CI 64–82%).
Of the 16 women who developed pre-eclampsia after
recruitment, nine (56%) had an elevated sFlt-1 level,
≥ 1.9 ng/mL, up to eight weeks before the onset of
pre-eclampsia. The positive likelihood ratio for this test
is 4.3 (95% CI 1.762–8.553) and the negative likelihood
ratio is 0.08 (95% CI 0.018–0.540) (Table 3).
There were five patients included in the data
analysis with particularly high levels of sFlt-1 at
recruitment. These values were 7.34, 5.45, 5.16, 4.82and 4.78 ng/mL. These patients all had evidence of
severe disease. All five patients were being treated
with intravenous antihypertensive therapy for blood
pressure ≥ 170/110 and four women were being treated
with magnesium sulphate at delivery. All five babies
were delivered prematurely at 28, 31, 33, 34 and 35
weeks gestation because of worsening pre-eclampsia.
Discussion
Our findings confirm that the maternal serum sFlt-1
concentration is markedly increased in women withpre-eclampsia when compared with controls. We
have also shown that in women with a new onset
rise in blood pressure, serum sFlt-1 concentrations
can ‘diagnose’ pre-eclampsia a maximum of eight
weeks before the onset of additional clinically
defining features. This study has also found that very
high levels of sFlt-1 were present in patients with
severe pre-eclampsia.
This study extends prior observations by
examining serum sFlt-1 concentrations in patients
with CH. Our data show that sFlt-1 levels may be a
useful test for this group of women at high risk of
developing SPE.
No single test exists to identify which women with
new onset ‘gestational’ hypertension or escalating
CH will develop pre-eclampsia. Serum uric acid
concentration has been suggested as one of the most
sensitive indicators of pre-eclampsia.9 Decreased
renal tubular excretion is the most likely mechanism
for uric acid being increased in pre-eclampsia.10,11
Figure 1 Serum sFlt-1 concentrations in normal
pregnancy and in patients with pre-eclampsia at
presentation. Individual patient data; median and
interquartile ranges shown. **P < 0.001 compared to
normal pregnancy.
Figure 2 Serum sFlt-1 concentrations at the time of
recent elevation in blood pressure according to final
diagnosis. Individual patient data; median and interquartile
ranges shown. **P < 0.001 compared to gestational
hypertension and chronic hypertension.
Table 3 Serum sFlt-1 as a diagnostic marker for
pre-eclampsia for sFlt-1 concentration ≥ 1.9 ng/mL
95% CI
Sensitivity 94% 73–100%
Specificity 78% 64–82%
Positive predictive value 75% 59–80%
Negative predictive value 95% 77–100%Positive likelihood ratio 4.3 1.97–9.46
Negative likelihood ratio 0.08 0.018–0.540
CI, confidence interval.

7/26/2019 Soluble Flt-1 as a Diagnostic Mrker of Preeclampsia 2008
http://slidepdf.com/reader/full/soluble-flt-1-as-a-diagnostic-mrker-of-preeclampsia-2008 5/7
J. Woolcock et al .
68 © 2008 The Authors
Journal compilation © 2008 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists; 48: 64–70
Oxidative stress may also give rise to the hyper-
uricaemia seen in pre-eclampsia.12 Serum uric acid
levels used for the diagnosis of pre-eclampsia gave a
sensitivity of 69% and specificity of 51% with a cut-off
of 0.33 mmol/L.13 There may be some correlation
between elevated serum uric acid levels and both the
severity of pre-eclampsia and the neonatal morbidity.14–16
The clinical utility of serum uric acid values in
differentiating various hypertensive diseases of
pregnancy, however, appears to be limited.17
Serum creatinine levels have also been used to help
confirm a diagnosis of pre-eclampsia. A level greater
then 106 µmol/L in pregnancy supports the diagnosis
of pre-eclampsia;18 however, levels may not help
differentiate CH because of underlying renal disease.9
Some investigators have retrospectively looked at
the usefulness of Down syndrome screening markers
for the prediction of pre-eclampsia. Second trimester
serum levels of alpha-fetoprotein (AFP), human
chorionic gonadotrophin (hCG), unconjugated estriol
(uE3) and inhibin A (inh A) have been usedindividually and in combination for risk assessment of
pre-eclampsia. The most promising of these markers
seems to be inh A, which has been reported to be
significantly increased in the second trimester in
women destined to develop pre-eclampsia with a
sensitivity of up to 48% for a specificity of 90%.19 inhA
may be useful for the prediction of pre-eclampsia
as early as ten weeks gestation;20 however, levels
appear to be more markedly increased closer to
disease onset in pre-eclamptic women.21 In a small
study, Wald et al . reported that combining the values
of inh A, hCG and uE3 from second trimestermaternal screening would detect women who would
subsequently develop pre-eclampsia in their pregnancy
with a sensitivity of 55% and specificity of 95%.22
Second trimester serum markers combined with
other maternal indices show greater predictive value.
For example maternal age, body mass index and
parity with free βhCG predicted 70% of women who
developed pre-eclampsia with a specificity of 71%.23
inh A with Doppler ultrasound predicted 71% of
cases of pre-eclampsia with a specificity of 93%.24
Longitudinal blood sampling has shown that
leptin concentrations are increased in established
pre-eclampsia, as well as before pre-eclampsia is
clinically evident from 20 weeks gestation until delivery.25
Serum leptin and placental growth factor in combination
have been used as a screening test for pre-eclampsia
at 24 weeks gestation with reported sensitivity of 67%
for a specificity of 100%. These authors also showed
a decrease in insulin-like growth factor binding
factor-1 prior to the onset of pre-eclampsia.26
Fibronectin levels, a marker of endothelial
dysfunction, are elevated up to four weeks before the
onset of pre-eclampsia.27,28 A longitudinal study of
378 women showed as early as nine to 12 weeks of
gestation, there was a difference in fibronectin levels
between women who developed pre-eclampsia in their
pregnancy and controls. At 22–26 weeks gestation the
sensitivity of fibronectin for predicting pre-eclampsia
was 73% with a specificity of 87%.29
Similarities between pre-eclampsia and insulin
resistance syndrome have led to theories that
measurements of glucose tolerance and insulin resistance
may predict pre-eclampsia. A recent study has shown
that fasting insulin sensitivity indexes can predict in
early (16–20 weeks) and late (26–30 weeks) pregnancy
the subsequent development of pre-eclampsia with a
sensitivity of 85% and 88%, respectively, for a
specificity of 97%.30
Placental sFlt-1 has been implicated as being
involved in the pathophysiology of pre-eclampsia
by disrupting maternal endothelial cell functionthrough antagonism of VEGF. sFlt-1 concentrations
in pre-eclamptic women were more than threefold
over the control which helps to confirm this hypothesis.
The findings of this study are consistent with
previous studies which have also found elevated
concentrations of sFlt-1 in patients with pre-eclampsia
at the time of diagnosis.2,31,32 A longitudinal study of
eight women who developed pre-eclampsia, six with
hypertension only (four CH and two gestational
hypertension) and nine with normal pregnancy showed
that sFlt-1 was significantly higher at 25–28 weeks in
women who developed pre-eclampsia compared towomen with hypertension alone or normal pregnancy.
The group with hypertension alone appeared not to
have substantially higher levels than women with
normal pregnancy.33
A larger longitudinal analysis of serum sFlt-1
concentrations in normal pregnancy and pre-
eclampsia showed that sFlt-1 levels were increased
only within five weeks before the onset of hypertension
and proteinuria.7
Pre-eclampsia causes significant morbidity and
methods for early identification and streamlined
management of women destined to develop pre-
eclampsia are needed urgently. In this cohort of women
there was a clear elevation in sFlt-1 at presentation
with pre-eclampsia compared to normotensive controls.
The sFlt-1 concentration also differentiated women
destined to develop pre-eclampsia from those with
CH and those who had presented with a diagnostic
rise in maternal blood pressure with no other feature
of pre-eclampsia (gestational hypertension).

7/26/2019 Soluble Flt-1 as a Diagnostic Mrker of Preeclampsia 2008
http://slidepdf.com/reader/full/soluble-flt-1-as-a-diagnostic-mrker-of-preeclampsia-2008 6/7
sFlt-1 as a diagnostic marker of pre-eclampsia
© 2008 The Authors 69
Journal compilation © 2008 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists; 48: 64–70
This test has important clinical utility as it targets
patients at high risk of developing pre-eclampsia, that
is, those women with uncertainty in their diagnosis.
Serum sFlt-1 measurements could be used to guide
important management decisions regarding whether
or not admission to hospital is required, closer
monitoring in a day-stay unit or consideration of
delivery. To reduce the risks that are associated with
the development of severe pre-eclampsia, early detection
and timely assessment of the disease are essential.
Serum sFlt-1 appears to be a useful tool as a one-off
test in the third trimester for patients with clinical
uncertainty of the cause of hypertension in pregnancy.
References
1 Roberts J, Lain K. Recent insights into the
pathogenesis of preeclampsia. Placenta 2002; 23:
359–372.
2 Maynard S, Min J, Merchan J et al . Excess
placental soluble fms-like tyrosine kinase 1 (sFlt1)may contribute to endothelial dysfunction, hypertension
and proteinuria in preeclampsia. J Clin Invest 2003;
111: 649–658.
3 Zhou Y, McMaster M, Woo K et al . Vascular
endothelial growth factor ligands and receptors that
regulate human cytotrophoblast survival are
dysregulated in severe preeclampsia and hemolysis,
elevated liver enzymes and low platelets syndrome. Am J Pathol 2002; 160: 1405–1423.
4 Makris A, Thornton C, Thompson J et al .
Uteroplacental ischemia results in proteinuric
hypertension and elevated sFLT-1. Kidney Int 2007:
Epub Mar 21.5 He H, Venema VJ, Gu X, Venema RC, Marrero MB,
Caldwell RB. Vascular endothelial growth factor
signals endothelial cell production of nitric oxide and
prostacyclin through Flk-1/KDR activation of c-Src. J Biol Chem 1999; 274: 25130–25135.
6 Shibuya M. Structure and function of VEGF/VEGF-
receptor system involved in angiogenesis. Cell Struct
Funct 2001; 26: 25–35.
7 Levine R., Maynard S, Qian C et al . Circulating
angiogenic factors and the risk of preeclampsia. N
Engl J Med 2004; 350: 672–683.
8 Brown MA, Hague WM, Higgins J et al . Australasian
Society for the Study of Hypertension in Pregnancy.
The detection, investigation and management of hypertension in pregnancy: Executive summary.
Aust N Z J Obstet Gynaecol 2000; 40: 133–138.
9 Roberts J. Pregnancy-related hypertension. In: Creasy
R, Resnick R, eds. Maternal-Fetal Medicine, 4th edn.
Philadelphia, PA: W.B. Saunders Company, 1999;
833–871.
10 Chesley L, Williams L. Renal glomerular and
tubular function in relation to the hyperuricaemia of
preeclampsia and eclampsia. Am J Obstet Gynecol
1945; 50: 367–375.
11 Boyle J, Campbell S, Duncan A. Serum uric acid
levels in normal pregnancy with observations on the
renal excretion of urate in pregnancy. J Clin Pathol
1966; 19: 501–503.
12 Many A, Hubel C, Roberts J. Hyperuricaemia and
xanthine oxidase in preeclampsia, revisited. Am J
Obstet Gynecol 1996; 174: 288–291.13 Shuster E, Weppelman B. Plasma urate measurements
and fetal outcome in preeclampsia. Gynecol Obstet
Invest 1981; 12: 162.
14 Acien P, Lloret G, Lloret M. Perinatal morbidity
and mortality in pregnancy hypertensive disorders:
Prognostic value of the clinical and laboratory
findings. Int J Gynaecol Obstet 1990; 32: 229–235.
15 Redman C, Beilin L, Bonnar J, Wilkinson R.
Plasma-urate measurements in predicting fetal death
in hypertensive pregnancy. Lancet 1976; 1: 1370–1373.
16 Sagen N, Kjell H, Nilsen S. Serum urate as a
predictor of fetal outcome in severe preeclampsia. Acta Obstet Gynecol Scand 1984; 63: 71–75.
17 Lim K, Friedman S, Ecker J, Kao L, Kilpatrick S.The clinical utility of serum uric acid measurements
in hypertensive diseases of pregnancy. Am J Obstet
Gynecol 1998; 178: 1067–1071.
18 Report of the National High Blood Pressure Education
Program Working Group on High Blood Pressure in
Pregnancy. Am J Obstet Gynecol 2000; 183: S1–S22.
19 Aquilina J, Barnett A, Thompson O, Harrington K.
Second-trimester maternal serum inhibin A
concentration as an early marker for preeclampsia. Am J Obstet Gynecol 1999; 181: 131–136.
20 Sebire N, Roberts L, Noble P, Wallace E, Nicolaides
KH. Raised maternal serum inhibin A concentration
at 10–14 weeks of gestation is associated withpreeclampsia. Br J Obstet Gynaecol 2000; 107: 795–797.
21 Lambert-Messerlain G, Silver H, Petraglia F et al .
Second trimester levels of maternal serum human
chorionic gonadotrophin and inhibin A as predictors
of preeclampsia in the third trimester of pregnancy. J
Soc Gynecol Invest 2000; 7: 170–174.
22 Wald N, Morris J. Multiple marker second trimester
serum screening for preeclampsia. J Med Screen 2001;
8: 65–68.
23 Lee L, Sheu B, Shau W et al . Mid-trimester β-hCG
levels incorporated in a multifactorial model for
prediction of severe preeclampsia. Prenat Diagn 2000;
20: 738–743.
24 Aquilina J, Thompson O, Thilaganathan B,Harrington K. Improved early prediction of
preeclampsia by combining second-trimester maternal
serum inhibin-A and uterine artery Doppler.Ultrasound Obstet Gynecol 2001; 17: 477–484.
25 Anim-Nyame N, Sooranna S, Steer P, Johnson MR.
Longitudinal analysis of maternal plasma leptin
concentrations during normal pregnancy and
preeclampsia. Hum Reprod 2000; 15: 2033–2036.

7/26/2019 Soluble Flt-1 as a Diagnostic Mrker of Preeclampsia 2008
http://slidepdf.com/reader/full/soluble-flt-1-as-a-diagnostic-mrker-of-preeclampsia-2008 7/7
J. Woolcock et al .
70 © 2008 The Authors
Journal compilation © 2008 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists; 48: 64–70
26 Anim-Nyame N, Hills FA, Sooranna SR, Steer PJ,
Johnson MR. A longitudinal study of maternal plasma
insulin-like growth factor binding protein-1
concentrations during normal pregnancy and
pregnancies complicated by pre-eclampsia. Hum
Reprod 2000; 15: 2215–2219.
27 Ballegeer V, Spitz B, Kieckens L, Moreau H, Van
Assche A, Collen D. Predictive value of increased
plasma levels of fibronectin in gestational hypertension. Am J Obstet Gynecol 1989; 161: 432–436.
28 Lazarchik J, Stubbs T, Romein L, Van Dorsten JP,
Loadholt CB. Predictive value of fibronectin levels
in normotensive gravid women destined to become
preeclamptic. Am J Obstet Gynecol 1986; 154:
1050–1052.
29 Chavarria M, Lara-Gonzalez L, Gonzalez-Gleason A,
Sojo I, Reyes A. Maternal plasma cellular fibronectin
concentrations in normal and preeclamptic pregnancies:
A longitudinal study for early prediction of
preeclampsia. Am J Obstet Gynecol 2002; 187: 595–601.
30 Parretti E, Lapolla A, Dalfra M et al . Preeclampsia in
lean normotensive normotolerant pregnant women
can be predicted by simple insulin sensitivity indexes.Hypertension 2006; 47: 449–453.
31 Koga K, Osuga Y, Yoshino O et al . Elevated serum
soluble vascular endothelial growth factor receptor 1
(sVEGFR-1) levels in women with preeclampsia. J Clin Endocrinol Metab 2003; 88: 2348–2351.
32 Chaiworapongsa T, Romero R, Espinoza J et al .Evidence supporting a role for blockade of the
vascular endothelial growth factor system in the
pathophysiology of preeclampsia. Am J Obstet Gynecol
2004; 190: 1541–1547.
33 Hertig A, Berkane N, Lefevre G et al . Maternal
serum sFlt1 concentration is an early and reliable
predictive marker of preeclampsia. Clin Chem 2004;
50: 1702–1703.
34 Levine R, Maynard S, Qian C et al . Circulating
angiogenic factors and the risk of preeclampsia. N
Engl J Med 2004; 350: 672–683.