socio-economic determinants of bedsharing in a population-based survey of new oregon mothers:...
Post on 21-Dec-2015
214 views
TRANSCRIPT

Socio-economic determinants of bedsharing in a population-based survey
of new Oregon mothers:Analysis of the 1998-1999 Oregon PRAMS Dataset
Martin B. Lahr, M.D., M.P.H.*Kenneth D. Rosenberg, M.D., M.P.H. †‡
Jodi A. Lapidus, Ph.D. ‡
* Oregon Department of Human Services, Disability Determination Services† Oregon Department of Human Services, Office of Family Health
‡ Oregon Health & Science University, Dept. of Public Health and Preventive Medicine
Eleventh Annual Maternal and Child Health Epidemiology ConferenceMiami, FL, December 9, 2005

BACKGROUNDMETHODS
RESULTSDISCUSSION

Bedsharing in context
• Bedsharing has become a controversial practice, despite its growing prevalence.
• There is little population-based U.S. data on who bedshares.
• This information would be useful to:– interpret the significance of case series and
anecdotal reports of SIDS deaths. – inform public policy.– guide clinical practice.– help to focus research.

BACKGROUNDMETHODS
RESULTSDISCUSSION

Oregon PRAMS
“Oregon PRAMS, the Pregnancy Risk Assessment Monitoring System, is a project of the DHS Office of Family Health with support from the national Centers for Disease Control and Prevention (CDC). PRAMS collects data on maternal attitudes and experiences prior to, during, and immediately after pregnancy for a sample of Oregon women.”

Oregon PRAMS
• Stratified, random within strata, over-sampling of first five strata
1. Hispanics
2. Non-Hispanic (NH) blacks
3. NH Asians & Pacific Islanders
4. NH American Indians & Alaskan Natives
5. NH whites with low birthweight babies
6. NH whites with normal birthweight babies
• Weighted 1) to Oregon’s population, 2) for non-response, and 3) for non-coverage

Oregon PRAMS• Monthly sample from birth certificates • Nov. 1998-Oct. 1999 • 2919 surveys mailed• 1867 surveys completed• Mixed mode:
• 1st mailing – 1308 responses
• 2nd mailing - 230
• Computer-assisted telephone interview – 329
• 73.5% strata-weighted response

PRAMS Response
• 1867 completed• 53 excluded
– babies were no longer alive and/or no longer living with mother
• 38 excluded– did not indicate whether or not their babies
were alive and living with mother• 1776 eligible for analysis. • 32 did not answer bedsharing question • 1758 (99% of those eligible) included in the
analysis.

PRAMS Question 62. Maternal-infant bedsharing.
• 62. How often does your new baby sleep in the same bed with you?
Check only one.
Always
Almost always
Sometimes
Never
• “Always” and “almost always” responses combined as “frequent” bedsharing for logistic regression.
• “Sometimes” and “never” responses combined as “infrequent” bedsharing for logistic regression.

Potential factors• Race/ethnicity• Maternal education• Maternal age• Parity• Marital status• Urban vs. mixed density vs.
rural county of residence• Initiation of prenatal care• Adequacy of prenatal care• WIC enrollment• Birthing hospitals by size
• Insurance - at labor & delivery and current
• Family income• Infant gender• Infant birthweight • Bed-sharing status• Breastfeeding duration• Smoker before, during
or after pregnancy• PRAMS mode of
administration
• Analysis performed using SUDAAN 8.0.1
• Multivariable analysis using reverse stepwise regression, entry p < .05, removal p > .10

BACKGROUNDMETHODSRESULTS
DISCUSSION

Bedsharing prevalence among respondents
20.5
14.7
41.4
23.4
0
5
10
15
20
25
30
35
40
45
Always Almost Always Sometimes Never

Statistically significant predictors of bedsharing
• Race/ethnicity• Younger maternal age• Single marital status• Less maternal
education• Lower annual family
income• Type of insurance at
delivery & currently
• Longer breastfeeding duration
• Timing of prenatal care• WIC enrollment• Prenatal care site• Usual infant sleep
position• Not parity• Not maternal smoking

Bedsharing & race/ethnicity, univariable logistic regression
Characteristic Crude Odds Ratio (95% CI)
Hispanic 3.03 (2.29-4.01)
Black † 4.12 (2.96-5.72)
Asian/Pacific Islander † 1.90 (1.41-2.56)
American Indian/Alaskan Native † 1.66 (1.21-2.28)
White † 1.00 (referent)
† non-Hispanic

Bedsharing & maternal age & education,univariable logistic regression
Characteristic Odds Ratio (95% CI)
Maternal Age
13-19 years 2.17 (1.32-3.57)
20-25 years 1.05 (0.71-1.56)
26-30 years 1.00 (referent)
31-48 years 0.85 (0.56-1.31)
Maternal Education
< 12 years 2.77 (1.89-4.05)
12 years 1.48 (1.02-2.13)
> 12 years 1.00 (referent)

Bedsharing & marital status & income, univariable logistic regression
Characteristic Odds Ratio (95% CI)
Marital Status
Single/Divorced 2.09 (1.51-2.89)
Married/Separated 1.00 (referent)
Annual family income
< $30,000 3.06 (1.93-4.85)
$30,000-49,999 1.43 (0.82-2.48)
≥ $50,000 1.00 (referent)

Bedsharing & breastfeeding, initiation of prenatal care & WIC
Characteristic Odds Ratio (95% CI)
Breastfeeding
More than 4 weeks 2.11 (1.43-3.09)
No more than 4 weeks 1.00 (referent)
Initiation of prenatal care
After the first trimester or none 1.46 (1.01-2.10)
First trimester 1.00 (referent)
WIC enrollment
Yes 2.52 (1.81-3.51)
No 1.00 (referent)

Bedsharing & parity, univariable logistic regression
Characteristic Odds Ratio (95% CI)
Parity
Firstborn 1.00 (referent)
Second born 0.75 (0.53-1.08)
Third born 0.91 (0.58-1.42)
Fourth or higher 0.88 (0.51-1.52)

Multivariable logistic, reverse stepwise regression, frequent bedsharing
† non-Hispanic
Characteristic Odds Ratio (95% CI)
Race/Ethnicity
Hispanic 1.69 (1.17 – 2.43)
Black† 3.11 (2.03 – 4.76)
Asian/Pacific Islander† 2.14 (1.51 – 3.03)
American Indian/Alaskan Native†
1.17 (0.80 – 1.71)
White† 1.00 (referent)
Breastfeeding
4 weeks 2.65 (1.72 – 4.08)
< 4 weeks 1.00 (referent)
Annual Family Income
< $30,000 2.44 (1.44 – 4.15)
$30,000-49,999 1.57 (0.88 – 2.82)
$50,000 1.00 (referent)
Characteristic Odds Ratio (95% CI)
Prenatal care site
Health Department clinic
2.41 (1.41 – 4.14)
Private doctor’s or HMO clinic
1.00 (referent)
Hospital clinic 1.11 (0.67 – 1.85)
Other 1.68 (0.88 – 3.19)
Marital Status
Single/divorced 1.55 (1.03 – 2.35)
Married/separated 1.00 (referent)
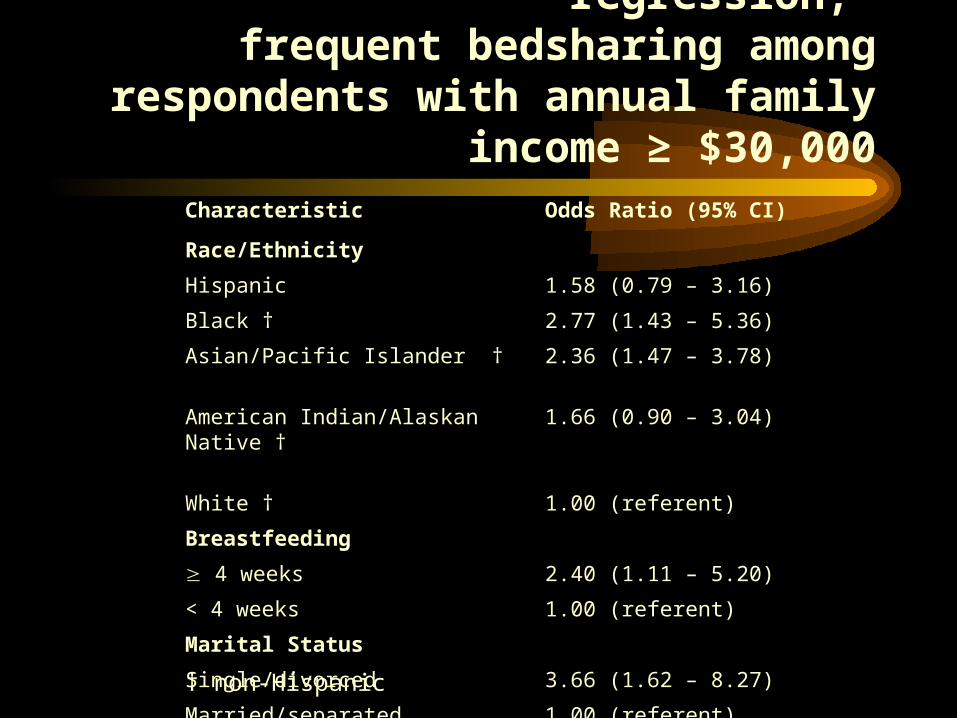
Multivariable logistic regression, frequent bedsharing among respondents with
annual family income ≥ $30,000Characteristic Odds Ratio (95% CI)
Race/Ethnicity
Hispanic 1.58 (0.79 – 3.16)
Black † 2.77 (1.43 – 5.36)
Asian/Pacific Islander † 2.36 (1.47 – 3.78)
American Indian/Alaskan Native †
1.66 (0.90 – 3.04)
White † 1.00 (referent)
Breastfeeding
4 weeks 2.40 (1.11 – 5.20)
< 4 weeks 1.00 (referent)
Marital Status
Single/divorced 3.66 (1.62 – 8.27)
Married/separated 1.00 (referent)† non-Hispanic

BACKGROUNDMETHODS
RESULTSDISCUSSION

Conclusions
• Bedsharing is very common in Oregon, as elsewhere.• Low income, single, breastfeeding mothers are more
likely to bedshare than others.• Black and Asian women are more likely to bedshare
than others, and this appears to be independent of income level. Hispanics are also more likely to bedshare but SES status is an influence.
• Non-economic, as well as economic, factors are important determinants of maternal-infant bedsharing.
• Bedsharing is not solely due to lack of access to cribs and provision of cribs will not eliminate bedsharing.

Published studies on SIDS & bedsharingSummary of studies
– 8 uncontrolled case series raising a question of risk– 9 large case control studies
• 3 did not report results stratified by maternal smoking status but none found an association between bedsharing & SIDS (1,2,3)
• 6 provided stratified results– 3 found no association between SIDS and bedsharing among
nonsmoking mothers; among smoking mothers, risk was increased (4,5,6)
– 1 found an increased risk for infants < 11 weeks old, adjusted for maternal smoking, but not > 11 weeks old; and an increased risk for smoking mothers but not nonsmokers (7)
– 2 found no association between SIDS and bedsharing among nonsmoking mothers of infants > 11 weeks old but did find a risk for infants < 8-11 weeks old and for all infants of smoking mothers (8,9)

SIDS and diagnostic drift
• There is good evidence of diagnostic drift– The decline in overall postneonatal mortality has been
less than that of SIDS mortality– Since 1999, SIDS mortality has continued to fall, while
postneonatal mortality has been flat and other causes of sudden unexpected death have risen
• The evidence regarding bedsharing is clear and consistent and unlikely to have been significantly affected by diagnostic drift
• Further studies must take this phenomenon into account

Crib provision programs
• Valuable public health campaign?• Culturally insensitive?• Supported by scientific evidence?• Bedsharing appears to be the result of combination
of economic, cultural and racial/ethnic factors • Follow up study in St. Louis found that less than
half of those given cribs were using them regularly

Recommendations
• The popularity of bedsharing must be considered when evaluating uncontrolled studies or anecdotal reports.
• The relative importance of cultural and economic factors in choice of bedsharing should be further explored.
• Bedsharing recommendations should be based on the best available scientific evidence, not prejudice or “common sense.”

Recommendations• Cultural values should not be imposed on diverse
groups, without good scientific evidence; bedsharing should be a matter of choice, unless and until there is scientific justification to discourage all bedsharing.– There is strong evidence that bedsharing by smoking mothers
is a significant risk for SIDS.– There is some evidence that bedsharing with infants < 3
months of age by nonsmoking mothers is a risk for SIDS and this practice should be discouraged based on current scientific evidence.
– There is no evidence that maternal bedsharing with infants > 3 months of age by nonsmoking mothers is a significant risk for SIDS.
– Cribs should be a choice and an option, not an obligation

References1. Klonoff-Cohen H, Edelstein SL. Bed sharing and the sudden infant death syndrome. Br
Med J 1995;311:1269-72.2. Hauck FR, Herman SM, Donovan M, al. et. Sleep environment and the risk of Sudden
Infant Death Syndrome in an urban population: the Chicago Infant Mortality Study. Pediatrics 2003;111:1207-14.
3. Brooke H, Gibson A, Tappin D, Brown H. Case control study of sudden infant death syndrome in Scotland, 1992-1995. Br Med J 1997;314:1516-20.
4. Scragg RK, Mitchell EA, Taylor BJ, al. et. Bed sharing, smoking, and alcohol in the sudden infant death syndrome. Br Med J 1993;307:1312-8.
5. Mitchell EA, Tuohy PG, Brunt JM, et al. Risk factors for sudden infant death syndrome following the prevention campaign in New Zealand: a prospective study. Pediatrics 1997;100:835-40.
6. Fleming PJ, Blair PS, Bacon C, et al. Environment of infants during sleep and risk of the sudden infant death syndrome: results of 1993-5 case-control study for confidential inquiry into stillbirths and deaths in infancy. Br Med J 1996;313:191-5.
7. McGarvey C, McDonnell M, Hamilton K, O’Regan M, Matthews T. An eight-year study of risk factors for SIDS: Bedsharing vs. non bed-sharing. Arch Dis Child 2005 (doi:10.1136/adc.2005.074674):1-7.
8. Carpenter RG, Irgens LM, Blair PS, et al. Sudden unexplained infant death in 20 regions in Europe: case control study. Lancet 2004;363:185-91
9. Tappin D, Ecob R, Brooke H. Bedsharing, roomsharing, and Sudden Infant Death Syndrome in Scotland: a case-control study. J Pediatr 2005;147:32-7.