sneak preview in+care campaign clemens steinbock director, national quality center...
TRANSCRIPT

Sneak PreviewSneak Previewin+care in+care CampaignCampaign
Clemens SteinbockClemens SteinbockDirector, National Quality CenterDirector, National Quality Center [email protected]@NationalQualityCenter.org212-417-4730212-417-4730

Agenda
• Retention – a major HIV public health issue
• HAB/NQC National in+care Campaign• Campaign video premiere (get your
popcorn…)• Q&A

Where Are My Patients?
Retention - an Independent Predictor for Improved HIV Health Outcomes

Facts about Retention
• Retaining patients in care results in better health outcomes and lower costs for the patient as regular appointments with a provider correlate with higher CD4 count, suppressed viral load, and fewer hospital admissions/emergency room visits [1]
• Mortality rates are significantly lower among patients seen 3 or 4 times per year versus once or twice annually [2]
• Attending all medical appointments during the first year of HIV care doubled survival rates for years afterwards, regardless of baseline CD4 cell count or use of ART [3]
[1] Horstmann, E., J. Brown, F. Islam, J. Buck, & B. Agins. “Retaining HIV-Infected Patients in Care: Where Are We? Where Do We Go from Here?” Clinical Infectious Diseases (2010); 50: 752-761.[2] Giordano TP, Gifford AL, White AC Jr, et al. Retention in care: a challenge to survival with HIV infection. Clin Infect Dis. 2007;44:1493-9. [3] Giordano TP, Hartman C, Gifford AL, et al. Predictors of retention in HIV care among a national cohort of US veterans.HIV Clin Trials. 2009;10:299-305.

Facts about Retention
• A Baltimore, MD community health clinic showed 85% of home-less patients who received street outreach interventions attended at least one clinical appointment over a 12-month period [1]
• Same-day scheduling for marginalized populations improved retention rates at two Bronx, NY clinics [2]
• Use of care coordinators increased retention in a Washington, DC clinic even among traditionally hard-to-reach populations; those with coordinators had higher retention rates compared to those without [3]
[1] Tommasello AC, Gillis LM, Lawler JT, et al. Characteristics of homeless HIV-positive outreach responders in urban U.S. and their success in primary care treatment. AIDS Care. 2006; 18(8): 911-7. [2] Cunningham CO, Sanchez JP, Heller DI, et al. Assessment of a medical outreach program to improve access to HIV care among marginalized individuals. APHA. 2007; 97(10): 1758-61. [3] Ukman, J. Eliminating no-shows at Whitman-Walker. Washington Post. May 30, 2005.

“My clinic fed me when I was hungry. They helped me get an apartment when I was homeless. They gave me good care when I had nowhere else to go. They cared for me first as a person and then as a patient. They treated me like family. That’s why I stayed in care. That’s why I keep coming back. And that’s why I’m alive today.”
Ronald, HIV-infected patient

Non-Engager Sporadic User Fully Engaged
Engagement in Care Continuum
[1] Health Resources and Services Administration, HAB. August 2006. Outreach: Engaging People in HIV Care Summary of a HRSA/HAB 2005 Consultation on Linking PLWH Into Care. [2] Eldred L, Malitz F. Introduction [to the supplemental issue on the HRSA SPNS Outreach Initiative]. AIDS Patient Care STDS 2007; 21(Suppl 1):S1–S2.

Stages of Engagement
HIV-Infected
Gardner E, The Spectrum of Engagement in HIV Care and its Relevance to Test-and-Treat Strategies for Prevention of HIV Infection; Clin Infect Dis. (2011) 52 (6): 793-800.
HIV-Diagnosed
Linked to HIV Care
Retained in Care
Need ART and On ART
Adherent/Undetectable

HIV-Infected ~ 1.1 million
[1] HIV prevalence estimates–United States, 2006. MMWR Morb Mortal Wkly Rep 2008; 57:1073–6.[2] District of Columbia HIV/AIDS epidemiology update 2008. Washington, DC: Government of the District of Columbia, Department of Health, HIV/AIDS Administration. http://dchealth.dc.gov/DOH/frames.asp?doc5/doh/lib/doh/pdf/dc_hiv-aids_2008_updatereport.pdf.[3] Nguyen TQ, Gwynn RC, Kellerman SE, et al. Population prevalence of reported and unreported HIV and related behaviors among the household adult population in New York City, 2004. AIDS 2008; 22:281–7.
• At the end of 2006, 1.1 million adults and adolescents were living with the HIV across the U.S. (prevalence 0.45%) [1]
• Geographic variability is substantial; in some US cities, HIV seroprevalence exceeds 1%–2% [2]
• HIV seroprevalence in populations at high risk of infection, such as men who have sex with men in New York City, exceeds 13% [3]
Stages of Engagement

HIV-Infected ~ 1.1 million
[1] Campsmith ML, Rhodes PH, Hall HI, Green TA. Undiagnosed HIV prevalence among adults and adolescents in the United States at the end of 2006. J Acquir Immune Defic Syndr 2010; 53:619–24.[2] Campsmith ML, Rhodes PH, Hall HI, Green TA. Undiagnosed HIV prevalence among adults and adolescents in the United States at the end of 2006. J Acquir Immune Defic Syndr 2010; 53:619–24.[3] Klein D, Hurley LB, Merrill D, Quesenberry CP Jr. Review of medical encounters in the 5 years before a diagnosis of HIV-1 infection: im- 445 plications for early detection. J Acquir Immune Defic Syndr 2003; 32:143–52.
• 232,700 (21%) are estimated to be unaware of their HIV infection [1]
• Those not diagnosed have a higher risk of transmitting HIV to others than do those who are aware of their HIV infection [2]
• 35%–45% of individuals with newly diagnosed HIV infection have AIDS within 1 year after diagnosis [3]
HIV-Diagnosed ~874k
Stages of Engagement

HIV-Infected ~ 1.1 million
[1] Perkins D, Meyerson BE, Klinkenberg D, Laffoon BT. Assessing HIV care and unmet need: eight data bases and a bit of perseverance. AIDS Care 2008; 20:318–26.[2] Torian LV, Wiewel EW, Liu KL, Sackoff JE, Frieden TR. Risk factors for delayed initiation of medical care after diagnosis of human immunodeficiencyvirus. Arch Intern Med 2008; 168:1181–7.
• In St. Louis, Missouri, 73% of individuals with newly diagnosed HIV infection received HIV care within 1 year after diagnosis of HIV infection [1]
• In New York City, 64% of individuals with newly diagnosed HIV infection initiated care within 3 months, and 83% entered care within 4 years [2]
Stages of Engagement
Linked to HIV Care ~655k

HIV-Infected ~ 1.1 million
[1] Perkins D, Meyerson BE, Klinkenberg D, Laffoon BT. Assessing HIV care and unmet need: eight data bases and a bit of perseverance. AIDS Care 2008; 20:318–26.[2] Olatosi BA, Probst JC, Stoskopf CH, Martin AB, Duffus WA. Patterns of engagement in care by HIV-infected adults: South Carolina, 2004–2006. AIDS 2009; 23:725–30.
• Three U.S. population-based studies have found that 45%–55% of known HIV-infected individuals fail to receive HIV care during any year [1]
• Over longer periods, approximately one-third of HIV-infected individuals fail to access care for 3 consecutive years in some communities [2]
Stages of Engagement
Retained in Care ~437k
HIV-Infected ~ 1.1 million
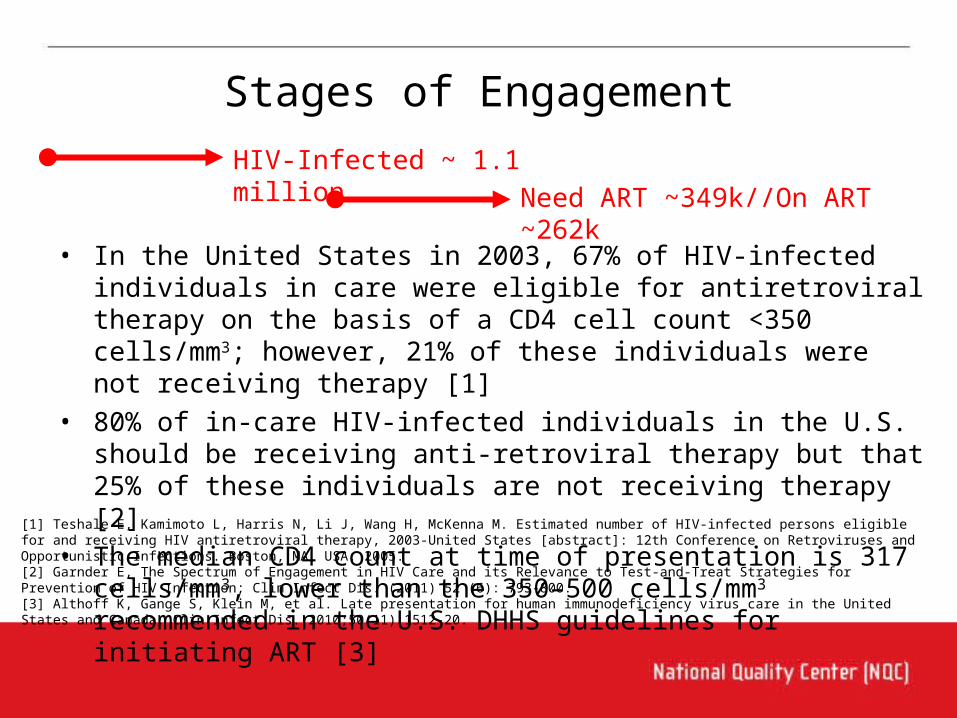
[1] Teshale E, Kamimoto L, Harris N, Li J, Wang H, McKenna M. Estimated number of HIV-infected persons eligible for and receiving HIV antiretroviral therapy, 2003-United States [abstract]: 12th Conference on Retroviruses and Opportunistic Infections. Boston, MA, USA: 2005.[2] Garnder E, The Spectrum of Engagement in HIV Care and its Relevance to Test-and-Treat Strategies for Prevention of HIV Infection; Clin Infect Dis. (2011) 52 (6): 793-800.[3] Althoff K, Gange S, Klein M, et al. Late presentation for human immunodeficiency virus care in the United States and Canada. Clin Infect Dis. 2010;50(11):1512-20.
• In the United States in 2003, 67% of HIV-infected individuals in care were eligible for antiretroviral therapy on the basis of a CD4 cell count <350 cells/mm3; however, 21% of these individuals were not receiving therapy [1]
• 80% of in-care HIV-infected individuals in the U.S. should be receiving anti-retroviral therapy but that 25% of these individuals are not receiving therapy [2]
• The median CD4 count at time of presentation is 317 cells/mm3, lower than the 350–500 cells/mm3 recommended in the U.S. DHHS guidelines for initiating ART [3]
Stages of Engagement
Need ART ~349k//On ART ~262k

HIV-Infected ~ 1.1 million
[1] Gardner E, The Spectrum of Engagement in HIV Care and its Relevance to Test-and-Treat Strategies for Prevention of HIV Infection; Clin Infect Dis. (2011) 52 (6): 793-800.[2] Das M, Chu PL, Santos GM, et al. Decreases in community viral load are accompanied by reductions in new HIV infections in San Francisco.PLoS One 2010; 5:e11068.
• Nonpersistence, nonadherence, and antiretroviral resistance are barriers to effective antiretroviral therapy, contributing to detectable HIV viremia in 15%–25% of individuals receiving therapy [1]
• Two recent studies found that 78%–87% of individuals receiving antiretroviral therapy, including individuals receiving initial and subsequent regimens, had an undetectable viral load [2]
Stages of Engagement
Adherent/Undetectable ~209k

Stages of Engagement
HIV-Infected - 100%
[1] Gardner E, The Spectrum of Engagement in HIV Care and its Relevance to Test-and-Treat Strategies for Prevention of HIV Infection; Clin Infect Dis. (2011) 52 (6): 793-800.
HIV-Diagnosed - 79%
Linked to HIV Care – 59%
Retained in Care - 40%
Need ART - 32%
On ART - 24%
Adherent/Undetectable - 19%

1 in 5 do not know their HIV status2 in 5 have not seen an HIV primary care doctor3 in 5 don’t regularly see their HIV doctor4 in 5 are not viral load suppressed
Care Continuum Summary
Adopted from Gardner E, The Spectrum of Engagement in HIV Care and its Relevance to Test-and-Treat Strategies for Prevention of HIV Infection; Clin Infect Dis. (2011) 52 (6): 793-800.

“Not staying in care is the
biggest barrier to better heath!”

What Can Quality Improvement Contribute?
• Focus on systems of care delivery
• Systematize processes of routine measurement
• Interdisciplinary team approach
• Application of quality improvement methodologies
and tools
• Innovative (“out of the box”) solutions

At What Level Do We Measure Retention?
a) The patient
b) The clinic
c) The district
d) The region/state
e) The nation
f) All of the above

Examples of Patient Retention Measures
• Number of unique patients with at least one visit in past 4 months / Number of unique patients with at least one visit in past 12 months
• Number of unique patients with at least one visit during the 4-month interval following a defined 12-month period / Number of unique patients with at least one visit in the defined 12-month period
• Number of unique patients with 2 or more visits during a defined 12 month period / Number of total unique patients in the clinic registry during the defined 12 month period
• Number of unique patients with at least 2 or more visits in past 12 months at least one of which in the last 6 months / Number of unique patients with at least one visit in past 12 months.
• Number of unique patients with 2 or more visits in the past 12 months with at least one visit in each six month period / Number of unique patients with at least one visit in past 12 months
• Number of unique patients with 2 or more visits in the past 12 months with at least one visit in each six month period and a minimum of 60 days between the two visits / Number of unique patients with at least one visit in past 12 months
* For each measure, a "visit" is defined as an HIV medical visit with a clinical provider (MD, PA, NP)

ADAPTED FROM MUGAVERO ET AL (2010) From Access to Engagement: Measuring Retention in Outpatient HIV Clinical Care. AIDS Patient Care and STDs. 24: 607-614.

Agins, B and staff at All Country Learning Network Meeting in Windhoek, Namibia, 2011.

Upcoming HRSA HIV/AIDS Bureau-funded National Quality Improvement Initiative

2010 Survey Results with HIV Providers
Answer Options
Response Percent
Retaining HIV-positive patients in HIV primary care 67.40%Increasing the number of HIV-positive persons not in care linked to HIV care
45.30%
Increasing the rate of cervical cancer (PAP) screening for women with HIV
45.30%
Improving health literacy among HIV-positive persons in care
26.70%
Increasing the rate of annual mental health screening 24.40%Increasing the proportion of HIV-positive persons in care who receive an annual oral health screening
24.40%
Increasing the rate of syphilis screening for HIV-positive patients
19.80%
Increase the rate of anal cancer screening for men with HIV
18.60%
[1] NQC 2010 Online Survey representing 136 Ryan White programs to indicate the most important topic for a national quality improvement campaign


This HIV Campaign is designed to facilitate local, regional, or even state-level efforts to retain more HIV patients in care and to prevent HIV patients falling out of care while building and sustaining a community of learners among Ryan White providers.

Recruitment Video – YouTube.com/incarecampaign
Development of an Awareness and Recruitment Video
• to highlight the importance of retention in HIV care and its affect on health outcomes
• to increase awareness about the Campaign
• to link those who are interested in joining the Campaign with recruitment information

in+care Campaign Video

Campaign Framework
• participation in the Campaign is voluntary and Ryan White grantees across all funding streams and subgrantees are invited to join
• participating agencies enroll for a 12-month commitment
• routine reporting of performance data on up to 4 uniform Campaign-related measures
• routine submission of a simple progress report to highlight improvement strategies and challenges
Campaign Framework
• monthly webinars provide content expertise and promote peer sharing
• participating agencies have access to coaches for support
• where possible, regional/local meetings of Campaign participants are held
• consumers will be involved in this Campaign wherever possible

Why Sign-up?
• Keeping patients in care extends their lives and makes for healthier communities
• Participation will align your HIV program with the National HIV/AIDS Strategy
• The Campaign isn’t just about measuring-we’re actively implementing improvement strategies
• National real-time benchmarking data on key retention measures are immediately available for all participating agencies
• Take advantage from successes of your peers and share your best practices with them
• Today’s leading quality improvement and retention experts are available for support, coaching, and to answer your questions

Recruitment Activities• Email invitations to all Ryan White
grantees• Recruitment tool kits to be mailed to all
Ryan White grantees and NQC contacts• Information on campaign to be
advertised on HRSA HAB Information E-mail
• HAB Project Officers to inform their grantees
• Recruitment video to be posted on YouTube, HRSA YouTube, NQC websites
• Campaign information to be listed on HRSA TARGET site
• NQC reaching out to stakeholder organizations to get their support and increase awareness
• HRSA plans to reach out to SPNS Part B System Linkages and Retention in Care grantee recipients once selected

Campaign Website
• Design of Campaign website– background information– upcoming events– Campaign and
retention resources– information about
who’s involved• Sign-up/registration page• Access to online
Campaign database and progress reports

Campaign Database
• Allows participating agencies to self-report their performance data based on established indicator definitions
• Individuals need to register to access the database
• Organizations can sign up to form a group of grantees, which would allow them to generate group reports, such as HIVQUAL regional groups
• Immediate access – to individual scores trended over time– to group scores – to regional/national benchmarking
reports– to reports based on common search
criteria• Coaches have access to individual/groups
scores to better assist participating agencies

Technical Working Group
• Chaired by Dr. Bruce Agins and Dr. Laura Cheever
• Comprised of distinguished experts in the field of retention, including clinical experts, researchers, national stakeholders and other strategic thinkers from the Ryan White and other health care communities
• Committee meets during the start-up phase of the Campaign to provide suggestions on the following areas:– Retention Measures: Suggest up to 3 retention measures to be used in
Campaign– Change Packet: Suggest clusters of interventions to guide participating
grantees– Overall Aim for Collaborative: suggest realistic aims for this Campaign
• Upcoming 1 day meeting

in+care Participants by Zip Code (9/4/11)
(# of providers: 132; # of HIV patients: 144,778)

Campaign Headquarters:National Quality Center
(NQC)90 Church Street, 13th floorNew York, NY 10007
Phone: 212-417-4730
incarecampaign.org