snakes and other pets - tucson osteopathic medical …€¦ · · 2011-03-29• antivenom •...
TRANSCRIPT

1
Snakes and other Pets
Frank LoVecchio, DO, MPH, FACEPCo-Medical Director, Banner Good Samaritan Poison Center
Maricopa Medical Center, Research Director and Vice-ChairmanDepartment of Emergency Medicine
Phoenix, AZ
Case: A new antidote for an old problem
• A 30 year old man is envenomated by a rattlesnake.
• He has no history or asthma and takes no meds
• He has no allergies

2

3
Tongue Bites
24 hours
RULE ONE:PLEASE DON’T KISS SNAKES

4
Penetrating Ocular Injury Caused by Venomous Snakebite Chien-Chung Chen et alAJOM
RULE TWO:PLEASE DON’T HANDLE DEAD SNAKES
5
CroFabTM Dose
NoAdminister Additional 4 - 6 Vials of CroFab (TM)
Initial Control Achieved?
Establish Initial ControlBy Administering 4-6 Vials of CroFab(TM)
Over 1 Hour
Patient with Indication forCroFab(TM) Administration

6
VIPERIDAE ELAPIDAE COLUBRIDAE HYDROPHIDAE ATRACTASPIDIDAE
Families of Poisonous Snakes
mobile, front fangs
fixed, front fangs
fixed, rear fangs
fixed, front fangs
rear/lateral – direct-ed front fangs
US: Thousands of snake bites occur annually
Hundreds in Arizona
< 10 deaths per year
5 million snake bites
125,000 deaths

7
Families of Venomous Snakes
• Viperidae
• Elapidae
• Hydrophiidae
• Atractaspididae
• Colubridae
CrotalinaeViperinae
subfamilies
(coral snakes)
Crotalinae• New world or ‘pit’
vipers• Front, mobile fangs• Triangular shaped
head• Heat sensing pits
• >95% venomous bites in US
US Pit Vipers
CottonmouthCopperhead
Rattlesnake

8
MojaveWestern diamondback(C atrox) (C scutulatus)
Arizona Rattlesnakes
Speckled Rattlesnake Northern Blacktail Rattlesnake
Tiger Rattlesnake(C tigris)
(C mitchellii) (C molossus)
Massasauga(Sistrurus catenatus)
Sidewinder(C cerastes)
Ridgenose rattlesnake Rock rattlesnake(C lepidus)
Twin-spotted rattlesnake(C pricei)
(C willardi)

9
Hopi Rattlesnake
Western Rattlesnake
Grand Canyon Rattlesnake
(C viridis)Arizona Black Rattlesnake
Who are the victims?
Unlucky
unintelligent
Leg bites
Hand bites
About 60% of all bites illegitimate
Illegitimate Bitesmale 97.9%female 2.1%alcohol 56.0%
Legitimate Bitesmale 72%female 28%alcohol 16%

10
Lower extremities-39.3%
Upper extremities-60.2%
Other-0.4%
Location of Rattlesnake Bites
“Mighty Fighting Sun of Love and Ecstasy”
VIPERIDAE
Crotalinae Viperinaepit vipersnew world vipers
old world vipers
Crotalus Sistrurus Agkistrodon
rattlesnakes cotton mouthscopperheads

11
Legitimacy of Snakebite• Legitimate Bite
– did not recognize encounter with snake before being bitten
– recognized encounter and immediately attempted to move away, but was bitten anyway
• Illegitimate Bite– recognized encounter with
snake, but did not try to immediately move away
– pet snakes, moving snakes, killing snakes, kissing snakes, playing with snakes, feeding snakes
Demographics and Characteristics236 patients
Populationmale 81%female 19%children 22%
Locationupper extremity 60.2%lower extremity 39.4%other 0.4%
Edema After Snakebite
• Swelling looks very scary
• Long, linear incisions on envenomated extremity would decrease tissue pressure and might “restore” blood flow
• Tissue necrosis would then be prevented

12
Rattlesnake Bite
noswelling
mildswelling
severeswelling
noinsurance
excellentinsurance
long linearincisions
Compartment Syndrome• Other management options
• Antivenom• Antivenom and mannitol
Venom
• Enzymes– Proteolytic– Thrombin-like– Hyaluronidase– Phospholipase A2
– Many others….
• Non-enzymatic proteins
• Metals • Lipids• Biogenic amines• Amino acids
NecrosisHematologic toxicityTissue
damageDisrupts cell membranes
13
Tissue Hypertension
• Tissue hypertension quite exceptional despite edema
• Fasciotomies and SQ decompression do not prevent myonecrosis in animals receiving IM or SQ venom injections
• Noninvasive vascular studies demonstrate increased blood flow in envenomated extremities in most all patients
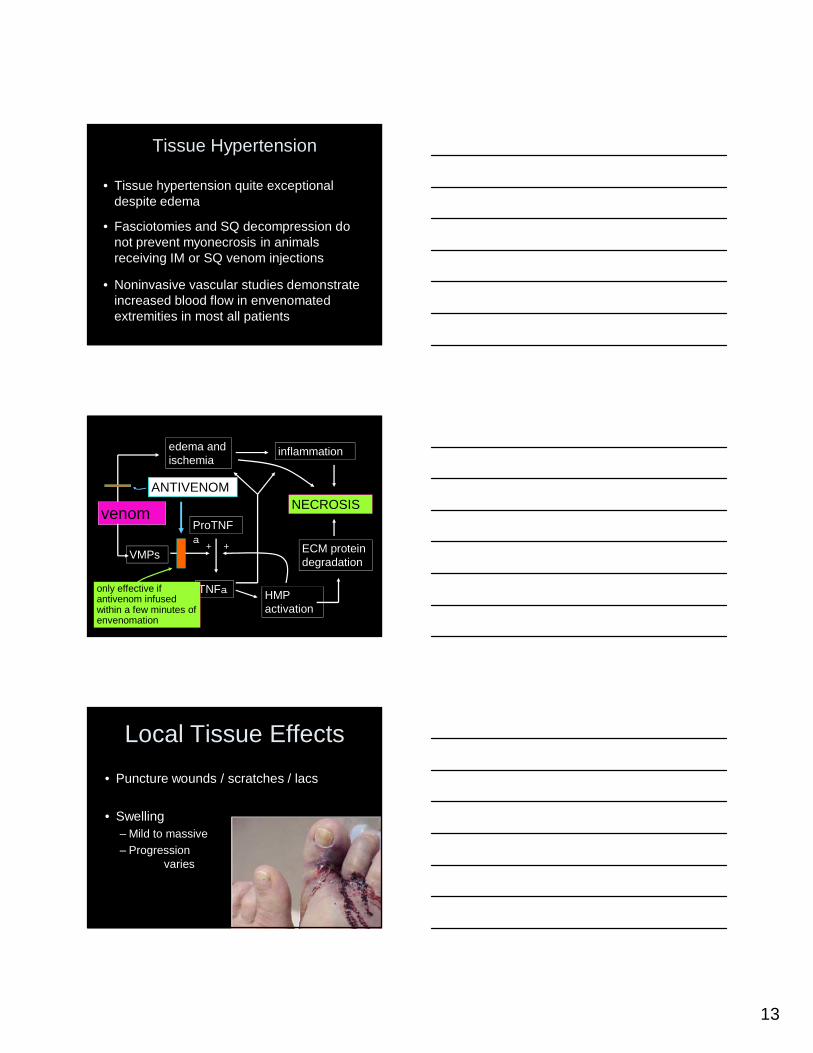
venom
edema and ischemia
inflammation
VMPs
ProTNFa
TNFa HMP activation
ECM protein degradation
NECROSIS
+ +
ANTIVENOM
only effective if antivenom infused within a few minutes of envenomation
Local Tissue Effects• Puncture wounds / scratches / lacs
• Swelling – Mild to massive– Progression
varies

14
Local Tissue Effects• Hemorrhagic bulla (blebs)
• Local necrosis– Tissue loss– Amputation
• VMPs and other digestive enzymes
Blebs

15
Blebs
Myotoxicity
• Digestive enzymes and metalloproteinases
• More specific myotoxins– myotoxin a and similar proteins
• prairie rattlesnake (C. viridis viridis)• midget faded rattlesnake (C. viridis concolor)• common in other Crotalus and Sistrurus
species

16
Myotoxicity
venom
direct injection into muscle produces local myonecrosis
digestive enzymesmetalloproteinasesmyotoxins
venom
subcutaneous
systemicrhabdomyolysis
digestive enzymesmetalloproteinasesmyotoxins
systemicabsorption
Coagulopathy
• About 60% of victims develop coagulopathy
• Hypofibrinogenemia with prolonged clotting times by far the most common
Coagulopathy
clotting cascade
prothrombin thrombin
fibrinogen fibrin chain
inactive XIII
active XIII
fibrinopeptide A & B
Normal Coagulation
cross linking
inhibited by heparin
fibrin mesh

17
Coagulopathy
thrombin-like enzymes
fibrinogenpoorly-constructed fibrin chain
fibrinopeptide A
Crotalinae Thrombin-like Enzymes
fibrinopeptide B OR
only split FP-A or FP-B from fibrinogen
Coagulopathy
thrombin-like enzymes
fibrinogenpoorly constructed fibrin chain
fibrinopeptide A
Crotalinae Thrombin-like Enzymes
fibrinopeptide B OR
inactive XIII
active XIII
only split FP-A or FP-B from fibrinogen
doesn’t activate factor XIII
fibrin mesh
Coagulopathy
thrombin-like enzymes
fibrinogenpoorly constructed fibrin chain
fibrinopeptide A
Crotalinae Thrombin-like Enzymes
fibrinopeptide B OR
inactive XIII
active XIII
only split FP-A or FP-B from fibrinogen
doesn’t activate factor XIII
fibrin mesh
not inhibited by heparin

18
Hypofibrinogenemia
• Two main mechanisms1.Thrombin-like enzymes2.Fibrinolysis/Fibrinogenolysis
• degrade fibrinogen• degrade fibrin
FibrinolysisFibrinogenolysis
fibrinogen fibrin chaincross linking
fibrin mesh
enzymatic degradation of fibrinogen and fibrin
degradation products
Benign Defibrination
• hypofibrinogenemia and prolonged clotting times
• no abnormal intravascular coagulation
• significant bleeding unusual in absence of thrombocytopenia or trauma
• occasional blood loss into envenomated extremity requires transfusion

19
Venom-Induced Thrombocytopenia
• About 30% of victims experience thrombocytopenia
• Nadir in untreated patients commonly between 72 and 96 hours

20
Anaphylaxis
• Rare• IgE mediated• Pre-sensitized to crotalids
– Previous bites– Dermal exposure– Ingestion of rattlesnake meat?

21
Case• 25 yo man presents 25 min following RSB to
hand
• SBP = 68/28 mmHg, intoxicated
• 20 min later develops tongue, facial, and neck edema with airway compromise
Case
• IVF, epinephrine (SBP 90 x 2 hr)• Difficult intubation (sat>90%)
• Minimal swelling• Mild coagulopathy• Treated with AV
• Rhabdomyolysis(CPK = 120,000)
• Renal failure• Hemodialysis

22
Outcome• Complicated course
– Recurrent large bowel enterocutaneous fistulas
– Sepsis– Malnutrition– Died one year later in rehab facility
• History of capturing and cooking RS
Respiratory Failure• Patient presents following RSB with muscle
weakness and diplopia.
• Rapidly progresses to hypoventilation and respiratory failure.
• Despite antivenom treatment, patient requires intubation.
DIC• Extremely uncommon• Labs similar to
venom-induced thrombocytopenia and defibrination, with additional findings of:– Hemolysis– Red cell fragmentation– Organ infarction– Diffuse bleeding

23
ED Management• IV fluids• Pain control • Measure
circumference• Neurovascular
checks• Elevate extremity
Antivenom?
Indications for Antivenom
• Rapid progression of swelling• Significant coagulopathy or
thrombocytopenia• Neurotoxicity • Shock
The Case of the Concerned Citizen• A guy on I-17
The Alleged Scene

24
Venomous Lizards
Heloderma suspectumGila Monster
Heloderma horridumMexican Beaded Lizard
Helodermatidae
H. s. suspectum
H.s. cinctumH. h. horridum
H. h. exasperatum
H. h. alvarezi
Gila Monster bite
Resulting in allergic rxn
...and tabloid story!

25
Gila Monster Distribution
Reticulated Gila MonsterH. s. suspectum
Banded Gila MonsterH. s. cinctum
Gila MonsterVenom Delivery
• Venom glands on mandible
• Ducts lead to labial mucosa
• Venom flows through grooved teeth and into wounds

26
Removing a Gila Monster• Pry mouth apart with pliers• Jam screwdriver down monster’s throat• Dip monster in gasoline and set on fire• Pour gasoline into mouth and set on fire• Place fire under jaw without gasoline• Strike back of lizard’s head with large
stone
Scorpions• 40 species of scorpions in the US• Only one dangerous, considered to
be potentially fatal– Found in Arizona, some areas of
Texas, New Mexico, California, and Nevada
• >6000 calls/year to Samaritan Regional Poison Control Center
• Most managed at home

27
The Bark Scorpion
• Centruroides sculpturatus/exilicauda– Yellow/tan/brown– Up to 5 cm in length– Hard exoskeleton– Segmented tail curves up, ends in a
telson, containing venom glands and stinger
Exoskeleton
Telson

28
The Bark Scorpion• Body fluoresces under UV light• Resides in or near trees; wood
–Climbs, but not up glass
Bark Scorpion
Envenomation• Most stings cause only local pain • Onset of symptoms immediate, progress up to 5
hours• Children tend to be most severely affected• No deaths reported in the US since 1968

29
Management• Most symptoms improve within 9 to
30 hours without treatment• Pain and paresthesias may last up
to 2 weeks• Options:
–Antivenin (not currently available)–Sedation and pain control
Antivenin
• Recommended for Grade III and IV envenomations
• Results in rapid reversal of neurologic and respiratory toxicity within one hour
• Risks– Hypersensitivity reactions– Serum sickness
Scorpion Antivenin
• Goat serum derived• Contraindications
–Previous scorpion antivenin–Asthma–Beta Blockers–CAD

30
Black Widow
• Latrodectus mactans• Female is 8-10 mm, black
with red hourglass mark on ventral surface
• Live in woodpiles, crevices, barns…
Envenomation• Female bite produces
sharp pain• Pair of fang marks with
surrounding erythema• 15 minutes to 6 hours
following the bite, “latrodectism”

31
Venom
• a-latrotoxin– Potent neurotoxin– Induces neurotransmitter release
from nerve terminals
Latrodectism– Neuromuscular
• Muscle cramps – site, chest, abdomen (may mimic acute abdomen), thighs
• Rigidity, tremor, weakness, priapism
– Systemic • Nausea, diaphoresis,
pavor mortis (fear of death), salivation, urinary retention
– Cardiopulmonary• Hypertension, tachycardia,
bronchorrhea

32
Management• Airway • Tetanus
prophylaxis• Pain control • Antivenin to speed
recovery
Management• Airway • Tetanus prophylaxis• Pain control • Antivenin to speed recovery

33