smoking cessation may present a positive impact on mandibular bone quality and periodontitis-related...
TRANSCRIPT
Volume 76 • Number 4
520
* Department of Prosthodontics and Periodontics, Division of Periodontics, School ofDentistry at Piracicaba, University of Campinas, Piracicaba, São Paulo, Brazil.
† Department of Oral Diagnostic, Division of Radiology, School of Dentistry at Piracicaba,University of Campinas.
Astrong positive correlation betweencigarette consumption and in-creased incidence and severity of
periodontal disease has been demon-strated.1-3 Clinical observations of differ-ences between smokers and non-smokersregarding their periodontal status havestimulated extensive research activity.Cigarette smoking has been shown torepresent a strong risk marker, and pos-sibly, a true risk factor for periodontal dis-ease.4,5 Moreover, it has been shown thatsmokers not only run an increased risk ofdeveloping periodontal disease, but alsoenhance the severity of existing perio-dontal disease.4,6
The hallmark of periodontitis is achronic destruction of periodontal attach-ment apparatus following an intenseinflammatory response to bacteria. Theinfluence of smoking on the periodontalbiofilm is still controversial. In general,there is some agreement that cigaretteconsumption has a negative impact onthe host response. Animal studies re-ported that nicotine7,8 and cigarettesmoke inhalation (CSI),9 when admin-istered after periodontitis induction, en-hanced ligature-induced periodontalbreakdown, and could be associated witha higher level of matrix metallopro-teinase-2 (MMP-2) in the gingival tis-sues.9 Furthermore, higher levels oftumor necrosis factor-alpha (TNF-α)were observed in the gingival crevicularfluid of smokers with moderate to severe
Smoking Cessation May Present a PositiveImpact on Mandibular Bone Quality andPeriodontitis-Related Bone Loss: A Studyin RatsJoão B. César-Neto,* Bruno B. Benatti,* Francisco Haiter Neto,† Antonio W. Sallum,*Enilson A. Sallum,* and Francisco H. Nociti Jr.*
Background: It has been previously shown that cigarettesmoke inhalation (CSI) enhances bone loss in ligature-inducedperiodontitis. In this study, the hypothesis that the interruptionof smoke exposure would reverse the impact of CSI on mandibu-lar bone quality and periodontitis-related bone loss was tested.
Methods: Fifty-three Wistar rats were randomly assigned toone of the following groups: group 1: control, N = 16; group 2:83 days of CSI prior to ligature placement, N = 17; or group 3:90 days of CSI before and 60 days after ligature placement, N =20. Animals were sacrificed 60 days after ligature placement,the jaws removed and immediately radiographed for photoden-sitometry analysis. Bone loss was histometrically evaluated.
Results: CSI did not affect unligated sites in either condition(P >0.05); however, smoke inhalation during the whole experi-mental period significantly enhanced bone loss in ligated teeth(P <0.05). Moreover, similar levels of bone loss were observedfor ligated teeth between the control and cessation groups (0.90 ±0.33 mm2; 0.96 ± 0.32 mm2; 1.64 ± 0.65 mm2; groups 1, 2and 3, respectively). Radiographically, continuous exposure tocigarette smoke promoted a significantly reduced bone density(1.74 ± 0.38 aluminum equivalence [Al eq]; 1.74 ± 0.14 Al eq;and 0.68 ± 0.10 Al eq for groups 1, 2, and 3, respectively).
Conclusions: Within the limits of the present investigation, itcan be assumed that CSI may enhance bone loss in ligature-induced periodontitis, and negatively impact mandibular bonequality. Additionally, smoke exposure cessation seems to reverseits impact on mandibular bone, and, therefore, may be of clin-ical relevance. J Periodontol 2005;76:520-525.
KEY WORDSAnimal studies; bone and bones; bone loss/prevention andcontrol; periodontitis/etiology; smoking/adverse effects.
40138.qxd 4/18/05 8:49 AM Page 520

521
J Periodontol • April 2005 César-Neto, Benatti, Neto, Sallum, Sallum, Nociti
periodontal disease.10 It has alsobeen reported that tobacco com-ponents may alter morphologyand metabolism of periodontalcells without the presence of bac-terial contamination.11-18 In vitrostudies have shown that nicotinenegatively affects osteoblasts,11,12
gingival13 and periodontal liga-ment fibroblasts,14 and stimulatesosteoclast activity.12,15 Reportsshowed that acrolein and acetalde-hyde, volatile components of cig-arette smoke, also have a negativeeffect on fibroblast cultures.16-18
Likewise, it has been reported thatperipheral mononuclear cells ofsmokers release more interleukin-(IL)-1β when treated with cigarettesmoke.19 Clinical studies haveshown that abstinence from smok-ing reduces incisional woundinfection,20 reduces complicationsof postmastectomy breast recon-struction,21 reduces the risk ofsenile cataract,22 and helps reversethe negative impact of cigarette smoking on spinalfusion outcomes.23 Regarding periodontal disease, arecent prospective study24 reported that individualswho stopped smoking lost significantly less marginalbone than those who did not. Therefore, the aim ofthe present study was to test, in a rat model, thehypothesis that CSI cessation would reverse its impacton mandibular bone quality and on periodontitis-relatedbone loss.
MATERIALS AND METHODSAnimalsFifty-three male Wistar rats (300 to 400 g) were in-cluded in the study. The animals were kept in plasticcages with access to food and water ad libitum. Priorto the surgical procedures all animals were allowed toacclimatize to the laboratory environment for a periodof 5 days. The protocol was approved by the Univer-sity of Campinas Institutional Animal Care and UseCommittee.
Experimental Design (Fig. 1) At the beginning of the study, the animals were ran-domly assigned to one of the following groups: group1: control (N = 16); group 2: 83 consecutive days ofintermittent cigarette smoke inhalation (CSI) prior toligature placement (N = 17); or group 3: 90 days of CSIbefore and 60 days after ligature placement (N = 20).Animals in groups 2 and 3 were intermittently housedin an exposure chamber (45 × 25 × 20 cm3) as previously
described.25-27 Briefly, five animals were housed at thesame time in the chamber for 8 minutes three timesdaily, and the cigarette smoke of 10 cigarettes con-taining 1.3 mg of nicotine, 16.5 mg of tar, and 15.2 mgof carbon monoxide each, was pumped into the cham-ber. Ligatures were placed, under general anesthesiaobtained by intramuscular administration of ketamine(0.5 ml/kg), around one of the mandibular first molarsof each animal. The ligature was left in position for 60days before the sacrifice of the animals. The serumlevels of nicotine and cotinine obtained using thismodel have been previously reported.27
Radiographic AnalysisImmediately after sacrifice, the jaws were removed andradiographed‡ with an exposure time of 0.3 seconds(60 Kvp, 10 mA) and 31 × 41 mm radiographic film.§
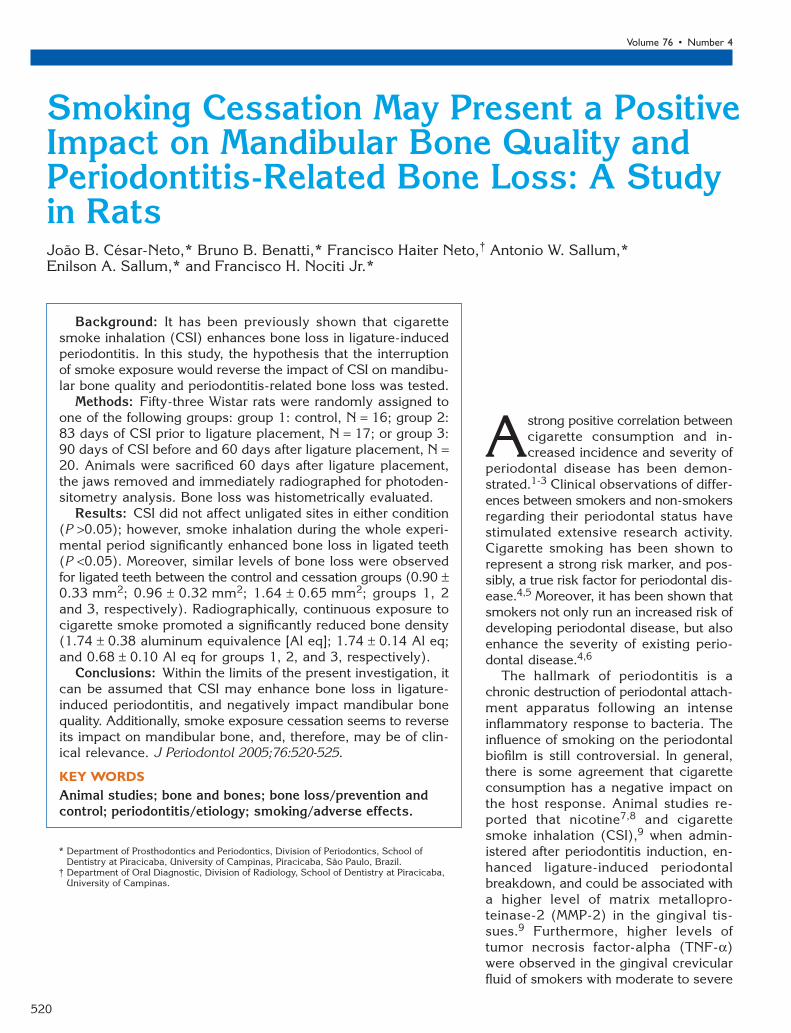
A reference radiograph of an aluminum step-wedgewas then taken using the same apparatus and expo-sure time. The films were developed in an automaticprocessing machine� and the optical density was mea-sured with a densitometer¶ with an aperture of approx-imately 2 mm. Five measurements were performed inthe mandible (Fig. 2). The optical density of the step-wedge was also evaluated in order to express theresults in aluminum equivalence (Al eq).
Figure 1.Schematic illustration of the experimental design.
‡ GE 1000, General Electric Co., Milwaukee, WI.§ Insight Film, Eastman Kodak, Rochester, NY.� Gendex GXP Dental X-Ray Processor, Des Plaines, IL.¶ MRA Equipamentos Electrônicos, Ribeirão Preto, SP, Brazil.
40138.qxd 4/18/05 8:49 AM Page 521
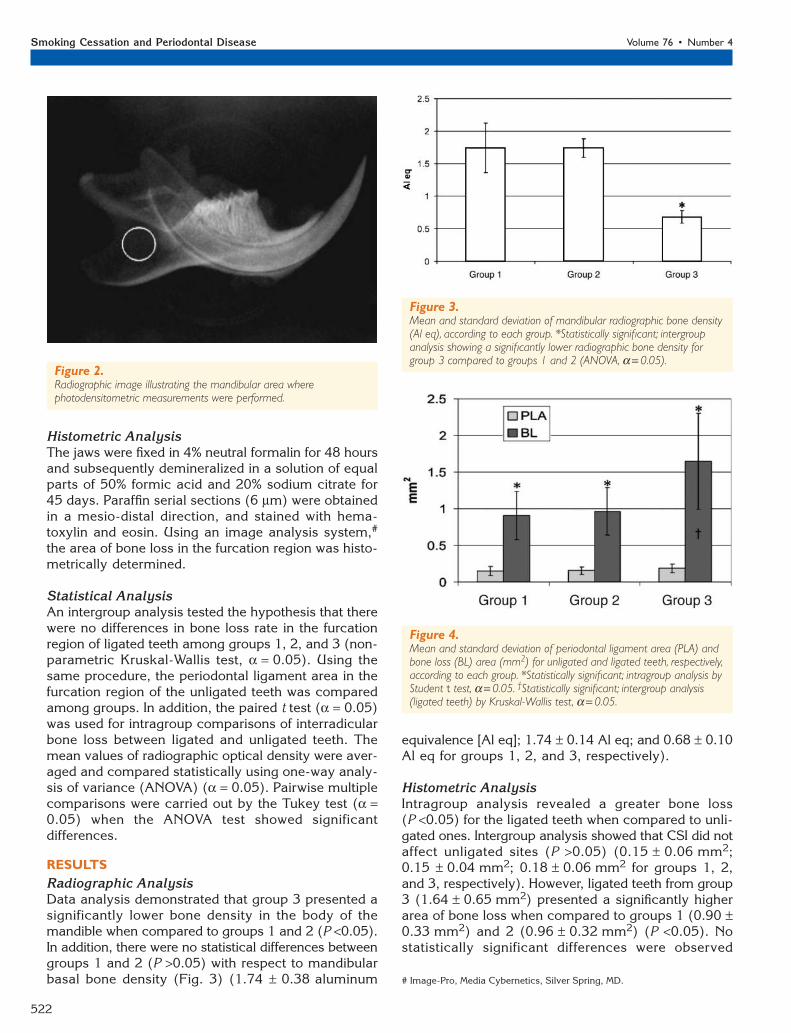
Figure 4.Mean and standard deviation of periodontal ligament area (PLA) andbone loss (BL) area (mm2) for unligated and ligated teeth, respectively,according to each group. *Statistically significant; intragroup analysis byStudent t test, α = 0.05. †Statistically significant; intergroup analysis(ligated teeth) by Kruskal-Wallis test, α = 0.05.
522
Smoking Cessation and Periodontal Disease Volume 76 • Number 4
Figure 2.Radiographic image illustrating the mandibular area wherephotodensitometric measurements were performed.
Figure 3.Mean and standard deviation of mandibular radiographic bone density(Al eq), according to each group. *Statistically significant; intergroupanalysis showing a significantly lower radiographic bone density forgroup 3 compared to groups 1 and 2 (ANOVA, α = 0.05).
Histometric AnalysisThe jaws were fixed in 4% neutral formalin for 48 hoursand subsequently demineralized in a solution of equalparts of 50% formic acid and 20% sodium citrate for45 days. Paraffin serial sections (6 µm) were obtainedin a mesio-distal direction, and stained with hema-toxylin and eosin. Using an image analysis system,#
the area of bone loss in the furcation region was histo-metrically determined.
Statistical AnalysisAn intergroup analysis tested the hypothesis that therewere no differences in bone loss rate in the furcationregion of ligated teeth among groups 1, 2, and 3 (non-parametric Kruskal-Wallis test, α = 0.05). Using thesame procedure, the periodontal ligament area in thefurcation region of the unligated teeth was comparedamong groups. In addition, the paired t test (α = 0.05)was used for intragroup comparisons of interradicularbone loss between ligated and unligated teeth. Themean values of radiographic optical density were aver-aged and compared statistically using one-way analy-sis of variance (ANOVA) (α = 0.05). Pairwise multiplecomparisons were carried out by the Tukey test (α =0.05) when the ANOVA test showed significantdifferences.
RESULTSRadiographic AnalysisData analysis demonstrated that group 3 presented asignificantly lower bone density in the body of themandible when compared to groups 1 and 2 (P <0.05).In addition, there were no statistical differences betweengroups 1 and 2 (P >0.05) with respect to mandibularbasal bone density (Fig. 3) (1.74 ± 0.38 aluminum
equivalence [Al eq]; 1.74 ± 0.14 Al eq; and 0.68 ± 0.10Al eq for groups 1, 2, and 3, respectively).
Histometric AnalysisIntragroup analysis revealed a greater bone loss(P <0.05) for the ligated teeth when compared to unli-gated ones. Intergroup analysis showed that CSI did notaffect unligated sites (P >0.05) (0.15 ± 0.06 mm2;0.15 ± 0.04 mm2; 0.18 ± 0.06 mm2 for groups 1, 2,and 3, respectively). However, ligated teeth from group3 (1.64 ± 0.65 mm2) presented a significantly higherarea of bone loss when compared to groups 1 (0.90 ±0.33 mm2) and 2 (0.96 ± 0.32 mm2) (P <0.05). Nostatistically significant differences were observed
# Image-Pro, Media Cybernetics, Silver Spring, MD.
40138.qxd 4/18/05 8:49 AM Page 522
523
J Periodontol • April 2005 César-Neto, Benatti, Neto, Sallum, Sallum, Nociti
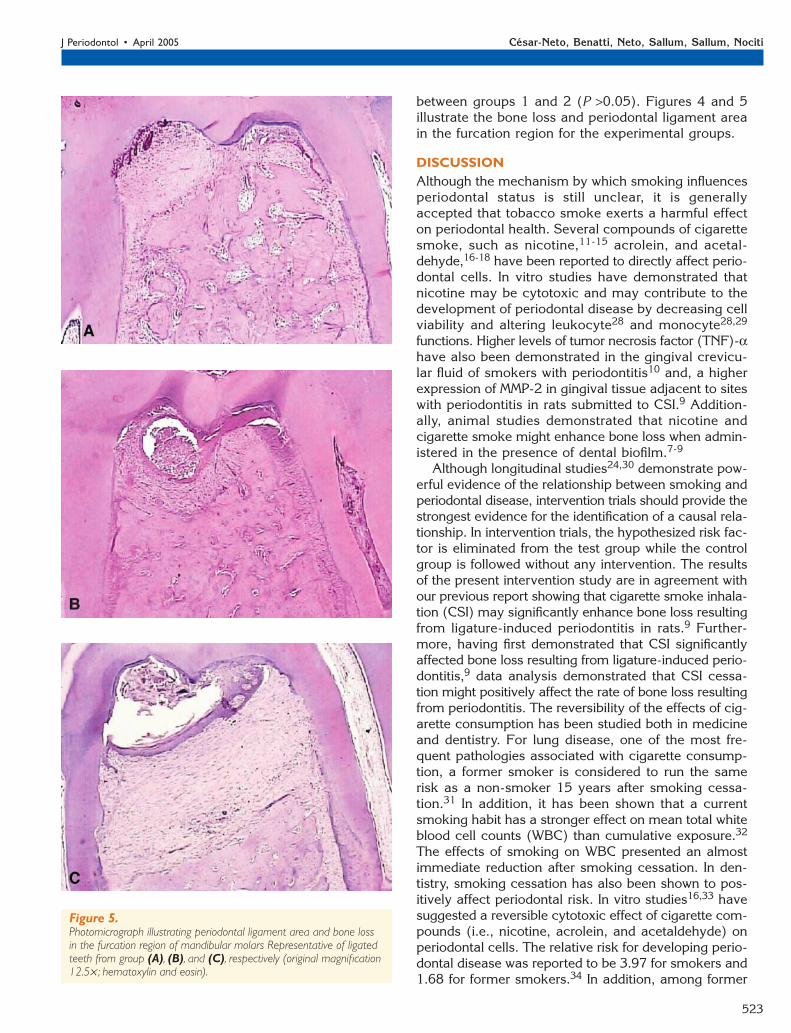
Figure 5.Photomicrograph illustrating periodontal ligament area and bone lossin the furcation region of mandibular molars Representative of ligatedteeth from group (A), (B), and (C), respectively (original magnification12.5× ; hematoxylin and eosin).
between groups 1 and 2 (P >0.05). Figures 4 and 5 illustrate the bone loss and periodontal ligament areain the furcation region for the experimental groups.
DISCUSSIONAlthough the mechanism by which smoking influencesperiodontal status is still unclear, it is generallyaccepted that tobacco smoke exerts a harmful effecton periodontal health. Several compounds of cigarettesmoke, such as nicotine,11-15 acrolein, and acetal-dehyde,16-18 have been reported to directly affect perio-dontal cells. In vitro studies have demonstrated thatnicotine may be cytotoxic and may contribute to thedevelopment of periodontal disease by decreasing cellviability and altering leukocyte28 and monocyte28,29
functions. Higher levels of tumor necrosis factor (TNF)-αhave also been demonstrated in the gingival crevicu-lar fluid of smokers with periodontitis10 and, a higherexpression of MMP-2 in gingival tissue adjacent to siteswith periodontitis in rats submitted to CSI.9 Addition-ally, animal studies demonstrated that nicotine andcigarette smoke might enhance bone loss when admin-istered in the presence of dental biofilm.7-9
Although longitudinal studies24,30 demonstrate pow-erful evidence of the relationship between smoking andperiodontal disease, intervention trials should provide thestrongest evidence for the identification of a causal rela-tionship. In intervention trials, the hypothesized risk fac-tor is eliminated from the test group while the controlgroup is followed without any intervention. The resultsof the present intervention study are in agreement withour previous report showing that cigarette smoke inhala-tion (CSI) may significantly enhance bone loss resultingfrom ligature-induced periodontitis in rats.9 Further-more, having first demonstrated that CSI significantlyaffected bone loss resulting from ligature-induced perio-dontitis,9 data analysis demonstrated that CSI cessa-tion might positively affect the rate of bone loss resultingfrom periodontitis. The reversibility of the effects of cig-arette consumption has been studied both in medicineand dentistry. For lung disease, one of the most fre-quent pathologies associated with cigarette consump-tion, a former smoker is considered to run the samerisk as a non-smoker 15 years after smoking cessa-tion.31 In addition, it has been shown that a currentsmoking habit has a stronger effect on mean total whiteblood cell counts (WBC) than cumulative exposure.32
The effects of smoking on WBC presented an almostimmediate reduction after smoking cessation. In den-tistry, smoking cessation has also been shown to pos-itively affect periodontal risk. In vitro studies16,33 havesuggested a reversible cytotoxic effect of cigarette com-pounds (i.e., nicotine, acrolein, and acetaldehyde) onperiodontal cells. The relative risk for developing perio-dontal disease was reported to be 3.97 for smokers and1.68 for former smokers.34 In addition, among former
40138.qxd 4/18/05 8:49 AM Page 523

524
Smoking Cessation and Periodontal Disease Volume 76 • Number 4
smokers, the risk decreased with the number of yearssince quitting (3.22 after 2 years and 1.15 after 11 years).In a prospective study over 20 years,24 507 individualswere radiographically evaluated and the results showedthose who stopped smoking during the experimentalperiod lost significantly less marginal bone when com-pared to current smokers. Another longitudinal study30
evaluated the changes in periodontal status of 101patients over 10 years. Clinically, an increased frequencyin diseased sites was observed in smokers, while for-mer and non-smokers presented decreased and simi-lar frequencies. Radiographically, an increased boneloss was noted for current smokers when compared toformer and non-smokers. No significant differences wereobserved between former and non-smokers. Moreover,smoking cessation has also been reported to be bene-ficial for periodontal treatment outcome. Grossi et al.35
demonstrated that former and non-smokers presentedsignificantly more healing and reduction of Tannerellaforsythensis and Porphyromonas gingivalis than cur-rent smokers. Therefore, the results of the present studyare in agreement with previous reports showing areversible condition promoted by cigarette consumption.
Misclassification of smoking status has been a con-cern in the literature,36 and is considered a confounderin epidemiological studies. Inaccurate reports mayoccur for many reasons such as individual metabolism,frequency of inhalation, depth of inhalation, capacity fordilution with room air, amount of cigarette stub left,and cigarette brand.37 Biochemical validation of smok-ing status seems to be useful in order to minimize theinfluence of confounders in clinical studies, mainly forthe determination of light, regular and heavy smokers.In animal studies, such confounders may be more accu-rately controlled. It has been previously reported27 thatthe CSI regimen used in the present study promotedcontinine serum levels closely correlated with smokerswho smoke between 10 to 20 cigarettes/day.3 How-ever, future comparisons with humans should be treatedwith caution, because of differences in the metabolismof nicotine between humans and rats, and the frequencyof smoke administration used in this study.
In the present investigation, radiographic analysisadditionally demonstrated that CSI significantly affectedmandibular bone density, leading to a lower opticaldensity of the mandibular bone. Furthermore, radio-graphic analysis suggests that the adverse effect ofCSI on mandibular bone may be reversible since therewas no significant difference between groups 1 (con-trol) and 2 (cessation). However, although the effectof smoke inhalation on bone density was clear on day150, caution should be used here since the experi-mental design used in the present study does not pro-vide absolute evidence that CSI affected bone densityon day 83. In addition, as shown in Figure 2, the read-ers should remember that the present study radio-
graphically examined loss of mandibular basal bonerather than bone loss around the teeth. Despite smok-ing being considered one of the main risk factors forosteoporosis, most studies did not report a correlationbetween nicotine administration and lower bone den-sity.38-42 Akhter et al.38 suggested that tobacco agentsother than nicotine are responsible for the decreasedbone density and increased fracture risk observed insmokers. Similarly, it has been reported that smokeexposure may affect mineralized tissue in healingareas25,27 and around titanium implants placed in rattibiae.26 Therefore, the results of the present investi-gation support the hypothesis that smoking maydecrease bone density not only in areas of new boneformation, and suggests that the mandibular bone mayalso be affected. Additional studies should be consi-dered in order to further investigate the interactionsbetween smoking and mandibular bone density, espe-cially because it may be of great clinical significancein the dental implant field and whether the influenceof smoking on mandibular bone density may alsoaccount for the increased bone loss resulting fromligature-induced periodontitis.
In conclusion, within the limits of the present study,data analysis suggests that smoking cessation shouldbe considered when dealing with individuals diagnosedwith periodontitis or when mandibular bone density isan important issue for clinical procedures.
ACKNOWLEDGMENTDr. César-Neto was supported by the São Paulo StateFoundation (FAPESP, Brazil 02/08554-0).
REFERENCES1. Bergstrom J. Cigarette smoking as a risk factor in
chronic periodontal disease. Communuity Dent Oral Epi-demiol 1989;17:245-247.
2. Bergstrom J, Eliasson S. Noxious effect of cigarettesmoking on periodontal health. J Periodontal Res 1987;22:513-517.
3. Gonzalez YM, De Nardin A, Grossi SG, Machtei EE,Genco RJ, De Nardin E. Serum cotinine levels, smoking,and periodontal attachment loss. J Dent Res 1996;75:796-802.
4. Genco RJ. Current view of risk factors for periodontaldiseases. J Periodontol 1996;67:1041-1049.
5. Tonetti MS. Cigarette smoking and periodontal disease:Etiology and management of disease. Ann Periodontol1998;3:88-101.
6. Kinane DF, Radvar M. The effect of smoking on mecha-nical and antimicrobial therapy. J Periodontol 1997;68:467-472.
7. Nociti FH Jr, Nogueira-Filho GR, Primo MT, et al. Theinfluence of nicotine on the bone loss rate in ligature-induced periodontitis. A histometric study in rats. J Perio-dontol 2000;71:1460-1464.
8. Nociti FH Jr, Nogueira-Filho GR, Tramontina VA, et al.Histometric evaluation of the effect of nicotine admin-istration on periodontal breakdown: An in vivo study.J Periodontal Res 2001;36:361-366.
40138.qxd 4/18/05 8:49 AM Page 524

525
J Periodontol • April 2005 César-Neto, Benatti, Neto, Sallum, Sallum, Nociti
9. César-Neto JB, Souza AP, Barbieri D, Moreno H Jr,Sallum EA, Nociti FH Jr. Matrix metalloproteinase-2may be involved with increased bone loss associatedwith experimental periodontitis and smoking. A study inrats. J Periodontol 2004;75:995-1000.
10. Bostrom L, Linder LE, Bergstrom J. Smoking and crevic-ular fluid levels of IL-6 and TNF-α in periodontal disease.J Clin Periodontol 1999;26:352-357.
11. Walker LM, Preston MR, Magnay JL, Thomas PB, El HajAJ. Nicotinic regulation of c-fos and osteopontin expres-sion in human-derived osteoblast-like cells and humantrabecular bone organ culture. Bone 2001;28:603-608.
12. Yuhara S, Kasagi S, Inoue A, Otsuka E, Hirose S,Hagiwara H. Effects of nicotine on cultured cells suggestthat it can influence the formation and resorption ofbone. Eur J Pharmacol 1999;383:387-393.
13. James JA, Sayers NM, Drucker DB, Hull PS. Effectsof tobacco products on the attachment and growth ofperiodontal ligament fibroblasts. J Periodontol 1999;70:518-525.
14. Tanur E, McQuade MJ, McPherson JC, Al-Hashimi IH,Rivera-Hidalgo F. Effects of nicotine on the strength ofattachment of gingival fibroblasts to glass and non-diseasedhuman root surfaces. J Periodontol 2000;71:717-722.
15. Henemyre CL, Scales DK, Hokett SD, et al. Nicotinestimulates osteoclast resorption in a porcine marrow cellmodel. J Periodontol 2003;74:1440-1446.
16. Cattaneo V, Cetta G, Rota C, et al. Volatile componentsof cigarette smoke: Effect of acrolein and acetaldehydeon human gingival fibroblasts in vitro. J Periodontol 2000;71:425-432.
17. Rota MT, Poggi P, Boratto R. Human gingival fibroblastcytoskeleton is a target for volatile smoke components.J Periodontol 2001;72:709-713.
18. Poggi P, Rota MT, Boratto R. The volatile fraction ofcigarette smoke induces alterations in the human gin-gival fibroblast cytoskeleton. J Periodontal Res 2002;37:230-235.
19. Ryder MI, Saghizadeh M, Ding Y, Nguyen N, Soskolne A.Effects of tobacco smoke on the secretion of interleukin-1β, tumor necrosis factor-α, and transforming growthfactor-β from peripheral blood mononuclear cells. OralMicrobiol Immunol 2002;17:331-336.
20. Sorensen LT, Karlsmark T, Gottrup F. Abstinence fromsmoking reduces incisional wound infection: A ran-domized controlled trial. Ann Surg 2003;238:1-5.
21. Padubidri AN, Yetman R, Browne E, et al. Complicationsof postmastectomy breast reconstructions in smokers,ex-smokers, and nonsmokers. Plast Reconstr Surg 2001;107:342-351.
22. Weintraub JM, Willett WC, Rosner B, Colditz GA, SeddonJM, Hankinson SE. Smoking cessation and risk of cataractextraction among US women and men. Am J Epidemiol2002;155:72-79.
23. Glassman SD, Anagnost SC, Parker A, Burke D, JohnsonJR, Dimar JR. The effect of cigarette smoking andsmoking cessation on spinal fusion. Spine 2000;25:2608-2615.
24. Jansson L, Lavstedt S. Influence of smoking on mar-ginal bone loss and tooth loss – a prospective study over20 years. J Clin Periodontol 2002;29:750-756.
25. Nociti FH Jr., César-Neto JB, Carvalho MD, Sallum EA,Sallum AW. Intermittent cigarette smoke inhalation mayaffect bone volume around titanium implants in rats. JPeriodontol 2002;73:982-987.
26. Nociti FH Jr., César-Neto JB, Carvalho MD, Sallum EA.Bone density around titanium implants may be influ-
enced by intermittent cigarette smoke inhalation: Ahistometric study in rats. Int J Oral Maxillofac Implants2002;17:347-352.
27. Cesar-Neto JB, Duarte PM, Sallum EA, Barbieri D,Moreno H Jr, Nociti FH Jr. A comparative study on theeffect of nicotine administration and cigarette smokeinhalation on bone healing around titanium implants. JPeriodontol 2003;74:1454-1459.
28. Pabst MJ, Pabst KM, Collier JA, et al. Inhibition of neu-trophil and monocyte defensive functions by nicotine. JPeriodontol 1995;66:1047-1055.
29. Payne JB, Johnson GK, Reinhardt RA, et al. Nicotineeffects on PGE2 and IL-1β release by LPS-treated humanmonocytes. J Periodontal Res 1996;31:99-104.
30. Bergstrom J, Eliasson S, Dock J. A 10-year prospec-tive study of tobacco smoking and periodontal health.J Periodontol 2000;71:1338-1347.
31. Fielding JE. Smoking: Health effects and control (1).New Engl J Med 1985;313:491-498.
32. Smith MR, Kinmonth AL, Luben RN, et al. Smoking sta-tus and differential white cell count in men and womenin the EPIC-Norfolk population. Atherosclerosis 2003;169:331-337.
33. Peacock ME, Sutherland DE, Schuster GS, et al. Theeffect of nicotine on reproduction and attachment ofhuman gingival fibroblasts in vitro. J Periodontol 1993;64:658-665.
34. Tomar SL, Asma S. Smoking-attributable periodontitisin the United States: Findings from NHANES III. J Perio-dontol 2000;71:743-751.
35. Grossi SG, Zambon J, Machtei EE, et al. Effects ofsmoking and smoking cessation on healing aftermechanical periodontal therapy. J Am Dent Assoc 1997;128:599-607.
36. Scott DA, Palmer RM, Stapleton JA. Validation of smok-ing status in clinical research into inflammatory perio-dontal disease. J Clin Periodontol 2001;28:715-722.
37. Benowitz NL, Perez-Stable EJ, Fong I, Modin G, Herrera B,Jacob P 3rd. Ethnic differences in N-glucuronidationof nicotine and cotinine. J Pharmacol Exp Ther 1999;291:1196-1203.
38. Akhter MP, Iwaniec UT, Haynatzki GR, Fung YK, CullenDM, Recker RR. Effects of nicotine on bone mass andstrength in aged female rats. J Orthop Res 2003;21:14-19.
39. Nociti FH Jr, Stefani CM, Sallum EA, Duarte PM, SallumAW. Nicotine and bone density around titanium implants:A histometric study in rabbits. Implant Dent 2002;11:176-182.
40. Iwaniec UT, Fung YK, Cullen DM, Akhter MP, Haven MC,Schmid M. Effects of nicotine on bone and calciotropichormones in growing female rats. Calcif Tissue Int 2000;67:68-74.
41. Fung YK, Iwaniec U, Cullen DM, Akhter MP, Haven MC,Timmins P. Long-term effects of nicotine on bone andcalciotropic hormones in adult female rats. PharmacolToxicol 1999;85:181-187.
42. Syversen U, Nordsletten L, Falch JA, Madsen JE, NilsenOG, Waldum HL. Effect of lifelong nicotine inhalationon bone mass and mechanical properties in female ratfemurs. Calcif Tissue Int 1999;65:246-249.
Correspondence: Dr. Francisco H. Nociti Jr., Av. Limeira 901,Caixa Postal: 052, CEP: 13414-903, Piracicaba, SP, Brazil.Fax: 55-19-34210144; e-mail: [email protected].
Accepted for publication July 23, 2004.
40138.qxd 4/18/05 8:49 AM Page 525