small mammal exotic animal and wildlife nursing
TRANSCRIPT

Small mammal, exotic animal and wildlife nursing 171
Small mammal,exotic animal andwildlife nursingSharon Redrobe and Anna Meredith
This chapter is designed to give information on:
• The principal aspects of hospitalization of the exotic pet and wildlife patient• The common diseases of these animals• The main points of perioperative care of these species• Zoonoses of these species and how to minimize the risks associated with their handling• The correct administration of medicines to these species
88
Introduction
This chapter will deal with the group of small animalscommonly presented for veterinary treatment that are‘not cats or dogs’. This includes common pet smallmammals, birds and reptiles. The reptile group includessnakes, lizards and chelonians. The term chelonian refersto those reptiles that possess a shell (turtles, terrapinsand tortoises). Some native UK wild animals that arebrought into the veterinary surgery by the public willalso be considered.
All these animals require a different approach to inpatientcare from that given to dogs and cats. Correct veterinarynursing forms a vital part of the care of these patients andaffects whether treatment is successful or otherwise.
Hospitalization
• Weigh patients daily to evaluate body condition andclinical progress and to ensure accurate treatment dosage
• Handle correctly to minimize stress, trauma and injury toboth handler and animal
• Minimize handling to reduce stress (tame social species arean exception)
• Offer correct feed to stimulate the animal to eat and toprevent gastrointestinal upset and dietary deficiencies
• Ensure that each individual animal can be identifiedfrom the moment it is admitted to the veterinarysurgery. A description of the animal is sufficient insome cases; stickers with names may be affixed toreptile shells; and cages should be clearly labelled.Some species may be microchipped for permanentidentification (Figure 8.1).
Animal Suggested siteFish Midline, anterior to dorsal finAmphibians Lymphatic cavityReptiles It is recommended that tissue glue is
placed over the needle entry site in allreptiles
Chelonians Subcutaneously in left hindleg(intramuscularly in thin-skinnedspecies)
Subcutaneously in the tarsal area in giantspecies
Crocodilians Cranial to nuchal clusterLizards Left quadriceps muscle, or
subcutaneously in this area (all species)In very small species, subcutaneously onthe left side of the body
Snakes Subcutaneously, left nape of neck placedat twice the length of the head fromthe tip of the nose
Birds Left pectoral muscleExceptions: ostriches – pipping muscle;penguins – subcutaneously at base ofneck
Mammals Large: left mid neck subcutaneouslyMedium and small: between scapulae
8.1 Suggested sites for identificationmicrochip (based on guidelines of the BritishVeterinary Zoological Society)
Clinical parametersIt is important to be able to distinguish the normal from theabnormal animal. The level of activity or stress should be
172 Manual of Advanced Veterinary Nursing
taken into account when evaluating whether the rates for vitalsigns are within the normal range.
It is also important to examine the animal and gain anappreciation of body condition (e.g. obese, very thin) ratherthan rely on absolute figures for body weight.
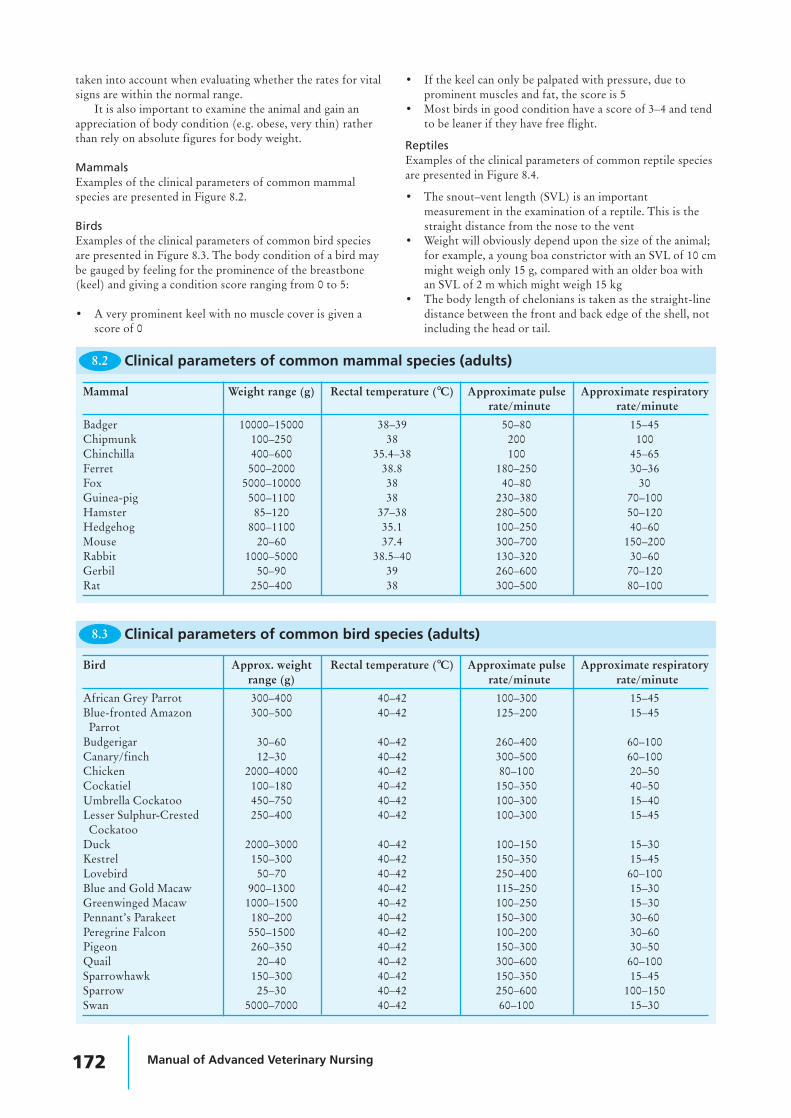
MammalsExamples of the clinical parameters of common mammalspecies are presented in Figure 8.2.
BirdsExamples of the clinical parameters of common bird speciesare presented in Figure 8.3. The body condition of a bird maybe gauged by feeling for the prominence of the breastbone(keel) and giving a condition score ranging from 0 to 5:
• A very prominent keel with no muscle cover is given ascore of 0
• If the keel can only be palpated with pressure, due toprominent muscles and fat, the score is 5
• Most birds in good condition have a score of 3–4 and tendto be leaner if they have free flight.
ReptilesExamples of the clinical parameters of common reptile speciesare presented in Figure 8.4.
• The snout–vent length (SVL) is an importantmeasurement in the examination of a reptile. This is thestraight distance from the nose to the vent
• Weight will obviously depend upon the size of the animal;for example, a young boa constrictor with an SVL of 10 cmmight weigh only 15 g, compared with an older boa withan SVL of 2 m which might weigh 15 kg
• The body length of chelonians is taken as the straight-linedistance between the front and back edge of the shell, notincluding the head or tail.
Mammal Weight range (g) Rectal temperature (°C) Approximate pulse Approximate respiratoryrate/minute rate/minute
Badger 10000–15000 38–39 50–80 15–45Chipmunk 100–250 38 200 100Chinchilla 400–600 35.4–38 100 45–65Ferret 500–2000 38.8 180–250 30–36Fox 5000–10000 38 40–80 30Guinea-pig 500–1100 38 230–380 70–100Hamster 85–120 37–38 280–500 50–120Hedgehog 800–1100 35.1 100–250 40–60Mouse 20–60 37.4 300–700 150–200Rabbit 1000–5000 38.5–40 130–320 30–60Gerbil 50–90 39 260–600 70–120Rat 250–400 38 300–500 80–100
8.2 Clinical parameters of common mammal species (adults)
Bird Approx. weight Rectal temperature (°C) Approximate pulse Approximate respiratoryrange (g) rate/minute rate/minute
African Grey Parrot 300–400 40–42 100–300 15–45Blue-fronted Amazon 300–500 40–42 125–200 15–45Parrot
Budgerigar 30–60 40–42 260–400 60–100Canary/finch 12–30 40–42 300–500 60–100Chicken 2000–4000 40–42 80–100 20–50Cockatiel 100–180 40–42 150–350 40–50Umbrella Cockatoo 450–750 40–42 100–300 15–40Lesser Sulphur-Crested 250–400 40–42 100–300 15–45Cockatoo
Duck 2000–3000 40–42 100–150 15–30Kestrel 150–300 40–42 150–350 15–45Lovebird 50–70 40–42 250–400 60–100Blue and Gold Macaw 900–1300 40–42 115–250 15–30Greenwinged Macaw 1000–1500 40–42 100–250 15–30Pennant’s Parakeet 180–200 40–42 150–300 30–60Peregrine Falcon 550–1500 40–42 100–200 30–60Pigeon 260–350 40–42 150–300 30–50Quail 20–40 40–42 300–600 60–100Sparrowhawk 150–300 40–42 150–350 15–45Sparrow 25–30 40–42 250–600 100–150Swan 5000–7000 40–42 60–100 15–30
Clinical parameters of common bird species (adults)8.3

Small mammal, exotic animal and wildlife nursing 173
Common name Species Typical SVL Weight Environmental Approx. pulse Approx.(cm) range (g) temperature rate/minute respiratory
range (°C) rate/minute
Boa Constrictor Boa constrictor 200–400 10000–18000 25–30 30–50 6–10
Cornsnake Elaphe guttata 100–180 150–250 25–30 40–50 6–10
Day Gecko Phelsuma 10–15 15–40 23–30 40–80 6–10cepediana
Garter Snake Thamnophis sp. 50–120 50–100 22–26 20–40 6–10
Green Iguana Iguana iguana 100–150 900–1500 26–36 30–60 10–30
Leopard Gecko Eublepharus 10 25–50 23–30 40–80 20–50macularius
Royal Python Python regius 80–150 400–800 25–30 30–50 6–10
Red-eared Terrapin Trachemys scripta 20 (shell 800–1200 20–30 40–60 2–10elegans length)
Mediterranean Testudo graeca 20–30 (shell 1000–2500 20–35 40–60 2–10(spur-thighed) length)Tortoise
8.4 Clinical parameters of common reptile species (SVL = snout–vent length of adult)
When calculating drug dosages, the whole weight of thechelonian is used. A common mistake is to attempt to deductthe weight of the shell. The shell is part of the skeleton –trying to ignore this weight is similar to trying to deduct theweight of a dog’s skeleton from its body weight whencalculating doses and is clearly not sensible.
Body condition is estimated from the soft tissue(muscle) covering the pelvis and tail bones – these bonesshould be barely visible. Figure 8.5 illustrates the tail of anemaciated green iguana. Some animals store fat in the tail(e.g. leopard gecko) and so the tail base should be thickerthan the pelvis width if the animal has adequate fat storage(Figure 8.6).
Reptiles regulate their internal body temperature bymoving between hot and cool areas in their enclosure. Thetemperatures listed reflect the normal temperature range towhich the animals should have access in order to regulatesuccessfully.
Note the high variation in ‘normal’ rates; for example,these are low when basking but higher when exercising orstressed. The level of activity or stress should be taken intoaccount when evaluating whether the rates are within thenormal range.
AmphibiansAmphibians can tolerate a wide range of environmentaltemperatures but the lower temperatures may beimmunosuppressive. Clinical parameters for common petamphibian species are given in Figure 8.7.
Common name Species Typical SVL Weight Environmental Approx. pulse Approx.(cm) range (g) temperature rate/minute respiratory
range (°C) rate/minuteCrested Newt Triturus cristatus 10 5–15 18–22 40–80 10–40Tiger Salamander Ambyostoma 10 100–150 15–25 40–80 5–40
tigrinumLeopard Frog Rana pipiens 8 50 15–25 60–80 50–80Tree Frog Hyla arborea 3 20–50 15–25 60–80 50–80
Clinical parameters of common amphibian species (SVL = snout–vent length of adult)8.7
8.5The tailbones arereadily visible inthis emaciatedGreen Iguana.
The tail of this well-fed LeopardGecko is wider than the pelvis.
8.6
174 Manual of Advanced Veterinary Nursing
Special techniques
Bandaging techniquesBandages are not required to cover lesions or wounds in allcases. They should be used only after due consideration of theadvantages and disadvantages of bandage application in aparticular situation.
In some cases the use of dressing or bandages can create aproblem: for example, the stress of repeated restraint toperform regular bandage changes can be detrimental to thewelfare of a captive wild animal. Some animals willconsistently chew a bandage but would not interfere with theunderlying lesion if it were left uncovered.
MammalsMany of the bandaging techniques used for domesticmammals can be applied to exotic mammals. Some individualswill not tolerate bandaging and will self-traumatize in an effortto remove the bandage. Certain rabbits will tolerate anElizabethan collar, whereas others will not; the use of theseappliances should be judged on a case-by-case basis.
BirdsMost birds will not remove subcutaneous sutures and sobandaging may not be necessary. Bandages should be placed soas not to restrict chest movements, or respiration will becompromised. The use of strong adhesive tape on the skinshould be avoided as avian skin is easily torn.
AmphibiansBandaging of amphibians is impractical and adhesive tapes willeasily damage the thin skin. The use of human oral ulcerbarrier creams on the skin will protect underlying lesions andseal the skin to prevent secondary infection.
FishBandaging of fish is impractical. The use of human oral ulcerbarrier creams on the skin will protect the underlying lesionsand reduce osmotic stress on the fish.
Assisted feeding and oral therapyIf the animal is bright and alert, warmed oral fluids may begiven. Oral rehydration fluids may be given daily equal to4–10% of body weight initially. Liquidized feed may be usedonce the animal is rehydrated. The general points concerningassisted feeding of animals are:
• A small amount of the food should also be available totempt the animal to self-feed
• To prevent digestive disturbances, an appropriate foodsubstance should be used – i.e. vegetable-based diets forherbivores, meat-based diets for carnivores.
MammalsMost mammals have a strong chewing response and willreadily feed from a syringe placed gently into the cornerof the mouth. Appropriate food substances should begiven; feeding the incorrect diet can lead to digestivedisturbances that may severely compromise the healthof an already sick animal.
The use of a nasogastric tube for assisted feeding is auseful technique in the supportive care of larger mammalsthat tolerate an amount of handling (e.g. rabbits, ferrets)(Figure 8.11).
Rabbits are obligate nose breathers, so avoidplacing a nasogastric tube in those animalsalready showing signs of respiratory distress,or they may be further compromised.
• Swimming upright• Smooth scales• No evidence of skin lesions• No rubbing• No petechiation
8.8 Signs of health in commonornamental fish
FishFish should be examined initially in the tank or pond, wheretheir behaviour should be noted. For closer examination,individual fish may then be transferred with some water into asmall clear plastic bag.
Checking the water quality is an important part of theinvestigation of disease in fish. Clinical parameters evaluatedin the examination of fish are presented in Figures 8.8 and8.9 along with the water parameters required to ensure fishhealth.
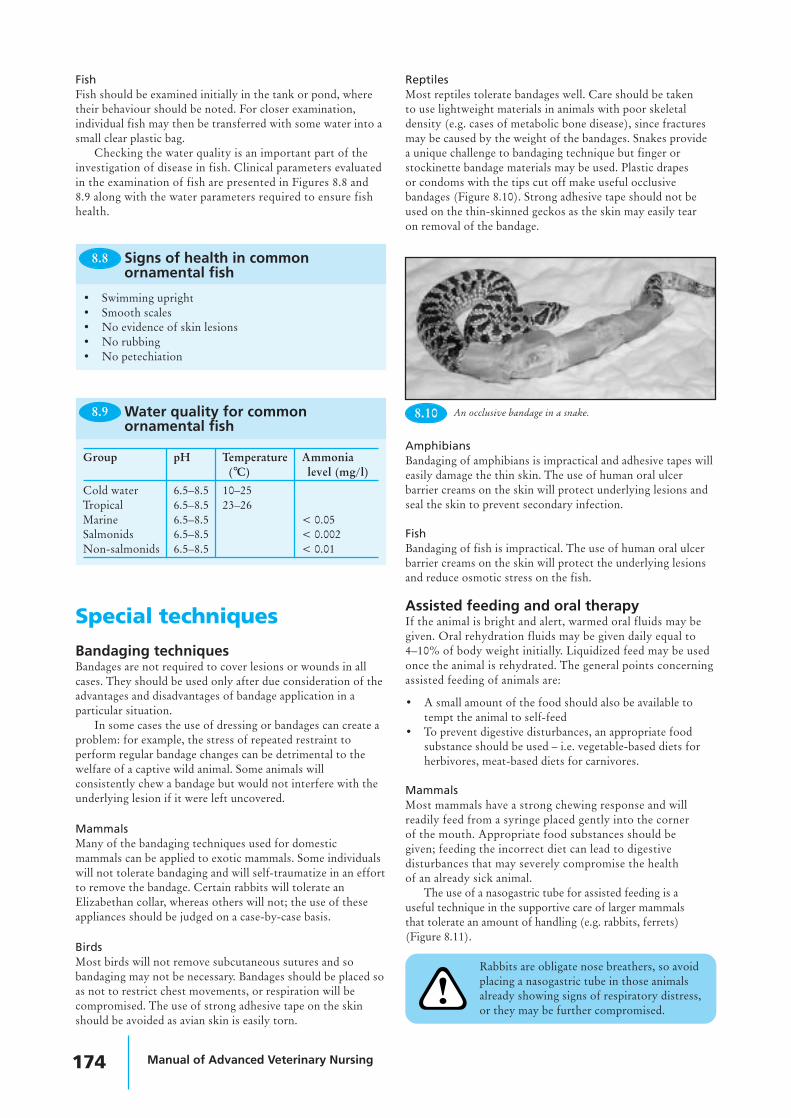
ReptilesMost reptiles tolerate bandages well. Care should be takento use lightweight materials in animals with poor skeletaldensity (e.g. cases of metabolic bone disease), since fracturesmay be caused by the weight of the bandages. Snakes providea unique challenge to bandaging technique but finger orstockinette bandage materials may be used. Plastic drapesor condoms with the tips cut off make useful occlusivebandages (Figure 8.10). Strong adhesive tape should not beused on the thin-skinned geckos as the skin may easily tearon removal of the bandage.
Water quality for commonornamental fish
8.9
Group pH Temperature Ammonia(°C) level (mg/l)
Cold water 6.5–8.5 10–25Tropical 6.5–8.5 23–26Marine 6.5–8.5 < 0.05Salmonids 6.5–8.5 < 0.002Non-salmonids 6.5–8.5 < 0.01
8.10 An occlusive bandage in a snake.
Small mammal, exotic animal and wildlife nursing 175
1. Sedate the animal or restrain safely2. Instil topical local anaesthetic drops into the nose and
allow to take effect3. Measure the distance from the nose to the position of
the stomach externally and mark the length on the tube4. Lubricate the tube with lubricant gel5. Gently introduce the tube into the ventral medial
aspect of the nostril and advance it into the nose6. If resistance is detected: stop, withdraw the tube,
relubricate and reposition7. Gently advance the tube until it is in the stomach as
indicated by the mark on the tube8. Check the tube is in place9. Glue the tube to the head using a flap of tape and tissue
glue10. Some animals will require a restriction collar to prevent
them pulling out the tube.
How to place a nasogastric tubein mammals
8.11
Never administer fluids into any nasogastric tube withoutfirst checking that it is in place. Many sick rabbits will passivelyinhale the tube. Check that the tube is in the stomach: eitheruse radiography (if a radiopaque feeding tube has been used) orquickly inject 5 ml of air into the tube whilst listening over thestomach area with a stethoscope for a ‘pop’ noise. Figure 8.12describes how to use a nasogastric tube safely.
1. Warm fluids to 38–40°C2. Restrain bird upright3. Extend neck4. Insert gag if using plastic crop tube, or use metal crop tube5. Insert crop tube into mouth at left oral commissure and
angle into right side of neck6. Palpate placement in crop7. Infuse fluid slowly8. Check during infusion for regurgitation, if seen release
bird immediately and allow bird to swallow
8.13 How to crop tube a bird
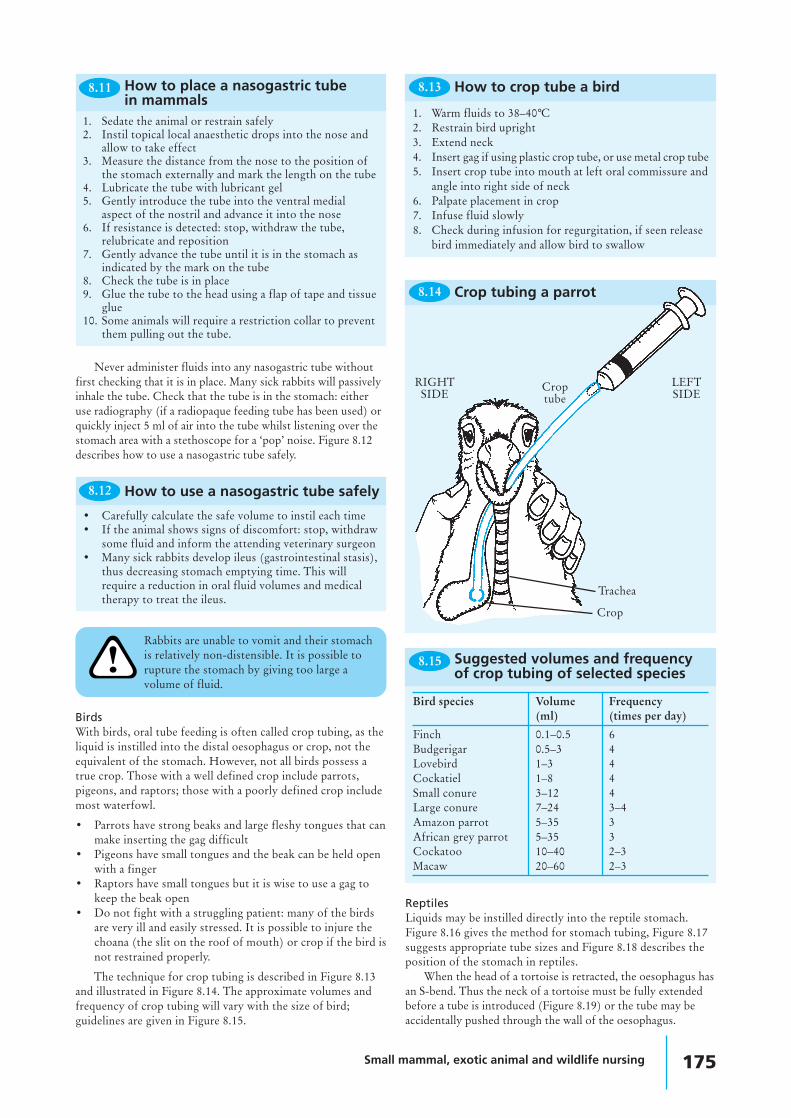
BirdsWith birds, oral tube feeding is often called crop tubing, as theliquid is instilled into the distal oesophagus or crop, not theequivalent of the stomach. However, not all birds possess atrue crop. Those with a well defined crop include parrots,pigeons, and raptors; those with a poorly defined crop includemost waterfowl.
• Parrots have strong beaks and large fleshy tongues that canmake inserting the gag difficult
• Pigeons have small tongues and the beak can be held openwith a finger
• Raptors have small tongues but it is wise to use a gag tokeep the beak open
• Do not fight with a struggling patient: many of the birdsare very ill and easily stressed. It is possible to injure thechoana (the slit on the roof of mouth) or crop if the bird isnot restrained properly.
The technique for crop tubing is described in Figure 8.13and illustrated in Figure 8.14. The approximate volumes andfrequency of crop tubing will vary with the size of bird;guidelines are given in Figure 8.15.
Bird species Volume Frequency(ml) (times per day)
Finch 0.1–0.5 6Budgerigar 0.5–3 4Lovebird 1–3 4Cockatiel 1–8 4Small conure 3–12 4Large conure 7–24 3–4Amazon parrot 5–35 3African grey parrot 5–35 3Cockatoo 10–40 2–3Macaw 20–60 2–3
Suggested volumes and frequencyof crop tubing of selected species
8.15
ReptilesLiquids may be instilled directly into the reptile stomach.Figure 8.16 gives the method for stomach tubing, Figure 8.17suggests appropriate tube sizes and Figure 8.18 describes theposition of the stomach in reptiles.
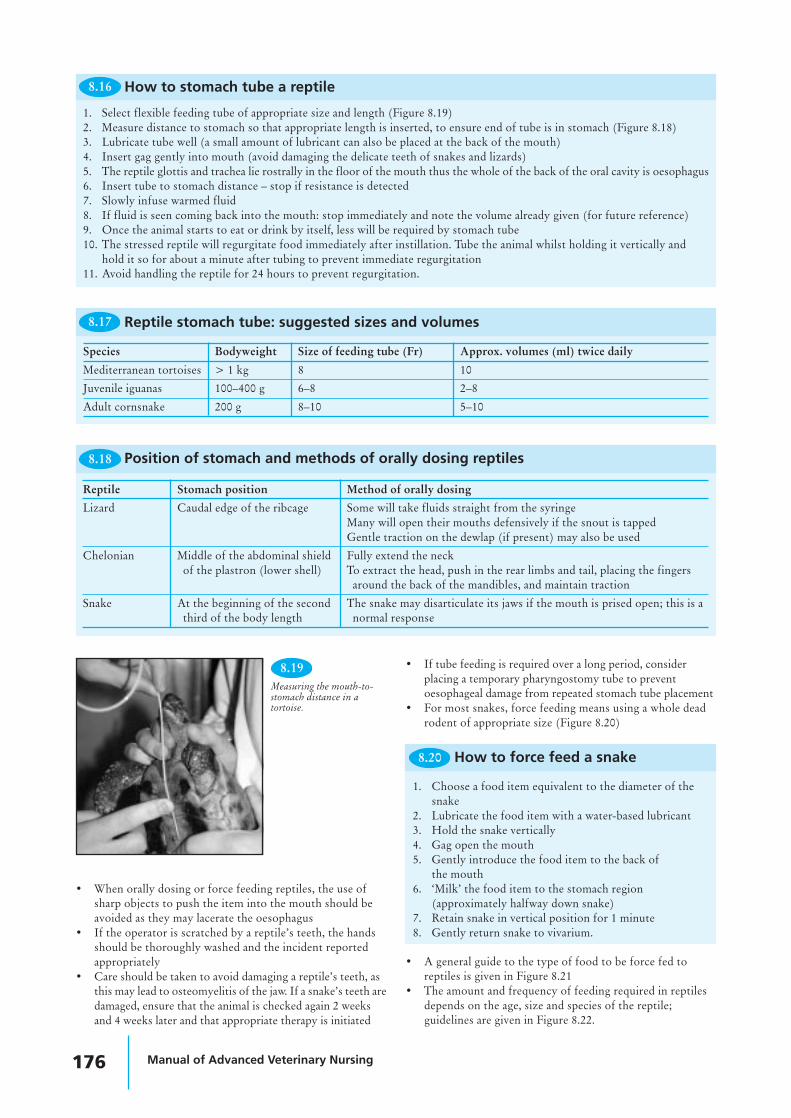
When the head of a tortoise is retracted, the oesophagus hasan S-bend. Thus the neck of a tortoise must be fully extendedbefore a tube is introduced (Figure 8.19) or the tube may beaccidentally pushed through the wall of the oesophagus.
Rabbits are unable to vomit and their stomachis relatively non-distensible. It is possible torupture the stomach by giving too large avolume of fluid.
• Carefully calculate the safe volume to instil each time• If the animal shows signs of discomfort: stop, withdraw
some fluid and inform the attending veterinary surgeon• Many sick rabbits develop ileus (gastrointestinal stasis),
thus decreasing stomach emptying time. This willrequire a reduction in oral fluid volumes and medicaltherapy to treat the ileus.
8.12 How to use a nasogastric tube safely
8.14 Crop tubing a parrot
RIGHTSIDE
Croptube
LEFTSIDE
Crop
Trachea
176 Manual of Advanced Veterinary Nursing
8.16
1. Select flexible feeding tube of appropriate size and length (Figure 8.19)2. Measure distance to stomach so that appropriate length is inserted, to ensure end of tube is in stomach (Figure 8.18)3. Lubricate tube well (a small amount of lubricant can also be placed at the back of the mouth)4. Insert gag gently into mouth (avoid damaging the delicate teeth of snakes and lizards)5. The reptile glottis and trachea lie rostrally in the floor of the mouth thus the whole of the back of the oral cavity is oesophagus6. Insert tube to stomach distance – stop if resistance is detected7. Slowly infuse warmed fluid8. If fluid is seen coming back into the mouth: stop immediately and note the volume already given (for future reference)9. Once the animal starts to eat or drink by itself, less will be required by stomach tube10. The stressed reptile will regurgitate food immediately after instillation. Tube the animal whilst holding it vertically and
hold it so for about a minute after tubing to prevent immediate regurgitation11. Avoid handling the reptile for 24 hours to prevent regurgitation.
How to stomach tube a reptile
8.17
Species Bodyweight Size of feeding tube (Fr) Approx. volumes (ml) twice daily
Mediterranean tortoises > 1 kg 8 10
Juvenile iguanas 100–400 g 6–8 2–8
Adult cornsnake 200 g 8–10 5–10
Reptile stomach tube: suggested sizes and volumes
8.18
Reptile Stomach position Method of orally dosing
Lizard Caudal edge of the ribcage Some will take fluids straight from the syringeMany will open their mouths defensively if the snout is tappedGentle traction on the dewlap (if present) may also be used
Chelonian Middle of the abdominal shield Fully extend the neckof the plastron (lower shell) To extract the head, push in the rear limbs and tail, placing the fingers
around the back of the mandibles, and maintain traction
Snake At the beginning of the second The snake may disarticulate its jaws if the mouth is prised open; this is athird of the body length normal response
Position of stomach and methods of orally dosing reptiles
1. Choose a food item equivalent to the diameter of thesnake
2. Lubricate the food item with a water-based lubricant3. Hold the snake vertically4. Gag open the mouth5. Gently introduce the food item to the back of
the mouth6. ‘Milk’ the food item to the stomach region
(approximately halfway down snake)7. Retain snake in vertical position for 1 minute8. Gently return snake to vivarium.
8.20 How to force feed a snake
• When orally dosing or force feeding reptiles, the use ofsharp objects to push the item into the mouth should beavoided as they may lacerate the oesophagus
• If the operator is scratched by a reptile’s teeth, the handsshould be thoroughly washed and the incident reportedappropriately
• Care should be taken to avoid damaging a reptile’s teeth, asthis may lead to osteomyelitis of the jaw. If a snake’s teeth aredamaged, ensure that the animal is checked again 2 weeksand 4 weeks later and that appropriate therapy is initiated
• If tube feeding is required over a long period, considerplacing a temporary pharyngostomy tube to preventoesophageal damage from repeated stomach tube placement
• For most snakes, force feeding means using a whole deadrodent of appropriate size (Figure 8.20)
• A general guide to the type of food to be force fed toreptiles is given in Figure 8.21
• The amount and frequency of feeding required in reptilesdepends on the age, size and species of the reptile;guidelines are given in Figure 8.22.
Measuring the mouth-to-stomach distance in atortoise.
8.19

Small mammal, exotic animal and wildlife nursing 177
Species Products for assisted feeding
Group Examples Diet Examples
Snakes Boas, pythons, rat snakes, gopher snakes, bull Meat-based Proprietary liquid meat products forsnakes, vipers, garter snakes, water snakes, dogs or catsracers, vine snakes
LizardsHerbivores Green iguanas Vegetable-based Purees, baby foodCarnivores Monitors, geckos, anoles, skinks, chameleons Meat-based Meat-based products
CheloniansCarnivores Turtles and terrapins Meat-based Meat-based productsHerbivores Tortoises Vegetable-based Purees, baby food
8.21 Type of food for assisted feeding of reptiles
Reptile Frequency
Small snakes and lizards Once or twice/week
Young of boas and pythons Three times/week
Herbivores Daily
Large snakes Once/2–4 weeks
Guide to feeding frequency forreptiles
8.22
Animal Site(s)
Small mammal Jugular (ferret, rabbit, chinchilla)Marginal ear vein (rabbit)Cephalic (rabbit, chinchilla, guinea-pig)Lateral tail vein (rodents)
Bird Jugular, brachial, medial metatarsal
Snakes Ventral tail vein, jugular vein, cardiac
Lizard Ventral tail vein, jugular vein
Chelonian Jugular vein, dorsal tail vein
Amphibian Central ventral abdominal vein, cardiac
Fish Caudal vein
Intravenous injection and bloodsampling sites
8.23
AmphibiansFood may be placed directly into the mouth of an amphibian.It will usually be swallowed if it is placed at the back of themouth. Care must be taken not to damage the delicate skinwhen attempting to open the mouth to introduce feed.
Administration of medicines
Oral routeThe methods described above for assisted feeding are alsoapplicable to individual oral dosing of animals. These are themost accurate methods of oral administration of drugs.
Administering drugs in the drinking water is of limiteduse. Success of treatment using this method depends upon:
• The amount of water consumed – most psittacines andreptiles drink too little to make this a useful option
• The oral bioavailability of the drug – if the drug is notabsorbed from the gastrointestinal tract then it can only beused to treat gut infections using this method.
BirdsProprietary medicated seed is available to treat birds. It isdifficult to assess an accurate dose for the bird as not all theseed offered may be eaten. This method is obviously notsuitable for the anorexic or non-seed-eating bird.
AmphibiansAmphibians may be dosed from a syringe placed directly intothe mouth.
FishSome types of medicated fish feed are commercially available.Homemade medicated feed can be produced by combiningfish flakes and the required drug with gelatine. A dose of
medicine per fish is calculated and the amount of food thefish will eat is assessed. The concentration of drug to be usedin the feed is then calculated. The necessary amount ofgelatine is made up with water to which the drug has beenadded. Fish flakes are then added to the liquid mixture; themixture is allowed to set and then grated for feeding to thefish at the required dose.
Intravenous routeFigure 8.23 lists accessible intravenous sites. These may beused for the introduction of fluids and drugs or forwithdrawing a blood sample.
MammalsThe use of the intravenous site to deliver fluids or drugsin small mammals is arguably only practical in the rabbit,where access to the marginal ear veins is relatively simple(Figures 8.24 and 8.25). It is useful to apply a localanaesthetic cream to the skin prior to venepuncture tominimize discomfort.
BirdsThree main intravenous sites are used in birds. The brachialvein is readily identified in the medial elbow (Figure 8.26) butis prone to haematoma formation after sampling. The medialmetatarsal vein (Figure 8.27) is less fragile and can be used inlarger birds. The right jugular vein is larger than the left. Eachjugular vein is located in a featherless tract on the neck and sois easily visualized.

178 Manual of Advanced Veterinary Nursing
1. Shave the lateral ear over the vein and prepare thesite aseptically
2. Apply local anaesthetic cream and leave forappropriate amount of time
3. Insert catheter of suitable size and glue inplace, using cyanoacrylate adhesive
4. Flush with heparin saline5. Pack inside of ear with roll of gauze and tape in place6. Connect catheter to giving set or mini extension set7. Apply Elizabethan collar to the rabbit if required.
How to place an intravenouscatheter in a rabbit
8.24
Rabbit with anintravenous infusionline in place.
8.25
8.28
1. Extend the neck fully by using continuous traction,placing fingers behind head. Sedation may be requiredfor strong patients
2. The vein runs from the tympanic membrane to the baseof the neck
3. The vein may be raised by placing a finger at the base ofthe neck
4. Insert the needle parallel to the neck into the vein5. After access, apply pressure to the site for a few
minutes to limit haematoma formation.
How to access the jugular vein inthe chelonian
1. Restrain the animal and hold the tail with the ventralaspect facing the operator
2. Insert the needle in the exact midline at a point distal tothe vent and hemipenes (if present)
3. Advance to touch ventral aspect of the tail vertebra (atright angles to tail in snake, at 45 degree angle in lizard)
4. Aspirate slowly and withdraw slightly until blood isseen in the hub of the needle.
8.30 How to access the ventral tail veinin a lizard or snake
1. Fully extend the tail2. Insert the needle into the exact midline of the dorsal
tail close to the shell3. Advance the needle to touch the vertebrae4. Aspirate the syringe and withdraw it slightly until
blood is seen in the hub of the needle.
8.33 How to access the dorsal tail veinin a tortoise
ReptilesThe choice of vein used for the intravenous sites dependsupon the type of reptile under consideration. The jugular veinis useful in chelonians (Figures 8.28 and 8.29), but access tothis vein requires a surgical cut-down in snakes and lizards; theventral tail vein is useful in snakes and lizards (Figures 8.30,8.31 and 8.32). Care must be taken if injecting into the dorsaltail vein of a chelonian (Figure 8.33) as the injection may beinadvertently placed in the epidural space and may producehindlimb paresis or paralysis. Intracardiac catheters may beplaced in snakes to access the circulation if the peripheral veinsare too small for ready access. Aseptic technique is requiredwhen accessing the veins or heart.
Metatarsal vein of aswan.
8.27
Brachial vein of apigeon.
8.26
Obtaining a jugularblood sample from atortoise.
8.29
Obtaining a ventraltail vein blood samplefrom an iguana.
8.32
Obtaining a ventraltail vein blood samplefrom a snake.
8.31
Small mammal, exotic animal and wildlife nursing 179
AmphibiansThe only accessible vein in amphibians is the central ventralabdominal vein. The heart may be accessed for blood samplingin the anaesthetized animal. The lymphatic system is a usefulsite for injection in amphibians and appears to be effective indelivering parenteral therapy. The site is dorsal, just off themidline of the body.
FishThe caudal vein in fish is accessed on the ventral aspect onthe midline, just cranial to the tail and caudal to the anal fin.The vein lies immediately ventral to the vertebral column. Themethod is similar to accessing the ventral tail vein of thesnake or lizard.
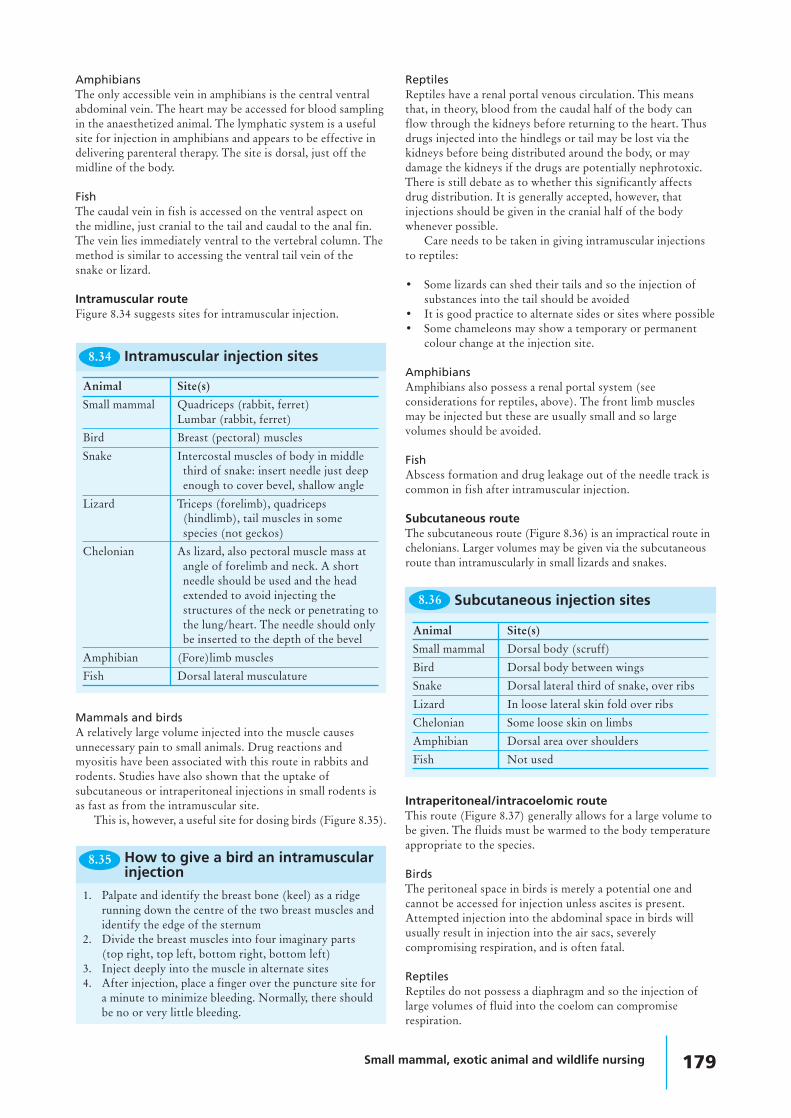
Intramuscular routeFigure 8.34 suggests sites for intramuscular injection.
ReptilesReptiles have a renal portal venous circulation. This meansthat, in theory, blood from the caudal half of the body canflow through the kidneys before returning to the heart. Thusdrugs injected into the hindlegs or tail may be lost via thekidneys before being distributed around the body, or maydamage the kidneys if the drugs are potentially nephrotoxic.There is still debate as to whether this significantly affectsdrug distribution. It is generally accepted, however, thatinjections should be given in the cranial half of the bodywhenever possible.
Care needs to be taken in giving intramuscular injectionsto reptiles:
• Some lizards can shed their tails and so the injection ofsubstances into the tail should be avoided
• It is good practice to alternate sides or sites where possible• Some chameleons may show a temporary or permanent
colour change at the injection site.
AmphibiansAmphibians also possess a renal portal system (seeconsiderations for reptiles, above). The front limb musclesmay be injected but these are usually small and so largevolumes should be avoided.
FishAbscess formation and drug leakage out of the needle track iscommon in fish after intramuscular injection.
Subcutaneous routeThe subcutaneous route (Figure 8.36) is an impractical route inchelonians. Larger volumes may be given via the subcutaneousroute than intramuscularly in small lizards and snakes.
Animal Site(s)
Small mammal Quadriceps (rabbit, ferret)Lumbar (rabbit, ferret)
Bird Breast (pectoral) muscles
Snake Intercostal muscles of body in middlethird of snake: insert needle just deepenough to cover bevel, shallow angle
Lizard Triceps (forelimb), quadriceps(hindlimb), tail muscles in somespecies (not geckos)
Chelonian As lizard, also pectoral muscle mass atangle of forelimb and neck. A shortneedle should be used and the headextended to avoid injecting thestructures of the neck or penetrating tothe lung/heart. The needle should onlybe inserted to the depth of the bevel
Amphibian (Fore)limb muscles
Fish Dorsal lateral musculature
8.34 Intramuscular injection sites
1. Palpate and identify the breast bone (keel) as a ridgerunning down the centre of the two breast muscles andidentify the edge of the sternum
2. Divide the breast muscles into four imaginary parts(top right, top left, bottom right, bottom left)
3. Inject deeply into the muscle in alternate sites4. After injection, place a finger over the puncture site for
a minute to minimize bleeding. Normally, there shouldbe no or very little bleeding.
8.35 How to give a bird an intramuscularinjection
Mammals and birdsA relatively large volume injected into the muscle causesunnecessary pain to small animals. Drug reactions andmyositis have been associated with this route in rabbits androdents. Studies have also shown that the uptake ofsubcutaneous or intraperitoneal injections in small rodents isas fast as from the intramuscular site.
This is, however, a useful site for dosing birds (Figure 8.35).
8.36
Animal Site(s)
Small mammal Dorsal body (scruff)
Bird Dorsal body between wings
Snake Dorsal lateral third of snake, over ribs
Lizard In loose lateral skin fold over ribs
Chelonian Some loose skin on limbs
Amphibian Dorsal area over shoulders
Fish Not used
Subcutaneous injection sites
Intraperitoneal/intracoelomic routeThis route (Figure 8.37) generally allows for a large volume tobe given. The fluids must be warmed to the body temperatureappropriate to the species.
BirdsThe peritoneal space in birds is merely a potential one andcannot be accessed for injection unless ascites is present.Attempted injection into the abdominal space in birds willusually result in injection into the air sacs, severelycompromising respiration, and is often fatal.
ReptilesReptiles do not possess a diaphragm and so the injection oflarge volumes of fluid into the coelom can compromiserespiration.
180 Manual of Advanced Veterinary Nursing
Intraosseous routeThe intraosseous route is a useful one for parenteral therapy,especially in small animals, because:
• Placing an intraosseous catheter or needle into a boneenables fluids to be given into the medullary cavity, whereabsorption is as rapid as the intravenous route
• Small veins are fragile and easily lacerated by catheters or‘blown’ when introducing fluids, whereas an intraosseouscatheter is stable in bone
• If the animal displaces or damages the intraosseouscatheter, it is unlikely to haemorrhage from this sitecompared with intravenous catheterization.
Figure 8.38 describes how to place an intraosseouscatheter; suggested sites for intraosseous catheters are given inFigure 8.39 and illustrated in Figure 8.40. The management ofan intraosseous catheter (Figure 8.41) is similar to thetechnique used to manage an intravenous catheter.
Animal SiteSmall mammal Proximal femur, proximal tibiaBird Distal radius, proximal tibiotarsusReptile Proximal or distal femur, proximal tibia;
bridge between carapace and plastronin chelonians
Suggested sites for intraosseouscatheters
8.39
• Use aseptic technique when giving drugs/fluids• To prevent clot formation, fill catheter with heparin or
heparinized saline between use• Flush three times daily with heparinized saline if not
used for drug or fluid administration.
8.41 How to manage an intraosseouscatheter
8.37
Animal Site(s)Small mammal Off midline, caudal to level of umbilicusBird
Snake Immediately cranial to vent on lateralbody wall
Lizard Off midline, caudal to ribs, cranial topelvis
Chelonian Extend hindlimb, inject cranial tohindlimb in fossa
Amphibian Ventrolateral quadrantFish Immediately rostral to vent on ventral
surface
Intraperitoneal/intracoelomicinjection sites
Not possible in healthyanimal – avoid as attemptsmay drown animal
1. Prepare site aseptically2. Inject local anaesthesia into site (unless animal is under
general anaesthesia)3. Introduce spinal needles or plain needles of appropriate
size into the bone (needle size sufficient to entermedullary cavity, based on knowledge or guided byradiographic image of cavity)
4. Flush with heparinized saline to ensure patency5. Secure in place with surgical cyanoacrylate adhesive or
suture6. Attach short extension tube7. Bandage area to maintain cleanliness and reduce
mobility of limb.
How to place an intraosseous catheter8.38
NebulizationThis is a useful technique for delivering drugs to the respiratorysystem. Drugs given by nebulization are not systemicallyabsorbed and so potentially nephrotoxic or hepatotoxic drugsmay be used relatively safely. This technique is especially usefulin the treatment of respiratory tract disease in birds and reptiles,where adequate drug levels may not reach the respiratory tractfollowing oral or parenteral dosing. It also minimizes the stressof handling and potential damage caused by repeated injections.The animal is placed in a chamber and nebulized with the drugfor an appropriate length of time (Figure 8.42). The nebulizermust generate particles of less than 3 microns in order to enterthe lower respiratory tract of birds.
Via the water environmentThis route can be used for fish, amphibians and aquaticinvertebrates.
• Antibiotics should not be administered via the water if abiological filtration system is in use
• The calcium present in hard water may chelate someantibiotics and so reduce their availability
• Many of the drugs used are toxic in high doses• Calculations of water volume and drug required must be
made accurately
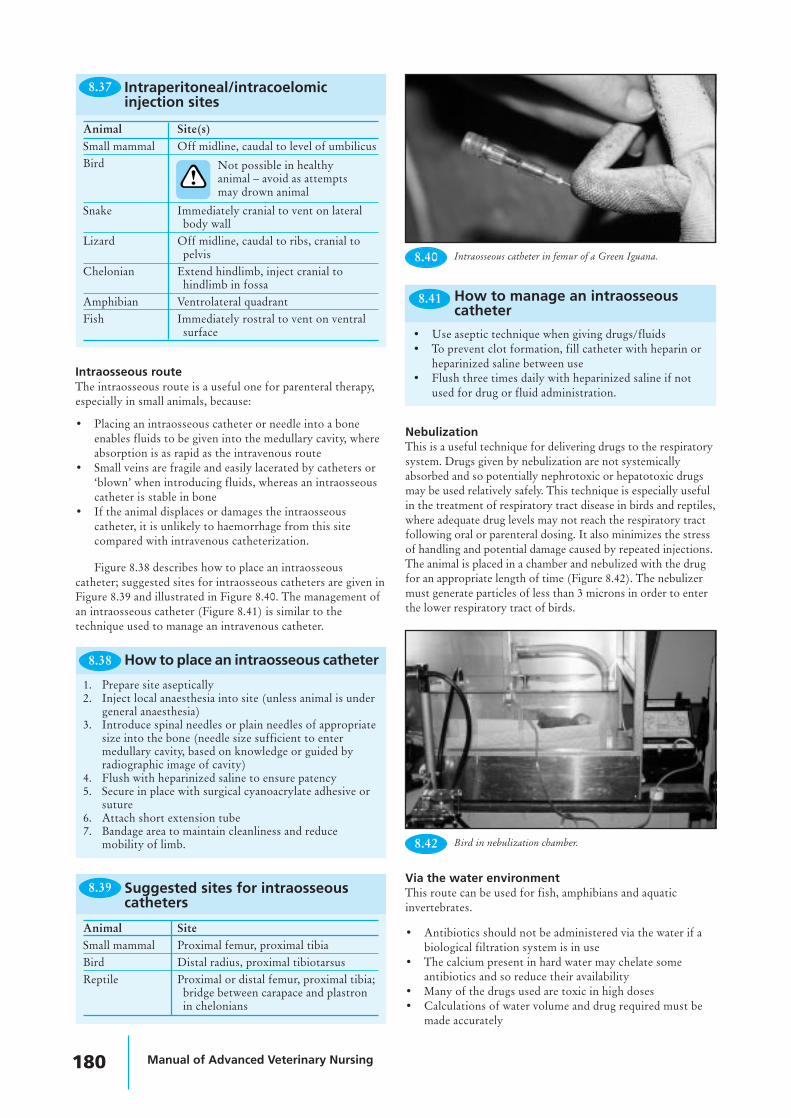
8.40 Intraosseous catheter in femur of a Green Iguana.
8.42 Bird in nebulization chamber.

Small mammal, exotic animal and wildlife nursing 181
• If possible, test the solution using a few animals beforedosing a large number
• Mix the water thoroughly to ensure that the drug is evenlydispersed
• Starve the animal for 24 hours before treatment.
There are two methods of administering drugs usingthe water:
• Dipping the animal into a strong solution for a shortperiod (usually administered in a separate ‘hospital tank’,then the animal is returned to its home environment)
• Bathing the animal in a weaker solution for a longerperiod. If the animal shows any signs of distress, thetreatment should be stopped. This may be performed inthe home tank to minimize disturbance, or in a separate‘hospital tank’.
Topical application of medicine
MammalsMammals commonly groom off any topical treatment,reducing its effectiveness. Any medication applied to the skinshould be non-toxic if ingested. Collars may be used toprevent the animal from removing the topical medication.
BirdsTopical medication should be applied to the skin, not feathers,of a bird. Collars may be tolerated by some animals and can beused to prevent ingestion of the medicine.
Weight of animal (g) Maximum safe volume ofblood to take (ml)
500 5
200 2
100 1
50 0.5
8.43 Guide to small animal weights andmaximum blood volume that maybe taken safely
ReptilesMost reptiles will tolerate topical therapy without groomingor licking the medicine. It is useful to bandage the area afterapplication to prevent the animal rubbing the medicine off;this is especially important in snakes.
AmphibiansMost topically applied medications will be systemicallyabsorbed by amphibians and so any wound dressings should beapplied with care. This route may therefore be used toadminister medicines. The dose should be carefully calculated.Ophthalmic drops are often used for this purpose.
Fluid therapy
• Volumes required are usually 1–2% of bodyweight• The advantages and disadvantages of subcutaneous,
intramuscular and intraperitoneal routes have beendescribed above
• Placement and maintenance of intravenous catheters is asfor larger domestic animals (see Figure 8.23 for descriptionof accessible veins)
• Intraosseous catheters are useful to administer fluids tosmaller animals or those in which a vein is not readilyaccessible (see Figure 8.39 for suggested sites and Figure8.38 for method of placement).
Blood samplingSee Figure 8.23 for blood sampling sites.
• Up to 10% of the blood volume may be safely taken froman animal. This must be carefully calculated using anaccurate weight when dealing with small animals (Figure8.43 gives examples)
• EDTA may lyse some avian and reptile cells• A fresh blood smear is useful when examining cell
morphology and checking for blood parasites• The laboratory should be contacted for guidance on
(minimum) sample volume and tubes required.
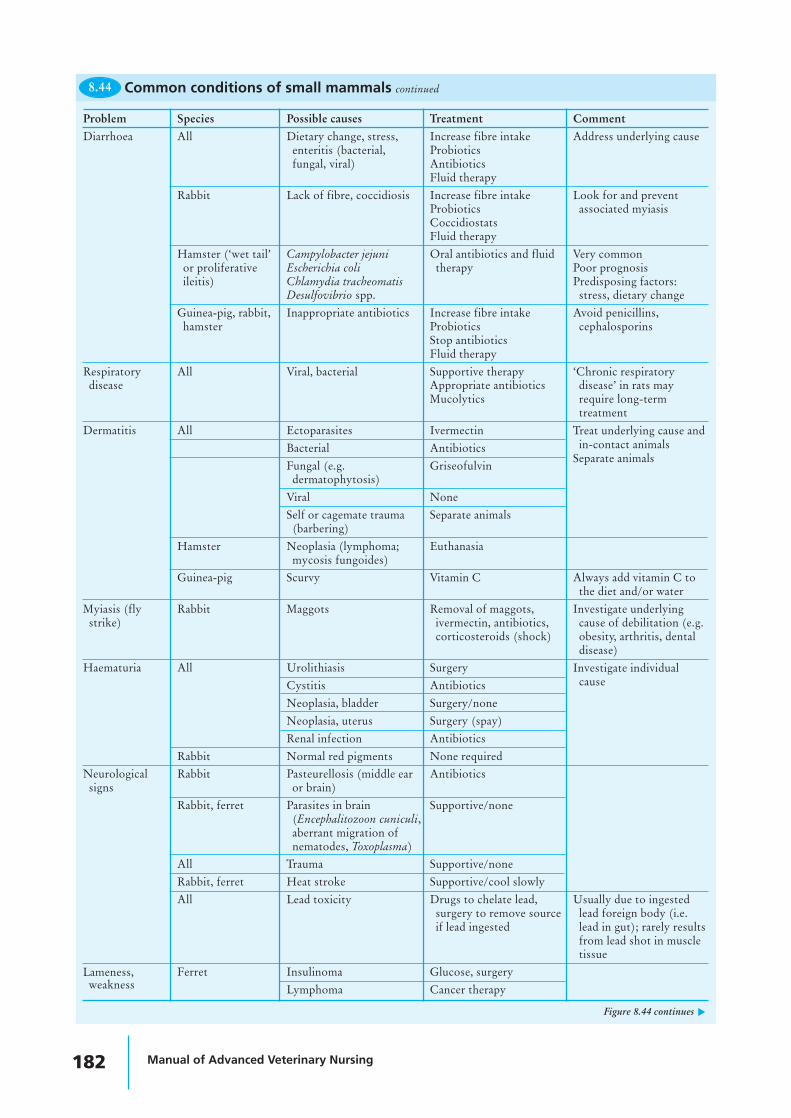
Common diseasesCommon diseases for various animals, along with their causesand treatment, are described in Figures 8.44–8.50.
Problem Species Possible causes Treatment CommentAnorexia All Urolithiasis Surgery when stable
All Renal disease, liver disease Supportive Especially older animalsGuinea-pig, young Change in diet or Reduce stress Very common in new petsrabbit, hamster environment Probiotics
Guinea-pig, Dental disease Burring/removal of Usually due to lack ofchinchilla, rabbit affected teeth dietary fibre or genetic
factorsGuinea-pig, rabbit Pregnancy toxaemia Corticosteroids Especially in obese animals
DextroseEmergency surgery
Rabbit Viral haemorrhagic disease None (fatal) Routine vaccinationVaccinate in-contact recommendedanimals
8.44 Common conditions of small mammals
Figure 8.44 continues ▼
182 Manual of Advanced Veterinary Nursing
Problem Species Possible causes Treatment CommentDiarrhoea All Dietary change, stress, Increase fibre intake Address underlying cause
enteritis (bacterial, Probioticsfungal, viral) Antibiotics
Fluid therapyRabbit Lack of fibre, coccidiosis Increase fibre intake Look for and prevent
Probiotics associated myiasisCoccidiostatsFluid therapy
Hamster (‘wet tail’ Campylobacter jejuni Oral antibiotics and fluid Very commonor proliferative Escherichia coli therapy Poor prognosisileitis) Chlamydia tracheomatis Predisposing factors:
Desulfovibrio spp. stress, dietary changeGuinea-pig, rabbit, Inappropriate antibiotics Increase fibre intake Avoid penicillins,hamster Probiotics cephalosporins
Stop antibioticsFluid therapy
Respiratory All Viral, bacterial Supportive therapy ‘Chronic respiratorydisease Appropriate antibiotics disease’ in rats may
Mucolytics require long-termtreatment
Dermatitis All Ectoparasites IvermectinBacterial AntibioticsFungal (e.g. Griseofulvindermatophytosis)
Viral NoneSelf or cagemate trauma Separate animals(barbering)
Hamster Neoplasia (lymphoma; Euthanasiamycosis fungoides)
Guinea-pig Scurvy Vitamin C Always add vitamin C tothe diet and/or water
Myiasis (fly Rabbit Maggots Removal of maggots, Investigate underlyingstrike) ivermectin, antibiotics, cause of debilitation (e.g.
corticosteroids (shock) obesity, arthritis, dentaldisease)
Haematuria All Urolithiasis SurgeryCystitis AntibioticsNeoplasia, bladder Surgery/noneNeoplasia, uterus Surgery (spay)Renal infection Antibiotics
Rabbit Normal red pigments None requiredNeurological Rabbit Pasteurellosis (middle ear Antibioticssigns or brain)
Rabbit, ferret Parasites in brain Supportive/none(Encephalitozoon cuniculi,aberrant migration ofnematodes, Toxoplasma)
All Trauma Supportive/noneRabbit, ferret Heat stroke Supportive/cool slowlyAll Lead toxicity Drugs to chelate lead, Usually due to ingested
surgery to remove source lead foreign body (i.e.if lead ingested lead in gut); rarely results
from lead shot in muscletissue
Ferret Insulinoma Glucose, surgeryLymphoma Cancer therapy
8.44 Common conditions of small mammals continued
Figure 8.44 continues ▼
Treat underlying cause andin-contact animals
Separate animals
Investigate individualcause
Lameness,weakness

Small mammal, exotic animal and wildlife nursing 183
Problem Species Possible causes Treatment CommentFerret continued Anaemia Specific therapy Common in entire
unmated female ferretswho develop persistentoestrus. May not respondto mating withvasectomized male
Aleutian disease (viral) None, supportiveCanine distemper None, supportive Vaccinate with canine
vaccineAll species, Pododermatitis As above, husbandry, May progress toespecially rat and (‘bumblefoot’) bandaging feet amyloidosis and renalrabbit failure
All species, Arthritis (limbs, spine) Analgesia,especially rat and anti-inflammatoriesrabbit
All Fractures, intervertebral Supportive, surgery ifdisc protrusion fractures, euthanasia if
spinalSubcutaneous Rabbit, rodents, Abscess Lance, drain, antibiotics, Facial abscesses in rabbitmasses ferret treat underlying cause often related to dental
infection or osteomyelitisGuinea-pig Cervical adenitis Surgical removal of
(Streptococcus infected lymph node(s),zooepidemicus) antibiotics, euthanasia
All Lipoma, other neoplasia SurgeryRabbit Myxomatosis Supportive, vaccinate Usually fatal
other animals in contactsGuinea-pig Sebaceous adenoma Surgery
Corneal ulcer All Trauma, entropion Antibiotics, surgeryRodents Viral infection of None; supportive (eye
lachrymal glands (SDAV) may perforate)Rodents Calcification of cornea NoneFerret Distemper, influenza Supportive
Ocular Rabbit Dacryocystitis (infection Flush ducts, antibiotics Check molar roots notdischarge of tear duct) impinging on duct
(radiography required toevaluate)
Chinchilla, rabbit Overgrown molar teeth Dental treatment Poor prognosisroots impinging on duct
Red staining All Stress, concurrent Treat underlying cause Known as porphyria/tears disease chromodacryorrhoea
8.44 Common conditions of small mammals continued
Lameness,weaknesscontinued
Problem Common clinical condition Treatment
Skin/face
Periocular swelling Ocular or sinus disorder Investigate and treat appropriately
Epiphora, conjunctivitis Ocular or sinus disorder, partial lid Investigate and treat appropriatelyparalysis (cockatiel), psittacosis (cockatiel,duck)
Scabs, scars, pustules Pox virus Vaccination of in-contacts
Brown hypertrophy of cere Endocrinopathy (budgerigars) None
Hyperkeratosis Cnemidocoptes spp. (mites) IvermectinCrusting of cere
8.45 Common conditions of birds
Figure 8.45 continues ▼
184 Manual of Advanced Veterinary Nursing
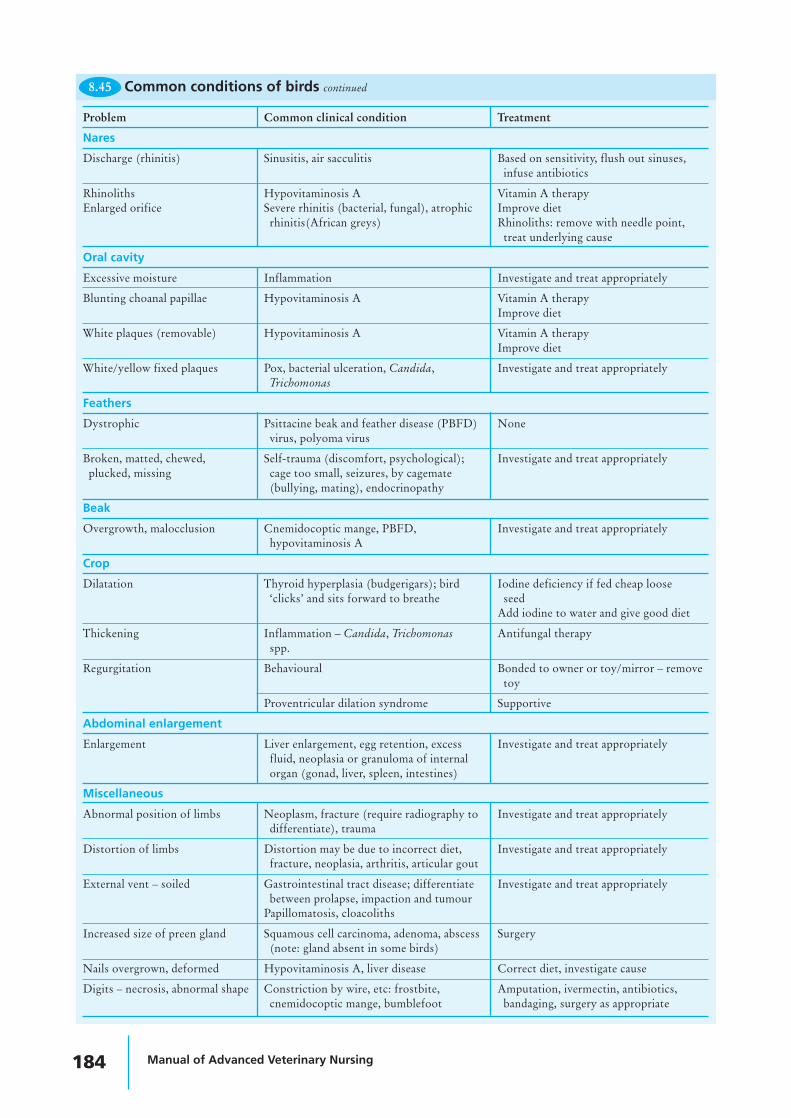
Problem Common clinical condition Treatment
Nares
Discharge (rhinitis) Sinusitis, air sacculitis Based on sensitivity, flush out sinuses,infuse antibiotics
Rhinoliths Hypovitaminosis A Vitamin A therapyEnlarged orifice Severe rhinitis (bacterial, fungal), atrophic Improve diet
rhinitis(African greys) Rhinoliths: remove with needle point,treat underlying cause
Oral cavity
Excessive moisture Inflammation Investigate and treat appropriately
Blunting choanal papillae Hypovitaminosis A Vitamin A therapyImprove diet
White plaques (removable) Hypovitaminosis A Vitamin A therapyImprove diet
White/yellow fixed plaques Pox, bacterial ulceration, Candida, Investigate and treat appropriatelyTrichomonas
Feathers
Dystrophic Psittacine beak and feather disease (PBFD) Nonevirus, polyoma virus
Broken, matted, chewed, Self-trauma (discomfort, psychological); Investigate and treat appropriatelyplucked, missing cage too small, seizures, by cagemate
(bullying, mating), endocrinopathy
Beak
Overgrowth, malocclusion Cnemidocoptic mange, PBFD, Investigate and treat appropriatelyhypovitaminosis A
Crop
Dilatation Thyroid hyperplasia (budgerigars); bird Iodine deficiency if fed cheap loose‘clicks’ and sits forward to breathe seed
Add iodine to water and give good diet
Thickening Inflammation – Candida, Trichomonas Antifungal therapyspp.
Regurgitation Behavioural Bonded to owner or toy/mirror – removetoy
Proventricular dilation syndrome Supportive
Abdominal enlargement
Enlargement Liver enlargement, egg retention, excess Investigate and treat appropriatelyfluid, neoplasia or granuloma of internalorgan (gonad, liver, spleen, intestines)
Miscellaneous
Abnormal position of limbs Neoplasm, fracture (require radiography to Investigate and treat appropriatelydifferentiate), trauma
Distortion of limbs Distortion may be due to incorrect diet, Investigate and treat appropriatelyfracture, neoplasia, arthritis, articular gout
External vent – soiled Gastrointestinal tract disease; differentiate Investigate and treat appropriatelybetween prolapse, impaction and tumour
Papillomatosis, cloacoliths
Increased size of preen gland Squamous cell carcinoma, adenoma, abscess Surgery(note: gland absent in some birds)
Nails overgrown, deformed Hypovitaminosis A, liver disease Correct diet, investigate cause
Digits – necrosis, abnormal shape Constriction by wire, etc: frostbite, Amputation, ivermectin, antibiotics,cnemidocoptic mange, bumblefoot bandaging, surgery as appropriate
8.45 Common conditions of birds continued
Small mammal, exotic animal and wildlife nursing 185
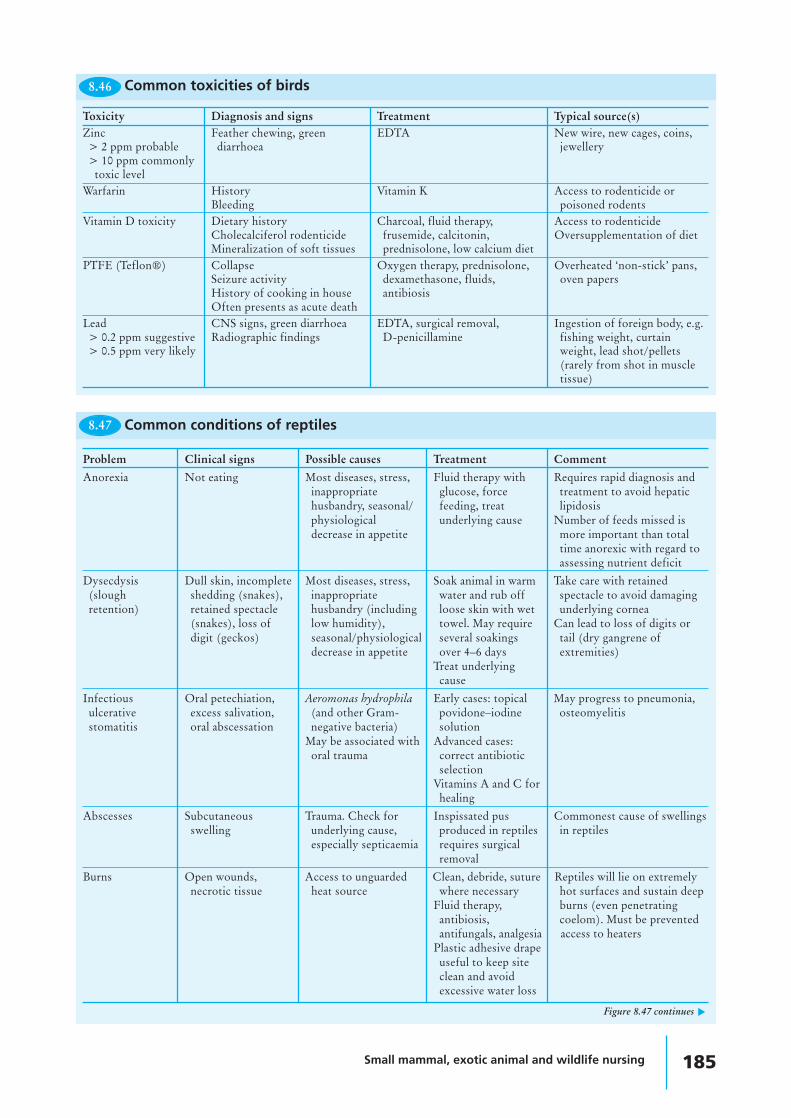
Toxicity Diagnosis and signs Treatment Typical source(s)Zinc Feather chewing, green EDTA New wire, new cages, coins,> 2 ppm probable diarrhoea jewellery> 10 ppm commonly
toxic levelWarfarin History Vitamin K Access to rodenticide or
Bleeding poisoned rodentsVitamin D toxicity Dietary history Charcoal, fluid therapy, Access to rodenticide
Cholecalciferol rodenticide frusemide, calcitonin, Oversupplementation of dietMineralization of soft tissues prednisolone, low calcium diet
PTFE (Teflon®) Collapse Oxygen therapy, prednisolone, Overheated ‘non-stick’ pans,Seizure activity dexamethasone, fluids, oven papersHistory of cooking in house antibiosisOften presents as acute death
Lead CNS signs, green diarrhoea EDTA, surgical removal, Ingestion of foreign body, e.g.> 0.2 ppm suggestive Radiographic findings D-penicillamine fishing weight, curtain> 0.5 ppm very likely weight, lead shot/pellets
(rarely from shot in muscletissue)
8.46 Common toxicities of birds
8.47 Common conditions of reptiles
Figure 8.47 continues ▼
Problem Clinical signs Possible causes Treatment Comment
Anorexia Not eating Most diseases, stress, Fluid therapy with Requires rapid diagnosis andinappropriate glucose, force treatment to avoid hepatichusbandry, seasonal/ feeding, treat lipidosisphysiological underlying cause Number of feeds missed isdecrease in appetite more important than total
time anorexic with regard toassessing nutrient deficit
Dysecdysis Dull skin, incomplete Most diseases, stress, Soak animal in warm Take care with retained(slough shedding (snakes), inappropriate water and rub off spectacle to avoid damagingretention) retained spectacle husbandry (including loose skin with wet underlying cornea
(snakes), loss of low humidity), towel. May require Can lead to loss of digits ordigit (geckos) seasonal/physiological several soakings tail (dry gangrene of
decrease in appetite over 4–6 days extremities)Treat underlyingcause
Infectious Oral petechiation, Aeromonas hydrophila Early cases: topical May progress to pneumonia,ulcerative excess salivation, (and other Gram- povidone–iodine osteomyelitisstomatitis oral abscessation negative bacteria) solution
May be associated with Advanced cases:oral trauma correct antibiotic
selectionVitamins A and C forhealing
Abscesses Subcutaneous Trauma. Check for Inspissated pus Commonest cause of swellingsswelling underlying cause, produced in reptiles in reptiles
especially septicaemia requires surgicalremoval
Burns Open wounds, Access to unguarded Clean, debride, suture Reptiles will lie on extremelynecrotic tissue heat source where necessary hot surfaces and sustain deep
Fluid therapy, burns (even penetratingantibiosis, coelom). Must be preventedantifungals, analgesia access to heaters
Plastic adhesive drapeuseful to keep siteclean and avoidexcessive water loss

186 Manual of Advanced Veterinary Nursing
8.47 Common conditions of reptiles continued
Problem Clinical signs Possible causes Treatment Comment
Nutritional Pathological fractures Calcium deficiency Correct diet and Educate owner in properosteodystrophy/ Lameness, weakness Improper husbandry, minimal husbandry of animalmetabolic bone Fibrous calcium:phosphorous handling, calciumdisease osteodystrophy ratio injections with fluid
Muscle tremors Lack of vitamin D3 therapySeizures Lack of ultraviolet lightTetany Protein deficiency
(disease of kidneys,liver, small intestine,thyroid orparathyroid – rare)
Vitamin A Swollen eyes Deficient diet (meat Vitamin A (correct Common in terrapinsdeficiency only) dose for weight) Renal damage may be fatal
Correct diet Overdosage results in skinsloughing
Vitamin B1 Neurological signs Deficient diet (e.g. fed Thiamine Common in garter snakesdeficiency (fitting, twitching) frozen fish without Correct diet Nervous system damage may
supplementing with be fatalB1) Cardiomyopathy may develop
Respiratory Nasal discharge, Poor husbandry Appropriate Reptiles do not possessdisease open-mouth Lack of exercise antimicrobial diaphragms so cannot cough
breathing, extended Poor ventilation Nebulization to expel debrisneck/head, cyanosis Incorrect temperature Coupage (hold upside
Bacterial, fungal down and tap bodyto expel debris fromlungs)
Correct husbandry
Dystocia Straining, lethargy Lack of nesting site Stabilize Common in captivity (lack ofCloacal discharge Oviduct infection Provision of nest site nesting site, poor husbandry)
Oversized eggs CalciumDebilitation Oxytocin if not
oversized eggSurgery
Pre-ovulatory Swollen abdomen, (Unknown) Supportive care in Common problem in captivefollicular stasis constipation, Lack of nesting site early stages and iguanas and some other
anorexia Poor nutritional status animal may ovulate, lizardsPoor husbandry for Advanced cases: Prophylactic ovariectomy tonesting stabilize and be recommended for these
ovariectomize species
Shell disease Pitted shell to large Poor husbandry Debride, appropriate Extensive defects must beshell defects with Trauma antimicrobial, repaired with acrylicunderlying Infection (bacterial, bandage, fibreglassosteomyelitis fungal) reconstruction
Correct husbandry
Cloacal prolapse Part of distal Calculi Treat underlyingintestinal tract Parasitism causeeverted Polyps Clean and replace
Infection prolapseDiarrhoea Amputate necroticObstruction of the tissuelower intestinal tract Retaining sutures
Post-hibernation Anorexia on Any concurrent disease Glucose saline i.p., PHA is not a diagnosisanorexia emergence from Frost damage to retina i.v. or i.o. Requires further investigation
hibernation Aural abscess Treat underlying to find underlying causeRhinitis causePneumonia

Small mammal, exotic animal and wildlife nursing 187
Problem Clinical signs Possible causes Treatment
Bloat Swollen body Gastric fermentation If air: remove by aspirationAir swallowing If fluid: treat underlying causePeritoneal effusions (infection, neoplasia)
Cloacal prolapse Organ protruding from Foreign body, parasites, masses, Treat underlying causevent gastroenteritis Replace prolapse
Diarrhoea Increased faecal output Bacterial infection Treat underlying causeParasites Supportive careToxins (e.g. lead, rancid feed)
Masses Masses in skin or Parasites Investigate causeinternal organs Bacteria Surgery or medical therapy
Mycobacterium Spontaneous tumours causedNeoplasia by Lucke tumour herpes virus
Corneal oedema Cloudy eye(s) Poor water quality Improve husbandryTrauma Treat underlying causeOcular infection
Corneal keratopathy White patches on Lipid keratopathy (high fat diet) Evaluate diet and husbandrycornea Trauma and amend as required
Poor water quality
Metabolic bone Curved limb bones Poor diet (low calcium, Correct diet and husbandrydisease Spinal deformities calcium:phosphorus imbalance,
Poor growth vitamin D deficiency)Fractures Lack of UV light
Poor condition Weight loss Parasites Treat underlying causePoor growth Bacterial/fungal systemic infection
8.48 Common conditions of amphibians
Problem Clinical signs Possible causes Treatment
Cataract Opacity of lens Nutritional deficiency (e.g. zinc, copper, None – treat underlying causeselenium)
Eye fluke
Corneal opacity Eye appears cloudy Trauma Treat underlying causeGas bubble traumaPoor water qualityNutritional imbalanceEye fluke
Exophthalmia Enlarged eye Spring viraemia of carp (see below) None – treat underlying causeSwim bladder inflammationSystemic infection
Vertebral deformity Deviation in spine, fish Nutritional deficiency (e.g. phosphorus, None – treat underlying causeswimming in circles vitamin C)
Respiratory distress Gasping, crowding at Low dissolved oxygen Treat underlying causeinlets Gill disease
Toxins in the waterAnaemia
Skin irritation Jumping, rubbing Ectoparasites Treat underlying causeToxins in water
White spots or As described Ichthyophthirius infection Treat underlying causecotton wool Saprolegnia infectionpatches on skin Cytophagia infection
Skin ulceration Loss of scales, deep or Nutritional imbalance Treat underlying causesuperficial defect, Trauma Surgically debride ulcer, applyunderlying muscles Ectoparasite barrier cream and administerexposed Bacterial/ fungal infection (Aeromonas parenteral antimicrobials as
salmonicida) requiredSystemic infection
Common conditions of fish8.49
Figure 8.49 continues ▼

188 Manual of Advanced Veterinary Nursing
Problem Clinical signs Possible causes Treatment‘Hole in the head Large erosions in head Hexamita Metronidazoledisease’
Fin rot Ragged fins, loss of fins Trauma Treat underlying causeCytophagia infectionSaprolegnia infectionAeromonas/Pseudomonas infectionEctoparasiteNutritional imbalance
Spring viraemia of Lethargy, dark skin, Virus (Rhabdovirus carpio) None. Notifiable in UK undercarp respiratory distress, the Diseases of Fish Act 1937
loss of balance, (as amended)abdominal distension,petechial haemorrhages
Common conditions of fish continued8.49
Problem Clinical signs Possible causes TreatmentTrauma Lost or damaged limbs Mishandling If losing haemolymph, surgical
Damaged body Attacks by others glue can be used to seal thedefect
Limbs may regenerateMinor injuries will heal at thenext slough
Alopecia Loss of hairs (especially Overhandling Reduce handlingspiders) Stress Provide hiding places in
Incorrect husbandry enclosureCorrect husbandry
Infectious disease Larvae become wet Bacteria Isolation of diseased stockAdults have diarrhoea, Fungi Improve husbandryexudates, discharges Viruses Quarantine new arrivals
Parasites Weight loss Parasitic wasps and flies Improve husbandry‘Eaten alive’ by parasites Nematodes Use effective barriersDeath Mites Mite treatment licensed for
beesNutritional Weight loss Incorrect food Provide correct feed and
Death Too little food conditionsPoor growth Incorrect humidity, temperature
Toxicity Death Accidental use of insect sprays or powders Remove toxin by ventilation,near invertebrates dust off animal, give bathing
facilities
Common conditions of invertebrates8.50
ZoonosesDiseases that can be transmitted from animal to human(zoonoses) are found in common domestic as well as ‘exotic’species. It is therefore wise to adopt appropriate precautionarymeasures with all species. Note that an animal can appearperfectly healthy but be carrying a disease that may affecthumans. Figure 8.51 lists some zoonoses and their symptomsin animals and humans.
Steps to decrease the risks of exposure to potentialzoonoses include the following.
• Appropriate protective clothing (e.g. hats, masks, gloves)should be worn
• Animals should not be ‘petted’ unnecessarily• Hands should be washed after handling an animal or its faeces• Care should be taken to rinse thoroughly any cuts, scratches
or bites incurred and they should be reported appropriately• It should be ensured that staff tetanus and other
appropriate vaccinations are up to date• The doctor should be made aware of staff contact with animals.
If an animal is suspected of, or confirmed to have, azoonotic disease:
• Euthanasia of the animal for public health reasons maybe considered and submission of its body for postmortem to check for the zoonotic disease underconsideration
• The animal may be treated (only after carefulconsideration of the first point)
• A minimal number of people should have contact withthat animal
• Only suitably trained staff should have contact withthat animal
• Appropriate precautions should be taken when in contactwith that animal
• If a zoonosis in a human is suspected, or staff have beenin contact with a zoonosis, the doctor should be informedas soon as possible
• Some diseases must be reported to the appropriateauthorities.

Small mammal, exotic animal and wildlife nursing 189
8.51
Dis
ease
Cau
sati
ve a
gent
Com
mon
Sign
s in
ani
mal
Sym
ptom
s in
hum
ans
Prec
auti
ons
requ
ired
anim
al h
osts
Rin
gwor
mM
icro
spor
um c
anis
Hed
geho
gSc
aly
patc
hes,
hai
r lo
ssSc
aly
patc
h of
ski
n, m
ay b
eW
ear
glov
es, c
hang
e cl
othe
s be
twee
n an
imal
sTr
ichp
hyto
n gy
pseu
mH
amst
erpr
urit
ic(A
ll ro
dent
s, ra
bbits
)Fe
rret
Scab
ies
Sarc
opte
s sca
biei
Ferr
et, f
ox,
Der
mat
itis
, pru
ritu
sD
erm
atit
is, p
ruri
tus
Wea
r gl
oves
rode
nts
Ces
todi
asis
/tap
ewor
mH
ymen
olep
is s
pp.
Mou
se, y
oung
rat
Wei
ght
loss
, con
stip
atio
nD
iarr
hoea
, con
stip
atio
nC
auti
on w
hen
hand
ling
anim
al o
r it
s fa
eces
Salm
onel
losi
sSa
lmon
ella
spp
.R
epti
les
Non
e, d
iarr
hoea
Dia
rrho
eaC
auti
on w
hen
hand
ling
anim
al o
r it
s fa
eces
Fox,
bad
ger,
ferr
etB
irds
Inve
rteb
rate
sC
rypt
ospo
ridi
osis
Cry
ptos
pori
dium
spp
.R
epti
les
Non
e, d
iarr
hoea
Dia
rrho
eaC
auti
on w
hen
hand
ling
anim
al o
r it
s fa
eces
Ferr
etT
hick
enin
g of
sto
mac
h(e
spec
ially
if h
uman
is im
mun
ocom
prom
ised
)m
ucos
a ca
usin
gre
gurg
itat
ion
in s
nake
sG
iard
iasi
sG
iard
ia s
pp.
Rep
tile
sN
one,
dia
rrho
eaD
iarr
hoea
, abd
omin
al p
ain,
Cau
tion
whe
n ha
ndlin
g an
imal
or
its
faec
esB
irds
sept
icae
mia
Ferr
etPs
itta
cosi
sC
hlam
ydia
psi
ttaci
Bir
dsN
one,
res
pira
tory
, let
harg
yH
eada
che,
feve
r, co
nfus
ion,
Wea
r m
ask/
resp
irat
ory
appa
ratu
s, g
love
s,m
yalg
ia, n
on-p
rodu
ctiv
ech
ange
of
clot
hing
coug
h, ly
mph
aden
opat
hyR
epor
tabl
e in
som
e ar
eas
Infl
uenz
a (’
flu)
Ort
hom
yxov
irus
Ferr
etSn
eezi
ng, n
asal
dis
char
ge,
Snee
zing
, nas
al d
isch
arge
, fev
erM
ask
feve
r, le
thar
gyle
thar
gyM
ore
com
mon
ly fr
om h
uman
to
ferr
etL
epto
spir
osis
Lep
tosp
ira
spp.
Ferr
et, r
oden
tsN
one
Seve
re ’f
lu-l
ike
sym
ptom
sA
void
con
tact
wit
h ur
ine
Am
phib
ians
Wea
r m
ask
and
glov
esTu
berc
ulos
isM
ycob
acte
rium
bov
is,
Ferr
et, b
adge
r, de
erN
one,
was
ting
, pne
umon
iaPn
eum
onia
, cou
ghW
ear
mas
k an
d gl
oves
M. t
uber
culo
sis
Fish
Not
ifia
ble
Am
phib
ians
Lym
phoc
ytic
Are
navi
rus
Rod
ents
Non
e, r
espi
rato
ry s
igns
,’F
lu-l
ike,
cho
riom
enin
giti
sVe
ry r
are
chor
iom
enin
giti
sC
NS
sign
sW
ear
mas
k an
d gl
oves
Han
tavi
rus
Han
tavi
rus
genu
sSm
all m
amm
als,
Non
eFe
ver,
vom
itin
g, h
aem
orrh
ages
,Ve
ry r
are
rode
nts
rena
l fai
lure
Rep
orte
d in
wild
rat
s in
UK
Rab
ies
Rha
bdov
irus
All
mam
mal
sC
NS
sign
sC
NS
sign
sN
ot e
ndem
ic in
UK
Non
eVa
ccin
ate
staf
f if a
t ri
skFu
ll ba
rrie
r pr
otec
tion
if s
uspe
cted
Not
ifia
ble
Cam
pylo
bact
erio
sis
Cam
pylo
bact
erB
irds
Non
e, d
iarr
hoea
Dia
rrho
eaC
auti
on w
hen
hand
ling
anim
al o
r it
s fa
eces
Co
mm
on
zo
on
ose
s

190 Manual of Advanced Veterinary Nursing
Perioperative carePreoperative care
• Every effort should be made to minimize the anaesthetictime
• Prior to anaesthetizing the animal, all equipment,personnel and drugs should be prepared
• The postoperative recovery area should be set up inadvance.
Anaesthesia is required for humane restraint, musclerelaxation and analgesia. There are particular factors to betaken into account when considering anaesthetizing exoticand wild animals. These factors include species, age, weight,percentage of body fat, environmental temperature, and thepresence of concurrent cardiovascular or respiratory disease.Any animal that is compromised by dehydration, bloodloss, cachexia, anorexia or infection will pose a greateranaesthetic risk than a clinically normal animal. Completepreanaesthetic assessment and stabilization are thereforeespecially important for wild animals for which no priorhistory is available.
• A thorough clinical examination is carried out to ensurethat the animal is free from clinical disease, especially withregard to respiratory and cardiovascular function
• Food and water intake should be measured preoperativelyand used to assess postoperative recovery
• An intravenous or intraosseous catheter may be pre-placedfor intraoperative and postoperative care
• The patient should be weighed immediately before surgeryto enable the correct dosing of the animal
• The patient should be handled correctly to minimizetrauma and stress.
Mammals
• Preanaesthetic fasting is not required in rodents as they donot vomit and there is a risk of hypoglycaemia withprolonged starvation
• Food (not water) may be withheld from rabbits andguinea-pigs for 3–6 hours to reduce the amount ofingesta in the gut
• Fasting may significantly alter the body weight of theanimal
• It is beneficial to administer subcutaneous fluids as aroutine at a rate of 10 ml/kg Hartmann’s fluid beforesurgery.
Birds
• Assessment of the hydration status, blood glucose leveland liver function is particularly important
• Preanaesthetic starvation is restricted to the time requiredto empty the crop (in those species that have one). Thiscan be easily palpated as full or empty. In emergency cases,the crop can be manually evacuated once generalanaesthesia has been induced.
Reptiles
• Premedication is not considered necessary• Reptiles should be maintained at their correct
temperatures prior to anaesthesia and during recovery
• Fluid therapy is essential to maintain hydration, especiallyif the recovery period is prolonged (e.g. followingketamine anaesthesia)
• Preoperative starvation is generally not considerednecessary, provided no food is present in the oesophagusor live insects in the stomach
• Larger chelonians and lizards may be starved for 18 hours,snakes for 72–96 hours, to ensure digestion is completed.
Amphibians and fishAmphibians and fish should be starved for 24–48 hours priorto anaesthesia.
Anaesthetic agents and methods ofadministration
Inhalation anaesthesiaInhalation is a relatively simple method of anaestheticinduction and maintenance of most species. Rapid variationsin depth and rapid recoveries are possible. Induction ofanaesthesia can be achieved via a face mask or by placing thewhole animal in an anaesthetic chamber. Endotrachealintubation should be used whenever possible to allowscavenging of waste gases, to reduce the amount of gas usedand to allow positive pressure ventilation if required. Ingeneral, isoflurane is the preferred agent, at 4% for inductionand 1–2% for maintenance of general anaesthesia. Manyreptiles can breath-hold, making induction by mask orchamber impractical.
MammalsThe technique of endotracheal intubation in the largermammals is essentially similar to that for a similar-sizeddomestic animal (e.g. badger and dog). Endotrachealintubation, however, is technically difficult in rabbits and smallrodents: these animals have a relatively large tongue and bigteeth, small oral cavities and a small deep larynx that makevisualization of the laryngeal opening difficult.
• Techniques for endotracheal intubation in the rabbit aregiven in Figures 8.52 (visual technique) and 8.53 (blindtechnique). Tube sizes and equipment required are given inFigure 8.54
• Unsuccessful intubation attempts can producelaryngospasm in rabbits, which is often fatal. The animalshould be sufficiently anaesthetized so that swallowing andcoughing reflexes are abolished
• Most rodents can be intubated using the blind technique(Figure 8.53). Endotracheal tubes may be made out ofinfusion set tubing or plastic intravenous catheters.
Birds
• An uncuffed tube should be used, as birds possesscomplete tracheal rings that may be ruptured by inflationof a cuff
• Ensure that the bird is anaesthetized by mask inhalation oran injectable regime before attempting intubation
• Use a gag to keep the beak open in those with powerfulbeaks (e.g. parrots). A finger may be used to keep openthe mouth of some birds (e.g. pigeons)
• Visualize the glottis (Figure 8.55). This is easy to see inpasserines and raptors but difficult in psittacine species,due to their fleshy tongue – use a tongue depressor toallow visualization of the glottis.

Small mammal, exotic animal and wildlife nursing 191
TipEndotracheal tubes for birds and reptiles may be madefrom appropriate gauge intravenous plastic catheters orintravenous drip tubing.
Reptiles
• An uncuffed tube should be used, as reptiles possesscomplete tracheal rings that may be ruptured by inflationof a cuff
• A gag should be used to keep the mouth open• The glottis of the snake is easily visualized on the floor of
the mouth• The lizard glottis (Figure 8.56) is positioned at the back of
the tongue and is sometimes difficult to visualize inanimals with a large fleshy tongue. To aid visualization,pressing beneath the chin externally may raise the glottis
• The chelonian possesses a large fleshy tongue thatobscures the view of the glottis. Pressing upwards belowthe chin raises the glottis; fully extending the head will aidvisualization
• Many chelonians have a very short trachea. A longendotracheal tube should not be used, as intubation ofone bronchus may occur – resulting in ventilation of onlyone lung.
1. Place the animal in sternal recumbency with the headlifted up and extended, or in dorsal recumbency withthe neck extended
2. Use a laryngoscope or an otoscope to visualize thelarynx
3. Place an introducer (e.g. 4 Fr cat urinary catheter) intothe trachea, thread the endotracheal tube over it intothe trachea and remove the introducer.
8.52 The visual method of endotrachealtube placement in rabbits
8.53
1. Estimate externally the position of the larynx2. Advance the endotracheal tube until it is at the position
of the laryngeal opening3. Listen for the breath sounds and advance the
endotracheal tube into the larynx on inspiration4. Alternatively, use a transparent endotracheal tube – this
will show condensation within the tube when it is nearthe larynx, when each expiration will fog the tube.Advance the tube on inspiration.
The ‘blind’ method of endotrachealtube placement in rabbits
8.54
Weight of Size of endotracheal Type of laryngoscoperabbit (kg) tube (mm O/D)
1–3 2–3 Wisconsin bladeNo. 0
3–7 3–6 Wisconsin bladeNo. 1
Endotracheal tube sizes andlaryngoscope types required forrabbit intubation
AmphibiansAmphibians may be intubated using plastic tubing of anappropriate size.
Injectable agents of anaesthesiaAgents of anaesthesia for the various animals are described inFigures 8.57–8.62. If an injectable agent is used to induceanaesthesia it is always good practice, and in some cases essential,to provide supplementary oxygen via mask or endotrachealtube, with or without the addition of gaseous anaesthesia.
Via the waterThis method is used for amphibians, fish and aquaticinvertebrates.
• Two containers of water should be available – one to makeup the anaesthetic solution and one to recover the animal
• The animal should be anaesthetized and recovered in watertaken from its tank or pond, to prevent any stress due totemperature, pH or other differences
• The anaesthetic agent is added to the water at a low doseinitially and mixed thoroughly
• The animal is introduced to the anaesthetic mixture• Once the righting reflex is lost, the animal may be taken
out of the anaesthetic solution and placed on a wet towel
8.55 The glottis of a raptor.Courtesy of N. Forbes.
8.56Glottis of aniguana.

192 Manual of Advanced Veterinary Nursing
8.57
Drug Dose per species and route Duration of anaesthesiaMouse Rat Guinea-pig Rabbit
Fentanyl/fluanisone 0.2–0.5 ml i.m. As mouse 0.2–0.4 ml Sedation only 30–45(Hypnorm; Janssen) 0.3–0.6 mg/kg i.p.
Fentanyl/fluanisone 0.4 ml/kg 0.3 ml/kg 1 ml/kg i.m. 0.3 ml/kg i.m. 45–60(Hypnorm; Janssen)/ 5 mg/kg 2.5 mg/kg 2.5 mg/kg 2 mg/kg i.p.diazepam
Fentanyl/fluanisone 10 ml/kga 2.7 ml/kga 8 ml/kga 0.3 ml/kg i.m. 45–60(Hypnorm; Janssen)/ 0.5–1 ml/kgmidazolama i.v.
Ketamine/medetomidine 200 mg/kg 90 mg/kg 40 35 20–300.5 mg/kg 0.5 mg/kg 0.5 0.5
Propofol 26 mg/kg i.v. 10 mg/kg i.v. – 10 mg/kg i.v. 5Atipamazole 1 mg/kg i.m., i.p., s.c., i.v., to reverse any combination using medetomidine
Anaesthetic agents for use in mammals
a One part fentanyl/fluanisone (Hypnorm; Janssen), one part midazolam (5 mg/ml), two parts water
(minutes)
8.58
Anaesthetic Dosage (mg/kg) CommentsIsoflurane Induction 4%, maintenance 2% Swift induction, rapid recoveryHalothane Induction 1%, increase to 3%, maintain at 1.5–3% Cardiac failure if too rapid induction,
unexpected deaths commonly reportedKetamine + diazepam 25 ketamine; 2.5 diazepam or midazolam i.m. 20–30 min deep sedationor midazolam
Ketamine/medetomidine Raptors 3–5 Ket/50–100 Med i.m. Reversed by atipamazole 250–380 µg/kg i.m.Psittacines 3–7 Ket/75–150 Med i.m.
Propofol 3–5 i.v. Wears off very quicklyCare with transfer to gaseous anaesthetic
Anaesthetic agents for use in birds
8.59
Drug Dosage (mg/kg) SiteAlphaxalone/alphadolone (Saffan; 6–9 i.v.Coopers Pitman Moore) 9–15 i.m.
Ketamine 20–100 (larger dose to smaller s.c. i.m. i.p.animals)
Propofol Tortoises 14 i.v. (agent of choice for induction)Lizards 10Snakes 10
Halothane 1–4% InhalationIsoflurane 1–6% Inhalation (agent of choice for maintenance)
Anaesthetic agents for use in reptiles
8.60
Anaesthetic agent Dosage for amphibians CommentsTadpoles, Frogs, Toadsnewts salamanders
Methanesulphate (MS222) 200–500 mg/l 500–2000 mg/l 1–3g/l To effect (begin with low concentration)Ethyl-4-aminobenzoate 50 mg/l 200–300 mg/l 200–300 mg/l Must be dissolved in methanol then added to(benzocaine) water, as not very soluble. Stock solution may
be kept in dark bottle for up to 3 monthsKetamine 50–150 mg/kgIsoflurane, halothane 4–5% bubbled through water Animals may be intubated using small
tubing and placed on moistened towelsDoxapram hydrochloride Empirical dosage (one drop) Useful to stimulate breathing
Anaesthetic agents for use in amphibians

Small mammal, exotic animal and wildlife nursing 193
• Fish and amphibians should be handled with wet gloves atall times
• Anaesthesia may be maintained by syringing the stockanaesthetic solution over the gills in fish or over the skinin amphibians, as required.
To recover, the fish is placed into the clean water andmoved in a slow circle until voluntary swimming movementscommence. Fish should never be dragged backwards throughthe water as this will damage the gills.
Amphibians may be recovered in a similar way, or byrunning the clean water over the animal until it regainsvoluntary and respiratory movements.
Monitoring anaesthesiaMonitoring anaesthesia in fish and amphibians is limited toobserving the heart beat and gill movements. Monitoring ininvertebrates is limited to observations of movements.
TemperatureA common reason for perianaesthetic deaths in small animalsis hypothermia. A decreased core temperature leads toprolonged recovery times, increases the potency ofanaesthetics and may lead to death during anaesthesia or onrecovery. The heat sources should be monitored to avoidhyperthermia or burns. All electronic monitoring equipmentmust be able to measure the heart rate, respiratory rate and
volume and core temperature of the particular species beingmonitored. The standard equipment used for dogs and catswill often not accurately measure these parameters in smallmammals (Figure 8.63), birds or reptiles (Figure 8.64).
Methods to minimize heat loss
• Heat loss via respiration and a cold flow of gas should beavoided by using humidifiers and warming the air in theanaesthetic circuit
• Hair/feather removal over surgical area should beminimized
• Excessive wetting of the patient should be avoided• The use of alcohol-based antiseptics should be avoided, as
these will chill the animal• Anaesthetic time should be minimized by adequate
preparation; prolonged surgery should be avoided• Areas of the body away from the surgical site should be
insulated• A regulated heat source should be provided• Core temperature should be monitored constantly.
8.61
Anaesthetic agent Dosage (into water) Comments
Methanesulphate (MS222) 100 mg/ml Only licensed product in UK
Ethyl-4-aminobenzoate 40 g into 1 l methanol; 11 ml of this Must be dissolved in methanol then added to water, as(benzocaine) solution into 9 l water not very soluble
Stock solution may be kept in dark bottle for up to 3months
Anaesthetic agents for use in fish
8.62
Anaesthetic agent Dosage Comments
Inhalational anaesthesia in Halothane (5–10%) Recovery may take hours but is well toleratedinduction chamber or bubbled Carbon dioxide (10–20%)through water
Tricaine 100 mg/l water Recover in fresh waterMethanesulphate (for aquaticspecies)
Benzocaine (for aquatic species) Dissolve in acetone, add 100 mg/l water Recover in fresh water
Anaesthetic agents for use in invertebrates
8.64 Small mammal under general anaesthesia.
Avoid excessive feather removal in birds, as manyonly moult once or twice a year. The extent offeather loss is especially important whenassessing whether wild birds are fit for release.
8.63 Reptile under anaesthesia.

194 Manual of Advanced Veterinary Nursing
Assessment of anaesthetic depthFigure 8.65 offers a guide to monitoring the depth ofanaesthesia in animals.
Monitoring respiratory and cardiovascular systemsThe respiratory rate, depth and pattern may be monitored bydirect observation of chest wall, movement of reservoir bagor electronic monitors. The heart rate can be monitored bydirect observation of the beating heart or palpation of a pulse(Figure 8.66), using an ECG (Figure 8.67) or indirectly byusing a pulse oximeter (Figure 8.68). Capillary refill times,mucous membrane colour and a peripheral pulse may be usedto assess cardiac output and tissue perfusion as in largerdomestic animals.
General management of animals undergeneral anaesthesia
MammalsIntraoperative care is as for domestic mammals.
Birds
• Rapid induction/recovery is possible with gaseousanaesthetic agents
• Restriction of ribs/sternal movement by weight on thesternum (e.g. surgeon’s hands, instruments, heavy drapes,bandages) can lead to suffocation
• The bird should be positioned in sternal (ideal) or lateralrecumbency, as dorsal recumbency compromisesrespiration by 10–60%
• Force ventilate with 100% oxygen every 5 minutes, asbirds easily become hypercapnic (excess carbon dioxide)
• Rapid position changes of the anaesthetized bird shouldbe avoided, as this can lead to a severe drop in bloodpressure
• If the bird has ascites, it should be placed in upright orhead-elevated position to avoid impairment of respirationand fluid entering the lung during surgery
• Some birds become apnoeic after approximately 30minutes of anaesthesia and require positive pressureventilation and careful monitoring during this period.
8.65
Depth Small mammals Reptiles and Birds Fish Invertebratesamphibians
Light plane – Absence of – Absence of righting – Absence of – Erratic swimming Loss of rightingrighting reflex reflex righting reflex – Loss of reactivity reflex
– Absence of tail – Intact pedal – Intact cornealpinch reflex withdrawal palpebral and
– Intact pedal – Snakes still respond pedal reflexeswithdrawal to stroking of
ventral surface
Surgical plane Absence of pedal – Absence of tongue – Eyelids closed – Absence of No response towithdrawal withdrawal (snake) – Pupils dilated righting reflex surgical
– Absence of limb stimuluswithdrawal
– Absence ofpalpebral reflex
Too deep Rabbit – palpebral – Fixed dilated pupils – Loss of corneal – Very shallow Difficult toreflex lost – Slow heart rate reflex opercular assess
– Slow shallow movementsrespiration – Gasping
– Respiratory arrest – Cessation ofoperculummovements
Monitoring depth of anaesthesia
Site Mammals Reptiles Birds Amphibians Fish
Chelonians Snakes Lizards
Carotid artery ✓ ✓ ✓ (rare) ✓ ✓
Heart beat ✓ ✓ ✓ ✓ ✓
Other arteries Ear (rabbit) Medial metatarsalMandibularTongueFemoral
8.66 Sites for manual monitoring of heart rate/pulse

Small mammal, exotic animal and wildlife nursing 195
Reptiles
• Many reptiles can maintain apnoea for a prolonged periodwhen conscious; thus induction by inhalation anaestheticis not recommended
• Many reptiles will require intermittent positive pressureventilation (IPPV) continuously throughout theoperation, as apnoea is common
• The respiratory rate required to maintain gaseousanaesthesia is often greater than the normal respiratoryrate of the conscious animal, but should be based on thisrate initially and the depth of anaesthesia monitored
• If the reptile had been maintained or induced with along-acting injectable agent (e.g. ketamine), the animalmay take hours to regain consciousness completely
• IPPV with oxygen should not be stopped until the reptilehas begun to breathe spontaneously.
TipThe careful use of dry heat (e.g. from a hairdryer) on therecovering reptile will speed the time taken to regainspontaneous breathing and voluntary movement. Monitorthe heat to avoid overheating the reptile.
• Apply to:
– Tongue, ears, tail, nail bed and footpads in mammalsand reptiles
– Wing web or tibiotarsal bone in birds
• Not validated for reptiles and so the trend rather thanabsolute figures should used to monitor the patient
• Allows measurement of the oxygen saturation of theblood and is an indication of respiratory depth,respiratory obstruction or equipment failure
• Displays the pulse rate to give an indication ofcardiovascular depression (if low and at a fast rate, mayindicate that anaesthetic plane is too light)
• Pulse signal is also evidence that blood is flowingthrough the tissues
8.68 Pulse oximeter sites and application
8.69
Causes• Overdose of anaesthetic• Blocked or displaced endotracheal tube• Equipment failure• Lack of oxygen• Pain• Laryngeal spasm (rabbits)• Weight on thorax (e.g. surgeon’s hands).
Signs• Respiratory rate less than 40% of conscious rate• Cyanosis of mucous membranes (iris in albino animals)
(note that oxygen saturation must fall to < 50% beforecyanosis is seen in mammals)
• If oxygen saturation falls by:> 5% = mild hypoxia> 10% = emergency> 50% = severe life-threatening hypoxia.
Action• If under gaseous anaesthesia, check oxygen is still
supplied, check patency of circuit, check endotrachealtube is not blocked, decrease the plane of anaesthesia
• If using injectable anaesthesia, reverse anaesthesia if atconvenient stage of procedure, provide oxygen byendotracheal tube (preferable) or face mask
• In all cases:– Provide oxygen– Begin chest compressions to aid ventilation– Administer doxapram (respiratory stimulant) every
15 minutes as required• Rocking or gently swinging the small animal is often an
effective method of ventilating, especially in small mammals• If stable, continue anaesthesia; if not, continue manual
ventilation and recover animal.
Respiratory failure
Causes• Overdose of anaesthesia• Hypoxia/hypercapnia• Blood loss (15–20% = hypovolaemia and shock)• Hypothermia (body temperature of < 25°C leads to
cardiac arrest in mammals).
Signs• Increased capillary refill time, cyanosis, pallor• Decreased body temperature (slow change)• Gradual decrease in blood pressure or pulse rate• Change in heart rate/rhythm.
Action• Administer 100% oxygen via endotracheal tube or mask
and ventilate• Administer fluids at a rate of:
– 10–15 ml/kg per hour for maintenance, or– 50 ml/kg over 1 hour in emergency due to
hypovolaemia• If cardiac arrest, start chest compressions at rate
appropriate for heart rate of animal• Reverse anaesthesia.
8.70 Cardiovascular failure
8.67
In generalRed electrode – place on the right forelegYellow electrode – place on the left forelegGreen electrode – place on the left hindlegBlack electrode – place on the right hindleg.
Special considerationsLarge mammals – attach to body wallSmall mammals – attach to feetBirds – attach pads or clips to wing web and feetReptiles – attach to the feet or space out along length of asnake.
Lead attachment sites for ECGmonitor
Care must be taken with interpretation: the electricalimpulse does not always equate with an adequatecardiac output.
Anaesthetic emergenciesFigures 8.69 and 8.70 describe how to recognize and treatrespiratory and cardiovascular failure, respectively.

196 Manual of Advanced Veterinary Nursing
Postoperative care
• The animal should be monitored until full recovery isnoted
• Animals should always be recovered individually in a quietdimly lit area
• The recovery area should be at the correct temperature forthe species
• The animal’s core temperature should be monitored untilit has recovered fully
• Fluids (including glucose) should be administered if theanimal does not begin to eat and drink within a reasonableperiod for the species
• Analgesia should be administered routinely after a procedureor if assessment on recovery indicates pain (Figure 8.71describes signs of pain or discomfort in animals)
• The animal should always be given the benefit of thedoubt. Analgesics administered appropriately will notharm the animal.
Postoperative analgesia is often overlooked when exoticanimal or wildlife surgery is conducted. This is not a humaneapproach. Animals in pain will reduce their food and waterintake and suffer from stress-related disorders. Inadequateanalgesia can seriously compromise postoperative recovery.Figure 8.72 suggests analgesic regimes in animals.
8.71
Aggression
Overgrooming/lack ofgrooming
Inactivity
Hiding at back of cage
Hunched posture
Increased respiratoryrate
Polydipsia
Anorexia
Hyperthermia/hypothermia
Tooth grinding
Self-trauma over painfularea
(Note: vocalizing is rare)
Signs of pain or discomfort
Immobility
Anorexia
Abnormallocomotion orposture
Increased aggression
Dull colouration
Small mammals Reptiles Birds Amphibians Fish
Immobility, collapse
Increased aggression
Abnormal posture orlocomotion
Less ‘talking’ orsinging
Less response tohuman if previouslytame and interactive
Picking or pluckingover painful area
Immobility
Anorexia
Abnormal locomotionor posture
Increased aggression
Dull colouration
Loss of appetite
Hollow sides orunderparts
Fins folded
Poor skin colour
Sluggish swimming
Unusual swimmingaction, e.g. jerkiness,imbalance
Rubbing on stones orornaments
Drug Small mammals Larger mammals(e.g. rat) (e.g. rabbit, badger)
Dosage Route Frequency Dosage Route Frequency(mg/kg) (hours) (mg/kg) (hours)
Buprenorphine 0.05–0.1 s.c. 6–8 0.01–0.05 s.c. 6–8
Butorphanol 1–5 s.c. 4–6 0.1–0.5 s.c. 4–8
Carprofen 5 s.c. 8–12 1–5 s.c. 8–12
Meloxicam 0.2 s.c. 12–24 0.1–0.2 s.c. 24
Drug Birds Reptiles
Dosage Route Frequency Dosage Route Frequency(mg/kg) (hours) (mg/kg) (hours)
Buprenorphine 0.02 i.m. 2–4 Not established (use mammalian dosage?)
Butorphanol 3 i.m. 1–4 Not established (use mammalian dosage?)
Carprofen 5–10 s.c. 4–8 5 s.c. 12–24
Meloxicam 0.2 s.c. 12–24 0.2 s.c. 24
8.72 Analgesia (many of these doses are anecdotal and approximate and may not belicensed for the species)

Small mammal, exotic animal and wildlife nursing 197
Additional considerationsfor the wildlife patientMany of the aspects of treating wild animal species can beadapted from the techniques used to treat their domesticcounterparts. Poisoning is perhaps seen more often in wildlifebut can also occur in captive species (see Figure 8.46). Thissection will deal with the extra information needed to treatwildlife effectively, safely and legally.
AssessmentOn accepting a wildlife patient, an assessment should be madeas soon as possible as to whether the animal should be treatedor humanely euthanased. This aspect of treating wildlife isperhaps the most difficult, but for the animal’s sake this harddecision should be made as soon as possible.
Questions to consider when assessing the wildlife casualtyare:
• Will the animal benefit from any form of medical orsurgical therapy?
• Will it ever be fit for release?• Will the prolonged rehabilitation period in itself cause
suffering to the animal?
It is important to record, in as much detail as possible,where and when the animal was found. This will aid its releaseto an appropriate area and will also help to gather informationon the prevalence of native wildlife in certain areas.
The animal should be correctly identified as to speciesand age so that the appropriate husbandry can be provided.Some species are covered by legislation that may requirespecific action or may affect how or if the animal is to bereleased.
An assessment should be made of whether the practicefacilities and staff are able to deal with the species concerned.It is useful to make contacts with local wildlife centres anddiscuss which facility would best deal with certain situations.
NursingImportant points when nursing the wildlife casualty are:
• Accurate daily records should be kept of body weight,amount eaten and drunk, passage of faeces and urine
• Handling and interaction with the animal should beminimized– To minimize stress– To avoid habituating the animal to humans
• The progress of the animal should be assessed daily withregard to continuation of treatment, fitness for release orrequirement of euthanasia.
• Do not euthanase animals by chilling orfreezing. This is not a humane approach:research has shown that animals perceivefreezing as painful
• Do not use ether to anaesthetize or euthanase animals.It is an irritant substance to the animal and to humans.It is also a fire hazard
• Do not attempt to perform an intraperitoneal injection ina bird. The peritoneal cavity is only a potential space inthe healthy bird. Injection into the body cavity will resultin injection into the air sac and will drown the bird.
Method of euthanasia Mammals Reptiles Birds Amphibians Fish Invertebrates
Overdose of anaesthetic via:
Intravenous route (conscious or ✓ ✓ ✓ ✓ ✓ –sedated animal)
Intraperitoneal route ✓ ✓ – ✓ ✓ –
Intrarenal or intrahepatic ✓ ✓ – ✓ ✓ –injection
Intrahepatic injection only – – ✓ – – –
Intraosseous route ✓ ✓ ✓ ✓ – –
Cervical dislocation (< 500 g ✓ – – – – –body weight only)
Overdose of inhalational ✓ (not – ✓ (not – – ✓ (terrestrialanaesthetic in chamber diving diving species)
species) species)
Overdose of anaesthetic in water – – – ✓ ✓ ✓ (aquaticspecies)
Concussion by striking back of – – – ✓ ✓ ✓
head, followed by destruction ofthe brain
Overdose of anaesthetic via ✓ ✓ ✓ ✓ ✓ –intracardiac injection aftersedation or induction ofanaesthesia by other methods
8.73 Methods of euthanasia
Methods of euthanasiaThe various methods used to euthanase animals humanely aredescribed in Figure 8.73.

198 Manual of Advanced Veterinary Nursing
Legislation
Wildlife and Countryside Act 1981 (as amended 1988,1991)This makes it illegal to kill, injure, take, possess or sellcertain UK native wild animals. An exception is made forthose taking and possessing sick or injured animals, oreuthanasing injured animals. The burden of proof falls onthe person in possession of the animal, and so accurate andup-to-date records must be kept.
Section 8 of the Act states that birds should be kept incages large enough for them to stretch their wings fully. Asmaller cage may be used for transport or while undergoingveterinary treatment.
If diurnal birds of prey are taken under this Act, they mustbe ringed and registered if kept for more than 6 weeks; if forless than 6 weeks they may be held under an exemption forveterinary surgeons.
Non-indigenous species may not be released into the wild,unless they are listed in the Act as already established.
Dangerous Wild Animals Act 1976 and (Modification)Order 1984A licence is required to keep certain species of venomous snakes,lizards and all crocodilians. This also includes all primates (exceptmarmosets) and some poisonous spiders and scorpions. UKwildlife included are the wild cat and the adder. An exceptionis made if the animal is in a veterinary surgery for treatment.
Protection of Animals Acts 1911, 1988; Protection ofAnimals (Scotland) Acts 1912, 1988This legislation makes it illegal to cause unnecessary suffering– which may include failure to provide food, water orveterinary treatment. Killing an animal is not an offence unlessit is carried out inhumanely.
Abandonment of Animals Act 1960This states that animals should not be abandoned incircumstances likely to cause them suffering. This is especiallyrelevant when considering the release of a wildlife casualty.
Animal Health Act 1981; Transit of Animals Order 1973(as amended 1988)This states that animals (including invertebrates) must betransported without causing unnecessary suffering. Appropriatecontainers and vehicles must be used and adequate food, water,ventilation and temperature must be provided.
Veterinary Surgeons Act 1966This Act restricts the veterinary treatment of mammals, birdsand reptiles to veterinary surgeons and practitioners. Fish,amphibians and invertebrates may be treated by anyone,provided the Protection of Animals Acts are complied with.Owners may give minor treatment to their own animals.Anyone may give emergency first aid to an animal.
Medicines legislation: Medicines Act 1968; Medicines(Veterinary Drugs) (Prescription Only) Order 1985;Misuse of Drugs Act 1971; Misuse of DrugsRegulations 1985Prescription-only drugs (POMs) must only be supplied by aveterinary surgeon to ‘animals under his care’. Theseregulations apply to any animal for which the drugs aresupplied – even the species that do not come under theVeterinary Surgeons Act.
Health and Safety at Work etc. Act 1974Staff, volunteers or students working with non-domesticatedspecies must be provided with additional safety procedures,depending upon risks involved. This includes training,working protocols and protective equipment.
Animals Act 1971Those in possession of non-domesticated species (whetherowned by them or not) that are likely to cause serious damagemust ensure that damage to property and injuries to people areprevented.
Further readingBeynon PH and Cooper JE (1991) BSAVA Manual of Exotic
Pets. British Small Animal Veterinary Association,Cheltenham
Beynon PH, Forbes NA and Lawton MPC (1996) BSAVAManual of Psittacine Birds. British Small Animal VeterinaryAssociation, Cheltenham
Beynon PH, Lawton MPC and Cooper JE (1992) BSAVAManual of Reptiles. British Small Animal VeterinaryAssociation, Cheltenham
Butcher (1992) BSAVA Manual of Ornamental Fish. BritishSmall Animal Veterinary Association, Cheltenham