slipped capital femoral epiphysis
TRANSCRIPT
Slipped Capital
Femoral
Epiphysis Dr. Fahad Al Hulaibi 2015
Orthopedic Surgery
National Guard Hospital-KSA

OPD PIC.

What is SCFE ?? Disorder of:
proximal femoral physis
that leads to slippage of the epiphysis
relative to the femoral neck

Risk factors
obese children
Males
Age 10-16 y/o Campbell
+ve family history
Endocrinopathy. < 10 y/o
Lt. hip is more common Campbell

In which zone of physis ?

Causes: local trauma.
inflammatory conditions.
Endocrine disorders (e.g., hypothyroidism, hypogonadisim, hypopituitarism, and chronic renal disease)
genetic factors,
Down syndrome
It is a multifactorial

presentation
Boy : Girl ( 2:1 ) Campbell
Knee pain (15-23%), thigh or groin pain.
Limping. (if stable)
symptoms usually for weeks to several
months.
Thigh atrophy.

obligatory external rotation
X-ray Finding

AP & frog lateral
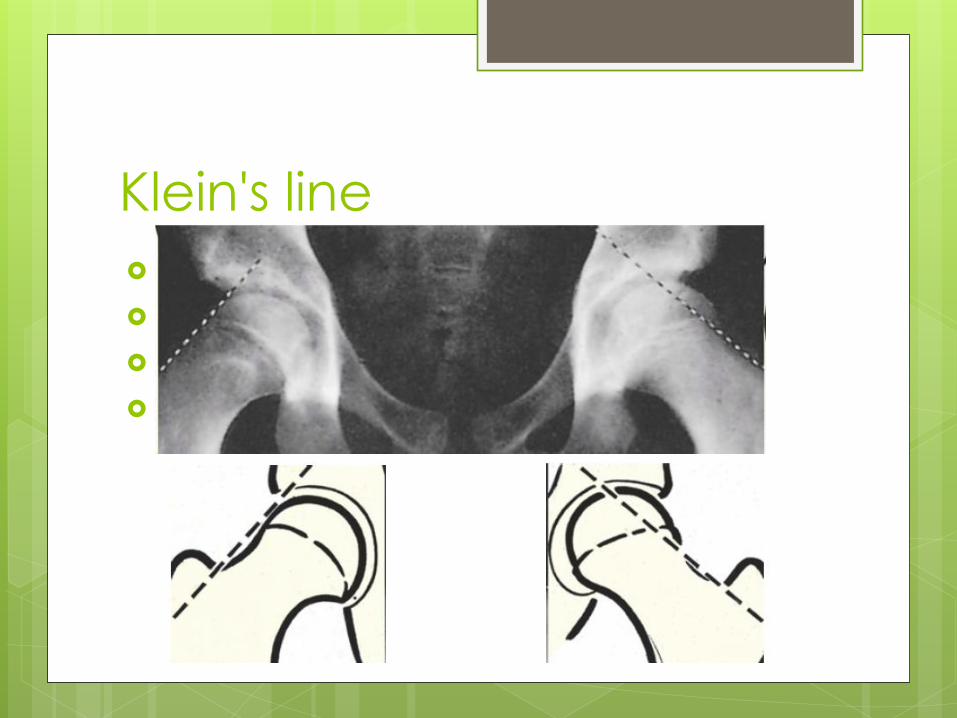
Klein's line
Dr. saleem patient
blurring of proximal femoral metaphysis
epiphyseal plate seems to be too wide
and too ‘lucent’
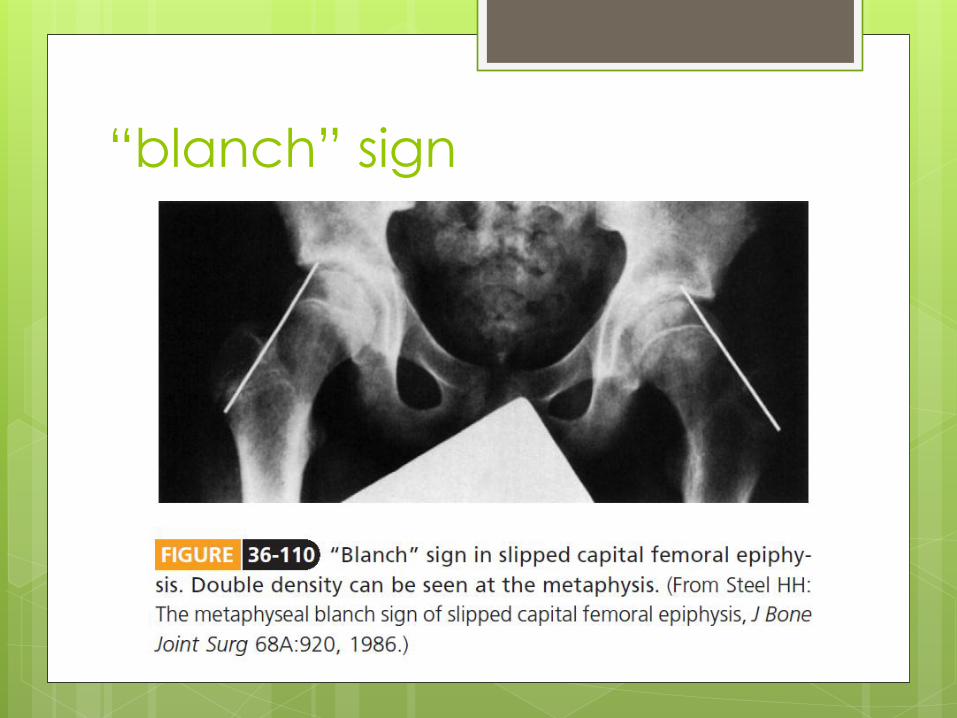
“blanch” sign

CT
Do we need CT ?
Classifications

Stability by Loder et al.
Stable:
can bear weight
Un-stable
can’t bear Wight >> 47% ? AVN
Chronicity Campbell
Acute:
Symptoms < 2 weeks
Chronic:
Symptoms > 2 weeks
Acute on chronic:
> 4 weeks with recent sudden exacerbation

Southwick Angle Classification
Mild:
< 30 °
Moderate:
30 ° - 60 °
Severe:
> 60 °
Head shaft angle
In frog lateral view

Grading System Campbell
Grade I :
0-33 % of slippage
Grade II :
30-50 % of slippage
Grade III :
> 50 % of slippage

TREATMENT
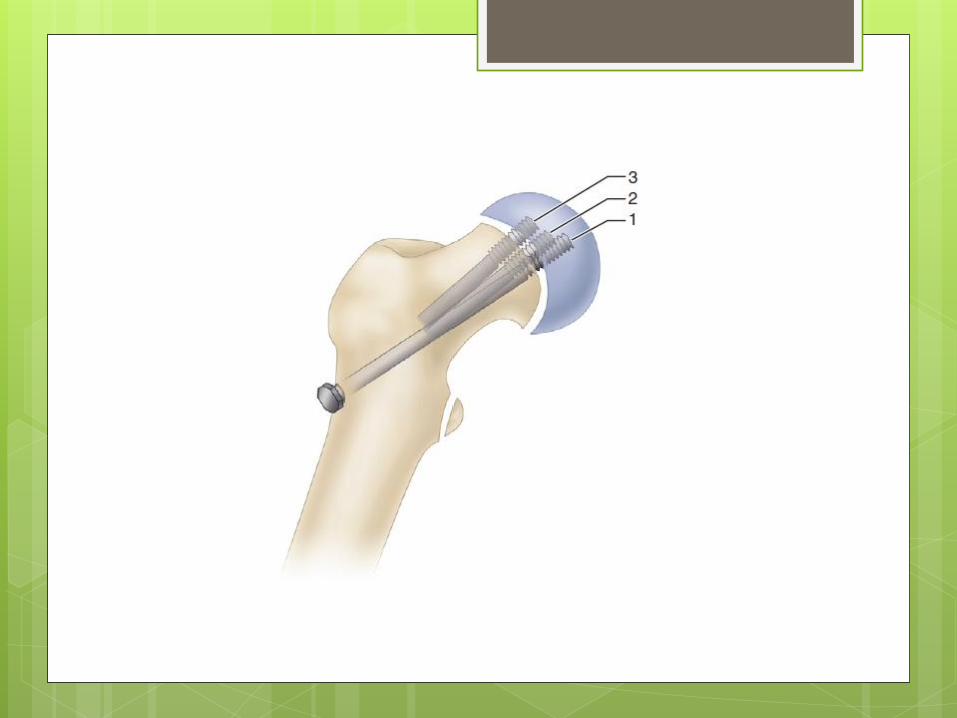
percutaneous in situ fixation
In all stable and unstable slip.
Goal:
- To stabilize the epiphysis from further slippage.
- Avoiding the complications.
One screw or 2 ??


POSTOPERATIVE CARE
discharged the same day.
partial weight-bearing crutch (2 to 3 wks)
for stable only
rigorous sports limited until the physes
have closed.
Screw removal is not necessary.

contralateral in situ
prophylactic pinning ??

If one side affected..
25-40% the other one will be
Benson EC, Miller M, Bosch P, Szalay EA. A new look at the incidence of slipped capital femoral epiphysis
in new Mexico. J Pediatr Orthop. 2008 Jul-Aug. 28(5):529-33
12 to 18 months of the initial slip

increased incidence
Endocrine abnormalities
Age < 10 y/o
for whom reliable follow-up is not feasible.
high risk factors for complications.
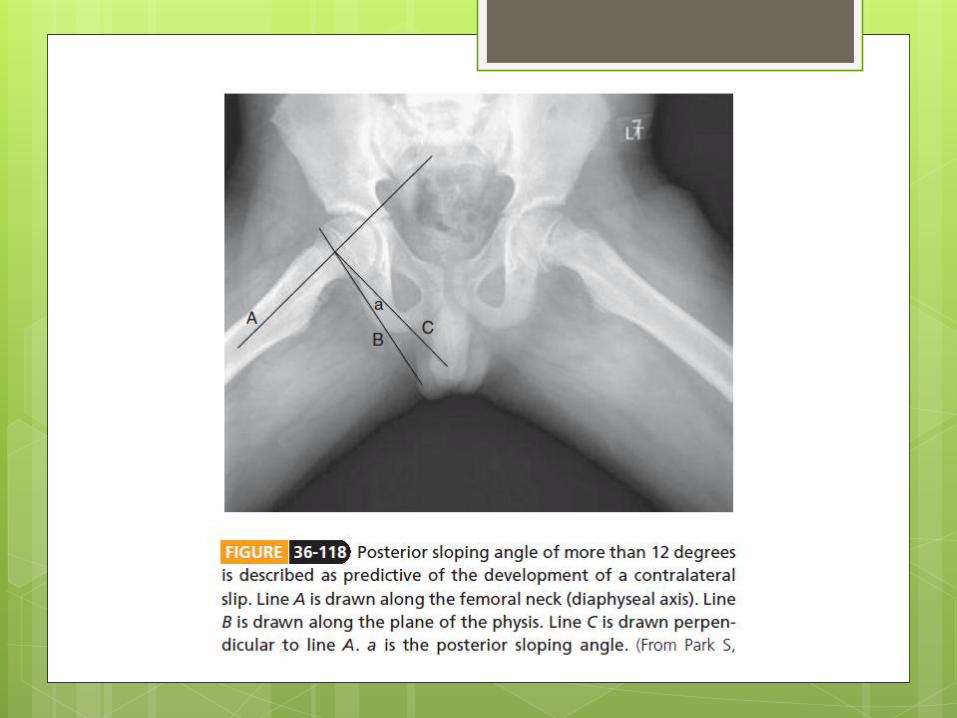
“posterior sloping” angle of more than 12
degrees
CLOSED REDUCTION
slips treated without reduction.
Only sever unstable acute Slip.

OPEN REDUCTION
if a severe acute or chronic slip cannot be
reduced closed.
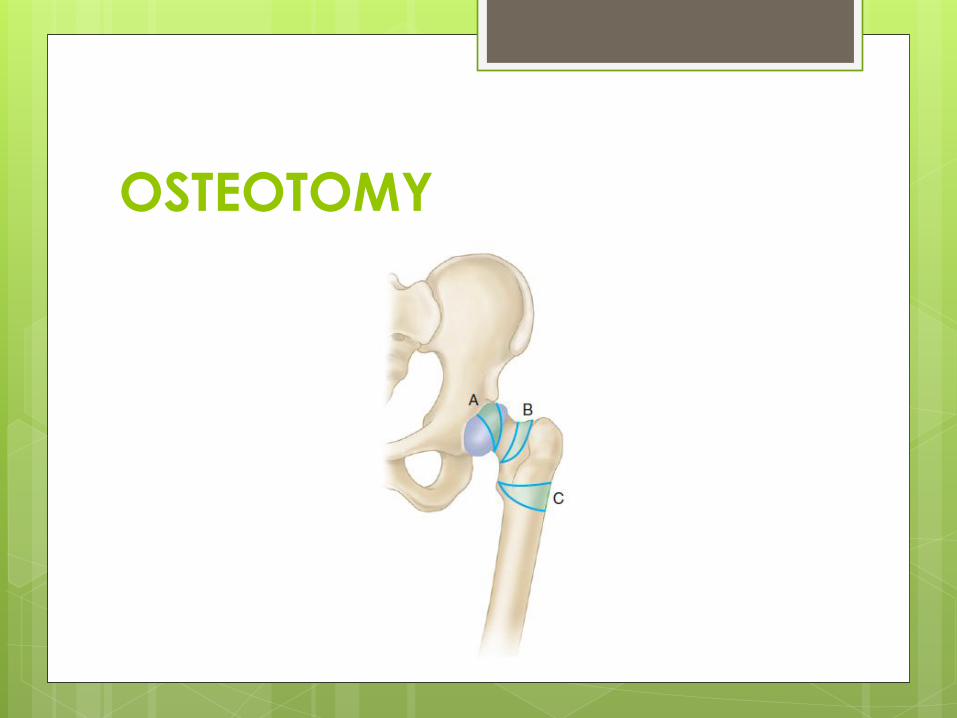
OSTEOTOMY

COMPLICATIONS
COMPLICATIONS

OSTEONECROSIS
Common in unstable.
Superolateral placement of pins

CHONDROLYSIS
a joint space less than 3 mm wide
(normal 4 to 6 mm)
decreased range of motion of the hip joint
Most serous complication.
Most painful.
End with Ankylosis of hip joint.
Tx: ??
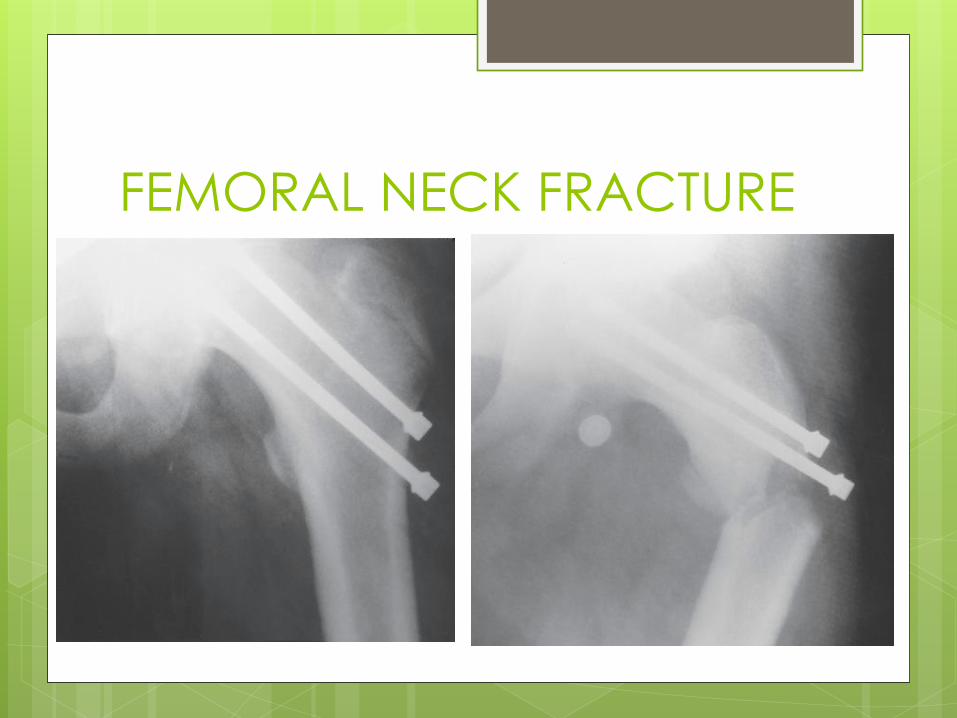
FEMORAL NECK FRACTURE

Message is:
avoiding drilling
unnecessary
holes in the bone
during surgery
CONTINUED SLIPPING
Patients who refused treatment.
Pins were not placed far enough proximally.
Remove pins before the physis had fused
completely

If you want a dream, Dream Big !!