six years of integrated behavioral health in a pace … years of...recovery support groups. anxiety...
TRANSCRIPT

Six Years of Integrated Behavioral Health in a PACE
ProgramSibyl Salisbury, MS, CNPElisabeth Broderick, MDKatelin Hartigan, LMHC
10/6/2017 1
Objectives
• Review features of Element Care’s Integrated Behavioral Health Program
• Discuss outcomes• Discuss cased-based example of program in action, including Smoking
Cessation initiative
10/6/2017 2
Element Care’s Integrated Behavioral Health Program
• Established 6.5 years ago• 4 APRNs, 4 psychotherapists, rotating geripsych fellow, and
Collaborating Psychiatrist for clinical supervision• Encouraged to transition to EC’s BH providers
10/6/2017 3

Integrated Behavioral Health
• Systematic, cost-effective teamwork approach between Primary Care and BH Clinicians
• Patient-centered experience• Clinical focus for BH clinicians• Shared mission and accountability
10/6/2017 4

Practice of Integration
• Space may be separate, co-located, or fully shared• Collaboration: referral-based to fully integrated• Identification of patients ranges from patient/clinician identified to
universal screening• Policies in place to support practice
10/6/2017 5

Core Strategies
Consulting Coordinating Collaborating Communicating Culture
10/6/2017 6

Strategies and services employed at EC
10/6/2017 7
Primary CareTraditional
BHMedication concerns
Coordinated care
Consultative support

Strategies and services employed at EC
Support of health
behaviors
BH clinician refers to PC
IDT support
Support to SNF
Care plans
10/6/2017 8

Strategies and services employed at EC
Utilization Management
Integrated EMR
Special evaluations
Crisis support on patient or IDT request
Enrollment process support
End of Life Care
10/6/2017 9

Strategies and services employed at EC
Program-wide initiatives
10/6/2017 10
BH led in-services BH rounds Avatar Program Recovery
Support Groups
Anxiety Management
Groups
Smoking Cessation Program

Behavioral Health Utilization • Element Care has a catchment area that includes 50+ communities in
Massachusetts with a current census of 992 participants across 8 sites• 80% received a behavioral health services in FY17
10/6/2017 11

# of Psych Admissions by Diagnosis
10/6/2017 12
0
50
100
150
200
250
300
2015 2016 2017
Psychosis/SchizophreniaCombined Mood DisordersDementiaSubstance Use Disorders

# of Psych Inpatient Days
10/6/2017 13
0
200
400
600
800
1000
1200
2015 2016 2017

EC Behavioral Health Acuity Management Data
10/6/2017 14
1412
10
19
15
20
27
0
5
10
15
20
25
30
January February March April May June JulyHigh Acuity Situations
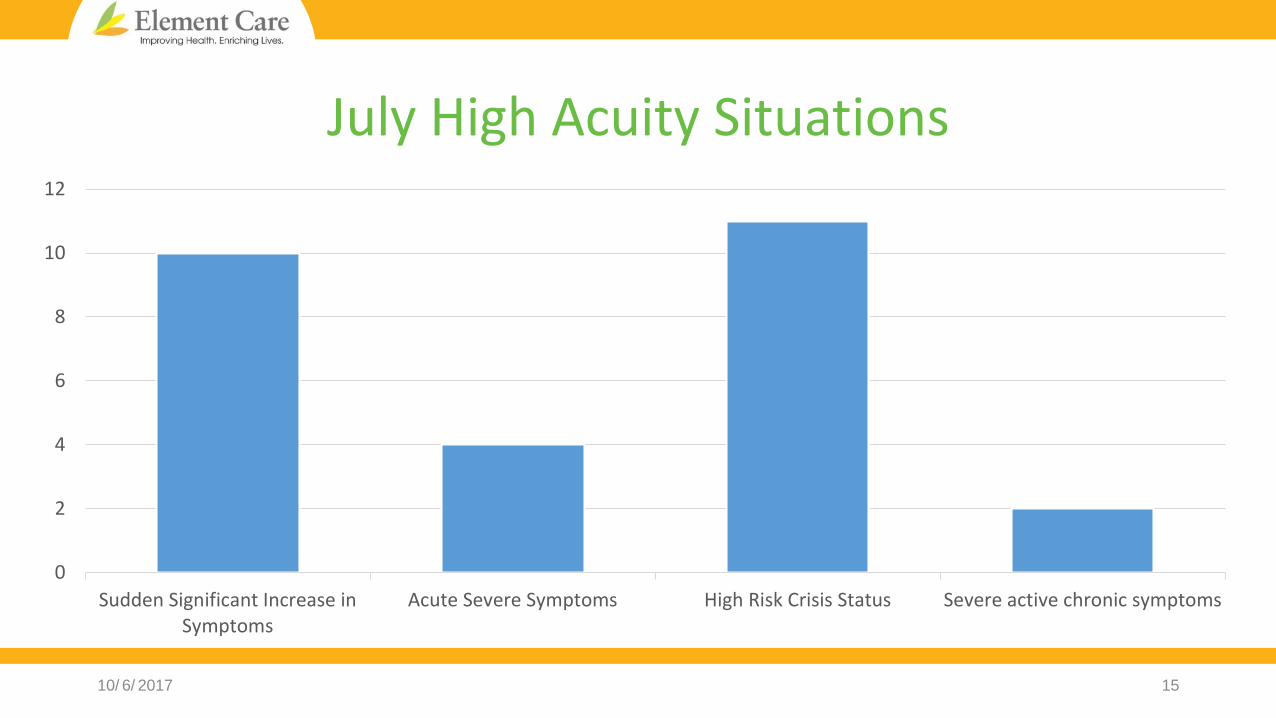
July High Acuity Situations
10/6/2017 15
0
2
4
6
8
10
12
Sudden Significant Increase inSymptoms
Acute Severe Symptoms High Risk Crisis Status Severe active chronic symptoms

Care Management Breakdown
10/6/2017 16
0
2
4
6
8
10
12
14
Crisis Stabilization SNF Admission Inpatient Admissions Medication/Visit FrequencyChanges to Avoid ED or
Inpatient
Integrated BH: A Day in the Life…
8a Morning Meeting 9a Care plans 930a-130p
Encounters Visit to hospital 2pm UM call 3pm
10/6/2017 17

Case 1: JZ• 72yo single Caucasian female, enrolled 2012• Schizoaffective disorder (bipolar type), Hoarding disorder, PTSD, Mild
Cognitive Impairment, history of extensive state hospitalization• Obesity, type II DM, hypertension, hyperlipidemia, chronic ischemic
heart disease, essential tremor, history of breast cancer, osteoporosis, chronic lymphocytic leukemia, emphysema, hypokalemia, spinal stenosis, urinary urge incontinence, anemia, peripheral edema, hxankle fracture October 2016, polypharmacy
10/6/2017 18
Case 1: JZ (cont.)• Lives alone in supportive housing near PACE ADH• Enjoys: shopping, fashion, painting, taking cruises• Permanent full guardian (since 1999), limited support from family/friends• Stable x5 years until ankle fracture October 2016, decompensated within 1
month• Intensive outpatient attempts at SNF for about a month• Hospitalized December 2016 (29 days), discharged with residual symptoms• Hospitalized July 2017 (14 days), discharged with ongoing severe symptoms
10/6/2017 19

Integrated BH: A Day in the Life…
8a Morning Meeting 9a Care plans 930a-130p
Encounters Visit to hospital 2pm UM call 3pm
10/6/2017 20

Case 2: AF• 78yo separated, Latino male (Spanish speaking), enrolled PACE 2000
• Schizoaffective disorder, bipolar type, Mild Cognitive Impairment
• Limited acceptance of BH by history
• History of incarceration for sexual assault charges
• Ischemic cardiomyopathy, ICD, hypertension, chronic systolic dysfunction of left ventricle and stenosis of left carotid artery, type 2 DM with stage 3 CKD and retinopathy, hypothyroidism, osteoporosis, BPH
• Lives in private apartment, accepts limited services
10/6/2017 21

Case 2: AF (cont.)
• Children are involved as much as he will allow • Baseline is mildly paranoid, hypomanic, grandiose with disordered
thought process• Decompensation in Spring 2017
• Expressed belief that PCA was trying to seduce him• Would not accept medical feedback re: need for insulin• MVA hit car of staff member at ADH
10/6/2017 22

Integrated BH: A Day in the Life…
8a Morning Meeting 9a Care plans 930a-130p
Encounters Visit to hospital 2pm UM call 3pm
10/6/2017 23

Case 3: JM• 65yo divorced Caucasian male, enrolled 2007
• Bipolar I disorder, PTSD, Hoarding disorder, Personality disorder, chronic SI
• No history of psychiatric hospitalizations until 2012, multiple since
• No history of self-harm but history of hoarding medications
• Uncontrolled DM II on insulin, CKD stage 3, COPD, hypertension, essential tremor, GERD, anemia
• Limited family involved (out of state)
• Relationship with another PACE prt (APS involvement)
10/6/2017 24

Integrated BH: A Day in the Life…
8a Morning Meeting 9a Care plans 930a-130p
Encounters Visit to hospital 2pm UM call 3pm
10/6/2017 25

Outcomes for EC’s Integrated
Model
Patient outcomes
Fiscal outcomes
Provider outcomes
10/6/2017 26

Primary Care’s experience of Integrated Care
10/6/2017 27
OK• Consultation psycho-pharm• Some therapy
Better•Assess all participants with BH need
Best• BH groups, support for addictions, on call support, ADH psych
rounds

Smoking Cessation Initiative
10/6/2017 28
Importance of Tobacco Cessation in PACE
• Tobacco use is a worldwide epidemic and continues to be the leading global cause of preventable death, killing nearly 6 million people a year.
• It worsens the health of our Element Care participants, complicates treatment and is very financially costly to our program.
• Element Care participants with respiratory disease are the highest utilizers of emergency room visits and inpatient care.
10/6/2017 29

Element Care Smoking Cessation Initiative
• EC has embarked on an initiative to fully integrate tobacco cessation into our clinical practice.
• This initiative is important because it has the potential to improve health and quality of life for our tobacco using participants and decrease utilization of expensive levels of care for participants with respiratory disease.
10/6/2017 30
Tobacco Cessation: Vision & Goals
• Our vision is for smoking cessation to become a permanent integrated component of clinical practice at EC for all IDT disciplines.
• Clinical evidence indicates that some simple interventions can have significant results when multiple disciplines contribute a small piece on an on-going basis to achieve success.
• Results have been most dramatic when multiple disciplines have ongoing conversations about smoking with a smoker.
10/6/2017 31

The Structure
• The Prochaska Stages of Change model is the foundation for our smoking cessation initiative.
• As with all addictions treatment, in order for the tobacco cessation efforts to be effective, interventions need to target the right stage of change for each individual.
10/6/2017 32

Prochaska Stages of Change
10/6/2017 33

Phases of Implementation1. Training for all behavioral health staff
2. Stages of Change Presentations
3. Appropriate Diagnosing
4. Quarterly Smoke Outs
5. Educational tool kits
6. Monthly Educational Posters
7. Assessment Tools
8. Nicotine Replacement Therapy
9. Smoking Cessation therapeutic groups
10. Recognition: Celebration and Reward rituals
10/6/2017 34

1. Training for Tobacco Cessation Initiative Leaders
• All Behavioral Health staff completed UMass: The Center for Tobacco Treatment Research and Training (CTTRT) online course on basic skills for working with smokers.
• The Center for Tobacco Treatment Research and Training (CTTRT) mission is to promote state of the art, evidence-based tobacco dependence treatment in healthcare and community settings through training, research and public service.
10/6/2017 35

2. Stages of Change Presentation
• It was critical for all of our clinical staff to understand the Stages of Change model.
• A presentation by behavioral health staff on Stages of Change was offered at each site.
10/6/2017 36

3. ICD 10 Codes
10/6/2017 37

4. Assessment Tools5 A’s: Element Care implemented a system that ensures that for every participant, at every visit, tobacco use status is documented. 1. Ask- systematically identify all tobacco users at each visit. 2. Advise- strongly advice all users to quit. 3. Assess- determine the willingness and readiness the prt is to make a quit
attempt.1. Use the Stages of Change
4. Assist- aid the participant in quitting or planning for the future.5. Arrange- schedule a follow up contact
10/6/2017 38

4. Assessment Tools
Fagerstrom Test: A standard instrument for assessing intensity of physical addiction to nicotine. Most widely used evidence based practice tool. Appropriate basis for prescribing NRT.
10/6/2017 39

5. Nicotine Replacement Therapy (NRT)
10/6/2017 40

6. Educational Tool Kits
• Each site has brochures, pamphlets and educational material readily available to distribute the participants.
• Participants are encouraged to join a helpline/hotline.
10/6/2017 41

7. Quarterly Smoke-Outs
• 4 Smokeouts a year are held at each site highlighting smoking education and the potential for smoking cessation, introducing the idea of cessation in a positive manner and generating some energy around the issue.
• Smokeouts were launched after our participation in the National Great American Smokeout last November. Quarterly Smokeoutswere initiated due to the positive energy stimulated about smoking cessation and healthy living.
10/6/2017 42

8. Monthly Education Posters
• Recent research has suggested that simple basic tobacco education has produced the best outcomes for promoting smoking cessation.
• Posters are displayed at every site to educate participants about the benefits of quitting and the negative effects of tobacco products.
• This intervention is most potent if, in the routine course of delivering care, staff from various disciplines talk to participants about the content of the posters.
10/6/2017 43

9. Smoking Cessation Groups: Fresh Starts
10/6/2017 44

10. Celebration and Reward Rituals • Colored Bracelets: Why is this so important?
• The bracelets are meant to motivate our participants throughout recovery and into sobriety. The bracelets are symbolic and mark success. It is a way to acknowledge the achievements the participants have made as well as marking the amount of time they have remained sober.
• The colors designate specific milestones for the participants: • White (1 week) • Yellow (2 weeks) • Orange (1 month) • Blue (3 months) • Green (6 months) • Purple (1 year)
10/6/2017 45
Future Plans• Policy and clinical guidelines on Nicotine treatment
10/6/2017 46

Case Examples• R.S.- Pre-contemplative• G.B.- Contemplative• C.B.-Preparation• R.S.- Action• B.F.- Maintenance
10/6/2017 47

Integrated BH enables a PACE program to:
• Increase enrollment of people with complex psychiatric/addictions co-morbidities• Manage complex BH disorder cases in close collaboration with the IDT• Support other disciplines in interacting with participants with challenging
symptoms and behaviors• Increase BH knowledge and BH skills of IDT members• Initiate programming that builds self-efficacy and wellness in the participant
population and that addresses addictions treatment• Reduce ED and inpatient costs related to BH disorders.
10/6/2017 48

References• Centers for Medicare and Medicaid Services. “Programs of All Inclusive Care for the Elderly (PACE)
Manual, Chapter 8 IDT, Assessment, & Care Planning.” Accessed 9/16/17 at https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/pace111c08.pdf
• Cohen DJ, Davis M, Balasubramanian BA, Gunn R, Hall J, et al. (2015) Integrating Behavioral Health and Primary Care: Consulting, Coordinating, and Collaborating Among Professionals. Journal of American Board of Family Medicine 28; S21-S31.
• Miller BF, Brown Levey SM, Payne-Murphy JC, and Kwan BM. (2014) Outlining the Scope of Behavioral Health Practice in Integrated Primary Care: Dispelling the Myth of the One-Trick Mental Health Pony. Families, Systems, & Health 32; 338-343.
• Peek CJ and the National Integration Academy Council. Lexicon for Behavioral Health and Primary Care Integration: Concepts and Definitions Developed by Expert Consensus. AHRQ Publication No.13-IP001-EF. Rockville, MD: Agency for Healthcare Research and Quality. 2013. Available at: /sites/default/files/Lexicon.pdf
10/6/2017 49