sirs dan sepsis
DESCRIPTION
recommendedTRANSCRIPT

Systemic Inflammatory Response Syndrome (SIRS) & SEPSIS
Dr.H.Asril Zahari Sp.B.KBD

SEPSIS and It’s Disease spectrum
Various stages of disease Bacteremia SIRS Sepsis syndrome Sepsis shock : early and refractory
Definition
Infection Presence of microorganisms in a normally
sterile site. Bacteremia
Cultivatable bacteria in the blood stream. Sepsis
The systemic response to infection. If associated with proven or clinically suspected infection, SIRS is called “sepsis”.
American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference Committee. Crit Care Med. 1992;20:864-874.
SIRS (Systemic Inflammatory Response Syndrome)
The systemic response to a wide range of stresses. Temperature >38°C (100.4°) or <36°C (96.8°F). Heart rate >90 beats/min. Respiratory rate >20 breaths/min or
PaCO2 <32 mmHg.
White blood cells > 12,000 cells/ml or < 4,000 cells/ml or >10% immature (band) forms.
Note Two or more of the following must be present. These changes should be represent acute alterations from
baseline in the absence of other known cause for the abnormalities.
American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference Committee. Crit Care Med. 1992;20:864-874.

Severe Sepsis
Sepsis with organ hypoperfusion one of the followings : SBP < 90 mmHg Acute mental status change PaO2 < 60 mmHg on RA (PaO2 /FiO2 < 250) Increased lactic acid/acidosis Oliguria DIC or Platelet < 80,000 /mm3
Liver enzymes > 2 x normal
American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference Committee. Crit Care Med. 1992;20:864-874.

MODS(Multiple Organ Dysfunction Syndrome)
Sepsis with multiorgan hypoperfusion
Two or more of the followings: SBP < 90 mmHg Acute mental status change PaO2 < 60 mmHg on RA (PaO2 /FiO2 < 250) Increased lactic acid/acidosis Oliguria DIC or Platelet < 80,000 /mm3
Liver enzymes > 2 x normal
American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference Committee. Crit Care Med. 1992;20:864-874.
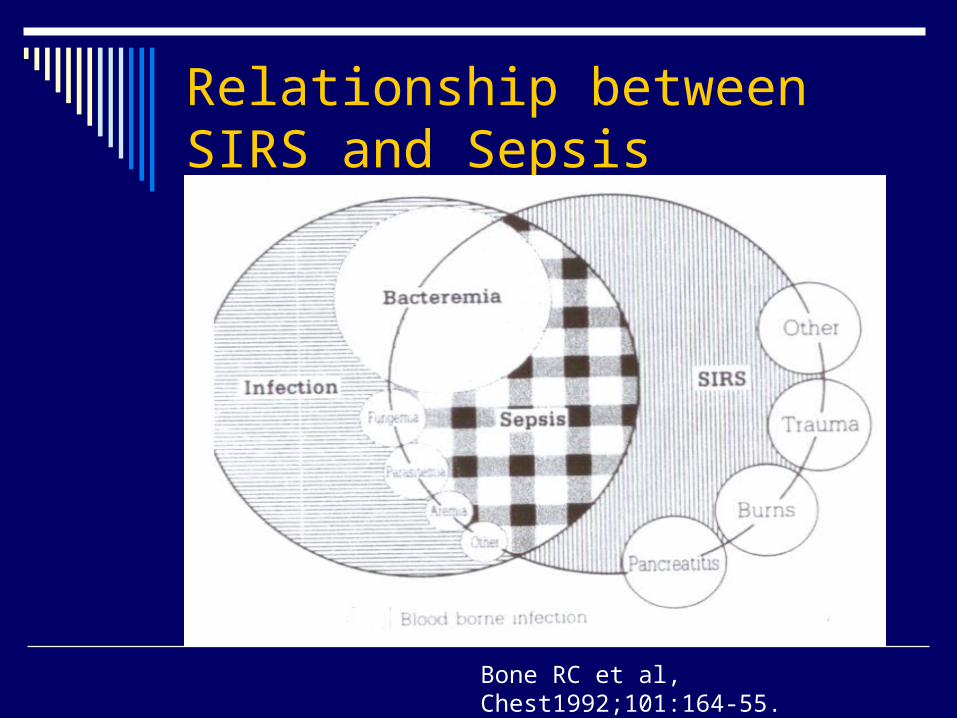
Relationship between SIRS and Sepsis
Bone RC et al, Chest1992;101:164-55.
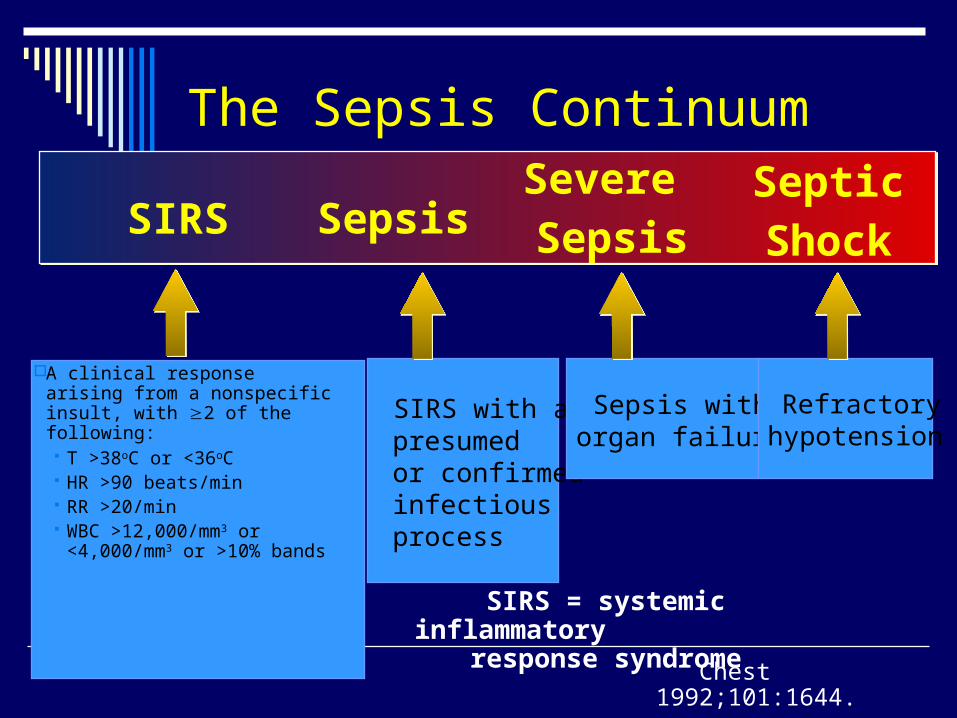
The Sepsis Continuum
A clinical response arising from a nonspecific insult, with 2 of the following: T >38oC or <36oC HR >90 beats/min RR >20/min WBC >12,000/mm3 or
<4,000/mm3 or >10% bands
SIRS = systemic inflammatory response syndrome
SIRS with a presumed or confirmed infectious process
Chest 1992;101:1644.
SepsisSIRSSevere Sepsis
SepticShock
Sepsis with organ failure
Refractoryhypotension

Mortality rate in SIRS
Rangel-Frausto, et al. JAMA 273:117-123, 1995.
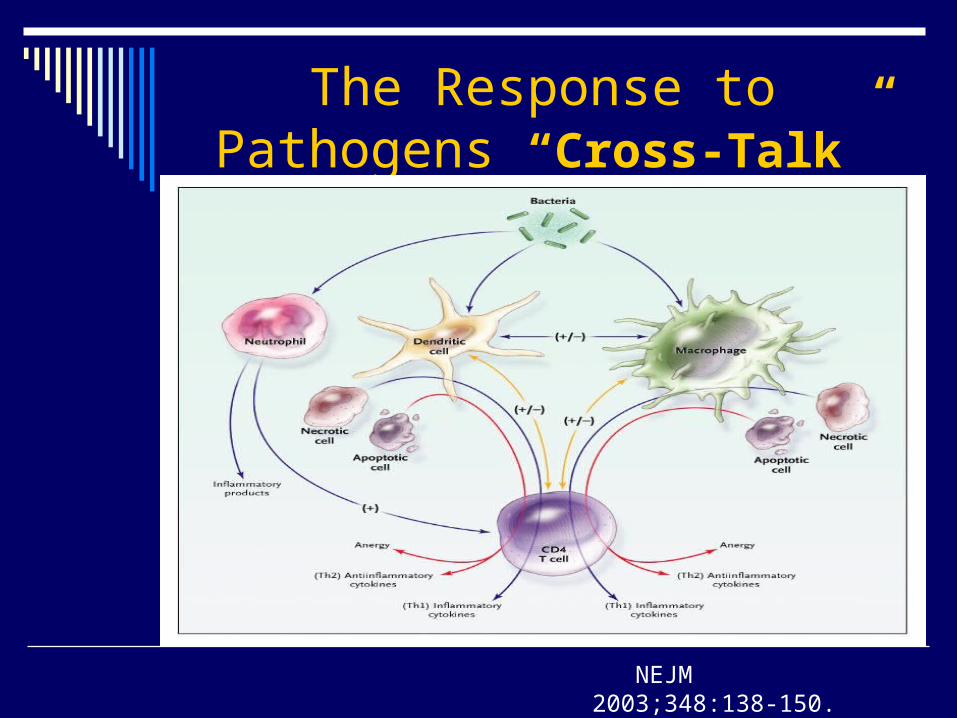
The Response to Pathogens “Cross-Talk”
NEJM 2003;348:138-150.

Inflammatory Response to Sepsis
NEJM 2006;355:1699-1713.

Procoagulant Response in Sepsis
NEJM 2006;355:1699-1713.

Pathogenesis of sepsis and septic shock
Angus DC, et al. Crit Care Med 2001, 29:1303-1310.

Pathogenesis of Severe Sepsis
InfectionInfection
Microbial ProductsMicrobial Products(exotoxin/endotoxin)(exotoxin/endotoxin)
Cellular ResponsesCellular Responses
OxidasesOxidasesPlateletPlatelet
ActivationActivationKininsKinins
ComplementComplement
Coagulopathy/DICCoagulopathy/DICVascular/Organ System InjuryVascular/Organ System Injury
Multi-Organ FailureMulti-Organ Failure
DeathDeath
EndothelialEndothelial damagedamage Endothelial damageEndothelial damage
CoagulationCoagulationActivationActivation
CytokinesCytokinesTNF, IL-1, IL-6TNF, IL-1, IL-6
Normal Systemic Response to Infection and Injury (1)
Leukocytosis Mobilizes neutrophils into the circulation Tachycardia Increases cardiac output, blood flow to
injuried tissue Fever Raises core temperature; peripheral
vasoconstriction shunts blood flow to injuried tissue. Occurs much more often when infection is the trigger for systemic responses
Mandell et al. Principals and Practice of Infectious Diseases6th ed;906:906-926.
Normal Systemic Response to Infection and Injury (2)
Acute-Phase Responses Anti-infective
Increases synthesis of complement factors, microbe pattern-recognition molecules(mannose-binding lectin, LBP, CRP, CD14, Others)
Sequesters iron (lactoferrin) and zinc (metallothionein)
Mandell et al. Principals and Practice of Infectious Diseases6th ed;906:906-926.

Normal Systemic Response to Infection and Injury (3)
Anti-inflammatory Releases anti-inflammatory neuroendocrine hormones
(cortisol, ACTH, epinephrine, α-MSH) Increases synthesis of proteins that help prevent
inflammation within the systemic compartmentCytokine antagonists (IL-1Ra, sTNF-Rs)Anti-inflammatory mediators (e.g.,IL-4, IL-6, IL-6R, IL-
10, IL-13, TGF-β)Protease inhibitors (e.g.,α1-antiprotease)Antioxidants (haptoglobin)
Reprograms circulating leukocytes (epinephrine, cortisol, PGE2, ?other)
Mandell et al. Principals and Practice of Infectious Diseases6th ed;906:906-926.

Normal Systemic Response to Infection and Injury (4)
Procoagulant Walls off infection, prevents systemic spread
Increases synthesis or release of fibrinogen, PAI-1, C4b Decreases synthesis of protein C, anti-thrombin III Metabolic
Preserves euglycemia, mobilizes fatty acids, amino acids Epinephrine, cortisol, glucagon, cytokines
Thermoregulatory Inhibits microbial growth
Fever
Mandell et al. Principals and Practice of Infectious Diseases6th ed;906:906-926.

Risk factors of sepsis
aggressive oncological chemotherapy and radiation therapy use of corticosteroid and immunosuppressive therapies for organ
transplants and inflammatory diseases longer lives of patients predisposed to sepsis, the elderly, diabetics,
cancer patients, patients with major organ failure, and with granulocyopenia.
Neonates are more likely to develop sepsis (ex. group B Streptococcal infections).
increased use of invasive devices such as surgical protheses, inhalation equipment, and intravenous and urinary catheters.
indiscriminate use of antimicrobial drugs that create conditions of overgrowth, colonization, and subsequent infection by aggressive, antimicrobial-resistant organisms.
Angus DC, et al. Crit Care Med 2001, 29:1303-1310.
Patients at increased risks of developing sepsis
Underlying diseases: neutropenia, solid tumors, leukemia, dysproteinemias, cirrhosis of the liver, diabetes, AIDS, serious chronic conditions.
Surgery or instrumentation: catheters. Prior drug therapy: Immuno-suppressive drugs, e
specially with broad-spectrum antibiotics. Age: males, above 40 y; females, 20-45 y. Miscellaneous conditions: childbirth, septic aborti
on, trauma and widespread burns, intestinal ulceration.
Angus DC, et al. Crit Care Med 2001, 29:1303-1310.

Source (usually an endogenous source of infection)
intestinal tract oropharynx instrumentation sites contaminated inhalation therapy equipment IV fluids. Most frequent sites of infection: Lungs, abdo
men, and urinary tract. Other sources include the skin/soft tissue and t
he CNS.
Angus DC, et al. Crit Care Med 2001, 29:1303-1310.

Diagnosis History
community or nosocomially acquired infection immunocompromised patient exposure to animals, travel, tick bites, occupational h
azards, alcohol use, seizures, loss of consciousness, medications
underlying diseases ; specific infectious agents Some clues to a septic event include
Fever or unexplained signs with malignancy or instrumentation
Hypotension Oliguria or anuria Tachypnea or hyperpnea Hypothermia without obvious cause Bleeding
Angus DC, et al. Crit Care Med 2001, 29:1303-1310.

Specific Infectious agents
Splenectomy (traumatic or functional) S pneumoniae, H influenzae, N meningitidis
Neutropenia (<500 neutrophil/ml) Gram-negative, including P aeruginosa, gram-
positives, including S aureus Fungi, especially Candida species
Hypogammaglobulinemia (e.g.,CLL) S pneumoniae, E coli
Burns MRSA, P aeruginosa, resistant gram-negatives
MacArthur RD, et al. Mosby, 2001:3-10. Wheeler AP, et al. NEJM 1999;340:207-214. Chaowagul W, et al. J Infect Dis 1989;159:890-899.
Specific Infectious agents
Aids P aeuginosa (if neutropenic), S aureus, PCP
pneumonia Intravascular devices
S aureus, S epidermidis Nosocomial infections
MRSA, Enterococcus species, resistant gram-negative, Candida species
Septic patients in NE of Thailand Burkholderia pseudomallei
MacArthur RD, et al. Mosby, 2001:3-10. Wheeler AP, et al. NEJM 1999;340:207-214. Chaowagul W, et al. J Infect Dis 1989;159:890-899.

Diagnosis
Physical Examination essential In all neutropenic patients and in patients wit
h as suspected pelvic infection the physical exam should include rectal, pelvic, and genital examinations
perirectal, and/or perineal abscesses pelvic inflammatory disease and/or absce
sses, or prostatitis
Angus DC, et al. Crit Care Med 2001, 29:1303-1310.
Signs and Symptoms
Nonspecific symptoms of sepsis : not pathognomonic fever chills constitutional symptoms of fatigue, malaise anxiety or confusion
absent symptoms in serious infections, especially in elderly individuals
Angus DC, et al. Crit Care Med 2001, 29:1303-1310.

Complications
Adult respiratory distress syndrome (ARDS) Disseminated Intravascular Coagulation (DIC) Acute Renal failure (ARF) Intestinal bleeding Liver failure Central Nervous System dysfunction Heart failure Death
Angus DC, et al. Crit Care Med 2001, 29:1303-1310.

Surviving Sepsis Campaign
Guidelines for Management of Severe Sepsis and Septic Shock
Dellinger RP, et al. Crit Care Med 2004; 32:858-873.

Before the initiation of antimicrobial therapy, at least two blood cultures should be obtained
At least one drawn percutaneously At least one drawn through each vascular access device if
inserted longer than 48 hours Other cultures such as urine, cerebrospinal fluid, wounds, respiratory
secretions or other body fluids should be obtained as the clinical situation dictates
Other diagnostic studies such as imaging and sampling should be performed promptly to determine the source and causative organism of the infection
may be limited by patient stabilityWeinstein MP. Rev Infect Dis 1983;5:35-53
Blot F. J Clin Microbiol 1999; 36: 105-109.
Diagnosis
Dellinger, et. al. Crit Care Med 2004, 32: 858-873.

Sepsis resuscitation bundle
Serum lactate measured Blood cultures obtained before antibiotics administered Improve time to broad-spectrum antibiotics In the event of hypotension or lactate > 4 mmol/L (36 mg/dL)
a. Deliver an initial minimum of 20 mL/kg of crystaloid (or colloid equivalent)
b. apply vasopressors for ongoing hypotension In the event of persistent hypotension despite fluid
resuscitation or lactate > 4 mmol/L (36 mg/dL) a. achieve central venous pressure of > 8 mmHg b. achieve central venous oxygen saturation of > 70%
Hurtado FJ. et al. Crit Care Clin;2006; 22:521-9.

Sepsis management bundle
Fluid resuscitation
Appropriate cultures prior to antibiotic administration
Early targeted antibiotics and source control
Use of vasopressors/inotropes when fluid
resuscitation optimized
Surviving Sepsis Campaign Management Guidelines Committee. Crit Care Med 2004; 32:858-873.

Sepsis management bundle
Evaluation for adrenal insufficiency Stress dose corticosteroid administration Recombinant human activated protein C (xigris)
for severe sepsis Low tidal volume mechanical ventilation for
ARDS Tight glucose control
Surviving Sepsis Campaign Management Guidelines Committee. Crit Care Med 2004; 32:858-873.

Infection Control
Appropriate cultures prior to antibiotic
administration Early targeted antibiotics and source control
Surviving Sepsis Campaign Management Guidelines Committee. Crit Care Med 2004; 32:858-873.

CVP : central venous pressure MAP : mean arterial pressure
ScvO2: central venous oxygen saturation
Early Goal-Directed Therapy
NEJM 2001;345:1368-77.

49.2%
33.3%
0
10
20
30
40
50
60
Standard Therapy n=133
EGDTn=130
P = 0.01*
*Key difference was in sudden CV collapse, not MODS
28-day Mortality
Early Goal-Directed Therapy Results
NEJM 2001;345:1368-77.

Antibiotic use in Sepsis (1)
The drugs used depends on the source of the sepsis Community acquired pneumonia
third (ceftriaxone) or fourth (cefepime) generation cephalosporin is given with an aminoglycoside (usually gentamicin)
Nosocomial pneumonia Cefipime or Imipenem-cilastatin and an aminoglycoside
Abdominal infection Imipenem-cilastatin or Pipercillin-tazobactam and
aminoglycoside
Angus DC, et al. Crit Care Med 2001, 29:1303-1310.
Antibiotic use in Sepsis (2)
Nosocomial abdominal infection Imipenem-cilastatin and aminoglycoside or Pipercillin
-tazobactam and Amphotericin B Skin/soft tissue
Vancomycin and Imipenem-cilastatin or Piperacillin-tazobactam
Nosocomial skin/soft tissue Vancomycin and Cefipime
Urinary tract infection Ciprofloxacin and aminoglycoside
Angus DC, et al. Crit Care Med 2001, 29:1303-1310.
Antibiotic use in Sepsis (3)
Nosocomial urinary tract infection: Vancomycin and Cefipime
CNS infection: Vancomycin and third generation cephalosporin or
Meropenem Nosocomial CNS infection:
Meropenem and Vancomycin Drugs will change depending on the most likely cause of the patient
's sepsis Single drug regimens are usually only indicated when the organism
causing sepsis has been identified and antibiotic sensitivity testing
Angus DC, et al. Crit Care Med 2001, 29:1303-1310.

New Drug in Treating Severe Sepsis
It is the first agent approved by the FDA effective in the treatment of severe sepsis proven to reduce mortality. Activated Protein C (Xigris) mediates many actions of body homeostasis. It is a potent agent for the: suppression of inflammation
prevention of microvascular coagulation reversal of impaired fibrinolysis
Angus DC, et al. Crit Care Med 2001, 29:1303-1310.

NEJM;355:1699-1723.

Sepsis Cascade

Activated Protein C (Xigris)
NEJM;355:1640, October 19, 2006.
