singhealth regional health system - wordpress.com · tiong bahru . telok blangah . chinatown ....
TRANSCRIPT

SingHealth Regional Health System Study Visit to Sweden
Oct – Nov 2017
1

2
ACUTE/SECONDARY
INTERMEDIATE/LONG TERM
SingHealth
PRIMARY CARE
TERTIARY/QUATERNARY
SingHealth
Total Population in the East: 1.36 Million 35% of Total Resident Population
Pop: 350,000
Pop: 745,000
Pop: 270,000

SingHealth
3
Voluntary Welfare Organisations
Community Development Councils (CDC) & Grassroots Organisations
Other Community Hospitals & Nursing Home
National Agencies
SingHealth Community Partners
Expanded Community
Partners

Beyond Programmes to Holistic Person-Based Care
Focusing on the needs of the population Moving from provider-centric (setting) to
person-centric (care themes)

Preparing our Healthcare System for Person-Based Communities Of Care
Outpatient to Community
Community Health Hospital Care Community Care
Community Health Screening
Primary Care Network
Falls and Frailty Screening
Mental Health Promotion
Community Health Post
Polyclinics
FMC/CHC
Community Nursing
Hospital To Home
Health Management
Unit (Biomedical) Geriatric Service Hub
End Of Life Care
Community Hospital
Nursing Home
Community Networks for Seniors
Care Line (Psychosocial)

Community Health Screening
Population segmentation
Population health and disease
prevention
Continuing Community Care
Synergising and Scaling Services
Objectives Increase accessibility of health screening and preventive health services to residents in the Eastern RHS through closer collaboration with grassroots and social agencies
Early detection of chronic disease conditions or risk factors for early intervention to prevent or delay onset of chronic diseases
3 KEY FOCUS AREAS
1 To improve follow up rate for individuals who
have been referred to GP for abnormal results (at least 65%)
2 Strengthening health screening intervention and follow-up at CHPs (~85%) or Pre-DICTED
Programme*
*Pre-Diabetes Interventions and Continued Tracking to Ease-out Diabetes (Pre-DICTED) programme
3 Transition to Enhanced Screen For Life (SFL) in FY17
Increased awareness of health conditions and predisposing bio-psychosocial risk factors
Increase adoption of healthy lifestyles • Healthy diets and regular exercise
Outcome
Prevent or delay onset of chronic diseases
10,424 10,083 9,288
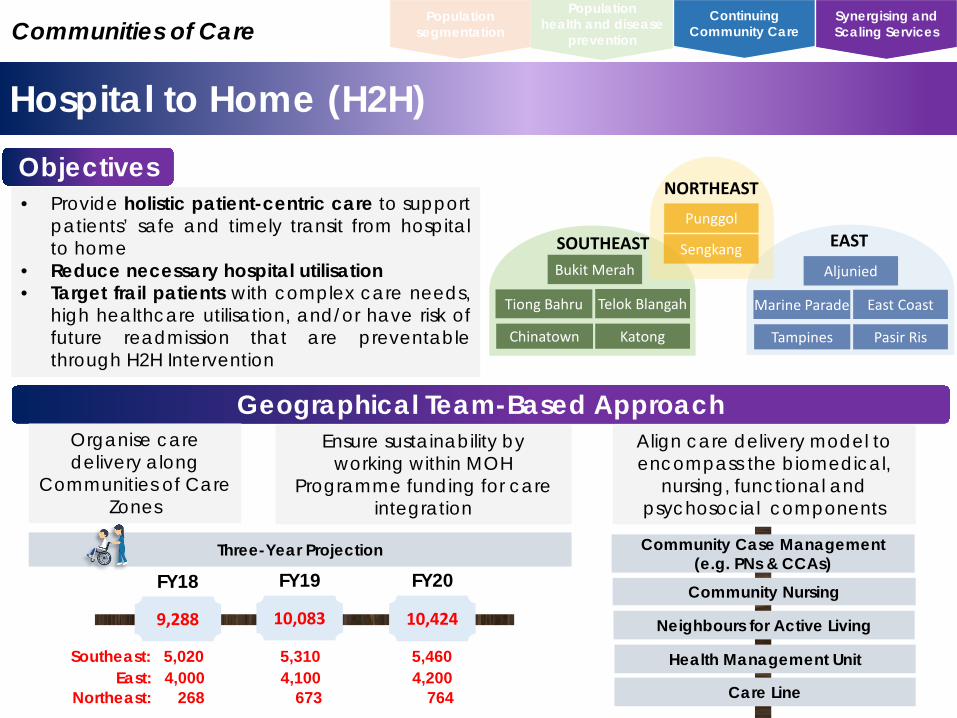
Hospital to Home (H2H)
Population segmentation
Population health and disease
prevention
Continuing Community Care
Synergising and Scaling Services Communities of Care
Objectives • Provide holistic patient-centric care to support
patients’ safe and timely transit from hospital to home
• Reduce necessary hospital utilisation • Target frail patients with complex care needs,
high healthcare utilisation, and/or have risk of future readmission that are preventable through H2H Intervention
Bukit Merah
Telok Blangah Tiong Bahru
Chinatown Katong
Aljunied
East Coast Marine Parade
Tampines Pasir Ris
Punggol
Sengkang SOUTHEAST
NORTHEAST
EAST
Geographical Team-Based Approach Organise care delivery along
Communities of Care Zones
Ensure sustainability by working within MOH
Programme funding for care integration
Align care delivery model to encompass the biomedical,
nursing, functional and psychosocial components
Neighbours for Active Living
Community Nursing
Three-Year Projection
FY18
Care Line
Health Management Unit
FY19 FY20
Southeast: 5,020 5,310 5,460 East: 4,000 4,100 4,200 Northeast: 268 673 764
Community Case Management (e.g. PNs & CCAs)
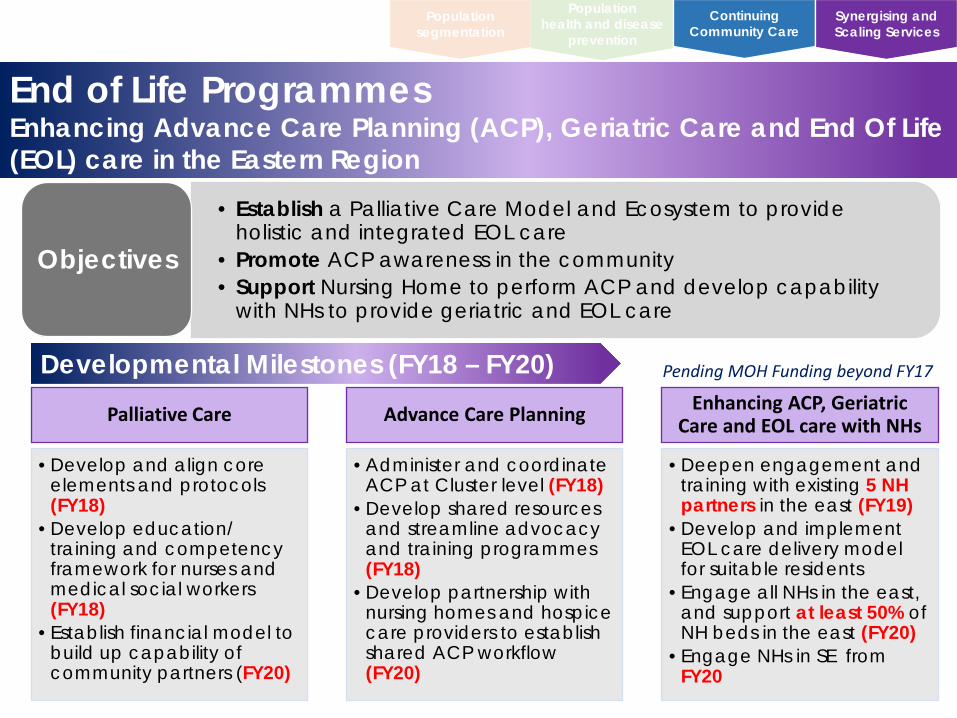
End of Life Programmes Enhancing Advance Care Planning (ACP), Geriatric Care and End Of Life (EOL) care in the Eastern Region
Population segmentation
Population health and disease
prevention
Continuing Community Care
Synergising and Scaling Services
• Establish a Palliative Care Model and Ecosystem to provide holistic and integrated EOL care
• Promote ACP awareness in the community • Support Nursing Home to perform ACP and develop capability
with NHs to provide geriatric and EOL care
Objectives
Developmental Milestones (FY18 – FY20) Palliative Care
•Develop and align core elements and protocols (FY18)
•Develop education/ training and competency framework for nurses and medical social workers (FY18)
•Establish financial model to build up capability of community partners (FY20)
Advance Care Planning
•Administer and coordinate ACP at Cluster level (FY18)
•Develop shared resources and streamline advocacy and training programmes (FY18)
•Develop partnership with nursing homes and hospice care providers to establish shared ACP workflow (FY20)
Enhancing ACP, Geriatric Care and EOL care with NHs
•Deepen engagement and training with existing 5 NH partners in the east (FY19)
•Develop and implement EOL care delivery model for suitable residents
•Engage all NHs in the east, and support at least 50% of NH beds in the east (FY20)
•Engage NHs in SE from FY20
Pending MOH Funding beyond FY17

Population segmentation
Population health and disease
prevention
Continuing Community Care
Synergising and Scaling Services
SingHealth Eastern Region
Individual Care
Communities of Care
Preventive Care
First Contact Care
Transitional Care
Chronic, Aged & End of Life Care
• Health promotion & protection • Disease prevention
• Perform assessment & triage • Meet immediate care needs • Refer or escalate as required
Simple • Support & empower self management • Chronic disease management • Facilitate emergent care plan
• Re-enablement approach • Support hospital to home (H2H)
Complex • Integrated case management • Key staff assigned to navigate • Coordinate and care manage
Roles of Community Nurses
SingHealth Community Nursing
Continuing quality care in community
and ageing in place
Right siting &
Integration of care
Building healthy &
empowered community
Community Nursing
Community Coordinators Physicians Allied Health
Professionals
Objectives

SingHealth Community Nursing Geographical Team-Based Nursing
Population segmentation
Population health and disease
prevention
Continuing Community Care
Synergising and Scaling Services
Geographical Team-Based Approach • Deeper understanding of the population
needs in the respective zones • Skill-mix to cater to different levels of
needs and care • Greater accessibility • Ease of collaboration and building
capability for health & social care personnel
• Increase efficiency in resource allocation
Communities of Care
*3 years pilot funded by MOH will be implemented by the east and southeast region
Bukit Merah
Telok Blangah Tiong Bahru
Chinatown Katong
Aljunied
East Coast Marine Parade
Tampines Pasir Ris
Punggol
Sengkang SOUTHEAST
NORTHEAST
EAST
Three-Year Pilot* – Workload & Manpower Targets
Year 1 Year 2 Year 3
Community Nurses
Care Coordinator Associates
Manpower (Cumulative) 44 56 72
16 23 31.0
Workload (Pending MOH Funding) East Southeast
2,720 5,140 8,160 3,500 4,150 5,105
E: 5; SE: 11 E: 10; SE: 13 E: 16; SE: 15
E: 16; SE: 28 E: 25; SE: 31 E: 37; SE: 35
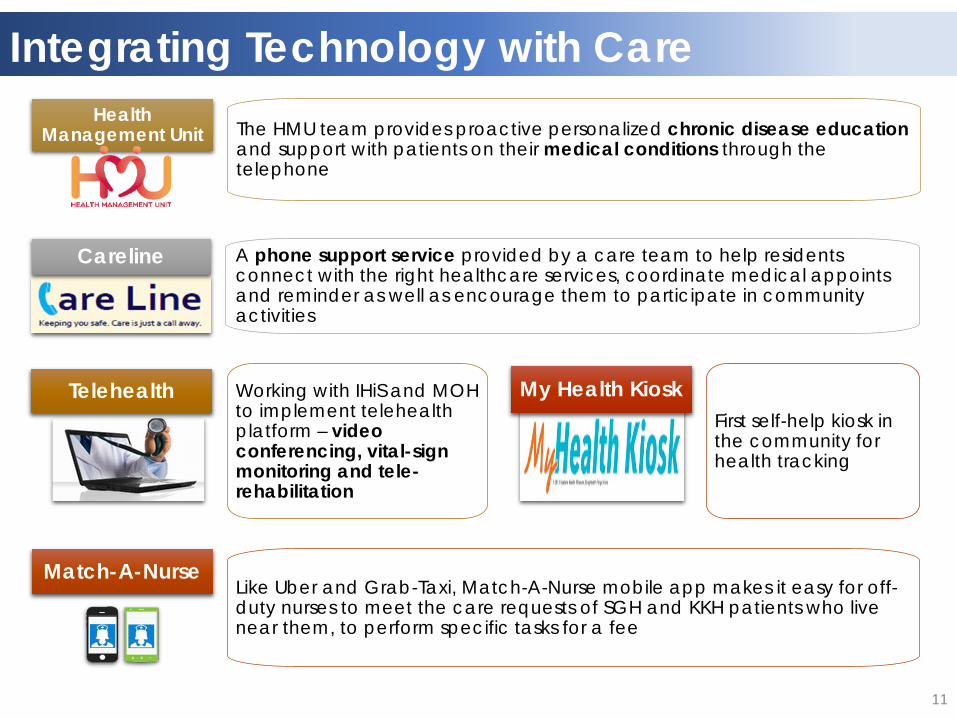
Integrating Technology with Care
A phone support service provided by a care team to help residents connect with the right healthcare services, coordinate medical appoints and reminder as well as encourage them to participate in community activities
Careline
The HMU team provides proactive personalized chronic disease education and support with patients on their medical conditions through the telephone
Health Management Unit
Working with IHiS and MOH to implement telehealth platform – video conferencing, vital-sign monitoring and tele-rehabilitation
Telehealth
Like Uber and Grab-Taxi, Match-A-Nurse mobile app makes it easy for off-duty nurses to meet the care requests of SGH and KKH patients who live near them, to perform specific tasks for a fee
Match-A-Nurse
First self-help kiosk in the community for health tracking
My Health Kiosk
11
Person-Centred Care

Expand & strengthen partnerships with community and MOH
Scale up “Esther” projects with potential for transferability at
SingHealth regional level
Mainstream person-centred initiatives with high impact at national level
A unifying care philosophy for care providers to provide person-
centred care
Person-centred improvements that can be scaled and shared
A common framework adopted nationally for high impact person-
centred care
Person-Centred Care Philosophy “Esther” Network
Objectives Outcomes
Developmental Milestones • Co-construct strategic plan with community partners and “Esthers”
• Engagement with stakeholders to further the impact of “Esther” improvement work (FY18 to FY20) • Establish the platforms and sponsors to own improvement initiatives in the eight domain areas identified
by “Esthers” • Run “Esther” Cafes in the community & SQ members (Target: 40 to 50 participants by FY18, 40 SQ
members by FY18) • Two-days workshop for Group Service Quality by FY18
• Ongoing Capacity Building and Improvement Work (FY18 – FY20) • Continue training of 50 “Esther” coaches & trainers for capacity building • Collaborate with HSR to interview community partners (Target: 15 to 20 community partners by
FY18) • Dovetail with the development of Community Network for Seniors (FY18 – FY20)
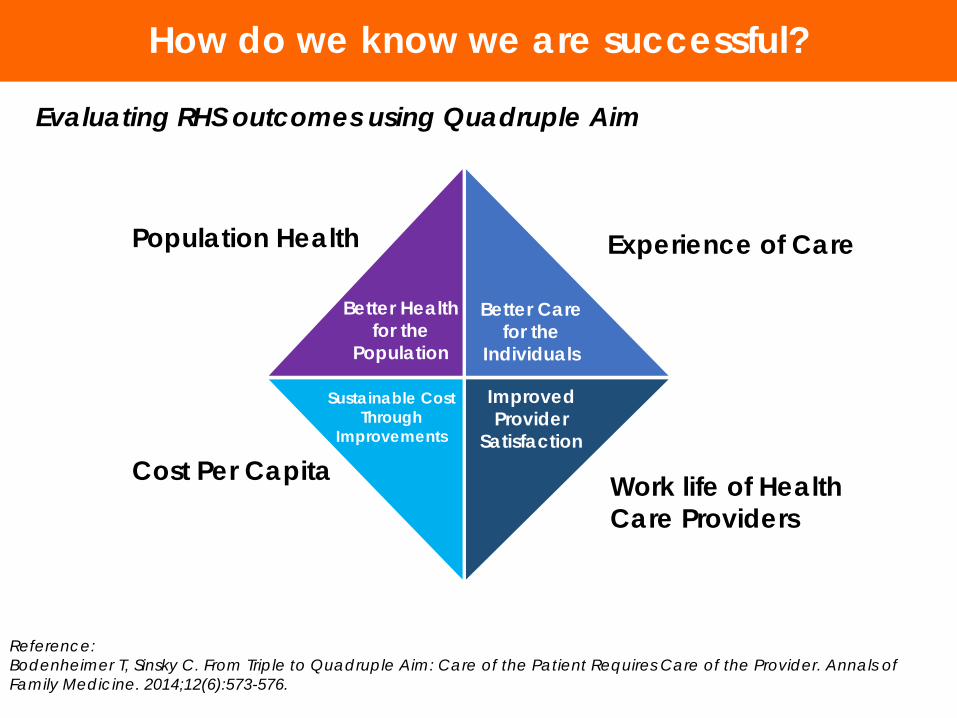
Evaluating RHS outcomes using Quadruple Aim
Work life of Health Care Providers
Experience of Care Population Health
Cost Per Capita
How do we know we are successful?
Reference: Bodenheimer T, Sinsky C. From Triple to Quadruple Aim: Care of the Patient Requires Care of the Provider. Annals of Family Medicine. 2014;12(6):573-576.
Better Health for the
Population
Better Care for the
Individuals
Sustainable Cost Through
Improvements
Improved Provider
Satisfaction

Thank You
15