simulator sickness in the uh-60 (black hawk) flight simulator
TRANSCRIPT

rILL C 2LUSAARL Roport No. 89-25
"--" ., -- I "
. ' , -. .=. .. .. . . . . - - .
Simulator Sickness in the UH-60(Black Hawk) Flight Simulator
V')
By
N Daniel W. Gower, Jr.
<Biodynamics Research Division
and
<Jennifer Fowkles
Essex CorporationOrlando, Florida
DTICSeptember 1939 ELC, i
Approved for public release; d)2tlibution unllmliod.
89 11 1-' 1 66United Sttes Army Aeromedical Research Laboratory
F:nrf Rm,-Lor A lhrami .( 1 ,9-9Q9
DISCLAIMER NOTICE
THIS DOCUMENT IS BEST
QUALITY AVAILABLE. THE COPY
FURNISHED TO DTIC CONTAINED
A SIGNIFICANT NUMBER OF
PAGES WHICH DO NOT
REPRODUCE LEGIBLY.

UNCLASSIFIEDS YZU71 T Y-T WuS F 'A T -0'v 0;'- .*
Form Apro~e'1
REPORT DOCUMENTATION PACE G %8 It, 077 ,,A0 18
a REPCO;T SEC' j CA t)('..
UNICLA SS IFIE~D
I2a SECURITY (LAn A .A T 3j > .~
IDeputv Commndi c tor Scitence Public r ~.s - -
20 DECLASSI CAT C'. .tA GS-~
4 PEAFGR%1iG 4TiA 70' 'NP i '.S M .~ .CC 'A
H UISAARL Report No. 89-256a NAVE OF 1CM G i6AN- 'A' C "' 7~C ~O a ',AVE OFN',&~;.' ~U.S. Army Aerormedical Research 0f av~i'fe) U. S . rm ed ica I RL ce~irch and 't-.'1-.n
l3boratorv ~P-'.
6( ADDRES5 (Cr,. State, j'~y ZIP C,--e)7 A 3 'ty. S:a t e a'x -J o,- eP.O. Box 577 Fort DetrickFort Ruck'r, M. 36362-52Q Frederick, "M 2170 -,,1
Ei %A.7 OF v0.. e0' OL. 4 CE E'~O Vt % T i 5
ORG ANI ZA';3 (;f appltcaibe)
8c ADDRE SS (Ctty. State, and ZiP Cxidp 10 $6 'C F LO'.G
f;0A 0, E CT S 7
E'EVt EO rO %
I I E (Inclde~p 5 'curirY CO' ii,(Jit
(U) S imilIato -S icknes s in th fie UN-0 B lac k H~a'< Flight S~rnulator
12 PERSONAL AU TH( R(S
Diqnie1 W. Co-t.r, .7r., and Jeinnjfr ale
1,1a TYPE OP REPORT T E WVE;: 1 DATE OF REPCRT (year, Month, Day S5 PACt LC-.
Final rT' ___ 1t'4 s C"t: 0 1 I e r 7
6 SUPPLE.%'AR T ~ 2
I7 IS I L'DjL S .: "e co ere~ee 4 rweeujr) Ind< Cc' . y L T, '~r
FTLE, 5 C) lr T-1) - i i. t r ; , Ti t -s s, t r ai n in , o I ion C c 'Kn ec;s !, I a L n,
i m , I- I
19 A,3S-RACT c)onvnupo er,,e,!re 4f neref#,, ,'x1 *dertt'v by bi'xk n t~re)
-The U . S. Ar%- vrn , a ra c 1 . *r 1 I 01)r'' 1 r'.'22re field ctj;or oPerati.on'l "ih t
fi, -e refcr I F t 1 t o n iT 0 rt -,* I~ an t t d ' p t that o c Ir i n T21':!I It 7r;
edue to vi Rull r . 'M ta ); 1 rt ;,t ,ritit ionT, or, CC'i ii n of tlw tW1' Tr''-C'
a t ,ni, of f I I ' -; oI ; ' -ae ,: (:c o f p. c I ti c -SvcpT~ t 7n] I
a. .' .ria'r .'xperientc-, cairrent "tate '
L ' th, I Il~ I rio, .nd fl ,i t uJ.-n -micc ire prait-wnr o. Thi;
rkeDort r' ti Srt Ai r -7, 1'11 to t!'e 10 lIv v q117oulatc'r s'!IdI'
th 11C .~ m I'- j I, 0I Ii Fl rti . II,- 2;f fairtl r roinfoict-; ti:, '!tar ot(( T ~T", I i .)-I ,~pT '17-1 rt
1P 1t 1n -r' - f' T :
S0 5 L . .. 2 'A(2,C..S A,'
C A" -- -
DODIorm 1473, JUN 836 -sn'gtr~' ~'A 'P'-t.
Table of coilte its
Page
List of figures................................................. 2I List of tables..................... ............................ 3
Introduction.................................................... 5U.S. Army's involvement with simulator sickness............. 5
The nature of simulator sickness............................ 6
Materials....................................................... 9es i t'-- zrafft system............
Description of the simulation system........................ 14
Method.......................................................... 25Aviators..................................................... 25Measures..................................................... 25Pro~cedure.................................................... 27
Results......................................................... 28Symptomatology............................................... 28Postural stability........................................... 34Correlations................................................. 34Pilot variables.............................................. 35Simulator variables.......................................... 3GTraining variables........................................... 37
Symptomatology by mission and seat............................ 36Mission...................................................... 38Seat................................... ...................... 49
Discussion...................................................... 42
Recommendations................................................ 43
References.................................................. *'*45
Appendix A. Simulat. z-:kness survey........................ 49
Appendix B. Variable Q--criptions............................ 65
Lisr of figures
Figure Page
1. General arranigement ................................... 10
2. General arrangement (continued) ......................... 11
3. Principal dimensions .................................. 12
4. Machine gun M60D installation ........................... 13
5. Typical UH-50 simulator installation ................... 15
6. Typical UH-60 flight simulator........................ 167. Simulator cockpit and instructor/operator
compartment ......................................... 20
8. Collimating optics representation .................... 22
9. Ocular convergence representation ....................... 22
10. Basic collimation concept .............................. 21
11. SSQ visuomotor subscale ........... ................... 32
12. SSQ nausea subscale ................................... 32
13. SSQ disorientation subscale ............................. 33
14. SSQ total severity score .............................. 33
Accession FoPr
NTIS GRA&I LDTIC TABnarnouncedJuatifloation
Distribution/
Avallabilit Codess
Avail and/or
list Spefial
2

List of tables
Table Page
1. Basic, advanced, and instrument maneuvers, andemergenzy procedures that can be performedin the simulator .................................... 18
2. Percentage (frequencies) of aircrews reportingpostflight symptomatology in the UH-60simulator ........................................... 29
3. Percentage of aircrews reporting key symptomatologyin seven helicopter simulators ........................ 30
4. Pre- and post-SSQ means (standard deviations) andpaired t-test values ................................ 31
5. Means, standard deviations, minimum/maximum scores,t-test values, and observations for pre- andpost--WOFLEC, SONLEC, and SOPLEC measures ............. 34
6. Interccirelations among variables ....................... 35
7. FrequenciEs for variable "Discomfort hamperstraining' ........................................... 37
8. SSQ scores by mission (means and standarddeviations) ......................................... 38
9. Scenario content data (means and standard deviations)for different missions flown in the UH-60simulator ........................................... 39
10. SSQ scores by seat (means and standard deviations) .... 40
11. Mission and scenario content data for copilot andpilots .............................................. 41
3

This page intentionally left blank.
4
Li

Introduction
U.S. Army's involvement with simulator sickness
Prior to the actual fielding of the AH-64 Apache combatmission simulator (CMS) at U.S. Army installations, training ofApache pilots was conducted in the Singer Link facility atBinghamton, New York. Anecdotal information indicated some ofthe pilots and instructor operators (10) were experiencingsymptoms of simulator sickness resembling those reported in U.S.Navy and U.S. Coast Guard systems. Some students took Dramamine'to alleviate their symptoms. In May 1986, documentation of theproblem reached the U.S. Army Aeromedical Research Laboratory(USAARL) at Fort Rucker, Alabama. In July 1986, the AviationTraining Brigade at Fort Rucker formed a study group to examinethe Apache training program. One of the issues studied wassimulator sickness.
A survey of existing training records and a literature searchwere conducted by USAARL in August 1986. Training records of 115students from the CMS showed that 7 percent of the students hadsufficient symptoms to warrant a comment on their grade slips.The literature search led USAARL investigators to visit the NavilTraining Systems Center (NTSC) in Orlando, Florida. From thatassociation has grown a working relationship geared to capitalizeon lessons learned from past research and expand the database ofsimulator sickness studies. As part of that search, it also wasdiscovered that a U.S. Army flight surgeon had conducted anindependent survey of the incidence of simulator sickness in theAH-1 Cobra flight weapons simulator (FWS) located in Germany(Crowley, 1987).
In the report to the Army study group, it was recommended aproblem definition study be conducted to ascertain more accurate-ly the scope and nature of the problem of simulator sickness in '1the Apache CMS. The request for that study was rcceived from theDirectorate of Training and Doctrine, Fort Rucker, Alabama, inFebruary 1987. The protocol for the study was approved by theUSAARL Scientific Review Committee on 4 May 1987. USAARL repor;88-1 documents the results of that first study.
As reported in 5altzley et al. (1989, in press), 25 percentof those reporting aftereffects indicated their symptoms per-sisted longer than 4 hours while 8 percent lasted 6 hours orlonger. The Army data presented in that report was contaminatedwith effects experienced by Apache pilots who had previousexperience with the Cobra FWS. Problems with other Ar-.y simula-tor systems also have been documented since the first study.Most notable, aviators training in the new AH-I Cobra simulatozwere complaining of postsimulator exposure aftereffects which
5
.. .. .... .. .. .... .. .. ...... . .... ... ... ... ..1 1 ,1 I III I 1 1 I I I_
outlasted the training period by several hours. The need forfurther studies was apparent.
In September 1988, USAARL received a request from the Direc-
torate of Training ana Doctrine at the U.S. Army Aviation Centerat Fort Rucker, Alabama, requesting further field studies toassess the incidence of simulator sickness in the remainingvisually-coupled flight simulators. The protocol was approved 19October 1988 and collection of data began in January 1989. Thisreport documents the results of the data collected at the UH-60simulator site at Fort Rucker.
The nature of simulator sickness
Simulator sickness is considered to be a form of motion
sickness. Motion sickness is a general term for the constella-tion of symptoms which result from exposure tc motion or certainaspects of a roving environment (Casali, 1986), although changingvisual motions (Crampton and Young, 1953; Teixeira and Lackner,1979) may induce the malady. Pathognomonic signs are vomitingand retching; overt signs are pallor, sweating, and salivation;symptoms are drowsiness and nausea (Kennedy and Frank, 1986).Postural changes occur caring and after exposure. Other signs(Colehour and Graybiel, 1966; McClure and Fregly, 1972; Money,1970; Stern et al., 1907) include changes in cardiovascular,respiratory, gastrointestinal, biomedical, and temperatureregulation functions. Other symptoms include general discomfort,apathy, dejection, headache, stomach awareness, disorientation,lack of appetite, desire for fresh air, weakness, fatigue,confusion, and incapacitation. Other behavioral manifestationsinfluencing operational efficiency include carelessness andincoordination, particularly in manual control. Differenceshet ,een the symptoms of simulator sickness and more common formsof motion sickness are that in simulator sicKness, visual sy..;p-
toms tend to predominate and vomiting is rare.
Advancing engineering technologies permit a ranqe of capabil-
ities to simulate the real world through very compelling kinemat-
ics and computer-generated visual scenes. Aviators demand
realistic simulators. Howcver, this synthetic environment can,on occasion, be so compelling that conflict is establisheabetween visual and vestibular information specifying orientation
(Kennedy, 1975; Om, n, 1980; Reason and Brand, 1q75). It has been
hypothesized that in simulators, this discrepancy occasionsdiscomtort, or "simulator sickness" as it has been labeled, andthe cue conflict theory has been offered as a working modol fcr
the phenomenon (Kennedy, Berbaum, and Frank, 1984). In brief,
the model postulates the referencing of motion informationsignaled by the retina, vestibular apparatus, or sources of
somatosensory information to "expected" values based on a neural
6

store which reflects past experience. A conflict between ex-pected and experienced flight dynamics of sutficient magnitucan exceed a pilot's ability to adapt, inducing in some case:;sirulator sickness.
The U.S. Navy conducted a survey of simulator sickness in 10flight trainers where motion sickness experience questionnairesand performance tests were administered to pilots before andafter some 1,200 separate exposures (Kennedy et al., 1987b).From these measures on pilots, several findings emergcd: (a)Specific histories of motion sickness were predictive of simula-tor sickness symptomatology; (b) postural equilibrium wasdegraded after flights in some simulators; (c) self-reports ofmotion sickness symptomatology revealed three major symptomclusters: Gastrointestinal, visual, and vestibular; (d) certainDilot experiences in simulators and aircraft were related toseverity of symptoms experienced; (e) simulator sickness in-cidence varied from 10 to 60 percent; (f) substantial perceptualadaptation occurs over a series of flights; and (g) there wasalmost no vomiting or retching, but some severe nausea anddrowsiness.
Another recent study suggests thaL inertial enerqy spectra inmoving base simulators may contribute to simulator sickness(Allgood et al., 1987). The results showed the incidence ofsickness was greater in a simulator with energy spectra in theregion described as nauseogenic by the 1981 Military Standard1472C (MIL-STD-1472C) and high sickness rates were experienced asa function of time exceeding these very low frequency (VLF)limits. Therefore, the U.S. Navy has recommended, for anymoving-base simulator which is reporLed to have high incidencesof sickness, frequency times acceleration recordings of pilot/simulator interactions should be made and compaied with VLFguidelines from MIL-STD-1472C. However, in those cases whereillness has occurred in a fixed-base simulator, other explana-tions and fixes are being sought.
Of particular concern in the area of safety are simulatorinduced posteffects. Go;er et al. (1987) showed that as symptoms
decreased over flights for pilots training in the AH-64 CMS,siggesting that pilots were adapting to the discordant cues inthe simuletor, postflight Pixia increased suggesting that pilotswere having to readapt to the normal environmenL. Such rt' ta-tion phenomena parallel findings from other motion environmentsincluding long-term exposure onboard ships (Fregly and Graybiel,
1965), centrifuges (Fregly and Kennedy, 19;5) and space flight(Homick and 11eschke, 1977). For example, Graybiel and Lackner(1983) found 54 percent of the posteffects of parabolic flightlasted longer than 6 hours and 14 percent lasted 12 hours ormore. In their report, the primary symptoms reported weredizziness and postural disequilibrium. The similarity of
7

symptomatolcgy between these experiences leads us to believes4Aulator sickness poses safety of flight issucs which cnrict beignored.
8
____ j m

Material -
DescriDtion of the aircraft 7eyster
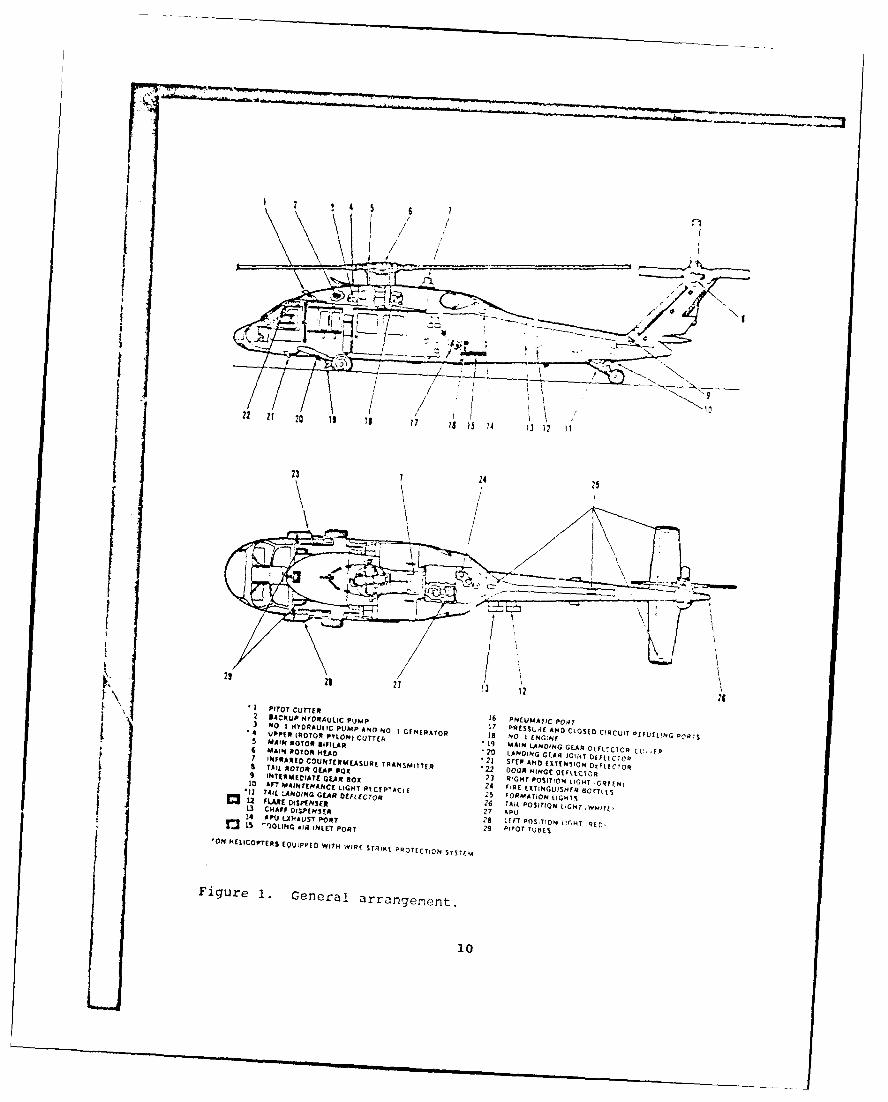
The UH-60A (Black Hawk) is a t.;in turbine ngine, singlerotor, semimonocoque fuselage, rotary-wing helic)pter manufac-tured by the Sikorsky Aircraft Company (Figires 1, 2, and 3)(TM 55-1520-237-10). The aircraft is designed to operate with acrew of three: Pilot, copilot, and crew chief. In that con-figuration, it can carry 11 ccmbat equipped soldiers. Alterna-eseating arrangements can be made to seat 11. In a _Iition, theaircraft also can carry internal and external carg:-. The primarymission of the aircraft is the transport cf troops, suepli s, anequipment. Other missions include training, mobilization,concept development as well as medical evacuaCion and discst.rrelief. The EH-60A aircraft is a rpecially-outfittd aircraftused for electronic surveillance and electronics counterme.surefunctions. When operating with the edical evacuation littercarousel installed, the aircraft operates with a crew of four,the additional crcwmemb r being a medical ?idman. The EH-5C) usesa crew of four with the additional crewmember to operate theelectronic warfare devices.
The main rotor system has four blades which are constructedof titanium and fiberglass. Propulsion is supplied by two T700-GE-700 engines operating in parallel. As opposed to th2 UH-!,which the Black Hawk is renlacing in the inventory, the U[i-60 hasa landing gear system consisting of two main landing gear whichare nonretractable and a tailwheel assembly, also ncnretractable.Design of the UH-60 is closely equated with titt specified in theCrashworthy Design Guide making the Black Hawk the first rotary-wing aircraft designed with crashwrthiness included from theoutset of the design proess.
Arimament consists of two 7.62 mm machine guns, one on eachside of the helicopter, mounted inside the forward cabin (Figure4). The weapons are mounted on : rotating arm assembly whichallows the weapon to be locked outboard in the firing position orstowed insid,:, the aircraft h'h the -,,-.icon is not needed. Theweapons can be remov:ed from T.ho uircratz and used in grounddefense with the bipod extend d. Medical evacuaticn aircraft donot have that armament installd and the crew is protected bypersonal side arms only.
The gross weight of the aircraf-t is 20,250 pounds. Addition-al kit installations includ e e en d range tank, both internaland external, interim 1 ret:.ue his-ts, the litter carousel formedical evacuation, infrar, i -uppre-3ion, htlde anti-icing,icing capability, blackout J* :vices, winterization kits, Astatic/rappelling kit.
9
23
CI.~AP OI~pNS ~ 22
A CKUP MVIH AU "C 'O -P 2 6 NE UMAOTICN L'oHT
F3u r 1 G enD RA L arrpAND N Il I
-4 P 1 R4R TORPVON) I NOE10h

3031 32 33 35 38
-1 Ti
30
10 UPPER ANTICOLLISION LIGHT31 TAIL WHEIL STRUT 46 AFT AVIONICS CO;APARTME NI DOOP$32 TAIL 0O1IE SHAFT (O N NELIrOFTTRS EQUIPPID33 M1AIN ROTO R EiDE O (FOUP) WITH AFT AVION. UPARTM1,NY34 P40. 2 HYDRAULIC PUMP AND0 NO 2 ENRATOR 47 1145 aLOWER mllk, (TYE
3~PYLON4 CUT TER 4-84~ .PLNP~SHNE36 HELAEER AIR INTAAKE PORT 49 TAI L PYLON SERV CE LAUDEA ISAME BOTH SIDIES)37 CEPIT ST tP (SAME 8 0TH SIDES) 50 STABILATOR38 EXTERNAL ELECT ICAL POWER RECEPTACLE 51 TAIL ROTOR BLAOE (IOURI39 NO2 ENGINE D2E/IIELAY AREA CCOOLINr AlR INTAKE (SAME 80TH SICPSI40 ICE OCTICTOR *53 WINDSHIELD 14'ST DE'l ECYOR1 Ak'aIENT SENSE PORT 1, 54 INUSIIILLD WIPER Clf FI.ECTOR42 ENI'.INE FA'RING/WORK PLATtORM (SAME BO1TH SIOE',l S5 AVICNICS CC14PARTIALNT
0I43 CONC0ENSER EXHAUST, STEP 56 OAT SE43CR". STEPS (tA'4E BOTH SDrlI) 57 ICE OCE TCOR45 t;RVITY PEFUELIHO PORT (SAME BU'H S,,l 51 58 PYLON COOLING AIR I4TAKE
ON HELICCPTfRS [QUPPEC WITH *IqE STPIKE PVlC/YTION SYST! M
Figure 2. Cenural LdrrmcjrIP(:7.Ift (contini.r J)

MT Ctvm~ I I;PTfsos W- T ~~Wm7TWFAND VRNAL
10EE FET.9 NHS20F( 2ICE
7 4INCH~~~~ AUSLANGE ER FUELGEEIt~FE IrEA
-7 FEET - ?cHs - FUSELAGE WIDTH WITH___
9FEET - 8~- INHE
9N2~E INCHES
-A
I FEET_____ *E FE
7 'N00 S INCHES
14FETH -iN OTRS ADPLNFL( 1Fl C
O.RA LNHE DIAMETER ~ )NIH S- --
Figure~~~~~ 3. PrPplETcn;~n;

M-60 DEKtOYED POSITONSAME BOTH SiDES) ----
AMM, WITION m-AO STO~BOX i (SAE BOTH SIDE5)
AMMUN11ION AND M-1C STOWVAGE
(J(S AME BOTH SWiD
NFORWARD AFT
) UECTOqCONTROL.BSAG
1'01*30' FORWARD AFT
70 /160-CX7I!AION
FIELD OF FiPC fit10 OF FRE
Ficuro 4. Machine rpmn M'CD in, tailation.
13
Both pilot and copilot have cmatrols for flying the aircraft.p The aircraft is fully instrument rated and can be tlown without
ref*ercnce to the outside environment cqually well from eitherpilot's station. fno aircraft is equipped with an automaticflight control system (\FCS) which enhances the stability andhandling qualities of the helicopter. This systea is comprisedof five subsystems. The stabilator subsystem positions thestabilator, which is located at the rear of the aircraft, bymeans of electromechanical actuators in response to crllective,airspeed, pitch rate, and lateral acceleration inputs. A pitchbias actudtor enhances the static stability in the 1ongitudinalaxis. The stability augmentation system (SAS) provides shortterm rate damping in the pitch, roll, and yaw axe . Thetrim/flight path stabilization systems serve as a basic autcpilotproviding control positioning an:'d force gradient functions.
Currently, there are several systems under consideration foraddition to the airframe for special missions. One of these is aforward looking infrared sensor (FLIP). In certain aircraft,this has been installed- by means of a turret on the nose of theaircraft displaying information on a CRT-type screen on thainstrument panel. Other devices which display the same informa-tion to the pilot by means of a full heads up display on thehelmet visor also have been tested but not yet approved foracquisition. In conjunction with the Doppler navigation systeminstalled in the aircraft, there aue rap sheet displays whichgain information from the Doppler system and display the ap-propriate map sheet to the pilot on a kneeboard-type dpparatus.These systems reflect the sophistication to which the Army hasgone in the war-fightinj capabilities of the avition fleet.
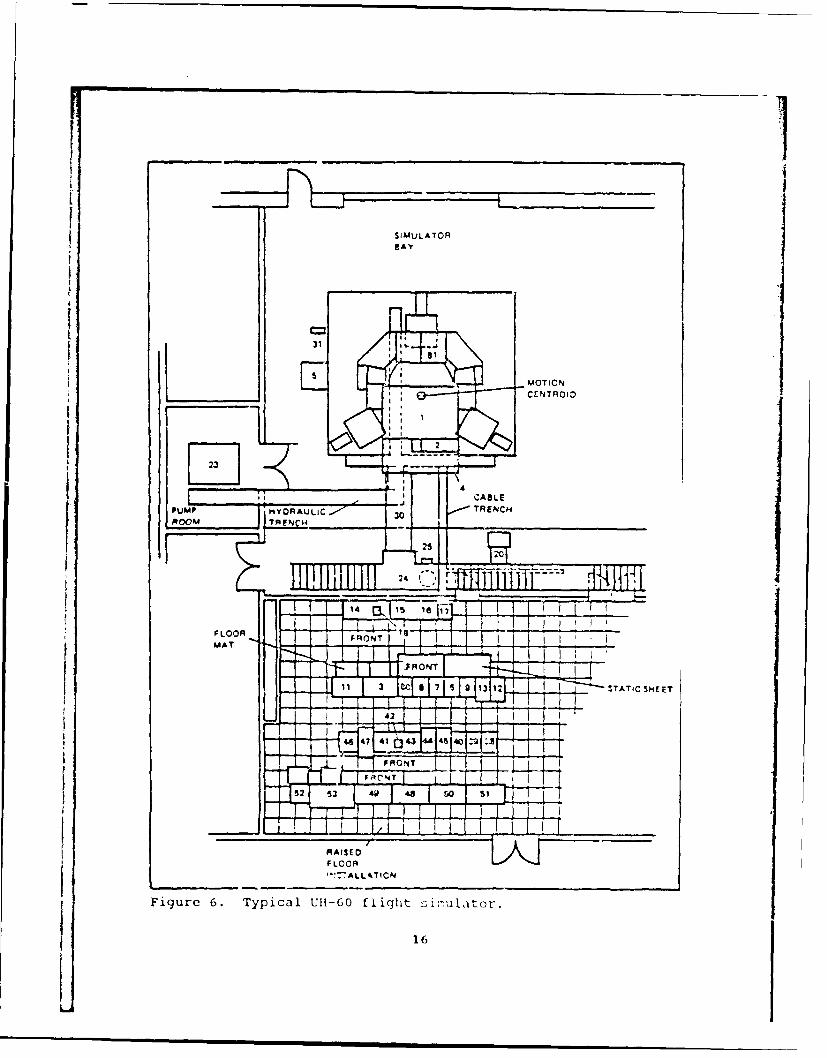
Description of the simulation system
The Ull-60 flight simulator is a motion-base device designedfor training aviators in the use of the UH-60 Black Hawk heliccp-ter (Figures 5 and 6). The device consists of a simulatorcompartment containing a cockpit with pilot and copilot stations,instructor operator (10) station and an observer station, and asix-degree-of-freedom motion system. The simulator is equippedwith a visual system that simulates natural environm-1ntal sur-roundings. A central computer system controls the operation ofthe simulator complex. The simulator is used to provide traininain aircraft control, cockpit preflight proceduros, instru-entflight operations, visual tlight operations, sling load opera-tions, external stores sthsystc -;, night vision gee training,as well as those tactical skl]-:I I-, ic ary to colupt in-of-tho-ear,-h (NlOE) flight', lot;-level ii iht, and contour fli iht . Apartial listing of training t sV; that can . or:., in th,'simu.ator is shown in Table 1.
14

- 4'
i:z~-Lii- .-. /
~-~4/ ,>~, ~
"-
-C
0-' ------ ~z~---~
.4~)
'-4'-4
,~- .--.- "
-'-4
- 0
'-4
"-4U')
/C
-- 4
- U
a'' a
15
16OTION
CE NTRFO ID
PupHAAALI ' TRNC
000o 3 0~ 3 T TC H E
FLOORF tLOONMAT F ,.OTtC
Figure6. Typcal UI-60 fIFh40:Wuatr
11 JCJ1617 1 9 1
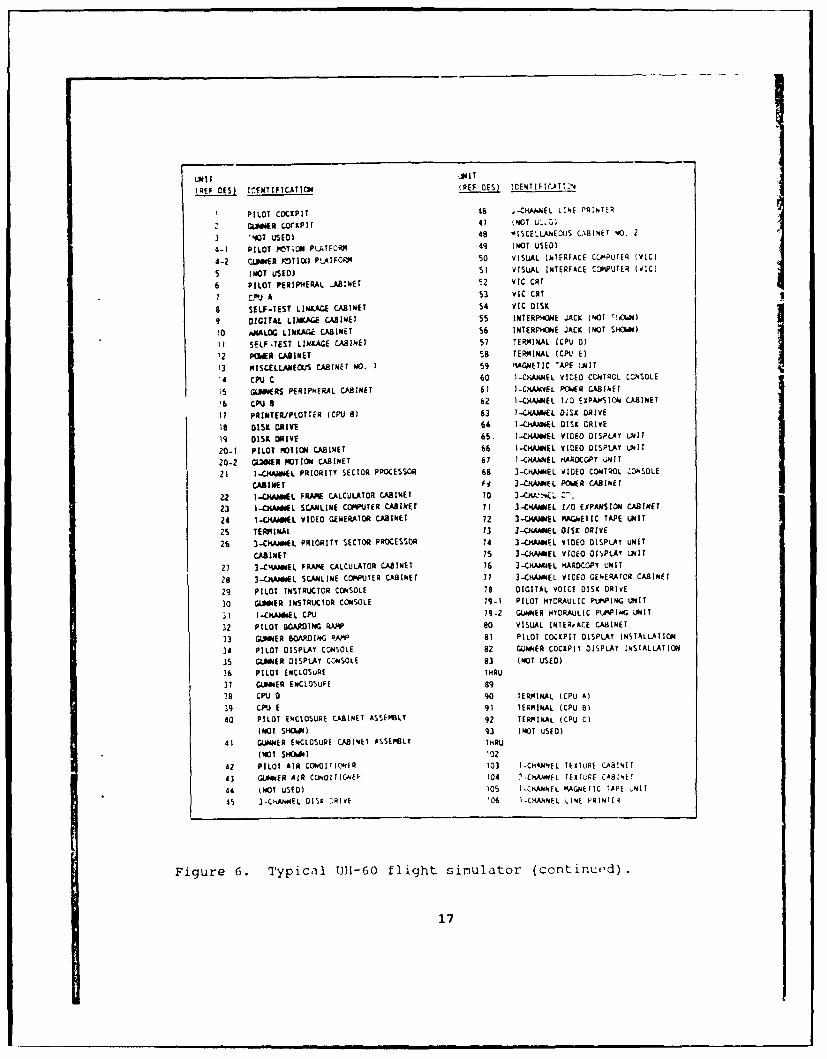
UN IT jmIT
(REF DES) ICENTIFICATION (REF DES) jCETIFIrJT12N
PILOT COCKPIT 46 .-Cl.AJ.EL LINE PRINTEq
GLNNER OCKPIT 41 (NOT U',Zl
3 :07 USEO 48 -ISCELLAECJS CABINET 40. 2
4-1 PILOT PMTiON PLATFCPRq 49 (MOT uSED)
4-2 C.JMER 3TI]OI PLATF044 50 VISUAL INTERFACE CCPPUTER (VIC)
5 (NOT USED) SI VISUAL INTERFACE CWPUTER (VIC)
6 PILOT PERIPHERAL .ARINET 52 VIC CRT
1 c!"J A 53 VIC CRT
a SELF-TEST LINKAGE CABINET 54 VIC DISK
9 DIGITAL LIWAE CABINET 55 INTERPMONE JACK (NOT '',OWN)
I0 ANALOG LINAGE CA8INET 56 INTERPV"E JACK (NOT SHOWND4)
II SELF-TEST LINKAGE CABINET 57 TERMINAL (CPU D)
'2 PIs R CABINET 58 TER4INAL (CPL' E)
I3 ISCELLANEOUS CABINET NO. 1 59 MAGNETIC 'APE t,IT14 CPUI C 60 I-CHANNEL VIDEO CCNTADL C,NSOLE
is GUWRS PERIPHERAL CABINET 61 I-CKiANNEL PCIWER CABINET'6 CPUSB 6 I.-CHAMEL 1/0 EXPA,SICN CABINET
I1 PRINTER./PLOTTiR (CPU 81 63 )-CNAAWEL OiSX DRIVE
is DISK DRIVE 64 1-CfANImEL DISK DRIVE
19 OISK DRIVE 65. I-C)WA EL VIDEO DISPLAY UNI T
20-1 PILOT MOTION CABINET 66 I-CiANiEL VIDEO DISPLAY UNIT
20-2 GLinER MOTION CA8INET 67 1-CHANEL KAROCOPY UNIT
21 I-CKAiEL PRIORITY SECTOR PROCESSOR 68 3-CHANNEL VIDEO CONTROL ,ONSOLE
CABINET f4 3-CANNEL PoR CASINEr
22 1-CH&i L FRAAIP CALCULATOR CABINET TO 3-C ' :.L '-
23 I-CiM*IL SCAJiLINE COMPUTER CABINET 1I 3-CHANNEL I/O EXPANSION CABINET
24 1-OtUM L VIDEO GENERATOR CABINET 72 3-CMANNEL ,GNET IC TAPE UNIT
25 TERMINAL T3 3-CANEL 0ISK DRIVE
26 3-CMANmEL PRIORITY SECTOR PROCESSOR 74 3-CHANNEL VIDEO DISPLAY UNIT
CABINET IS 3-CANNEL VIDEO oIWPLAY UNIT
27 3-CMNwEL FRAANE CALCULATOR CABINET 16 3--CHANUEL HARDCOPT UNIT
28 3-CHAIEL SCANLINE COPJUTER CABINET 11 3-CHANEL VIDEO GENERAtOR CABINET
29 PILOT INSTRUCTOR CONSOLE 78 DIGITAL VOICE DISK DRIVE
30 GUER INSTRUCTOR CONSOLE T9-T PILOT HYDRAULIC PtPWPING LUNIT
31 I-CAiL CPU 79-2 GUNNER HYDRAULIC PLAHPING UNIT
32 PILOT BOARING RAW' 80 VISUAL INTE~rAC.E CA8INET
33 GUIER SCA ING RAW* 81 PILOT COCKPIT DISPLAY INSTALLATION
34 PILOT DISPLAY CONSOLE 82 GUNNER COCKPIT DISPLAY INSTALLATION
35 GAUIOER DISPLAY CONSOLE 83 (NOT USED)
36 PILOT ENCLOSdRE THRU
37 GUMER ENCLOSUPE 89
28 C JD 90 TERMINAL (CPU Al
39 CPU E 91 TERMINAL (CPU B)
40 PILOT ENCLOSURE CABINET ASSEMBLY 9? TERIINAL (CPU C)(NOT SHCIWN) 93 (NOT USED)
41 GUNER ENCLOSURE CA814ET ASSEPSLT THRU(NOT SHOW) i0z
42 PILOT AIR CONDITiCNER 103 I-CHKNNEL TEXTuRE C.ABINET
43 GUMER AIR CONOITIG, NE 104 .-ChAhEL TEXTURE CA814T
44 (NOT USED) 0S I-CHMNEL AGNEIC TAPE NIT
45 3-C'IAL4EL DI ,K CRIVE 106 I-CKANNEL LINE PRINTER
Figure 6. Typical Ull-60 flight simulator (continuod).
17
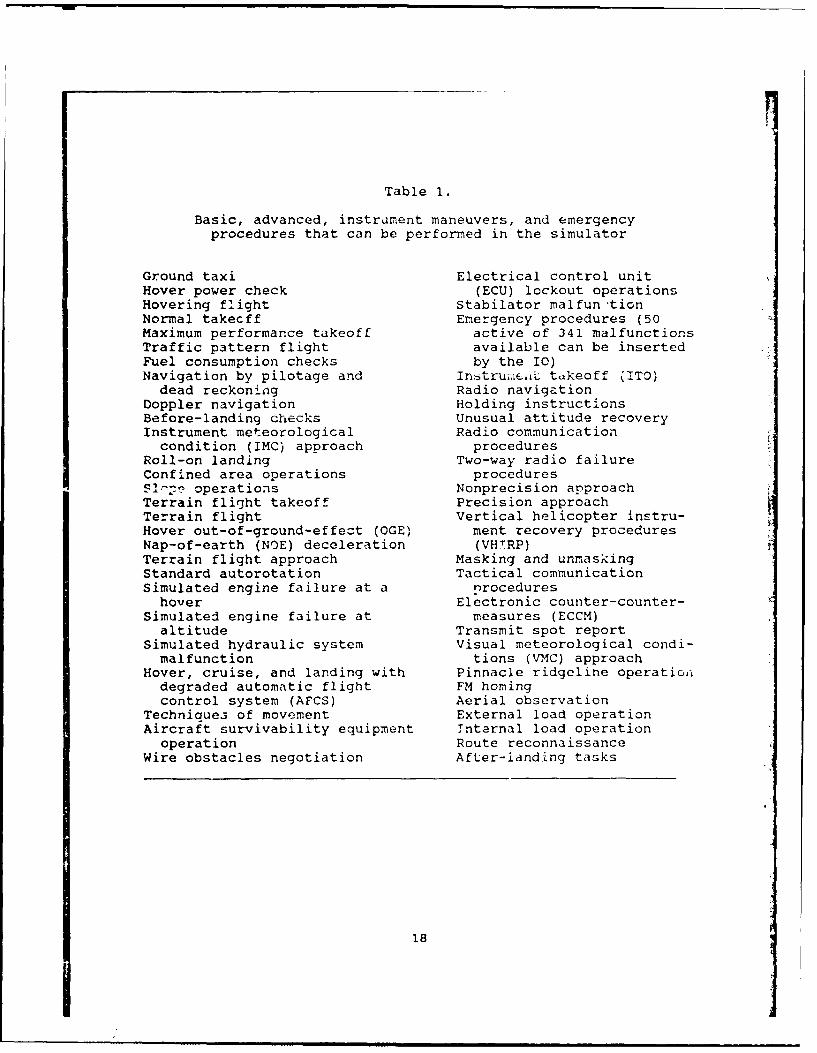
Table 1.
Basic, advanced, instrument maneuvers, and emergencyprocedures that can be performed in the simulator
Ground taxi Electrical control unitHover power check (ECU) lockout operationsHovering flight Stabilator malfun'tionNormal takecff Emergency procedures (50Maximum performance takeoff active of 341 malfunctionsTraffic pattern flight available can be insertedFuel consumption checks by the I)Navigation by pilotage and InstruiukLt tukeoff (ITO)dead reckoning Radio navigation
Doppler navigation Holding instructionsBefore-landing checks Unusual attitude recoveryInstrument meteorological Radio communication
condition (IMC) approach proceduresRoll-on landing Two-way radio failureConfined area operations procedures] operations Nonprecision approach
Terrain flight takeoff Precision approachTerrain flight Vertical helicopter instru-Hover out-of-ground-effect (OGE) ment recovery proceduresNap-of-earth (NOE) deceleration (VH-RP)Terrain flight approach Masking and unmaskingStandard autorotation Tactical communicationSimulated engine failure at a nrocedureshover Electronic counter-counter-
Simulated engine failure at measures (ECCM)altitude Transmit spot report
Simulated hydraulic system Visual meteorological condi-malfunction tions (VMC) approach
Hover, cruise, and landing with Pinnacle ridgeline operationdegraded automatic flight FM homingcontrol system (AFCS) Aerial observation
Techniaues of movement External load operationAircraft survivability equipment Tnternal load operation
operation Route reconnaissanceWire obstacles negotiation After-landing tasks
18

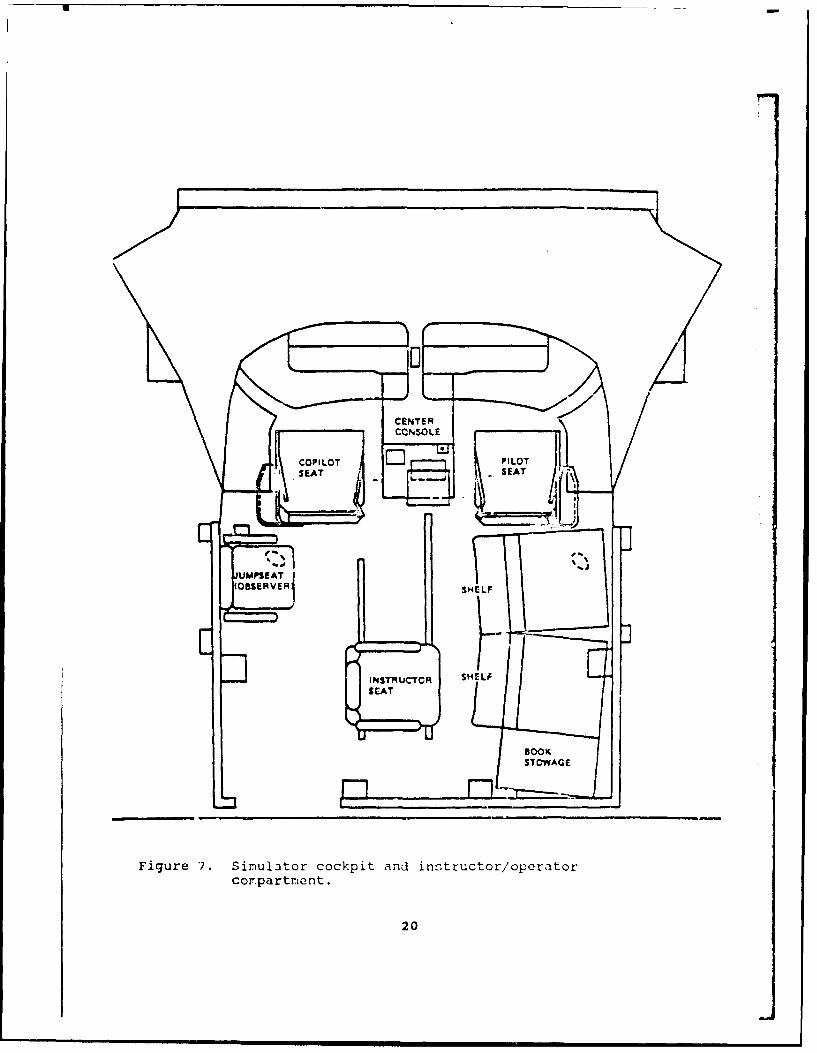
The simulator compartment houses the cockpit and 10 station(Figure 7). Within the cockpit are all the controls, indicators,and panels located in the aircraft. Controls which are notfunctional are physically present to preserve the appearance of a100 percent config-iration. Loudspeakers are located in thesimulator compartment to sim,'late aural cues.
Each of the pilot's seats are vibrated individually tosimulate both continuous and periodic oscillations and vibrationsexperienced by the crew during normal and emergency flightconditions and maneuvers. However, these vibrations are isolitedfrom the 10 and observer stations.
Cooling of the compartment is provided by a single airconditioner outside of the compartment enclosure on the simulatorroom floor. A thermostat mounted on the right bulkhead in theaft portion of the compa.tment and a two-speed fan providecontrol of the inside environment.
The simulator compartment is mounted on a 60-inch six-degree-of-freeaom motion system consisting of a moving platform assemblydriven and supported from below by six identical hydraulicactuators. The motion system provides pitch, roll, and yaw,lateral, lonqitudinal, and vertical movement, includi:ng combina-tions of them. Motion of the simulator compartment can be con-trolled to simulate motion due to pilot inputs as well as thoseresulting from rotor operation, rough air and wind, and changesin aircraft center-of-gravity, as well as emergency conditionsand system malfunctions. All .iotions except pitch are washed outto the neutral position after the computed accelerations havereached zero. Pitch attitude is maintained as necessary tosimulate sustained longitudinal acceleration cues.
The motion system simulates the complex and repeated cuesoccurring during all the maneuvers associated with the airwork.Turbulence, when used by the instructor-operator, is superimposedon the maneuver being performed with the apprcpriate effect onyaw and roll, climb and descent, and variations in airspeed. Themotion system supcrimpo us all normal periodic oscillations ofthe aircraft, lateral instability, and aircraft vibration up to 5cycles per second. The electrohydrauiic seat shaker is used tosimulate continucus high frequency vibrations while isolatingvibration effects Irom other cockpit-mounted hardware.
Motion can be frozen at any instant and the simulator has theability to enter a crash override mode where motion can continuedespite impact with the ground or other obstacles.
19
CONSOLE
FigureILO P.ILu~orccpt~d ntutrOpToCoSEArtSEAt
LIMPS2A
The pilot and copilot stations are provided with forward,left, and right side window displays. The visual generationsyst-m consists of two separate functional areas. The first isthe visual display system (VDS) which presents the wide-angle-collimating video image to the crew. The digital image generator(DIG) system is a full-color xisual display that provides imageryfor day, night, and dusk scenes as well as replicating theeffects of the searchlight/landing light on the visual displays.The instructor-operator must set the eye point in the initialcondition setup. This function sclects the viewpoint (eitherpilot's station or copilot's station) to be displayed on theforward displays. This is necessary because they both willdisplay the same image.
The database is a generic European scene of an area 100 by 80kilometers. The displays are either full color or monochromatic.The monochromatic scene display is designed specifically to becompatible with the use of night vision goggles (NVG). Duringselection of this mode, the leadship lights are blanked and anexhaust trail is generated from the leadship. The simulator doesnot input directly to the NVGs except for the out-the-window(OTW) imagery.
The computer system consists of a central processing unit andfive auxiliary processing units. The CPU has memory that can beaccessed by both itself and the auxiliary processing units.Visual displays are controlled by DIG inputs that are modified byinputs from other units such as the simulator navigation/communi-cation identification subsystem, instructional subsystem, and airvehicle subsystems. The navigation/communication identificationsubsystem provides position data for the aircraft the simulatoris replicating (ownship). The instructional subsystem forwardsinformation that details the visual environment, scene lighting,target paths through the database, target status, and landinglight status. The air vehicle subsystem sends informationrelevant to the ownship position rates, altitude, and attitude.All of these inputs are stored in the shared memory of the mainsimulator control computer.
The collimating optics used in this simulator are shown inFigure 8. The alignment of the optics ir. this system producesparallel light rays giving the appearance that the image is atoptical infinity. As shown in the diagram at Figure 9, our eyesprovide distance measuring information to the brain based partlyor, the angle between the eyes, or ocular convergence. As objectsmove closec tn the viewer, the eyes must converge in order forboth eyes to remain focused on the object. As the object mov-,mfurther away th2 angle increases giving the brain d ita on tho
21

distance. Beyond a point approximately 50 feet away from theviewer, the eyes point in virtually parallel directions.
CRT
BEAMVSPLITTE R~
fYEPOINTS SPHERICALCONCAVE
ci MIRR
Figure 8. Collimating optics representation.
vIEWEvR - -
EYEPOINT C -- ,-
Figure 9. Ocular converqence representaticn.
22

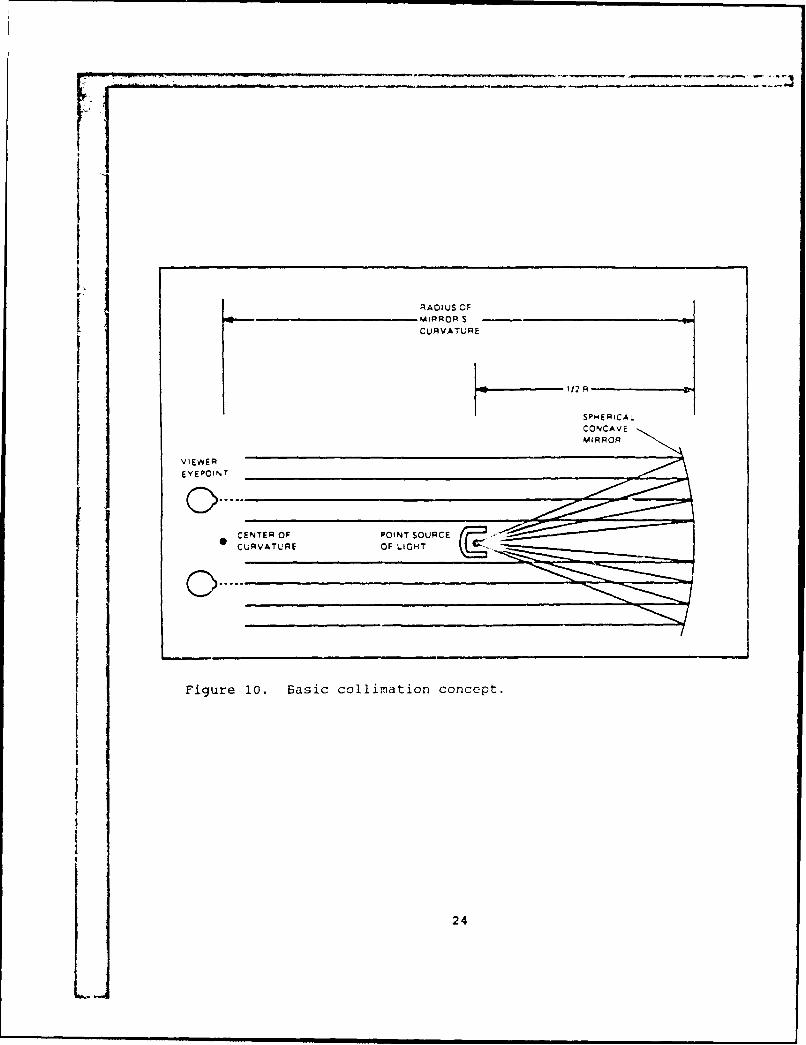
In the visual system of the simulator, a soherical mirror isused to effect the collimation of the light rays. Vhen the pointsource of light is place at a distance equal to one-half theradius of the mirror, rays will enter the mirror and reflect inparallel. 7fherefore, when the viewer looks at the reflectedimage, it has the illusion of being quite far away.
There are three main components of the collimating optics inthis simulator: The CRT, the spherical concave mirror, and abeam splitter. The beam splitter is necessary to eilsure the CRTis out of the line of sight of the pilot. The beam splitter ispartially reflective and allows only 50 percent of the light topas-; through, the rest is reflected to the mirror. Afterreflecting off the mirror, the light rays exit through the beamsplitter, again lose intensity, ana are viewed by the pilct. Asa result, the CRT is driven to near its maximum brightnesscapabilities to compensate for the resulting 82 percert loss oflight.
As shown in Figure 10, at any given point on the CRT, thedistance from the CRT to the bean splitter to the mirror is one-half the mirror's radius. At the design eyepoint, the rays oflight are virtually parallel.
The simulator can operate in three categories: Training,autoflight, and demonstration. In the training mode, the flightis under the control of the instructor-operator who can usenumerous capabilities of the siiuliator to effect the trainingrequired. These capabilities include automatic performancerecording, automatic demonstrations, numerous malfunctions, aswell as other automatic or semiautomatic instructor aids.
In the autoflight mode, a previously reco-rded demonstrationis played back for the trainee. During this re-creation, t1-simulator flies through an established mission. All motion andaural cues as well as instrument indications, and visual scenesare re-created.
In the demonstration mode, the simulator is used t) set up orto edit a demonstration. This includes recording and storing th?particular flight in memory, adding commentary, and synchronizirig3the two in order to effect the demonstration. Fifteen 10-minutedemos can be programmed. During this playback of the demonstra-tion, the primary flight controls are positioned and driven bythe computer.
23
RADIUS OFN4IPROR S-CURVATURE
112 R
SPHERICAL
VIEWER
EVEPOINT
CURVATURE O I a
Figure 10. Basic collimation concept.
24

Met >od
This field study was designed to assess incidence of simula-tor sickness in visually coupled Army flight simulators. Thesurvey measures were chosen to be comparable to those utilized inNavy and Coast Guard surveys. This way, data obtained wouldcomplement and expand the Navy's database of 10 simulators(Kennedy et al., 1987b, Van Hoy et al., 1987), the Coast Guarddata (Ungs, 1987) and previous Army research conducted in theApache Combat Mission Simulator (Gower et al., 1987). As employ-ed in previous surveys, this study consisted of an onsite surveyof pilots and IOs using a motion history questionnaire (MBQ), amotion sickness questionnaire (MSQ), and a postural equilibriumtest (PET) (Appendix A).
Aviators
The 87 Army aviators surveyed ranged from 21 to 48 years
(mean 30.3, SD 6.67). Their ranks ranged from warrant officer I(WOl) to chief warrant officer 4 (CW4) and first lieutenant (ILT)
to lieutenant colonel (LTC). Flight experience was in the range
150 to 8400 flight hours (mean 1583.48).
Measures
The MHQ, originally developed by Kennedy and Graybiel (1965),
is a self-report form designed to evaluate the subject's past
experience with different modes of motion and the subject's
reported history of susceptibility to motion sickness. The MHQwas administered once and was scored according t- proceduresdescribed in Lenel et al. (1987).
The MSQ is designed to assess the symptomatology experienced
as a result of training in the simulator. The MSQ is divided
into four sections. The first section obtains preflight back-ground information to place subjects in the proper category
accordinq to flight position, duties, total flight time in the
aircraft and in the sirulatoc, and history of recent tlight time
in both the aircraft and the simulator.
The second section is the preflight physiological status
section. This section is administered at the simulator site, and
gathers benchmark data as to the subject's recent exposure to
prescription redicaticn;, illness-, u-se of alcohol and/or tobacco
products, and amoijnt of sleep the orevious night.
The third soction ii t ho- si-ul itor si ckn,;,i q ,,:;t i Onn,, i rP(SSQ) (Lane and Kenn-dy, 11i,8). The Sl;Q is a st1-report fo:-m
25

consisting of 23 symptoms that are rated by the participant aseither being present or absent or in terms of degree of severityon a 4-point Likert-type scale. A diagnostic scoring techniqueis applied to the checklist resulting in scores on three sub-scales (nausea, visuomotor, and disorientation) in addition to atotal severity score. Scores on the nmjuo' (N) subscale arebased on the report of symptoms which relate to gastrointestina!distress such as nausea, stomach awareness, salivation, andburping. Scores on the visuomotor (V) subscale reflect thereport of eyestrain-related symptoms such as eyestrain, diffi-culty focusing, blurred vision, and headache, while those on thedisorientation (D) subscale are related to vestibular distur-bances such as dizziness and vertigo. Scores on the totalseverity (TS) scale are an indication of overall discomfort. Forall scales, a score of 100 indicates absence of sickness. Theaverage scores for all simulators ir the NTSC data Lase are107.7, 110.6, 106.4, and 109.8 on the N, Y, D, and TS scales,respectively. The SSQ is administered prior to the flight andthen immediately after the simulator flight, and provides dat3regarding any increase or decrease in severity of the syrrzcrsthat the subject is experiencing. If the subject was cxFerienc-ing an increase in any ot the symptoms, an attempt was made toconduct a structured interview with him in order to provide some
information regarding recovery from the experienced symptoms. Anew question added to the postflilht SSQ asked the pilots aboutthe symptoms experienced in the simulator and whether or not theywere the same as or worse than the same symptcms experienced inthe aircraft conducting the same maneuvers.
The fourth section is the postflight information sectionwhich provides data on the flight conditions the pilot experi-enced while in the simula,'nr and information concerning thestatus of the various systems within the simulator.
Postural equilibrium tust!; (Thomley, Kennedy, and Bittner,1986) were administered concurrently with the *MHQ and M.SQ. Thesetests consist of three r5ubtests, ,ach designed to n,esuL'e anaspect of postural equilibrium, as follows:
a. Walk-on-floor-with-eywt;-clo;od (WC 'iC) . The subject isinstructed to walk 12 he el-to-to'2 st,. with hi:; eyes; closed anAarms folded across hi:i chest. The sub j,:t is given a score(0-12) basea on the number of step-s ho is, ale to complotewithout sidestepping or fallino. The -ubjpct .; Qt,:;teA iivetimes, both pre- and posttlight. i;ibjct; "r. ;cor,.d on thoaverage number of 0-tep:. tke, usin, th" i-,st thr',' of th," fvetests.
b. Stand ing-on-pr,,f,;rr-,, ]- 1, , i- t h-.i y cs;:' (;~ lV ) T ,
subject designate; hi:- pr ,r Iej (tte l, . 1" 1 u.e tokick a football) and thi - is -innc t. t ti ; th. cr'. in sub) ',t
26

then is asked to stand on his preferred leg for 30 seconds withhis eyes closed and arms folded across his chest. Tha experi-menter records the number of seconds the subject is able to standwithout losing balance or tilting to greater than a 5 degree listfrom the vertical. The subject is scored on the number ofseconds he is able to stand. The test is administereci five timeswith the best three of the five being used for analysis.
C. Standing-on-nonpreferred-leg-with-eyes-closed (SONLEC).The SONLEC is administered and scored in the same manner as theSOPLEC. The SONLEC will use the opposite lea from the SOPLEC andis administered five times. The subject's score is the averagenumber of seconds he is able to stand, using the best three ofthe five tests for the analysis.
Procedure
In order to gather the most comprehensive data in the leastintrusive manner, the surveys were administered to ali aviatorswho presented themselves at the simulator site for flightperiods. No attempt was made to randomize the population, butrather to study the problem in the opera Lional setting in whichit is found ind using flight scenarios normally found duringtraining.
The site used wa Port Rucker, Alabama. A target sample sizeof 100 was the object ie, but due to time constrai,.ts and thenuances of operational usage of the simulator, only 95 observa-tions were obtained from 87 subjects. They performed the normalprogram ot instruction a- prescribed in the UH-60 aircraftqualification course, one of several operations orders (OPORD)designed to maintain proficiency, or other aircrew trainingmanual (ATM) tasks nectessary to maintain their proficiency. Theinvestigator did not perform any intervention or exercise anycontrol over the f] tihts in the conduct of this survey. Allaviators schedulei for 1li7ht were surveyed. Each was guaranteedanonyrnity and each wa- permitted nonputicipation. Data cbtainedfrom the questioin i re.s inl th(- PET were entered into ? genericdata)Lase using the proram7s in use at the NTSC, and data reduc-tior and anwlys(e ',re portormed a!; in previous studics. Thedati in this report no-, are incorporated into the Navy's simula-tor sickness databi:, , ,hich al,--o includes Coast Guard data inorder to dotemit:o cc:>-c.itl ity ot Jymptams , simulator usageand design (Gc'er 1t )I., 1037).
27

Results
Symptomatology
Table 2 shows the number of pilots reporting key postflightsymptomatology. To counter the possible inflationary effects ofpreflight symptomatology reported on postflight symptomatology,percentages for each particular symptom are based only on thepilots who did not report the symptom prior to training. Thisprocedure is likely to underestimate the severity of the problemin that pilots who reported a symptom prior to the flight thatwas worse after the flight are not included. Symptoms have beercategorized into those traditionally associated with notionsickness versus those which are associated with asthenopia(eyestrain).
Eyestrain was the most commonly reported asthenopic sympt:-followed by headache. Difficulty focusing and concentrating alr;cwere reported by a substantial number of pilots. An eyestraincomponent is present to some degree in other forms of motionsickness (Lane and Kennedy, 1988), but is a prominent facet ofsimulator sickness implicating visual and visual-vestibularinteractions as causal mechanisms. Improper cclibration ofvirtual image displays may lead to excessive accommodation andconvergence demands (i.e., beyond optical infinity), unequalaccommodative demands between the two cyes, and conflicts betweenaccommodation and vergence systems (Ebenholtz, 1988), all ofwhich may produce asthenopia. It should be noted that symptomsassociated with asthenopia per se include vertigo, indigestion,nausea and vomiting (Ebenholtz, 1988) and thus may be similar tomotion sickness in terms of cause (Morrissey and Bittner, 1986).
Fdtigue and sweating were the most commonly reported sy-iptomsassociated with motion sickness, followed by reports of nauseaand stomach awareness. The relative prominence of a:,thenopic andmotion sickness symptomatology is consistent with previoussurveys of simulator sickness (Gowev: et al., 1937; Kennedy etal., 1987b).
In Table 3, the information in Table 2 has 1,, ,resentdalong with comparable data available for other hell -pter sisul, -
tors. Incidence of eyestrain in the UH-60 simulator tpproach--:;that found in the 2F64C (SH-3H) simulator, the Naivy''s simulatorassociated with the highest incidence of simulator sickness.Moreover, incidenca of difficulty focusin(-, headich,, and nausei,in the Ull-60 siisulator is the seccnd highest in the s :7qpl, whilincidence of stomach awareness is the highest in tho -amplt.Therefore, it is clear that sfeverity of simulaitor ;icnes;experienced by pilots training in th, UH-6O i:s ',1Il Ab-)VO th.,average for helicopter simulators.
28
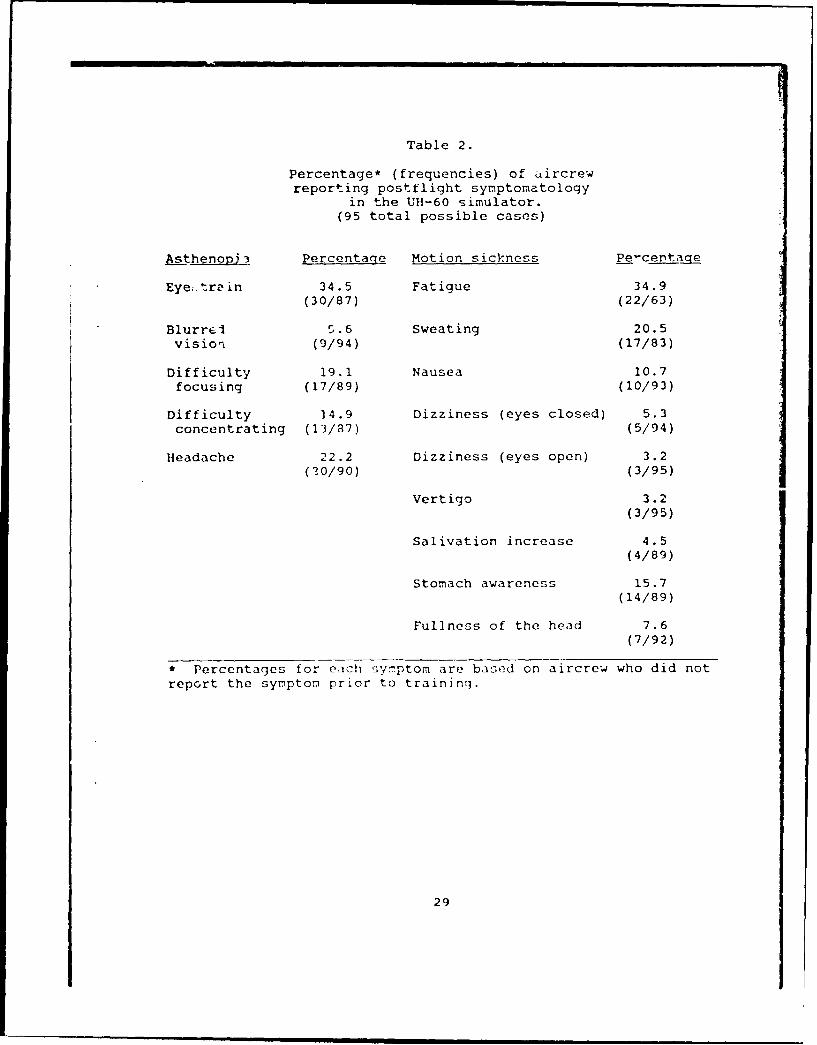
Table 2.
Percentage* (frequencies) of aircrewreporting postflight symptomatoloqy
in the UH-60 simulator.(95 total possible cases)
Asthenov53 Percentage Motion sickness Pe-centaqe
Eye;.tr in 34.5 Fatigue 34.9(30/87) (22/63)
Blurrel S.6 Sweating 20.5vision (9/94) (17/83)
Difficulty 19.1 Nausea 10.7focusing (17/89) (10/93)
Difficulty 14.9 Dizziness (eyes closed) 5.3concentrating (13/87) (5/94)
Headache 22.2 Dizziness (eyes open) 3.2(10/90) (3/95)
Vertigo 3.2(3/95)
Salivation increase 4.5(4/89)
Stomach awareness 15.7(14/89)
Fullness of the head 7.6(7/92)
* Percentages for each symptom are based on aircrew who did not
report the symptom prior to training.
29
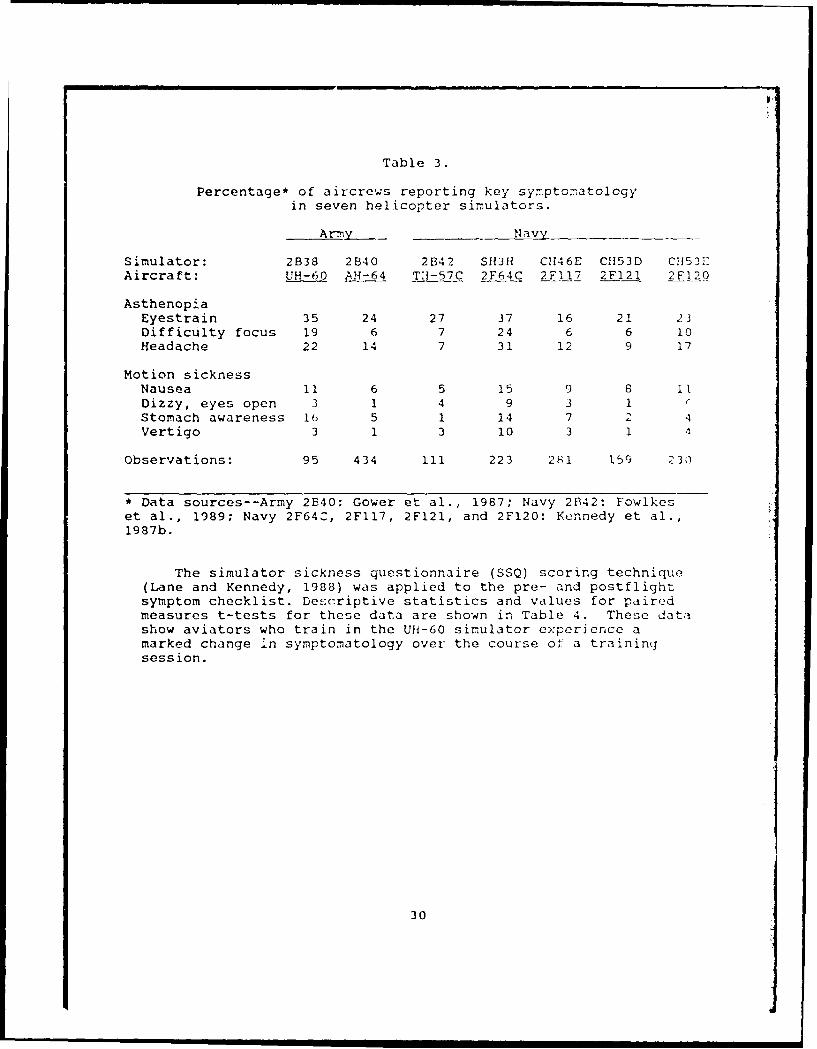
Table 3.
Percentage* of aircrews reporting key symptomatologyin seven helicopter simulators.
Army - N1 av
Simulator: 2B38 2B40 2B42 SH3H CH46E C1153D CH53EAircraft: UH-60 AH-64 Ti-57C 2F64C 2FI17 2F121 2FI20
AsthenopiaEyestrain 35 24 27 37 16 21 23Difficulty focus 19 6 7 24 6 6 10Headache 22 14 7 31 12 9 17
Motion sicknessNausea 11 6 5 15 9 8 11Dizzy, eyes open 3 1 4 9 3 1Stomach awareness 16 5 1 14 7 2 4Vertigo 3 1 3 10 3 1
Observations: 95 434 ill 223 281 159 230
* Data sources--Army 2B40: Gower et al., 1987; Navy 2B42: Fowlkeset al., 1989; Navy 2F64C, 2FI17, 2F121, and 2F120: Kennedy et al.,1987b.
The simulator sickness questionnaire (SSQ) scoring technique(Lane and Kennedy, 1988) was applied to the pre- and postflightsymptom checklist. Descriptive statistics and values for pairedmeasures t-tests for these data are shown in Table 4. These datashow aviators who train in the UH-60 simulator experience amarked change 'n symptomatology over the course of a trainingsession.
30

Table 4.
Pre- and post SSQ means (standard deviations) andpaired t-test values (95 observations).
Difference$SO scale Pre Post Mean t R
Nausea 105.0 113.0 7.93 4.20 .000(8.7) (18.0)
Visuomotor 106.1 117.1 11.01 6.77 .000(iO.i) k17.1)
Disorientation 101.9 109.7 7.77 4.75 .000(6.3) ,17.1)
Total severity 105.5 116.1 10.63 6.44 .000(8.7) (17.3)
Figures 11 through 14 show the severity of postflight SSQscores along with data available for other flight simulators ](both fixed- and rotary-wing). Following Lane and Kennedy's(1988) suggestion for examining postflight data, only pilots whoreported they were in their usual state of fitness were includcin the calculation of postflight SSQ scores presented in Fig-'c;11 through 14. It can be seen tnat the severity of postflic-1symptomatology on each of the SSQ scales for the UH-60 simul-toris the second highest in the sample, substantiating the dat-! forindividual symptoms shcwn in Tables 2 and 3. Lane and Ker.iudy(1988) suggest if means fall within the range of the upper threeto four simulators, closer examination of the simulator iswarranted. Simulator sickness in the UH-60 clearly -=.ts thiscriterion on each subscale and on the total severity ccale,
implicating perhaps both the visual and motion base systems incontributing to symptomatology.
31

I120-
i1s- r Navy
- Army
114 [1., 112-
W 110-
S106-c.e ]j0j]102-
100 , c
Simulator Designation/Aircraft
Figure 11. SSQ visu,,otor subscale.
116-
CD 114- E Navy
-ArmyU) 112-
110-
a) 108-U)0 106-
04
U) 102 ii!100 .... ...
Simulator Designation/Aircraft.
Figure 12. SSQ nausea subscale.
32

112-F
Navy
o 110 ArmyUI
; 108-
> 106-104-
Q)
~'104-CO
10 1 00
Simulator Designation/Aircraft
Figure 13. SSQ disorientation subscale.
120-
118- [3 Navy
[-] Army116-1
U)
112-
10
106-
Simulator Designation/ircraft
Figure 14. SSQ total severity score.
33
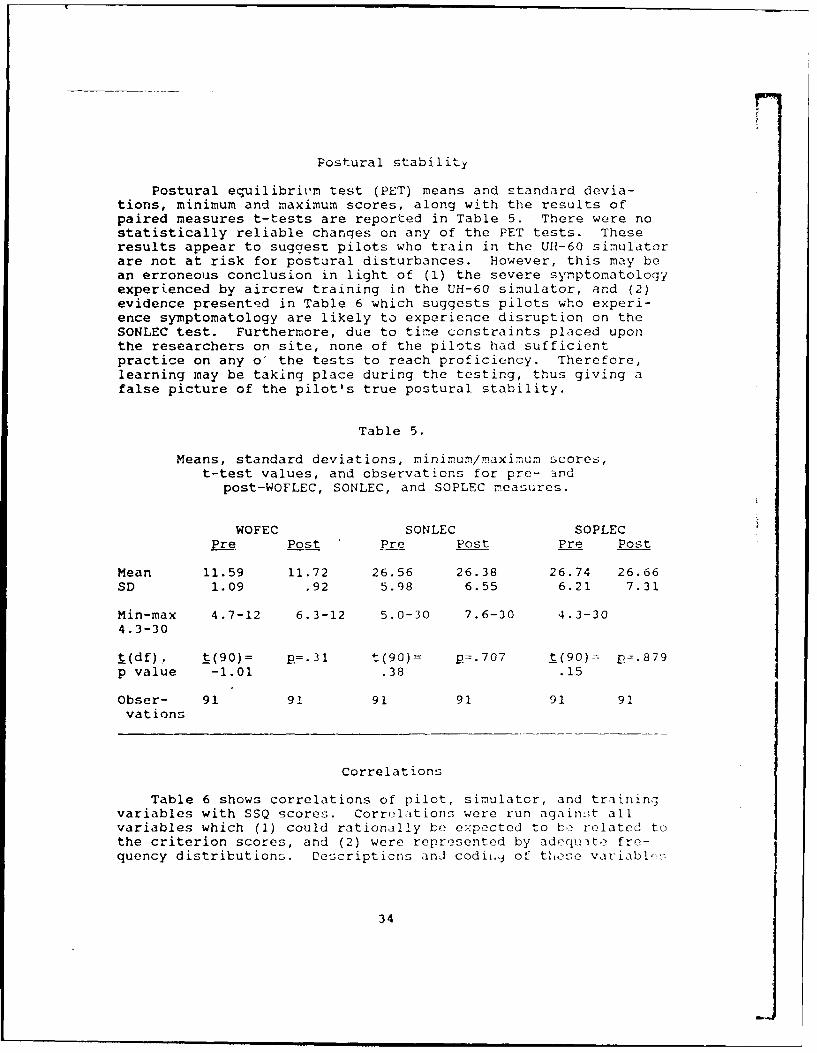
Postural stability
Postural equilibrit'm test (PET) means and standard devia-tions, minimum and maximum scores, along with the results ofpaired measures t-tests are reported in Table 5. There were nostatistically reliable chanqes on any of the PET tests. Theseresults appear to suggest pilots who train in the UH-60 simulatorare not at risk for postural disturbances. However, this may bean erroneous conclusion in light of (l) the severe symptomatologyexperienced by aircrew training in the UH-60 simulator, and (2)evidence presente d in Table 6 which suggests pilots who experi-ence symptomatology are likely to experience disruption on theSONLEC test. Furthermore, due to time constraints placed uponthe researchers on site, none of the pilots had sufficientpractice on any o' the tests to reach proficiency. Therefore,learning may be taking place during the testing, thus giving afalse picture of the pilot's true postural stability.
Table 5.
Means, standard deviations, minimum/maximum scores,t-test values, and observations for pre- and
post-WOFLEC, SONLEC, and SOPLEC measures.
WOFEC SONLEC SOPLECPre Post Pre Post Pre Post
Mean 11.59 11.72 26.56 26.38 26.74 26.66SD 1.09 .92 5.98 6.55 6.21 7.31
Min-max 4.7-12 6.3-12 5.0-30 7.6-30 4.3-304.3-30
t(df) , t(90) = p=.31 t(90) = p=.707 t(90) - p=.879p value -1.01 .38 .15
Obser- 91 91 91 91 91 91vations
Correlations
Table 6 shows correlations of pilot, simulator, and trainingvariables with SSQ scores. Correlations were run again;t allvariables which (1) could rationally bf expected to bo related tothe criterion scores, and (2) were represented by adecjuite fre-quency distributions. Descripticns and codii.,j of thtese variabl-!-.
34

appear as Appendix A. Only correlations thdt r-iched the .05level of statistical significance were presented in the table.
Table 6.
Intercorrelations among variables.(95 total possible observations)
SSQ scores
Pilot variables N V D TS
Rotary-wing hours .23 .24Recent flight hours .24Days since lastsimulator flight .29
Sleep -. 21 -. 18 -.25 -. 24Enough sleep .31 .36 .25 .37MHQ .33 .28 .24 .34Simulator sickness .23 .19 .20 .24SONLEC .26 .20 .21
Simulator variables
Seat L , ker on/off -. 24 -.28 -. 19 -. 29Collective .19Pitch .27Roll .30 .21 .22Torque .36 .22Percent NOE -. 19Percent upper air .21Night .25Lnandings attempted .21Visual traits -. 27Motion disruptions -. 17
Training variabios
Difteert from aircraft .33 .40 .38 .43Discomfort hamper training .43 .43 .44
Pilot variables
Greater total and recent tlight hours were a: :;ociate withhigher S2Q scores, a finding reported in prtviou; !mrvoy:;(McGuinness, Uouwmin, and Forbes, 11),1) th.It sug,;,-.t:< phlot, withmore tlight experience are at more risk for simulaitor sickness.The greater number of days since the last flight in the 1}1-(,O
35

simulator, the more severe the symPtom itology exporicncsd. This Ifinding would be expected; that is, if an Lircrew ar- adapting tothe provocative aspects of the sinmulation, then :.any days bctweensimulatioii flights would tend tD disrupt the learning prces.Inadequate sleep wa3 associated wirh higher symptomatoloayscores, in keeping with the view that pilots whu are not in theirusual state of fitness may be more susceptible to simulatorsickness. Sixteen percent of the sample rated their previousnight's sleep as "not enough." Pilots' ratings of wiether theygot enough sleep wac related to symptomarology, suggesting thismay be an easily obtained and useful prodctor variable. Twoother predictor variables also .ere identified: MH scores andwhether simulator sickness has occurred in the past were bothpredictive of SSQ scores.
Finally, SONLEC 3cores positively v'ere related to simulatorsickness severity suggesting that aviato rs who experier,e theworst symptomatology ar" mcz- dt risk for postural disturbances.
Simulator variables
Correlations between "seat shker" and SSQ scores suggeststhe seat shaker may contribute to symptomatolcgy. In postfiightinterviews, aircrews noted symptomatology was more severe withthe seat shaker on. Some referred to the seat shaker as a"vibrator that rattled their teeth."
Variables related to aircraft control ("collective, pitch,roll, and torque") suggest the wocse the aircrew rateJ thecontrols, the more severe the symptomatology. lmplicated fromthis finding are throughput delays ann visual-motion lags in thesimulator as possibly contributin, tc symptomatology.
Interestingly, the greater the percentage of NOE flight, thelower the symptomatology, while the opposite was true for per-centage of upper air worh. On ether scenario content vari bies,training under the night flying condition was associated with in-creased symptomatology, probably because it as associated withNVG training. In addition, gre ter number of landings wasassociated with increased severity of sickness, which may be dueto the increase in nnar ground interaction which is thought to benauseogenic (Kennedy et al., 1987a) . Finally, noed visualtraits that need correcting3 ind noted disruptions in the notionsystem were associated with more severe symptomatolcgy.
There was an inad1:1te distribution of the- "motion s'temon/of f" variable to ca Iculate a cor-re at ion (o nly one f1 ight .asconducted with the motion system o:t) . {ovever, it wa ! th,general consensus 1mng pilo, i instr0"tor cp-ratol- that
36

flying the simulator with the 1otion system off was far moreprovocative.
Training variables
It can be seen that pilots who experienced greater sy:ptc-a-tology were more likely to rate their synptoms as being wozsethan those they had experienced in the actual aircraft. Thisevidence simulator sickness symptomatology is more severe thansymptomatology experienced in the actual aircraft.
Also, it can be seen that greater symptomatology is associ-ated with a less favorable rating on whether simulator-inducoddiscomfort disrupts training. A fuller appreciation of thisrelationship can .)e seen in Table 7 which shows the frequencieisfor this variable. The majority of pilots felt sinulator-inducicdiscomfort does not hamper training. However, as the correlationindicates, those who experienced symptomatolcgy tended to give aless favorable rating.
Table 7.
Frequencies for variable
"Discomfort hampers training."
Simulator-induced discomfort hampers training
Response f Percent
Strongly disagree 57 66.3Tend to disagree 15 17,4Neutral 13 15.1Tend to agree 1 1.2Strongly agree 0 0.0
Observations 86
37
L
Symptoratology by mission and seat
Mission
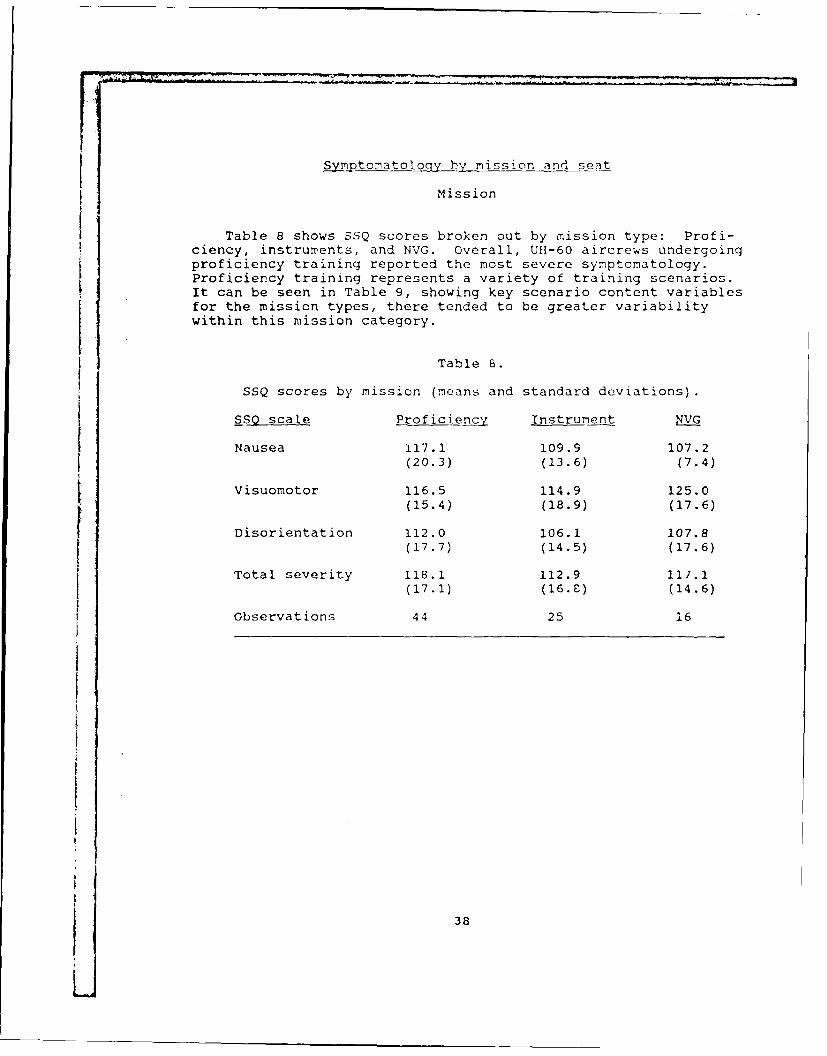
Table 8 shows SSQ scores broken out by mission type: Profi-ciency, instruments, and NVG. Overall, UH-60 aircrews undergoingproficiency training reported the most severe symptomatology.Proficiency training represents a variety of training scenarios.It can be seen in Table 9, showing key scenario content variablesfor the mission types, there tended to be greater variabilitywithin this mission category.
Table S.
SSQ scores by mission (means and standard deviations).
SS0 scale Proficiency Instrument NVG
Nausea 117.1 109.9 107.2
(20.3) (13.6) (7.4)
Visuomotor 116.5 114.9 125.0(15.4) (18.9) (17.6)
Disorientation 112.0 106.1 107.8
(17.7) (14.5) (17.6)
Total severity 118.1 112.9 117.1(17.1) (16.C) (14.6)
Observations 44 25 16
38
Li

Table 9.
Scenario content data (means and standard deviations)for different missions flown in the UH-60 simulator.
Mission
Proficiercy Instrument 1VG
Percent NOE 2.5 0.6 1.6(7.4) (3.1) (5.1)
Percent upper air 31.5 3.4 24.9(34.2) (7.0) (27.6)
Landings attempted 3.5 4.5 4.4(2.6) (6.9) (4.5)
Observations 44 25 16
NVG training resulted in extremely high scores on the SSQvisuomotor subscale. Comments from the aviators revealed many ofthem felt marked disdain for training with NVGs in the UH-60simulator. In addition, 9 of the 16 aviators who flew N VGmissions rated their symptoms as worse than those they experi-enced when using NVGs in the actual aircraft. Use of NVGs p!er -emay result in eyestrain, and, when coupled with use in a simula-tor that originally was not designed for NVG training, can beexpected to cause severe asthenopic symptoms.
Seat
SSQ scores are broken out by seat in Table 10. Comparisonsof severity of simulator sickness for pilots, copilot , and foraircrew training in both seats show that aircrew training in thecopilot's seat and in both seats are at most risk tor sirulatorsickness. A comparison of missions flown for the seat categories(Table 11) shows although they are comparable in terms of nuMberof NVG missions flown, there were more proficiency mir:sicn:; tlownby pilots in the copilot's and in both seats. In addition, otherkey scenario variables (from Table 6) could contribute to tWhdifference; aircrew training in the copilot and in both skitspent, on average, a greatrr percntage of the t ime in upr',r iirwork, shown in Tible 6 to be provocative.
39

Table 10.
SSQ scores by seat (means and standard deviations).
Seac
SSO scale CP Pilot CP/P I0
Nausea 115.9 107.2 114.6 113.9(17.0) (13.9) (17.5) (26.3)
Visuomotor 119.6 113.9 117.6 116.9(16.0) (17.1) (18.0) (18.1)
Disorientation 111.6 108.1 107.8 113.9(20.0) (16.9) (15.0) (18.0)
Total severity 119.0 111.8 116.5 117.6(17.5) (17.5) (15.7) (21.1)
Observations 24 24 34 13
There were 13 observations of instructor operators. Thesedata suggest, under the conditions of the simulation flightsflown by these individuals, instructor operators are at risk forsimulator sickness. In addition, experimenter interviews withinstructor op2rators revealed that symptomatology experiencedafter several periods in the simulator may be particularlysevere.
40

Table 11.
Mission and scenario content data for copilot and pilots
SeatCP £ilot
Percent aircrew flyingkey missions:
Proficiency 54.2 37.5 58.8
Instruments 20.8 25.0 20.6
NVG 20.8 20.8 17.6
Means (standard deviations) forkey scenario variables:
Percent NOE 1.25 5.00 3.53(5.16) (12.3) (15.1)
Percent upper air 23.96 10.70 30.76(30.9) (17.7) (35.1)
Landings attempted 3.63 4.42 3.88(3.4) (5.6) (3.0)
Observaticns 24 24 34
41

Discussion
The principal goal in this field study was to assess theincidence of simulator sickness in the UH-60 flight simulator.The results show training in this simulator produces a higherincidence of simulator sickness than the three other Army visual-ly coupled flight simulators, the AH-l, the CH-47, and the AH-64.As in other systems, eyestrain and headache were leading symptomsof asthenopia, while fatigue and sweating were leading symptomsassociated with motion sickness. The high scores on the N, V, D,and TS SSQ scales ranks the UH-60 as one of the two worst simula-tors for simulator sickness studied by the Army and the Navy.
The high scores are cause for concern and raise questionsabout the visual and motion base representation of flight experi-enced by the aviators in the UH-60 flight simulator. The tasksaccomplished in this simulator require close coordination betweenthe pilot and the copilot that should not be degraded because ofthe general discomfort of the aircrew due to simulator effects.The fact that copilots showed higher scores than pilots raisesconcern for the design of the visual representation of inforria-tion from the other aviators viewpoint as is done in the UH-60.Of further concern to us is the relatively high scores on the SSQscales seen for aircrews flying instrument flight which arerelatively benign scenarios. This time spent with no scenecontent should produce lower SSQ scores. If, in fact, theaviators are having problems with the simulator flying underinstrument conditions, then there is cause for concern.
The use of NVGs in the UH-60 simulator is associated withhigher scores on the SSQ, as seen in Table 8. The NVGs in actualflight tend to cause problems due to their added weight, limitedfield-of-view, and degraded visual qualities. Moreover, becausethey restrict the field-of-view, NVGs may cause recalibration ofthe vestibulo-oculir reflex. When combined with the artificialenvi-onment of the ;imulator, it is not surprising to see arelatively higher incidence of visuomotor symptoms.
As stated in the methods section, the researchers did notexercise any control over the flights in the simulator. In theabsence of detailed proqrams of i-struction (POIs) or standard-ized flight scenarios, it is vet difficult to accurately de-scribe provocative flight conditions. Further, the amount ofadaptation during the flight and on subsequent flights is notassessed. Th- ti-.- course of the symptoms experienced also wasnot possible to .> ;s in the study. Therefore, symptomatologymay be undere-,ti- .',_1 for so7e earlier flights and overcstimatcdfor later fllgh'.s;. In _jrcn.cral, tne manner in which the qucstio.n-
4:
naires were scored tends to be conservative. These topics shouldbe studied under controlled conditions.
The method of testing postural stability used in this studywas successful in demonstrating postexposure ataxia in a pr.eviousstudy (Gower et dl., 1987). However, due to the operationalconsiderations of the current study, none of the aviatorsreceived sufficient practice to reach a level of proficiency onthe tests prior to simulator exposure. In fact, time was verylimited during this study to the point that some had little or nopractice whatsoever. It is possible the lack of significantdecrements on any of the three te-:ts is due in part to themasking of simulator effects by practice effects. Experimenterrecords indicated that some aircrews felt unsteady after theirsimulator exposure but, nevertheless, performed well on thetests. Further controlled studies with more sensitive standing-and walking-based tests or stabilimeter men:;urement should beconsidered.
Recent anecdotal information received at USAARL from fieldedUH-60 flight simulator sites has indicated aviators flyingregular missions in the Ull-60 flight simulator have experienceddelayed effects beyond the simvlator flight itself. Some werereported to have occurred over 24 hours postexposure. Thisreport was not able to assess the time course of the postflightsymptomatology; however, the relative degree of severity andreports of other delayed symptoms is cause for a further look athe issue.
Pecom-endations
In view of the results of this study and other studiesconducted in A--, ...;ijilly-coupled flight simulators, it is ourrecommendation thiat:
a. Continued cattion be exercised with those aviators flyingin this simulator. Th % also should include adherence to the 6-hour waiting period Ld-cated in USAARL 88-1.
b. Commanders shouli, in conjunction with their flightsurgeons, implement monitoring of their aviators to assess thosewho have demonstrated pLoiems with the simulator -environ-ent.Those who do experience p,)blems should restrict flight in theactual aircraft for at lcz.:t one night's rest to allow them todissipate. Strict adheren, " to the guidelines published inKennedy et al. (1987a) shLi.1 be followed for iviators experienc-ing problems until thoy aJipt to the simulator.
43
c. Calibration and alignment of the visuals be accomplishedregularly and as a part of routine maintenance. Considerationshould be given to having the visual system of this and otherArmy simulators checked for excessive flicker, accommodation andveraence demands, unequal accommodative demands, and accomr-da-tion/vergence conflict.
d. Further controlled studies be conducted to ascertain therole of aviator susceptibility and its part in the phenomenon ofsimulator sickness. These studies also may involve the use ofpsychophysiological measurements in order to objectively deter-mine the time course of the aviator's simulator sickness ex-perience. One question still not answered is the actual timecnurqp rf the symptoms experienced bv the aviators in the simula-tor and the recurrenue oL. delayea effects. Anecdotal datacontinues to be received indicating there is a part of theaviation population that experiences delayed problems beyond thesimulator exposure and for periods that exceed 6 to 9 hours forapproximately 8 percent of the population and l-to-2 days for aneven smaller population.
e. Studies be conducted to determine which scenarios arelinked with simulator sickness and methods to prepare aviators todeal with those scenarios. A correlation of simulator sicknesswith actual flight experience under similar conditions should bedetermined in side-by-side studies conducted in the simulator andin the aircraft.
f. Studies be conducted to ascertain the period of time thatan aviator should wait postflight before piloting an actualaircraft or even driving a car.
g. Ccmmanders and supervisors should review the POIs beingflown in their particular simulator device against the requiredmissions that should be flown in the device. If aviators areavoiding the simulator for reasons of simulator sickness, then alarger problem exists than is indicated in this report. The uc;eof a visually-coupled flight simulator for instrument trainingshould be a caune for concern Lf it reaches proportions above ticrequirements.
44

rt
Allgood, G. 0., Kennedy, R. S., Van Hoy, B. H., Lilienthal, M.G., and Hooper, J. H. 1987. The effects of vory-1ow fre-auencv vil-r "tiors on sirulator sirkn, ;. Papar pr- ..ntce u
O +-h Aanua I scientific 1"et ma o t' -c edicalAssociation, !as Vegas, "c ,a.
Balt'ley, D. R., Kennedy, R. S., Allgood, G. 0., Li'lienthal, M.G., and Gower, D. W. 1987. Fa~ ;acks and other delayedeffects of simulator sickness: Tncaenco and _ioi ic-tions.Unpublished manuscript.
Casali, J. G. 1986. Vehicular sirulatle'.-induc,-d sickneSs:Volume I: An overview (NTSC-IR-86-010). Orlar.do, FL: NavalTraining Systems Center. NTIS No. AD A173-9C4.
Colehour, J. K., and Graybiel, A. 1966. Bioche-ical chnnceoccurring with adaptation to accelerative forces durirnrotation. Pensacola, FL: NASA/U.S. Naval Aercspae Insti-tute. Joint Report No. NANI-959.
Crampton, G. H., and Young, F. A. 1953. The differential effectof a rotary visual field on s'sceptibles and nonsusceptibles
to motion sickness. Journal of cornparative and physiolqgicalpsychology. 46"451-453.
Crowley, J. S. 1987. Simulator sicknes;s: A problem for Armyaviation. Aviation, sp)qcpan. environmental medicine.58(4) :355-357.
Department of Defense. 1981. H.unan rn, nrin j ikin criteria1for military sy'tem. oqpip..nt and fncilitie' Washington,D.C. Military Standard 1472C.
Ebenholtz, S. M. 1988. Sueoure of -i -;thennia in Tvyf_1 ihtsimulators. Re,;earch Tri.mnjle Park, NC: U.s. Amy ResearchOffice. TCN 8Y-635.
Fowlkes, J. E., Kennedy, R. S., and Btalt-.lry, ). R. 1989. Si u-lator sickness in the TH-,TC ho1 i(nrnt'r f__ ijhtsinllator.Orlanri- . FL, Essex Corporiticn. Firial Report.
Fregley, A. R., and Graybiel, A. 19(,5. 'sfl of _ '_ct-ffternconditions at !ra upon th,- iiirtura1 _li ihriu _ functioninjof vertibular nor.l i] _ _.? t ihnl.- _ ,¢,'i hI 'i_ nhjrIt .
Pensacola, Fl: Naval Scrhool of Avition "Idicine. ReportNo. NSAM-935.
413
Fregly, A. R., and Kennedy, R. S. 1965. Comparative effects ofprolonged rotation at 10 rpm on postural equilibrium investibular normal and vestibular defective human subjects.A.Lo-pace Medicine. 36:1160-1167.
Gowe,:, D. W., Liliei- il "'' 13.,Y n c y P.'_ F 0cC
J. E., and Baltzley, D. R. 1987. Simulator sickness in theAH-64 Apache combat mission simulator. Fort Rucker, AL:U.S. Army Aeromedical Research Laboratory. USAARL Report No.88-1.
Graybiel A., and Lackner, J. R. 1983. Motion sickness acquisi-tior and retention of adaption effects compared in threemotion environmcntu. :,'iation space, and environmentalmedicine. 54:307-11.
Homick, J. L., and Reschke, M. F. 1977. Postural equilibriumfollowing exposure to w:eightless space flight. Acta oto-laryngologica. 83:455-464.
Kennedy, R. S. 1975. Motion sickneqs questionnaire and fieldindependence scores as predictors of success in Naval avia-tion training. Aviation. space, and environmental medicine.46:1349-1352.
Kennedy, R. S., Berbaum, K. S., and Frank, L. H. 1984. Visualdistortion: The correlation model. (Technical Report No.841595). Proceedings of the SAE Aerospace Congress andExhibition, Long Beach, CA.
Kennedy, R. S., Berbaum, K. S., Lilienthal, M. G., Dunlap, W. P.,Mulligan, W., and cunaro, J. 1987a. Guidelines for allevia-tion of simultito- sickness s [.stonatoloy. Orlando, FL:Naval Training Systems Center. NTSC-TR-87-007.
Kennedy, R. S., an(! -ranik, L. H. 1986. A review of motionsickness withflpecial reference to simulator sickness. Paperpresented at the 65th annual meeting of the TransportationResearch Board, Washington, DC.
Kennedy, R. S., and Graybiel, A. 1965. The dial test: Astandardied o_ edue_-for the exrerimental production ofcanal sickness sy-ptomatoiogv in a rotating environment.Pensacola, FL: ilaval School of Aerospace Medicine. ReportNo. 113, NShM 930.
Kennedy, R. S., Lili,2nthil, M. G., Berbaum, K. S., T3altzley, D.R., and McC'iuley, M. E. 1987b. Simulator iicn n,__in 10I.S. PNavy_ f i _irhl: I -it r . Orlando, FL: Navai TrainingSystems Coer. NTSC-T -3-7- J61.
46

Lane, N. E., and Kennedy, R. S. 1988. A new method forauantifying sickness: Develonment and application of thesimulator skkness Uestionnaire (SSQ). Orlando, FL: EssexCorporation. EOTR 88-7.
Lenel, J. C. Berbaum, K. S., Kennedy, R. S., and Fowlkes, J. E.1987. A motion sickness history questionnaire: Scoring keyczi 3 f:"r v. Crland ,
'" Essex Corpnration.EOTR 87-3.
Link Flight Simulation Corporation. 1988. Operation and main-tenance, organizational and intermediate levels, UH-60 (BlackHawk) flight simulator, visual display. Link Flight Simula-tion Corporation, 15 August 1988. TIM-55-6930-217-23-3.
Link Flight Simulation CorporationL. 1988. Operator's manual forthe UH-60 flight simulator. Link Flight Simulation Corpora-tion, 15 March 1988. TM 55-6930-217-10.
McClure, J. A., and Fregly, A. R. 1972. Forehead sweating d-irin_motion sickness. Pensacola, FL: Naval Aerospace MedicalResearch Laboratory. (NTIS No. AD A743-975). NAMRL-1157.
McGuinness, J. Bouw ,an, J. H., and Forbes, J. M. 1981.Simulator sickness occurrence in the 2E6 air combat maneu-verntsiulator (AMCS). Orlando, FL: Naval Training Equip-ment Center. NAVTRAEQUIPCEN 80-C-0135-4500-I.
Money, K. E. 1970. Motion sickness. Psychological reviews.50(l) :1-39.
Morrissey, S. J., and Bittner, A. C., Jr. 1986. Vestibular,perceptual, and subjective changes associated with extendedVDU use: A motion sickness syndrome? In Karkowski, W.(Ed.), Trends in ergonomics/human factors IIT. New York:North-Holland.
Oman, C. M. 1980. A heuristic mathenatical model for thedynamics of sensory conflict and notion sickness. Cambridge,MA: Man-Vehicle Laboratory, Center for Space Research.Report No. UVT-80-1.
Operator's Manual. 8 January 1987. UH-60A and EH-60Ahelicopter. Headquarters, Department of the Army.TM 55-1570-237-10.
Reason, J. T., and Brand, J. J. 1975. Motion sickne fss. NewYork: Academic Press.
47

Stern, R. M., Koch, K. L., Stewart, W. R., and Lindblad, I. M. 11987. Spectral analysis of tachygastria recorded duringmotion sickness. Gastroenterolcgy. 92:92-97.
Teiv'ira, R. A. and Lackner, J. R. 1979. Optokinetic wlotionsickness: Attenuation of visually-induced apparent self-ro-tation by passive head movenents. Aviation, space, andenvironmental medicine. 50(3):264-266.
Thomley, K. E., Kennedy, R. S., and Bittner, A. C., Jr. 1986.Development of postural equilibrium tests for examiningenvironmental effects. Perceptual and motor skills. 63:555-564.
Ungs, T. J. 1987. Simulator sickness: Evidence of long-termeffects. Paper presented at the annual Human Factors meet-ing, New York.
Van Hoy, B. W., Allgood, G. 0., Lilienthal, M. G., Kennedy,R. S., and Hooper, J. M. 1987. Inertial and control systemsmeasurements of two motion-based flight simulators for eval-uation of the incidence of simulator sicknos. Pcucediaqsof the IMAGE IV conference. Phoenix, AZ.
48

apedx A.
49

SI.NrULATCR ICKZXESS £U°R.E:"
This is a survey of simulator aftereffects being ronucted for the U S'Army Aerome~ical Research Laboratory, Fort Rucker, Alabama, in cooperati.onwith the Naval Training Systems Center. The purpose of the s.rvev is todetermine the incidence of simulator aftereffects such as nausea or imbalanceoccurring in visually coupled flight simulators (UH-60, ;i-- C {-47)
te appreciate your cooperation in obtaining infurmation about thisproblem. The results of the stud'; will be used to improve the characterstw-sof future simulators. Your respcnses will be held in confid-nce and usedstatistically. Although we ask for your name on this page, no inf:rr..t',nwill be reported by name. This cover page will be removed and all :ala t i4abe identified by the coded serial number above.
Your Name Rank
Date Unit
Instructor (if in Qualification traininp'
iraining Stage Qualification Continuation
Refresher AAP.A.PT (Check Ride).
Mission
All rights reser-red
E:;,x Cororatie-n040 '..'uodcocK ?,oid, : 2, 7
Orlando,FL 32c03(UED BY PE2,IssU:CN;)
Oct 1983 Revision
50

This page intentionally left blank.
51

I
ra :o - -a 0
1. Approximatelv, how many total f : . ,t as pilot a:;o cc-pilot dohave? (in all aircraft, civilian and military time inclusive
a Fixed Wing
b ,Rotary Wing
How nften .ould ".Ou sa; vou get air'sco.
Always Frequently _ Sometimes R areli
3. a. How many tota. flight simulator hours? 'all except SFTS)
b. How many flight hours do you have in this thi- sisjator_
4. How much experience have you had at s2i aboard shipsr, boats'
Much Some __ Very little N__ Nen
5. How often would yn,- say iou get seaaio>:
Always __ Frequently __ Soneti-s R__ rP.rel; Never
Have vou ever been motion s .cni.- r an'y conditiois oter
li>-ed : far? No Yes
If "Yes,' under what ooiti:n __
7. In general, how susceptile to motion sic;:ess - .. -' ,
Extrenely - Ve ry - _ Moderatzl 1%i,,." -
3 , Hae IOU teen na'.eatd : - -. .. "
No _ Yes If "Yos," explain
52
Serial _I -ate
9, Vnen you were nauseated for any r~n (including afcho ,c..did you vomit?
Only with Retch and finallyEasily difficulty vomited with great l f' .
LO. If you vomited while experiencing motion sickness, did
a. Feel better and remain so?b. Feel better temporarily, then vcmit again?
c. Feel no better, but not vomit aain __?
d. Other - s-ecify
11. If you were in an experi.aent where 50% of the subject . .you think your chances of getting sick would be?
Almost Almos tcertainly Probably Probably certainlywould would would rot could not
12. Would you volunteer for an experiment where you knew that(Please answer all three)
a. 50% of the subjects did get motion sick? Yes Nob. 75% of the subjects did get 7otion sick? Yes -- __
c. 5% of the subjects did get motion sick? Yes
13. Most people experience slight dizziness (not a rsult o oo: to5 times a year. The past year you have been ditzzy:
more than this the same as less than nv', . __v
H.ave you ever had an ear illness or inj' r y hich a,- .i,-c :.i !dizziness and/or na,,sa? Yes o
53L__53

Listed below are a -.;:-er of s~-:;=:-.s nic rome : co-e nave re-ported moti.on si.ckness sn-tocns. 7'n c-e space providec. --neckc a, v~curFREFERENCE for each ac:v,.i: (-ha:: is, n.ow m,-ch Vou Ik;.e :0enzaze inthat activity) . and (b) any SYM4PIC.M(S) you mtav have ex 'Fr'-enced at any
C
C: 0
:her~~ Canya
~I> 0
- )
54

16. If you have ever experienced simulator sickness or discC,1fDrt (,,r anyother aftereffect):
a. What simulator was it?
b. What were the symptoms?
c. If they went away and then came back, describe wh .'enz; r'.:,:
their return.
d. How long did they last irediatelv post-flight?
e. How long did they last if they went away and then came Kack?
d. What do you think caused the problem?-.
E:D OF X,.::; H.sT?' , . ,
5
' 55

Serial No. -Date
PPE-FLICHT FAC'KCR--ND NNCy ''
instructions: Please fill this page out BEFORE you go into tne simulator.Fill in the blanks or circle the appropriate item.
I. Start time for your flight: Expected length of flight
2. Seat you will be in for :he simulator flight (Circle onl'; one,
Copilot Gunner (CFG) (,'-I only)
Copilot (CP)
Pilot (P)
Instructor/Cperator (10)
CPG seat for first part of flight, then P seat
P seat for first part of flight, thep CPG seat
3. Type of mission: Proficiency / Instrument / Tactics / Other
4a. Aircraft flight hours last 2 months
4b. How many days has it been since your last flight IN ThE ARz,2RAF-T'
5a. Simulator flights last 3 months Sir.ulator hours last 3 day s
6c. How ma. days has it been since your last flight :N THIS S\'C?
CO TO NE: FALE
6
56
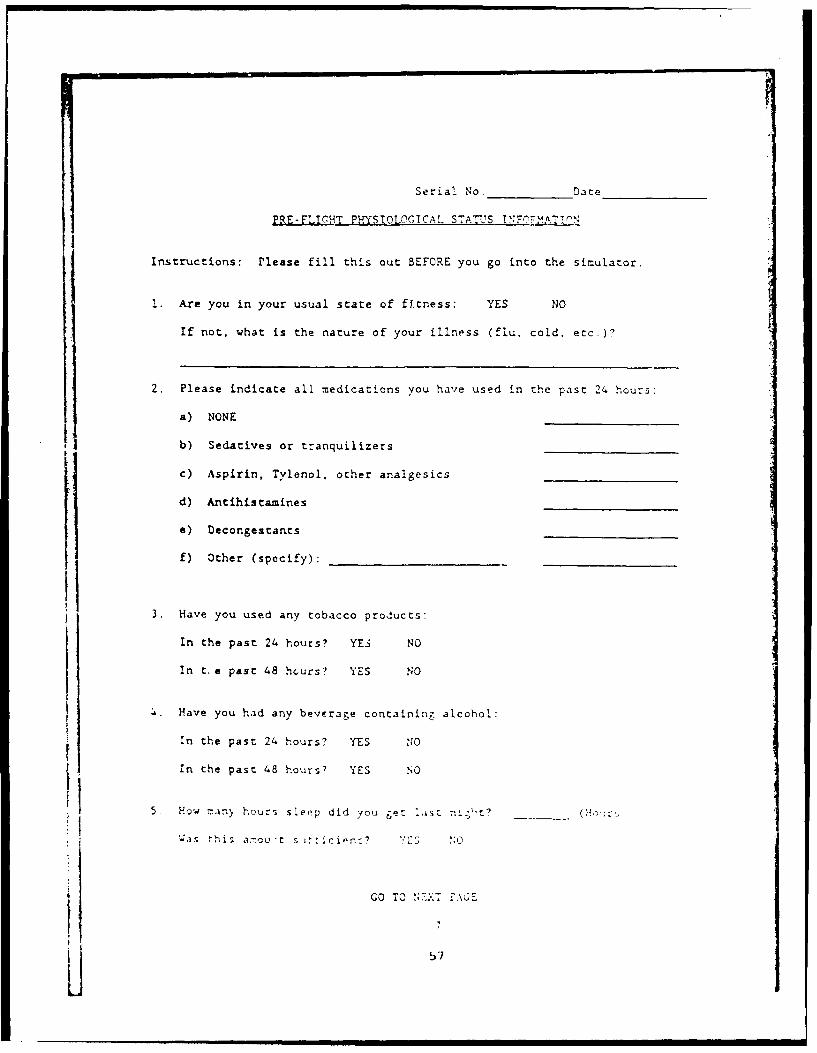
Serial No. Date
PRE-FL!CHT PHYSIOLOGICAL STATUS TNFnMv.T!nN
Instructions: Please fill this out BEFORE you go into the simulator.
Are you in your usual state of ftness: YES NO
If not, what is the nature of your illness (flu, cold, etc.)?
2. Please indicate all medications you have used in the past 24 hours
a) NONE
b) Sedatives or tranquilizers
c) Aspirin, Tylenol. other analgesics
d) Antihistamines
e) Decongestants
f) Other (specify):
3. Have you used any tobacco products:
In the past 24 hours? YE3 NO
In t,e past 48 ho-urs? YES NO
4. Have you had any beverage containinz alcohol:
in the past 24 hours? YES '1O
In the past 48 hours? YES h0
5. How rany hours s Leep did you get ast ni ;,t? ( r-s
-;a t h Is a:7ou t s j': c 0" NO 5 ;
GO TO,
J 57

Serial No. Date
PRE- FLICRTS'TC c*': EKIsT
Instructions: Please fill this out BEFORE you go into the simulator. Circlebelow if the symptoms apply to you right no. (After your
simulator flight you will be asked these quaecions again.)
1. General discomfort None Slight Moderate Severe
2. Fatigue None Slight Moderate Severe
3. Boredom None Slight Moderate Severe
4. Drowsiness None Slight Moderate Severe5. Headache _,one Slight Moderate Severe
6. Eye strain None Slight Moderate Severe7. Difficulty focusing None Slight Moderate Severe8. a. Salivation increased _ _ one Slight Moderate Severe
b. Salivation decreased N o ne Slight Moderate Severe
9. Sweatig None Slight Moderate Severe
10. Nausea None Slight Moderate Severe
11. Difficulty concentrating None Slight Moderate Severe
....... ._________ No Yes13. "Fullness of the Head" No Yes
14. Blurred vision No Yes15. a. Dizziness with eyes open_ _ No Y's
b. Dizziness with eys closed_ No Yes
16. Vertigo_ No Yes
17. *Visual flashbacks No Yes18. Faintness No Yes19. Aware of breathin_ _ No Yes
20. **Stomach awareness No Yes21. Loss of appetite No Yes
22. Increased appetite No Yes
23. Desire to move bowels No Yes24. ConfusionNo Yes25. Burping_ _ o Yes No. of tir.es_-26. Vomiting No Yes No. of times27. Other-
* Visual illusion of -ove=ent or false sensations similar to aircraf
dr,/amics, when not in the simulator or the aircraft.
Stomach awareness is usually used to inicate a feelirg of disceifortwhich is Jusc shacrt of riu e.
SO, . .... tet cir. ct r -. tell you whn c
8
59j

This page intentionally left blank.
59

Seri., No e
?OsT-F.:G}T s':TCM CH.ECMLIST
instructions: Circle below if any symptoms apply to you right now.
1. General discomfort _ None Slight Moderate Severe
2. Fatigue None- Slight Moderate Severe
3. Boredom None Slight Moderate Severe4. Drowsir.ess None Slight Moderate Severe5. Headache None Slight Moderate Severe6. Eye strain _one Slight Moderate Severe
7. Difficulty focusing None Slight Moderate Severe8. a. Salivation increased None Slight Moderate Severe
b. Salivation decreased _None Slight Moderate Severe
9. Sweating None Slight Moderate Severe
10. Nausea None Slight Moderate Severe11. Difficulty concentrating None Slight Moderate Severe12. Mental depression No Yes13. "Fullness of the Head" No Yes14: Blurred vision No Yes15 a. Dizziness with eyes open No Yes
b. Dizziness with eyes closed_ No Yes16. Vertigo No Yes17. *Visual flashbacks No Yes
18. Faintness No Yes19 . 't of breathing No Yes20. **Stomach awareness No Yes21. Loss of appetite No Yes22. Increased appetite No Yes23. Desire to move bowels No Yes
24. Confusion No Yes25. Burping No Yes No. of times26. Vomiting No Yes No. of times27. Other28. Would you describe the symptoms above as SAME AS
WORSE THAN
NO DIFFERENCEfrom flight in the actual aircraft under the same conditions youexperienced in the flight just completed.
* Visual illusion of movement or false sensations similar to aircraft
dynamics, when not in the simulator or the aircraft.
** Stomach awareness is u~.allv used to indicate a feelin.-, of discomfort
which is just short of niu;ea.
CO TO THE NR<T PACE
9
60
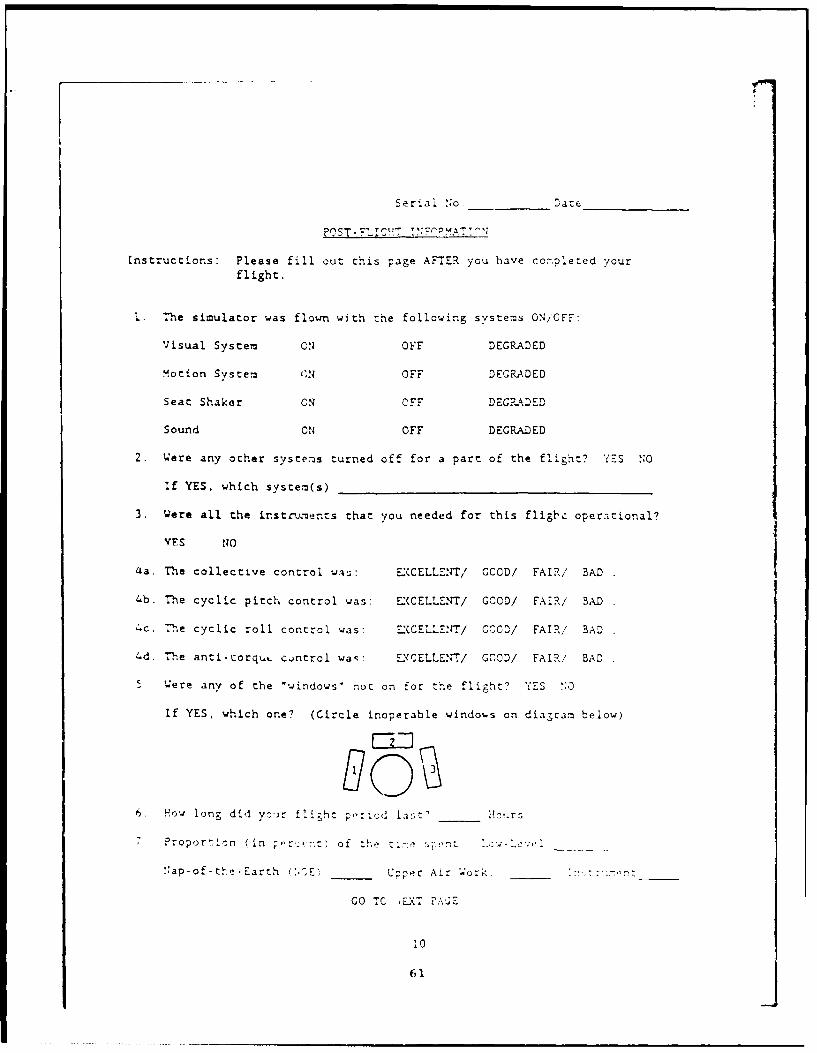
Serial No. _atc_
Instructions: Please fill out this page AFTER you have coMpleted your
flight.
I. The simulator was flown with the following systems ON/OFF:
Visual System ON OFF DEGRADED
Motion System (N OFF DEGRADED
Seat Shaker ON OFF DEGRADED
Sound ON OFF DEGRADED
2. Were any other systems turned off for a part of the flight? YES NO
If YES, which system(s)
3. Were all the instruents that you needed for this fligl," operational?
YFS NO
4a. The collective control was: EXCELLE:rr/ GCOD/ FAIR/ BAD
4b. The cyclic pitch control was: EXCELLENT/ GCOD/ FAIR/ BAD
4c. The cyclic roll control was: ExCELLENT/ CGD/ FAIR/ BAD
4d. The anti-corquL control wa-: EXCELLE./ GOOD/ FAIR/ BAD
5 Were any of the 'windows" not on for the flight? YES :0
If YES, which one? (Circle inoperable windows on diagram below)
6. How long did ;oir fi;hz p,"cd las;t' __tr_
7 Proportion (In of tl-
N:ap-of-the-Earth _____U_ __A___'o_:::, -:.-Up___Cper Air -;orkz: t___ . .
GO TC -E.XT FA.E
61

Serial No. - Date
8. Type of flight conditions: Night / Dusk / Instrument / DAY VFR /
9. Percentage of time looking out of windows
10. Percentage of time operating TSU heads down
11. Number of times the simulator was put on freeze
12. Number of times any scene was replayed _
.! Nu-ber of impacts/ near hits frcm enemy
14. Number of impacts with ground:
15. Number of landings attempted:
16. The time now
17. Did you have to wait long periods while in the simulator for any reason?
YES NO __ If YES, how 1ong?
18. In terms of training effectiveness, this simulatot accomplishes itspurpose of training me to be move proficient at flight skills?
Please circle the number which most closely corresponds to your ffelingsabout the statement above.
5 ---------4........... 3 ---------- --------- IStrongly Tend Neutral Tend Strongly
Agree to agree to agree Disagree
19. If you experienced discomfort of some degree in the simulator (enough t0
mark one or more of the Post-Flight Symptows), did their severity hamcoryour training during the flight? Circle the number which most closely
describes your experience in today's flight
5 .........4-- --------- 3......... 2 .-- ..---Complete ModerateDisruption Disruption Disruption
20. Scene Disturbances:
Describe any disruptive visual system probl.ems that vcru er'.ec
11
62
Serial No. - :)ate
Describe any bothersGme visual traits you would like to see corrected:
Describe any disruptive motion system problems that you observed:
Describe any bothersome motion system traits you would like corrected:
12
63

This page intentionally left blank.
64

Aopend i B.
Variable descriptions
Variable Descripticn Code
Pilot vari,'bles
Rot.,.ry-wing hours Total flight hours in rotary- Number of hourswing aircraft
Recei flight hours Flight hours in last 2 -onths Number of hours
Days since last flight iu.mJer of d3ys sirnce last flight Number si iad;in the aircraft
Sleep Hours sleep previous night .'Usurs sleep
Enough sleep Was the amount of sleep l=Yes, 2=Noprevious night sufficient?
MHQ Motion history questionnaire Range: 0 to 5stscepti.bility score 0 = low
susceptibility
Simulator sick.ness Have you ever experienced l=Yes, O=Nosimulator sickness?
SONLEC/SOPLEC Pre- minus post score
Siiun] ltor variablos
Seat shaker on/off Seat shaker on or off during I=Onflight 2-Of tC ra2-J
Collective control fow was the collective control? l ;c0l.-27t2 -Good3=Fair, -- aJ
Pitcn control How "ao the pitch control? 1-Excel1cnt2 Good,
=Fa*r, :
Poll Co0trol 1o'. was t>., roll "xnt ro1
65

Simulator variables Pescription Coe
Torque Control How was the torque control? l=Excellent2="rhod3=Fair, 4=bad
Percent nap-of-the- Percent of flight spent in Percentageearth flight NCE flight
Percent upper air Percent of flight spent in Percentageupper air work
Night Night flicght concitions !=Yes, OIlo
Lanaings attempted Number of landings attempted Number oflandings
Visual traits Are there bothersome visual l=Yes, 2=Notraits that need correcting?
Motion disruptions Notice any disruptive motion l=Yes, 2=Nosystem problems?
Training variables
Different from Are symptoms experienced the l=Same, 2=Worseaircraft same or worse than those
experienced in the actualaircraft.
Discomfort hampers Discomfort experiencnd I- rpered l:Strcnqlcytraining training disagree
2=Tend todisagree
3=Neutr. i4=Tend to agroe5=Strongly ,3r,c
C
66
L

Initial distribution
Commander CommanderU.S. Army Natick Research U.S. Army Research Institute
and Development Center of Environmental MedicineATTN: Documents Librarian Natick, MA 01760Natick, MA 01760
Naval Submarine Medical U.S. Army Avionics ReseirohResearch Laboratory and Development Activity
Medical Library, Naval Sub Base ATTN: SAVAA-P-TPBox 900 Fort Monmouth, NJ 07703-5401Groton, CT 05340
Commander/Director U.S. Army Research and DevelopmentU.S. Army Combat Surveillance Support Activity
& Tdrget Acquisition Lab Fort Monmouth, NJ 07703ATTN: DELCS-DFort Monmouth, NJ 07703-5304
Commander Chief, Benet Weapons Laboratoryloth Medical Laboratury LCWSL, USA ARRADCOMATTN: Audiologist ATTN: DK DAR-LCB-TLAPO NEW YORK 09180 Watervliet Arsenal, NY 12189
Commander CommanderNaval Air Development Center Man-Machine Integration System
Biophysics Lab Code 602ATTN: G. Kydd Naval Air Levelop-ent CenterCode 60B1 Warminster, FA 13'74Warminster, PA 18974
Naval Air Development Center CommanderTechnical Information Division Naval Air D'volopmnt CunterTechnical Support Detachment ATTN: Code 6021 (Mr. Brindle)Warminster, PA 18974 Warinster, PA 18974
Commanding Officer Comnanding Otticer"Naval Medical Research Harry G. Arm:;tronq- Aorcn-a&*,
and Development Command Medical Resfarch Laboratur';National Naval Mudical Center right-1PitterronBethesda, MD 20014 Air Force Ba-;e, Oil 4)133
Under Secretary of Defense Directorfor Research and Engineering Army Audioiogy an I Snrech C, mt<-r
ATTN: Milit.ary A,:;sistink Walter 1,--.d Ar-iy '-,,di :al C .2t,'rfor Med ical and Life Scier.c,; iishin'jton, DC 203)7--21
Wa;hington, DC 2001
67

Director CommanderWalter Reed Army Institute U.S. Army Instihute
of Research of Dental ResearchWashington, DC 20307-5100 Walter Reed Army Medical Center
Washington, 5C 20307-5300
HQ DA (DASG-PSP-0) Naval Air Systems Command5109 Leesburg Pike Technical Air Library 950DFalls Church, VA 22041-3258 Rm 278, Jefferson Plaza II
Department cf the NavyWashington, DC 20361
Naval Research Naval Research Laboratory LibraryLaboratory Library Shock and Vibration Infer-
Code 1433 mation Center, Code 5804Washington, DC 20375 Washington, DC 20375
Harry Diamond Laboratories DirectorATTN: Technical Infor- U.S. Army Human Engineer-
mation Branch ing Laboratory2800 Powder Mill Road ATTN: Technical LibraryAdelphi, MD 20783-1197 Aberdeen Proving Ground,
MD 21005-5001
U.S. Army Materiel Systems Commander
Analysis Agency U.S. Army Test
ATTN: Reports Processing and Evaluation CommandAberdeen proving Ground ATTN: AMSTE-AD-HMD 21005-5017 Aberdeen Proving Ground,
MD 21005-5055
U.S. Army Ordnance enter Directorand School Library U.S. Army Ballistic
Building 3071 Research LaboratoryAberdeen Proving Ground, ATTN. DRXBR-OD-ST Tech ReportsND 21005-5201 Aberdeen Proving Ground,
MD 21005-5066
U.S. Army Environment1l llygiene CommanderAgency U.S. Army Mr-dical 1 R',,firch
Building E2100 Institute ol Chemical Piien~ eAberdeen Pruvini Gr-nJ, :TTN: SGRD-UV-AOMD 21010 Aberdeen Urovi ] -Ground,
MD 21010-3425
Technical Library Com:vin,.'rChemical Resorch U.S. Army M > -iI • R , "'ch
and Development Conter and []evcc mnt Co:". n,
Aberdeen Trovinj Groundi, AT'IN - P-i (. ;. ." . n)MD 21010-5423 Fort De trick, [ruderick,
MD 21701
68

-.Commander Coi, manorU.S. Army Medical Research U.S. Amy Biomedical Resoarc-h
Institute of Infectious Diseases and Develcc-, ,nt Lo'Ga-'r'
Fort Detrick, Frederick, ATTN: SGPD-1;5--IMD 21701 Fort Detrick, Frederick,
MD 21701
Director, Biological Defense Technical
Sciences Division Information CenterOffice of Naval Research Cameron Station600 North Quincy Street Alexandria, VA 22313Arlington, VA 22217
Commander U.S. Army Foreign ScienceU.S. Army Materiel Command and Technolcgy CenterATlN: A.MCDE-XS ATTN: MTZ5001 Eisenhower Avenue 220 7th Street, NFAlexandria, VA 22333 Charlottesville, VA 2 2 1--:36
Commandant Director,U.S. Army Aviation Applied Technology Labcratory
Logistics School USARTL-AVSCCM4ATTN: ATSQ-TDN ATTN: Library, Building 401Fort Eustis, VA 23604 Fort Eustis, VA 23604
U.S. Army Training U.S. Army Trainingand Doctrine Command and Doctrine Ccmmand
ATTN: ATCD-ZX ATTN: SurgeonFort Monroe, VA 23651 Fort Monroe, VA 23651-5000
Structures Laboratory Library Aviation Medicine ClinicUSARTL-AVSCOM TMC 422, SAAFNASA Langley Research Center Fort Bragg, NC 28305
Mail Stop 266Hampton, VA 23665
Naval Aerospace Medical U.S. Air Force ArmimentInstitute Library Develop:cit and Test Cot2'-
Bldg 1953, Code 102 Eglin Air Force -e, F.I ,Pensacola, FL 32508
Command Surgeon U.S. Army Mi-;;ile 2o~ ,.,U.S. Central Command Redstone ScicntilicMacDill Air Force Base Informaticri Cer'trFL 33608 ATTN: Doc,:i ( nt ,t i on
*Reds;toe Ar:;i iAi3t'P,52;
Air University Librry U.S. Ar:iy P: r' A(A I L /I J 1,/ 1 , - ) I. dh rt 0 , ,-
Maxwell AFB, AL 36,112 I'ropuli;ior" r -NASA Lc"wi._; i.:;e'.t h CntorCevo I n r'. 14 0',
69

AFA.MRL/HEX U.S. A;.r Force instituteWright-Patterson AFB, OH 45433 of 'e.:hnolcqy (AFIT/LDEF)
Buildi.,g £40, Area BWr,.gnt- , .t? - -n AFB, Oil 45433
University of Michigan Henry L. 13ylorNASA Center of Excellence Director, Ynstitute of Aviation
in Man-Systems Research Universit; -,f Illinois-ATTN: R. G. Snyder, Director Willarl irportAnn Arbor, MI 48109 Savoy, IL 6187.
John A. Dellinger, COL Craig L. Urb'uer, ChiefSouthwest Research Institute Office of Army SLrgeon GeneralP. 0. Box 28510 National Guard BureauSan Antonio, TX 78284 Washington, DC 50310-2500
Product Manager CommanderAviation Life Support Ecuip,'ent U.S. Army AviationATTN: AMCPM-ALSE Systems Command4300 Goodfellow Blvd. ATTN: SGRD-UAX-AL (C!XJ Lacy)St. Louis, MO 63120-1798 4300 Goodfellow Blvd., Bldg 105
St. Louis, MO 61120
Commander U.S. Army Aviation System, CormandU.S. Army Aviation Library and Information
Systems Command Center BranchATTN: AMSAV-ED ATTN: AIMSAV-DIL4300 Goodfellow Bivd 4300 Goodfellow BlvdSt. Louis, M0 63120 St. Louis, MO 63120
Commanding Officer Federal Aviation AdministrationNaval Biodynanics Laboratory Civil Aeromedical InotituteP.O. Box 24907 CAMI Library AAC 64D1New Orleans, LA 70189 P.O. Box 25082
Oklahoma City, OK 73125
U.S. Army Field Artillery School -ammanderATTN: Library U.S. Army AcaJo,-iySnow Hill, Room 14 of Health NciencesFort Sill, OK 73503 TTN: Library
Fort Sam Huuston, TX 73234
Commander CommanderU.S. Army Health Services Command U.S. Arm/ In:stituteATTN: 1,H20P-SO of Surq ici 1 U>,'arch
Fort Sam Houston, TX 72234-6000 A'ITN: . (;ID-i;. (J i 1W:')Fort Simi llnu:;ton, TX 7:23. -,2
70

Commander, U.S. ArmyAviation Center
Directorate Directoriteof Combat Developnents of Trainiig Develop7ent
Bldg 507 Bldg 502Fort Rucker, AL 36362 Fort Rucker, AL 36362
Chief Ch-efArmy Research Institute Human Engineering Laboratory
Field Unit Field UnitFort Rucker, AL 36362 Fort Rucker, AL 36362
Commander CommanderU.S. Army Safety Center U.S. Army Aviation CenterFort Rucker, AL 36362 and Fort Rucker
ATTN: ATZQ-T-ATLFort Ruc!,er, AL 36362
U.3. Army Aircraft Development PresidentTest Activity U.S. Army Aviation Board
ATTN: STEBG-MP-QA Cairns AAFCairns AAF Fort Rucker, AL 36362Fort Rucker, AL 36362
CommanderU.S. Army Medical Research
and Development CommandATTN: SGRD-PLC (COL Sedge)Fort Detrick, FrederickMD 21701
72

LCDR Angus H. Rup2rt, MC, US:NRNaval Aerospz:ce Medical Fesearch LaboratoryNaval Air StationPensacola, FL 32503-5700
Mr. Anthony M. CookAssistant Chief (Operations)Flight Systems & Simulation Research DivisionNASA Ames Research Center, Mail Stop 243-1Moffett Field, CA 94035
Dr. Michael E. McCauley, PresidentMonterey Technologies, Inc.P. 0. Box 223699Carmel, CA 93922
Mr. Richard S. BrayFlight Dynamics and Controls BranchNASA Ames Research Center, Mail Stop 211-2Moffett Field, CA 94035-1099
Dr. Malcolm M. CohenLife Science DivisionNASA Ames Research Center, Mail Stop 239-7Moffett Field, CA 94035-1099
Mr. Hal GeltmacherChief, Technology Development BranchAir Force Human Resources LcIboratoryWilliams Air korce Base, AZ 85240-6457
COL Charles P. Hatsell, USAF, MCCommanderAAMRL/ CCWright-Patterson Air Force Base, TX 78235-5000
MAJ James Voorhees, MSC, USAChief, Crew Station Research & Development BranchArmy Aeroflightdynamics DirectorateMoffett Field, CA 94035-1099
Mr. Walter S. ChambersHead, Advanced Simulation Concepts DivisionNaval Training Systems Center, Code N-73Orlando, FL 32813-7300
LCDR Lawrence ". Frank, MSC, USNChief Scientist, Electronic Warfare DiroctoratePacific MiFsile Te:;t Center, Code 400rPoint Mdgu, CA 93042
73

Dr. Fred E. Guedry, Jr.Chief ScientistNaval Aerospace Medical Rcseai7. L, zcratc!'yNaval Air StationPensacola, FL 32508-5700
LCDR Michael G. Lilienthal, MSC. s:Naval Training Systems Center,12350 Research Parkway, Code 350AOrlando, FL 32826-3224
Mr. Alan J. Benson, M.B., Cn. F;.Head, Behavioural Sciences Div:-i.RAF Institute of Aviation Medi,,r:Royal Aircraft EstablishmentFarnborough, Hants, GU14 6SZ, England
Dr. Kenneth E. Money,Chief ScientistDefense and Civil Institute of Env'ronmental MedicineP. 0. 3ox 2000Downsview, Ontario, Can,,Ia M3M 3B9
Mr. Frank M. CardulloState University of New YorkWatson School of Engineering
Applied Science and TechnolcjyBinghamton, NY 13901
Dr. Robert S. Kennedy, Vice PresidentEssex Corporation1040 Woodcock Road, Suite 227Orlando, FL 32803
Mr. L. Matthew Landry, Jr.Mail Stop 531/C240Engineering and Training Simulation Dept.McDonnel Douglas Helicopter Company5000 East McDowell RoadMesa, AZ 85205
Mr. John B. Sinacori, PresidentJohn B. Sinacori AssociatesP.O. Box 360
Pebble Beach, CA 93953-0360
74