silent killer diseases.ppt
DESCRIPTION
SILENT KILLER DISEASESMany diseases are silent killers in that they are silent (no symptoms or only vague symptoms), and that they are deadly. There are a number of diseases that are known as "silent killers" because they gradually consume you without causing any serious symptoms in the early stages. Regular medical checkups and early diagnosis of unexplained or vague symptoms can safe your life.TRANSCRIPT


SILENT KILLER DISEASESSILENT KILLER DISEASESHypertensionAmyloidosisSleep Apnea
By IFFAT FATIMA (08)
SILENT KILLER DISEASESSILENT KILLER DISEASES
Many diseases are silent killers in that they are silent (no symptoms or only vague symptoms) killer that they are deadly.
There are a number of diseases that are known as "silent killers" because they gradually consume you without causing any serious symptoms in the early stages.

Facts of silent killersFacts of silent killers

SYSTEMIC HYPERTENSIONSYSTEMIC HYPERTENSION Definitions of hypertension:
Elevated arterial blood pressure is a major cause of premature vascular disease leading to cerebrovascular events, ischaemic heart disease and peripheral vascular disease.

Hypertension - IntroductionHypertension - Introduction
Silent Killer – painless complications It is the leading risk factor –MI, HF, CRF
Stroke Responsible for the majority of office visits, Number one reason for drug prescription. 25% of population Complications bring to diagnosis but late…
Regulation of BP:Regulation of BP:
BP = Cardiac Output x Peripheral ResistanceEndocrine Factors
– Renin, Angiotensin, ANP, ADH, Aldosterone.Neural Factors
– Sympathetic & ParasympatheticBlood Volume
– Sodium, Mineralocorticoids, ANPCardiac Factors
– Heart rate & Contractility.

Control of Blood Pressure:Control of Blood Pressure:
BPCardiac Output
PeripheralResistance
Blood VolumeNa+, Aldosterone
VasoconstrictorsAngiotensin II
CatecholaminesVasodilatorsPg & Kinins
Local FactorspH, Hypoxia
Neural FactorsAdrenergic – Consß Adrenergic - Dil
Cardiac FactorsRate & Contract..
Humoral Factors
EtiologyEtiology 1- Essential:In more than 95% of cases, an underlyingcause cannot be found. Proposed
mechanismsinclude:Excess renal sodium retentionOver activity of sympathetic nervous
systemExess of Renin angiotensinHyperinsulinemiaAlterations in vascular endothelium

Factors contributing to the development of Essential hypertension
•Genetic Factors: hypertension is more common in some families and in some ethnic groups like African Americans
•Environmental factors include obesity, alcohol, lack of exercise and excess salt intake

2- Secondary hypertension2- Secondary hypertension Renal:
These account for over 80% of the cases of secondary hypertension. The
common causes are diabetic nephropathy, chronic glomerulonephritis, adult
polycystic disease, chronic tubulointerstitial nephritis. Endocrinal:
These include Conn's syndrome, adrenal hyperplasia, acromegaly, Cushing's
syndrome. Drugs and toxins Pregnancy-induced hypertension Vascular:
coarctation of aorta, vasculitis

ComplicationsComplicationsCerebrovascular
disease and coronary artery disease are the most common causes of death, although hypertensive patients are also prone to renal failure and peripheral vascular disease.

HYPERTENSIONHYPERTENSIONClassification of blood pressure levels:(according to the British Hypertension Society)
Category Systolic blood pressure Diastolic blood pressure
Optimal < 120 < 80Normal < 130 < 85High normal 130-139 85-89
HypertensionGrade I (mild) 140-159 90-99Grade 2 (moderate) 160-179 100-109Grade 3 (severe) ≥180 ≥110
Isolated systolic hypertensionGrade 1 140-149 < 90Grade 2 ≥160 < 90
HISTORYHISTORY The patient with mild hypertension is usually
asymptomatic. Attacks of sweating, headaches and palpitations
may point towards the diagnosis of phaeochromocytoma.
Higher levels of blood pressure may be associated with headaches, epistaxis or nocturia.
Breathlessness may be present owing to left ventricular hypertrophy or cardiac failure.
Malignant hypertension may present with severe headaches, visual disturbances, fits, transient loss of consciousness or symptoms of heart failure.
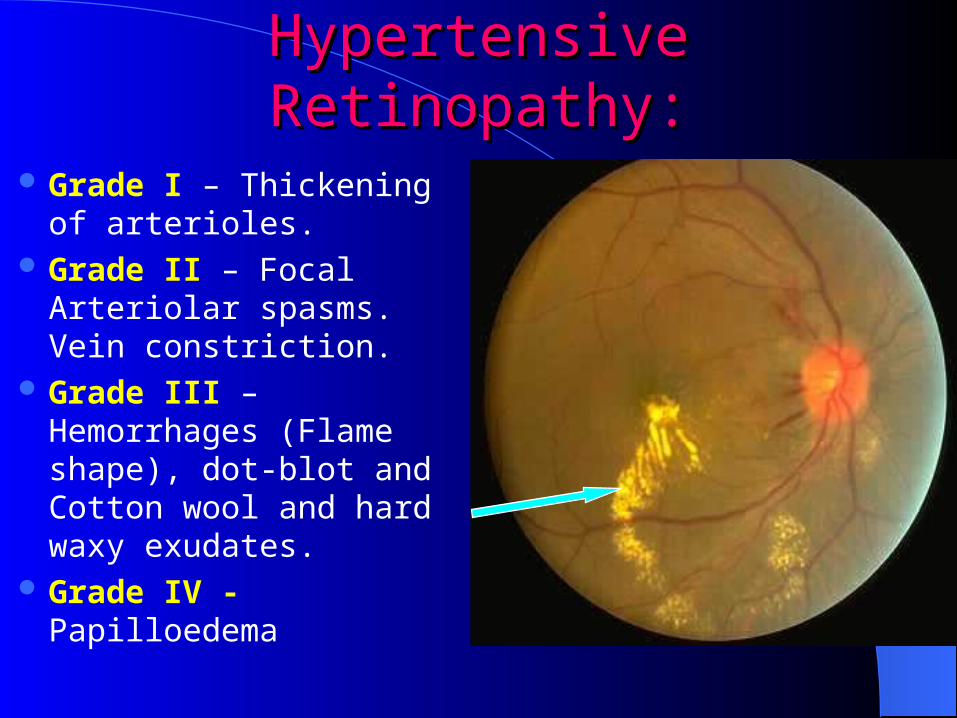
Hypertensive Retinopathy:Hypertensive Retinopathy:
Grade I – Thickening of arterioles.
Grade II – Focal Arteriolar spasms. Vein constriction.
Grade III – Hemorrhages (Flame shape), dot-blot and Cotton wool and hard waxy exudates.
Grade IV - Papilloedema

INVESTIGATIONSINVESTIGATIONSRoutine investigation of the hypertensive
patient should include: ECG Urine stix test for protein and blood Fasting blood for lipids (total and high-
density lipoprotein cholesterol) and glucose
Serum urea, creatinine and electrolytes.
Investigation of selected casesInvestigation of selected casesChest X-ray Ambulatory BP recordingEchocardiogram Renal ultrasoundRenal angiographyUrinary catecholaminesUrinary cortisol and dexamethasone
suppression testPlasma renin activity and aldosterone

Non-pharmcological treatmentNon-pharmcological treatment Weight reduction - BMI should be < 25 kg/m2 Low-fat and saturated fat diet Low-sodium diet - < 6 g sodium chloride per day Limited alcohol consumption - ≤ 21 units/week
for men and ≤ 14 units/week for women Dynamic exercise - at least 30 minutes' brisk walk
per day Increased fruit and vegetable consumption Reduce cardiovascular risk by stopping smoking
and increasing oily fish consumption.

AmyloidosisAmyloidosisAmyloidosis
is a group of diseases that result from the abnormal
deposition of a particular protein, called amyloid, in various
tissues of the body.
Amyloid protein
can be deposited in a localized area and may not be
harmful or only affect a single tissue of the body.
– Localized amyloidosis– Systemic amyloidosis

PathogenesisPathogenesis
