sidra medical and research center disclosure for potential ... · proximal gastrointestinal...
TRANSCRIPT
Fetal gastrointestinal anomalies
Daniel Kamil, MD, MBA Section Head - Antepartum & Clinics Division of Maternal-Fetal Medicine
Sidra Medical and Research CenterDisclosure for Potential Conflicts of Interest:
High GI Tract Obstruction:
Low GI Tract Obstruction:
Defects in Abdominal Wall Closure
High GI Tract Obstruction: Esophageal , gastric, duodenal and sometimes jejunal obstruction
=> Polyhydramnios 80%
Low GI Tract Obstruction: jejunoileal atresia, malrotation, intestinal duplication or meconium ileus and Large-bowel obstruction
=> Polyhydramnios < 25%
Polyhydramnios
• 1–2% of pregnancies
• Etiology:
Idiopathic (50%) Fetal (20%): gastrointestinal anomalies, CNS anomalies, aneuploidy, hydrops Maternal (30%): Diabetes mellitus, infections, lithium
• Retrospective cohort study (2003 - 2008)
• AFI ≥ 25 cm or a MVP ≥ 8 cm (even in the presence of AFI < 25 cm)
• N = 524 cases
• < 25 cm but with MVP ≥ 8 cm; 25–29.9 cm; 30–34.9 cm; and ≥ 35 cm

• Diabetes, gestational or pre-existing, was more frequent in women with mild polyhydramnios
• Almost 80% of pregnancies with an AFI ≥ 35 cm are associated with a prenatal diagnosis of fetal structural anomalies
• All the pregnancies complicated by fetal trisomy had associated anomalies in addition to polyhydramnios
• Almost 70% had mild polyhydramnios
Gastrointestinal atresia
▪Oesophageal atresia▪Duodenal atresia ▪ Jejuno-ileal atresia
Fetal intestinal volvulus
▪ Intestinal malrotation
Proximal gastrointestinal obstruction Congenital esophageal atresia
• 1/3500
• 50 % have other anomalies
• 25% cardiac anomalies
• Chromosomal anomalies in 6-10% (T18)
• VACTERL in 15%
Congenital esophageal atresiasign’s
• Polyhydramnion - after 20 weeks
• Small Stomach
• IUGR (in 2nd and 3rd trimester) - 40% A C
Prof. Dr. med. Karim Kalache Sidra's Division Chief of Maternal-Fetal Medicine
hypopharynx
Pouch Sign
Pouch Sign Pouch Sign Duodenal atresia
• 1-3/10,000
• 30 % have T21
• 5-15% of T21 will have DA
• 50-70% have other anomalies (cardiac, GI)
• Morality is 15-40%
Midgut Volvulus• The small bowel and
proximal colon twist around the superior mesenteric artery
• This leads to infarction of the involved intestine (Surgical emergency at birth!)
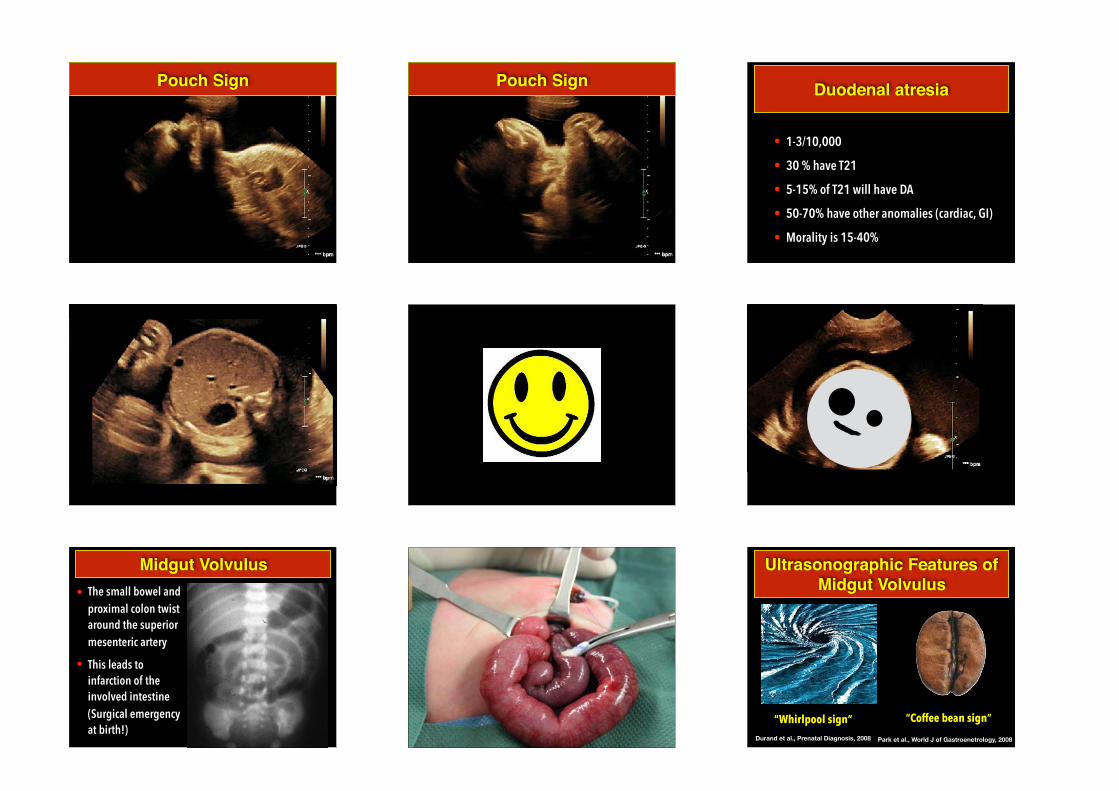
“Whirlpool sign“ Durand et al., Prenatal Diagnosis, 2008
“Coffee bean sign”
Park et al., World J of Gastroenetrology, 2008
Ultrasonographic Features of Midgut Volvulus

“Whirlpool sign“ Durand et al., Prenatal Diagnosis, 2008
“Coffee bean sign”
Park et al., World J of Gastroenetrology, 2008
Ultrasonographic Features of Midgut Volvulus
CF - small bowel obstruction
N = 29 Cases • Prenatal death: 4/28, 14% • Impaired neurological development:
4/28, 14%
1. Bradycardia/asystole following a vagal overactivity due to the distended esophagus, stomach, and cranial part of the duodenum
2. Raised levels of fetal serum bile acids
Relationship between Bowel Atresia & IUFT
3.
IOL @ 32 weeks if AF-bile acid > 10.0 mmol/L

Dead/IUFD: 9/16 Jejunal atresia: 8/16 Onset at 32-34 weeks: 9/16
? ▪ Omphalocoele (mainly polyhydramnios)
Abdominal wall defects
▪ Gastroschisis (mainly oligohydramnios)
Omphalocele Omphalocele = exomphalos
Intestines, liver, and occasionally other
organs remain outside in a sac (amnion
and peritoneum)
Abdominal contents herniates through
the umbilical cord = MIDLINE
Defect in the development of the
muscles of the abdominal wall
Omphalocelle
• 1/4000
• 50 % have other anomalies
• 25% mortality
• Genetic syndrome in 10%
• Chromosomal abnormalities in 60% (Non liver)
In week 8 (PM) abdominal cavity is too
small to contain all organs
Pathogenesis
Must disappear until week 12
Protrusion of intestine (never Liver!)
into the extracelomic space at the base
of umbilical cord = physiologic
herniation
The cause is unknown.Risk factors
under 20 years - OR 2,5
above 40 years - OR 8,5 !
Obese women
Male fetes
SSRI intake
Multi parity
Omphalocele
Cardiac anomalies (50%)
Neural tube defect (40%).
About15% of live-born have
chromosomal abnormalities.
Larger omphalocele are associated with
a higher risk of cardiac defects
50% will have other congenital defects
Omphalocele Diagnosis
Non liver - suspect aneuploidy
Liver containing can be diagnosed
before 12 weeks
alpha feto protein in maternal serum
High NT
Liver containing or not
Omphalocelle
• Always perform genetic testing
• Look for other anomalies / syndromes
• Heart
• NTD
• Genitourinary
• Cantrell / OEIS / Beckwith-Wiedemann…
Omphalocelle
• Overall survival 90%
• Recurrence risk:
• 1% - if trisomy
• Less than 1% if normal Karyotype
• No early delivery needed
• No caesarian section needed
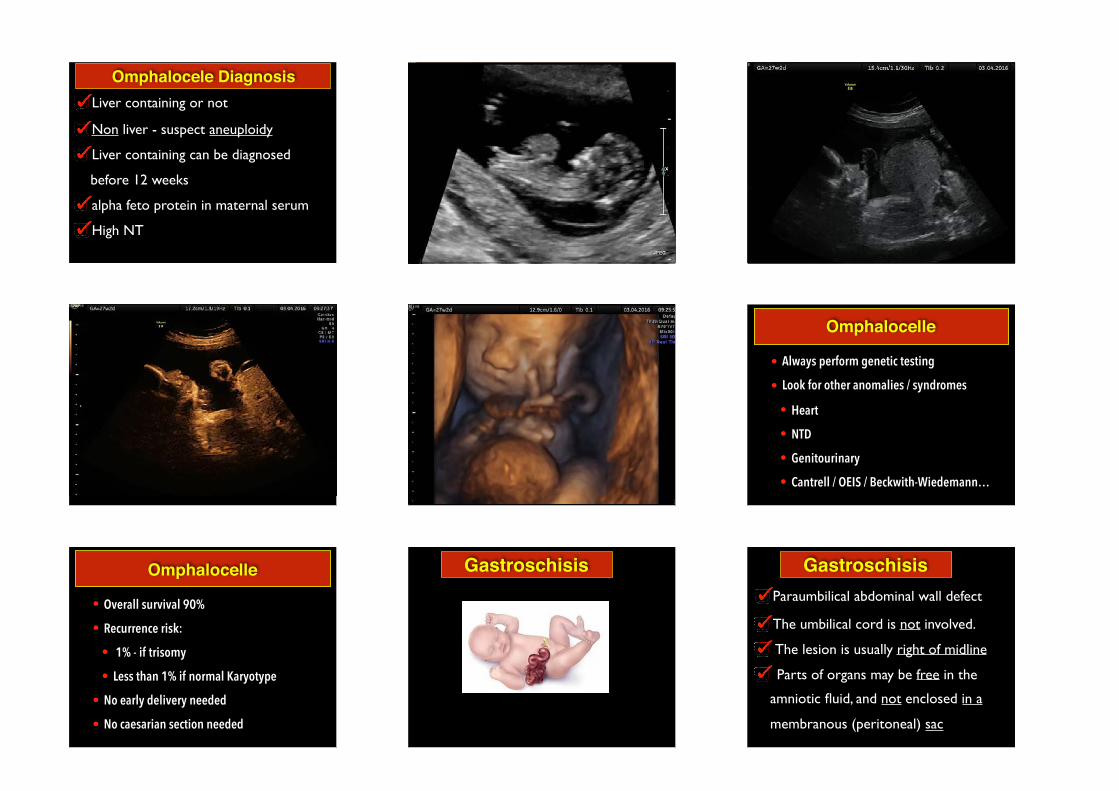
Gastroschisis Gastroschisis
The umbilical cord is not involved.
The lesion is usually right of midline
Parts of organs may be free in the
amniotic fluid, and not enclosed in a
membranous (peritoneal) sac
Paraumbilical abdominal wall defect

Gastroschisis
In most cases we will expect:
OLIGOHYDRAMNIOS
Might also present as PolyhydramniosDisruption of blood supply to the
developing abdominal wall from the
omphalomesenteric duct artery by the 8.
week of gestation.
Incidence: 1 of 2500-3000 live births
Gastroschisis Aspirin quadruples the risk Change in paternity - Immun?
Young mothers = RR 7! (Cigarets, Alcohol,
drugs, Genitourinary infections…)
Slightly more males than femalesIUGR?
• IUGR facilitates apparition of
gastroschisis, or abdominal wall defect impairs fetal growth - not clear
Gastroschisis - Risk factors
90% No other malformations
10% GI and Cardial
Multifactorial determination with a
2-3% recurrence risk.
Stand-alone congenital defect
Gastroschisis
Gastroschisis
Gastroschisis
• Genetic testing NOT needed (when isolated)
• Look for IUGR (30-60%)
• CAVE:
• Premature birth (30-65%)
• Bowl dilatation and wall thickening
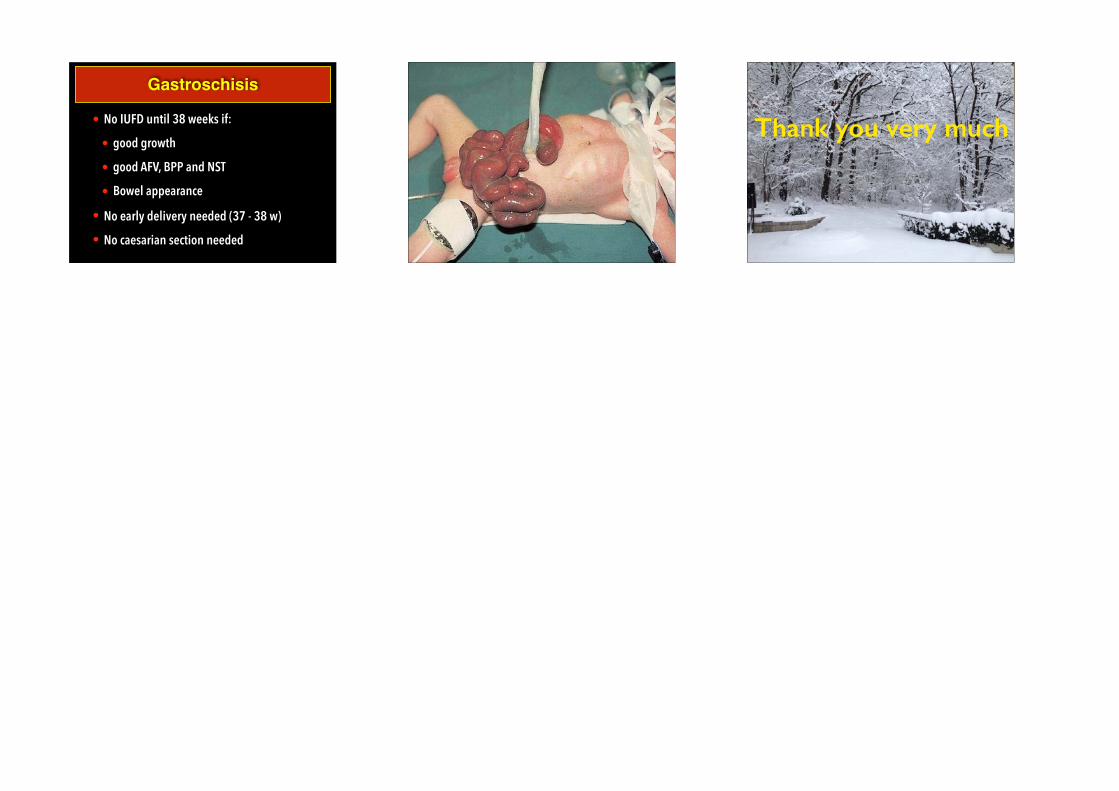
Gastroschisis
• No IUFD until 38 weeks if:
• good growth
• good AFV, BPP and NST
• Bowel appearance
• No early delivery needed (37 - 38 w)
• No caesarian section needed
Thank you very much