side effects from azathioprine in a patient with thiopurine s-methyl transferase deficiency
TRANSCRIPT

Respiratory Medicine CME (2009) 2, 102e105
CASE REPORT
Side effects from azathioprine in a patient withthiopurine S-methyl transferase deficiency
Daniel Park a, Anna Fergusson a, Loretta Ford b, Jonathon Berg b,Adel H. Mansur a,*
a Respiratory Department, Birmingham Heartlands Hospital, Bordesley Green, Birmingham, B9 5SS, UKb Department of Clinical Biochemistry, City Hospital, Dudley Road, Birmingham, B18 7QH, UK
Received 31 July 2008; accepted 15 October 2008
KEYWORDSazathioprine;thiopurine methyltransferase (TPMT);non specific intersitialpneumonia (NSIP);drug related toxicity
* Corresponding author. Tel.: þ44 (121 7720292.
E-mail address: adel.mansur(A.H. Mansur).
1755-0017/$34 ª 2008 Elsevier Ltd. Adoi:10.1016/j.rmedc.2008.10.005
Summary
Azathioprine is an immunosuppressant and cytotoxic pro-drug which acts to impair purinesynthesis. Side effects including nausea, rash, hepatotoxicity and bone marrow suppressionfrequently limit its use. Thiopurine S-methyl transferase (TPMT) is an important enzyme whichmetabolises thiopurines such as azathioprine to inactive metabolites. TPMT activity variesgreatly between individuals, and has a trimodal distribution. Individuals may be homozygousfor the highly active wild type allele, heterozygous with a low activity variant allele, or behomozygous for the low activity variant. Reduced TPMT activity conveys a greater risk of drugrelated side effects from thiopurines.
We report a case in which azathioprine used to treat non specific interstitial pneumonia re-sulted in marked pancytopaenia. Azathioprine treatment had been commenced without firstchecking the TPMT status. The subsequent discovery of TPMT deficiency in this patient ex-plained the development of complications. Limited therapeutic options led to the patientbeing treated with an extremely low azathioprine dose regime. The drug was tolerated withoutfurther toxicity.
This case highlights the benefits of screening the TPMT activity of all patients where azathi-oprine treatment is being considered. It also gives further evidence that TPMT deficient indi-viduals are able to tolerate a very low dose azathioprine regime without side effects.ª 2008 Elsevier Ltd. All rights reserved.
0) 121 4242746; fax: þ44 (0)
@heartofengland.nhs.uk
ll rights reserved.
Statement of clinical relevance/originality
This case report relates to the development of side effectsfollowing the use of azathioprine in a Thiopurine S-methyltransferase (TPMT) deficient individual. This is a topic of
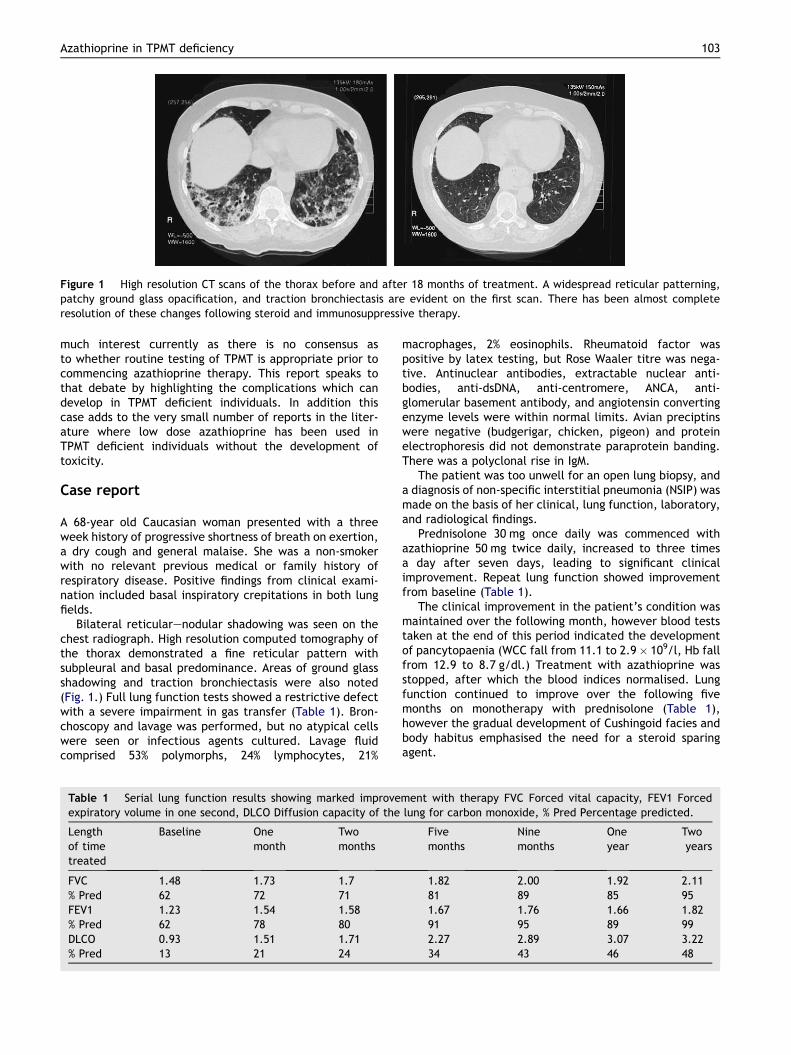
Figure 1 High resolution CT scans of the thorax before and after 18 months of treatment. A widespread reticular patterning,patchy ground glass opacification, and traction bronchiectasis are evident on the first scan. There has been almost completeresolution of these changes following steroid and immunosuppressive therapy.
Azathioprine in TPMT deficiency 103
much interest currently as there is no consensus asto whether routine testing of TPMT is appropriate prior tocommencing azathioprine therapy. This report speaks tothat debate by highlighting the complications which candevelop in TPMT deficient individuals. In addition thiscase adds to the very small number of reports in the liter-ature where low dose azathioprine has been used inTPMT deficient individuals without the development oftoxicity.
Case report
A 68-year old Caucasian woman presented with a threeweek history of progressive shortness of breath on exertion,a dry cough and general malaise. She was a non-smokerwith no relevant previous medical or family history ofrespiratory disease. Positive findings from clinical exami-nation included basal inspiratory crepitations in both lungfields.
Bilateral reticularenodular shadowing was seen on thechest radiograph. High resolution computed tomography ofthe thorax demonstrated a fine reticular pattern withsubpleural and basal predominance. Areas of ground glassshadowing and traction bronchiectasis were also noted(Fig. 1.) Full lung function tests showed a restrictive defectwith a severe impairment in gas transfer (Table 1). Bron-choscopy and lavage was performed, but no atypical cellswere seen or infectious agents cultured. Lavage fluidcomprised 53% polymorphs, 24% lymphocytes, 21%
Table 1 Serial lung function results showing marked improveexpiratory volume in one second, DLCO Diffusion capacity of the
Lengthof timetreated
Baseline Onemonth
Twomonths
FVC 1.48 1.73 1.7% Pred 62 72 71FEV1 1.23 1.54 1.58% Pred 62 78 80DLCO 0.93 1.51 1.71% Pred 13 21 24
macrophages, 2% eosinophils. Rheumatoid factor waspositive by latex testing, but Rose Waaler titre was nega-tive. Antinuclear antibodies, extractable nuclear anti-bodies, anti-dsDNA, anti-centromere, ANCA, anti-glomerular basement antibody, and angiotensin convertingenzyme levels were within normal limits. Avian preciptinswere negative (budgerigar, chicken, pigeon) and proteinelectrophoresis did not demonstrate paraprotein banding.There was a polyclonal rise in IgM.
The patient was too unwell for an open lung biopsy, anda diagnosis of non-specific interstitial pneumonia (NSIP) wasmade on the basis of her clinical, lung function, laboratory,and radiological findings.
Prednisolone 30 mg once daily was commenced withazathioprine 50 mg twice daily, increased to three timesa day after seven days, leading to significant clinicalimprovement. Repeat lung function showed improvementfrom baseline (Table 1).
The clinical improvement in the patient’s condition wasmaintained over the following month, however blood teststaken at the end of this period indicated the developmentof pancytopaenia (WCC fall from 11.1 to 2.9� 109/l, Hb fallfrom 12.9 to 8.7 g/dl.) Treatment with azathioprine wasstopped, after which the blood indices normalised. Lungfunction continued to improve over the following fivemonths on monotherapy with prednisolone (Table 1),however the gradual development of Cushingoid facies andbody habitus emphasised the need for a steroid sparingagent.
ment with therapy FVC Forced vital capacity, FEV1 Forcedlung for carbon monoxide, % Pred Percentage predicted.
Fivemonths
Ninemonths
Oneyear
Twoyears
1.82 2.00 1.92 2.1181 89 85 951.67 1.76 1.66 1.8291 95 89 992.27 2.89 3.07 3.2234 43 46 48

104 D. Park et al.
Measurement of the patients whole blood Thiopurine S-methyl transferase (TPMT) activity was requested andfound to be undetectable at <1 nmol 6-MTG/g Hb/hr.1 Thedeficient TPMT activity status of the patient was alsoconfirmed by TPMT genotyping. The patient was found tobe homozygous for the most common polymorphism asso-ciated with deficient TPMT enzyme activity in Caucasians,TPMT*3A, which is characterised by a double mutant allele(G to A transition at nucleotide 460 on exon 7, and A to Gtransition at nucleotide 719 on exon 10.)2,3
A very low dose of azathioprine (5 mg OD) was restarted,and the steroid dose to be weaned. No significant sideeffects were suffered by the patient. Lung functioncontinued to improve two years out from the initialpresentation (Table 1), and a repeat HRCT showed almostcomplete resolution of the previously observed radiologicalabnormalities (Fig. 1).
Discussion
Azathioprine is a mercaptopurine derivative with bothcytotoxic and immunosuppressive effects. Indications forits use are found across many medical specialties, andinclude rheumatoid arthritis, inflammatory bowel disease,vasculitis, chronic hepatitis, a number of dermatologicalconditions and the prevention of rejection of solid organtransplants.
The subject of this case report was diagnosed andtreated for NSIP. Whilst many respiratory physicians useazathioprine in the management of interstitial lung diseasethere is limited evidence of its efficacy, even for idiopathicpulmonary fibrosis (IPF) which is the most common and wellinvestigated of these conditions.4,5 Of the few good qualitystudies in this area, a randomised controlled trialcomparing an azathioprine and prednisolone combinationwith prednisolone alone in 27 patients with IPF demon-strated a small but statistically significant improvement insurvival for the combination therapy group when adjustedfor age.6
Side effects are common with azathioprine and includenausea, vomiting, rash, hepatotoxicity, and myelosup-pression. Severe toxicity has been recorded in 30e42% ofpatients treated with the drug.7,8 International guidelinesrecommend a cautious approach to azathioprine treat-ment, using small increments from a low initial dose.9 Therelatively high starting dose in our patient may havecontributed to the development of side effects.
The desire to identify patients at particular risk of drugrelated complications following the use of azathioprine ledto the introduction of TPMT testing to the UK in the early1990s. TPMT is one of the principal enzymes involved in themetabolism of thiopurines such as azathioprine to inactivemetabolites There is a marked variation in the activity ofTPMT between individuals, largely as a result of singlenucleotide polymorphisms, many of which result in a loss ofenzyme activity compared to the wild type. A trimodaldistribution in enzyme activity has been described whichcorresponds to homozygosity for a highly active allele,heterozygosity with a low activity allele, and homozygosityfor the low activity variant. Thus normal/high levels ofactivity are seen in approximately ninety percent of the
population, whilst ten percent have low TPMT activity, andone in three hundred has severely deficient TPMTactivity.10,11 Low levels of TPMT are strongly associatedwith marked toxicity secondary to azathioprine.12,13
However, individuals known to have low TPMT activity cansubsequently have their azathioprine dose adjusted,allowing continuing treatment without acute dose limitingtoxicity. Particular caution is necessary in treating individ-uals in the severely TPMT deficient group such as thesubject of this case report, although successful use of verylow doses of azathioprine has previously been described inboth inflammatory bowel disease14,15 and acute lympho-blastic leukaemia.13,16,17 Conversely, patients with partic-ularly high TPMT activity may require higher than usualazathioprine doses.
Current guidelines from different specialty professionalbodies vary greatly in whether to recommend routine TPMTtesting prior to the use of azathioprine.18e20 These differ-ences reflect the lack of evidence at present as to whetherroutine pre-treatment TPMT testing will actually reducethe number of adverse reactions in practice.
This case highlights the problems that can develop whena patient with TPMT deficient status is treated with stan-dard azathioprine doses, and the benefits which would begained from TPMT testing. Checking TPMT status isbecoming increasingly common practice and can bothensure that we do not normally use thiopurine drugs indeficient patients and also so that we can reduce the dosein heterozygote patients. We also give further evidencethat it is possible to treat TPMT deficient patients usingvery low doses of azathioprine without side effects.
Patient details
The subject of this case report has read the final version ofthe manuscript, understands the implications of publica-tion, and has given written consent.
Funding
No additional funding was required in the preparation ofthis case report.
Contributors
DP, AF, and LF carried out the first drafting of the manu-script. JB and AHM were responsible for initiating andreviewing the report, and final drafting of the manuscript.
Conflict of interest statement
The authors have no conflict of financial or other interest todeclare with regards to the contents of this case report.
Acknowledgements
We wish to thank Dr Madava Djearaman, Consultant Radi-ologist, Birmingham Heartlands Hospital, for his help withthe interpretation of the radiological findings in this case.

Azathioprine in TPMT deficiency 105
References
1. Ford L, Graham V, Berg J. Whole-blood thiopurine S-methyl-transferase activity with genotype concordance: a new,simplified phenotyping assay. Ann Clin Biochem 2006;43(Pt 5):354e60.
2. Otterness D, Szumlanski C, Lennard L, et al. Human thiopurinemethyltransferase pharmacogenetics: gene sequence poly-morphisms. Clin Pharmacol Ther 1997;62(1):60e73.
3. Krynetski E, Schuetz J, Galpin A, Pui C, Relling M, Evans W.A single point mutation leading to loss of catalytic activity inhuman thiopurine S-methyltransferase. Proc Natl Acad SciU S A 1995;92(4):949e53.
4. Davies H, Richeldi L, Walters E. Immunomodulatory agents foridiopathic pulmonary fibrosis. Cochrane Database Syst Rev2003;(3). CD003134.
5. Walter N, Collard H, King TJ. Current perspectives on thetreatment of idiopathic pulmonary fibrosis. Proc Am Thorac Soc2006;3(4):330e8.
6. Raghu G, Depaso W, Cain K, et al. Azathioprine combined withprednisone in the treatment of idiopathic pulmonary fibrosis:a prospective double-blind, randomized, placebo-controlledclinical trial. Am Rev Respir Dis 1991;144(2):291e6.
7. Martı́nez F, Nos P, Pastor M, Garrigues V, Ponce J. Adverseeffects of azathioprine in the treatment of inflammatory boweldisease. Rev Esp Enferm Dig 2001;93(12):769e78.
8. Stolk J, Boerbooms A, de Abreu R, et al. Reduced thiopurinemethyltransferase activity and development of side effects ofazathioprine treatment in patients with rheumatoid arthritis.Arthritis Rheum 1998;41(10):1858e66.
9. American Thoracic Society. Idiopathic pulmonary fibrosis:diagnosis and treatment. International consensus statement.American Thoracic Society (ATS), and the European RespiratorySociety (ERS). Am J Respir Crit Care Med 2000;161(2 Pt 1):646e64.
10. Weinshilboum R, Sladek S. Mercaptopurine pharmacoge-netics: monogenic inheritance of erythrocyte thiopurine
methyltransferase activity. Am J Hum Genet 1980;32(5):651e62.
11. McLeod H, Lin J, Scott E, Pui C, Evans W. Thiopurine methyl-transferase activity in American white subjects and blacksubjects. Clin Pharmacol Ther 1994;55(1):15e20.
12. Black A, McLeod H, Capell H, et al. Thiopurine methyl-transferase genotype predicts therapy-limiting severe toxicityfrom azathioprine. Ann Intern Med 1998;129(9):716e8.
13. Evans W, Hon Y, Bomgaars L, et al. Preponderance of thio-purine S-methyltransferase deficiency and heterozygosityamong patients intolerant to mercaptopurine or azathioprine.J Clin Oncol 2001;19(8):2293e301.
14. Kaskas B, Louis E, Hindorf U, et al. Safe treatment of thio-purine S-methyltransferase deficient Crohn’s disease patientswith azathioprine. Gut 2003;52(1):140e2.
15. Gardiner S, Gearry R, Barclay M, Begg E. Two cases of thio-purine methyltransferase (TPMT) deficiency e a lucky save anda near miss with azathioprine. Br J Clin Pharmacol 2006;62(4):473e6.
16. Evans W, Horner M, Chu Y, Kalwinsky D, Roberts W. Alteredmercaptopurine metabolism, toxic effects, and dosagerequirement in a thiopurine methyltransferase-deficient childwith acute lymphocytic leukemia. J Pediatr 1991;119(6):985e9.
17. Lennard L, Gibson B, Nicole T, Lilleyman J. Congenital thio-purine methyltransferase deficiency and 6-mercaptopurinetoxicity during treatment for acute lymphoblastic leukaemia.Arch Dis Child 1993;69(5):577e9.
18. Anstey A, Wakelin S, Reynolds N. Guidelines for prescribingazathioprine in dermatology. Br J Dermatol 2004;151(6):1123e32.
19. Chakravarty K, McDonald H, Pullar T, et al. BSR & BHPRguideline for disease-modifying anti-rheumatic drug (DMARD)therapy in consultation with the British Association of Derma-tologists. Rheumatology (Oxford); 2006 Sep.
20. Carter M, Lobo A, Travis S. Guidelines for the management ofinflammatory bowel disease in adults. Gut 2004;53(Suppl. 5):V1e16.