sickle cell disease (bone changes)_torfs
TRANSCRIPT

A 25-year old patient with a history of domestic violence?
M. Torfs
UZA
Staff meeting Radiology, 06-02-2014

Case presentation
• Medical history: unknown
• Current medical problems:o Unclear anamnesis
o Maxillofacial trauma: elbow strike against mandibula
o Painful temporomandibular joints
• Domestic violence?

CT-scan: VR

CT-scan: VR

CT-scan: VR

CT-scan: VR

CT-scan: VR

CT-scan: VR

CT-scan: VR

CT-scan: VR

CT-scan: VR

CT-scan: VR

CT-scan: VR

Diagnosis?
• No posttraumatic injury

CT-scan: bone window

Diagnosis?
• Sickle cell anemia:
Bone marrow hyperplasia
H vertebrae

Skeletal manifestations in sicklecell disease
Epidemiology Pathophysiology Clinical features
Imaging

Sickle cell disease (SCD)
• First described in the medical literature by the American physician James B Herrick in 1910
• Almost 300,000 children are born with a form of sickle-cell disease every year, mostly in sub-Saharan Africa, but also in other countries such as the West Indies and tribals of South Asia, and in people of African origin elsewhere in the world

Distribution of sickle celltrait
Historical distribution of malaria
Wikipedia

Sickle cell disease (SCD)
• Hereditary blood disorder, characterised by an abnormalityin the oxygen-carrying haemoglobin molecule in RBC’s(hemoglobinopathy)
• Homozygosity for the abnormal hemoglobin, hemoglobin S (HbS) – autosomal recessive
• The disorder is most severe in patients with homozygosityfor HbS, of intermediate severity in hemoglobin SC disease (HbSC, combined heterozygosity for hemoglobins S and C), and generally benign in those with sickle cell trait (heterozygosity for HbS)

The National Heart, Lung, and Blood Institute (NHLBI) - http://www.nhlbi.nih.gov/health/health-topics/topics/sca/

Sickle cell disease
• Clinically characterised by vaso-occlusive phenomenaand hemolysis
• Vaso-occlusion results in recurrent painful episodes (previously called sickle cell crisis) and a variety of serious organ system complications that can lead to life-long disabilities and/or early death.
• Various complications including stroke (silent or symptomatic), acute chest syndrome, serious bacterial infections due to hyposplenism, …

Skeletal manifestations in sickle celldisease
• Result of changes in bone and bone marrow caused by the chronic tissue hypoxia that is exacerbated by episodic occlusion of the microcirculation by the abnormal sickle cells
• Main processes that lead to bone and joint destruction in sickle cell disease are infarction of bone and bone marrow, compensatory bone marrow hyperplasia, secondary osteomyelitis, and secondary growth defects

Mystatdx.com

Skeletal manifestations in sickle celldisease
• Bone marrow hyperplasia caused by chronic anaemia• Infarction of bone and bone marrow in patients with
sickle cell disease can lead to the following changes:- osteolysis (in acute infarction)- osteonecrosis (avascular necrosis/aseptic necrosis)- articular disintegration- myelosclerosis- periosteal reaction (unusual in the adult)- H vertebrae (steplike endplate depression also known as
the Reynold sign or codfish vertebrae) - dystrophic medullary calcification- bone-within-bone appearance

Bone marrow hyperplasia in SCD
• The shortened survival time of the erythrocytes in sickle cell (10-20 days) leads to a compensatory marrow hyperplasia throughout the skeleton. The bone marrow hyperplasia has the resultant effect of weakening the skeletal tissue by widening the medullary cavities, replacing trabecular bone and thinning cortices.
Hair-on-end appearance. Medscape

Bone marrow hyperplasia in SCD
• Extramedullary hematopoiesis (EMH):
o Response to erythropoiesis failure in BM
o Occurs most often in the spleen and liver and occasionally in the lymph nodes. Less commonorgans include the pleura, lungs, gastrointestinaltract, breast, skin, brain, kidneys, and adrenalglands.
Gumbs RV, Higginbotham-Ford EA, Teal JS, Kletter GG, Castro O. Thoracic extramedullaryhematopoiesis in sickle-cell disease. AJR Am J Roentgenol. 1987 Nov;149(5):889-93

Bone infarctions
• Bone infarcts typically involve medullarycavities and epiphyses
• The proximal humeri, proximal femora, and vertebral bodies are often affected
Radiopaedia.org

Hand-foot syndrome
• Often initial manifestation, in child 0.5-2 years
• Swelling, decreased range of motion of digits
• Occurs with new onset of cold temperatures & resultant vasoconstriction
• Results from bone infarcts in the diaphyses of small long bones
• Self limiting, days to weeks

Patient B: 12-year old boy with SCD

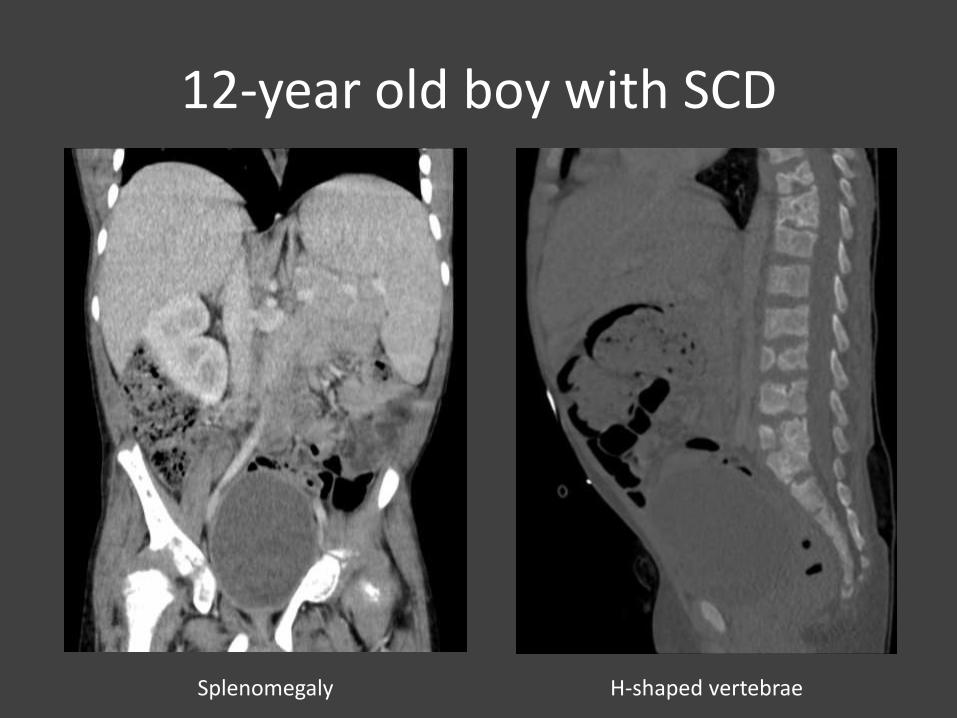
12-year old boy with SCD

12-year old boy with SCD
Dystrophic medullarycalcifications
12-year old boy with SCD
Splenomegaly H-shaped vertebrae

12-year old boy with SCD
Distortion of the proximalfemoral epiphyses (L>R) after Legg-Calvé Perthes

Patient C: 3-year old girl with proptosis
Subperiosteal hemorrhage associated to boneinfarction

SCD: take home messages
• Hereditary hemoglobinopathy, characterised byvaso-occlusive phenomena and hemolysis
• Various complications including stroke (silent or symptomatic), acute chest syndrome, serious bacterial infections due to hyposplenism, …
• Skeletal manifestations include bone marrow hyperplasia, extramedullary hematopoiesis and bone infarctions

References
• Statdx.com
• Uptodate.com
• Wikipedia.org
• Gumbs RV, Higginbotham-Ford EA, Teal JS, Kletter GG, Castro O. Thoracic extramedullaryhematopoiesis in sickle-cell disease. AJR Am J Roentgenol. 1987 Nov;149(5):889-93