shoulder shoulder dystocia dystocia learning … bone fracturedata suggest that a significant...
TRANSCRIPT

1
Shoulder Shoulder DystociaDystocia
Maurice L. Druzin, MDMaurice L. Druzin, MDCharles B. and Ann L. Johnson ProfessorCharles B. and Ann L. Johnson Professor
ViceVice--Chair, Department of Obstetrics and GynecologyChair, Department of Obstetrics and GynecologyChief, Division of MaternalChief, Division of Maternal--Fetal MedicineFetal Medicine
Stanford University Medical CenterStanford University Medical Center
Learning ObjectivesLearning Objectives
At the end of this activity, the learner will be At the end of this activity, the learner will be aware of:aware of:
1. Risk factors for shoulder 1. Risk factors for shoulder dystociadystocia2. Maternal and neonatal complications of 2. Maternal and neonatal complications of
shoulder shoulder dystociadystocia3. Systematic approach to shoulder 3. Systematic approach to shoulder dystociadystocia4. Training methods to address shoulder 4. Training methods to address shoulder
dystociadystocia
33
Shoulder DystociaShoulder Dystocia
Shoulder Dystocia is most often an Shoulder Dystocia is most often an unpredictableunpredictable and and unpreventableunpreventableobstetric emergency. obstetric emergency.
Failure of the shoulders to deliver spontaneously places both the Failure of the shoulders to deliver spontaneously places both the pregnant woman and fetus at risk for injury. pregnant woman and fetus at risk for injury.
Several maneuvers to release impacted shoulders have been Several maneuvers to release impacted shoulders have been developed, but the urgency of this event makes developed, but the urgency of this event makes prospective studies prospective studies impracticalimpractical for comparing their effectiveness.for comparing their effectiveness.
ACOG Practice Bulletin #40ACOG Practice Bulletin #40November 2002November 2002
44
Definition of Shoulder DystociaDefinition of Shoulder Dystocia
Shoulder dystocia is most often defined as Shoulder dystocia is most often defined as a delivery that a delivery that requires additional obstetric maneuvers following failure of requires additional obstetric maneuvers following failure of gentle gentle downward traction on the fetal head to effect delivery downward traction on the fetal head to effect delivery of the shouldersof the shoulders..
__________________________________________________________________________________________
Definition of the word:Definition of the word: GentleGentle
Definition: Free from harshness, sternness, or violence. Definition: Free from harshness, sternness, or violence.
Soft, Delicate, Moderate Soft, Delicate, Moderate ACOG Practice Bulletin #40ACOG Practice Bulletin #40
November 2002November 2002

2
55
Risk Factors for Shoulder DystociaRisk Factors for Shoulder Dystocia
Fetal Macrosomia Labor Abnormalities
Diabetes Mellitus Post-term Pregnancy
Operative Vaginal Delivery Male Fetal Gender
History of Shoulder Dystocia Obesity and High Birth Weight Gain
Advanced Maternal Age Shoulder – Pelvic Disproportion
Other AnomaliesTumorsPelvic DeformitiesStature
UpToDateUpToDateDiagnosis and management of Diagnosis and management of
pregnancies at risk for shoulder dystociapregnancies at risk for shoulder dystocia
66
Maternal ComplicationsMaternal Complications
•• 11% rate of 11% rate of postpartum hemorrhagepostpartum hemorrhage•• 3.8% rate of 3.8% rate of 44thth degree lacerationsdegree lacerations
These complications were These complications were not more commonnot more common with with rotational rotational maneuvers or other fetal manipulation when compared with the maneuvers or other fetal manipulation when compared with the McRobertsMcRoberts maneuver alone.maneuver alone.
HeroicHeroic maneuvers in cases of maneuvers in cases of catastrophiccatastrophic shoulder shoulder dystociadystocia, , such as: such as: ZavanelliZavanelli maneuver maneuver
AbdominalAbdominal rescue rescue SymphsiotomySymphsiotomy, ,
may be associated with may be associated with significantsignificant maternal morbidity.maternal morbidity.
ACOG Practice ACOG Practice Bulletin #40Bulletin #40November 2002November 2002
O’Leary, 1992, O’Leary, 1992, O’Shaughnessy, 1998O’Shaughnessy, 1998
Neonatal ComplicationsNeonatal Complications�� Brachial plexus injuries and fractures of the clavicle and humerus Brachial plexus injuries and fractures of the clavicle and humerus
are associated with shoulder dystocia. are associated with shoulder dystocia.
�� The reported incidence of brachial plexus injuries following a The reported incidence of brachial plexus injuries following a delivery complicated by shoulder dystocia varies widely from 4% to delivery complicated by shoulder dystocia varies widely from 4% to 40%.40%.
�� Fortunately, most cases Fortunately, most cases resolveresolve without permanent disability: that without permanent disability: that is, is, fewer than 10%fewer than 10% of all cases of shoulder dystocia result in a of all cases of shoulder dystocia result in a persistent brachial plexus injury.persistent brachial plexus injury.
�� Data suggest that a significant proportion (34Data suggest that a significant proportion (34--47%) of brachial 47%) of brachial plexus injuries are plexus injuries are notnot associated with shoulder dystocia: associated with shoulder dystocia:
�� In fact, 4% occur In fact, 4% occur after cesarean deliveryafter cesarean delivery..
ACOG Practice Bulletin #40ACOG Practice Bulletin #40November 2002November 2002
Incident and Type of Fetal Injury Incident and Type of Fetal Injury Identified in 37,110 Cesarean DeliveriesIdentified in 37,110 Cesarean Deliveries
OBGYN, Fetal Injury and Cesarean Delivery
Vol. 108, No 4, October 2006
Table 1. Incidence and Type of Fetal Injury Identi fied in 37,110 Cesarean Deliveries
Total number of injuries * 418 (11.3)Skin laceration 272 ( 7.3)Cephalohematoma 88 ( 2.4)Clavicle fracture 11 ( 0.3)Facial nerve palsy 11 ( 0.3)Brachial plexus injury 9 ( 0.2)Skull fracture 6 ( 0.2)Long bone fracture 8 ( 0.2)Intracranial hemorrhage 2 ( 0.1)Other† 20 ( 0.5)
* Nine patients had two fetal injuries.† Includes abnormal bruising, subconjunctival hemorr hage, abrasion, and minor
injuries not able to be classified.

3
Neonatal ComplicationsNeonatal Complications
�� Some severe cases of shoulder dystocia Some severe cases of shoulder dystocia may result in may result in hypoxichypoxic--ischemic ischemic encephalopathy and even death.encephalopathy and even death.
�� A study of outcomes from 6,238 cases of A study of outcomes from 6,238 cases of shoulder dystocia found that shoulder dystocia found that asphyxiaasphyxia was was more common among births complicated more common among births complicated by shoulder dystocia regardless of by shoulder dystocia regardless of maternal diabetic status.maternal diabetic status.
1010
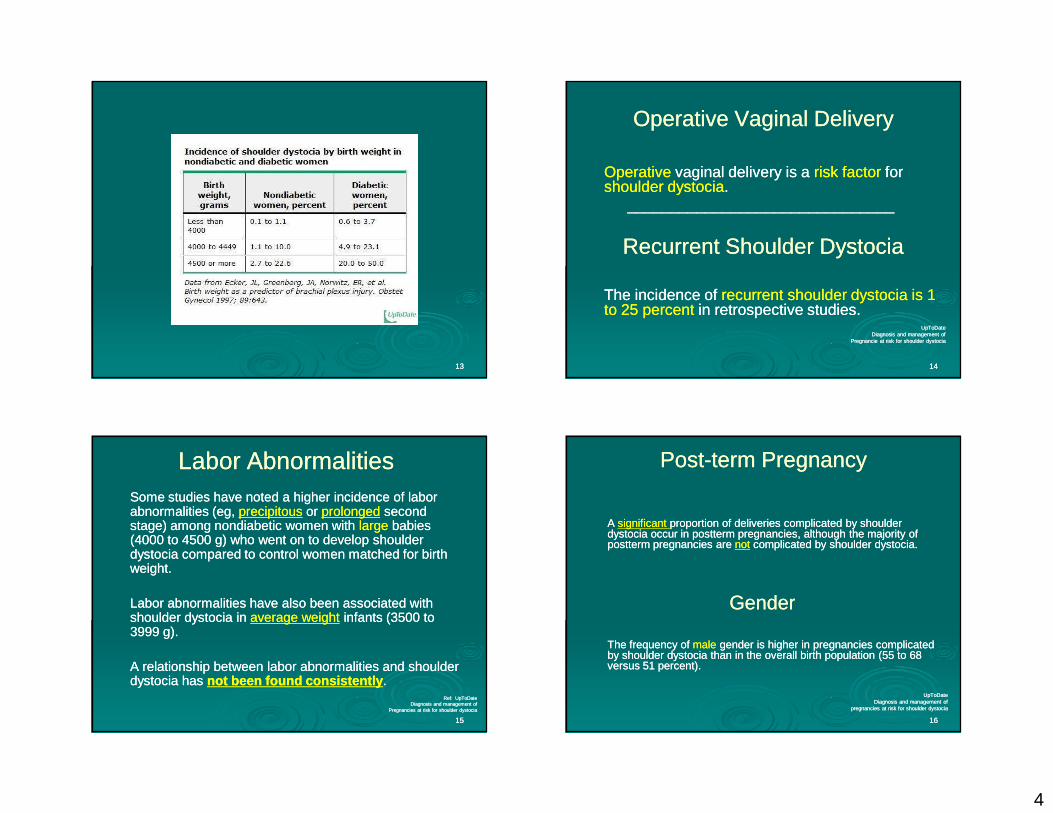
Fetal MacrosomiaFetal Macrosomia
�� ACOGACOG --Greater than Greater than 40004000 gramsgrams
�� Studies have consistently shown that Studies have consistently shown that macrosomiamacrosomia is a major risk factor is a major risk factor for shoulder dystocia for shoulder dystocia
��
�� Defined as an estimate fetal weight of greater than or equal to Defined as an estimate fetal weight of greater than or equal to 4500 4500 gramsgrams, as morbidity and mortality increase above this level. , as morbidity and mortality increase above this level.
��
�� The overall prevalence of birth weight The overall prevalence of birth weight over 4000over 4000 grams in the general grams in the general obstetric population of the USA is 10% but falls to 1.5% for birth weight obstetric population of the USA is 10% but falls to 1.5% for birth weight over 4500 grams.over 4500 grams.
�� Macrosomia tends to be Macrosomia tends to be repetitiverepetitive. . UpToDateUpToDate
Diagnosis and management of Diagnosis and management of Pregnancies at risk for shoulder dystocia Pregnancies at risk for shoulder dystocia
1111 1212
Diabetes MellitusDiabetes Mellitus
Higher incidenceHigher incidence of fetal macrosomia in pregnancies of fetal macrosomia in pregnancies complicated by precomplicated by pre--gestational and gestational gestational and gestational diabetes than in diabetes than in nonnon--diabeticdiabetic pregnancies. pregnancies.
There are also differences in the There are also differences in the anthropomorphicanthropomorphicmeasurements of infants of diabetic mothers (IDMs) measurements of infants of diabetic mothers (IDMs) compared to offspring of women without diabetes. compared to offspring of women without diabetes.
The The chestchest--toto--headhead and and shouldershoulder--toto--headhead ratios are ratios are increased in IDMs, thereby increasing the risk of increased in IDMs, thereby increasing the risk of shoulder dystocia independent of fetal weight shoulder dystocia independent of fetal weight
UpToDateUpToDateDiagnosis and management of Diagnosis and management of
Pregnancies at risk for shoulder dystociaPregnancies at risk for shoulder dystocia
4
1313 1414
Operative Vaginal DeliveryOperative Vaginal Delivery
OperativeOperative vaginal delivery is a vaginal delivery is a risk factorrisk factor for for shoulder dystociashoulder dystocia..
______________________________________________________________
Recurrent Shoulder DystociaRecurrent Shoulder Dystocia
The incidence of The incidence of recurrent shoulder dystocia is 1 recurrent shoulder dystocia is 1 to 25 percentto 25 percent in retrospective studies.in retrospective studies.
UpToDateUpToDateDiagnosis and management of Diagnosis and management of
Pregnancie at risk for shoulder dystociaPregnancie at risk for shoulder dystocia
1515
Labor AbnormalitiesLabor AbnormalitiesSome studies have noted a higher incidence of labor Some studies have noted a higher incidence of labor abnormalities (eg, abnormalities (eg, precipitousprecipitous or or prolongedprolonged second second stage) among nondiabetic women with stage) among nondiabetic women with largelarge babies babies (4000 to 4500 g) who went on to develop shoulder (4000 to 4500 g) who went on to develop shoulder dystocia compared to control women matched for birth dystocia compared to control women matched for birth weight.weight.
Labor abnormalities have also been associated with Labor abnormalities have also been associated with shoulder dystocia in shoulder dystocia in average weightaverage weight infants (3500 to infants (3500 to 3999 g).3999 g).
A relationship between labor abnormalities and shoulder A relationship between labor abnormalities and shoulder dystocia has dystocia has not been found consistentlynot been found consistently . .
Ref: UpToDateRef: UpToDateDiagnosis and management of Diagnosis and management of
Pregnancies at risk for shoulder dystociaPregnancies at risk for shoulder dystocia
1616
PostPost--term Pregnancy term Pregnancy
A A significant significant proportion of deliveries complicated by shoulder proportion of deliveries complicated by shoulder dystocia occur in postterm pregnancies, although the majority of dystocia occur in postterm pregnancies, although the majority of postterm pregnancies are postterm pregnancies are notnot complicated by shoulder dystocia.complicated by shoulder dystocia.
GenderGender
The frequency of The frequency of male male gender is higher in pregnancies complicated gender is higher in pregnancies complicated by shoulder dystocia than in the overall birth population (55 to 68 by shoulder dystocia than in the overall birth population (55 to 68 versus 51 percent).versus 51 percent).
UpToDateUpToDateDiagnosis and management of Diagnosis and management of
pregnancies at risk for shoulder dystociapregnancies at risk for shoulder dystocia

5
1717
Obesity and High Weight GainObesity and High Weight Gain
Some studies have reported that Some studies have reported that high maternal body mass indexhigh maternal body mass index((BMIBMI) and ) and excessive weight gainexcessive weight gain during pregnancy are during pregnancy are risk factorsrisk factorsfor shoulder dystocia.for shoulder dystocia.
Advanced Maternal AgeAdvanced Maternal Age
Advanced maternal age has been identified as a Advanced maternal age has been identified as a risk factorrisk factor for for shoulder dystocia.shoulder dystocia.
Confounding variables such as an Confounding variables such as an increasedincreased prevalence of prevalence of gestational diabetesgestational diabetes and and higher maternal weighthigher maternal weight probably account probably account for these associations.for these associations.
UpToDateUpToDateDiagnosis and management of pregnancies Diagnosis and management of pregnancies
at risk for shoulder dystociaat risk for shoulder dystocia
Management Management
�� Following delivery of the head, the umbilical cord is Following delivery of the head, the umbilical cord is compressedcompressed within the vagina, and fetal oxygenation within the vagina, and fetal oxygenation declines. declines.
�� Thus, reduction in the time from delivery of the head to Thus, reduction in the time from delivery of the head to delivery of the body is of great importance for survival.delivery of the body is of great importance for survival.
�� An initial An initial gentlegentle attempt at traction, assisted by maternal attempt at traction, assisted by maternal expulsive efforts, is recommended.expulsive efforts, is recommended.
�� Some clinicians have advocated performing a large Some clinicians have advocated performing a large episiotomy, and adequate analgesia is certainly ideal.episiotomy, and adequate analgesia is certainly ideal.
Williams Obstetrics23rd Edition
Shoulder DystociaShoulder Dystocia
www.brooksidepress.org
PULL PULL -- SaFESaFE
• Applied force was measured during each simulation.
• All participants managed the same scenario with an identical fetus and pelvic mannequin.
• There was enormous variation in the pattern and degree of traction.
• Two thirds pulled more than 100N, a level of force at which neonatal injury has been observed.
OBGYN, Vol 112, No 4October 2008
6
PULL PULL -- SaFESaFE
The wide range of applied force suggests a need for instruction in the use of “Minimal Traction.”
We demonstrated that those staff who received force perception training subsequently applied asignificantly lower total force during shoulderdystocia simulations when compared with thosewho did not receive the training.
OBGYN, Vol 112, No 4October 2008
PULL PULL -- SaFESaFE
Training must aim to instill the notion that
traction will not overcome the bony
obstruction of shoulder dystocia and that the recommended sequence of maneuvers
must be followed appropriately.
OBGYN, Vol 112, No 4October 2008
ManagementManagement
�� A variety of techniques can be used to A variety of techniques can be used to free the anterior shoulder from its free the anterior shoulder from its impacted position behind the symphsis impacted position behind the symphsis pubis:pubis:
�� Moderate suprapubicModerate suprapubic pressurepressure
�� McRobertsMcRoberts ManeuverManeuverOBGYN, Vol 112, No 4
October 2008
Definition of the Word: Definition of the Word: ModerateModerate
�� Definition: Definition: Calm, temperateCalm, temperate
�� Part of Speech: Part of Speech: AdjectiveAdjective
�� Synonyms: careful, cautious, Synonyms: careful, cautious, conservative, controlled, deliberate, mild, conservative, controlled, deliberate, mild, soft, steady, tame, soft, steady, tame,
www.thesarus.com
7
SupraSupra--Pubic Pressure Pubic Pressure
www.brooksidepress.org
Shoulder DystociaShoulder Dystocia
www.brooksidepress.org
McRoberts ManeuverMcRoberts Maneuver
The The McRobertsMcRoberts Maneuver consists of removing Maneuver consists of removing the legs from the stirrups and sharply flexing the legs from the stirrups and sharply flexing them up on to the abdomen.them up on to the abdomen.
Hyper flexion and abduction of the hips causing Hyper flexion and abduction of the hips causing cephalad rotation of the symphysis pubis and cephalad rotation of the symphysis pubis and flattening of the lumbar lordosis that frees the flattening of the lumbar lordosis that frees the impacted shoulder.impacted shoulder.
Williams Obstetrics23rd Edition
2828
McRoberts ManeuverMcRoberts Maneuver
Ref: www.brooksidepress.org

8
ManagementManagement
�� Rotational Maneuvers Rotational Maneuvers -- Woods Corkscrew Maneuver Woods Corkscrew Maneuver (Anterior aspect of the posterior shoulder)(Anterior aspect of the posterior shoulder)
Posterior Rubin IIPosterior Rubin IIPosterior aspect of the posterior shoulder Posterior aspect of the posterior shoulder
Anterior Rubin IIAnterior Rubin IIPosterior aspect of the anterior shoulder Posterior aspect of the anterior shoulder
�� Delivery of the Posterior Arm/ShoulderDelivery of the Posterior Arm/Shoulder
Posterior Rubin IIAnterior Rubin II
Woods ManeuverWoods Maneuver
The hand is placed behind the The hand is placed behind the posteriorposteriorshoulder of the fetus. The shoulder is then shoulder of the fetus. The shoulder is then rotated progressively 180 degrees in a rotated progressively 180 degrees in a corkscrewcorkscrew manner so that the impacted manner so that the impacted anterior shoulder is released.anterior shoulder is released.
Williams Obstetrics23rd Edition
Woods ManeuverWoods Maneuver
Williams Obstetrics23rd Edition

9
Delivery of the Posterior Delivery of the Posterior Shoulder/ArmShoulder/Arm
Williams Obstetrics23rd Edition
Delivery of the Posterior Delivery of the Posterior Shoulder/ArmShoulder/Arm
Grasp hand, flex elbow and deliver arm by traction on Grasp hand, flex elbow and deliver arm by traction on hand.hand.
Williams Obstetrics23rd Edition
ManagementManagement
Deliberate Deliberate fracture of the clavicle by pressing the fracture of the clavicle by pressing the anterior clavicle against the pubic ramus can be anterior clavicle against the pubic ramus can be performed to free the shoulder impaction. performed to free the shoulder impaction. However, it is However, it is difficultdifficult to deliberately fracture the to deliberately fracture the clavicle of a large neonate. clavicle of a large neonate.
If successful, the fracture will heal rapidly and is If successful, the fracture will heal rapidly and is usually usually trivialtrivial compared with brachial nerve compared with brachial nerve injury, asphyxia or death. injury, asphyxia or death.
Williams Obstetrics23rd Edition
10
Across The PondAcross The Pond
3838
Lessons for Skills TrainingLessons for Skills Training
Observations from 450 Observations from 450 Shoulder Dystocia SimulationsShoulder Dystocia Simulations
From the Departments of Obstetrics and GynecologyFrom the Departments of Obstetrics and GynecologyTaunton and Somerset NHS TrustTaunton and Somerset NHS Trust
North Bristol NHS TrustNorth Bristol NHS TrustUnited KingdomUnited Kingdom
Current CommentaryCurrent Commentary-- Obstetrics and GynecologyObstetrics and GynecologyVol. 112, No 4, October 2008Vol. 112, No 4, October 2008
Authors: Joanna Crofts, BM, BS, Robert Fox, MB, Denise Ellis, RM, Authors: Joanna Crofts, BM, BS, Robert Fox, MB, Denise Ellis, RM, Catherine Winter, RM, Kim Hinshaw, RM and Timothy J. Draycott, MDCatherine Winter, RM, Kim Hinshaw, RM and Timothy J. Draycott, MD
3939
“At present, shoulder dystocia remains a relatively unpredictable and therefore largely unpreventable event.”
OBGYN, Vol 112, No 4October 2008
4040
SaFESaFE StudyStudy
The SaFE (Simulation and Firedrill Evaluation) Study was a trial commissioned by the Department of Health of England and Walesto investigate the effectiveness of multiprofessional obstetric emergency training.
The management of shoulder dystocia was one of the obstetric emergencies investigated.
During the SaFE Study, 450 simulated shoulder dystocia scenarios were video recorded and analyzed.
OBGYN, Vol 112, No 4October 2008

11
4141
SaFE StudySaFE StudyPre-training data revealed the following:
� 80 of 140 (57%) were unable to deliver the fetus
� Almost two thirds (85/134, 63%) failed to call for pediatric support
� 1 in 27 (5/134, 4%) used a potentially harmful maneuver (fundal pressure).
OBGYN, Vol 112, No 4October 2008
4242
Summary Training PointsSummary Training Points
OBGYN, Vol 112, No 4October 2008
SBAR
FIRST ?
4343
Communication ProblemsCommunication Problems
� Inadequate communication betweenthe obstetrician or midwife and the summoned assistant was observed during simulations.
� Senior doctors were least likely to communicate well (P.001), with only 7 of 22 (32%) stating the problem before training.
OBGYN, Vol 112, No 4October 2008
4444
Training MessageTraining Message
� Good communication with the mother during and after shoulder dystocia is likely to enhance cooperation and limit psychological and possibly medico-legalproblems.
� Training programs should consider the inclusion of patient–actors with mannequins to increase the fidelity of simulation exercises.
OBGYN, Vol 112, No 4October 2008

12
4545
Note KeepingNote Keeping
� “Documentation” should be comprehensiveand unambiguous.
� Note keeping can be aided by a reformatted sheet, but instruction in the key componentsand the importance of their documentation still should be given.
OBGYN, Vol 112, No 4October 2008
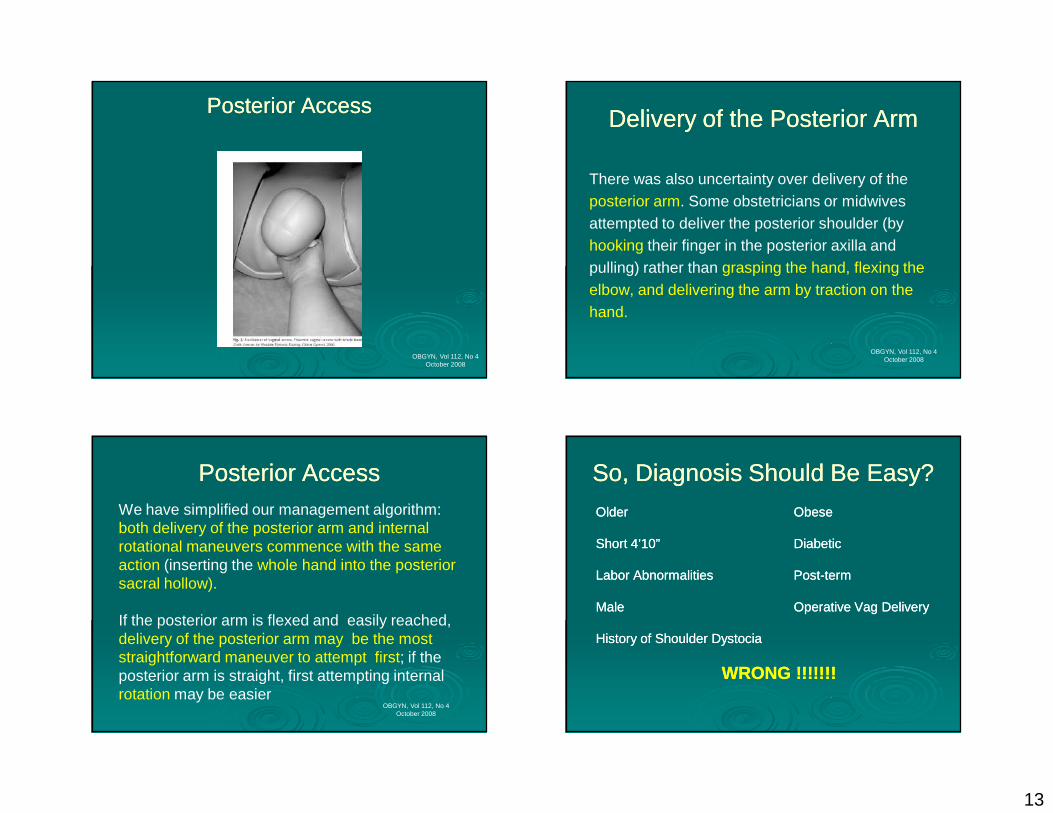
Description on How to Gain Access Description on How to Gain Access with the Examining Handwith the Examining Hand
The following descriptions to help obstetriciansor midwives understand how to gain access with the examining hand. We have likened the process to:
1. Performing a manual removal of a placenta
2. Putting on a tight bracelet
3. Removing the last potato chip in the tube!
OBGYN, Vol 112, No 4October 2008
Posterior AccessPosterior Access
OBGYN, Vol 112, No 4October 2008
Posterior AccessPosterior Access
OBGYN, Vol 112, No 4October 2008
13
Posterior AccessPosterior Access
OBGYN, Vol 112, No 4October 2008
Delivery of the Posterior ArmDelivery of the Posterior Arm
There was also uncertainty over delivery of the posterior arm. Some obstetricians or midwives attempted to deliver the posterior shoulder (by hooking their finger in the posterior axilla and pulling) rather than grasping the hand, flexing theelbow, and delivering the arm by traction on the hand.
OBGYN, Vol 112, No 4October 2008
Posterior AccessPosterior AccessWe have simplified our management algorithm: both delivery of the posterior arm and internal rotational maneuvers commence with the same action (inserting the whole hand into the posterior sacral hollow).
If the posterior arm is flexed and easily reached, delivery of the posterior arm may be the most straightforward maneuver to attempt first; if the posterior arm is straight, first attempting internal rotation may be easier
OBGYN, Vol 112, No 4October 2008
So, Diagnosis Should Be Easy?So, Diagnosis Should Be Easy?
OlderOlder ObeseObese
Short 4’10”Short 4’10” DiabeticDiabetic
Labor AbnormalitiesLabor Abnormalities PostPost--termterm
MaleMale Operative Vag DeliveryOperative Vag Delivery
History of Shoulder DystociaHistory of Shoulder Dystocia
WRONG !!!!!!!WRONG !!!!!!!

14
So, Delivery Should Be Easy and So, Delivery Should Be Easy and atraumatic if You Follow the Rules?atraumatic if You Follow the Rules?
Maybe?Maybe?
Evidence based?Evidence based?
The Real WorldThe Real World
5555
Summary of RecommendationsSummary of Recommendations
The following recommendations are based on The following recommendations are based on limited or inconsistent scientific evidence limited or inconsistent scientific evidence (Level B):(Level B):
�� Shoulder dystocia Shoulder dystocia cannot be predictedcannot be predicted or or preventedpreventedbecause because accurate accurate methods for identifying which fetuses methods for identifying which fetuses will experience this complication will experience this complication do not existdo not exist..
�� Elective inductionElective induction of laborof labor or or elective cesarean deliveryelective cesarean deliveryfor all women suspected of carrying a fetus with for all women suspected of carrying a fetus with macrosomia is macrosomia is not appropriatenot appropriate..
ACOG Practice Bulletin #40ACOG Practice Bulletin #40November 2002November 2002
5656
Summary of RecommendationsSummary of Recommendations
The following recommendations are based The following recommendations are based primarily on primarily on consensus and expert opinionconsensus and expert opinion::
In patients with a In patients with a historyhistory of shoulder dystocia, of shoulder dystocia, estimated estimated fetal weightfetal weight, gestational , gestational ageage, maternal , maternal glucoseglucose intolerance, and the severity of the prior intolerance, and the severity of the prior neonatal injury should be evaluated and the neonatal injury should be evaluated and the risks and benefits of cesarean deliveryrisks and benefits of cesarean deliverydiscussed with the patientdiscussed with the patient. .
ACOG Practice Bulletin #40ACOG Practice Bulletin #40November 2002November 2002
15
5757
Summary of RecommendationsSummary of Recommendations
Planned Planned cesarean deliverycesarean delivery to prevent to prevent shoulder dystociashoulder dystocia may be considered for may be considered for suspected fetal macrosomia with EFW suspected fetal macrosomia with EFW exceeding 5,000 gexceeding 5,000 g in women in women without without diabetesdiabetes and and 4,500 g4,500 g in women in women with with diabetes.diabetes.
ACOG Practice Bulletin #40ACOG Practice Bulletin #40November 2002November 2002
5858
Summary of RecommendationsSummary of Recommendations
There is There is no evidenceno evidence that any one maneuver is that any one maneuver is superiorsuperior to another in releasing an impacted to another in releasing an impacted shoulder or reducing the chance of injury. shoulder or reducing the chance of injury.
Performance of the Performance of the McRobertsMcRoberts maneuver is a maneuver is a reasonable initial approach.reasonable initial approach.
It is clear that brachial plexus injury can occur It is clear that brachial plexus injury can occur regardlessregardless of the procedure or procedures used of the procedure or procedures used to disimpact the shoulders.to disimpact the shoulders.
ACOG Practice Bulletin #40ACOG Practice Bulletin #40November 2002November 2002
Posterior AccessPosterior AccessWe have simplified our management algorithm: both delivery of the posterior arm and internal rotational maneuvers commence with the same action (inserting the whole hand into the posterior sacral hollow).
If the posterior arm is flexed and easily reached, delivery of the posterior arm may be the most straightforward maneuver to attempt first; if the posterior arm is straight, first attempting internal rotation may be easier
OBGYN, Vol 112, No 4October 2008
Summertown, Tennessee, USAThe Farm Midwives
A New (Old) Maneuver for the Management of Shoulder Dystocia
Anna L. Meenan, MD, Ina May Gaskin, MA, Pamela Hunt, and Charles A. Ball, MD
The inspiration for the use of the all-fours maneuver in this case, which was managed by the principal author, came from an informal article written by Ina May Gaskin on the results of a previously unpublished series of shoulder dystocias in which the maneuver had proven to be extremely effective.
www.thefarm.org
Evidence Based Practice ?
16
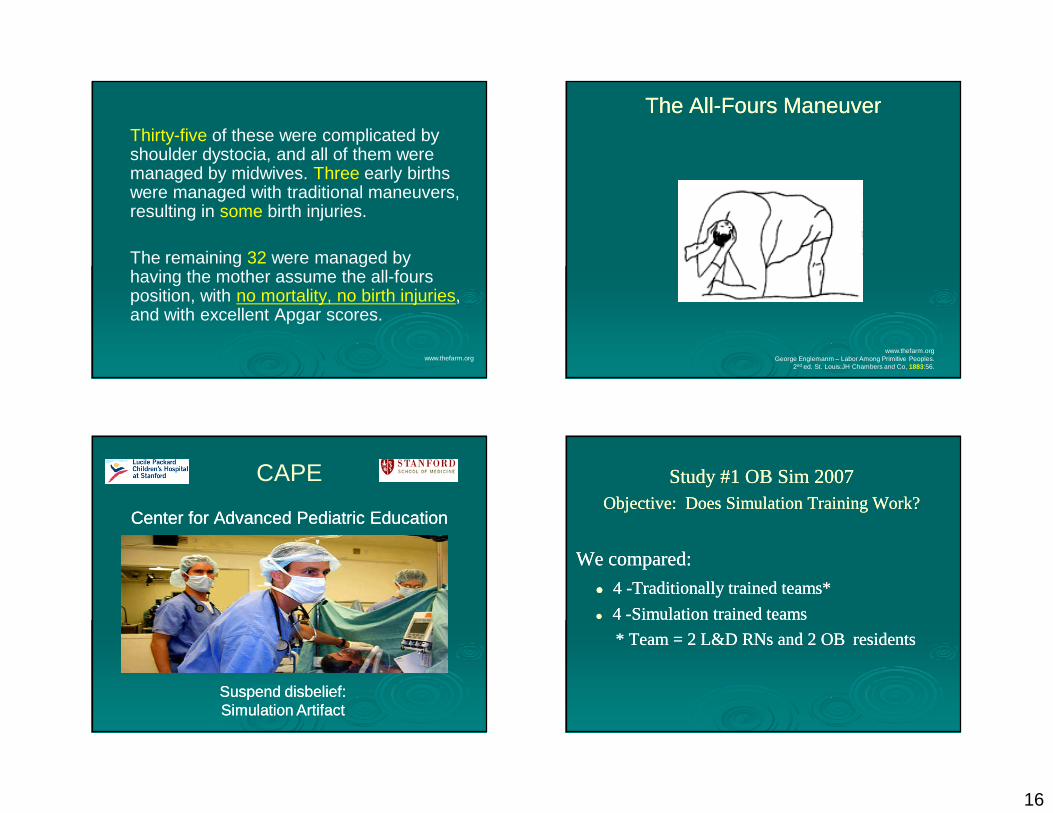
Thirty-five of these were complicated by shoulder dystocia, and all of them were managed by midwives. Three early births were managed with traditional maneuvers, resulting in some birth injuries.
The remaining 32 were managed by having the mother assume the all-fours position, with no mortality, no birth injuries, and with excellent Apgar scores.
www.thefarm.org
The AllThe All--Fours ManeuverFours Maneuver
www.thefarm.orgGeorge Englemanm – Labor Among Primitive Peoples.
2nd ed. St. Louis:JH Chambers and Co, 1883:56.
CAPE
Center for Advanced Pediatric EducationCenter for Advanced Pediatric Education
Suspend disbelief: Suspend disbelief: Simulation ArtifactSimulation Artifact
Study #1 OB Sim 2007Study #1 OB Sim 2007Objective: Does Simulation Training Work?Objective: Does Simulation Training Work?
We compared:We compared:
�� 4 4 --Traditionally trained teams*Traditionally trained teams*
�� 4 4 --Simulation trained teamsSimulation trained teams
* Team = 2 L&D RNs and 2 OB * Team = 2 L&D RNs and 2 OB residentsresidents

17
Simulation versus TraditionalSimulation versus Traditional
Training StudyTraining Study
2 obstetrical crises: 2 obstetrical crises:
•• Shoulder dystocia Shoulder dystocia
•• EclampsiaEclampsia
Traditional TrainingTraditional Training
Three hours of traditional training:Three hours of traditional training:
1). 1). Lectures2). Video2). Video3). Task Training3). Task Training
Simulation TrainingSimulation Training
No lectures/videosNo lectures/videos
�� Training in the simulator onlyTraining in the simulator only
Simulation RoomSimulation Room
�� 400 square feet400 square feet�� “Built to code”“Built to code”�� 6 pan tilt cameras6 pan tilt cameras�� Multiple microphonesMultiple microphones
18
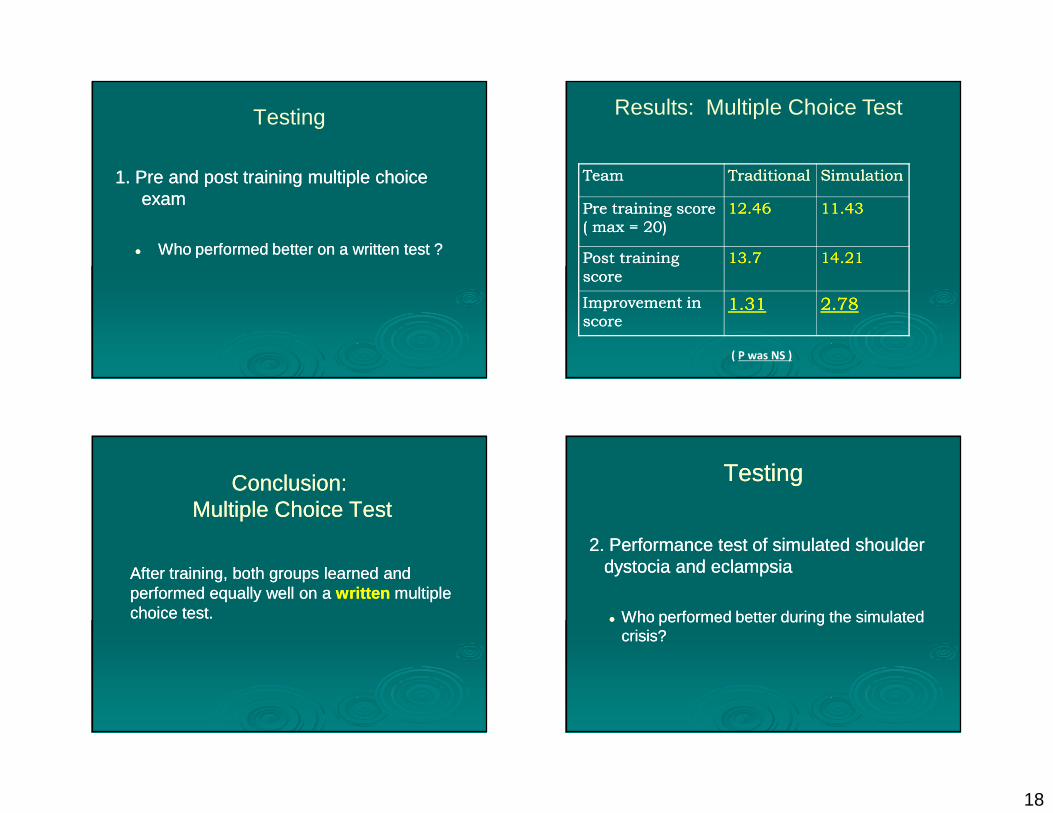
Testing
1. Pre and post training multiple choice 1. Pre and post training multiple choice examexam
�� Who performed better on a written test ?Who performed better on a written test ?
TeamTeam TraditionalTraditional SimulationSimulation
Pre training score Pre training score
( max = 20) ( max = 20)
12.4612.46 11.4311.43
Post training Post training
scorescore
13.713.7 14.2114.21
Improvement in Improvement in
scorescore1.311.31 2.782.78
( P was NS )
Results: Multiple Choice Test
After training, both groups learned and After training, both groups learned and performed equally well on a performed equally well on a writtenwritten multiple multiple choice test. choice test.
Conclusion:Conclusion:Multiple Choice TestMultiple Choice Test
2. Performance test of simulated shoulder 2. Performance test of simulated shoulder dystocia and eclampsiadystocia and eclampsia
�� Who performed better during the simulated Who performed better during the simulated crisis?crisis?
TestingTesting

19
�� Performance testing as L&D drillPerformance testing as L&D drill
•• All performance tests videotapedAll performance tests videotaped
•• Performance grading done by a Performance grading done by a “blinded” reviewer who was unaware “blinded” reviewer who was unaware of each teams’ mode of trainingof each teams’ mode of training
Performance Testing
(p=0.002)
Tech
nic
al S
core
(T
=1
4)
TeamTeam
Score Score (Total: (Total:
14)14) RangeRange
TraditionalTraditional 6.886.88 5.55.5--88
SimSim 11.7511.75 1010--1313
Performance Testing ResultsShoulder Dystocia
Simulation trained teamsSimulation trained teams demonstrated demonstrated superiorsuperior clinical skills as compared to clinical skills as compared to traditional trained teams. traditional trained teams.
Conclusion: Performance Testing Testimonial:Testimonial:
“On May 30th, I attended the OB Sim training “On May 30th, I attended the OB Sim training during which one of our scenarios was during which one of our scenarios was shoulder dystocia…the very next day at work shoulder dystocia…the very next day at work in L&D my exact same scenario would be in L&D my exact same scenario would be replicated! I took care of a patient…who replicated! I took care of a patient…who proceeded to have a three minute shoulder proceeded to have a three minute shoulder dystocia! dystocia!
I felt so much better equipped in my skills to I felt so much better equipped in my skills to handle this emergency situation as a result of handle this emergency situation as a result of my attendance at OB Sim. Communication my attendance at OB Sim. Communication among the team was very clear and the among the team was very clear and the emergency was handled very smoothly. emergency was handled very smoothly.
The outcome was very good (Apgars 7&9), I The outcome was very good (Apgars 7&9), I am convinced of the value and benefit of OB am convinced of the value and benefit of OB Sim validated by my own personal experience Sim validated by my own personal experience in the real L&D setting.” in the real L&D setting.”