short- and long-term antibiotic treatment reduces airway and systemic inflammation in non–cystic...
TRANSCRIPT

Short- and Long-Term Antibiotic Treatment ReducesAirway and Systemic Inflammation in Non–CysticFibrosis Bronchiectasis
James D. Chalmers1, Maeve P. Smith2, Brian J. McHugh1, Cathy Doherty3, John R. Govan3, andAdam T. Hill1,2
1The University of Edinburgh/Medical Research Council Centre for Inflammation Research, The Queen’s Medical Research Institute, Edinburgh,
United Kingdom; 2Department of Respiratory Medicine, Royal Infirmary of Edinburgh, Edinburgh, United Kingdom; and 3School of Medicine and
Veterinary Medicine, Cystic Fibrosis Group, Centre for Infectious Diseases, University of Edinburgh, Edinburgh, United Kingdom
Rationale: The vicious cycle hypothesis of bronchiectasis argues thatbacterial colonization leads to airway inflammation and progressivelungdamage.The logical extensionof this hypothesis is that acuteorchronic antibiotic therapy should improve airway inflammation andclinical outcome. There are little data to support this hypothesis inpatients with non–cystic fibrosis (CF) bronchiectasis.Objectives: To determinewhether acute or chronic antibiotic therapyimproves airway inflammation and clinical outcome in non-CF bron-chiectasis.Methods: The relationship between bacterial load and airway andsystemic inflammation was investigated in 385 stable patients, 15stable patients treatedwith intravenous antibiotics, and 34 patientswith an exacerbation of bronchiectasis treated with intravenousantibiotics. Long-term antibiotic therapy was investigated usingsamples from a 12-month controlled trial of nebulized gentamicin.Measurements and Main Results: In stable patients, there was a directrelationship between airway bacterial load and markers of airwayinflammation (P, 0.0001 for all analyses). Highbacterial loadswereassociated with higher serum intercellular adhesion molecule-1,E-selectin, and vascular cell adhesion molecule-1 (P , 0.05 abovebacterial load>13 107 cfu/ml). In stable patients, therewas a directrelationship between bacterial load and the risk of subsequentexacerbations (odds ratio, 1.20; 95% confidence interval, 1.11–1.29; P , 0.0001) and severe exacerbations (odds ratio, 1.11; 95%confidence interval, 1.01–1.21; P¼ 0.02). Short- and long-term anti-biotic treatments were associated with reductions in bacterial load,airways, and systemic inflammation.Conclusions: High airway bacterial loads in non-CF bronchiectasis areassociatedwith airway and systemic inflammation and a greater riskof exacerbations. Short- and long-term antibiotic therapy reducemarkers of airways and systemic inflammation.Clinical trial registeredwithwww.clinicaltrials.gov (NCT00749866).
Keywords: bronchiectasis; inflammation; cytokines; Pseudomonas;
bacteria
The vicious cycle hypothesis of bronchiectasis argues that bacterialcolonization of the normally sterile respiratory tract provokes andperpetuates airway inflammation (1). This neutrophil-mediatedinflammation leads to airway structural damage and further im-pairment of the mucociliary escalator leading to increased bacte-rial load (1–3). This cycle repeats continuously throughout thecourse of the disease leading to the clinical syndrome of cough,sputum production, and recurrent exacerbations that is charac-teristic of bronchiectasis (4). According to this hypothesis, if bac-teria are the primary drivers of airway inflammation, bacterialclearance through the use of short- or long-term antibiotic ther-apy would be expected to reduce airway inflammation, allowairway healing, and modify the long-term course of the disease.
There is strong evidence from cystic fibrosis (CF) bronchiec-tasis to support this view, with data suggesting that bacterial col-onization is associated with airway inflammation and thatantibiotic treatment during stability and at exacerbation canreduce markers of inflammation (5–7). Extrapolation from CFto non-CF bronchiectasis is difficult because the pathophysiol-ogy is different and the failure of recombinant DNase treatmentto provide benefit in non-CF bronchiectasis demonstrates thatresponses to treatment can be very different in CF comparedwith non-CF bronchiectasis (8). The evidence base in non-CFbronchiectasis is limited, although a study of 49 patients withstable bronchiectasis using bronchoalveolar lavage demon-strated a link between bacterial load and airway inflammation,as did a study of patients with chronic obstructive pulmonarydisease that included 43 with bronchiectasis (9, 10). Raised sys-temic inflammation has been shown to be associated with disease
(Received in original form March 16, 2012; accepted in final form June 19, 2012)
Supported by the Medical Research Council, United Kingdom, and the Chief
Scientists Office, Scotland, United Kingdom.
Author Contributions: All authors participated in study design, data analysis, and
interpretation of the data. All authors were involved in writing and revising the
article before submission.
Correspondence and requests for reprints should be addressed to James D.
Chalmers, M.B.Ch.B., Royal Infirmary of Edinburgh, Department of Respiratory
Medicine, Edinburgh, United Kingdom. E-mail: jamesdchalmers@googlemail.
com
This article has an online supplement, which is accessible from this issue’s table of
contents at www.atsjournals.org
Am J Respir Crit Care Med Vol 186, Iss. 7, pp 657–665, Oct 1, 2012
Copyright ª 2012 by the American Thoracic Society
Originally Published in Press as DOI: 10.1164/rccm.201203-0487OC on June 28, 2012
Internet address: www.atsjournals.org
AT A GLANCE COMMENTARY
Scientific Knowledge on the Subject
Bronchiectasis is frequently associated with bacterial colo-nization, but the relationship between bacterial colonizationand airway and systemic inflammation is unclear. Whetherantibiotic therapy modifies inflammation is also unclear.
What This Study Adds to the Field
There is a direct relationship between airway bacterial loadand airway and systemic inflammation, exacerbations, andhealth-related quality of life in stable patients with bron-chiectasis. Airway and systemic inflammation can be re-duced with short- and long-term antibiotic therapy. Thisstudy highlights the importance of monitoring sputumbacteriology when clinically stable and provides a basis forfuture intervention studies to reduce bacterial burden in theairways.

severity and lung function impairment in 87 stable patients withbronchiectasis (11).
There are limited studies evaluating the effect of bacterialclearance in non-CF bronchiectasis. A 2007 Cochrane reviewof randomized controlled trials of antibiotic therapy in non-CF bronchiectasis suggested no benefit in terms of lung functionor exacerbation frequency (12). In addition, some studies sug-gest that antibiotic therapy in bronchiectasis had little or noeffect on markers of airway inflammation, further questioningthe hypothesis that antibiotics can “break the cycle” (12, 13).Conversely, three studies of long-term antibiotics have demon-strated reduced levels of myeloperoxidase (MPO) and neutrophilelastase activity in sputum after prolonged antibiotic treatment(14–16).
The aim of this study was to determine if bacterial load wasassociated with markers of airways and systemic inflammation inpatients with bronchiectasis, and to determine if antibiotic ther-apy during stability and during acute exacerbations impacted onthis. Finally, we aimed to determine the association of bacterialload with key clinical markers of severity in bronchiectasis,including exacerbation frequency and health-related quality oflife. Some of the results of this study have been previouslyreported in the form of an abstract (17).
METHODS
Consecutive adult patients with non-CF bronchiectasis confirmed byhigh-resolution chest computed tomography scan were recruited froma regional specialist clinic based at the Royal Infirmary of Edinburgh,Edinburgh, United Kingdom (2007–2011). The study was approved bythe South East Scotland Research Ethics Committee and all partici-pants gave written informed consent.
Exclusion criteria were as follows: age less than 18 years; poorly con-trolled asthma; active allergic bronchopulmonary aspergillosis; currentsmoking (within 2 yr); CF; active mycobacterial disease; HIV; long-termoral or nebulized antibiotic therapy before the study; or long-term oralcorticosteroid therapy.
Study Design
This study is composed of four components, each described next withfurther details in the online supplement. Study 1 examined the relation-ship between bacterial load and airway and systemic inflammation duringclinical stability. A total of 385 stable patients with non-CF bronchiectasiswere recruited. Clinically, stability was determined by a respiratory phy-sician on the day of recruitment and all patients were free from antibiotictherapy for more than 4 weeks. Patients were taught to provide appro-priate samples under supervision of a specialist nurse. Spontaneousearly morning sputum was collected at each study visit for qualitativeand quantitative bacteriology and assessment of airways inflamma-tion. Paired serum samples were collected for assessment of systemicinflammation.
Bacteriology
Samples containing less than 10 squamous cells and more than 25 leu-kocytes per low-power microscope field were acceptable. Sputum wasseparated from saliva and the sample split for bacteriology and assess-ment of airway inflammation. Samples were processed for quantitativeand qualitative bacteriology as previously described (14).
Airway Inflammation
Unprocessed sputumwas ultracentrifuged at 50,0003 g for 90 minutes at48C. The sol phase was removed and frozen at 2708C (14). MPO andneutrophil elastase activity were measured as described (14). IL-8, tumornecrosis factor (TNF)-a, and IL-1b were measured by commerciallyavailable ELISA (R&D Systems, Abingdon, UK) using kits that hadbeen validated for sputum use according to established methodology(18).
Systemic Inflammation
It has been reported that bronchiectasis and other inflammatory lungdiseases are associated with systemic elevation of adhesion moleculesinvolved in leukocyte recruitment to the inflamed lung (11, 19–21).To determine if bacterial load correlates with these markers, solubleintercellular adhesion molecule-1 (ICAM-1), soluble E-selectin, andsoluble vascular cell adhesion molecule-1 (VCAM-1) were measuredin serum using commercially available ELISA kits (R&D Systems).C-reactive protein and erythrocyte sedimentation rate were also mea-sured as systemic inflammatory markers.
Clinical Assessments
Patients were clinically assessed and managed using a protocol based onthe British Thoracic Society guidelines for non-CF bronchiectasis (4).The underlying cause of bronchiectasis was assigned after standardtesting recommended by the British Thoracic Society guidelines (4).All stable patients had 6 monthly assessments and underwent spirom-etry (22) and completed the St. Georges Respiratory Questionnaire(23) and the Leicester Cough Questionnaire (24). The minimal impor-tant clinical difference is 4 Units and 1.3 Units, respectively, for thesequestionnaires. Severity of bronchiectasis on CT scanning was assessedusing a modified Reiff score (25). Patients were followed-up for 1 year.Patient-reported exacerbations were recorded and verified against elec-tronic prescription records for antibiotics. Unscheduled hospital visitswere confirmed using electronic medical records that record all hospitalvisits (emergency department, inpatient, and outpatient visits) region-ally. Severe exacerbations were defined as unscheduled hospital admis-sions or emergency department visits for exacerbation of bronchiectasis.
Study 2 examined the effect of long-term antibiotic therapy usingnebulized gentamicin for 12 months on markers of airway and systemicinflammation. We used samples from a randomized controlled trial ofnebulized gentamicin (n ¼ 57). Details of this randomized controlledtrial have been described previously (14). Microbiology and assess-ments of airway and systemic inflammation were performed at enrol-ment; 12 months (end of antibiotic treatment); and 15 months (3 mopost end of antibiotic treatment).
Study 3 examined the effect of bacterial clearance using 14 days in-travenous antibiotic therapy on markers of airway and systemic inflam-mation in stable patients. Fifteen patients with a bacterial load ofgreater than or equal to 1 3 107 cfu/ml when stable were treated withintravenous antibiotic therapy for 14 days.
Study 4 recruited 34 patients with severe exacerbations of non-CFbronchiectasis requiring intravenous antibiotic therapy (defined accord-ing to British Thoracic Society guideline definitions) (4). Patients weretreated with intravenous antibiotic therapy based on their previousmicrobiology results. Sputum and serum samples were taken for bac-teriology and assessment of airway and systemic inflammation at startof treatment and after 14 days of therapy.
Control Groups
As a control group for Studies 3 and 4, these patients were matched to11 stable patients who gave sputum and serum samples 2 weeks aparthaving received no antibiotic therapy. Serum samples from 100 controlsubjects (matched for age and sex) without a history of respiratory dis-ease were also assayed for ICAM-1, soluble E-selectin, and VCAM-1.
Statistical Analysis
The chi-square test and unpaired t test and Mann Whitney U test wereused for comparison of categorical and numerical data, respectively.For comparisons of more than two groups, one-way analysis of varianceor the Kruskal-Wallis test were used as appropriate. Multivariablelogistic regression adjusting for confounders was used to determinethe relationship between inflammatory markers and chronic coloniza-tion, and the relationship between bacterial load and exacerbations.Details of models are described in the online supplement. P less than0.05 was considered statistically significant.
RESULTS
The study included a final cohort of 385 patients. Median agewas 67 years, interquartile range 56–74, and 42.9% of the study
658 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 186 2012

cohort was male. A total of 81.6% of patients had idiopathic/postinfective bronchiectasis in the stable cohort. The othercauses of bronchiectasis were previous allergic bronchopulmo-nary aspergillosis (n ¼ 36); rheumatoid arthritis (n ¼ 19); in-flammatory bowel disease (n ¼ 13); and one patient each witha1-antitrypsin deficiency, yellow nail syndrome, and Kartagenersyndrome. A total of 40.3% of the population was using inhaledcorticosteroids. The demographics of the study population areshown in Table 1.
Relationship between Airway Bacterial Load
and Airway Inflammation
Pathogenic microorganisms were isolated in the baseline sputumcultures from 75.3% of patients. Of those with positive cultures,predominant organisms isolated were Haemophilus influenzae(38.6%); Pseudomonas aeruginosa (21%); Staphylococcus au-reus (12.4%); Moraxella catarrhalis (11.4%); Streptococcuspneumoniae (9.7%); and others (primarily enteric gram-negativeorganism, 9.3%). Total numbers add up to greater than the totalnumber of patients because some patients grew more than oneorganism.
Bacterial load was strongly associatedwith each of themarkersof airway inflammation measured in sputum (Figure 1). Com-pared with the 22.1% of patients that grew no potentially path-ogenic microorganisms (PPMs), statistically significantly higherlevels of inflammatory markers were found at 105 cfu/ml. Themedian levels of each of the five markers increased progressivelywith increasingly bacterial load. Analyses adjusting for inhaledcorticosteroid use found the same results (see online supple-ment). The same results were observed when examining patientswith idiopathic and postinfective bronchiectasis and other causes(see online supplement).
Relationship between Airway Bacterial Load
and Systemic Inflammation
Analysis of soluble adhesion molecules in serum showed ele-vated levels of ICAM-1, E-selectin, and VCAM-1 in patientsgrowing 1 3 107 cfu/ml or more compared with the group withno PPMs (Figure 2). Differences between bacterial loads of 1 3105 and 1 3 106 cfu/ml with the no-PPM group were notstatistically significant (P . 0.05).
When compared with the healthy control population, overallpatients with bronchiectasis had higher levels of ICAM-1(171 ng/ml [interquartile range 114.2–296.2] in control subjectsvs. 270.2 ng/ml [168.7–459] in patients with bronchiectasis;
P , 0.0001), whereas less striking differences in E-selectin(56.8 ng/ml [36.4–80.9] in control subjects vs. 64.9 ng/ml [43.7–94.6] in patients with bronchiectasis; P ¼ 0.02) were observedand the levels of VCAM-1 (582 ng/ml [456–924.1] in controlsubjects vs. 686.6 [527.8–921.4]; P ¼ 0.07) were not significantlydifferent between patients with bronchiectasis and controlsubjects.
The Impact of 14-Day Antibiotic Therapy on Markers
of Airway Inflammation and Systemic Inflammation
plus Exacerbations
For stable patients, 15 were treated with intravenous antibioticsfor 14 days and 11 received no therapy for 14 days. Sputum andserum markers were then compared between these two groups.At baseline, all patients had sputum cultures that grew PPMs at1 3 107 cfu/ml or greater (bacteriology of the 26 patients in-cluded in this study are shown in the online supplement). After14 days of intravenous antibiotic therapy, all patients had nosignificant bacterial growth in sputum. In contrast, in the controlgroup that received no antibiotic therapy, there was no reductionin the bacterial load (baseline mean, 3.23 108 vs. 2.13 108 cfu/mlat Day 14; P ¼ 0.4).
Bacterial clearance through 14 days antibiotic therapy was as-sociated with a significant reduction in all of the markers of air-way inflammation measured (Figure 3). In addition, antibiotictreatment was associated with a statistically significant reduc-tion in ICAM-1 concentration in serum and E-selectin alsodecreased with treatment (76.7 ng/ml, 61.7–91.8 ng/ml pretreat-ment vs. 53.3 ng/ml, 44.6–68.8 ng/ml post-treatment; P ¼ 0.04).Although VCAM-1 serum levels decreased with treatment(782 ng/ml, 302.2–1,001 ng/ml pretreatment vs. 387.1, 121.3–919.7 post-treatment) this difference was not statistically signif-icant (P ¼ 0.4). There were no significant differences in patientsreceiving no treatment for any markers between Days 0 and 14.
For patients with acute exacerbations of bronchiectasis (n¼ 34),all patients had a significant growth of pathogens at baseline. Themost frequent pathogens wereH. influenzae (11 patients); S. pneu-moniae (nine patients); P. aeruginosa (eight patients); S. aureus(three patients); M. catarrhalis (two patients); and gram-negativeEnterobacteriaceae (four patients) (numbers add up to more than34 because three patients grew more than one pathogen). At Day14, only four patients still had a significant growth of bacteria (allP. aeruginosa). The data demonstrated a significant reduction inall markers of airway inflammation (P , 0.0001 for all compar-isons) (Figure 3) and ICAM-1 (P , 0.05) after 14 days antibiotic
TABLE 1. BASELINE CHARACTERISTICS OF THE STUDY POPULATION
Cohort N Age
Gender,
% Male FEV1% Predicted FVC% Predicted
Radiological
Severity
Score Body Mass Index
% Idiopathic/
Postinfective
Bronchiectasis
Study 1
Stable cohort 385 67 (56–74) 42.9 69.2 (51–91.1) 81 (67.4–101) 4 (2–5) 25.9 (22.4–29.6) 81.6
Study 2
Nebulized gentamicin group 27 58 (53–67) 33.3 72.9 (60–81.2) 88.9 (82.7–94) 9 (4–12) 25.4 (20.9–29) 71.3
Nebulized 0.9% saline group 30 64 (56–69) 50 63.4 (45.5–80.4) 85 (71.1–94.4) 6 (3–12) 27.1 (24.1–29.5) 66.7
Study 3
Stable patients intravenous
antibiotics (14 d)
15 66 (55–70) 53.3 61.3 (36–77.1) 73.5 (60–97) 9 (4–12) 25 (20.8–26.9) 66.7
Stable patients (no
treatment for 14 d)
11 61 (48–70) 54.5 62.3 (39.5–75.3) 81.3 (57.6–90.1) 8 (3–12) 25.3 (20.3–28.2) 63.6
Study 4
Acute exacerbation of
bronchiectasis–intravenous
antibiotics (14 d)
34 66 (54–71) 52.9 61.4 (39.5–81.8) 77.4 (60.3–95.9) 9 (3–12) 24.8 (22.1–27.7) 79.4
All patients in Studies 2–4 were also included in Study 1.
Chalmers, Smith, McHugh, et al.: Antibiotic Treatment Reduces Inflammation in Bronchiectasis 659

therapy in patients with exacerbations of bronchiectasis (Figure 3).Differences in serum E-selectin and VCAM-1 were not statisti-cally significant (P ¼ 0.1 and P ¼ 0.3, respectively).
The Impact of 12-Month Nebulized Gentamicin on Markers
of Airway and Systemic Inflammation
The organisms isolated in the patients treated with nebulizedgentamicin and nebulized 0.9% saline in this study have beenreported previously (14). In addition, it has been previouslyreported that nebulized gentamicin resulted in a statisticallysignificant reduction in MPO activity and neutrophil elastase
activity in the treatment group, which was not evident in thesaline group (14). Results are therefore only presented for spu-tum IL-8, TNF-a, IL-1b, and the soluble adhesion molecules inserum. Nebulized gentamicin resulted in significant reduction insputum IL-8, TNF-a, and IL-1b compared with patients treatedwith saline. For the soluble adhesion molecules, reductions wereevidence in ICAM-1 compared with baseline and the saline-treated groups at 12 months. E-selectin was significantly differ-ent from baseline in the gentamicin group but did not differcompared with the saline group. No differences were evidentin the levels of VCAM-1 at any stage in the study. These dataare shown in Table 2.
Figure 1. The relationship between bacterial load when stable and markers of airway inflammation in sputum. Data are presented as median (boxes)
with interquartile range (bars). *P , 0.05, **P , 0.001, ***P , 0.0001. All display comparisons are Mann-Whitney U test compared with patients
growing no potentially pathogenic microorganisms. Comparison across multiple groups (Kruskal-Wallis test) showed a direct relationship betweenairway bacterial load and airway inflammation (P , 0.0001 for all markers). TNF ¼ tumor necrosis factor.
Figure 2. The relationship between bacterial load when stable and markers of systemic inflammation in serum. Data are presented as median (boxes)
with interquartile range (bars). *P , 0.05, **P , 0.001, ***P , 0.0001. All display comparisons are Mann-Whitney U test compared with patients
growing no potentially pathogenic microorganisms. Comparison across multiple groups (Kruskal-Wallis test) showed a direct relationship betweenairway bacterial load and systemic inflammation (P ¼ 0.003 for intercellular adhesion molecule [ICAM]-1, P ¼ 0.001 for E-selectin, and P ¼ 0.0007
for vascular cell adhesion molecule [VCAM]-1).
660 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 186 2012

Pseudomonas aeruginosa and Radiologic Severity of
Bronchiectasis Influence Airway Inflammation
Pseudomonas aeruginosa. Pseudomonas aeruginosa was associ-ated with increased airway inflammation independent of thebacterial load compared with isolation of other pathogens.Patients with P. aeruginosa were each matched by log bacterialload and radiologic severity (6 1) to patients that had isolatedother PPMs (n ¼ 81 and 162, respectively). The median bacte-rial load was 4.43 107 versus 4.63 107 cfu/ml (P ¼ 0.3). Medianradiologic severity was 8 (4–12) versus 7 (4–12), with P equalto 0.8.
Patients isolating P. aeruginosa had higher levels of MPOactivity (13.5 U/ml [4–38.6] vs. 2.6 [0.6–50.8]; P , 0.0001); elas-tase activity (4.9 [1.2–68] vs. 1.2 mg/ml [0.4–147.2]; P , 0.0001);IL-8 (52.2 [34–64.5] vs. 39.5 ng/ml [30–49.7]; P ¼ 0.001); andTNF-a (2,722 [971.2–5,098] vs. 1,024 pg/ml [277–2,529]; P ,
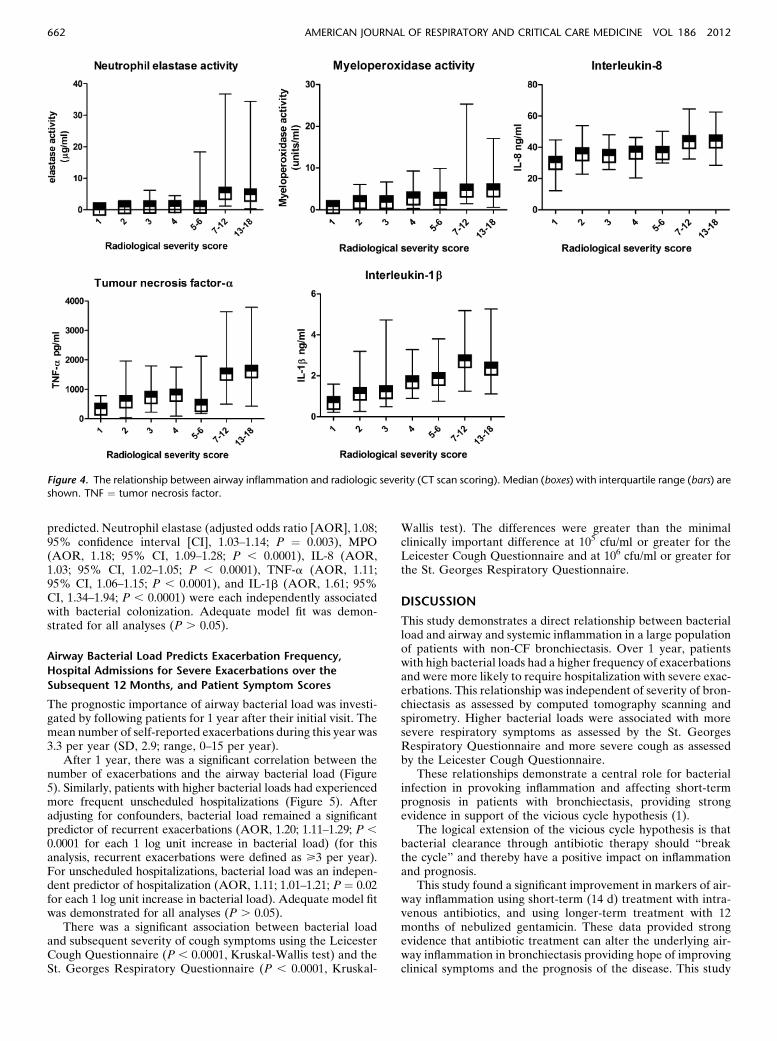
0.0001). The difference between the two groups in levels of IL-1b (2.8 [0.9–5.8] vs. 2.3 ng/ml [1.3–4.9]; P ¼ 0.8) was not statisti-cally significant.Radiologic severity. There was a direct relationship between
increasing radiologic severity and severity of airway inflamma-tion (P , 0.0001 for sputum elastase, MPO, TNF-a, and IL-1b; P ¼ 0.001 for IL-8) (Figure 4).
Independent Relationship between Airway Inflammation
and Bacterial Colonization
In addition to bacterial colonization, airway inflammation wascorrelated to some extent with the degree of lung functionimpairment (see online supplement).
A multivariable logistic regression analysis was performed todetermine if airway inflammation was associated with a positivebacterial culture, independent of radiologic severity and FEV1%
Figure 3. Response of markers of airway and systemic inflammation to 14 days of intravenous (IV) antibiotics. *P , 0.05 when compared with the
Day 0 values. All other comparisons P . 0.05. Box plots show median with interquartile range with the whiskers representing the minimum and
maximum values. ICAM ¼ intercellular adhesion molecule; MPO ¼ myeloperoxidase; TNF ¼ tumor necrosis factor.
TABLE 2. THE IMPACT OF NEBULIZED GENTAMICIN TREATMENT ON MARKERS OF AIRWAY AND SYSTEMIC INFLAMMATION
Gentamicin (n ¼ 27) Saline (n ¼ 30)
Time Point, mo: 0 12
15 (3 mo after
Treatment) 0 12
15 (3 mo after
Treatment)
IL-8, ng/ml 38.4 (34.8–44.1) 33.2 (25–37.5)*† 36.4 (33.4–42.8)† 39.1 (37.8–46.8) 42.9 (36.1–48.5) 42.5 (39.9–50.1)
TNF-a, pg/ml 1,346 (485.1–3,581) 485.4 (115.1–1,286)*† 1,028 (600.1–3,920) 1,281 (374.9–2,874) 1,421 (290–3,074) 1,295 (409.6–4,246)
IL-1b, ng/ml 2.2 (0.96–4) 0.99 (0.46–2.2)*† 2.2 (0.90–3.7) 2.1 (0.59–3.4) 2 (0.68–3) 2.4 (1.1–3.4)
ICAM-1, ng/ml 304.7 (190.9–463.8) 245.3 (167.4–359.4)*† 299.2 (245.9–436.9) 278.8 (163.2–459.7) 318.7 (177–458.3) 299.4 (174–444.9)
E-selectin, ng/ml 72.7 (50.7–91.7) 54.4 (36.5–77.1)* 67.4 (41.4–81.8) 65.6 (45.1–80.1) 63.1 (47.2–80.8) 61.5 (40.7–80.2)
VCAM-1, ng/ml 671.2 (473.4–869) 591.5 (362.7–836.6) 712 (378.3–891) 671.6 (399.1–878.7) 642 (447.1–862) 643.8 (391.6–894.1)
% Positive microbiology 100% 33.3%*† 66.7% 100% 96.7% 96.7%
Definition of abbreviations: ICAM ¼ intercellular adhesion molecule; TNF ¼ tumor necrosis factor; VCAM ¼ vascular cell adhesion molecule.
* P , 0.05 when compared with baseline (time point 0).y P , 0.05 when compared with the same time point in the saline-treated group.
Chalmers, Smith, McHugh, et al.: Antibiotic Treatment Reduces Inflammation in Bronchiectasis 661
predicted. Neutrophil elastase (adjusted odds ratio [AOR], 1.08;95% confidence interval [CI], 1.03–1.14; P ¼ 0.003), MPO(AOR, 1.18; 95% CI, 1.09–1.28; P , 0.0001), IL-8 (AOR,1.03; 95% CI, 1.02–1.05; P , 0.0001), TNF-a (AOR, 1.11;95% CI, 1.06–1.15; P , 0.0001), and IL-1b (AOR, 1.61; 95%CI, 1.34–1.94; P , 0.0001) were each independently associatedwith bacterial colonization. Adequate model fit was demon-strated for all analyses (P . 0.05).
Airway Bacterial Load Predicts Exacerbation Frequency,
Hospital Admissions for Severe Exacerbations over the
Subsequent 12 Months, and Patient Symptom Scores
The prognostic importance of airway bacterial load was investi-gated by following patients for 1 year after their initial visit. Themean number of self-reported exacerbations during this year was3.3 per year (SD, 2.9; range, 0–15 per year).
After 1 year, there was a significant correlation between thenumber of exacerbations and the airway bacterial load (Figure5). Similarly, patients with higher bacterial loads had experiencedmore frequent unscheduled hospitalizations (Figure 5). Afteradjusting for confounders, bacterial load remained a significantpredictor of recurrent exacerbations (AOR, 1.20; 1.11–1.29; P ,0.0001 for each 1 log unit increase in bacterial load) (for thisanalysis, recurrent exacerbations were defined as >3 per year).For unscheduled hospitalizations, bacterial load was an indepen-dent predictor of hospitalization (AOR, 1.11; 1.01–1.21; P ¼ 0.02for each 1 log unit increase in bacterial load). Adequate model fitwas demonstrated for all analyses (P . 0.05).
There was a significant association between bacterial loadand subsequent severity of cough symptoms using the LeicesterCough Questionnaire (P , 0.0001, Kruskal-Wallis test) and theSt. Georges Respiratory Questionnaire (P , 0.0001, Kruskal-
Wallis test). The differences were greater than the minimalclinically important difference at 105 cfu/ml or greater for theLeicester Cough Questionnaire and at 106 cfu/ml or greater forthe St. Georges Respiratory Questionnaire.
DISCUSSION
This study demonstrates a direct relationship between bacterialload and airway and systemic inflammation in a large populationof patients with non-CF bronchiectasis. Over 1 year, patientswith high bacterial loads had a higher frequency of exacerbationsand were more likely to require hospitalization with severe exac-erbations. This relationship was independent of severity of bron-chiectasis as assessed by computed tomography scanning andspirometry. Higher bacterial loads were associated with moresevere respiratory symptoms as assessed by the St. GeorgesRespiratory Questionnaire and more severe cough as assessedby the Leicester Cough Questionnaire.
These relationships demonstrate a central role for bacterialinfection in provoking inflammation and affecting short-termprognosis in patients with bronchiectasis, providing strongevidence in support of the vicious cycle hypothesis (1).
The logical extension of the vicious cycle hypothesis is thatbacterial clearance through antibiotic therapy should “breakthe cycle” and thereby have a positive impact on inflammationand prognosis.
This study found a significant improvement in markers of air-way inflammation using short-term (14 d) treatment with intra-venous antibiotics, and using longer-term treatment with 12months of nebulized gentamicin. These data provided strongevidence that antibiotic treatment can alter the underlying air-way inflammation in bronchiectasis providing hope of improvingclinical symptoms and the prognosis of the disease. This study
Figure 4. The relationship between airway inflammation and radiologic severity (CT scan scoring). Median (boxes) with interquartile range (bars) are
shown. TNF ¼ tumor necrosis factor.
662 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 186 2012

provides the basis for future large randomized controlled trials oflong-term antibiotics in non-CF bronchiectasis. A number of tri-als of inhaled and oral antibiotics in non-CF bronchiectasis arenow underway. To date, results of trials of long-term antibioticsin non-CF bronchiectasis have produced conflicting results, withmany trials limited in terms of sample size and duration. A sys-tematic review of clinical trials published in 2007 reported nobenefit of prolonged antibiotics in bronchiectasis (nine trials in-cluding 378 patients) in terms of reducing exacerbations (OR,0.96; 95% CI, 0.27–3.46) (12). The authors could find no evi-dence on benefits in terms of markers of airway inflammation.A previous study randomized patients with bronchiectasis ina double-blind placebo-controlled study to erythromycin or pla-cebo and found no benefit of antibiotic treatment on airwayinflammatory markers, including IL-1a, IL-8, TNF-a, andleukotriene B4 (13). Conversely Hill and coworkers (16) showedreduced elastase activity in patient’s sputum after treatmentwith amoxicillin. A study of nebulized gentamicin demonstratedreduced levels of MPO with nebulized antibiotics and mostrecently our group demonstrated reduced MPO and elastaselevels in patients treated with nebulized gentamicin (14, 15).An important finding of the present study was that inflamma-tory markers returned to baseline in patients treated with neb-ulized gentamicin 3 months after cessation of treatment. Thissuggests that to maintain efficacy, treatment has to be continu-ous or to have off-drug intervals of less than 3 months. This isimportant for designing future antibiotic interventions.
One of the goals of this study was to demonstrate that bacte-rial clearance with antibiotics reduced markers of airway inflam-mation. This provides strong evidence first that bacterialcolonization directly influences airway inflammation, rather thanreflecting the underlying lung damage, which should not beaffected by antibiotics. Second, it provides a basis for futurelarge trials of long-term antibiotic therapy. If bacterial infectiondirectly contributes to airway inflammation and independentlypredicts exacerbations and hospitalization for severe exacerbations,
long-term antibiotic treatment should be expected to improvethe long-term prognosis of the disease and quality of life (26,27). A recent study has demonstrated that chronic bacterialcolonization, severe exacerbations, and systemic inflammationwere all associated with more rapid lung function decline over24 months (28). Our data suggest that these three importantphenomena are closely linked.
Bronchiectasis has been described as an “orphan” disease. Incontrast to CF, where guidelines recommend the use of surveil-lance sputum cultures and the evidence base for suppressive an-tibiotic therapy is strong (29), there is no such standard of care innon-CF bronchiectasis. The British Thoracic Society has recentlypublished guidelines for the management of non-CF bronchiec-tasis (4) that includes recommendations to monitor sputumcultures when patients are stable and to consider long-term anti-biotic therapy in patients with frequent exacerbations. These rec-ommendations are based on expert opinion and there is a clearneed for studies specifically in non-CF bronchiectasis.
Our study strongly supports the use of surveillance bacteriol-ogy in stable patients with non-CF bronchiectasis, becausebacterial colonization predicts future exacerbation risk, hospital-izations, and quality of life. Furthermore, our study providesevidence to support antibiotic treatment in stable patients be-cause short- and long-term antibiotic treatment is associated withreduced airways and systemic inflammation.
The relationship between airway bacterial load and airway in-flammation is recognized in chronic obstructive pulmonary dis-ease where several studies have demonstrated a progressiveincrease in MPO, elastase, and proinflammatory cytokines withincreasing bacterial load (10). The data reported in this study aresupported by Angrill and coworkers (9), who performed bron-choalveolar lavage on 49 patients with non-CF bronchiectasisand demonstrated an increase in neutrophil numbers, MPO,elastase, and cytokines in patients with bronchiectasis comparedwith control subjects along with an increase in these markerswith increasing bacterial load in bronchoalveolar lavage fluid.
Figure 5. Outpatient exacerbations, un-
scheduled hospital admissions, and symptom
questionnaires after 1 year of follow-up. Dataare presented as mean and standard er-
ror for outpatient exacerbations, and box
plots show median with interquartile
range with the whiskers representingthe minimum and maximum values for
symptom questionnaires. For unscheduled
hospital admissions, data are presented as
percentage of patients hospitalized duringfollow-up. *P , 0.05, **P , 0.01, ***P ,0.0001. LCQ ¼ Leicester Cough Question-
naire; SGRQ ¼ St. Georges RespiratoryQuestionnaire.
Chalmers, Smith, McHugh, et al.: Antibiotic Treatment Reduces Inflammation in Bronchiectasis 663

The present study expands on this previous work by demon-strating the importance of bacterial colonization in a large cohortof patients with exclusively non-CF bronchiectasis. The advan-tage of this large cohort was the ability to adjust for other poten-tial modifiers of inflammation, such as the severity of radiologiclung disease and airflow obstruction. Even after accounting forthese variables, patients with high bacterial loads had higherlevels of airway inflammation.
We expand on the data in stable patients by demonstrating inpatients with exacerbations of bronchiectasis that antibiotictreatment for 14 days results in a significant reduction in airwayand systemic inflammation.
Bronchiectasis is a neutrophil-driven inflammatory disorder(1–3). Release of proinflammatory cytokines, such as IL-1b,IL-8, TNF-a, and leukotriene B4, in the airway promotes neu-trophil recruitment from the peripheral circulation (30). Proin-flammatory cytokines, particularly TNF-a and IL-1b, increase theexpression of ICAM-1 and E-selectin on vascular endothelial cells(30). Activation of CD11/CD18 on circulating neutrophils allowsneutrophils to adhere to these ligands on the inflamed endothe-lium leading to neutrophil migration (31).
In this study we measured ICAM-1, E-selectin, and VCAM-1 as soluble vascular adhesion molecules. Because bacterialload was associated with markers of neutrophil-mediated air-way inflammation, we hypothesized that bacterial colonizationwould promote neutrophil recruitment through up-regulationof adhesion markers. Previous studies have shown that thesemarkers are elevated in patients with bronchiectasis comparedwith control subjects and that they are elevated in other infla-mmatory lung diseases including chronic obstructive pulmo-nary disease and CF (19–21). Our data showed that ICAM-1was elevated in patients with bronchiectasis compared withmatched control subjects and that E-selectin and VCAM-1were also elevated at bacterial loads of 107 cfu/ml or greater.These data suggest that even during clinical stability there isan increased drive to recruit leukocytes to the airway, contrib-uting to the cycle of inflammation. These findings may haverelevance beyond airway inflammation because raised levelsof endothelium-derived inflammatory markers (particularlyICAM-1) have been linked to an increased frequency of myo-cardial infarction (32), stroke (33), and diabetes (34), which areincreased in patients with chronic lung disease, in addition topredicting lung function decline (35). The finding that thismarker decreases with antibiotic treatment is an interesting areafor further research.
It should be noted that although this study found a significantrelationship between airway cytokines and neutrophil markerswith bacterial load, the overlap between the groups was largeand the role of these markers in clinical practice is unclear.
Conclusions
Chronic colonization with high bacterial loads in non-CF bron-chiectasis is associated with airway and systemic inflammation,a greater risk of exacerbations, and worse health-related qualityof life. Short- and long-term antibiotic therapy reduces markersof airway and systemic inflammation. This study highlights theimportance of monitoring sputum bacteriology when clinicallystable and provides the evidence base for future interventionstudies to reduce the bacterial burden in the airways.
Author disclosures are available with the text of this article at www.atsjournals.org.
References
1. Cole PJ. Inflammation: a two-edged sword–the model of bronchiectasis.
Eur J Respir Dis Suppl 1986;147:6–15.
2. Fuschillo S, De Felice A, Balzano G. Mucosal inflammation in idiopathic
bronchiectasis: cellular and molecular mechanisms. Eur Respir J 2008;
31:396–406.
3. Watt AP, Brown V, Courtney J, Kelly M, Garske L, Elborn JS, Ennis M.
Neutrophil apoptosis, proinflammatory mediators and cell counts in
bronchiectasis. Thorax 2004;59:231–236.
4. Pasteur MC, Bilton D, Hill AT. British Thoracic Society guideline for
non-CF bronchiectasis. Thorax 2010; 65(Suppl 1):1–58.
5. Sagel SD, Kapsner R, Osberg I, Sontag MK, Accurso FJ. Airway in-
flammation in children with cystic fibrosis and healthy children assessed
by sputum induction. Am J Respir Crit Care Med 2011;164:1425–1431.
6. Ordonez CL, Henig NR, Mayer-Hamblett N, Accurso FJ, Burns JL,
Chmiel JF, Daines CL, Gibson RL, McNamara S, Retsch-Bogart GZ,
et al. Inflammatory and microbiologic markers in induced sputum
after intravenous antibiotics in cystic fibrosis. Am J Respir Crit Care
Med 2003;168:1471–1475.
7. Downey DG, Brockbank S, Martin SL, Ennis M, Elborn JS. The effect
of treatment of cystic fibrosis pulmonary exacerbations on airways
and systemic inflammation. Pediatr Pulmonol 2007;42:729–735.
8. O’Donnell AE, Barker AF, Ilowite JS, Fick RB. Treatment of idiopathic
bronchiectasis with aerosolized recombinant human DNase. rhDNase
study group. Chest 1998;133:1329–1334.
9. Angrill J, Agusti C, De Celis R, Filella X, Rano A, Elena M, De La
Bellacasa JP, Xaubet A, Torres A. Bronchial inflammation and col-
onization in patients with clinically stable bronchiectasis. Am J Respir
Crit Care Med 2001;164:1628–1632.
10. Hill AT, Campbell EJ, Hill SL, Bayley D, Stockley RA. Association
between airway bacterial load and markers of airway inflammation in
patients with stable chronic bronchitis. Am J Med 2000;109:288–295.
11. Wilson CB, Jones PW, O’Leary CJ, Hansell DM, Dowling RB, Cole PJ,
Wilson R. Systemic markers of inflammation in stable bronchiectasis.
Eur Respir J 1998;12:820–824.
12. Evans DJ, Bara AI, Greenstone M. Prolonged antibiotics for purulent
bronchiectasis in children and adults. Cochrane Database Syst Rev
2007;18:CD001392.
13. Tsang KW, Ho PL, Chan KN, Ip MS, Lam WK, Ho CS, Yuen KY, Ooi
GC, Amitani R, Tanaka E. A pilot study of low-dose erythromycin in
bronchiectasis. Eur Respir J 1999;13:361–364.
14. Murray MP, Govan JR, Doherty CJ, Simpson AJ, Wilkinson TS,
Chalmers JD, Greening AP, Haslett C, Hill AT. A randomized
controlled trial of nebulized gentamicin in non-cystic fibrosis bron-
chiectasis. Am J Respir Crit Care Med 2010;183:491–499.
15. Lin HC, Cheng HF, Wang CH, Liu CY, Yu CT, Kuo HP. Inhaled
gentamicin reduces airway neutrophil activity and mucus secretion in
bronchiectasis. Am J Respir Crit Care Med 1997;155:2024–2029.
16. Hill SL, Burnett D, Hewetson KA, Stockley RA. The response of
patients with purulent bronchiectasis to antibiotics for four months.Q
J Med 1988;66:163–173.
17. Chalmers JD, Mandal P, McHugh B, Smith M, Doherty C, Govan JR, Hill
AT. The relationship between airway bacterial load and airways in-
flammation in stable non-cystic fibrosis bronchiectasis. Presented at the
European Respiratory Society Annual Congress. September 24–28,
2011, Amsterdam. Abstract 1927.
18. Stockley RA, Bayley DL. Validation of assays for inflammatory medi-
ators in sputum. Eur Respir J 2000;15:778–781.
19. Zheng L, Tipoe G, Lam WK, Leung RY, Ho JC, Shum IH, Ooi GC, Ip
MS, Tsang KW. Up-regulation of circulating adhesion molecules in
bronchiectasis. Eur Respir J 2000;16:691–696.
20. De Rose V, Oliva A, Messore B, Grosso B, Mollar C, Pozzi E. Circu-
lating adhesion molecules in cystic fibrosis. Am J Respir Crit Care
Med 1998;157:1234–1239.
21. Riise GC, Larsson S, Lofdahl CG, Andersson BA. Circulating cell ad-
hesion molecules in bronchial lavage and serum in COPD patients
with chronic bronchitis. Eur Respir J 1994;7:1673–1677.
22. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A,
Crapo R, Enright P, van der Grinten CP, Gustafsson P, et al. Stand-
ardisation of spirometry. Eur Respir J 2005;26:319–338.
23. Wilson CB, Jones PW, O’Leary CJ, Cole PJ, Wilson R. Validation of the
St. Georges Respiratory Questionnaire in bronchiectasis. Am J Respir
Crit Care Med 1997;156:536–541.
664 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 186 2012

24. Murray MP, Turnbull K, MacQuarrie S, Hill AT. Validation of the
Leicester Cough Questionnaire in non-cystic fibrosis bronchiectasis.
Eur Respir J 2009;34:125–131.
25. Pasteur MC, Helliwell SM, Houghton SJ, Webb SC, Foweraker JE,
Coulden RA, Flower CD, Bilton D, Keogan MT. An investigation
into causative factors in patients with bronchiectasis. Am J Respir Crit
Care Med 2000;162:1277–1284.
26. Loebinger MR, Wells AU, Hansell DM, Chinyanganya N, Devaraj A,
Meister M, Wilson R. Mortality in bronchiectasis: a long-term study
assessing the factors influencing survival. Eur Respir J 2009;34:843–849.
27. Wilson CB, Jones PW, O’Leary CJ, Hansell DM, Cole PJ, Wilson R.
Effect of sputum bacteriology on the quality of life of patients with
bronchiectasis. Eur Respir J 1997;10:1754–1760.
28. Martinez-Garcia MA, Soler-Cataluna JJ, Perpina-Tordera M, Roman-
Sanchez P, Soriano J. Factors associated with lung function decline in
adult patients with stable non-cystic fibrosis bronchiectasis. Chest
2007;132:1565–1572.
29. Flume PA, O’Sullivan BP, Robinson KA, Goss CH, Mogayzel PJ Jr,
Willey-Courand DB, Bujan J, Finder J, Lester M, Quittell L, et al.
Cystic fibrosis pulmonary guidelines: chronic medications for main-
tenance of lung health. Am J Respir Crit Care Med 2007;176:957–969.
30. Stockley RA, Shaw J, Hill SL, Burnett D. Neutrophil chemotaxis in
bronchiectasis: a study of peripheral cells and lung secretions. Clin Sci
(Lond) 1988;74:645–650.
31. Downey DG, Bell SC, Elborn JS. Neutrophils in cystic fibrosis. Thorax
2009;64:81–88.
32. Ridker PM, Hennekens CH, Roitman-Johnson B, Stampfer MJ, Allen J.
Plasma concentration of soluble intercellular adhesion molecule-1 and
risks of future myocardial infarction in apparently healthy men. Lancet
1998;351:88–92.
33. Fassbender K, Bertsch T, Mielke O, Muhlhauser F, Hennerici M. Ad-
hesion molecules in cerebrovascular diseases. Evidence for an in-
flammatory endothelial activation in cerebral large-and small-vessel
disease. Stroke 1999;30:1647–1650.
34. Song Y, Manson JE, Tinker L, Rifai N, Cook NR, Hu FB, Hotamisligil
GS, Ridker PM, Rodriguez BL, Margolis KL, et al. Circulating levels
of endothelial adhesion molecules and risk of diabetes in an ethnically
diverse cohort of women. Diabetes 2007;56:1898–1904.
35. Walter RE, Wilk JB, Larson MG, Vasan RS, Keaney JF Jr, Lipinska I,
O’Connor GT, Benjamin EJ. Systemic inflammation and COPD: the
Framingham Heart Study. Chest 2008;133:19–25.
Chalmers, Smith, McHugh, et al.: Antibiotic Treatment Reduces Inflammation in Bronchiectasis 665