shifting the balance of care: great expectations
TRANSCRIPT

Candace Imison, Director of Policy, Nuffield Trust
Shifting the balance of
care Great expectations

A long term ambition
2
“The general availability of medical
services can only be effected by new
and extended organisation,
distributed according to the needs of
the community. This organisation is
needed on grounds of efficiency and
cost, and is necessary alike in the
interest of the public and of the
medical profession.”
Interim Report on the Future Provision of
Medical and Allied Services (Dawson
1920)
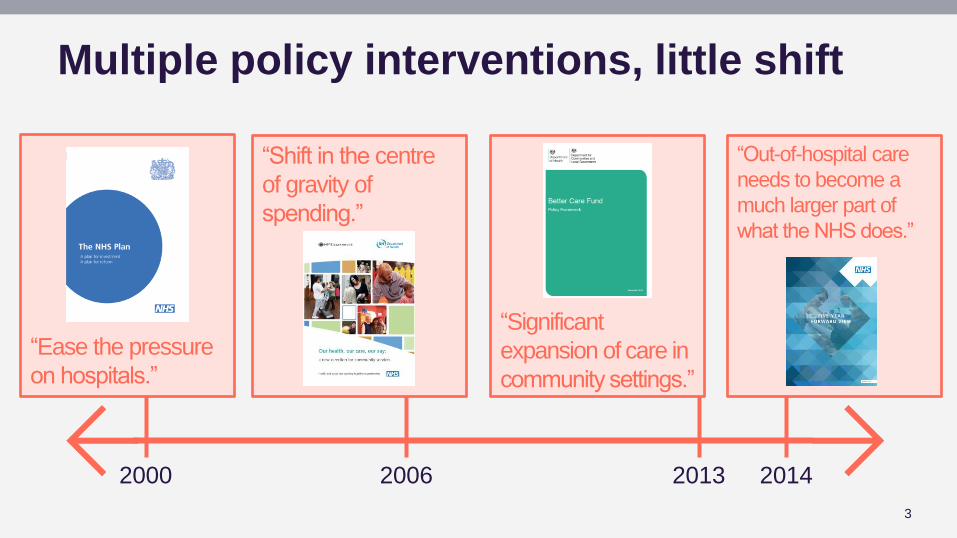
Multiple policy interventions, little shift
3
2000 2006 2013 2014
“Shift in the centre
of gravity of
spending.”
“Significant
expansion of care in
community settings.”
“Out-of-hospital care
needs to become a
much larger part of
what the NHS does.”
“Ease the pressure
on hospitals.”

Multiple policy interventions, little shift
4
2000 2006 2013 2014
“Shift in the centre
of gravity of
spending.”
“Significant
expansion of care in
community settings.”
“Out-of-hospital care
needs to become a
much larger part of
what the NHS does.”
“Ease the pressure
on hospitals.”
£4bn of
£22bn
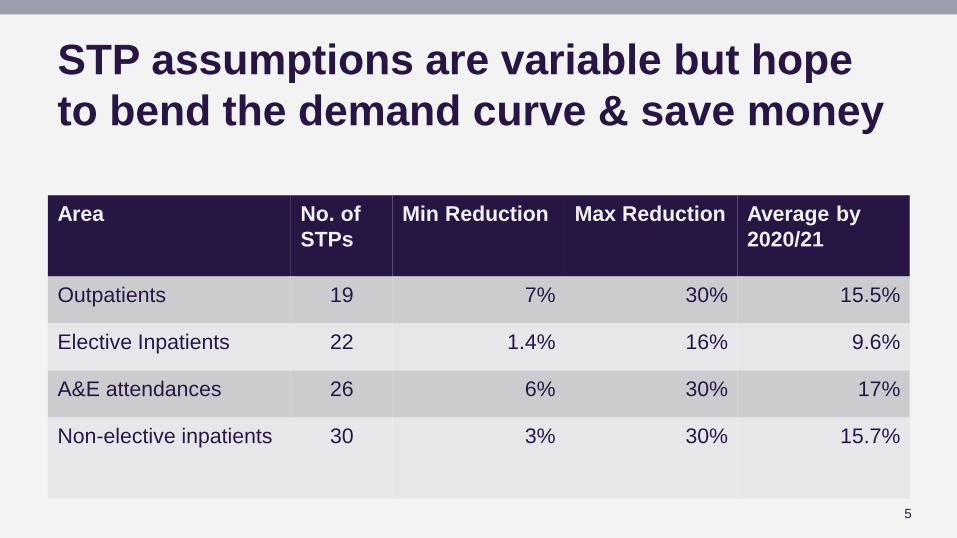
STP assumptions are variable but hope
to bend the demand curve & save money
5
Area No. of
STPs
Min Reduction Max Reduction Average by
2020/21
Outpatients 19 7% 30% 15.5%
Elective Inpatients 22 1.4% 16% 9.6%
A&E attendances 26 6% 30% 17%
Non-elective inpatients 30 3% 30% 15.7%

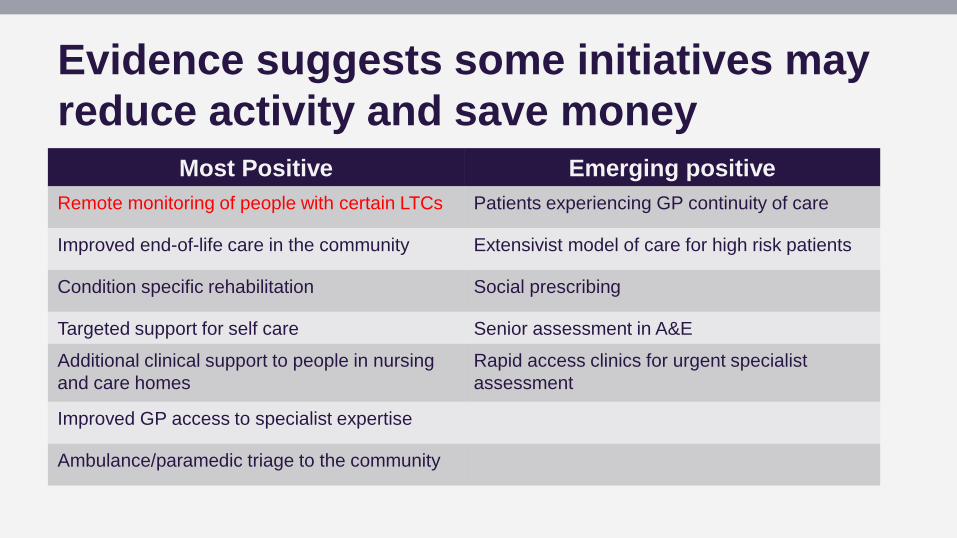
Evidence suggests some initiatives may
reduce activity and save money
Most Positive Emerging positive
Remote monitoring of people with certain LTCs Patients experiencing GP continuity of care
Improved end-of-life care in the community Extensivist model of care for high risk patients
Condition specific rehabilitation Social prescribing
Targeted support for self care Senior assessment in A&E
Additional clinical support to people in nursing
and care homes
Rapid access clinics for urgent specialist
assessment
Improved GP access to specialist expertise
Ambulance/paramedic triage to the community
Evidence suggests some initiatives may
reduce activity and save money
Most Positive Emerging positive
Remote monitoring of people with certain LTCs Patients experiencing GP continuity of care
Improved end-of-life care in the community Extensivist model of care for high risk patients
Condition specific rehabilitation Social prescribing
Targeted support for self care Senior assessment in A&E
Additional clinical support to people in nursing
and care homes
Rapid access clinics for urgent specialist
assessment
Improved GP access to specialist expertise
Ambulance/paramedic triage to the community

Evidence suggests some initiatives may
reduce activity and save money
Most Positive Emerging positive
Remote monitoring of people with certain LTCs Patients experiencing GP continuity of care
Improved end-of-life care in the community Extensivist model of care for high risk patients
Condition specific rehabilitation Social prescribing
Targeted support for self care Senior assessment in A&E
Additional clinical support to people in nursing
and care homes
Rapid access clinics for urgent specialist
assessment
Improved GP access to specialist expertise
Ambulance/paramedic triage to the community
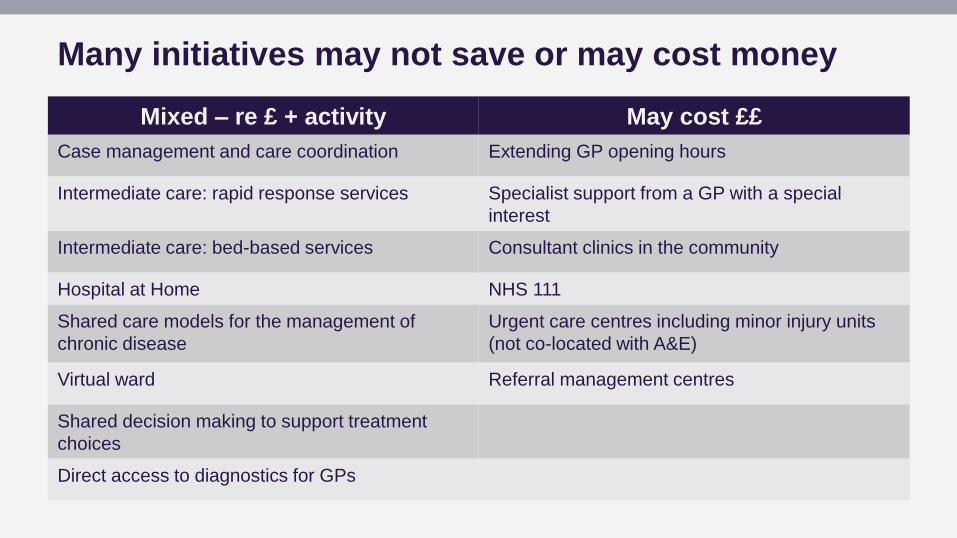
Many initiatives may not save or may cost money
Mixed – re £ + activity May cost ££
Case management and care coordination Extending GP opening hours
Intermediate care: rapid response services Specialist support from a GP with a special
interest
Intermediate care: bed-based services Consultant clinics in the community
Hospital at Home NHS 111
Shared care models for the management of
chronic disease
Urgent care centres including minor injury units
(not co-located with A&E)
Virtual ward Referral management centres
Shared decision making to support treatment
choices
Direct access to diagnostics for GPs

Many initiatives may not save or may cost money
Mixed – re £ + activity May cost ££
Case management and care coordination Extending GP opening hours
Intermediate care: rapid response services Specialist support from a GP with a special
interest
Intermediate care: bed-based services Consultant clinics in the community
Hospital at Home NHS 111
Shared care models for the management of
chronic disease
Urgent care centres including minor injury units
(not co-located with A&E)
Virtual ward Referral management centres
Shared decision making to support treatment
choices
Direct access to diagnostics for GPs

Many initiatives may not save or may cost money
Mixed – re £ + activity May cost ££
Case management and care coordination Extending GP opening hours
Intermediate care: rapid response services Specialist support from a GP with a special
interest
Intermediate care: bed-based services Consultant clinics in the community
Hospital at Home NHS 111
Shared care models for the management of
chronic disease
Urgent care centres including minor injury units
(not co-located with A&E)
Virtual ward Referral management centres
Shared decision making to support treatment
choices
Direct access to diagnostics for GPs

What do systems leaders think?
12
Care in the community is cheaper and provides better
care for patients. 38%
Care in the community provides better care for
patients but is not cheaper. 38%
Care in the community is cheaper but does not provide better care for
patients. 3%
Care in the community is neither cheaper nor
provides better care for patients.
7%
I am not sure. 14%
With regard to moving care out of hospitals, which of the following statements most accurately reflects your view?
(n=58)

9%
25%
26%
40%
Risk stratification: not the whole solution
• Regression to mean
• Requires holistic view of patient
• Patient’s capacity to engage
• Need very high impact on those at greatest risk to have impact overall
Adapted from: Roland and Abel, 2012
High relative risk (x 5.5)
Very high relative risk (X 18.6)
Moderate relative risk (x1.7)
Low relative risk (x0.5)
Case management
Disease management
Supported self care
Prevention and
wellness promotion
13
% Total Emergency Admissions X Average rate of
emergency
admission
The gap between theory and practice
“Improvement initiatives are sometimes planned on the hard high ground, but are put into effect in the swampy lowlands.”
- Marshall and others, 2016
© Kenneth Allen

Implementation needs to take wide range
of factors into account
• Requires rigorous framing of the problem and contextual factors that could influence feasibility and effectiveness
• Including influencing professional behaviour such as attitudes to risk
Source: Imison and others, 2012 15
Bed use
System governance factors
• Governance models
• Commissioner behaviour/ relationships
• Provider behaviour/ relationships
• Staff beliefs and values
• Leadership
Hospital factors (supply side)
• Access (rurality)
• Internal processes – admission, treatment and discharge
Community factors
• Primary care supply and capacity
• Community care supply and capacity
• Local authority care supply and capacity
Patient factors (demand side)
• Age
• Socioeconomic status
• Sex
• Health needs
• Beliefs and values

Why is it so hard to release savings from
shifting care?
16
• Lower unit costs in community does not mean lower costs overall. Price Cost
• Additional services supply- induced demand
• Care coordination can cost more than it saves
• Targeting overuse can expose underuse 0
4
0 2 4
Co
st
(£)
Level of activity

Community
An unequal battle?
Hospital
17

Community
An unequal battle?
Hospital
18
No funding
to support
transition
Primary and community care facing
significant challenges
19
• 1/3 GP practices have a vacancy for at least one partner
• 2016 - NHS England identified 20% GP practices as vulnerable
• 1/5 district nurse posts vacant

Will economic impact only be visible
when we have whole system change?
20
• A more radical approach needed?
• Initiatives have been too small and underpowered?
• Unsupported by wider system incentives
• Lack of time
• Inappropriate measures of success
Conclusion
21
• The NHS is undertaking the herculean task of changing its modus operandi at the same time as experiencing the leanest years in its history.
• Nobody can argue against the principle of better, more appropriate care closer to home.
• But we cannot assume that this will save money, especially in the short term.
• To succeed, we need a relentless focus on what works
• Crucially, to admit when the funding envelope simply isn’t big enough to deliver the transformation needed.
www.nuffieldtrust.org.uk
Follow us on Twitter – twitter.com/NuffieldTrust
Sign up for our newsletter – www.nuffieldtrust.org.uk/newsletter-signup